a study of the relation between health attitudes, values …
TRANSCRIPT

ASTUDYOFTHERELATIONBETWEENHEALTHATTITUDES,VALUESANDBELIEFSANDHELP‐SEEKINGBEHAVIOURWITHSPECIALREFERENCETOAREPRESENTATIVESAMPLEOFBLACKPATIENTSATTENDINGAGENERAL
HOSPITALby
BASILJOSEPHPILLAY
submittedinpartialfulfilmentoftherequirementsforthedegreeof
DOCTOROFPHILOSOPHY
intheSub‐DepartmentofMedicallyAppliedPsychology,FacultyofMedicine,UniversityofNatal
1993

ii
ABSTRACT
Thereisstrongevidencesupportingtheviewthatbeliefsandattitudesinfluencehealth
behaviour.Furthermore,culturalandsocialbeliefsalsohavebeenshowntoinfluencethe
wayhealthcarefacilitiesareused.Althoughwesternmedicineplaysadominantroleinthe
masscontrolofdisease,traditionalorfolkmedicinecontinuestoplayanimportantrolein
thehealthcareofblackcommunities.Theytherefore,possessuniqueattitudes,valuesand
beliefsabouthealthandillnesswhichintegrallyinfluencetheirhealthbehaviour.
Thisstudyaimsthereforeto:understandphenomenologicallytheurbanAfrican’s
perceptionofillness,diseaseandhealth;identifyattitudesthatdirectlyinfluencehealth
behaviour:identify“triggerfactors”thatprecipitatehealthactionandisolatefactorsthat
contributeto“negative”healthbehaviour.
Thesampleinthisstudyconsistedof3groupsofurbanAfricanswhowere20yearsand
older.Group1comprisedfirsttimeattenderstoamedicaloutpatientsdepartmentGroup2
andGroup3weresamplegroupsdrawnfromtheUmlaziTownshipandtheKwaMashu
Townshiprespectively.TheHealthandIllnessBatteryinthelanguageoftheparticipants
wereadministeredbytrainedinterviewers.
Thisstudyhasdemonstratedthefollowing:urbanAfricanshaveapersonalconceptionof
illness,healthanddiseasethatinfluencestheirmannerofhelp‐seeking;therearecertain
attitudesandbeliefsthatdirectlyinfluencebothpositiveandnegativehealthbehaviour;.
thereareseveralhealthbeliefswhichinteractinacomplexwayandmayleadtomedical
help‐seeking.Healthactionwasfoundtobeinfluencedbysignificantindividualsinthe
subject'senvironment;demographicvariables,suchas,age,sex,educationandurbanisation
stronglyinfluencethehealthandillnessbeliefs;theseresultsvalidatedsomeofthe

iii
fundamentalaspectsofthecommonwesternhealthandillnessmodels;theuseofservices
andfacilitiesaredeterminedbythelocation,accessibilityandthequalityofservices;
financialcosts,time,transport,lackofcommunitysupports,negativelyaffectedhelp‐
seeking;symptomshavebeenidentifiedasa“triggerfactor”ofhelp‐seeking.Individualsuse
otherformsoftreatmentsindependentofmedicaltreatments.Amodelofhelp‐seekingfor
urbanAfricansisproposed.

iv
PREFACE
Thisstudyrepresentsoriginalworkbytheauthorandhasnotbeensubmittedinanyformto
anotherUniversity.Whereusewasmadeoftheworkofothersithasbeenduly
acknowledgedinthetext.
ThisresearchdescribedinthisthesiswascarriedoutatKingEdwardVIIIHospital,Durban,
SouthAfricaandintheSub‐DepartmentofMedicallyAppliedPsychology,Departmentof
Psychiatry,FacultyofMedicine,UniversityofNatal,underthesupervisionofProfessorL
Schlebusch.
Inthisresearchthestatisticalplanningandanalysis,andrecommendationsarisingfrom
theseanalyses,havebeendonewiththesupportoftheInstituteforBiostatisticsofthe
MedicalResearchCouncil.ThisresearchwasalsopartiallyfundedbyaMedicalResearch
CouncilPostGraduateScholarship.

v
ACKNOWLEDGEMENTS
Iamindebtedtomanypeoplewhohavegreatlyassistedmyresearchandsupportedme
duringthepreparationofthisthesis.
ImustespeciallythankmypromoterProfessorL.Schlebusch,ProfessorandHeadofthe
Sub‐DepartmentofMedicallyAppliedPsychology,FacultyofMedicine,UniversityofNatal,
whoseadviceandcontinuedsupportIhavegreatlybenefitedfrom.
TheotherswhoImustmentionare:
ProfessorW.H.Wessels,ProfessorandHeadofPsychiatry,FacultyofMedicine,University
ofNatal.
DrA.J.Lasich,DeputyHeadofPsychiatry,FacultyofMedicine,UniversityofNatal.
DrM.Nair,PrincipalPsychiatristandHeadofPsychiatry,KingEdwardVIIIHospital.
DrJ.Ndlovu,Psychiatristinprivatepractice.
DrT.Mayekiso,SeniorLecturerandClinicalPsychologist,DepartmentofPsychology,
UniversityofTranskei,Transkei.

vi
MsR.Eiselen,SeniorLecturerandStatistician,DepartmentofStatistics,UniversityofSouth
Africa.
DrP.J.BeckerandMsE.Gouws,InstituteforBiostatisticsoftheMedicalResearchCouncil,
Durban.
ThesuperintendentsofKingEdwardVIIIHospitalforpermissiontoconductthisresearchin
thehospital.
MrB.Rortarg,TownPlanner,ScottWilsonKirkpatrickAssociates,Durban.
MrE.N.Iyer,TownPlanningTechnician,PaulMitkula&Associates,Durban.
DrL.Khan,SeniorLecturer,DepartmentofLandSurveying,UniversityofNatal.
MsL.RichmanandMrD.R.Sawyer,CentralStatisticalService,Durban,Departmentof
HomeAffairs.
NazereneJob,DianneJob,SelvumJ.Abel,RobinAbel,JenniferS.Madhan,JennetS.Hansen,
GeraldJPillay,NirmalaPillayandMarkNaidoo
Mymumandlatedadfortheirsupportandencouragement
Mywife,Cecilia,andchildren,Loren‐JosephandCassandraSuminthra,Iamalwaysgrateful
fortheirpatience,encouragementandsacrificesinorderformetocompletethisresearch.

vii
TABLEOFCONTENTS
CHAPTER1
INTRODUCTION ...................................................................................................................... 1
CHAPTER2
PSYCHOLOGYANDHEALTH .................................................................................................... 8
2.1PSYCHOLOGICALCONCEPTSINHEALTHANDILLNESS ....................................... 12
2.1.1 HEALTH,ILLNESS,ANDDISEASE......................................................... 12
2.1.2 SOMESPECIFICTYPESOFHEALTHBEHAVIOUR................................. 14
2.1.2.1PreventativeBehaviour ......................................................... 14
2.1.2.2HealthProtectiveBehaviour.................................................. 15
2.1.2.3IllnessBehaviour .................................................................... 15
2.1.2.4SickRoleBehaviour................................................................ 16
2.2HEALTHBELIEFS,ATTITUDESANDVALUES......................................................... 17
2.3MODELSOFHEALTH‐RELATEDBEHAVIOUR ....................................................... 18
2.3.1 THEHEALTHBELIEFMODEL............................................................... 18
2.3.2 KASLANDCOBB'SMODEL ................................................................. 20
2.3.3 SUCHMAN'SMODEL ......................................................................... 21
2.3.4 FABREGA'SMODEL ............................................................................ 23
2.3.5 MECHANIC'SMODEL.......................................................................... 24

viii
2.3.6 ANDERSEN'SMODEL.......................................................................... 26
2.3.7 SOCIALLEARNINGTHEORY ................................................................ 26
2.4CRITICALISSUESINHEALTHBEHAVIOUR............................................................ 29
2.4.1 PERSONALANDDEMOGRAPHIC........................................................ 29
2.4.2 HEALTHBELIEFS ................................................................................. 31
2.5SOCIALSUPPORTANDHEALTH........................................................................... 32
2.6SYMPTOMSANDSYMPTOMPERCEPTION.......................................................... 33
2.7LIFEEVENTS,STRESSANDILLNESS ..................................................................... 34
CHAPTER3
HEALTHINSOUTHAFRICA..................................................................................................... 40
3.1CULTURALINFLUENCESONHEALTH................................................................... 44
3.2AETIOLOGYOFILLNESSINTHEAFRICANWORLDVIEW ..................................... 47
3.2.1 EnvironmentalImbalance.................................................................. 47
3.2.2 SorceryandIllness ............................................................................. 48
3.2.3 AncestorsandIllness ......................................................................... 49
3.2.4 Umnyama andIllness......................................................................... 51
3.3ILLNESS,SICK‐ROLEANDHELP‐SEEKINGBEHAVIOUR........................................ 52
3.4TRADITIONALTREATMENTS ............................................................................... 54
CHAPTER4
METHOD ............................................................................................................................... 57
4.1SUBJECTS ............................................................................................................ 57
4.1.1 GeneralHospitalGroup ..................................................................... 60
4.1.1 CommunityGroups............................................................................ 61
4.2METHODOFDATACOLLECTION......................................................................... 62
4.2.1 HospitalGroup................................................................................... 62

ix
4.2.2 CommunityGroup ............................................................................. 63
4.3MATERIALS.......................................................................................................... 64
4.3.1 HealthandIllnessQuestionnaire(HIQ) ............................................. 65
4.3.2 HealthBeliefQuestionnaire(HBQ) .................................................... 66
4.3.2.1ConstructionofQuestionnaire .............................................. 67
4.3.3 SocialSupportQuestionnaire(SSQ)................................................... 67
4.3.3.1ConstructionofQuestionnaire .............................................. 68
4.3.4 SymptomInventory(SI) ..................................................................... 69
4.3.5 LifeExperienceSurvey(LES) .............................................................. 70
4.4TRANSLATIONOFQUESTIONNAIRES .................................................................. 70
4.5PILOTSTUDY ....................................................................................................... 72
CHAPTER5
RESULTS................................................................................................................................. 73
5.1DEMOGRAPHICDATA ......................................................................................... 73
5.2TIMEANDTRANSPORTCOSTSOFHOSPITALPATIENTS ..................................... 83
5.3HELPSEEKINGBEHAVIOUROFHOSPITALPATIENTS .......................................... 83
5.3.1 ChoiceofDaytoAttend..................................................................... 84
5.3.2 Patient'sFirstSuspicionsofIllnessandAttendance.......................... 84
5.3.3 PatientsReasonsfornotAttendingEarlier........................................ 87
5.3.4 Feelingsorexperiencesthatsuggestedtothepatientsthat
theywereIll ....................................................................................... 87
5.3.5 IllnessDisclosure................................................................................ 89
5.4SERVICES ............................................................................................................. 90
5.4.1 Choiceofdoctor,hospitalandpharmacybythecommunity
groups. ............................................................................................... 90
5.5SUBJECTSPERCEPTIONSOFTREATMENT ........................................................... 95
5.6RELIGIOUSANDCULTURALBELIEFS.................................................................... 99
5.7HEALTHANDILLNESSBELIEFS(QUALITATIVERESPONSES) ............................... 105

x
5.7.2 Whatdoesitmeantobesick?.......................................................... 106
5.7.3 Whatdoesitmeantobeill?............................................................. 107
5.7.4 Whatdoesitmeantobewell? ........................................................ 107
5.8ILLNESSBEHAVIOUR ...................................................................................................... 113
5.9HEALTHANDILLNESSBELIEFS ........................................................................... 114
5.10SOCIALSUPPORT............................................................................................. 134
5.10.1 Comparisonsofgroupsonaccessibilityandproximity..................... 139
5.11SYMPTOMPERCEPTIONS................................................................................. 145
5.12SUBJECTSRATINGOFSEVERITYOFSYMPTOMS............................................. 149
5.13EXPERIENCESTRESSORSANDLIFECHANGES .................................................. 151
CHAPTER6
DISCUSSION.......................................................................................................................... 163
6.1HELPSEEKINGBEHAVIOUROFHOSPITALSUBJECTS ......................................... 167
6.2USEOFSERVICESBYCOMMUNITYGROUPS...................................................... 171
6.3HEALTHANDILLNESSBELIEFS(QUALITATIVE)................................................... 178
6.4THEHEALTHANDILLNESSBELIEF(QUANTITATIVE) .......................................... 180
6.5SOCIALSUPPORTANDHEALTH.......................................................................... 188
6.6SYMPTOMPERCEPTIONS................................................................................... 192
6.7STRESSANDHELPSEEKINGBEHAVIOUR ........................................................... 193
6.8ACOMPARISONOFTHERESULTSWITHOTHERHEALTHANDILLNESS
MODELS ........................................................................................................ 195
6.9TOWARDSAMODELOFHEALTHANDILLNESS................................................. 197
6.10SUMMARYANDCONCLUSION......................................................................... 201
REFERENCES ......................................................................................................................... 207

xi
APPENDIX ............................................................................................................................. 231

xii
LISTOFTABLES
TABLEI
DISTRIBUTIONOFSAMPLEBYSEX ........................................................................................ 57
TABLEII
SAMPLESELECTIONFORHOSPITALGROUP .......................................................................... 63
TABLEIII
AGEDISTRIBUTIONOFGROUPS ............................................................................................ 75
TABLEIV
ETHNICDISTRIBUTION........................................................................................................... 76
TABLEV
EDUCATIONALLEVELOFGROUP........................................................................................... 76
TABLEVI
YEARDISTRIBUTIONOFURBANLIVING................................................................................. 77
TABLEVII
DESTINATIONSOFHOSPITALSUBJECTS ................................................................................ 80
TABLEVIII

xiii
SUBJECTSOCCUPATIONS....................................................................................................... 81
TABLEIX
ILLNESSPRECIPITATIONANDATTENDANCETOHOSPITAL ................................................... 85
TABLEX
LOCATIONOFDOCTOR.......................................................................................................... 90
TABLEXI
REASONSFORCHOOSINGADOCTOR ................................................................................... 91
TABLEXII
CHOICEOFHOSPITAL ............................................................................................................ 92
TABLEXIII
REASONSFORCHOOSINGAHOSPITAL ................................................................................. 93
TABLEXIV
CHOICEOFPHARMACY.......................................................................................................... 94
TABLEXV
REASONSFORCHOOSINGAPHARMACY............................................................................... 94
TABLEXVI
SUBJECTSPERCEPTIONSOFTREATMENT.............................................................................. 95
TABLEXVII
TREATMENTFACTORSSUBJECTSWEREPLEASEDABOUT..................................................... 96
TABLEXVIII
TREATMENTFACTORSSUBJECTSWERENOTPLEASEDABOUT............................................. 96
xiv
TABLEXVIX
SOURCESOFMEDICATION .................................................................................................... 97
TABLEXX
SUBJECTSPERCEPTIONSOFWESTERNMEDICINES............................................................... 98
TABLEXXI
REASONSFORTAKINGVITAMINS.......................................................................................... 99
TABLEXXII
RELIGIOUSANDCULTURALBELIEFS ..................................................................................... 100
TABLEXXIII
USEOFTRADITIONALHEALERS. ........................................................................................... 101
TABLEXXIV
TREATMENTGIVEN.............................................................................................................. 101
TABLEXXV
FREQUENCYOFVISITSTOTRADITIONALHEALERS............................................................... 102
TABLEXXVI
SUBJECTSPERCEPTIONSOFTHEEFFECTIVENESSOFTRADITIONAL
TREATMENT.......................................................................................................................... 103
TABLEXXVII
CONTINUATIONOFTRADITIONALTREATMENT................................................................... 103
TABLEXXVIII
PRAYERASATREATMENTFORILLNESS ............................................................................... 104

xv
TABLEXXIX
CONSULTATIONOFHERBALISTS........................................................................................... 104
TABLEXXX
USEOFTRADITIONALOR“LAY”SUBSTANCES...................................................................... 105
TABLEXXXI
MEANINGOFBEINGILL........................................................................................................ 108
TABLEXXXII
MEANINGOFBEINGWELL ................................................................................................... 109
TABLEXXXIII
INDICATORSOFBEINGWELL............................................................................................... 110
TABLEXXXIV
INDICATORSOFBEINGILL .................................................................................................... 111
TABLEXXXV
REASONSPEOPLEGETSICK/ILL ........................................................................................... 112
TABLEXXXVI
ILLNESSBEHAVIOUROFSUBJECTS ....................................................................................... 114
TABLEXXXVII
COMPARISONSOFGROUPSRESPONSESONHBQITEMS(IN%) ........................................ 115
TABLEXXXVIII
MEANSANDSTANDARDDEVIATIONSOFEACHHBQITEMFORGROUP ............................. 127
TABLEXXXIX
xvi
FACTORANALYSISOFTHEHBQ(COMBINED) ...................................................................... 128
TABLEXL
MEANFACTORSCORESONTHENINEFACTORSRELATINGTOHEALTHBELIEF ................... 133
TABLEXLI
COMPARISONSOFSSQITEMSBETWEENGROUPS(in%) .................................................... 135
TABLEXLIV
MEANSANDSTANDARDDEVIATIONSOFSSQITEMSBYGROUPS ...................................... 139
TABLEXLII
ANOVAOFACCESSIBILITYANDPROXIMITY ......................................................................... 140
TABLEXLIII
DUNCAN'SMULTIPLERANGETEST....................................................................................... 141
TABLEXLV
FACTORANALYSISOFTHESSQ(COMBINED) ....................................................................... 142
TABLEXLVI
MANOVAONFACTOR1OFSSQ........................................................................................... 144
TABLEXLVII
MANOVAONFACTOR2OFSSQ........................................................................................... 145
TABLEXLVIII
EXPERIENCEOFSYMPTOMSBYEACHSUBJECTBYGROUP.................................................. 146
TABLEXLIX
MEANANDSTANDARDDEVIATIONOFSEVERITYOFSYMPTOMS ...................................... 149

xvii
TABLEL
EXPERIENCEOFSTRESSORPERGROUP................................................................................ 152
TABLELI
EXTENTOFIMPACTPERGROUP........................................................................................... 156
TABLELII
MANOVAOFTOTALLIFEEXPERIENCESBETWEENGROUPS................................................ 160
TABLELIII
DUNCAN'SMULTIPLERANGETEST....................................................................................... 160
TABLELIV
MANOVAOFNEGATIVELIFEEXPERIENCESBETWEENGROUPS.......................................... 161
TABLELV
DUNCAN'SMULTIPLERANGETESTONNEGATIVELIFEEXPERIENCES.................................. 161
TABLELVI
MANOVAONPOSITIVELIFEEXPERIENCESBETWEENGROUPS........................................... 161
TABLELVII
DUNCAN'SMULTIPLERANGETESTONPOSITIVELIFEEXPERIENCES ................................... 162

xviii
LISTOFFIGURES
Figure1 Conventionalstress‐vulnerabilitymodel ....................................................... 37
Figure2 Elaboratestressmodel .................................................................................. 39
Figure3 TheAfricanconceptofillness........................................................................ 45
Figure4 Sampledistribution ....................................................................................... 58
Figure5 Male‐femaledistributionofthesample........................................................ 59
Figure6 Agedistributionofgroups ............................................................................. 74
Figure7 Educationlevelofgroups .............................................................................. 78
Figure8 Numberofyearslivinginanurbanarea ....................................................... 79
Figure9 Occupationofsubjects .................................................................................. 82
Figure10 Illnessprecipitationandattendancetothehospital ..................................... 86
Figure11 Reasonsfornotattendingthehospitalearlier .............................................. 88
Figure12 ModelofAfricanhelpseekingbehaviour..................................................... 198

xix
GLOSSARY
χ2 ChiSquare
ANC AfricanNationalCongress
ANOVA AnalysisofVariance
CAT ComputerisedAxialTomography
df DegreesofFreedom
Dx Disease
ECG Electrocardiogram
EEG Electroencephalogram
HBM HealthBeliefModel
HBQ HealthBeliefQuestionnaire
HIB HealthandIllnessBattery
HIQ HealthandIllnessQuestionnaire
IFP InkathaFreedomParty
Km Kilometre
LES LifeExperienceSurvey
MANOVA MultivariateAnalysisofVariance
MEDUNSA TheMedicalUniversityofSouthernAfrica
Mn Mean
MRC MedicalResearchCouncil
NAMDA NationalMedicalandDentalAssociation
NEHAWU NationalEducation,HealthandAlliedWorkersUnion
p pvalue
PASA PsychologicalAssociationofSouthAfrica
SD StandardDeviation

xx
SI SymptomInventory
SSQ SocialSupportQuestionnaire
USA UnitedStatesofAmerica
Rx Treatment
Zuluwordsusedinthisthesisareexplainedinthetext.
Boththeterms"black"and"African"willappearinthisthesisandrefertoBlackSouth
Africans."Black"isusedininstances,suchas,"blackgroups"or"blackcommunity"and
"African"isusedmainlyinreferencestothetraditionalAfricanworld‐viewandtoaspects
ofAfricancosmology,asin,"Africanmedicine","Africanillness"and"Africanhealers".

1
CHAPTER1
INTRODUCTION
ThehealthsystemofSouthAfricahasreceivedheightenedattentionbothlocally(Daily
News,9March1990;NationalMedicalandDentalAssociation[NAMDA],1987),and
internationally(AnderssonandMarks,1988;Zwi,MarksandAndersson,1988),largely
becauseithasbeenstronglyinfluencedbythepoliticalsysteminthecountrybasedon
racialseparation.ThehealthserviceshereareacombinationofbothFirstandThirdWorld
medicalpractice.Thesolutionssuggestedwithregardtotheunificationofhealth
departmentsandtheimprovementofthehealthsystemhavemainlydealtwithissues
suchaspoliticalchange,thesharingofpoliticalandeconomicpowerandtheequalization
ofeducation,housing,employmentandwages.Allthesechangeshavedirect
consequencesforthehealthcare(Price,1988)andwouldhavetheeffectofequalizing
healthcarefacilitiesandovercomingpresentobstaclestoeffectivecare,suchas,the
affordabilityofhealthcareandthemaldistributionofhealthworkersandfacilities.
Butthereisanother,lessobvious,obstaclethatendemicallyaffectsthecareandhealing
processwhichcannotbeignoredinthepresentconcerntoimprovethehealthsystem.
ForthemajorityoftheSouthAfricanpopulation,whoareblackandsociallydisinherited,
thepracticeofwesternmedicineis“alien”inmanyways.Thisgrosslyneglectedareahas
todowithanaspectofthepsychologicaldimensionofhealthandisthesubjectofthis
study.Inordertoobtainmaximumutilisationandbenefitofthehealthsystemitisof

2
primeimportancetounderstandtheblackpatient'svieworpsychologicalperceptionof
healthandillness.Althoughwesternmedicineplaysadominantroleinthemasscontrolof
disease,traditionalorfolkmedicinecontinuestoplayanimportantroleinthehealthcare
ofblackcommunitieshereandintherestofAfrica.Individuals,inblackcommunities,
therefore,possessuniqueattitudes,valuesandbeliefsabouthealthandillnesswhich
integrallyinfluencetheirhealthbehaviour.Healthbehaviour,accordingtoStone(1979),is
agenerictermusedtoreferto“allmolarbehaviourthatisguidedbyhealthpurposesor
reinforcedbyhealthoutcomes”(p.24).KaslandCobb(1966a,1966b)suggestthathealth
behaviourcanbedifferentiatedintopreventativehealthbehaviour(actionstakento
preventillness),illnessbehaviour(actionstakenaftersymptomsareexperienced)andsick
rolebehaviour(actionsafterdiagnosis).[Thesecategoriesofhealthbehaviourwillbedealt
withingreaterdepthinChapterTwo].
Thereisstrongevidencesupportingtheviewthatbeliefsandattitudesinfluencehealth
behaviour.Forexample,Lewisetal.(1976)andMechanic(1976a,1976b,1976c)have
shownthathealthcarefacilitiesaredirectlyaffectedbyfactorssuchasdominantbelief
aboutillnessandthestigmaassociatedwithseekinghelp.Theclinicaldiagnosisofillnessis
notalwaysrelatedtothepatient'ssubjectiveresponsetotheirsymptomsand“feeling
better”maybeassociatedwitheventswhicharequiteindependentofprofessional
treatment(Knowles,1977).[TheseaspectsareexploredfurtherinChapterTwounder
“Beliefs,AttitudesandValues”].
Thewayindividualsinterprettheirsymptomsofanillnessisanessentialstepinthe
processofseekinghelpandofthehealingprocessitself.Frequently,theseinterpretations
haveledtomanysymptomseitherbeingignoredorgoinguntreated(Mechanic,1978;
Pennebaker,1982;RoghmanandHaggerty,1972).Bishop'sstudy(1984)oflayresponses
toillness(refertoChapterTwo,sub‐section“Health,IllnessandDisease”fordefinitionof
illness)illustratedtheproblemofserioussymptomsgoingunnoticedbecausetheyfellout
ofthepurviewofthepatient'sinterpretationastowhatwasgoingon.[Thisaspectof
symptominterpretationisdealtwithinChapterTwounder“SymptomInterpretationand
HealthBehaviour”].

3
Furthermore,culturalandsocialbeliefsalsohavebeenshowntoinfluencethewayhealth
carefacilitiesareused.Ngubane(1977),indiscussingmodelsofillnessamongZulus,noted
thedistinctionmadeinZulusocietybetweenillnessesthatareuniversalandtreatable
biomedically(umkhuhlane)andthosewhichmayrequireritualisedandindigenous
methodsofhealing(ukufa Kwabantu‐“diseaseoftheAfricanpeople”).Thisdistinction
between“African”and“non‐African”illnessesisoftenalludedto(CheetamandCheetam,
1976;Edwardsetal.1983;Wessels,1984a).However,asMills(1983,1985)indicates,
someillnessessuchastuberculosismaybeunderstoodpurelybiomedicallyinsome
contextsandashavingAfricanelementsinothers.Ngubane(1977)observedthatthe
conceptsofecologyarecentraltotheZuluideaofhealth.Explanationsofillhealthmay
oftenlieininterpretationsofenvironmentalimbalancescreatedbysorcery(ubuthakathi)
ordisturbancesinthesocialorder.[Theseaspectsandtheroleofculturearetreatedmore
fullyinChapterThree].
Itappearsthatagreatdealofthehealthcareoccursquiteindependentlyofthe
formalisedhealthcaresystem(ChristmanandKleinman,1983).AccordingtoMills(1985),
thereisarangeofnon‐formalandsocio‐culturalresourcesforillnessmanagement
availableincommunities.Popularhealthcare(givenbyfamily,friendandothermembers
ofthecommunity)andfolkmedicine(whichincludetheformalisedculturalexperienceof
healing,faithhealers,traditionalhealersandpriests),arestillconsideredmoresignificant
thantheformalisedwesternhealthservices.
Theattitudesthatpeopleholdabouthealthareclearlyimportanttohealthcareitself.
Someresearchershaveevenarguedfordifferingmodesofservicesbasedondifferent
viewsofillness(Millon,1982).Changesintheattitudesofhealthandillnesswill,inturn,
haveadirecteffectonthehealingprocessitself.Oneexampleisthe“germtheoryof
illness”whichdirectlyledtochangesintheattitudestotheuseofsterilemedical
procedures,improvementofsanitationandpersonalhygiene(Clymeretal.,1984).
[Cultural,popularandfolkmedicinesarediscussedinChapterThreetogetherwithcertain
otherrelatedissues].

4
Althoughthereisanabundanceofresearchintothisaspectofhealthcareworld‐wide,
verylittlehasbeendoneinAfricancommunities,andthisdearthofresearched
informationistrueforSouthAfricaaswell.Inthisstudy,therefore,thefocusisonthe
relationbetweenhealthattitudes,valuesandbeliefsandaspecificareaofhealth
behaviour,namely,“helpseekingbehaviour”or“healthaction”inurbanAfricans.The
attemptisalsomadetogainanunderstandingofurbanAfricanbeliefs,attitudesand
valuesabouthealthandillnessandtoseehowthesebeliefs,attitudesandvalues
influencetheirhealthbehaviouraswellastheuseofhealthcarefacilities.Inaddition,
relatedurbanAfricanhealthandillnessissues,suchas,symptomsandsymptom
interpretation,theinfluencesofculturalandsocialbeliefsontheuseofhealthcare
facilities,theroleofpopularhealthcareandfolkmedicine,theroleofsocialsupportin
theseekingofmedicalhelpandtheeffectsoflifechangesorstressesonhelp‐seekingare
alsoinvestigated.Inthisconnection,theexistinghealthandillnessmodelsarecompared
andanAfricanmodelforhelp‐seekingbehaviourisproposed.
AstudyofthiskindhasdirectrelevanceforboththeSouthAfricancontextandother
“ThirdWorld”countries.Itwillassistinthedevelopmentofhealtheducation
programmes;planningofhealthfacilities;thetimeouspromotionofhealthaction;the
controlofdiseaseandtheraisingofthehealthstatusofthepopulation.However,itisits
contributiontomedicalpsychologythatistheimmediateobjective.Ihavebeenespecially
interestedinitsdirectbenefitforclinicalpsychologists,especiallythoselikemyselfwho
workinageneralhospitalsettinglikethepioneeringSub‐DepartmentofMedicallyApplied
PsychologyunitattheKingEdwardVIIIHospitalinDurban,SouthAfrica.
Insummary,thisstudyaimsto:
1 understandphenomenologicallytheurbanAfrican’sperceptionofillness,
diseaseandhealth;
2 identifyattitudesthatdirectlyinfluencehealthbehaviour;

5
3 studytherelationshipbetweenthekeyattitudesthatinfluencehealth
behaviour,andotherrelevantenvironmental,socialandpsychological
factors;
4 identify“triggerfactors”thatprecipitatehealthaction;
5 isolatefactorsthatcontributeto“negative”healthbehaviour;
6 assessthevalidityofexistingmodelsofhealthandillnessforthesample
studied;and
7 understandtheprocessunderlyingtheassociationofsymptomstodisease
andtheinterpretationsgiventosymptoms(i.e.theunderstandingof
illness).
Inordertoachievetheaboveaims,thefollowinghypotheseswillbetestedina
representativesampleofurbanAfricansdrawnfrombothaclinicalandgeneral
population:
1 thatthesubject'spersonalconceptionofillnessstronglyinfluencesthe
mannerorwayofseekinghelp;
2 thatcertainattitudesdirectlyinfluencepositiveand/ornegativehealth
behaviour;
3 thatcertaineventsinthesubject'senvironmentcontributetotheseeking
ofhelp;and
Trigger factors refer to factors, such as, circumstances, events, cognitions or sensations.

6
4 thathealthactionisinfluencedbysignificantindividualsinthesubject's
environment.
Thisthesisisorganisedinthefollowingway.InChaptersTwoandThreenecessary
backgroundinformationandareviewofthepertinentliteratureispresented.Chapter
Twoalsoprovidesabriefhistoryofpsychologyanditsinvolvementinhealthandillnessas
wellasadescriptionofvarioustermsanddefinitionsthathaveemergedfromthis
relationship.Alsoprovidedinthischapteraredefinitionsofthepsychologicalconceptsin
healthandillnessthatwillbeusedthroughoutthisthesis.Toprovidesomeperspectiveon
health‐relatedbehaviourareviewofsomeofthemorepopulartheoreticalmodelsof
health‐relatedbehaviourfollows.Finally,areviewofsomeofthecriticalissuesinhealth
behaviourareprovided.
ChapterThreedealswithissuesspecifictotheSouthAfricancontext.Theseincludeissues
suchashealthinSouthAfrica,culturalinfluencesonhealthwithspecialreferencetothe
aetiologyofillnessintheAfricanworld‐viewandtraditionaltreatments.
InChapterFourthemethodologyofthisstudyispresented.Adescriptionofthesubjects,
theselectionofthesampleandthematerialsusedinthestudyarethendescribed.Other
issues,suchas,thechoiceofthequestionnairesused,thevalidationofthequestionnaire
andproblemsexperiencedtogetherwithavailablemeasurementsfollow.
TheresultsandtheanalysisofthedataappearinChapterFive.Theresultsarepresented
mostlyintabularand,wherevernecessary,ingraphicalform(Briscoe,1990),intheorder
itwasobtainedfromtheHealthandIllnessBattery(HIB)sothattheyareeasily
comprehensibleandallowforeasycomparison.Theresultssectionsummarisesthedata
collectedandtheirstatisticalanalysis.
InChapterSix,thediscussionsection,themainfindingsareexaminedandinterpreted.
Finally,themainconclusionsandthetheoreticalimplicationsofthestudyarepresented.
See chapter four “Method of Data Collection” for a description of the HIB.

7

8
CHAPTER2
PSYCHOLOGYANDHEALTH
Althoughthehistoryofpsychologymaybetracedtotheperiodofearlycivilisation(Kimble
andSchlesinger,1985a,1985b),asascientificdisciplineitcoversaperiodjustovera
century(Brennan,1986).Likemanyoftheothersciences,psychologyoriginatedin
philosophyandemergedasaseparatedisciplineinthelatenineteenthcentury.Itwas
initiallyconcernedwithsensationsandperceptionsbutthereaftermovedtothestudyof
humanbehaviourandbecamemore“applied”.Oneofthefirstappliedsub‐specialities
wasclinicalpsychology.Althoughthebeginningofclinicalpsychologyismarkedbythe
foundingofthefirstAmericanpsychologicalclinicin1896byWitmer,itwasonlyinthe
1940'sthatitbecomeawellorganizedandrecognizedacademicdiscipline.Intheearly
1970'sfurtherspecializationtookplacewithinpsychologywithpsychologistsbecoming
moreinvolvedinareasofhealthandillness.Thisinvolvement,however,shouldnotbe
construedasatotallynewphenomenonbutratherasare‐newedinterest.
Thecombinedroleofpriestandhealer,philosopher,scholarandteacher,howeveris
mucholderandremainsaphenomenonstillcommonintraditionalsocietiesandinthe
practiceoftraditionalmedicine(Schlebusch,1990).
Psychologists'interestinhealthandillnesshasledtonewchallengesandopportunities
andhascontributedtoatransformationoftheirtraditionalrole.Howardetal.(1986)
notedthat53.2percentofnewpsychologydoctoratesin1984wereinthehealthservice
providersubfields.Theseauthorsalsopointoutthatnotonlyhastherebeenadramatic
riseintheemploymentofpsychologistsinthehealthservice,butthattherehasalsobeen
arelateddeclineintheiracademicandresearchroles.Furtherevidenceforthisoverall
rateofgrowthofpsychologicalinterestintheareaofhealthistheincreasedemployment

9
ofpsychologistsinmedicalandhealthcarepositions;theriseinmembershiptobodies
suchasTheAmericanPsychologicalAssociationinthedivisionsofHealthPsychologyand
Neuropsychology;theincreaseintheamountofliteraturepublishedintheareaandthe
riseinthenumberofpsychologistsemployedatmedicalschools(GentryandMatarazzo,
1981;Millon,1982;Sweet,etal.1991).SimilarchangeshaveoccurredintheUnited
Kingdomaswell(Nicholas,1983).
InSouthAfricanasimilartrendistakingplace.Therehasbeenthedevelopmentofclinical
psychologicalservicesingeneralhospitals(Schlebusch,1983a,1983b;Schlebusch,1987;
Schlebusch,PillayandLouw,1989;Pillay,SchlebuschandLouw,1992);thetrainingof
internsinclinicalpsychologyatgeneralhospitals(Schlebusch,1983b,1989);the
establishmentofteachingprogrammesatmedicalschoolsinmedicalpsychology,clinical
healthpsychologyandbehaviouralmedicine(Schlebusch,1989);thedevelopmentof
employmentopportunitiesintheseareasandplannedfuturedevelopmentinacademic
hospitals(Schlebusch,1987;1989).However,thesedevelopmentsvaryconsiderably
withinthecountry(Schlebusch,1989,1990).Insomeprovinces,forexample,Natal,a
fairlywellestablishedserviceexistsinhospitals,suchas,KingEdwardVIIIHospital(alarge
teachinghospitalattachedtotheUniversityofNatalMedicalSchool)andAddington
Hospital.TheNatalUniversity'sMedicalFacultywasthefirstSouthAfricanmedicalschool
toestablishadepartmentofaMedicallyAppliedPsychologywiththeappointmentofa
fullprofessorshipinthisfield(SchlebuschandWessels,1986).ElsewhereinSouthAfrica,
clinicalpsychologyattheteachinghospitalsoperateswithintheDepartmentsof
Psychiatrywithprincipalpsychologistsasclinicalheads.AnexceptionisTheMedical
UniversityofSouthernAfrica(MEDUNSA)inGarankuwa,whichhastwodepartmentsof
psychology.Oneofthesedepartmentsteachesgeneralpsychologyandtheothertrains
clinicalpsychologists.Morerecently,thePsychologicalAssociationofSouthAfrica(PASA)
feltitnecessarytodevelopaDivisionofHealthPsychology.
Notonlyarepsychologistsfromallsub‐disciplines(e.g.clinical,social,academic,etc)
showingagreaterinterestinhealthandillness,others,suchas,socialworkers,
occupationaltherapists,psychiatristandmedicalpractitionersarealsoshowingagrowing

10
interestinpsychologicalprinciplesandconceptsfortheirwork.Theiremphasesand
practicesnaturallyvary.Theattemptbytheseinterandintra‐disciplinestodefinetheir
workhasledtoaplethoraoftermsanddefinitions;Forexample,“healthpsychology”,
“clinicalhealthpsychology”,“medicalpsychology”,“behaviouralmedicine”,“psychological
medicine”,“psychosomaticmedicine”,“behaviouralhealth”and“healthbehaviour”.The
similaritiesanddistinctionsbetweenthesetermsarenotalwaysclearandattimesthey
areinappropriatelyused.Broadlyspeaking,theseareascanbedividedintothosethat
arediscipline‐specificandthosethataremulti‐disciplinary(Schlebusch,1990).Areassuch
aspsychosomaticmedicine,psychologicalmedicineandconsultation‐liaisonpsychiatryare
allsub‐specialitiesofpsychiatryandusuallyinvolveprofessionalstrainedinmedicineand/
orpsychiatry.Clinicalpsychology,rehabilitationpsychology,healthcarepsychology,
generalhospitalpsychology,neuropsychologyandhealthpsychologyarespecifictothe
disciplineofpsychologyandinvolveprofessionalstrainedinpsychology.Otherareassuch
asbehaviouralmedicine,behaviouralhealthandhealthbehaviouraremultidisciplinary.
Someareasarebroadlydefinedwhileothersaremuchmorespecific.Forexample,health
psychology,whichisdisciplinespecific,isdefinedas:
theaggregateofthespecificeducational,scientificandprofessional
contributionsofthedisciplineofpsychologytothepromotionand
maintenanceofhealth,thepreventionandtreatmentofillness,the
identificationofetiologicanddiagnosticcorrelatesofhealth,illnessand
relateddysfunction,andtheanalysisandimprovementofthehealthcare
systemandhealthpolicyformation(Matarazzo,1982,p.4).
Itisevidentfromthisdefinitionthathealthpsychologyembracesanyactivityof
psychologyrelatingtoanyaspectofhealth,illness,healthcaresystemorhealthpolicy
formation.Clinicalhealthpsychology,ontheotherhand,ismorespecific,accentuating
thesignificantrelationshipbetweenclinicalpsychologyandhealthpsychology
(Schlebusch,1990).
11
Insomeinstances,healthpsychologyissometimeserroneouslyusedtoreferto
behaviouralmedicine.Thisisgrosslyinaccuratesincebehavioural medicine accordingto
SchwartzandWeiss(1978)isdefinedasthe
interdisciplinaryfieldconcernedwithdevelopmentandintegrationof
behaviouralandbiomedicalscience,knowledgeandtechniquesrelevantto
theunderstandingofphysicalhealthandillnessandtheapplicationofthis
knowledgeandthesetechniquestoprevention,diagnoses,treatmentand
rehabilitation(citedinGochman,1988).
Essentially,behaviouralmedicineisthe‘interface’ofthebehaviouralandbiomedical
sciences.
Anemerginginterdisciplinaryfieldwhichisstillintheprocessofestablishingitsidentity
andwhichisparticularlyrelevantforthisstudy,is health behaviour.Amoreconcise
definitionthanthatusedearlier(Stone,1979)isthatofGochman(1982)whodefines
healthbehaviouras
thosepersonalattributessuchasbeliefs,expectations,motives,values,
perceptionsandothercognitiveelements:personalitycharacteristics,
includingaffectiveandemotionalstatesandtraits;andovertbehaviour
patterns,actionsandhabitsthatrelatetohealthmaintenance,tohealth
restorationandtohealthimprovement(p.169).
AccordingtoGochman(1982)theword“behaviour”referstosomethingthatpeopledoor
avoiddoingandisnotnecessarilyconsciouslyorvoluntarilydone.Thisdefinitionexcludes
treatment,reflectionsofbodilystates,clinicalimprovementsorphysicalrecoveryor
healthstatus.Aperson'sperceptionsofhis/herhealthstatusorofimprovement,recovery
orotherchangesinhealthstatusarealsoregardedashealthbehaviours.Thisdefinition
alsoincludes“notonlydirectlyobservable,overtactionsbutalsothosementalevents,
feelingsandfeelingstatesthatareobservedormeasuredindirectly”(Gochman,1982).In
addition,accordingtothisdefinitiontheseattributesareunderstoodtobeinfluencedby
familystructure,thepeergroupandsocialfactors,andsocial,institutionalandcultural
determinants.

12
Healthbehaviour,therefore,isnotsynonymouswithbehaviouralmedicinealthough
someaspectsarecommontoboth.AccordingtoGochman(1988)thebasicparadigm
proposedforbehaviouralmedicineisthemedicalmodel,whereashealthbehaviouris
definedindependentofpathology,diagnosisandtreatmentofspecificdisordersbut
includesconcernforgeneralhealthmaintenanceandwellbeing.Itdoesnotautomatically
beginwithinamedicalframeworkoritsassumptions.Healthbehaviourdoes,however,
encompassrelatedconceptssuchas“preventative”and“protective“illnessandsick‐role
behaviour.
2.1PSYCHOLOGICALCONCEPTSINHEALTHANDILLNESS
2.1.1 HEALTH,ILLNESS,ANDDISEASE
Althoughverywidelyused,theconceptshealth, illness and disease areverydifficultto
definesincetheyhavebeeninterpretedquitedifferentlyamonglaypeopleandscholars
(Schlebusch,1990).Inspiteofthevaryingusesoftheseterms,Diaz‐Guerrero(1984),in
searchforauniversalconceptionofhealth,studiedtheresponsesofsubjectsinasample
drawnfromthirtydifferentculturesandfoundthatthereissomecross‐cultural
agreementthathealthischaracterizedas“good”,“potent”and“active”.
“Health”isfrequentlyconsideredtobeanormalcondition,implyinganabsenceof
disease,symptomatologyorlaboratoryabnormalities.Suchaviewwhichaccentuatesthe
absenceofbiomedicalsymptomatologyconstitutesanegativeconceptofhealth.
Schlebusch(1990)suggests,incontrast,amorepositiveconceptofhealthinwhich
psychosocialvariablesplayacentralrole.Thesevariablesinter aliaincludeeducation,
socialclass,diet,income,socialandoccupationalenvironment,life‐style,interpersonal
relationships,personalhabits,accesstohealthcareandoccupationalfunctioning.Sucha
positiveconceptofhealth,hebelieves,willfacilitateamorecomprehensiveapproachto
thedeliveryofhealth,unlikethetraditionalmedicalmodelanditsconceptofdisease

13
whichtendstofocusondiagnosisandthecureofdiseasetotheneglectofpreventionof
diseaseandmaintenanceofgoodhealth.
Even“disease,”whichhasbeennarrowlydefinedas“amedicalhypothesisthatimplies
particularpathologicalprocessesunderlyingaspecificsyndrome”(Mechanic,1978,p.25),
isnowincreasinglyusedtorefertobehaviouralandsocialprocessesforwhichnosuch
specificitycanbedemonstrated(Schlebusch,1990).Oftentheterms“illness”and
“disease”areusedinterchangeably.Onewayofdistinguishing“disease”from“illness”is
toregardtheformerasa“condition”,andthelatterasa“behaviour”.However,asalready
mentioned,thetermsareusedinterchangeablybecauseofthepsychologicalinterplay
betweenthem(Schlebusch,1990).Inessence,diseaseischaracterizedbystructuralor
physiological,functionalandbiochemicalchangesandreferstoabiologicalprocess.Its
basiccharacteristicsremainthesameregardlessofwhenorwherethediseaseoccurs
(Schlebusch,1989).
“Illness”,ontheotherhand,impliesasubjective,psychologicalandsocialexperience
whichisthereforeopentointerpretationbybothpatientsandthesocietytheylivein.In
fact,illnessmayoccurintheabsenceofdisease.Incontrast,therearetimeswhendisease
maybepresentbutthepatientmaynotfeelill.Thisissometimesreferredtoasthe
“preclinicalphaseofdisease”(Braunstein,1981).AccordingtoCott(1986),illnessoften
remainssubsequenttooptimalmedicaltreatmentand,therefore,constitutesasignificant
health‐careproblem.Inaddition,illnessbringsaspecificmeaningtoapatient'slifeand
crystallizesspecialmeaningthatconstitutesandexpressesitselfasawayoflife(Kleinman,
1986).Itisbecauseoftheseidiosyncraticelementsandtheorientationtowardsproblems
ofexistenceandcopingthatpromptedHunt(1988)tosuggestthatthemeasurementof
illnessmustbedirectedtowardsthepatient'sviewpoint.
Gochman(1988)pointsoutsixelementsthatcontributetothecomplexityanddifficultyin
definingtheseconcepts.Thefirstelementheattributestothe“simultaneousexistenceof
layandprofessionalorscientificdefinitions.”Althoughtheyoverlaptherearealso
differenceswhichhaveimportantlifeordeathrelevanceintheareahealth.Thesecond
14
elementisthe“existenceofmultipleprofessionalorscientificdefinitions.”Forinstance,
themedicaldefinitionsemphasizethepresenceorabsenceofpathologywhile
psychologicaldefinitionsemphasizeperceptions,feelingsofwellbeingandequilibrium.
Thethirdelementisthe“pluraldefinitionswithineachprofession(p.8).”.The
acknowledgementthatatleastthreedimensions,namely,thebiomedical,personaland
socio‐culturalmustbetakenintoaccount,constitutesthefourthelementofdifficultyin
definition.Thefifthelementaffirmsthat,becauseoftheimportanceofthesethree
dimensions,therearevaryingdegreesofjuxtaposition,conflictandequilibriumamong
themedical,personalandsocialperspectives.Thelastelementreferstothesimultaneous
existenceofseveraldifferenthealthpracticesystems;theseinclude“scientific”medicine,
religiousor“traditional”medicine,publichealthpracticeandfolkmedicine.
2.1.2 SOMESPECIFICTYPESOFHEALTHBEHAVIOUR
KaslandCobb(1966a,1966b);Mechanic(1978,1986);Suchman(1972)andParsons
(1951)havemadecertaincriticaldistinctionsbetweenthevarioustypesofhealth
behaviours.Thesedistinctionsindefinitionsofhealth‐relatedbehaviourarediscussed
below.

15
2.1.2.1PreventativeBehaviour AccordingtoKaslandCobb(1966a),preventativebehaviourreferstotheactionsof
individualswhobelievetheyarewell(i.e.notexperiencinganysignsorsymptomsof
illness)inordertoremainwell.Suchaviewconfineshealthbehaviourtopreventative
activitiesandinclude,butisnotlimitedto,“everyday”nonmedicalbehaviourssuchas,
durationofsleep,eatinghabits,weightmanagement,physicalandrecreationalactivity,
non‐consumptionofalcoholandnon‐smoking(BellocandBreslow,1972).Primary
preventivemedicalbehavioursincludebehaviourssuchasimmunizationagainstinfectious
diseases,whilesecondarypreventivemedicalbehaviourswillincludeperiodicmedical
examinationsandscreeningformedicalproblems.Thesemeasuresdonotnecessarily
preventdiseasebutcontributetoitsearlydetection(Gochman,1988).
2.1.2.2HealthProtectiveBehaviour
Healthprotectivebehaviourreferstotheactionsofindividualsthataugmentprimaryand
secondarypreventativebehavioursandaredirectedtowardsprotectingtheirhealth,
whethermedicallyapprovedornot(HarrisandGutten,1979).Examplesofhealth
protectivebehavioursarepraying,repairinghouseholdimplements,consuminglarge
dosesofvitamins,takinglaxatives,emetics,enemasandcoldshowers.Thecommon
rationaleofthesebehavioursisthattheyprotectandmaintainhealth(Feuerstein,Labbe
andKuzcmierczyk,1986).
2.1.2.3IllnessBehaviour
Theactionsofindividualstoascertaintheirstateofhealth,thatis,whentheyarenotsure
thattheyarewelloraretroubledbyfeelingsorsensationsthattheybelievemaybesigns
orsymptomsofanillnessareregardedasillnessbehaviour(KaslandCobb,1966a).
Examplesofillnessbehavioursareresponsestophysicalsymptomatology,seekingexpert

16
helpandadvice(eitherfromhealthcareprofessionalsorlayandfolktherapists),seeking
theopinionsoffriendsandrelatives,aswellasdelayingactiontoseeifthesignsor
symptomsremit(Gochman,1988).AccordingtoMechanic(1978),illnessbehaviourhas
severaldeterminantsincludingtheperceptionandseverityofsymptoms,theirdisruptive
andpersistentnature,individualneeds,theavailabilityofalternativeinterpretationsand
treatment,aswellascostsintimeandmoneyincurredbytheindividual.Theseare
discussedingreaterdetailwhenMechanic's(1976a)modelofillnessbehaviourisgiven
fullertreatmentbelow.
Illnessbehaviouralsoinvolveshelp‐seekingbehaviour(Mechanic,1986)andmanifests
whenpatients'decidetodosomethingabouttheirsymptomsordistress.Help‐seeking
behaviourincludesnotonlytheconsultingofamedicaldoctorbutalsothesolicitingof
generalhelpfromcommunityadvisers,tribalauthorities,traditionalfaithhealers,the
sangoma(diviner)orministersofreligion.
Itis,therefore,importanttobearinmindthatthepatient'sbehaviourinpreventingand
dealingwithillnesscanbeviewedinthecontextofthepatient'sownrepresentationof
theillness,whichisbasedlargelyontheexperienceofcertainconcretesymptoms.The
self‐understandingofthesesymptomsandthenatureofthepatient'sownrepresentation
oftheillnessisnaturallyopentosocio‐culturalinterpretationaswell.However,thisself‐
understandingofillnessactsasaregulatingsystemtoguidecopingbehaviourandtoset
goalsthroughwhichcopingisevaluated(Laventhalletal.1980)andispowerfullypresent
evenduringtheformalscientificprocessofhealing.Thepsychologicalimplicationsofthis
areobvious.
2.1.2.4SickRoleBehaviour
Sickrolebehaviourreferstothoseactionsadoptedbyindividualswhohavealreadybeen
designatedsick,eitherbyothersorthemselves,inordertogetwell(KaslandCobb,
1966b;Parsons,1951).Examplesofsuchbehavioursarecompliancewithaprescribed

17
medicalregimen,limitationofactivityandactionsrelatedtorecoveryandrehabilitation.
Sicknessiscloselyalliedtosickrolebehaviourasitgenerallyreferstosociallysanctioned
waysthatinferillness;itisnotnecessarilyimpliedbyillnessordiseaseandcanbe
observedintheabsenceofeither(Hunt,1988).Itinvolvesvariousbehavioursincluding
labelling,communicatingdistress,seekingmedicaladvice,absencefromworkandstaying
inbed.(Schlebusch,1990).
2.2HEALTHBELIEFS,ATTITUDESANDVALUES
Thesocio‐culturalattitudes,valuesandbeliefsofapersonguideandinfluencehisorher
perceiving,filtering,interpreting,understandingandpredictingofnews,informationand
daytodayevents.Hermeneuticalunderstanding,inotherwords,maybeinfluencedby
bothcognitiveandnon‐cognitiveprocessessuchasperceptionsandvalues.Similarly,as
mentionedearlierintheintroduction,theattitudes,valuesandbeliefsofindividuals
abouthealthandillnessinfluencestheirhealthbehaviouraswell.
‘Attitude’ismostcentralinsocialpsychology.Anattitudemaybedefinedasa
“predispositiontofeel,thinkandacttowardssomeobject,person,grouporeventina
moreorlessfavourableorunfavourableway”(Richardson,1980,p.299).Accordingtothis
definitionattitudesaremadeupofthreecomponents—cognitive,affectiveand
behavioural.Beliefsconstitutethecognitive component;attitudesformtheaffective
componentandtheactionsconstitutethebehavioural component.Eachofthethree
componentsmayvaryinintensityandcomplexity.
Attitudesderivefromunderlyingvalues.Avaluemaybedefinedasabasicattitude
towardscertainbroadmodesofconduct,suchas,courage,honesty,friendshiporcertain
statesofexistence,forexample,equality,salvationandfreedom.Valuesarethusakinto
attitudesbuttheyrefertotheendsandnotthemeans.

18
2.3MODELSOFHEALTH‐RELATEDBEHAVIOUR
Overthepastfourdecades,severaltheoreticalmodelshavebeenproposedinanattempt
toexplainoraccountforhealthbehaviours.Cummingsetal.(1980)haveidentified
fourteenmodelswhichtheyregardas“mostnotableintermsofpredictiveabilityand
frequencyofcitation”(p.124).Areviewofallfourteenmodelsareneitherwithinthe
scopeofthisstudyornecessaryforitsobjectives.Thefollowingsectionwillbriefly
highlightafewofthemorefrequentlyusedmodels.
Amodel(orparadigm)isasystemofbeliefsaboutthestructureandworkingsofreality.
Kuhn(1962)pointedoutthatmodelsdefinethelegitimateproblemsandmethodsofa
researchfieldforsucceedinggenerationsofpractitioners.Amodel,heheld,guidesand
limitsobservation.Asamodelisusedanomaliesemergewhenexplanationsdonotquite
fitrealityandtheorieslosetheirexplanatoryvalue.Anomaliesemergewhenthe
legitimacyofexplanationleadstothesearchfornewwaysofexplanation.Thereisoftena
periodofcompetingmodelsuntilonedominatestoachievewidespreadlegitimacy,
sufficientlyenoughtobecometheprevailingparadigm.Itistheemergenceofanomalies
thatforceonetoseekalternatemodels.
Forourpurposesweseemodelsascomplexhypothesesthatattempttoexplainhealth
andillnessbehaviours.Allofthemodelsdiscussedbelow,exceptsociallearning,were
specificallydevelopedashealthmodels.
2.3.1 THEHEALTHBELIEFMODEL
TheHealthBeliefModel(HBM)wasdevelopedintheearly1950sbyagroupofsocial
psychologists(Hochbaum,1958;Rosenstock,1974)inthePublicHealthServiceofthe
UnitedStatesofAmericainordertounderstandwhypeoplefailedtoaccept“disease
preventativesandscreeningtestsforearlydetectionofasymptomaticdiseases”
(Rosenstock,1974,p.328.).Itwaslaterusedtounderstandsickrolebehaviours,illness

19
behavioursandcompliancewithprescribedmedicaltreatment(Wallstonand
Wallston,1984).Thecomponentsofthemodelemergedoutofwellestablished
psychologicalandbehaviouraltheoriesthathypothesizethatbehaviourdependsmainly
ontwovariables:thevalueplacedbytheindividualonagoal(ie.desiretoavoidillnessor
togetwell)andtheindividual’sbeliefthatagivenactionwillachievethegoal(thata
specifichealthactionwillpreventoramelioratetheillness).TheHBMconsistsofthe
followingdimensions:
(1)perceived susceptibility whichreferstoanindividual’ssubjective
perceptionoftheriskofcontractinganillness;
(2)perceived severity—thisreferstothefeelingsconcerningthe
seriousnessofcontractinganillness;
(3)perceived benefits refertothebeliefsregardingtheeffectivenessofthe
variousactionsavailableinreducingthethreatofdisease;and,
(4)perceived barriers—thesearethepotentialnegativeaspectsofa
particularhealthactionwhichmayactasimpedimentstoundertakingthe
recommendedhealthbehaviour.These‘barriers’includesideeffects,pain,
inconvenienceandtime‐consumption.
TheHBMassumesthatthereisa“cuetoaction”thatmaytriggerofthedecision‐making
processandmaybeeitherinternal(ie.symptoms)orexternal(eg.mediaand
interpersonalinfluences).Thismodelacceptsthatdiversedemographical,socio‐
psychologicalandstructuralvariablesmayaffecttheindividual’sperceptionand,asa
result,influencehealth‐relatedbehaviour(JanzandBecker,1984).
Althoughthismodeliswidelyacceptedbyhealthresearchers,ithaselicitedcriticismsas
well.Haefer(1974)describedtheHBMas“aconfusingmelangeofinconsistent(thoughby
nomeansdisconfirming)resultsobtainedunderwidelyvaryingconditionsandsusceptible
tonounivocalinterpretation”.Atpresenttherearesomanyvariablesthathavebeen
identifiedthatthetheorybecomesuntestableandunabletobefalsified,animportant
criterionforthevalidationofatheorysayWallstonandWallston(1984)followingKarl

20
Popper's(1959)‘falsificationprinciple.’Inaddition,essentialelementsidentifiedbythis
model,suchas,demographic,structuralandattitudes,donotalwayspredictasexpected.
Thelackofspecificationofrelationshipamongthevariablesresultsinrelativepredictions
ratherthanquantitativeones(Stone,1979).Anotherproblemisthelackofconsistent
operationalizationofvariableswhichresultindifferentmeasuresbeingusedindifferent
studies.Whilethisvariationmayenhancetheadaptabilityofthemodel,itmakes
comparisonsbetweendifferentstudiesdifficult,ifnotimpossible.
2.3.2 KASLANDCOBB'SMODEL
KaslandCobb(1966)haveformulatedtwomodels,onefor“health”andanotherfor
“illness”behaviours.ThesemodelssharesomesimilaritywiththeHBM.Thevariation,
accordingtotheirmodel,isthepossibilityofanindividualundertakingaspecificbehaviour
inthepresenceofparticularsymptoms.Furthermore,thesemodelstakeparticular
cognizanceoffactors,suchas,pain,discomfort,psychologicaldistress,personaltolerance
forpain,disability,copingmechanismsandsocio‐demographiccharacteristics.
Thismodelofhealthbehaviourshypothesizesthatbehaviouroccurringintheabsenceof
symptomsisinfluencedbythethreatofdiseaseandbeliefsconcerningthevalueofhealth
action.Socialcharacteristicsandknowledgeareseenasinfluencingboththeperceived
threatandhealthaction.Otherfactorsthatinfluencebehaviourincludethepast
utilizationofmedicalservices,thecostofhealthaction,thecostofinactionandthe
probabilityofthehealthactionresultinginthedesiredoutcome.
Themodelonillnessandsickrolebehaviourshypothesizesthatbehaviourundertakenin
thepresenceofsymptomsisinfluenceddirectlybytheindividual'sperceptionofthe
threatofthediseaseandthebeliefconcerninghealthaction.Painanddiscomfortare
seenasinfluencinganindividual'sperceptionsaswellasdirectlyinfluencingbehaviour.
Socialcharacteristics,personaltoleranceforpain,disability,andcopingmechanismsare
assumedtoaffectbehaviourindirectly.The‘threat’componentincludestheperceived

21
importanceofhealth,perceivedsusceptibilitytoillnessandseverityoftheconsequences.
The‘value’componentincludestheprobabilityofactionleadingtoadesiredoutcomeand
thedifferentialratioofthecostofactiontothecostofnottakingaction.
2.3.3 SUCHMAN'SMODEL
Thismodel(Suchman,1965a,1965b)resultsfromtheeffortstoadoptasociological
perspectivetounderstandanindividual'sdecisionswithrespecttotheutilizationof
health‐services.Healthbehavioursareexaminedwithintheirsocialandculturalcontexts
andhypothesizedlinksaremadebetweenspecifiedhealthorientationsorbehavioursand
socialrelationshipsorgroupstructures.Centraltothismodelarethesocialpatternsof
illnessbehaviour.Therearefourprincipalfactorsinfluencingillnessbehaviour:
1.Content—whichinvolvesaseriesofconceptsfacilitatingdescriptionsofalternative
behavioursandtheiroutcomes.Forexample,
(a)shopping—theseekingofmedicalcarefromdifferentproviders;
(b)fragmentation of care—receivingmedicalcarefromdifferentproviders
atthesamesource;
(c) procrastination—delayinseekingcaresubsequenttotheobservation
ofsymptoms;
(d) self‐medication—self‐initiateduseoftherapies;and,
(e) discontinuity—interruptionsinthetreatmentorprocessofcare.
2.Sequence—thisfactorisdividedintofivetransitionalstages:
(a)symptomexperience;
(b)theassumptionofasickrole;
(c)medical‐carecontact;
(d)dependent‐patientrole;and,
(e)recoveryorrehabilitation.
Initially,thedimensionofthesymptomexperiencealertstheindividualthatsomethingis
wrong.First,thepainordiscomfortorabnormalityisexperienced;secondly,thephysical

22
sensationsorsymptomsareinterpretedanddefinedonthebasisoftheirdegreeof
interferencewithusualsocialfunctioning(cognitivedimension);andfinally,theanxiety
andfearassociatedwiththeillnessemerge(emotionaldimension).
Although,accordingtothismodel,theindividualwillmovefromthesymptomexperience
totheassumptionofthesickrole,heorshemaydecideonalternatives,suchas,denying
thepresenceofillnessordelayingtheseekingofmedicalhelp.Duringtheassumptionof
thesickrole,theindividualwillattempttoreducethesymptomsbyself‐initiatedtherapies
ortreatmentswhilesimultaneouslyconsultingfamilyandfriendsforadviceand
information.Followingtheconsultationofadoctortoassistwiththeorganicand
psychosocialneeds(medical‐carecontactstage),theindividualentersintoarelationship
whichinvolvestheacceptanceofaprescribedregimen(dependent‐patientrolestage).
Duringthemedicalcontactstage,however,thepatientmayneitherbelievethediagnosis
noraccepttherecommendedtreatmentandmayturntoothersourcesforhelp.Further,
variousfactors,suchas,physical,administrative,social,psychologicalaswellasthequality
ofthedoctor‐patientrelationships,mayinterferewithprescribedtreatmentduringthe
dependent‐patientstage.Inthefinalstage(recoveryandrehabilitation)theindividual
givesupthepatientrole.
3.Spacing referstothesocialcohesionofthegrouptowhichtheindividualisamember;
thatis,thecommunity,friendshipandfamilylevelsoftheindividual’ssocialwell‐being.
Thedegreeofsocialorganisationischaracterisedbythelevelofingroupattractionand
exgroupexclusionasmeasuredby“ethnicexclusivity”onthecommunitylevel,“friendship
solidarity”onthesocialleveland“orientationtofamilytraditionandauthority”onthe
familylevel.Thesethreedimensionsarecombinedinanindexofcosmopolitan‐parochial
socialstructure,whereparochialismisdefinedbyhighexclusivity,highfriendshipgroup
solidarityandhighorientationtotraditionandauthority.Thehealthorientationofthe
individualisseenasacontinuum,varyingfromthescientific(objective,professionaland
impersonal)tothepopular(subjective,layandpersonal)basedonthe“knowledgeabout
disease,”“scepticismofmedicalcare”and“dependencyinillness.”Popularhealth
orientationischaracterisedbythefollowingdimensions:cognitive(lowknowledgeabout

23
disease),affective(highscepticismofmedicalcare)andbehavioural(highdependency
duringillness).
4.Variabilityreferstothevariationsinbehaviourduringthefivestagesofillness.These
variationsaffecttheprogressionfromonestagetothenext.
WhileSuchman'sstudy(1965a)seemstosupportarelationshipbetweensocialsupport,
healthorientationandvariationsinresponsetoillness,otherstudies(Reederand
Berkanovic,1973;Geertsenetal.,1975;Farge,1978)wereunabletoreplicatethese
findings.
2.3.4 FABREGA'SMODEL
Fabrega's(1973)modelusesananthropologicalapproachtounderstandingillness
behaviour.Thismodelsuggestninestagesofinformationprocessingwhichleadthe
individualtoadecisiontoactinacertainway.Itassumesthattherearefoursystems
involvedintheinformationprocessing.Theseare(a)thebiological system whichfocuses
onchemicalandphysiologicalprocesses;(b)thesocial systemwhichaffectsrelationships
withotherindividuals,groupsandinstitutions;(c)thephenomenological systemwhichis
concernedwiththeindividual'sstateofawarenessandself‐definition.;and(d)the
memory systemwhichincludesearlyillnessexperiences,medicalattitudesandbeliefs.
Thesesystemsareopenedandinter‐joined.
Thefirsttwostagesofthismodeldealwiththerecognitionandevaluationofsymptoms.
Instageonetheindividualcomestorealizethepresenceofillnessorchangestakingplace
andactstoalleviatetheperceivedillness.Atthenextstagethenegativecomponentsof
theillnessareevaluatedonthebasisofpresentandpastexperiences.Thisevaluation
leadstoanegativevaluebeingattachedtotheconditionreflectingthedanger,disability,
discomfort,socialstigmaandthepsychosocialdisruptionsassociatedwiththeillness.In
thethirdstage,avarietyofmutuallyexclusivetreatmentalternativesareconsidered.

24
These‘plans’arelearnedresponsesbasedonpastexperienceswithillnessrangingfrom
theuseofhomeremediesandpatentmedicinestolayreferralsinordertoobtainmedical
careorhealing.Stagesfourtosevenrelatetotheindividualsevaluationofdifferent
treatmentplans.Theseincludealternativesthatwillreducethe“disvalue”,thebenefits
andutilityofeachaction,aswellaspersonalandeconomiccostsoftheaction.Thisleads
totheeighthstagewhichistheselectionofatreatmentplan.Intheninthstage,further
processingandupdatingtakeplaceasaresultofthetreatmentplanselectedinstage
eight.Theillnessmayberelabelledandarecyclingofthestagesmayoccur.
2.3.5 MECHANIC'SMODEL
Mechanic'smodel(1978)focusesonhelp‐seekingbehaviourandshowsthevariationwith
whichdifferentpeopleperceive,evaluateandreact(ornotreact)tosymptoms.The
emphasisisonwhatoccursbeforeanindividualseesahealth‐careprovider.Mechanic
(1978)identifiestenvariablesthatinfluence“help‐seeking.”Theseare:
1 “thevisibility,recognizabilityorperceptualsalienceofdeviantsignsand
symptoms;
2 theextenttowhichsymptomsareperceivedasserious(thatis,the
person'sestimateofpresentandfuturedanger);
3 theextenttowhichthesymptomsdisruptfamily,work,andothersocial
activities;
4 thefrequencyoftheappearanceofthedeviantsignsorsymptoms,—their
persistenceandrecurrence;
5 thetolerancethresholdofthosewhoareexposedtoandevaluatethe
deviantsignsandsymptoms;
6 availableinformation,knowledge,andculturalassumptionsand
understandingoftheevaluator;
7 basicneedsthatleadtodenial;
8 needscompetingwithillnessresponses;

25
9 competingpossibleinterpretationsthatcanbeassignedtothesymptoms
oncetheyarerecognized;and,
10. theavailabilityoftreatmentresources,physicalproximityandpsychological
andmonetarycostsoftakingaction(including,physicaldistance,costsof
time,moneyandeffort,aswellas,costsofstigma,socialdistanceand
feelingsofhumiliation)”(p.268‐269).
Variables2,3,9and10closelyresemblethebasicelementsoftheHBM.Inaddition,
Mechanic(1978)distinguishesbetween“otherdefined”and“self‐defined”illness.Both
thesituationsinvolvelayreferralsystems.Thedifferenceoccursinthe“other‐defined”
category,wherethedefinitionofillnessoriginatesfromothersintheenvironmentandthe
sickpersonseemstoresisttheevaluationandmayhavetobebroughtfortreatment
involuntarily,forexample,inthecasesofpsychosis,illnessofchildrenandincasesof
adultdenialofillness.
2.3.6 ANDERSEN'SMODEL
Thisisabehaviouralmodel(AdayandAndersen,1974)thathasbeenusedwidelyfor
assessingmedicalutilisation.Accordingtothismodel,healthutilisationisdependent
uponthreecomponents:
1 thepredispositionofthefamilytousehealthservices;
2 theabilitytosecureservices;and,
3 theneedforservices.
Thefirstcomponentincludesinformation,suchas,age,sex,maritalstatus,education,
occupation,andhealthbeliefsandattitudesaboutmedicalcare,physiciansanddisease
(eg.familiesthatbelieveintheefficacyofmedicaltreatmentwillseekcaresoonerand
moreoften).Thesecondcomponentreferstotheconditionsthat“enable”theuseof
healthservicesorwhichmakesthemavailable,theseinclude,familyresourcessuchas

26
incomeandmedicalaidorcommunityresourcessuchastheavailabilityofhealthservices
andhealthpersonnel,traveltimesandwaitingtimes.Whenthesetwocomponentsare
present,twofactors,(namely,thevariationinperceptionofillnessandthemannerof
responsetoillness),willdeterminewhetherhealthservicesareused.Perceivedneedis
measuredbybothsubjectiveperceptionsofillnessandtheclinicalevaluationofillness.
2.3.7 SOCIALLEARNINGTHEORY
ThesociallearningtheorywasdevelopedbyRotteretal.(1972)toexplainhuman
behaviourincomplexsituations.Therearefourbasicconstructstothetheory,namely:
behaviourpotential(BP);expectancy(E);reinforcementvalue(RV);and,thepsychological
situation(S).Accordingtothetheory,aspecificbehaviour(BP),occurringinagiven
situation(S),isthefunctionoftheexpectancy(E)thatthebehaviourwillleadtoa
particularreinforcementinthatsituationandthevalueofthereinforcement(RV)tothe
individualinthatsituation(WallstonandWallston,1984).Theequationrelatingsocial
behaviourtobehaviourisrepresentedasfollows:
BP=f(E,RV)
Ofalltheconstructs,expectancyreceivesthemostattention.Theexpectancyconstruct
particularlyresearchedis“internalversesexternallocusofcontrolofreinforcement.”This
referstothegeneralizedexpectancy(withregardstoeachelementintheequation,itcan
bemeasuredingeneralorspecificterms,specifictoexpectancy)astowhetherone'sown
behaviourorforcesexternaltooneselfcontrolone’sreinforcement.
WallstonandWallston(1984)usedthistheorytoexplainhealthbehaviour.Theymodified
theequationasfollows:
1.HB=f (HLC× HV)

27
2.HB=IHLCT× HVT+PHLC‐CHLC
Where HB = healthbehaviour;
HLC = healthlocusofcontrol;
HV = healthvalue;
IHLC= internalhealthlocusofcontrol;
PHLC = powerfulothershealthlocusofcontrol
CHLC = chancehealthlocusofcontrol
(The subscript (T) indicate that the raw scores were converted to standardized T‐scores to
eliminate negative values before multiplying).
UsingtheseequationsWallstonandWallston(1984)generalizedsociallearningtheoryto
predicthealthbehaviour.Accordingtothem,“apersonismostlytoengageinahealth
behaviourgivenabeliefininternalhealthlocusofcontrolandahighvaluingofhealth.”
Lowbeliefinachancehealthlocusofcontrolcouldalsofacilitatehealthbehaviour.Ifa
personbelievesthathealthisstrictlyamatterofchance,thereisnoreasontotakeaction.
Highbeliefinpowerfulothersasahealthlocusofcontrolwillfacilitatehealthbehaviour
recommendedbyhealthprofessionals.WallstonandWallston(1984)alsopointoutthat
thedistinctionbetweenexternalbeliefsPandChasprovenusefulinhealthresearch.
Someauthorsinrecentyearshaveadvancedtheunderstandingofhealthbehavioursby
modifyingthesetraditionalmodels(Hersheyetal.,1975;BerkiandAshcraft,1979)in
ordertomakethemrelevanttotheircontexts.Onesuchmodelisthatpostulatedby
Young(1980)whichisacrossculturaladaptationoftheHBMaimedatexplaining
treatmentdecision‐making.Therearefourmajorelementstothemodel.
1 Gravity—whichreferstothelevelofperceivedseverityoftheillnessheld
bytheindividual'sreferencegroup(thisassumesthatthereexists,priorto
theonsetofillness,somegroupconsensusabouttherelativeand/or
absolutelevelofseriousnessofvariousillnesses);

28
2 Knowledge of a home remedy—derivedfromalayreferralsystem(ifsuch
aremedyisunknown,orifitistriedandfoundtobeineffective,the
individualisthenlikelytoturntotheprofessionalreferralsystem).;
3 Faith—thelevelofbeliefintheefficacyofadifferentoftensupernatural
treatmentoption(especiallyfolkremedies);and
4 Accessibility—thecostandavailabilityofhealthservices(similartothe
“perceivedbarriers”intheHBMandto“enablingfactors”inAndersen's
model).
Theproliferationofmodelsleadstoconfusionwithregardtochoosingaviablemodelfor
studyinghealthbehaviour.Thepresentationaboveofafewmodelshighlightsthis
problem.However,Cummingsetal.(1980)afterexamining14modelsofthiskindpointed
outthatalthoughthemodelsdifferintheirtheoreticalperspective,thetypesofhealth
behaviourstheyexplainandthesetoftermstheyusetolabelthedifferentdimensions
andvariables,thegeneralclassesoffactors,atleastsuperficially,appeartobequite
similar.Theyhavesuggested“thatthenumberoftrulydistinctconceptsrelevantto
explaininghealth‐relatedactionsisconsiderablylowerthanthelargenumberofvariables
currentlyemployed”.(p.123).Theseauthors,usingtheactualmodeldeveloperstoactas
judges,examined109variablesextractedfromthefourteenmodelsandcategorisedthem
onthebasisoftheirsimilarities.Sixmajorcategoriesemerged:
“1 accessibility to health care,suchastheindividual'sabilitytopayforhealth
careandawarenessofhealthservices,andtheavailabilityofservices;
2 attitudes towards health,suchas,beliefsinthebenefitoftreatmentand
beliefsaboutthequalityofmedicalcareprovided;
3 threat of illness,suchas,theindividual'sperceptionofsymptomsand
beliefsaboutsusceptibilitytoandtheconsequencesofdisease;
4 knowledge about disease;
5 social interactions, social norms and social structure,and,
6 demographic characteristics(socialstatus,incomeandeducation),”(p.137).

29
Thisstudycontributestowardsamoreunifiedapproachtounderstandinghealth
behavioursanditsintegrativeapproachhasgreatermeritsforinvestigatinghealth
behavioursinvariouspopulationsandsocio‐culturalsettings.

30
2.4CRITICALISSUESINHEALTHBEHAVIOUR
2.4.1 PERSONALANDDEMOGRAPHIC
Severalstudieshavedocumentedcertaindemographicpatternsrelatedtohealth
behaviours.Onesuchstudy(ChristieandLawrence,1978)foundthatattitudestowards
hospitalizationwascorrelatednegativelywithageamongmenandpositivelywithage
amongwomen.
Otherresearchershavenotedgenderdifferencesinhealthbehaviours.Morementhan
womensmokealthoughtherateofdeclineofsmokingismorerapidamongmenthan
women(Fioreetal,1989).Higheralcoholconsumptionhasbeenreportedinmen,
althoughmorewomenhavemoremultipleaddictioninwhichalcoholiscombinedwith
prescriptiondrugs(KossandWoodruff,1991).Withregardtoproblemsofeating,obesity
anddietingtheincidenceofthesedisordersaremorecommonamongwomenthanmen.
Regardingtheutilisationofmedicalcare,itwasfoundthatwomenbetweentheages17
and44maketwiceasmanyvisitstoadoctorthanmen(Verbrugge,1985).Verbrugge
pointsoutthatthemeannumberofvisitsmadebywomentoadoctoris30percent
higherthanformen(ie.aftercontrollingforvisitsrelatedtochildbirth)andthatafterthe
ageof45yearswomen'soutpatientvisitsstillexceedthatofmenby10percentto20
percent.Althoughwomenseemtohavemorechronicillnessesandvisitdoctorsmore
frequently,therateofhospitalisationbetweenthegendergroupsarenotdifferent.
Women'saveragelengthofstayinhospitalsaremuchshorterthanthatofmen.Itis
generallyacceptedthatwomenusemoretypesofmedicationsandtoagreaterextent
thanmendo(Svarstadetal.,1987;Verbrugge,1985).
ZadoroznyjandSvarstad(1990)haveshownthattogetherwithgender,employmentis
alsoassociatedwithlowerincidenceofdruguseamongmenbutnotamongwomen.Ina
studybyLaveetal.(1979)itwasfoundthatlow‐income,unmarriedmaleswhohad
recentlymovedintoacommunitywereleastlikelytohavearegularsourceofhealthcare.

31
Womenandmarriedpersonsresidinginacommunityforsometimeandwhohadhigher
incomeshadamorestablesourceofhealth.Anotherstudyshowedthatevenwhen
economicbarrierstohealthcareareremoved,poorpeoplestilldonotusedentalcareto
thesamedegreethatricherpeopledo.Luft,HersheyandMorrel(1976)observedthatin
aruralcommunitythe“healthstatus”andthe“regularsourceofcare”werebetter
predictorsoftheuseofservicesthanincomeormedicalinsurance.Wan(1976)showed
thathealthstatusisafunctionofemploymentstatusinadditiontotheseverityof
disability,theneedforassistanceinmobilityandpsychologicalwell‐being.Working
womentendtohaveadifferentsetofhealthbeliefsandpracticesthannon‐working
womenandthisisconsideredanimportantfactorresponsibleforlowermorbidityintheir
children(Murabaketal.,1990).
Educationhasbeenfoundtoinfluencetheselectionofservicesotherthanthoseofdistrict
clinics(Titkow,1983).IntheU.S.A.educationhasalsobeenfoundtobepositively
correlatedwiththeuseofhospitals(Okafor,1983)andtheseekingofabortionatclinics
(Liet.al.,1990)
AccordingtoMcClain(1977)peoplewhoareacculturated(i.e.especiallythosewhoare
younger,wealthier,andbettereducated)usewesterntreatmentfacilitiestoagreater
extentthanthosewhoarelessacculturated.
2.4.2 HEALTHBELIEFS
Thehealthbeliefsthatpeoplehaveinfluencehowtheyrespondwhentheyperceive
themselvesasill,howtheypreventillness,maintaingoodhealth,diagnosesymptomsand
treatbothersomeand/orpersistentconditions.Theymaytreatthemselvesorconsult
familyorfriends.Clymer,BaumandKrats(1984)foundthatpatientsafterevaluatingtheir
symptomsmostlytreatthemselvesorseekhelpfrommedicalprofessionalsor
alternativelyconsultfolkortraditionalhealers.AccordingtoMechanic(1983)and
ChristmanandKleinman(1983)medicalpractitionersarenormallythelastchoice.

32
AccordingtoMechanic(1976a)healthcarefacilitiesarealsoaffectedbyinter aliathe
dominantbeliefsaboutillness,accessibility,financialmeans,thestigmaassociatedwith
help‐seekingandorganisationalbarriers.Ofthesefactorssharedculturalbeliefsandstyles
(i.e.culturallysanctionedwayofdoingthings)areparticularlyimportant.Inthefollowing
chapterculturalbeliefsspecifictoAfricanpeoplewillbediscussed.
2.5SOCIALSUPPORTANDHEALTH
Thereisanabundanceofresearchthatdemonstratesthepositiveeffectsofsocialsupport
tohealthandhealthbehaviour(CohenandSyme,1985).Theabsenceofsocialsupporthas
beendirectlyrelatedtoincreaseofpsychologicalandpsychiatricsymptomatology
(Henderson,etal.,1978,1980;KesslerandMcLeod,1985)aswellasphysicalillnesses
(Gore,1978;Sarason,etal.,1985;WortmanandConway,1985;Schaefer,Coyneand
Lazarus,1981;Östergren,etal.,1991).Socialsupportisknowntoactasabufferbetween
stressfullifeeventsandhealth(Östergren,1991;Turner,1981;BillingsandMoos,1981)
eveninextremestressfulsituations,suchas,theviolenceinSouthAfrica(Dawes,1990).
CohenandSyme(1985),inattemptingtointegratethefindingsinthisvastarrayof
literaturethatincludesmultipleperspectives,definitionsandoutcomes,definesocial
supportas“theresourcesprovidedbyotherpersons.”(p.4).Socialsupportincorporates
severaldimensions,whichTardy(1985)dividesasfollows:thedirection of support(ie.it
canbegivenorreceived),disposition (theavailabilityvs.utilizationofresources),
description of support versus evaluation of satisfactionwithsupport,content(whatform
thecontacttakes),andnetwork(whatsocialsystem/sprovidethesupport).Social
networkshavebeenfoundtoinfluenceavarietyofhealthbehaviours,namely,theseeking
ofmedicalcare,theinfluenceoflayreferralsandtheutilisationofservicesinfluencedby
family,relativesandfriends.
Twoviewshavebeenputforwardonhowsocialsupportoperatestoimprovehealth.One
viewisthatsupportactsasabuffer thatprotectstheindividualfromtheharmfuleffects
ofstressorstressfulsituations.(CohenandMckay,1984;Dawes,1990).Accordingtothis

33
view,supportmayintervenebetweenthestressfulevent(orexpectationofit)andthe
stressexperience,byreducingorpreventingastressresponse,orbyeliminatingthe
stressexperiencebyinfluencingresponsibleillnessbehavioursorphysiologicalprocesses
(CohenandSyme,1985).
Theotherviewisthedirect effecthypothesisthatsupportenhanceshealthandwell‐
beingregardlessofthelevelofstress.Itisbelievedthattheperceptionthatothersare
willingtohelpcouldresultinincreasedoverallpositivefeelings,enhancedself‐esteem,
stabilityandcontroloverone’senvironmentwhichinturnmayinfluencesusceptibilityto
illnessbyindirectlystrengtheningtheimmunesystem(Zimetetal.,1988).
Itmaybethatbothviewshavevalidity.Whilesocialsupportmaybedirectlyhelpfulinall
circumstances,itmaybeparticularlyeffectiveasabufferduringstressfultimes(Zimetet
al.,1988).
2.6SYMPTOMSANDSYMPTOMPERCEPTION
Leventhal(1986)pointsoutthattheimportanceofsymptomscanbeviewedfromthree
perspectives:thatofpublichealth,medicineandlaypeople.Firstly,fromthepublichealth
perspective,householdsurveysprovideusefulinformationontheincidenceand
prevalenceofavarietyofdiseaseswhicharenecessaryforthecontrolandplanningof
publichealth.Secondly,inmedicine,symptomreportingisoftentheinitialcontactwith
medicalprofessionalsthatguidesthehypothesisformationaboutunderlyingconditions,
theorderingoffurthertestsandthemakingofadiagnosis.Lastly,symptomsareof
particularimportancetothelay‐personsinceitisanessentialstepintheprocessof
seekinghelpforillness.
Peopleexperiencesymptomsofillnessonafairlyregularbasis(Bishop,1984;Mechanic,
1978)althoughmanyofthesesymptomsareignoredandgountreated.InBishop'sstudy
(1984),some“seeminglyserious”symptomswentuntreated.Itwouldappearthenthat

34
theconceptualizationofillnessplaysacriticalroleindeterminingaperson'sillness
behaviour(BishopandConverse,1986).Matthews,etal.,(1983)haveshownthatthe
interpretationgiventosymptomsinfluencesboththeurgencywithwhichhelpissought
aswellassick‐rolebehaviouritself.Illnessrepresentationshavebeenfoundtoplaya
crucialroleinillnessbehaviour.BishopandConverse(1986)inastudyonhowlaypeople
cometoidentifyasetofsymptomsasindicatingaparticulardisease,found“that
informationaboutphysicalsymptomsisorganisedandprocessedaccordingtopre‐existing
beliefsabouttheassociationbetweenparticularsymptomsanddiseases.”(p.95).
Accordingly,these“diseaseprototypes”helpindividualsmakesenseofthechangesthey
experienceandwhattodoaboutthem.Thesediseaseprototypes,however,mayormay
notbeaccurateandmaynotalwaysresultinoptimalhelp‐seeking.
Ontheotherhand,symptomsarenotalwaysreliableindicatorsofdisease.Reasonsfor
suchaviewcomefromsexdifferencesinreportingsymptoms.Womenontheaverage
reportmoresymptomsthanmen(Verbrugge,1985).Thereisalsoalackofclarity
betweenpsychologicalconditionsandsymptoms(somatoformdisorders),symptomsas
productsofenvironmentalconditioningandsymptomsasindicatorsofmental,socialand
diseasestatus(Leventhal,1986).Levenstein(1990),isoftheopinionthatsymptomson
theirownhaveno‘objectivereality’andthat,therefore,aphysicianshouldunderstandhis
patientratherthaninterprethisorhersymptoms.
2.7LIFEEVENTS,STRESSANDILLNESS
Stresshasbeenlinkedtothedevelopment,exacerbationandmaintenanceofanumberof
healthproblems.Severalstudieshaveshownthatthereisadirectrelationbetweenstress
andphysicalillness(RaheandLind,1971;HolmesandRahe,1967;Feuerstein,Labbéand
Kuczierczyk,1987;Selye,1956;TurtonandChalmers,1990;Steptoe,1991).
Severalmodelshavebeenpostulatedtoexplaintheroleofstressintheetiology,
exacerbationandmaintenanceofphysicalillness.Oneofthemostfrequentlycitedisthat
ofSelye(1956),whofocusedonneuro‐endocrineaspects,andconceptualizedstressasa

35
non‐specificresponseadaptedtoprotecttheindividualfromanydemandsmadeonhim
orher.Further,thatstresscanresultfrombothpositiveandnegativeresponses.Levi's
model(1972)suggeststhatanypsycho‐socialchangecanactasastressorandthatthis
stimulusactsneuro‐endocrinolgicallyinapredisposedway.
InRaheandArthur'smodel(1978),emphasisisplacedonthesignificanceofrecentlife
changesorsituationswhichareinfluencedbytheindividual'sperceptiveset.The
perceptivesetisinfluencedbythesocialsupportsandearlylifeexperiences.Includedin
thismodelistheuseofpsychologicaldefenseswhichreducephysicalarousalandasa
resultreducesusceptibilitytoillness.Figure1belowpresentsanoverallviewofthe
conventionalstress‐vulnerabilitymodel(Steptoe,1991).
Steptoe(1991)maintainedthatthepsychobiologicalstressresponse(StageIIinFigure1)
isalooselycoupledsysteminvolvingadjustmentsattheaffective,cognitiveand
behaviourallevels,togetherwithassociatechangesinneuroendocrine,autonomicand
immunefunctionwhichhavebeenchallengedinmodernresearch.Firstly,hechallenges
thenotionofnonspecificity(Selye's‘nonspecificpatternofactivation’)becauserecent
studieshaveshownthatthepatternofneuroendocrineandautonomicresponsesvaries
accordingtotheemotionaldemands.Thatis,itisnotsimplyanintensityeffectbuta
consequenceofcopingbehavioursengagedinthesituation.Secondly,itisdifficultto
applytheviewthatphysiologicalstressresponsesareadaptedtobolstertheorganism's
biologicaldefenceswhichmanifestasanti‐inflammatoryandimmunosuppressiveeffects
ofglucocorticoids.Itissuggestedthatseveralcomponentsoftheactivationprofilemay
havea“regulatoryratherthanadirectresistancefunction.”(p.635).Thirdly,theviewthat
peripheralphysiologicalchangesaresecondarytocentralnervoussystemactivationinthe
stressprocessismisleadingsincerecentevidencesuggestsabi‐directionaltrafficbetween
thetwo.
AccordingtoSteptoe(1991)therearetwomajorissueswiththemodelslinking
psychobiologicalstressresponseswithillness.Firstly,whydosomepeoplebecomeill
whenexposedtoadversecircumstancesandexperienceswhileothersdonot(‘intensity

36
issue’).Secondly,whydosusceptiblepeoplewhohavesimilarlifeexperiencesdevelop
differenttypesofillness(variabilityissue).Theseindividualdifferencesinillness
susceptibilityisascribedtobiologicalpredispositions(refertoFigure1‐StageIII)suchas
geneticmake‐up,healthstatus,nutritionalstate,physicalfitness,andpre‐existing
pathology.Anotherpossibleexplanationforsomeoftheindividualdifferencesinthe
susceptibilityofillnessmaybetheresultofspecificpatternsofpsycho‐biological
responsestoparticularexperiences.Inadditiontothepsycho‐physiologicalview,another
position,whichisoftenoverlooked,throughwhichpsycho‐biologicalresponsesmay
influencehealthisthecognitive‐behaviouralposition.Thisviewimpliesthatcognitive,
affectiveandbehaviouralcomponentsofthepsychobiologicalresponsecaninfluence
healthindependentlyofanydirectactionofstressonthephysiologicalsystem;thatis,
thatpsychosocialstressorsinfluencehealthalterationsinhealth‐relatedbehavioursand
practices,suchas,drinkingalcohol,smoking,regularexercise,sexualbehaviourortheuse
ofseatbelts.Itwouldappearthatthefrequencyofpatternsarealteredbypsychosocial
stressratherthaninfluencingthem.Othercognitivebehaviouralprocessesinclude
attentiontobodilysymptoms,rangingfromextremepreoccupationtoavoidanceordenial
influencehelp‐seekingbehaviour.

37

38
Emotionallyexpressivebehavioursmayalsoaccountforassociationsbetween
psychobiologicalstressandillness.Forexample,in“crying‐inducedasthma”
bronchospasmisprecipitatedbycryingthroughanonspecificpathophysiological
mechanismsuchasbronchialhyperactivityratherthanaspecificpsychophysiological
cause.Studiesofcryinginducedasthmashowthatitistriggeredoffduringstress‐related
episodesofemotionaldisturbanceandismaintainedbyparentalresponses.Also,adverse
lifeexperiencesmayaffectillnessprogressionbydisruptingadherencetomedical
regimensoradvice.Thepointhereisthatcognitive‐behaviouralelementsofthe
psychobiologicalstressresponsescaninfluencethehealthstatusirrespectiveof
psychophysiologicalconnections.Hence,Steptoe(1991)suggestsanelaboratemodel
detailingthecognitive‐behaviouralandpsychophysiologicalprocessesthatmediatestress‐
illnessrelationships(seeFigure2).
Whatisclearintheprecedingdiscussionisthatstressinfluenceshealthinacomplexway.
Morespecifichypothesesrelatedtovariouscognitive‐behaviouralandphysiological
processesareneededinordertofullyunderstandtheactualprocess.

39

40
CHAPTER3
HEALTHINSOUTHAFRICA
ThehealthsystemofSouthAfricaisuniqueinmanyrespectsbecauseitsdevelopmentand
structurehasbeenstronglyinfluencedbyauniquepoliticalideologyofracialseparation.
Althoughthisideology(theapartheidsystem)hasundergoneradicalchangesinthepast
twoyears,theproblemsandeffectsofthepastwillcontinuetobeexperiencedforavery
longtime.Theracialsegregationofthehealthsystemhasledtodiscriminationand
fragmentationinhealthservicesaswellaslargedisparitiesinhealthservicesbetweenthe
differentpopulationgroups.
Therelationshipbetweenapartheidandhealth,bothdirectandindirect,ismulti‐levelled
anditseffectsarefeltinseveralways:
1 thestate‐providedhealthservicesforblackpeoplearegrosslyinadequate
(DeBeer,1984;Reddy,1990;ZwarensteinandBradshaw,1989;Chetty,1990).This
deficiencyhas,obviously,anegativeeffectonhealthcare;
2 theinequalitiesanddiscriminationshaveledtoseveresocialproblems,suchas,
poverty,unemployment,over‐crowding,pooreducationandinadequatehousing
whichnaturallyadverselyaffectthehealthstatusofthesecommunities
(DeBeer,1984);
3 dietarydeficienciesaffecthealthstatus(DeBeer,1984);
4 disruptionsinfamilylifethroughmigrantlabourandinfluxcontrolhaveincreased
thevulnerabilitytoillnessanddiseases(Uyanga,1983;Maforah,1988);

41
5 thestressoflivingunderanoppressivesystem(Dawes,1990)alsodirectlyaffects
thehealthstatusofbothindividualsandwholecommunities;
6 therestrictionanddistortionofnormalpersonalitydevelopment
(Manganyi,1977);and
7 thepromotionandmaintainingofnegativehealthbehaviourandhelp‐seeking
behaviour.
Thissectionwillfocusonthosefactorsthatcontributetonegativehealthbehaviours.One
factorthathasreceivedmuchattentionisthegrosslackofadequatehealthservicesand
healthfacilitiesforblackSouthAfricans.Theterm“healthfacility”refersnotonlytothe
physicalstructurefromwhichhealthcareisdeliveredbutalsotothequantity,rangeand
qualityofcareprovidedbythefacility.ThehealthfacilitiesinSouthAfricaarebiasednot
onlyinfavourofwhitepeoplebutalsotheaffluentandtheurban.Duringtheperiod1983‐
84,theavailabledataforthehospitalsintheTransvaalshowthattherewere6,27beds
per1000populationforwhitesand3,14bedsper1000forblacks(Buch,1987).Thelackof
servicesandfacilitiesundoubtedlyrestrictedappropriatehealthactiononthepartof
thesepeople.Moreover,thesefacilitiesarealwaysovercrowdedandasaresultthereisa
tendencytodelayseekinghelpbecauseoftheinconvenienceofspendingaconsiderable
amountoftimeinordertoseeadoctor.Patientsoftenspendawholedayinordertobe
seenbythedoctorforafewmoments.Itisnotunusualforpatientslivinginruralareasto
leavehomeandspendaweekintransit,sleepingoveratdifferenthospitalsen routein
ordertoobtaintransporttothemainteachinghospitalinthecity,onlytobeseenbya
doctorforfivetotenminutes(Dr.Hunter,personalcommunication,May1992).Within
suchacontextmedicalhelp‐seekingbehaviourwillbedeterminedalmostsolelybythe
severityoftheillness.Thereisverylittlemotivationtovisitadoctorforacheck‐uporto
screenforillnessordiseases.Itistobeexpectedthatlayorfolkmedicinewillbe
substitutedinthesecases.
Inaddition,healthcareconcernsitselfmainlywithcurativeandhospitalservices.In
certaincommunitiessuchassquatterorinformalsettlements,healthfacilitiesarevirtually
non‐existent.Buch(1987)suggeststhatoneofthereasonsforthisabsenceoffacilitiesnot
42
becomingaseriousproblemforthesesettlersisthat“suchcommunitiesarenotyetina
positiontojudgetheirhealthservicesinthesameastutemannerinwhichtheyjudgetheir
educationandhousing.”(p.52).
Healthservicelocationalsoplaysanimportantroleintermsofutilizationofservicesand
help‐seeking.Thebesthealthfacilitiesavailablehavebeendevelopedincloseproximityto
thecitycentre.Theironyofthesituationisthatnotonlyisitdifficultforruralpeopleto
reachthesefacilitiesbutitisalsonotimmediatelyaccessibletothoselivinginurbanareas
aswell.ThereasonforthisisthatduetotheGroupAreasAct,theurbanblackissettled
awayfromthecitycentre.Blacksarethusfacedwithproblems,suchas,accessibilityof
hospitalsandclinics,transportcostsandtheirinability,especiallyiftheyareold,toget
someonetoaccompanythemontheirlongtriptothecity.Thesefactorsobviously
negativelyinfluencehealthbehaviour.
Anotherfactorthatnegativelyinfluenceshealthbehaviouristhepoliticalclimateinthe
country.Intheprocessoflobbyingforademocraticgovernmentandbetterfacilities,the
ideologiesandstrategiesemployedbyvariousorganisationshavetosomedegree
influencedandaffectedthehealthbehaviouroftheAfricanpeople.“Stayaways”inJune
1991andJune1992showedsignificantdecreaseinvisitsbypatientstohospitals
providingservicesprimarilytoblacks(e.g.KingEdwardVIII)andatblackprivatepractices
aswell.Theprotestsandboycottsbynursesin1991andthestrikescalledbytheNational
EducationHealthandAlliedWorkersUnion(NEHAWU)inJune1992resultedinsevere
disruptionofhospitalservices,creatinginmanyinstanceshealthcrises.Hospitalswere
forcedtoreduceadmissionsandprovideonlyemergencyservices.Whiletheseprotests
andboycottsmayhavecertainnationalpoliticalimplications,itsimpactonhealth
behaviouraswellashealthcareontheimmediate,shorttermandlongtermisnotfully
considered,assessedorcomprehended.Notonlyisthehealthofindividualsjeopardized
butthesesexperienceshavethepotentialofbecomingintegratedaspartoftheirhealth
beliefs.

43
Anothercloselyrelatedfactorthathasanegativeinfluenceonhealthbehaviouristhe
responsetohealtheducationprogramsandtheuseorlackofuseofpresentservicesby
someindividualsasaresultoftheirpoliticalbeliefsandaffiliations.Stateeducation
programsandservicesareoftenviewedwithsuspicion;Forexample,therumourdoingits
roundsinsomeblackcommunitiesisthatAIDShadbeenintroducedintoSouthAfricaby
theStatetodestroytheAfricanrace.Suchviewsobviouslycontributetopoormotivation
inindividualstoattendstatehospitalsandaffectstheirattitudeandbehaviour.Another
concernisthatsometimesstatehospitalsbecomeassociatedwithpro‐government
groups.ItisworthnotingthatinNataltherearestrongaffiliationsamongblackstoboth
theAfricanNationalCongress(ANC)andtheInkathaFreedomParty(IFP).Thelatteris
oftenregardedaspro‐government.(MuchoftheviolenceinNatalhasbeenascribedby
mostpoliticalanalystsasemanatingfromclashesbetweenthesestwogroups.Thereisa
beliefinsomeblackcirclesthatthegovernmenthasperpetuatedtheviolence).For
example,itisquitecommonforpsychoticpatients,whoareadmittedtothepsychiatric
wardatstatehospitals,todevelopdelusionsofbeingindangerfromotherpoliticalgroups
becauseofthebeliefthatthehospitalisinsympathywiththatparticulargroup,orthey
maydevelopadelusionthattheyaregoingtobe“brainwashed”bythegovernmentif
theyarehospitalised.Insomecasesmedicalfacilitiesmaybeunderutilisedpartlybecause
ofthepoliticalallegianceofpeopleinitsenvironmenttoanti‐governmentgroups.Acase
inpointisthePrinceMshiyeniMemorialHospitalinUmlazi.Thisdistrustofmedicalcare
systemshasbeennotedamongstminoritygroups,suchas,Jews,PuertoRicansandBlacks
inNorthAmericaaswell(Geertsen,etal.1975;Lendt,1960).
Further,aperson’sbeliefthatbettertreatmentisprovidedatonlycertainhospitalsmay
alsoinfluenceequitableuseofhealthservices.Forexample,patientsofteninsiston
comingtoKingEdwardVIIIHospitalandnotattendafacilityclosertothembecausethey
believethatsuperiortreatmentisprovidedhere.
3.1CULTURALINFLUENCESONHEALTH

44
Itiswellknownthatculturaldeterminantsplayanimportantpartinmaintainingasense
ofgoodhealth.Culturalvalues,normsandexpectationsinfluenceandshapebeliefs,
lifestyles,familyinteractions,roles,socialorganisationandinstitutions(Gochman,1988).
Culturalinfluencesaffectnotonlyperspectivesonhealth,illnessanddisease(e.g.patterns
ofdiseases)butalsoavarietyofhealthrelatedbehaviours,suchas,beliefsthatunderlie
theutilizationofservices(BerkanovicandReeder,1974),seekingofmedicalcare
(BerkanovicandTelesky,1985)responsestopain,responsestosymptoms,(Guttmucher
andElinson,1971;KlienmanandSung,1979),thesick‐role(Davis,1984)andtheuseof
traditionalhealers(Uyanga,1983;FreemanandMotsei,1992).Suchman(1965a)
emphasizedtheplaceofculturalpatterningonsocialorganizationandhealthservices.The
“totalculture'sbeliefsandbehavioursrelatedtohealth,anditssanctioningandorganizing
ofhealingpracticesarereferredtoasa‘healthculture’”(Gochman,1988,p.243).
ForblackSouthAfricans,alongsidethewesternmedicalsystemexistsanoldtraditional
systemofhealingandhealthcare.Theirculturalandsocialbeliefshavebeenshownto
contributetothewaytheyconceptualizeillnessanddiseaseandusehealthcarefacilities.
Traditionally,theyviewillnessintermsofnatural,moralandmagicalaetiologies.See
Figure3below(Wessels,1985a,1985b).

45

46
Ngubane(1977),indiscussingmodelsofillnessamongZulus,notesthedistinction
betweenillnessesthatareuniversalandtreatablebiomedically(umkhuhlane)andthose
whichmayrequireritualisedandindigenouscures(ukufa Kwabantu‐diseaseofthe
Africanpeople).Umkhuhlane,accordingtoNgubane,refersmainlytothoseillnessesthat
“justhappen.”Theyincludeillnessesthatrangefromcommoncoldstoseriousepidemics
suchassmallpox.Theyareseenaspartoftheprocessofageingresultinginthe
dysfunctionofindividualbodyorgansandalsoincludeorganmalfunctionthatmayleadto
otherillnesses,suchas,excessivebileaccumulation(inyongo)whichisbelievedtocause
headaches,nauseaandgeneraldebility.Includedinthiscategoryarediseasesassociated
withdevelopmentininfants;forinstance,measles(masisi),mumps(uzagiga)and
discomfortduringteething.Alsoincludedinthiscategoryareillnessesassociatedwith
seasonalchanges,suchas,diarrhoea(uhudo)andhayfever(isithimulane)whichoccur
mainlyinthesummer.Umkhuhlane mayalsorefertodiseasesthatarebelievedtobe
inherited.Theseincludeepilepsy(isithuthwane),chronicchestpain,asthmaorchronic
bronchitis(ufuba),skininfections(umzimba omubi)aswellasmentalretardationand
certainmentalillnesses(ufuzo).
Medicinesthatareusedtotreattheumkhuhlane categoryofillnessesarebelievedtobe
verypotentandthereforethereisnoneedfortheiradministrationtobeaccompaniedby
rituals.Peoplearereadytoexperimentandtryanynewmedicinetotreattheseillnesses.
Hencewesternmedicinesforthisclassofillnessesarereadilyaccepted.
Theothercategory(ukufa kwabantu)includesillnesseswhoseaetiologyandmeaningis
basedonAfricanculture.AccordingtoNgubane(1977),ukufa kwabantuisusedto
indicatethat“notonlythedisease,ortheirsymptoms,areassociatedwithAfrican
peoplesonly,butthattheirinterpretationisboundupwithAfricanwaysofviewinghealth
anddisease.”(p.24).Itiswiththiscategorythatmentalhealthworkers,suchasclinical
1 Ngubane's Body and Mind in Zulu Medicine represents the most comprehensive primary source on Health and Disease in the Nyuswa- Zulu thought and practice and is very frequently referenced by most researchers in cross-cultural studies. This source is extensively used in this study. This study has also greatly benefited from this source.

47
psychologistandpsychiatrist,aredirectlyinvolved.(Itisthereforegivenfullertreatmentin
3.2).
Itisimportanttonotethatalthoughthisdistinctionbetween“African”and“non‐African”
illnessesisoftenreferredtointheavailableliterature(Cheetam&Cheetam,1976;
Edwardsetal.1983;LeRoux,1973;Wessels,1984a),itisnotwithoutsomelackofclarity.
Forinstance,Mills(1983;1985)hasfoundthatsomeillnessessuchastuberculosisare
viewedbysomeAfricancommunitiespurelybiomedicallywhereasinothercontextsthey
areviewedinthetraditionalway.
3.2AETIOLOGYOFILLNESSINTHEAFRICANWORLDVIEW
3.2.1 EnvironmentalImbalance
AccordingtoNgubane(1977)conceptsofecologyarecentraltotheZuluideaofhealth
andexplanationsofill‐healthmayoftenlieininterpretationsofenvironmental
imbalances.Thebeliefisthatthereisaspecialrelationshipbetweenapersonandhis
environment,andthatplantandanimallifeaffecttheenvironmentaswell.Because
differentplaceshavedifferenttypesofplantsandanimals,environmentsandatmospheric
conditionsvarybetweenregions.Peopleareacclimatizedtowheretheyliveandmoving
toanewregionmayleadtoillnessuntiltheyhaveadaptedtothenewplace.Itisalso
believedthatwhenmoving,bothanimalsandpeopleleavesomethingofthemselves
behindandalsoabsorbsomethingfromtheatmosphereintowhichtheymove.This
“something”thatisleftbehindiswhatisusedbydogswhentrackingandisknownas
umkhondo(track).These“foreignelements”arethusintroducedintoaregionbypeoplein
theirtravelsorwildanimalsandbirdsthattravellongdistances.Theumkhondomaybe
visibleorinvisible;harmlessorharmful.Harmfultracksarereferredtoasemibi(bad).A
personmaycontactadiseasebysteppingoveradangeroustrackorbreathingitin.The
wordumequisusedtorefertoalldiseasescontractedbysteppingoveradangeroustrack,
regardlessofthesymptoms.Theenvironmentmaynotonlybepollutedbytracksbutby
48
thingsdiscardedduringthetraditionalhealingofsomeone,aswellasbynoxious
substancesplacedbysorcerers.Inthiswaytheenvironmenthasthepotentialtobecome
dangerous.Inordertodevelopandmaintainresistancetoevilorillnessesanequilibrium
mustbeestablishedbetweenapersonandhisorherenvironmentaswellasbetween
individualsinasociety.Thisresistanceisneededbecauseitisalsobelievedthataperson
maybeoverpoweredbythepresenceofanotherpersonandbecomeill.Thebalancewith
theenvironmentisachievedbytheuseof“strengtheningmedicines”.Ideally,
strengtheningshouldoccuratleastonceayearinspringbeforethethunderstorms
becausethesestrengtheningtreatmentsprotectagainstlightningaswell.
Ecologicalfactorsareconsideredtheprimarycauseofavarietyofillness.Forexample,
babiesthatcrycontinuously,appearfearfulorshowgeneraldistressaresaidtosuffer
frominyamazana(problemsresultingfromcertainwildanimaltracks).Greenstool
resultingfromdiarrhoeaandawhite‐coatedtonguearebelievedtobetheresultof
contaminationfromlighteningfumes.Miscarriages,still‐birthsandinfantmortalityisalso
associatedwithpollutantsintheenvironmentwhicharecontractedbypregnantor
nursingmotherswhotheninfecttheirbabies.Inadults,symptomsrangingfromgeneral
infirmityofthebodytoevilpossessionareassociatedwithdangersintheenvironment.
3.2.2 SorceryandIllness
Illnessesmayalsoresultfromsorcery(ubuthakathi).Therearethreetypesofsorcerers:
Thefirst,isthe“nightsorcerer”whoisbelievedtobeevil.Theyarealwaysmenandthey
harmothersfornoapparentreason.Anightsorcererusesevilmedicines(potions)andis
believedtohavesupernaturalpowers,suchasresurrectingcorpsesbut,hecannotfly,
changeshape,becomeinvisibleorperformactsassociatedwithwizards.Hisaim,
accordingtoNgubane(1977),istomaketheenvironmentdangerousorputpeopleoutof
balancewiththeenvironment.Heachievesthisbyplacingharmfulmedicinesinthe
environmentsothatpeoplemaystepoveritandcontractumeqo.Thesecondtypeis
referredtoasthe“daysorcerer”whoactsoutrivalryandcompetition.Thesesorcerers

49
maybemenorwomen;thelatterareinthemajority.Theirmethodofharmingpeopleis
referredtoasukudlisa,whichistheaddingofnoxioussubstances,includingwestern
poisons,tothevictim'sfood.Theymayusesupplementarytechniques,suchas,placing
harmfulsubstancesinthevictimspathorstealportionsoftheirvictimssacrificialanimalin
ordertonullifythesacrificeorreverseitspurpose.Thethirdtypeisthe“lineagesorcerer”
(uzalo).Theuzalo aremembers(onlymen)ofacommonlineagewhosharecertainritual
andsocialobligationstowardseachother.Theyarenotsupposedtopractisenightorday
sorceryagainsteachotherbecausethiswillangertheancestors.However,amancan
persuadetheancestortofavourhimandabandononeormoreoftheothermembersof
thelineage.Thisisachievedbytheuseof“blackmedicines”(ukuphehla amanz'amnyama)
inthetreatmentofdisease.
3.2.3 AncestorsandIllness
Ancestors(Ngubane,1977)areprimarilyconcernedwiththewelfareoftheirdescendants.
Whenthingsgowell,peoplebelievethattheyhavethesupportoftheancestors
(Abaphansi banathi)andwhenmisfortunebefallsthem,theancestorsarebelievedtobe
“facingawayfromthem”(Abaphansi basifulathele).Therearetwoclassesofancestors:
thosewhocanpunishorprotectandreward,suchas,aman'smother,father,paternal
grandparentaswellaspaternaluncles;andthosethreegenerationremoved,whodonot
punishorrewardbutareallowedasguestsoftheformerancestralgroup.Theancestors
arebelievedtoliveunderneaththeearth.Theyfrequentthehutofthemostsenior
womenofthegroup(indlu enkulu)andthebyre.Theancestorsareappeasedthrough
sacrifices.Thefollowingisthelistofthesacrificesthatareperformed:
1 Imbeleko‐asacrificetoplaceababyundertheprotectionofancestors;
2 Ukubuyisa‐asacrificetointegratethedeceasedwiththerestofthebody
ofancestralspirits;
3 Ukubonga‐asacrificeforgoodthingsinlife,eg.winningmoneyand
obtainingagoodjob;
50
4 Ukucela izinhlanhla‐asacrificetoseekblessingsfromtheancestorsbefore
undertakinganymajororriskytask,eg.goingtoamajorcitytoseek
employment;
5 Ukushweleza ‐asacrificetoappeasetheancestorsifthereisevidencethatthey
havebeenannoyed;.
6 Ukuthetha‐asacrificeto“scold”theancestorsifmisfortunecontinuesin
spiteoftheirattempttoappeasethem;and
7 Ukukhomba inxiwa‐asacrificewhenmovinghousetoshowtheancestors
thenewhome(Nugubane,1977).
Withouttheprotectionofancestorsthepeoplebecomevulnerabletomisfortuneaswell
asdiseases.Ancestorsaremostoftenannoyedbyquarrellinginahome,lackofpeaceor
thenon‐fulfilmentofmaritalduties.Examplesofillnessesandmisfortunesresultingfrom
thedispleasureoftheancestorsareinfertility,miscarriages,delayedconception,the
suddenillnessofchildren,strokes,paralyses,sleeplessnessandtensionorstrifeinthe
household.

51
3.2.4 Umnyama andIllness
AnotherimportantconceptintheAfricanviewofillnessisumnyama(Ngubane,1977).It
canbetranslated“pollution”whichisconceptualizedas“amysticalforcewhich
diminishesresistancetodisease,andcreatesconditionsofbadluck,misfortune
(amashwa),‘disagreeableness’and‘repulsiveness’(isidina)wherebypeoplearoundthe
patienttakeadisliketohimwithoutprovocation”(p.78).Umnyama initsworstformis
contagious.
Thebehaviouralpatternofthoseinastateofumnyamaisreferredtoasukuzilaandis
characterizedbywithdrawal,asocialbehaviourandabstinencefrompleasurableactivity;
Thoseinflictedbecomepassive,softlyspokenandlethargic;theylosetheirappetitesor
eatsmallquantitiesofpoorqualityfoodanddresssloppily.Post‐partumwomenare
regardedaspolluted(umdlezane)andcanpolluteandcauseill‐healthtotheirchildrenand
family.Thevirilityofmenisaffectediftheyeatfoodcookedbyherorshareeatingutensils
withher.Sheistobeconfinedbecauseevencontactwithcattlewillstoptheirproduction
ofmilk.Shemaynotevengointothefieldslestthecropswither.Otheroccasionsof
pollutionaremenstruation,sexualintercourse(menandwomenareconsideredpolluted
thedayfollowingsexualintercourse),premaritalsex(i.e.thefemalesareconsidered
polluted)andfighting.
Pollutionisalsoassociatedwithdeath.Itisbelievedthatpollutionemanatesfromthe
corpseandthosethathandlecorpsesandthoseassociatedwithdeatharepolluted.This
pollutioniscontagious.Certaindeathsareregardedasmoreintenselypollutingthan
others.Thesearedeathsthroughcaraccidents,drowning,beingstruckbylightning,
fighting,murderand,thosewhodieofincurablediseases,epilepsyandchronicchest
diseases.Theirbodiesareneverbroughttothehomebutareburiedoutsideandweeping
isrestrained.Withregardtomurder,inadditiontothepollutionofthedeath,the
murdererisespeciallypolluted.

52
Itisinterestingintheresolutionofthispollutionthroughritualthatpsychologicalaspects
ofimportantlifeeventsareaddressedanddealtwith.Thetraditionalritualsandcultusis
endemictotheprocessofcopingwiththestresses,anxietiesandemotionalinstabilitythat
accompanyimportanteventsinboththelifeofindividualsandcommunities.Clinical
psychologistsprobablyobtaintheirmostimportantcluestounderstandingthepsycheof
theirAfricanpatientstotheextenttheattitudesinformingtheseritualresolutionsare
understood.AsNgubane(1977)pointsout“emotionalstressesenduredduringbothbirth
anddeath—thetwomainspringsofpollution—arepreventedfrominitiatingneurosesby
thediversionoffocusfromunpleasantexperiencestoacomplexityofritualbehaviour.
Thementalstressesandstrainsexperiencedduringthemajorlifecrisesareseenasa
possiblecauseofpermanentdamagetosomepeople'smentalbalance,andthisis
expressedasanoutcomeoffloutingthebehaviourpattern.”(p.82).Wemayaddthateven
wherethereisnodangerofmentalimbalance,thetraditionalperceptionoftheall‐
pervadingpossibilitythatpollutionaffectsgeneralattitudestopsychologicalwell‐being
andsicknessorhealthbehaviour.
3.3ILLNESS,SICK‐ROLEANDHELP‐SEEKINGBEHAVIOUR
AccordingtoNgubane(1977),inZulusociety,whenpeoplefeelsicktheyreportthisto
thosearoundthem.Theyobservethesymptomsandtryandassociateitwithadisease,at
firsttodecidewhetheritisaminorailmentwhichcouldbetreatedathomeoraserious
illnesswhichneedstheattentionofanexpert.Theseverityoftheillnessisassessedbythe
behaviouroftheperson.Ifapersonissickbutcontinuesworkingheorsheissick“but
goesaboutwithit”(uhamba nako).Ifheorsheliesdown(ulele phansi)theillnessis
consideredseriousandthosearoundhimorherbecomeconcerned.
Ifminorailmentspersistorworseninspiteofhomeremedies,anoutsideopinionis
soughtbytakingthepersontoeitheradoctororatraditionalhealer.Itwouldappearthat
noparticularhelp‐seekingbehaviourpatternisfollowedhere.Thedecisiontocontacta
doctororhealerisinfluencedbyfactorssuchastheseriousnessoftheillness,availability
53
ofhealthservices,financialimplicationsandthepersonresponsibleforthedecision.The
headofthehomehastomakethedecisionwhethertoseeatraditionalhealer,doctoror
homeremedies.Iftheheadofthehouseholdisabsentanothermaymakethedecisionbut
nomajordecisionsuchashospitalisationcanbemadewithoutconsultingtheheadofthe
home.Itisimportanttonoteherethatsincetheheadisusuallyawayfromhome(e.g.he
maybeamigrantlabourerinanothercity)thedelayinconsultationcontributestodelays
inhealthaction.
Supportisusuallyprovidedbytheimmediatefamilywhonurseandgivethepatient
attentiondayandnightifrequired.MsengiandDaynes(1981)reportedthatthe
managementofillnessofAfricansintheTranskeiwasprimarilydonebyrelativesandthen
neighbours.Doctors’ordersarestrictlyadheredtoandifnecessaryoutsidevisitorsmay
notbeallowedtovisitthepatient.Familymembersinastateofumnyamamaynotcome
intothehousewerethepatientis.
Ngubane(1977)referstocertaintypicalattitudesandbeliefsthatareimplicitinthis
world‐view.Forinstance,malingeringistreatedwithgreatcontemptandnoself‐
respectingpersonwouldconsiderit.Withregardstosick‐role,apersonisencouragedto
getupassoonasheorshecanbecauseitisbelievedthatlyingdown(unlessabsolutely
necessary)weakensthebody.Gettingupandmovingaroundisbelievedtospeedup
recovery.Africansocietyencouragesstoicism.Painisexpectedtobetoleratedwithout
complaining.Forexample,awomaninlabourwhodoesnotutterasoundiscongratulated
andcomplimentedwhereasthosethatcrydisgracetheirfamily.Inaddition,asickperson
isencouragedtoeattostrengthenthebodyandpromoteaspeedyrecovery.Softfoods
andliquidsarepreparedforthosewithpoorappetites.Inthecaseofinfantswithlossof
appetite,theyare“forcedfed”bytheprocessukaxaka,whichistheholdingofthenoseof
childrensothattheybreathethroughtheirmouthwhichforcesthemouthopensothat
theycanbefed.
3.4TRADITIONALTREATMENTS

54
Traditionaltreatment,accordingtoNgubane(1977),isprovidedbytheinyanga
(traditionaldoctor)andisangoma(diviner).Theinyanga,usuallyaman,mustfirstserve
anapprenticeshipforaperiodnotlessthanayear.Sometimestheskillispassedfroma
fathertoasonwhoshowsaninterestintraditionalmedicine.Theisangoma,usuallya
woman,isrequiredtohaveacomprehensiveknowledgeoftraditionalmedicine.Aperson
is“called”orchosentobeaisangomabytheancestorswhobestowspecialpowersonthe
individual.Inadditiontotheinyangaandtheisangomatherearethosewhoprepare
medicinesforaparticulartypeofillnessorpossessknowledgeonhowtodealwith
particularhealthrelatedsituations—theyareknownasthe inyangaofaparticular
diseaseorcondition,forexample,inyanga yomhlabelo—thedoctorwhohandles
fracturedbones.Thesearetheequivalentsofspecialisthealers.
TraditionalhealersplayacentralroleinAfricanruralcommunitiesbuttheirinfluenceis
stillfairlyextensiveamongindustrialisedandurbancommunitiesaswell(Wessels,
1984b).TraditionalhealersaccordingtoCheetamandGriffiths(1980)andWessels(1983;
1985c)arehighlyrespectedindividualsintheircommunitiesandareusuallyconsultedfirst
byallAfricansexceptthosewhohavebecomehighlywesternized.(Wessels,1985c).De
Beer(1980)reportedthat60percentofconsultstotraditionalhealerswerefortreatment
ofadisease.Watts(1980)foundthatthereisatendencytounder‐reporttheuseof
traditionalhealerswhichmeansthatDeBeer'sestimateislowerthanitmayinfactbe.
Withtheriseanddevelopmentoftheindigenouschurches,anewtypeofhealerhas
emerged‐the“prophets”or“faithhealers”(Wessels,1987a,1987b).Theyuseboth
traditionalmethodsaswellas“Christianapproaches”intheirtreatments.Themain
differencesbetween“faithhealers”and“traditionalhealers”arethattheseprophetsare
Christianswhoarechurchleaders;Theyprayanduseholywater,andthesacramentsof
baptism,theeucharistandunction,whereasdivinersusetraditionalherbs,bonesand
medicines(Wessels,1987b;1989).Theprophetsmaybelessknowledgeableofthe
sicknessspecifictoAfricanculturethantraditionalhealers.Inadditiontohealingthose
whohavesufferedmisfortune,faithhealersministertothosewhosufferfrom

55
schizophrenia,epilepsy,mentalretardation,andinheriteddisorders.AccordingtoWessels
(1987b),faithhealersplayaveryusefulroleintheAfricancommunityinhandlingdayto
dayproblemsofliving.Hemaintainsthatbecauseoftheirefficacyinassistingpeoplein
needtheyshouldbegivenrecognitionandtrainedasvillagementalhealthworkers.The
factthattheAfricanIndependentChurchesarethefastestgrowingreligiousmovementin
Africa(thereareover3000differentchurchesinSouthAfricaalone)indicatestheextent
oftheirsuccessinAfricansocieties(Oosthuizen,1986;Sundkler,1976).
Inadditiontoritualssuchasdancing,callingupthespiritsoftheancestorsandbone
throwing(Ngubane,1977;Wessels,1985c)medicinesarealsoadministered.Theseare
usuallymadefromleaves,bark,rootsstems,bulbs,fruitand/orseedthatareeitherfresh
ordriedandsometimespowdered.Thesemedicinesareoftenboiledandtakenorally.
Theyaresometimesusedaspurgatives,usuallytoreduceexcessgallwhichisbelievedto
bethecauseofstomachdisorders.Purgativesarealsotakenintheformofanenema.Itis
believedthatthepurgativescleanoutthecauseoftheillness.Thispractice,however,has
oftencontributedtoirreparablephysicaldamageandevendeath.Inthehospitalsitisa
verycommonexperiencetofindchildrenandadultseriouslyillasaresultoftheuseof
purgatives.Variouslethalsubstanceshavebeenfoundtobeusedasenemas;themost
commonareJeyesFluid,detergents,batteryacidandpotassiumpermanganatethatare
believedtohavecleaningproperties.Someoftheherbsthatareused(e.g.impela)are
extremelypoisonous.Sometimesherbsarebelievedtomakeindividualsomnipotent.For
example,intelezi,whichisgiventoindividualstomurderothersbuttheseindividualswill
notcometodangerorfeelremorseovertheiractions.
Theherbalmedicinesaredividedintothosethathavehealingpropertiesandthosethat
areusedinritualsandhavesymbolicmeaning.Thislattergroupisusuallyusedas
prophylacticsortoremovethecauseofillnessratherthantocureorganicsymptoms.
Faithhealersuseprayerandholywater(iziwasho)forthispurpose.
Based on actual cases seen by the author.
Based on actual cases seen by the author.

56
CHAPTER4
METHOD
4.1SUBJECTS
Thetotalsampleinthisstudy(N=892)consistedof3groupsofurbanAfricanswhowere
20yearsandolder.Group1(N=376)comprisedfirsttimeattenderstothemedical
outpatientsdepartmentattheKingEdwardVIIIHospitalinDurban,SouthAfrica.Theages
rangedfrom20to74yearswithameanof34,88years.Group2(N=362)andGroup3
(N=154)weresamplegroupsdrawnfromtheUmlaziTownshipandtheKwaMashu
Townshiprespectively(seefigures4and5).Thenumberofsubjectsselectedforeachof
theGroups1,2and3weredrawnpro ratatothetotalpopulationofthehospitalout‐
patients,UmlaziandKwaMashutownships,respectively.Throughoutthestudythe
groupswillbereferredtoandidentifiedasfollows:Group1willbereferredtoasthe
HospitalGroup,Group2astheUmlaziGroupandGroup3astheKwaMashuGroup.
TABLEIDISTRIBUTIONOFSAMPLEBYSEXGroup Male(%) Female(%) TotalHospital 164 (43.62) 212 (56.38) 376Umlazi 160 (44.20) 202 (55.80) 362KwaMashu 64 (41.56) 90 (58.44) 154Total 387 (43.50) 498 (56.50) 892

57

58

59
4.1.1 GeneralHospitalGroup
TheKingEdwardVIIIHospital,wherethehospitalsamplewasobtained,wasofficially
openedinDecember1936.Originally,itspurposewastoprovidegeneralmedicalcarefor
AfricansandIndianspatientswhowereatthattimeinadequatelycateredforinthe
existingprovincialhospitals(Dyeretal.,1986).Dyeretal.(1986)pointoutthatthe
hospitalwasbesetwithfinancialproblemsfromitsinception.Thelackoffundswas
partiallyalleviatedbysecond‐handequipmentfromAddingtonHospital,Durbanandthe
initiativeofthenurseswhomademattressesfromthegrassgrowinginthehospital
grounds.Themajorproblemwastheshortageofbeds.Theproblemoftheshortageof
fundsandbedspersiststodayinspiteofthegradualbutsignificantimprovementsmade
overtheyears.Thehospitalwasextendedasmoregroundadjacenttothehospitalwas
acquired.AnotherextensionwastheacquisitionoftheWorldWarIIImperialForces
transitcampatClairwood,Durban,whichwasthendevelopedintothepresent1400‐bed
ClairwoodHospital.Furtherfacilitiesweredevelopedawayfromthehospital,suchasthe
BeatriceClinicinthecitycentrewhichisstillpresentlyoperative.Withtheinceptionofthe
MedicalSchoolin1951,majorexpansionofthehospitalwasundertaken(Dyeretal.,
1986).Today,KingEdwardVIIIHospitalisoneofthemajortraininghospitalsinthe
country.
ThemedicaloutpatientsdepartmentattheKingEdwardVIIIHospitalannuallyattendsto
over1millionpatients.Approximately1500newpatientsareseeneachweek.A
representative,stratifiedsampleoffirsttimeattenderswasselected.Aproportionofthe
samplewasdrawnoneachdayoftheweekattheoutpatientsbecauseofthevariationof
thenumberofnewpatientsattendingeachdayoftheweek.Theformulausedtoobtain
thesamplewas:
2 The choice of sampling techniques, statistical methods and analysis employed in this study were done in consultation with and under the supervision of two statisticians of the Medical Research Council (MRC).

60
where:N1 = No.ofpatientsperNday
(averageover4consecutiveweeks)
N = No.ofpatientsperweek
(averageover4consecutiveweeks)
376 = totalgroupsample
Nday = dayoftheweek
4.1.1 CommunityGroups
ThecommunitysamplesweretakenfromthetwolargestAfricantownshipsclosestto
Durbannamely,UmlaziandKwaMashu.TheUmlaziTownshipwhichislocatedtothe
southofDurbanwithapopulationof306490(populationcensus,1991‐providedbythe
CentralStatisticalServices,Durban)andtheKwaMashuTownshipissituatednorthof
Durbanwithapopulationof156621(populationcensus,1991‐providedbytheCentral
StatisticalServices,Durban).
Arepresentative,randomsamplewasused.Withtheaidofsiteplansalldwellingswere
countedandassignedanumber.Acomputerwasusedtogeneraterandomnumbers
whichwereusedtoselecttheactualhomestobevisitedbytheinterviewers.Alistof
‘spare’homeswasalsogeneratedintheadventofalternativenumbersbeingrequired.
3 This figure represents the last official census of the township. However, this figure does not take into account the large number of squatters in the area.

61
Theurbantownshipsampleswereusedasacontrolgroupbothagainstwhichthehospital
clinicgroupwascompared,andinordertovalidatesomeofthequestionnairesthatwere
usedinthestudy.
4.2METHODOFDATACOLLECTION
TheHIB(AppendixA)inthelanguageoftheparticipants,wasadministeredbytrained
blackinterviewers.Theinterviewersemployedforthisstudyhadatleastamatric
qualificationandwerefluentinEnglishandZulu.Theywerepersonallytrainedbythe
authorandafterdemonstratingsufficientexpertisewereacceptedfortheproject.They
wereaskedtoadherestrictlytotheinstructionsandthetermsdefinedinordertoreduce
thelevelofbias.Theanswerstotheopen‐endedquestionsweretakenverbatiminZulu
andsubsequentlytranslatedverbatimintoEnglish.Ifthequestionwasnotproperly
understooditwasexplainedagaininanopen‐ended,non‐suggestivewayandtheanswer
wasoncemorerecordedverbatim.Therewereseveralreasonsfortheuseofopen‐ended
questions:toascertainpopularandfolkideas,attitudes,valuesandbeliefs;toidentifythe
predominantfactorsofconcernandtoavoidthepossibilityofsuggestionintheanswers.
Thisapproachisconsideredanacceptablewayofobtaininginformationincross‐cultural
settings(Schlebuschetal.,1990).
4.2.1 HospitalGroup
Theinterviewerselectedevery10thnewpatientwaitingtobeseenbythemedicalofficer
atthemedicaloutpatientsdepartment.TableIIbelowshowshowthesamplewas
obtainedsothatitwouldberepresentativeofallthepatientsseenatthehospital.The
finalnumberperday,includedinthehospitalsample,wasbasedonanaveragetakenover
threeweeks.

62
TABLEII SAMPLESELECTIONFORHOSPITALGROUPWk Mon Tues WedThurs Fri Sat T1 310 300 269 242 240 64 14252 297 279 261 208 207 45 12973 280 271 206 214 173 22 1166T l887 850 736 664 620 131 3888Av 295.67 283.33 245.33 221.33206.6743.67 1296Sm 79.84 76.51 66.26 59.78 55.83 11.80 T=total;Av=averageandSm=sample
Interviewersintroducedthemselves,explainedtothepatientwhatthestudywasallabout
andrequestedtheirparticipation.Theyweretoldthattheirparticipationwasvoluntary
andthattheirrefusaltoparticipatewouldnotprejudicetheminanyway.Ifthepatient
decidedtoparticipate,theinterviewerassistedthepatientcompletetheHIB.
Aftercompletion,theinterviewerthankedthesubjectfortheircooperationandthetime
theyhadvolunteered.
4.2.2 CommunityGroup
Theinterviewersequippedwithasiteplanoftheareawiththeselecteddwellingsmarked,
visitedthepre‐determinedaddressesduringtheeveningsandonweekendsinorderto
ensurethatallthemembersofthefamilywereathome.Theyintroducedthemselves,

63
explainedthepurposeofthestudyandrequestedtheirparticipation.Whenpermissionto
conductthestudywasobtained,theinterviewerallocatedanumber(printedonadisc)to
eachmemberofthehousehold,eventhoseunavailableatthetime.Thediscswere
thrownintoapacketandonewasrandomlyselected.Theindividualrepresentedbythe
selecteddiscwasaskedtocompletetheHIBwiththehelpoftheinterviewer.(Ifthe
personselectedwasabsent,theinterviewerreturnedbyappointmenttocomplete
theHIB).
OncompletionoftheHIB,theinterviewerthankedthesubjectandothermembersofthe
familyfortheircooperationandthetimetheyhadvolunteered.
Theinterviewerswentthroughthelistofpre‐selectedhomesinexactlythesamemanner.
Ifpermissiontoconducttheinterviewwasrefusedoraparticularhomecouldnotbe
visited,theinterviewerselectedoneofthehomesfromthesparelistinstead.The
completedHIBwasreturnedtothewriterforanalysis.
4.3MATERIALS
TheHIBcomprisedofthefollowingquestionnairesandinventorieswhichwereusedto
elicitinformation:
1. HealthandIllnessQuestionnaire(HIQ)
2. HealthBeliefQuestionnaire(HBQ)
3. SocialSupportQuestionnaire(SSQ)
4. Hopkin'sSymptomChecklist(HSCL)‐(modified)
5. LifeExperienceSurvey(LES)‐(modified)
4.3.1 HealthandIllnessQuestionnaire(HIQ)

64
Thisquestionnairewasdesignedbythewritertoelicitinter aliainformationonhealthand
illness(seeAppendixA,pp1‐6).Thequestionnaireisdividedintoseveralsub‐sections.
Section1.1‐7(p.1)wasusedtocollectbiographicalinformationsuchasage,sex,ethnic
group,educationallevel,district,thenumberofyearsofresidenceinanurbanareaand
natureofemploymentorworkingskills.
Section2.1‐5(p.1)wascompletedbythehospitalgrouponly.Thissectionassessedfactors
suchascostoftransport,timetakentotraveltothehospital,availabilityofsickleaveby
patientswaspertinent,therefore,onlytothehospitalgroup.
Section3.1‐8(p.2)wascompletedbythehospitalgrouponlybecauseitelicited
informationthatdealtwithfactorsassociatedwithhospitalattendance.Thesewere
factorsthatprecipitatedthepatientsattendanceatthehospital,theperson's
understandingoftheseprecipitatingfactors,thechoiceofhospitalandthenatureofthe
disclosuretoothersabouthisorherillness.
Section4.1‐3(p.3)wascompletedbythecommunitygrouponlybecausethesequestions
assessedthechoiceofservicesinthecommunity.
Section5.1‐5(pp.3‐4)lookedattheuseofmedicalandsupplementaryservicesand
medication,andwascompletedbyallthegroups.
Section6.1‐5(pp.4‐5)elicitedinformationonreligiousandculturalbeliefs.Theseincluded
religiousaffiliations;consultationwithtraditionalhealers,faithhealersandherbalists;
costofservicesprovidedbytraditionalhealersandtheuseofprayer.Allgroups
completedthissub‐sectionofthequestionnaire.
Section7.1‐5(pp.5‐6)assessedhealthandillnessbeliefs.Subjectswererequiredtoexplain
whattheyfeltconceptssuchas'ill','sick','well'meant.Theywererequiredtolistwhat
65
theythoughtmadepeoplesick,whathealthactionsweretakenand/orwhathelp
seekingoccurred.
4.3.2 HealthBeliefQuestionnaire(HBQ)
Thisisa31itemquestionnaire(seeAppendixA,p.7)designedforthepurposesofthis
studytoascertainhealthandillnessbeliefs.Asdiscussedalreadyinthepreviouschapters,
thehealthandillnessbeliefsarenotonlystronglycolouredbythetraditionalworld‐view
butthattheAfricanviewofillnessisuniqueinmanyrespects.Further,thegroupsbeing
assessedareacculturatingandareadoptingwesternbeliefsaswell.Noneoftheexisting
scalesonhealthandillnessbeliefswerefoundtobesuitablebecausetheyeitherdidnot
takeintoaccounttheAfricanconceptofhealthandillnessorwerestandardisedfor
westernpopulations.Inaddition,theydidnotassessthesevariablesatalevelsuitablefor
thepurposeofthisstudy.Further,somescaleswereeithertoogeneralforourpurposeor
werespecificallyconstructedtomeasurementalhealth.Theseincludescalessuchas,the
HealthLocusofControlScale(Wallston,Wallstonetal.,1976)ortheMultidimensional
HealthLocusofControlScale(WallstonandWallston,1981)andRotter'sInternal‐
ExternalLocusofControlScale(Rotter,1966).
Thecomplexsystemofhealthandillnessbeliefsofthiscommunity,therefore,
necessitatedthedevelopmentofanappropriatequestionnaire.Thequestionnairehadto
haveitemsthatwererelevantforthiscultureandhadtobebroadenoughtomeasurea
varietyofhealthbeliefstotakeintoaccounttheacculturationprocessatworkinthis
community.
TheHBQrequirestherespondentstorateonafourpointLikertscalewhethertheyagree,
sometimesagree,disagreeorwere‘notsure’aboutthestatementpresented.

66
4.3.2.1ConstructionofQuestionnaire
BasedonareviewofliteratureonAfricanbeliefs,thesuggestionsofsixmentalhealth
professionalsworkinginacross‐culturalsettingandwhodealprimarilywithAfrican
patientsandthepersonalexperienceofthewriter,38itemswereselected.Thefaceand
contentvalidityofthequestionnairewasestablishedbyaskingapanelofexpertsinthe
areaofcross‐culturalissuestochecktheitems.Thepanelofexpertsweremadeupof
threeclinicalpsychologistsandtwopsychiatristswhomaderecommendationstoimprove
theselectionofquestionsandthesesuggestionswereincorporatedinthescale.
4.3.3 SocialSupportQuestionnaire(SSQ)
AsocialsupportmeasurewasincludedintheHIBbecauseoftheviewthatsocialsupport
actsasabufferagainstdiseaseandare,therefore,necessaryfortheindividualtocope
withlifechangesandadverseevents.TheSSQisa15itemquestionnaire(seeAppendixA,
p.8)designedbythewritertomeasureprimarilythequalitativeandquantitativeaspects
ofaperson’snetworkofrelationshipsthathelphimorherinadversecircumstances.A
reviewofseveralsocialsupportquestionnairesshowedthattheywereinappropriateasa
measurementinthecontextofAfricanculture,apointmadealsobyMcFarlaneauthorof
‘TheSocialRelationshipScale’(personalcommunication,10September,1990).The
variationinthestandardsofsocialadjustmentfromoneculturetoanotherisregardedas
amajorprobleminthemeasurementofsocialsupport(Weissman,1975).
ThesocialnetworkamongblackSouthAfricansisuniqueinmanywaysastheusualsocial
supportsarenotavailable.Africanfamilyunitshavesteadilybeenbrokenup.Maforah
(1988)pointsoutthatthedisintegrationoftheAfricanfamilyhasbeeninfluencedinter
aliabyEuropeancontactwithAfricawhichdisruptedfamilylife;neweconomicsystems;
politicalexploitationbroughtaboutbyforcedlabour,racialsegregationandalienation
fromtheland.Inourpresentcontext,fathersandmothersaswellareforcedtoliveaway

67
fromtheirfamiliesinordertofindworkorfurthertheirstudies.Lawsgoverningblackre‐
settlement(e.g.theNativeLandActsof1913and1936,thehomelandspolicyandthe
GroupAreasAct)haveallcontributedtotheerosionofblackfamilies.Theireffectslast
longaftertheyhavebeenremovedfromthestatutebooks.
IndevelopingthisquestionnaireIwasguidedmainlybytheSarason'setal.(1985)Social
SupportQuestionnaire,McFarlaneetal.(1981)SocialRelationshipScaleandThe
MultidimensionalScaleofPerceivedSocialSupport(Zimetetal.,1988).
Eachquestionhasatwopartresponse.Firstly,therespondentsarerequiredtolistthe
peopleintheirenvironmentwhoprovidethesupportsuggestedbythequestion.
Secondly,theyarerequestedtoratetheirlevelofsatisfactionwiththesupporteitheras
verysatisfied,satisfied,dissatisfiedorverydissatisfied,ona4pointLikertscale.The
questionnairealsoallowstherespondenttoratetheaccessibilityofsupport,theproximity
ofthesupportandthemodeofsupport.
4.3.3.1ConstructionofQuestionnaire
Afterselectingtheitemsforthequestionnaire,theyweregiventothreepsychiatristsand
twoclinicalpsychologistswhohadworkedwithAfricanpatientsforover10years,fortheir
opinions.Therewasgeneralagreementamongthemthatthequestionnaireshouldalso
assesswhetherthereissomeoneavailableatalltimeswhowouldprovidehelp,whether
thesepersonswereavailableimmediatelyorlivedadistanceaway,themodethrough
whichsocialsupportisobtained(whetherinperson,bytelephoneorthroughthepost)
andtheassessmentofnon‐familysupport(forexample,neighbours,priestsand
communityleaders).Othersuggestionsincludedincreasingthenumberofitemssothat
itemswouldbemorespecificandthere‐phrasingofsomeitems.Theserecommendations
wereassessedandseveralincludedinthequestionnaire.

68
4.3.4 SymptomInventory(SI)
Anessentialstepintheprocessofseekinghelpforone'sillnessistheinterpretationthat
thesufferergivesofthesymptomsheorsheexperiences(Bishop,1984;Mechanic,1978;
Pennebaker,1982).Mostoftensymptomsareignoredorgountreatedandsometimes
evenserioussymptomsareignored(Bishop,1984).AccordingtoBishopandConverse
(1986),itisessentialtotakeintoconsiderationthewaysinwhichlaypersons
conceptualizephysicalsymptomsanddiseasesincethisprocessplaysacriticalrolein
determiningaperson'shealthbehaviour.Forexample,Matthewsetal.(1983)showed
thattheinterpretationgiventosymptomsofmyocardialinfarctioninfluencestheurgency
ofmedicalhelp‐seekingaswellasillnessbehaviourandsickrolebehaviour.
Itwas,therefore,alsonecessarytoassesstheperceptionsandinterpretationofthe
commonsymptomsinthisstudyaswell.TheSIusedinthisstudyisamodifiedversionof
theHopkin'sSymptomChecklist(1974).Thewriterusedtheoriginal58itemsandadded
25additionalitemstomakethescaleappropriateforthepurposeofthisstudy.The
additionalitemswereobtainedthroughaprocessofinterviewswithseveralmedical
doctorsfromboththemedicaldepartmentsandpsychiatricdepartmentsattheKing
EdwardVIIIHospital.Thoseconsideredascommonsymptomswereincludedasthe
additionalitems.
Thesubjectshadtoindicatedwhethertheyhadexperiencedthesymptomandthereafter
rateitsseverityonafourpointLikertscalerangingfromveryserioustonotserious.A
categoryofnotsurewasalsoincluded.
Itwasenvisagedthatthepresentstudycouldalsobeusedtodevelopastandardised
symptominventoryscaleforSouthAfricanconditions.SeeAppendixA.
4.3.5 LifeExperienceSurvey(LES)

69
Twowidelyusedinstrumentsusedforassessinglifechangesandexperiencesarethe
ScheduleofRecentExperiences(HolmesandRahe,1967,andtheLifeExperienceSurvey
(Sarasonetal.,1978).AmodifiedversionoftheLifeExperienceSurveywasusedinthis
study.Thewriterusedtheoriginalscaleinordertodevelopaninstrumentspecifically
usefulfortheSouthAfricancontext.AsinthecaseoftheSItheoriginalitemsoftheLife
ExperienceSurveywasexpanded,inthisinstancebythreeadditionalitems.Theitems
thatwereincludedreferredtotherecentexperiencesofviolenceandtheresultanteffects
inthepopulationunderstudy.Theothermodificationstothisquestionnaireincluded
changingmonetaryvaluesfromU.S.dollarstoSouthAfricanequivalents.
4.4TRANSLATIONOFQUESTIONNAIRES
AllquestionnairesweretranslatedintoZulu,thespokenlanguageofthepeople
participatinginthestudy.TheEnglishversionofthequestionnairewasgivenfor
translationtotwoqualifiedandexperiencedhealthworkers(aclinicalpsychologistanda
psychiatrist),whohavebeenworkingwithAfricanpatientsandwhowerefluentinboth
ZuluandEnglish.
Thetranslatedquestionnairewasthengiventoanindependenthealthworker(a
psychiatrist,whowasfluentinbothEnglishandZulu)totranslatebackintoEnglish.
Whereverdiscrepancieswerefound,theywerecorrected.Thismethodofbacktranslation
isanacceptedmethodandisknowntoproducetranslationsofagoodquality.(Brislin,
1980).Inaddition,thetranslationandconstructionofallquestionnairesweredonein
accordancewiththeguidelinesandrulessuggestedbyRetief(1988)onthewritingand
modifyingofitemsforcross‐culturaluse.
ItshouldbeborneinmindthatthereismuchvariationintheZuluthatisspokeninthe
ruralareascomparedtothatspokeninthetownshipsandcities.Theaimwastoachievea
levelsuitablefortheurbangroupbeingstudiedandtoalsomakeitunderstandableata
muchbroaderlevel.
70
4.5PILOTSTUDY
TenvolunteerssimiliartothoserequiredinthesamplewereaskedtocompletetheHIB.At
thisstagethetrainedinterviewerswerequalifiedpsychiatricnursingsisters.Theywere
chosenbecauseoftheirexperienceinsocialscienceresearch.Thepurposeofthisphase
wastoascertainproblemsintervieweesmayexperienceincompletingthequestionnaires,
toidentifyanyitemsthatwereperhapsambiguousandtolocateotherdifficultiesthat
mayaffectthestudy.
Thisexerciseprovedtobeveryuseful.Firstly,severalambiguousitemsemergedandwere
corrected.Secondly,sometranslationerrorswereidentified.Anexampleofsuchanerror
isthesymptom“runnynose”whichwastranslated“anosethatliterallyran”.These
translationerrorswerecorrected.Thirdly,itwasfoundthatemotional,psychological
and/orpsychiatricitemswerebeingendorsedbyrespondents.Thereasonforthiswasthe
influenceofthetrainedpsychiatricnursingsisters.Itwasdecidedhereaftertousenursing
sistersnottrainedinpsychiatryandnon‐medicalpersonnel.
Thispre‐testprocedurealsohelpedtoassessthequalityofthetranslation,amethod
suggestedbyBrislin(1980),whostatedthattheefficacyofthismethoddependsonthe
controlexercisedduringthetestingandtheextenttowhichthefeedbackisincorporated
inthefinalrevisionsofthetest.Bothoftheserequirements,thatisthestrictcontroland
theintegrationoffeedback,werestrictlyadheredto.

71
CHAPTER5
RESULTS
Theresultsoftheinterviewsandthefindingsofthequestionnairesarepresentedinfive
mainsections.Theanalysisofthedatafromquestionnaireoneispresentedfirst,followed
bytheanalysisoftheHealthBehaviourQuestionnaire,theSocialSupportQuestionnaire,
theSymptominventoryandtheLifeExperienceSurvey,inthatorder.
5.1DEMOGRAPHICDATA
TheageofthesubjectsintheHospitalGrouprangedfrom20to99years(Mn=33.23
years).TheageofthesubjectsintheUmlaziGrouprangedfrom20to74years
(Mn=34,88years)andtheKwaMashuGrouphadarangeof20to58years(Mn=33,41
years).Themeanageforthethreegroupscombinedwas33.84.
TableIIIbelowgivesabreakdownoftheagesforeachgroup.Mostofthecombined
sample(90,71%)wereinthe20to49yeargroup.Fortythreepercentofthesamplewere
intheagegroup20to29,26%inthe30‐39yearagegroupand21%inthe40to49year
agegroup.Therewasnosignificantdifferencebetweenthemeanageforeachgroup.
Figure6representstheagedistributiongraphically.

72
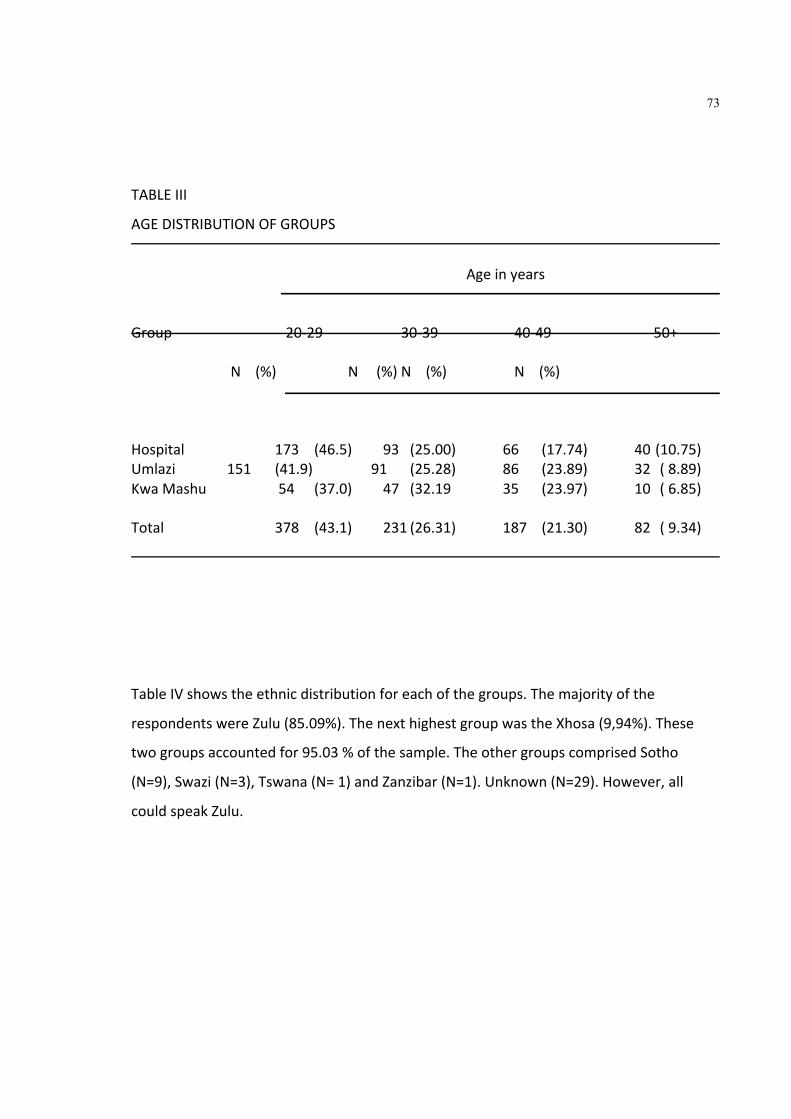
73
TABLEIII
AGEDISTRIBUTIONOFGROUPS
AgeinyearsGroup 20‐29 30‐39 40‐49 50+ N(%) N(%)N(%) N(%)Hospital 173 (46.5) 93 (25.00) 66 (17.74) 40(10.75)Umlazi 151 (41.9) 91 (25.28) 86 (23.89) 32 (8.89)KwaMashu 54 (37.0) 47 (32.19 35 (23.97) 10 (6.85)Total 378 (43.1) 231(26.31) 187 (21.30) 82 (9.34)
TableIVshowstheethnicdistributionforeachofthegroups.Themajorityofthe
respondentswereZulu(85.09%).ThenexthighestgroupwastheXhosa(9,94%).These
twogroupsaccountedfor95.03%ofthesample.TheothergroupscomprisedSotho
(N=9),Swazi(N=3),Tswana(N=1)andZanzibar(N=1).Unknown(N=29).However,all
couldspeakZulu.

74
TABLEIV ETHNICDISTRIBUTION Group Zulu Xhosa Other
N (%) N (%) N (%) Hospital 321 (85.83)38 (10.16)15 (4.01) Umlazi 295 (86.01)35 (10.20)13 (3.79) KwaMashu 120 (81.08)13 (8.78) 15 (10.14) Total 736 (85.09)86 (9.94) 43 (4.97)
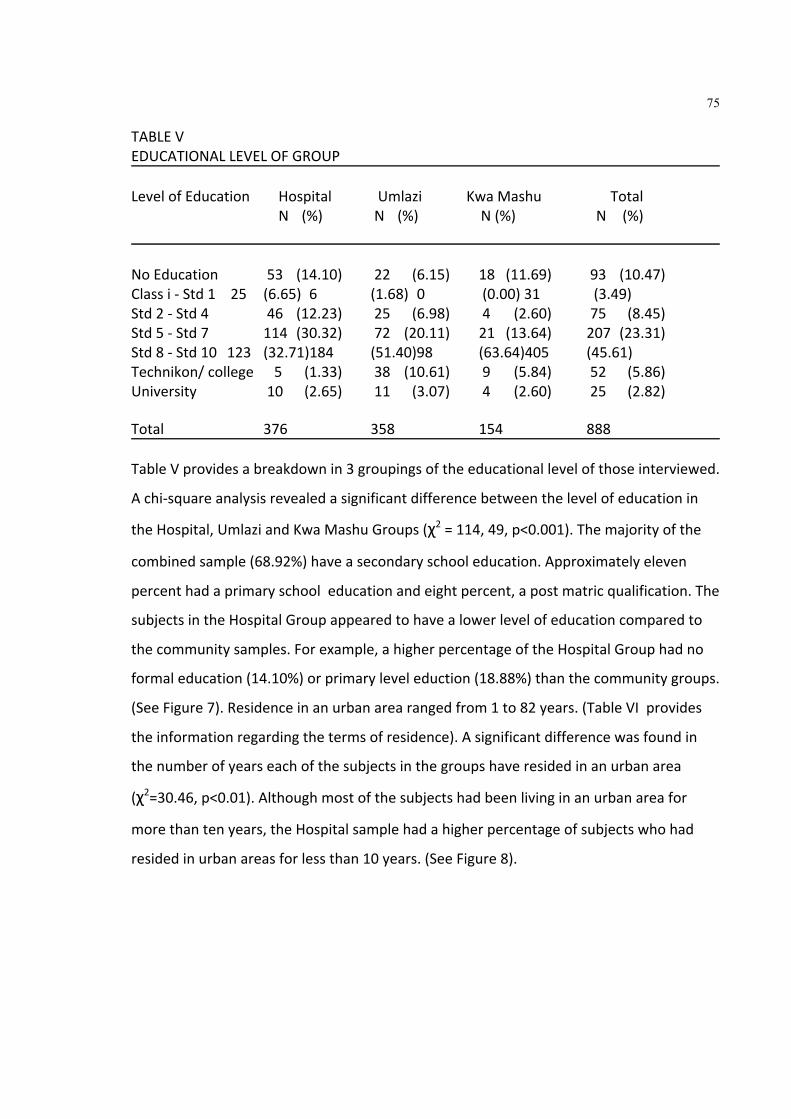
75
TABLEV EDUCATIONALLEVELOFGROUP LevelofEducation Hospital Umlazi KwaMashu Total
N (%) N (%) N(%) N (%) NoEducation 53 (14.10) 22 (6.15) 18 (11.69) 93 (10.47) Classi‐Std1 25 (6.65)6 (1.68)0 (0.00)31 (3.49) Std2‐Std4 46 (12.23) 25 (6.98) 4 (2.60) 75 (8.45) Std5‐Std7 114 (30.32) 72 (20.11) 21 (13.64) 207 (23.31) Std8‐Std10 123 (32.71)184 (51.40)98 (63.64)405 (45.61) Technikon/college 5 (1.33) 38 (10.61) 9 (5.84) 52 (5.86) University 10 (2.65) 11 (3.07) 4 (2.60) 25 (2.82) Total 376 358 154 888 TableVprovidesabreakdownin3groupingsoftheeducationallevelofthoseinterviewed.
Achi‐squareanalysisrevealedasignificantdifferencebetweenthelevelofeducationin
theHospital,UmlaziandKwaMashuGroups(χ2=114,49,p<0.001).Themajorityofthe
combinedsample(68.92%)haveasecondaryschooleducation.Approximatelyeleven
percenthadaprimaryschooleducationandeightpercent,apostmatricqualification.The
subjectsintheHospitalGroupappearedtohavealowerlevelofeducationcomparedto
thecommunitysamples.Forexample,ahigherpercentageoftheHospitalGrouphadno
formaleducation(14.10%)orprimaryleveleduction(18.88%)thanthecommunitygroups.
(SeeFigure7).Residenceinanurbanarearangedfrom1to82years.(TableVIprovides
theinformationregardingthetermsofresidence).Asignificantdifferencewasfoundin
thenumberofyearseachofthesubjectsinthegroupshaveresidedinanurbanarea
(χ2=30.46,p<0.01).Althoughmostofthesubjectshadbeenlivinginanurbanareafor
morethantenyears,theHospitalsamplehadahigherpercentageofsubjectswhohad
residedinurbanareasforlessthan10years.(SeeFigure8).

76
TABLEVI
YEARDISTRIBUTIONOFURBANLIVING
No.ofYearsGroups <5 5‐10 >10 TotalHospital 93(24.73) 34(9.04) 249(66.22) 376Umlazi 39(10.77) 23(6.35) 300(82.87) 154KwaMashu 23(14.95) 10(6.49) 121(78.57) 362Total 155(17.38) 67(7.51) 870(75.11) 892

77

78

79
ThesubjectsintheHospitalGroup(N=376)werereferredtothehospitalfromdistricts
throughoutNatalandevenbeyonditsborders.TableVIIliststhesubjects'residential
areas.Thehospital,however,ismostfrequentedbypatientsinandaroundtheDurban
area.Thesouthandnorthareaswhichhasthehighestrepresentation(71.27%),naturally
includedtheUmlaziandKwaMashutownships.Ofthe38.56%ofpatientsintheDurban
(south)group,29.5%werefromUmlazi.Theremainingsubjectsfromthisgroup(9.06%)
residedintheIsipingo,Amanzimtoti,Malvern,ChatsworthandMerebankareas.Ofthe
northgroup32.71%ofthepatientsfromtheDurban(north)area,20.2%residedinKwa
Mashu.Theremaining12.51%ofthesouthgroupcamefromtheInanda,Verulam,
TongaatandareasuptotheTugelaRiver.Theresultssuggestthatthemaincatchment
areasforthishospitalextendsfromAmanzimtotiinthesouthtoPinetownand
surroundingareasinthewest,andtheTugelaRiverinthenorth.Thiscatchmentarea
accountsfor82.97%ofitspatients.
TABLEVII DESTINATIONSOFHOSPITALSUBJECTS
District N % Durban(south) 145 38.56 Durban(north) 123 32.71 Pinetownandsurroundingarea 36 9.04 NatalMidlandsPietermaritzburg
andsurrounding 14 3.72 CentralSouthUmzintoandsurrounding 12 3.19 SouthPortShepstoneandsurrounding 10 2.66 Durbancentralandsurrounding 10 2.66 NorthTugelaZululand 7 1.86 Transkei 5 1.33 NorthernNatal(Drakensbergarea) 3 0.80 Lesotho 1 0.27 Unknown 10 3.20

80
Achi‐squaredanalysisontheoccupationsofthesubjectsbetweenthethreegroups
showedsignificantdifferences(χ2=171.52,p<0.01).TableVIIIgroupstheoccupationsof
thesubjectsaccordingtothecodingofoccupationguide(SchlemmerandStopforth,
1979).Thisguidewasdevelopedtoencouragestandardisationofthecodingof
occupationsinSouthAfrica.Inaddition,thisguidewaschosenbecauseitwasdeveloped
withcarefulconsiderationofcodesforAfricans.Thesubjectsattendingthehospitalwere
foundtobelessskilledcomparedtothoseinthecommunitygroups(seeFigure9).
However,acomparisonofthecommunitygroupsshowthattheKwaMashuGrouphavea
higherpercentageofsemi‐skilledartisansandprofessionalsthantheUmlaziGroup.
TABLEVIII SUBJECTSOCCUPATIONS
Semi‐ MiddleProfess‐ Group Unskilled skilled Artisans White‐collar ional Hospital 272 (72.34) 27 (7.18) 25 (6.65) 2 (0.53) 35 (9.31) Umlazi155 (42.82)30 (8.29)44 (4.93)11 (3.04) 79 (21.82) KwaMashu 28 (18.18) 29(18.83) 34 (22.08) 5 (3.25) 49 (31.82) Total 455 (51.01) 86 (9.64) 103(11.55) 18 (2.02) 163(18.27)

81

82
5.2TIMEANDTRANSPORTCOSTSOFHOSPITALPATIENTS ThecostoftravelincurredbypatientsattendingthehospitalrangedfromR1.00toR52.00.dependingfromwheretheycame.TheaveragecostwasR6.27.Thisrefersonlytothecostoftraveltothehospitalandnotothercostssuchashospitalfeesandlunch. Somepatientslefthomeasearlyas2h00toattendthehospital.Allleftby8h00.Ontheaveragetheyarrivedatthehospital1hourandfortythreeminuteslater.Ofthosewhoattendedthehospital,160(42.60%)reportedthattheywereunemployed.Ofthoseemployed,179patients(47.60%)reportedthattheyhadtotakethedayofffromworkinordertoattendthehospital.Forty‐two(23.46%),whotookthedayoff,reportedthattheywouldnotgetpaidorcompensatedforlossofearnings. Theresultsshowthat298patients(79.26%)wereunaccompaniedtothehospital.Ofthe20.74%whowereaccompanied,21(26.92%)wereaccompaniedbytheirspouse;12(15.38%)bytheirchildren;5(6.41%)byfriends;5(6.40%)bytheirbrothers;3(3.85%)byauntsand3(3.85%)byneighbours.Inmostofthecasespatientswereaccompaniedbyfemalesratherthanmales.Apossiblereasonforthismaybethatthemenmorelikelywouldbeatwork. 5.3HELPSEEKINGBEHAVIOUROFHOSPITALPATIENTS Inordertounderstandthefactorsand/orattitudesthatinfluencedthepatientsmedicalhelpseekingbehaviour,severalopen‐endedquestionswereasked.Thequalitativedataobtainedfromthesequestions,arepresentedbelow.ThedatarepresentstheviewsoftheHospitalGroupsinceonlytheyhadtocompletethissection. Twohundredandtwenty‐onepatients(59%)chosetoattendKingEdwardVIIIHospitalbecausetheybelievedthatitprovidedthebestserviceforAfricanpatients.Thesepatientsfeltthattheservices,facilitiesandtreatmentatthehospitalwereverygood,thatthehospitalhadplentyofdoctorstoattendtotheirneedsandthatthehospitalwaswellknownandrecognizedforitsgoodtreatment. Forty‐six(12%)ofthepatientschosetocometothehospitalbecausetheywerereferredbytheirgeneralpractitioner;38(10.3%)wereeitherreferredortransferredfromanotherhospitalorclinic.Twenty‐six(7%)wereencouragedtoattendthehospitalbytheiremployersorfamilymembersbecausetheythoughtthatthehospitalprovidedthebesttreatment.
The term spouse is used inclusively of boyfriend or girlfriend, since couples live together and only regard their partner as a spouse when the lobola has been paid. Lobola refers to the payment of bride price or dowry, that the husband is required to pay the brides father.
83
Eightpatients(2.2%)attendedthehospitalbecausetheyfeltthatthecostoftreatmentwasmuchcheaperthanotherhospitals.Sevensubjects(1.9%)didnotrespondorgaveinappropriateanswers. 5.3.1 ChoiceofDaytoAttend Twohundredandninety‐sixofthe376patientsrespondedtothequestionthataddressedthechoiceofdaytoattendthehospital. Themajorityofpatients(N=149,50.34%)attendedonthedaytheyfeltthattheywereeithergettingworse,theirconditionwasdeterioratingorthattheirpainwasbecomingunbearable.Ineighty‐sixcases(29.05%)thedayofattendancewasdeterminedeitherbyanappointmentorbecausetheyfeltthatthehospitalwillnotbebusy.Twenty‐three(7.77%)hadtowaittogetpaidbecausetheydidnothavesufficientmoneytoattend. About21(7.1%)attendedonthedaytheirreferringdoctorhadarrangedanappointmentwiththehospital.Asmallnumber,8,(2.70)reportedthattheyweretoobusyatworkorschoolandhadnotimetoattendearlier.Sevenhadtowaitfortransport(2.4%);1patienthadtoarrangeforsomeonetolookafterherchildrenandanotherattendedontheadviseandinsistenceofafriend. 5.3.2 Patient'sFirstSuspicionsofIllnessandAttendance Themajorityofpatientsattendedthehospitalwithinamonthofsuspectingtheywereill.Onehundredandthirty‐five(35,9%)attendedwithinaweek,42(11,2%)within2weeks,20(5,3%)bythethirdweekand45(12,0%)bythefourthweek—acumulativepercentageof65,4%(N=246).Themeanattendanceoverayearperiodwas5,85weeks(SD.9,82).TableIXprovidesabreakdownoftheattendance.Figure10depictstheattendancegraphically.

84
TABLEIX ILLNESSPRECIPITATIONANDATTENDANCETOHOSPITAL
Week/s N %
≤1 135 35.9 ≤2 42 11.2 ≤3 20 5.3 ≤4 45 12.0 5‐8 34 9.0 9‐12 11 3.0 13‐16 6 1.7 17‐20 4 1.1 21‐24 5 1.4 25‐28 5 1.4 29‐32 7 1.9 49‐52 8 2.2 >1year 50 13.9

85

86
5.3.3 PatientsReasonsfornotAttendingEarlier
Onehundredandsixty‐twopatients(43,50%)didnotattendthehospitalearlierbecause
theyfeltthattheirillnesswasnotseriousenough,thatthesymptomsdidnotbotherthem
ortheydeniedanyillnessexisted.Thesepatientsfeltthattheywouldgetbetterwithout
anymedicalintervention.Seventy‐four(19,90%)wereseeingaprivatedoctororattending
anotherclinicorhospital.“Nomoney”wasgivenby55(14,80%)asareasonfornot
attendingearlier.Eight(2,20%)wenttoapharmacyforhelp.Seven(1,90%)ofthepatients
indicatedthiswastheearliestappointmenttheycouldget.Seven(1,90%)hadeitherno
transportornoonetobringthemtothehospital.Six(1,60%)describedthemselvesas
beingtooseriouslyilltoattend.Onereportedthattheillnessremittedforashortwhile,
whereasanotherpatientwentto“churchpeople”forhelp.Oneofthepatientsreported
thatshewastooafraidtocomeearlier.Eleven(3,00%)feltthattheyhadnotdelayed.(See
Figure11).
5.3.4 FeelingsorexperiencesthatsuggestedtothepatientsthattheywereIll
Twohundredandthirty‐eightpatients(63,3%)feltthattheyweresickbecausethey
experiencedonlyphysicalsymptoms.Sixty‐four(20,8%)felttheyweresickbecausethey
hadexperiencedonlypsychologicalsymptoms,suchas,forgetfulness,worry,or
depression,aswellaschangesinaffect,sleeppatterns,energylevelsanddecreased
appetite.Twohundredandforty‐three(79,2%)hadacombinationofphysicaland
psychologicalsymptoms.
Threehundredandtwenty‐sevenpatients(87,0%)wereworriedaboutthesymptomsthey
wereexperiencingasopposedto42(11,2%)whowerenotreallyconcernedalthoughthey
felttheyweresick.

87

88
Asmanyas148(46,2%)patientsdidnotknowwhatwaswrong.Theresponsesofthose
whofeltthattheydidknowwhatwaswrongwiththemwerevaried.Forty‐three(13,4%)
thoughttheyhadflu;40(12,5)feltthattheirillnesswasduetosomeformofinfection
becausetherewerevisiblesigns,suchas,soresorlacerations.Twenty‐six(8,1)thought
thattheyhadaterminalillnesssuchascancerorAIDSandthattheyweregoingtodie.
Otherexplanationsincluded,17(5,3%)whofeltthattherewassomethingwrongwith
theirblood,thattheirbladderwasdirtyorthattheyhadwaterintheirheads.Twelve
(3,7%)feltthattheirillnesswasduetowitchcraft,thecrossingofapathwheresomeritual
wasperformed,theinhalingofabadspiritorthattheywerepoisonedbysomeone.
Twelve(3,7%)feltthatitwassomeknownclinicalsyndrome,suchas,diabetes,asthmaor
highbloodpressure.11(3,4%)feltthattheirillnesswastheresultofnormal
developmentalprocesses,suchas,puberty,pregnancyandoldage.Nine(2,8%)attributed
theirillnesstoseasonalortemperaturechangesand2(0.6%)feltthatitwasduetoapast
surgicalprocedure.
5.3.5 IllnessDisclosure
Threehundredandtwenty‐two(86%)ofthehospitalpatientstalkedabouttheirillness
andconcernstootherspriortoattendingthehospitalwhileonly49(13,2%)didnot.Of
thosewhodidspeaktoothers,92(28,3%)hadspokentotheirmothers;76(23,4%)to
theirspousesorboy/girlfriends;30(9,2%)tofriends;21(6,5%)totheirchildren;20(6,2%)
totheiremployer;17(5,2)toasister;12(3,7%)toabrother;12(3,7%)toarelative;10
(3,1)totheirfather;7(2,2%)tobothparentsand5(1,5%)totheirgrandmother.Only8
(2,5%)hadspokentoadoctor.

89
5.4SERVICES
5.4.1 Choiceofdoctor,hospitalandpharmacybythecommunitygroups.
Thechoiceofadoctorbyindividualsinthecommunitysamplegroupsarereflectedin
TableX.Thesubjectswereaskedtoindicatethelocationofadoctortheywouldvisitif
theyhadtoandwhytheywouldchoosethatparticulardoctor.Itappearsfromthe
responsesthatthereisatendency,naturally,forpeopletouseservicesthatarethe
closesttothem(58.6%).
TABLEX LOCATIONOFDOCTOR Choice Umlazi KwaMashu Total
N(%) N(%) N(%) Withintownship 211 (63.7) 66 (42.9) 277 (58.6) Outsidetownship 106 (32.1) 54 (35.1) 160 (33.8) City 3 (0.9) 21 (14.8) 24 (5.1) StaffDoctor 5 (1.5) 1 (0.7) 6 (1.3) Anywhere 6 (1.8) 0 6 (1.3) Total 331 142 473
ThereasonsforchoosingaparticulardoctorarelistedinTableXI.Themainfactorsthat
seemtomotivatethechoiceofadoctoraretheproximityandqualityofservice.The
majoritychoseadoctorclosesttothem(34.9%)orbecausetheyperceivedthatthey
wouldgetgoodservice(28.6%).Only11.6%consideredcostinthechoiceofadoctor.

90
TABLEXI REASONSFORCHOOSINGADOCTOR Reason/s Umlazi KwaMashu Total
N(%)N(%) N(%) Nearest 140 (38.5) 43 (30.5) 183 (34.9) Goodservice 98 (25.6) 52 (36.9) 150 (28.6) Familydoctor 67 (17.5)9 (6.4)76 (14.5) Cheapest 42 (11.0) 19 (13.5) 61 (11.6) Nearesttowork 18 (4.7) 14 (9.9) 32 (6.1) Staffservices 13 (3.4) 4 (2.8) 17 (3.2) Medicalaid 5 (1.3) _ 5 (0.9) Total 383 141 524
ThechoiceofhospitalandthereasonsfortheirchoicearefoundinTableXIIandTableXIII
respectively.Hereagain,theproximityandqualityofserviceplayanimportantroleinthe
choiceofservices.KingEdwardVIIIHospitalisstillpreferredbybothcommunities
althoughPrinceMshiyeniMemorialHospital(whichisinUmlazi)isequallypopularinthe
Umlazicommunity.However,KwaMashudoesnothaveahospitalclosetothemwhich
accountsforthehighernumberofpatientsattendingKingEdwardVIIIHospitalfrom
there.Theseresultsalsoshowthatasmuchas12.8%useprivateservices.Thefactthat
44.9%feltthattheirchoiceofhospitalwasdeterminedaccordingtothequalityofservice
and33.8%becauseitwasnearesttothem,supportstheviewthatconvenienceand
qualityofservicearethemostimportantfactorsforuseoftheseservices.

91
TABLEXII CHOICEOFHOSPITAL Hospital Umlazi KwaMashu Total
N(%) N(%) N (%) KingEdwardVII 122 (35.3) 84 (58.4) 206 (40.7) PrinceMshiyeni 147 (42.5) 9 (6.3) 156 (30.8) Private(Indian,city) 18 (5.2) 17 (11.9) 35 (6.9) Clairwood 31 (8.9) 1 (0.6) 32 (6.3) McCords ‐ 16 (11.2) 16 (3.2) MedicalTowers 14 (4.0) 1 (0.6) 15 (3.1) Private(White,city) 9 (2.6) 5 (3.5) 14 (2.8) St.Mary's 1 (0.3) 4 (2.7) 5 (1.0) KingGeorgeV 3 (0.9) ‐ 3 (0.6) KwaDabekaDay . ‐ 3 (2.1) 3 (0.6) Addington ‐ 3 (2.1) 3 (0.6) Madedeni 1 (0.3) 1 (0.6) 2 (0.4) Total 350 156 506

92
TABLEXIII REASONSFORCHOOSINGAHOSPITAL Reason/s Umlazi KwaMashu Total
N(%) N(%)N(%) Goodservice 119 (34.0) 108(69.2) 227(44.9) Nearest 146 (41.8) 25 (16.1) 171(33.8) Nearesttowork 50 (14.3) 10 (6.4) 60 (11.9) Cheapest 19 (5.4) 8 (5.1) 27 (5.3) Referred 12 (3.4) 5 (3.2) 17 (3.4) MedicalAid 3 (0.8) ‐ 3 (0.6) Noreferralrequired 1 (0.3) ‐ 1 (0.2) Total 350 156 506

93
Thechoiceofapharmacy(TablesXIVandXV)isinkeepingwithchoicesofotherservices.
Thesetablesshowthatproximityandqualityofservicearethemostimportantfactors
relatedtochoiceofmedicalandhealthservices.
TABLEXIV CHOICEOFPHARMACY Location Umlazi KwaMashu Total
N(%) N(%)N(%) Localtownship 143 (49.7) 46 (35.1) 189 (44.7) City 93 (31.8) 45 (34.4) 138 (32.6) Outsidetownship 47 (16.1) 37 (28.2) 84 (19.9) Anywhere 7 (2.4) 3 (2.3) 10 (2.4) Total 292 131 423
TABLEXV REASONSFORCHOOSINGAPHARMACY Reason/s Umlazi KwaMashu Total
N(%) N(%)N(%) Nearest 100 (33.0) 54 (37.8) 154 (34.5) Goodservice 67 (22.1) 31 (21.6) 98 (22.0) Nearesttowork 67 (22.1) 23 (16.1) 90 (20.2) Cheapest 44 (14.5) 7 (4.9) 51 (11.4) Wellstocked 19 (6.3) 20 (14.0) 39 (8.7) Trustthem 3 (0.9) 7 (4.9) 10 (2.2) Referred 3 (0.9) 1 (0.6) 4 (0.9) Total 303 143 446
5.5SUBJECTSPERCEPTIONSOFTREATMENT

94
Themajorityinthesample(n=739,83,8%)whohadreceivedmedicalservicesfroma
privatedoctororahospitalreportedthattheywerepleasedwiththetreatment.χ2=93.18
(p<0,01)wasobtained.SeeTableXVIforeachofthegroupsresponses.Itappears,
however,thatthecommunitysamples,Umlazi(83.9%)andKwaMashu(84.7%)were
generallymorepleasedwithtreatmentatthehospitalthantheHospitalgroup(53.2%).
TABLEXVI SUBJECTSPERCEPTIONSOFTREATMENT Perception Hospital UmlaziKwaMashu Total
N(%)N(%) N(%) N(%) PleasedwithRx 152(53.2) 281(83.9) 111(84.7) 544(72.3) NotpleasedwithRx89 (31.1) 24 (7.2) 10 (7.6) 123(16.4) Notsure 45 (15.7) 30 (9.0) 10 (7.6) 85 (11.3) Total 286 335 131 752
Thetwofactorsthatpleasedpatientsmostabouttheirtreatmentwerethattheirillnesses
werecured(N=224,37.71%)andtheserviceandcarewereverygood(N=330,55.55%).
TableXVIIliststheaspectsthesubjectsweremostpleasedwithandTableXVIIIliststhose
aspectsoftreatmentthatrespondentswerenotpleasedabout.

95
TABLEXVII TREATMENTFACTORSSUBJECTSWEREPLEASEDABOUT Factors Hospital Umlazi KwaMashu Total
N(%) N(%) N(%) N(%) Goodservice
andcare 83 (48.0) 167 (54.4) 80 (70.2) 330 (55.5) Illnesscured 78 (45.1) 117 (38.1) 29 (25.4) 224 (37.7) Gaveinjection5 (2.9) 19 (6.2) 2 (1.8) 26 (4.4) Gavemedication 4 (2.3) 4 (1.3) 3 (2.6) 11 (1.9) Cost 2 (1.1) ‐ ‐ 2 (0.3) GaveRxnever
seenbefore 1 (0.6) ‐ ‐ 1 (0.2) Total 173 307 114 594
TABLEXVIII TREATMENTFACTORSSUBJECTSWERENOTPLEASEDABOUT Factors Hospital Umlazi KwaMashu Total
(N=146) (N=133) (N=54) (N=333) PoorDr‐Pt relationship 38 (26.0) 72 (54.1) 31 (57.4) 141 (30.3) Poorfacilities 21 (14.4) 67(50.4)34 (63.0)122 (26.2) Timedelays 17 (11.6) 52 (39.1) 17 (31.5) 86 (18.5) Illnessnotcured 67 (45.9) 15 (11.3) 2 (3.7) 84 (18.1) Cost 10 (6.8) 18 (13.5) 4 (7.4) 32 (6.9)
Asignificantnumberofthesubjects(N=702,92,2%)werewillingtoseekmedicalservices
inthefuture(χ2=2,359,p<0,01).Whereas24(3,1%)didnotwanttoand37(4,7%)felt
thattheywerenotsureiftheywouldseekmedicaltreatmentagain.

96
TableXIXshowsthatpatientsobtaintheirmedicationthroughconsultationswithmedical
doctors.Averysmallpercentageobtainedmedicationfrompharmaciesorfriends.Asto
whytheyweregivenmedicationpatientrespondedthus:352(46,8%)knewthattheyhad
totakemedicationbecauseoftheirillnessalthoughtheydidnotunderstandthenatureof
theillness;304(40,4%)tookmedicationhavingunderstoodquitewellthenatureoftheir
illness.Onlyasignificantfew(p<0,01)prescribedmedicationforthemselvesbecausethey
felttheyhadtheflu(5,1%)orbecausetheyhadpain(7,7%).
TABLEXIX SOURCESOFMEDICATION Source Hospital UmlaziKwaMashu Total
(N=296) (N=334) (N=130) Privatedoctor177 (59.8)207 (62.0)48 (36.9)432 (57.1) Clinic/hospital 77 (26.0) 104(31.1) 66 (50.8) 247(32.6) Pharmacy 24 (8.1) 16 (4.8) ‐ 40 (5.3) Staffdoctor 12 (4.1) 6 (1.8) 13 (10.0) 31 (4.1) Friends/ relatives 6 (2.0) 1 (0.3) ‐ 7 (0.9)
Thereweresignificantdifferencesinthewaythesubjectsrespondedtowhetherwestern
medicineswerebeneficialtothem.TableXXliststheresponses.Differencesoccurred
betweentheHospitalandthecommunitygroup.Westernmedicationswereperceivedby
thehospitalattendersasbeinglessbeneficial.TheHospitalGroup(20.00%)demonstrated
greaterdoubtabouttheefficacyofwesternmedicationthanbothcommunitygroups;
Umlazi(5.1%)andKwaMashu(5.4%)

97
TABLEXX SUBJECTSPERCEPTIONSOFWESTERNMEDICINES Perception Hospital Umlazi KwaMashu Total
N(%)N(%) N(%) N(%) Helpful 160 (51.6) 299 (89.5) 116 (89.9) 575 (74.4) Nothelpful 88 (28.4) 18 (5.4) 6 (4.7) 112 (14.5) Notsure 62 (20.0) 17 (5.1) 7 (5.4) 86 (11.1) Total 310 334 129 773
Withregardtotheuseofvitaminsupplements,466(53.1%)didnottakesupplements
whereas412(46.9%)respondentsreportedhavingusedthem.MoreoftheKwaMashu
Group(55.7%)usedvitaminsupplementsthantheUmlaziGroup(40.4%).(χ2=141.76,
p<0.05).Thereasonfortakingvitaminsupplementsalsosignificantlydifferedbetweenthe
groups(p<0.01).SeeTableXXI.
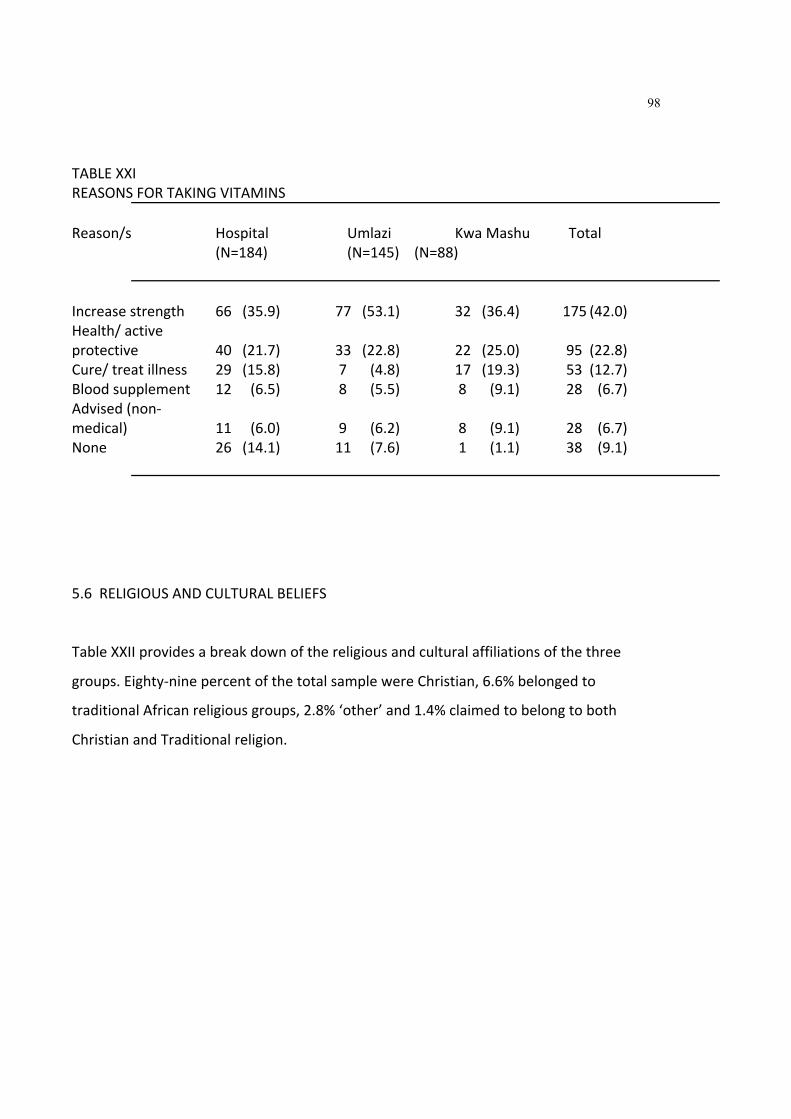
98
TABLEXXI REASONSFORTAKINGVITAMINS Reason/s Hospital Umlazi KwaMashu Total
(N=184) (N=145) (N=88) Increasestrength 66 (35.9) 77 (53.1) 32 (36.4) 175(42.0) Health/active protective 40 (21.7) 33 (22.8) 22 (25.0) 95 (22.8) Cure/treatillness 29 (15.8) 7 (4.8) 17 (19.3) 53 (12.7) Bloodsupplement 12 (6.5) 8 (5.5) 8 (9.1) 28 (6.7) Advised(non‐ medical) 11 (6.0) 9 (6.2) 8 (9.1) 28 (6.7) None 26 (14.1) 11 (7.6) 1 (1.1) 38 (9.1)
5.6RELIGIOUSANDCULTURALBELIEFS
TableXXIIprovidesabreakdownofthereligiousandculturalaffiliationsofthethree
groups.Eighty‐ninepercentofthetotalsamplewereChristian,6.6%belongedto
traditionalAfricanreligiousgroups,2.8%‘other’and1.4%claimedtobelongtoboth
ChristianandTraditionalreligion.

99
TABLEXXII RELIGIOUSANDCULTURALBELIEFS Beliefs Hospital Umlazi KwaMashu Total
(N=357) (N=343) (N=151) Christian 317(88.8) 321(93.6) 121(80.1) 759(89.2) Traditional 21 (5.9) 17 (5.0) 18(11.9) 56 (6.6) Other 10 (2.0) 2 (0.6) 12 (7.9) 24 (2.8) Christianand traditional 9 (2.5) 3 (0.9) ‐ 12 (1.4)
SubjectsresponsestoseekingtraditionalhealingfortheirillnessesarefoundinTableXXIII.
Helpfromtraditionalhealersweresoughtby14.5%;24,4%visitedfaithhealersand5.67%
soughthelpfrombothtraditionalandfaithhealers.Themajorityofthesubjectsreported
non‐useoftraditionalreligiousservices(55.4%).Thereappearstobeagreaterrejectionof
thesetraditionalservicesbyboththeHospitalGroup(57.4%)andtheUmlaziGroup
(58.7%).Ofthosethatusetraditionalservices,faithhealersarefrequentedmoreoften
thantraditionalhealers.

100
TABLEXXIII USEOFTRADITIONALHEALERS. Type Hospital UmlaziKwaMashu Total
(N=357) (N=339) (N=151) None 205(57.4) 199(58.7) 65 (43.1) 469(55.4) FaithHealer 93 (26.1) 76 (22.4) 38 (25.2) 207(24.4) Traditionalhealer 42 (11.8) 51 (15.1) 30 (19.9) 123(14.5) Traditionaland faithhealer 17 (4.8) 13 (3.8) 18 (12.0) 48 (5.67)
ThetreatmentsadministeredbythesehealersarelistedinTableXXIV.Thesubjects
reportedthatthetreatmentveryoftenwasacombinationofmethods.Holywater
(64.44%)andherbs(24.60%)aremostoftenused.Althoughtheyarefaithhealersprayer
isusedinonly13.63%ofthecaseswhoapproachedthesehealersforhelp.
TABLEXXIV TREATMENTGIVEN Treatment Hospital UmlaziKwaMashu Total
(N=148) (N=87)(N=139) Holywater 100(67.6) 63 (72.4) 51 (36.7) 241 (64.44) Herbs 26 (17.6) 47 (54.0) 19 (13.7) 92 (24.60) Trad.medicines 36 (24.3) 13 (14.9) 19 (13.7) 68 (18.18) Prayer 13 (8.8) 17 (19.5) 21 (15.1) 51 (13.63) Candles 3 (2.0) 11 (12.6) 5 (3.6) 19 (5.08

101
ThefrequencyofvisitstotraditionalhealersislistedinTableXXV.Subjectsgenerally
consultedtraditionalhealersforabout3timesandthereafterthereappearstobea
declineinattendance.Ofthosewhosoughttraditionalhealers,33.8%attendmorethan6
times.
TABLEXXV FREQUENCYOFVISITSTOTRADITIONALHEALERS Noofvisits Hospital Umlazi KwaMashu Total
(N=150) (N=139) (N=87) 1 38 (25.3) 18 (12.95) 7 (8.1) 63 (17.0) 2 39 (26.0) 37 (26.6) 22 (25.3) 98 (26.1) 3 24 (16.0) 19 (13.7) 14 (16.1) 57 (15.2) 4 1 (0.7) 3 (3.5) 1 (0.7) 10 (2.7) 5 5 (3.3) 13 (9.4) 3 (3.5) 21 (5.6) 6+ 43 (28.7) 33 (38.0) 51 (36.7) 127 (33.8)
Theaveragepaymentpertreatmenttothetraditionalhealersvariedforeachgroup:the
HospitalGroup(R84.62),theUmlaziGroup(R68.23)andTheKwaMashuGroup(R95.29).
Thereweresignificantdifferences(p<0.01)betweenthegroupsabouthowtheyfeltabout
theusefulnessorbenefitofthetraditionalorculturaltreatment.TableXXVIshowsthat
80.5%oftheKwaMashuGroupfeltthatthetraditionaltreatmentswerebeneficial
whereasonly40.4%oftheHospitalGroupand64.3%oftheUmlaziGroupfeltitwas
beneficial.However,theHospitalGroupindicatedgreaterdispleasurewithtraditional
treatments.

102
TABLEXXVI SUBJECTSPERCEPTIONSOFTHEEFFECTIVENESSOFTRADITIONALTREATMENT Perception Hospital UmlaziKwaMashu Total
(N=151) (N=140) (N=87) Rxhelped 70 (40.4) 90 (64.3) 70(80.5) 230 (60.9) Rxdidnothelp 40 (26.5) 13 (9.3) 7 (8.1) 60 (15.9) Notsure 41 (27.2) 37 (26.4) 10(11.5) 88 (23.3) Rx=treatment
ThedatainTableXXVIIsupportstheviewthatofthosewhousedtraditionaltreatment
methods,anoverall47.40%,willcontinuetraditionaltreatment.Ap<0,05significancewas
obtainedbetweenthegroups(χ2=35.65).AgreaternumberintheHospitalGroup
(58.55%)indicatedthattheywillcontinuetraditionaltreatmentthantheUmlaziGroup
(38.88%)andKwaMashuGroup(42.22%)
TABLEXXVII CONTINUATIONOFTRADITIONALTREATMENT
Hospital UmlaziKwaMashu Total (N=152) (N=144) (N=90)
Cont.trad.Rx89 (58.55) 56(38.88)38 (42.22)183 (47.40) Discont.tradRx 63 (41.5) 88 (61.1) 52 (57.8) 203(52.6) Rx=treatment
TableXXVIIIindicatestheuseofprayerbyindividualsasamethodof‘treatment’fortheir
illness.Prayerismostoftensoughtfromchurchpeople,suchas,ministers,
deaconsandwoman'sprayergroups,(50,0%).Othersourcesfromwhichprayerissought
arethefamily(25,4%)andfriendsorneighbours(16,4%).

103
TABLEXXVIII PRAYERASATREATMENTFORILLNESS
Hospital UmlaziKwaMashu Total N(%)N (%) N(%) N(%)
Pray 59 (16.1) 65 (18.8) 50 (35.5) 174(20.4) Donotpray 308(83.9) 281(81.2) 91 (64.5) 680(79.6) Total 367(43.0) 346(40.5) 141(16.5) 854
Twenty‐onepercentreportedconsultingaherbalistfortheirillness.SeeTableXXIX.There
issignificantlygreateruseofherbalistbythecommunitygroupsthantheHospitalGroup
(χ2=6.23,p<0.05).
TABLEXXIX CONSULTATIONOFHERBALISTS
Hospital UmlaziKwaMashu Total N(%)N(%) N(%) N(%)
Herbalistseen61 (16.5)77 (21.8)45 (30.4) 183 (21.0) Herbalistnotseen 309(83.5) 276(78.0) 103(70.0) 688(79.0) Total 370(42.4) 353(41.0) 148(17.0) 872 Severalfolkmedicineswerereportedtohavebeenused.Laxativesappeartobethemost
popularsubstanceconsumed.TableXXXprovidesabreakdownofthesubstanceseach
groupused.

104
TABLEXXX USEOFTRADITIONALOR“LAY”SUBSTANCES Substance Hospital Umlazi KwaMashu Total
N(%) N(%) N(%)N(%) Laxatives 316 (84.0) 328 (90.6) 138 (90.0) 782 (88.0) Ointments 135 (35.9) 145 (40.1) 63 (41.0) 343 (38.5) Vomitingmeds. 130 (35.0) 106 (29.3) 74 (48.1) 310 (35.0) Strengthening meds. 135 (36.0)118 (33.0)38 (25.0)291 (33.0) Holywater 124 (33.0) 105 (29.0) 47 (31.0) 276 (31.0) Herbs 78 (20.7) 69 (19.1) 53 (34.4) 200 (22.4) Hot/cold preparations 40 (10.6) 41 (11.3) 38 (25.0) 119 (13.3) OTHER....................................................................................................................................... Glucose 42 (11.1) 55 (15.2) 2 (1.3) 99 (11.1) Castoroil 42 (11.1) 35 (9.7) 6 (4.0) 83 (9.3) Warmwater 42 (11.1) 32 (8.8) 1 (0.6) 75 (8.4) Epsomsalts 16 (4.3) 19 (5.2) 1 (0.6) 36 (4.0)
5.7HEALTHANDILLNESSBELIEFS(QUALITATIVERESPONSES)
Thesubjectswereaskedtorespondtoseveralopen‐endedquestionabouthealthand
illnessbeliefs.Belowisasummaryoftheirresponses.
5.7.1 Whatiswrongwithyouandwhydoyouthinkso?
OnlytheHospitalGrouphadtorespondtothisquestionbecauseitwasmostappropriate
forthesesubjectssincetheywereseekingmedicalhelpatthehospital.Ofthosethat
answered43.40%(n=152)didnotknowwhatwaswrongwiththem.Themostcommon
explanationsfortheirsymptomswere:14.00%(n=51)understoodthesesymptomsasa

105
recognizedmedicaldisorder;11.80%(n=43)feltitwasduetoinfection;6.00%(n=22)felt
iswasaresultof‘somethingwrongwiththeblood(thatis,theirbloodwaseitherdirtyor
weak),thattheyhadtoomuchofgallinthebody,theirbodywasweakortheyhaddirty
organs';4.40%(n=16)feltthatitwasduetoinjury;4.10%(n=15)duetobewitchment,evil
orevilspiritpossession,crossingapathwherearitualwasperformedorasaresultofthe
ancestorsbeingangry;2.50%(n=9)oldage;2.20%(n=8)poornutrition,theusedirty
drinkingwaterorpoorlivingconditionsand1.70%(n=6)feltthatitwasduetotheirbrain
notfunctioningproperly.Otherlesscommonreasonswereseasonalchanges0.80%(n=3),
alcoholanddrugabuse1.10%(n=4),bodymalfunctioning1.10%(n=4),sideeffectsof
medication0.80%(n=3),anger0.80%(n=3)andtemperaturechange0.50%(n=2)
Thereasonstheygaveformakingtheabove'diagnoses'were:38.80%(n=132)gavea
reasonableexplanation;13.80%(n=47)becausetheyhadphysicalsymptomsand/or,they
werenotfunctioningastheyhadpreviously;2.10%(n=7)hadbeentoldsobyothers;
1.80%(n=6)becauseofcognitivechangesand/orvegetativeshifts;0.6%(n=2)cessationof
traditionbeliefsorbeliefinGodand0.30(n=1)environmentalchange.
5.7.2 Whatdoesitmeantobesick?
Therespondentsexperienceddifficultyrespondingtothisquestion.Mostrespondedto
thisquestionasfeeling"nauseous","tovomit"or"feelweak".Thereappearedtobeno
differenceintheconceptbetweensickandill.Theterm'ukugula'isusedmostoftenfor
beingorfeelingill.
5.7.3 Whatdoesitmeantobeill?
PatientsresponsestothisquestionarefoundinTableXXXIbelow.Generallyillnessmeant
notfeelingwellor'free'inthebody,soulandlife;notfeelinggoodornormal;being
worried,havingproblems,beinguncomfortableandunrelaxed;perceivingpain;and

106
experiencingphysicalandpsychologicalsymptoms.Theresponsesmadeshowthatthe
subjectsholdanholisticviewofillness.Biopsychosocialsymptomatologyisconsideredas
causeorreasonsforillness.
5.7.4 Whatdoesitmeantobewell?
Thesubjectsviewofhealthisinkeepingwiththeirviewofillness.Yetagainthesubjects
holdaholisticviewofhealth.Wellnessisassociatedwithfeeling'free'andgoodinbody,
soulandlifeingeneral;havingnoworries,problems,feelingcomfortableandrelaxed;no
perceptionofpainandnophysicalorpsychologicalsymptoms.Theirresponsesarefound
inTableXXXII.
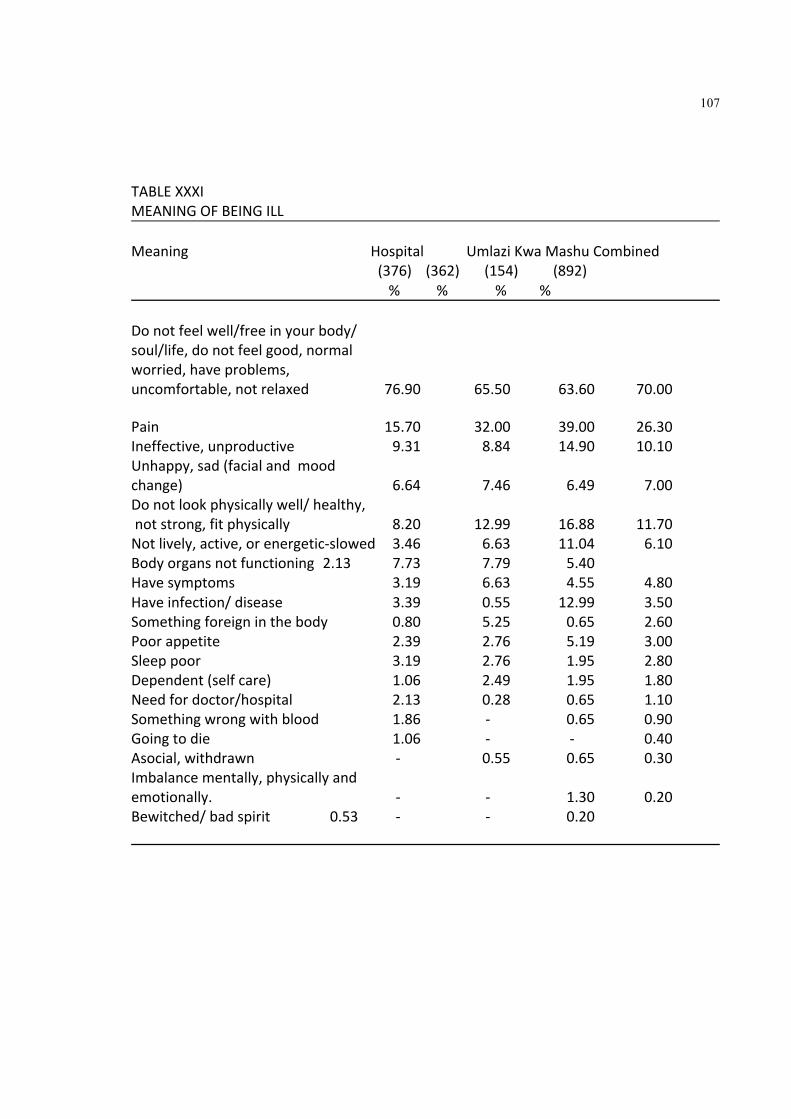
107
TABLEXXXI MEANINGOFBEINGILL Meaning Hospital UmlaziKwaMashuCombined
(376) (362) (154) (892) % % % %
Donotfeelwell/freeinyourbody/ soul/life,donotfeelgood,normal worried,haveproblems, uncomfortable,notrelaxed 76.90 65.50 63.60 70.00 Pain 15.70 32.00 39.00 26.30 Ineffective,unproductive 9.31 8.84 14.90 10.10 Unhappy,sad(facialandmood change) 6.64 7.46 6.49 7.00 Donotlookphysicallywell/healthy, notstrong,fitphysically 8.20 12.99 16.88 11.70 Notlively,active,orenergetic‐slowed 3.46 6.63 11.04 6.10 Bodyorgansnotfunctioning2.13 7.73 7.79 5.40 Havesymptoms 3.19 6.63 4.55 4.80 Haveinfection/disease 3.39 0.55 12.99 3.50 Somethingforeigninthebody 0.80 5.25 0.65 2.60 Poorappetite 2.39 2.76 5.19 3.00 Sleeppoor 3.19 2.76 1.95 2.80 Dependent(selfcare) 1.06 2.49 1.95 1.80 Needfordoctor/hospital 2.13 0.28 0.65 1.10 Somethingwrongwithblood 1.86 ‐ 0.65 0.90 Goingtodie 1.06 ‐ ‐ 0.40 Asocial,withdrawn ‐ 0.55 0.65 0.30 Imbalancementally,physicallyand emotionally. ‐ ‐ 1.30 0.20 Bewitched/badspirit 0.53 ‐ ‐ 0.20

108
TABLEXXXII MEANINGOFBEINGWELL Meaning Hospital UmlaziKwaMashu Combined
(376)(362) (154) (892) % % %%
Feelwellinyourbodyandsoul, feelinggood,normal,noworries, problems,freeinyoursoul,life, enjoyinglife/content 64.63 53.04 45.45 56.61 Healthy,goodweight,strong,fit, physical 32.45 48.07 57.14 43.05 Nopain 21.28 29.56 25.97 25.45 Happy,excited,joy 28.46 21.27 13.64 22.99 Lively,active,energetic 14.10 13.26 14.29 13.75 Effective,productive 9.04 8.01 18.18 10.20 Psychologicallyandmentallyfit 3.29 5.80 14.29 5.83 Bodyorgansfunctioning 1.60 4.97 6.49 3.81 Noinfection/disease 1.60 1.93 13.64 3.81 Goodappetite 2.39 3.31 1.30 2.58 Independent 4.26 0.28 2.60 2.35 Nosymptoms 0.79 2.21 3.90 1.91 Noneedfordoctor/hospital 2.13 0.28 1.95 1.35 Visitingothers 1.33 0.83 2.60 1.35 Bewitched/badspirit 0.27 ‐ ‐ 0.11
Thesubjects'responsestowhattheybelievedthattheindicatorsof'beingwell'and'being
ill'were,arefoundrespectivelyinTableXXXIIIandTableXXXIV.Physicalability,moodand
psychologicalwell‐beingareconsideredindicatorsofbeingwell.Poorvegetativefunction,
physicalability,moodaswellasphycologicalwell‐beingisconsideredindicatorsof'being
ill'.

109
TABLEXXXIII INDICATORSOFBEINGWELL Meaning Hospital UmlaziKwaMashuCombined
(376) (362) (154) (892) % % %%
Strong,fit,physical 28.19 38.95 38.31 34.30 Happy,excited,joy,singing,dancing, laughs,jokes,humour 27.39 24.59 43.51 29.04 Lively,active,energetic 30.59 10.54 24.03 27.58 Toworkproperly,workshard, effective,productive 16.76 25.41 31.17 22.76 Health,goodweight,notneglected 6.84 23.20 12.37 18.39 Good,normal,feelwellinyourbody, freeinyoursoul,life,enjoying life/content,comfortable 18.09 16.02 20.78 17.71 Goodappetite 15.96 16.22 13.64 15.92 Nopain 7.45 11.88 18.18 11.09 Facialexpression 9.84 12.99 1.95 9.75 Mobility 9.57 5.80 5.19 7.29 Playingwithothers,notvisitingothers 8.78 4.97 6.49 6.84 Quick,sharp,concentrate 4.52 7.46 7.79 6.39 Symptoms 3.46 7.18 13.64 6.73 Talksproperly,loud 5.05 5.52 8.44 5.83 Sleepwell 3.99 5.25 4.55 4.59 Psychologicallyandmentallyfit, talkappropriately 0.80 2.49 9.09 2.91 Changeofattitude,motivated 1.86 3.31 ‐ 2.13 Noneedfordoctor/hospital 2.39 0.55 0.65 1.34 Agitatednotrelaxed 0.53 0.28 ‐ 0.34
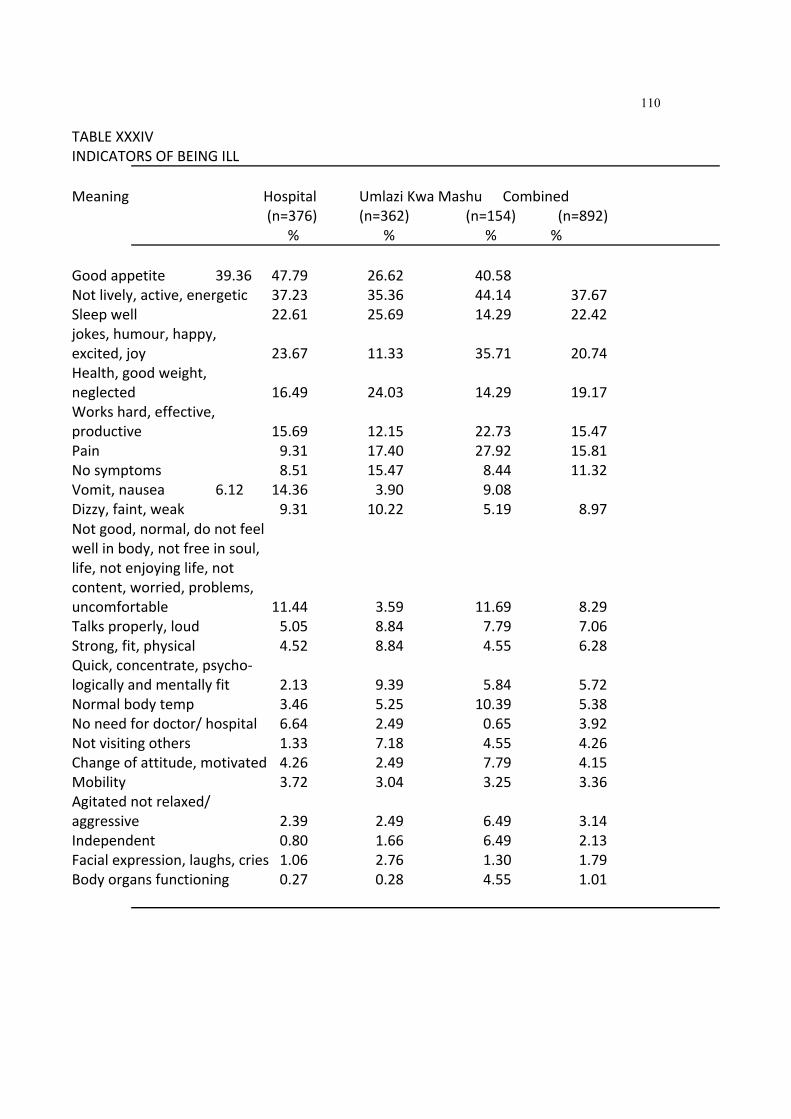
110
TABLEXXXIV INDICATORSOFBEINGILL Meaning Hospital UmlaziKwaMashu Combined
(n=376) (n=362) (n=154) (n=892) % % % %
Goodappetite 39.36 47.79 26.62 40.58 Notlively,active,energetic 37.23 35.36 44.14 37.67 Sleepwell 22.61 25.69 14.29 22.42 jokes,humour,happy, excited,joy 23.67 11.33 35.71 20.74 Health,goodweight, neglected 16.49 24.03 14.29 19.17 Workshard,effective, productive 15.69 12.15 22.73 15.47 Pain 9.31 17.40 27.92 15.81 Nosymptoms 8.51 15.47 8.44 11.32 Vomit,nausea 6.12 14.36 3.90 9.08 Dizzy,faint,weak 9.31 10.22 5.19 8.97 Notgood,normal,donotfeel wellinbody,notfreeinsoul, life,notenjoyinglife,not content,worried,problems, uncomfortable 11.44 3.59 11.69 8.29 Talksproperly,loud 5.05 8.84 7.79 7.06 Strong,fit,physical 4.52 8.84 4.55 6.28 Quick,concentrate,psycho‐ logicallyandmentallyfit 2.13 9.39 5.84 5.72 Normalbodytemp 3.46 5.25 10.39 5.38 Noneedfordoctor/hospital 6.64 2.49 0.65 3.92 Notvisitingothers 1.33 7.18 4.55 4.26 Changeofattitude,motivated 4.26 2.49 7.79 4.15 Mobility 3.72 3.04 3.25 3.36 Agitatednotrelaxed/ aggressive 2.39 2.49 6.49 3.14 Independent 0.80 1.66 6.49 2.13 Facialexpression,laughs,cries 1.06 2.76 1.30 1.79 Bodyorgansfunctioning 0.27 0.28 4.55 1.01

111
TABLEXXXV REASONSPEOPLEGETSICK/ILL
Reasons Hospital UmlaziKwaMashu Combined (n=376) (n=362) (n=154) (n=892) % % % %
Diet,poornutrition,junkfood 63.03 76.52 53.25 66.82 Coldwhilesleeping,noor poorshelter,dirty,squatter conditions,drinkingdirty water,pollution,poor environments 62.24 73.48 63.64 66.45 Disease/infection,germs 11.70 10.77 23.38 13.34 Noexercise 6.64 21.82 11.69 13.68 Psychologicalproblems, worry,badthoughts/moods, stress 9.57 10.77 25.97 12.89 Non‐complianttoDrsRx, notgoingforregularcheck ups,delaying/procrastinating attendancetodoctors 7.98 9.94 14.29 9.86 Largeconsumptionof alcohol 6.91 7.18 11.69 7.85 Beliefandfollowing traditionalRx. 10.90 2.47 10.39 7.50 Notkeepingyourselfhealthy5.057.18 3.90 5.72 Poverty 1.33 3.59 20.13 5.49 Overcrowding 2.663.87 15.58 5.38 Socialproblems 6.12 3.59 7.14 5.27 Smokeexcessively 1.33 6.63 5.19 4.15 Injuries,accidents, violence,war,unrest 3.46 3.59 1.95 3.25 Poorhealthfacilities/apartheid 1.60 3.04 5.19 2.80 Increasedresponsibility 2.66 3.31 0.65 2.58 Laziness 1.33 1.66 6.49 2.35 ForgetGod ‐ 1.38 3.25 2.32 Substanceabuse 1.06 3.87 1.30 2.24 Seasonorweatherchanges 1.06 3.31 2.60 2.24 Weak,notstrong 1.33 1.38 5.84 2.13 Overworking 1.06 0.83 3.25 1.34 Allergic,takingsomething notgoodforyourbody 0.53 2.76 0.65 1.64 Somethingforeignenters

112
theirbody ‐ 2.49 0.65 1.57 Pooreducation ‐ ‐ 1.30 1.30 Todie ‐ 1.10 ‐1.10 Lossofculture 1.060.28 1.95 1.10 Bewitchment ‐ 0.55 1.30 0.93 Bodymalfunctioning 0.53 0.55 2.60 0.90 Notrestingorrelaxing 0.27 1.38 1.30 0.90 Oldage 1.33 0.55 ‐ 0.78 Attackwithoutacause,natural 0.27 0.28 1.30 0.62 Promiscuity 1.06 0.28 ‐ 0.56 Inherited ‐ 0.28 0.65 0.47 Badtermswithneighbours/ family 0.79 0.28 0.65 0.45 Insufficientsleep 0.27 0.55 ‐ 0.34 Malingering ‐ 0.28 ‐ 0.28 Nosupport ‐ 0.28 ‐ 0.28 Don'tcleantheirstomachs 0.27 0.28 ‐ 0.22
TableXXXVliststheresponsesthesubjectsmadetothequestion,'whypeoplegetill?'
Poornutritionanddiet,poorlivingconditionsandpovertywerethemainreasonsgiven
forgettingill.Theotherpopularreasonswerediseasesandinfections,lackofexerciseand
psychologicalstressesandconflicts.Thereisalsoavarietyofotherreasonslisted.
5.8ILLNESSBEHAVIOUR
Thesubjectswereaskedwhattheywouldnormallydowhentheyfelttheywereill.Their
responsesappearinTableXXXVI.Significantdifferences(chi‐squared)werefoundinthe
waythegroupsrespondedtohelp‐seekingbehaviourfromahospital,pharmacy,
traditionalhealer,useofprayer,selfmedicationordenial.Themajorityofpatients
indicatedthattheywouldseeadoctor(81.5%).TheKwaMashuGroupdiffered
significantlyintheiruseofthehospitalandpharmacy,selfmedicatinganddenialoftheir
illness.TheHospitalGroupusedprayermoreoftenthanthecommunityGroups.

113
TABLEXXXVI ILLNESSBEHAVIOUROFSUBJECTS
Behaviour Hospital UmlaziKwaMashu Total n% n% n% n%
Gotoadoctor 295 (78.5) 301 (83.1) 131 (85.1) 727 (81.5) Gotoahospital 275 (73.1) 282 (77.9) 103 (66.9) 660 (74.0)** Gotoapharmacy 145 (38.6) 153 (42.3) 86 (55.8) 384 (43.1)* Pray 171 (45.5) 132 (36.5) 62 (40.3) 365 (41.0)** Askothersforhelp 137 (36.4) 137 (37.8) 70 (45.5) 344 (38.6) Ignoreit 129 (34.3) 104 (28.7) 83 (53.9) 316 (35.4)* Medicateyourself 101 (26.9) 92 (25.4) 99 (64.3) 292 (32.7)* Gotosomeonefor
prayer 63 (16.8) 76 (21.0) 30 (19.5) 169 (19.0) Readaboutit 31 (8.2)68 (18.8)17 (11.0)116 (13.0)* Gotoatraditional
healer 48 (12.8) 40 (11.0) 9 (5.8) 97 (10.9)
* p<0.01
** p<0.05
5.9HEALTHANDILLNESSBELIEFS
Cronbach'scoefficientalphatestwasdonetoestablishthereliabilityoftheHBQ.A
reliabilityof0.76wasobtained.Acomparisonofthegroupsoneachitemispresented
belowinTableXXXVII.
TABLEXXXVII COMPARISONSOFGROUPSRESPONSESONHBQITEMS(IN%)
HospitalUmlaziKwaMashuTotal (N=376)(N=362)(N=154)(N=892)

114
1. Peoplegetsickbecausethey
arenotstrong.
Agree 48.4 37.9 21.4 39.46* Sometimesagree 22.1 29.8 26.6 26.01 Disagree 22.6 28.4 37.7 27.58 Notsure 7.0 3.8 14.3 6.95
2. Peoplegetsickbecausethey
donoteattheproperfoods.
Agree 57.2 47.5 48.7 51.85 Sometimesagree 33.8 43.4 37.0 38.27 Disagree 6.4 6.6 11.0 7.30 Notsure 2.7 2.5 2.6 2.58
3. Illnessisduetodesertion
byGod.
Agree 11.2 11.9 3.2 10.10* Sometimesagree 21.0 26.2 12.3 21.66 Disagree 52.7 49.2 71.4 54.55 Notsure 15.2 12.4 13.0 13.69
4. Illnessiscausedbyinfection.
Agree 60.9 52.8 66.9 58.83** Sometimesagree 27.4 32.6 24.7 29.13 Disagree 8.5 6.9 2.6 6.86 Notsure 3.2 6.9 5.8 5.17
5. Illnessiscausedbywitchcraft
orsorcery.
Agree 22.9 20.4 11.0 20.02** Sometimesagree 30.3 22.9 33.1 28.05 Disagree 26.9 35.4 33.8 31.79 Notsure 20.0 19.9 20.8 20.14
6. Peoplegetsickbecausesomeone

115
hascursedordonesomething eviltowardsthem.
Agree 16.8 11.0 11.0 13.48 Sometimesagree 19.9 26.0 24.7 23.26 Disagree 38.3 39.8 40.9 39.44 Notsure 25.0 22.9 22.7 23.82
7. Peoplegetsickbecausethey
donotexerciseregularly.
Agree 36.2 36.5 32.5 35.69 Sometimesagree 34.3 35.9 46.1 37.04 Disagree 15.4 10.8 11.0 12.79 Notsure 14.1 16.6 10.4 14.48
8. Sickness'comes'fromthedevil.
Agree 13.6 11.3 13.6 12.70 Sometimesagree 15.7 13.0 9.1 13.48 Disagree 45.2 50.3 50.0 48.20 Notsure 25.5 25.1 26.6 25.62
9. Peoplegotodoctorsonlywhen
theyareseriouslyill.
Agree 42.3 35.1 38.3 38.76* Sometimesagree 27.9 27.9 42.9 30.56 Disagree 14.9 14.1 13.6 14.38 Notsure 14.6 22.7 5.2 16.29

116
10. Doctorsaretheonlyonesthat cantreatpeoplewhoareill.
Agree 20.2 9.1 13.0 14.53* Sometimesagree 22.3 19.9 9.7 19.26 Disagree 40.2 45.6 68.8 47.52 Notsure 17.3 24.6 7.8 18.69
11. Thereisnothingapersoncan
dotopreventthemselvesfrom gettingill.
Agree 19.9 12.7 18.2 16.74* Sometimesagree 25.0 23.5 10.4 21.91 Disagree 40.4 41.2 59.7 44.16 Notsure 14.6 22.1 11.7 17.19
12. Peoplegetsickbecausethey
donotkeepthemselvesclean.
Agree 34.0 30.1 39.6 33.56*** Sometimesagree 37.5 40.3 44.2 39.98 Disagree 16.5 13.5 11.0 14.41 Notsure 12.0 14.9 5.2 12.05
13. Therearesomeillnesses
thatdoctorscannottreat.
Agree 38.3 48.9 75.3 49.10* Sometimesagree 36.4 25.1 11.0 27.53 Disagree 12.8 11.0 5.2 10.79 Notsure 12.5 14.9 7.1 12.58
14. Peopleinheritillnessfrom
theirparents.
Agree 25.3 29.8 16.9 25.79* Sometimesagree 42.6 42.5 64.9 46.62 Disagree 18.4 14.4 9.1 15.20 Notsure 13.9 13.0 7.8 12.39

117
15. Ifapersontakesgoodcare ofthemselvestheywill notgetsick.
Agree 31.4 27.3 31.2 29.94** Sometimesagree 34.3 35.1 39.6 35.82 Disagree 19.9 17.1 21.4 19.21 Notsure 14.4 19.3 5.8 15.03
16. Peopleareabletocure
themselveswhentheyaresick.
Agree 19.1 23.8 16.2 20.61*** Sometimesagree 37.2 29.3 43.5 35.25 Disagree 28.5 26.0 27.3 27.36 Notsure 15.2 20.4 12.3 16.78
17. Ifapersongetssickit
istheirownfault.
Agree 11.7 9.1 3.2 9.29* Sometimesagree 23.7 22.4 33.8 25.14 Disagree 51.1 47.2 53.2 50.40 Notsure 13.6 19.6 7.8 15.18
18. Visitingadoctorforregular
checkupscanpreventaperson gettingsick.
Agree 42.8 29.8 38.3 36.98* Sometimesagree 29.8 31.5 40.3 32.47 Disagree 14.4 15.2 10.4 14.09 Notsure 13.0 22.4 10.4 16.46
19. Doctorscanmaketheillness
betterbuttheycannottreat thecause.
Agree 38.0 32.3 33.1 34.98*** Sometimesagree 32.7 28.7 40.3 32.51 Disagree 14.4 18.5 14.9 16.20 Notsure 14.9 20.2 10.4 16.31

118
20. Mostillnessescanbetreated athome.
Agree 26.9 22.9 21.4 24.49* Sometimesagree 31.6 34.0 19.5 30.70 Disagree 23.1 22.9 41.6 26.41 Notsure 18.4 19.3 15.6 18.40
21. Olderpeopleknowalotabout
illnessandcanadviceothers whattodo.
Agree 32.7 26.8 29.2 29.91** Sometimesagree 35.4 35.4 39.6 36.34 Disagree 15.2 13.3 20.1 15.35 Notsure 16.8 23.5 9.7 18.40
22. PeopleshouldpraytoGodto
curethemoftheirillness.
Agree 27.4 23.5 37.7 27.64* Sometimesagree 29.5 25.1 39.0 29.44 Disagree 23.4 25.4 14.3 22.70 Notsure 19.7 25.7 8.4 20.22
23. Peoplegetsickbecausethey
arelazyanddonotworkhard enough.
Agree 18.9 17.7 13.0 17.47** Sometimesagree 36.4 37.0 30.5 35.85 Disagree 28.5 22.7 37.7 27.85 Notsure 16.2 22.4 16.2 18.83
24. Whensickthetreatmentgiven
byeldersorolderpeoplecan reallybehelpful.
Agree 17.8 20.4 13.0 18.17* Sometimesagree 37.2 36.2 37.0 37.02 Disagree 23.1 14.4 31.8 21.22 Notsure 21.8 28.2 16.9 23.59

119
25. Illnessisaformof punishmentforthewrongor badthingsapersonhasdone.
Agree 13.0 10.5 7.8 11.17 Sometimesagree 21.3 18.8 15.6 19.41 Disagree 44.7 48.3 60.4 49.21 Notsure 21.0 21.3 15.6 20.20
26. Peoplegetsickwhensomething
foreigninvadestheirbody.
Agree 40.2 33.4 49.4 39.37** Sometimesagree 33.2 32.3 25.3 31.79 Disagree 16.0 16.6 10.4 15.38 Notsure 10.6 16.9 11.7 13.46
27. Sicknessoccursbecauseyoudo
notdotheritualsorprayer requiredbythepriestorancestors.
Agree 15.4 11.3 5.2 12.04* Sometimesagree 26.1 15.5 16.9 20.25 Disagree 37.8 42.3 59.7 43.53 Notsure 20.8 30.7 17.5 24.18
28. Apersoncanbecomeillif
theywalkorcrossoverapath orspotwheresomeritual wasperformed.
Agree 24.2 25.4 11.0 22.57** Sometimesagree 33.2 27.1 33.1 30.93 Disagree 22.6 24.3 32.5 25.17 Notsure 20.0 22.4 22.1 21.33
29. Sicknessoccursbecauseyour
bodyisnotfunctioningproperly.
Agree 33.0 29.6 50.0 34.76* Sometimesagree 35.6 37.6 33.1 36.23 Disagree 18.9 19.6 5.8 17.04 Notsure 12.5 12.4 9.1 11.96

120
30. Illnessisduetodemon.evil orbadspiritpossession.
Agree 14.9 9.9 9.7 12.06** Sometimesagree 14.9 17.4 24.0 17.59 Disagree 51.9 48.3 39.0 48.48 Notsure 18.4 23.8 25.3 21.87
31. Illnessisduetopunishment
ordesertionbytheancestors
Agree 15.8 16.3 7.1 14.53** Sometimesagree 15.0 13.0 22.1 15.43 Disagree 49.5 44.2 48.1 47.18 Notsure 19.8 26.5 21.4 22.86
*p<0.001
**p<0.01
***p<0.05
Thegroupsdifferedsignificantlyoncertainitems.Theseitemsandthestatistical
significantvaluesarepresentedbelow:item1,betweenall3groups(χ2=50.86,p<0.001);
item3,betweentheHospitalGroupandKwaMashuGroup(χ2=19.16,p<0.001)andthe
KwaMashuGroupandUmlaziGroup(χ2=27.69.p<0.001);item4,all3groups(χ2=17.85,
p<0.01);item5,betweenall3groups(χ2=17.93,p<0.01);item9,betweenall3groups
(χ2=33.24,p<0.001);item10,betweenall3groups(χ2=61.59,p<0.001);item11,between
all3groups(χ2=37.05,p<0.001);item12,betweentheHospitalGroupandKwaMashu
Group(χ2=9.37,p<0.05)andbetweentheKwaMashuandUmlaziGroup(χ2=12.30,
p<0.01);item13,betweenall3groups(χ2=68.92,p<0.001);item14,betweenthe
HospitalGroupandKwaMashuGroup(χ2=23.66,p<0.001)andtheKwaMashuGroupand
UmlaziGroup(χ2=22.96,p<0.001);item15,betweentheKwaMashuGroupandUmlazi
Group(χ2=15.14,p<0.01);item16,betweentheHospitalGroupandUmlaziGroup
(χ2=8.97,p<0.05)andbetweentheKwaMashuGroupandUmlaziGroup(χ2=13.37,

121
p<0.01);onitem17,betweentheHospitalGroupandKwaMashuGroup(χ2=15.89,
p<0.01)andtheKwaMashuGroupandUmlaziGroup(χ2=20.70,p<0.001);onitem18,
betweentheHospitalGroupandUmlaziGroup(χ2=17.92,p<0.001)andbetweentheKwa
MashuGroupandUmlaziGroup(χ2=14.87,p<0.01);item19,betweenKwaMashuGroup
andUmlaziGroup(χ2=11.30,p<0.01);item20,betweentheHospitalGroupandKwa
MashuGroup(χ2=20.65,p<0.001)andtheKwaMashuGroupandUmlaziGroups
(χ2=21.85,p<0.001);item21,betweentheKwaMashuGroupandUmlaziGroup
(χ2=14.63,p<0.01);item22,betweentheHospitalGroupandKwaMashuGroup
(χ2=19.64,p<0.001)andtheKwaMashuGroupandUmlaziGroup(χ2=36.65,p<0.001);
item23,betweentheKwaMashuGroupandUmlaziGroup(χ2=13.79,p<0.01);item24,
betweentheHospitalGroupandUmlaziGroup(χ2=11.53,p<0.01)andtheKwaMashu
GroupandUmlaziGroup(χ2=25.73,p<0.001);item26,betweentheKwaMashuGroup
andUmlaziGroup(χ2=13.69,p<0.01);item27,betweenall3groups(χ2=44.67,p<0.001);
item28,betweentheHospitalGroupandKwaMashuGroup(χ2=13.82,p<0.01)andthe
KwaMashuGroupandUmlaziGroup(χ2=14.65,p<0.01);item29,betweentheHospital
GroupandKwaMashuGroup(χ2=22.09,p<0.001)andtheKwaMashuGroupandUmlazi
Group(χ2=27.63,p<0.001);item30,betweentheHospitalGroupandKwaMashuGroup
(χ2=13.82,p<0.01)and,item31,betweenHospitalGroupandKwaMashuGroup(χ2=
14.09,p<0.01).Themeansandstandarddeviationsofeachitemforthegroupsappearin
TableXXXVIII
Item1assessedthebeliefthatapersongetssickbecausetheyarenotstrong.Onthisitem
theHospitalGroupagreedmorethanthecommunitygroups.Overalltherespondentsdid
'agree'or'sometimesagree'thatifapersonisnotstrongenoughhewillgetsick.Itseems
thatthosewhoattendthehospitalshaveastrongerbeliefthatthosewhoareillarenot
strong.Therewassomewhodisagreedwiththisviewrangingfrom22.6%intheHospital
Groupto37.7%inthecommunityGroup.Therewasgeneralagreementbyallgroupsthat
aperson'sdietmayleadtoillness(item2).Thisisinkeepingwithreasonsthesubjects

122
offeredwhypeoplegetsick(TableXXXV).Thesubjectstendedtodisagreewiththeview
thatillnessisduetodesertionbyGod(item3),especiallythoseintheKwaMashuGroup
(71.4%).Althoughthereisagreementthatitsometimescouldbetrue.Thebeliefthat
illnessiscausedbyinfectionwasoverwhelminglyendorsedbyallsubjects(item4).
Item5,whichrequiredthesubjectstorespondtothebeliefthatillnesswascausedby
witchcraftorsorceryyieldedmixedresponses.Halfofthesubjectseitheragreedor
sometimesagreedordisagreed.Althoughthebeliefisnotadominantoneitobviouslyis
animportantbeliefininterpretingandunderstandingtheirillnesses.Initem6thatdeals
withthebeliefthat'sicknessisduetoacurseorbewitchmentbyothers,therewerealso
mixedresponse.Thereis,however,aslightlyhighertendencytodisagreewithsuch
beliefs.Thereisageneralbeliefamongthesubjectsthatlackoforinadequateregular
exerciseleadstoillhealth(item7).Althoughsmall,therearesomewhodisagreeorare
notsureofthebenefitsofregularexercise.Mostsubjectsdisagreedwiththebeliefthat
sicknesscomesfromthedevil(item8).Ontheaverage25.62%wherenotsure.Asimilar
percentageagreedorsometimesagreed.
Theconsultingofdoctorsastheonlyhelp‐seekingbehaviourwhenseriouslyill(item9)
wasadominanthealthseekingbehaviour.Yetmostofthesubjectsdisagreedwiththe
beliefthatonlydoctorscantreatpeoplewhoareill(item10),thisbeingmoresointhe
communityGroupsthantheHospitalGroup.Ofthosewhoagreedwiththisbelief,the
HospitalGroupshowedgreateragreement.Onitem11,whichassessedthebeliefthat
thereisnothingapersoncandotopreventillness,alargenumberdisagreed;16.74%
agreed,21.91%sometimesagreedand17.19%werenotsure.Thismayindicatethat
thereisabeliefinaninternallocusofcontrolinthepreventionofillness.Sicknessasa
resultofpoorselfcareand/orhygienewasendorsedbymostofthesubjects(item12).
Theintervieweesagreedorsometimesagreedthatsomeillnesscannotbetreatedby
medicaldoctors(item13).Thiswouldsuggestthenthatifindividualsdonotbelievethat
doctorscantreatallillnessestheywouldseekhelpfromothersourcesandpersonsthey

123
feltwouldprovideappropriatetreatment.Subjectsalsoendorsedthebeliefthat
sometimesillnessesareinherited(item14).
Onitem15,subjectsendorsedthebeliefthattakingcareofoneselfcanprevent
illnesses.19,21%disagreedand15.03%werenotsure.Again,theissueofinternallocusof
controlinhealthbehaviourmustbeconsidered.Thesubjectsfeltthattheywereableto
effectacurethemselveswhenill(item16);27.36%disagreedand16.78%werenotsure.
However,theydidnotseeanyreasontoblamethemselvesfortheillness(item17).Only
inafewinstancesdidtheyagreethattheirillnesscouldbetheirfault.
'Visitingadoctorforregularcheckupscanpreventapersongettingsick'wasagreedor
sometimesagreedbymostrespondents(item18).However,14.09%disagreedand
16.46%werenotsure.Inaddition,subjectsexpressedthebeliefthatdoctorscantreat
symptomsbutnotthecause(item19).
Therewasageneralisedresponsetothebeliefthatmostillnessescanbetreatedathome
(item20);24.49%agreed,30.70%agreedsometimes,26.41%disagreedand18.40%were
notsure.Respondentsalsobelievedthatolderpeopleknowalotaboutillnessesandthat
theycanprovideappropriateadvice(item21);29.91%agreedand30.70%sometimes
agreed.
Item22dealtwiththebeliefthatpeopleshouldpraytoGodtocurethemoftheirillness.
Theresponsevariedfrom27.64%agreeing,29.44%agreeingsometimes,22.70%
disagreeingand20.22%notbeingsure.Item23lookedatthebeliefthatpeoplegetsick
becausetheyarelazyanddonotworkhardenough.Mostofthesubjectssometimes
agreed(35.85%).
Beliefsaboutthetreatmentgivenbyeldersorolderpeoplewasassessedbyitem24.The
mostcommonresponsewas'sometimesagree'(37.02%).Thesecondhighestresponse
wasnotsure(23.59%);18.17%agreedand21.22%disagreed.

124
Asmuchas49.21%ofthesubjectsdisagreedwiththebeliefthatillnessisaformof
punishmentforthewrongorbadthingsthatapersonasdone(item25).However,19.41%
agreedsometimes,11.17%agreedand20.20%werenotsure.
Thebeliefthatapersongetssickasaresultofsomethinginvadingtheirbody(item26)
wasawidelyacceptedbeliefbysubjectseitheragreeing(39.37%)orsometimesagreeing
(31.79%).Only13,46%werenotsureand15.38%disagreedwiththestatement.TheKwa
Mashusubjectsshowedthehighestagreementwiththestatement(49.4%)andlowest
disagreement(10.4%).Item27assessedthebeliefthatsicknessoccurredasaresultofnot
performingtherequiredritualsorprayerstotheancestors.Although43.53%disagreed
withthisbelief,12.04%agreed,20.25%agreedsometimesand24.18werenotsure.The
KwaMashusubjectsdemonstratedtheleastagreementwiththestatement(5.2%)and
highestdisagreement(59.7%).Avariedresponsewasobtainedforthebeliefthatpeople
canbecomeilliftheywalkorcrossoverapathorplacewheresomeritualwasperformed
(item28).Theresponse'sometimesagree'wasthemostcommon(22.57%),while22.57%
agreedand21.33%werenotsure.25.17%disagreedwiththebelief.TheKwaMashu
Groupdemonstratedthelowestagreementwiththisbelief.
Thebeliefthatsicknessistheresultofmalfunctioningorimproperfunctionofthebody
(item29)appearstobeacommonbeliefoftherespondents;34.76%agreedand36.23%
sometimesagreed.TheKwaMashusubjectsshowedahighagreementwiththestatement
(50.0%)andthelowestdisagreement(5.8%)
Therewasahighdisagreementwithstatement30thatillnessisduetodemon,evilorbad
spiritpossession(48.48%).BoththecommunityGroupsshowedlowagreement;Umlazi
9.9%andKwaMashu9.7%.TheHospitalGroupdemonstratedmoreagreementwiththe
belief(14.9%).However,theHospitalGroupalsorespondedwiththehighest
disagreement(51.9%).
Thelastitemassessedthebeliefthatillnessisduetopunishmentordesertionbythe
ancestors.Therespondentsshowedhighdisagreementwiththisbelief(47.18%).

125
Although,22.86%werenotsure,14.53%agreedand15.43%sometimesagreedwiththe
belief.TheKwaMashuGroupindicatedalowagreementwiththisbelief.
TABLEXXXVIII MEANSANDSTANDARDDEVIATIONSOFEACHHBQITEMFORGROUP
Item Hospital Umlazi KwaMashu No. MeanSD MeanSD MeanSD
1 1.88 0.99 1.98 0.912.45 0.98* 2 1.55 0.73 1.64 0.721.67 0.78 3 2.72 0.85 2.62 0.852.94 0.62* 4 1.54 0.78 1.68 0.881.47 0.81** 5 2.43 1.05 2.55 1.032.65 0.94** 6 2.72 1.02 2.75 0.932.76 0.93
7 2.07 1.04 2.07 1.071.99 0.93 8 2.83 0.96 2.89 0.912.90 0.95 9 2.02 1.08 2.24 1.161.86 0.84* 10 2.55 1.00 2.86 0.892.72 0.79* 11 2.50 0.97 2.73 0.952.65 0.91* 12 2.06 0.99 2.13 1.011.82 0.82*** 13 1.99 1.01 1.92 1.091.43 0.89* 14 2.20 0.97 2.11 0.982.08 0.76* 15 2.17 1.03 2.29 1.072.02 0.88** 16 2.39 0.96 2.43 1.072.36 0.90*** 17 2.66 0.85 2.79 0.872.67 0.67* 18 1.98 1.05 2.30 1.131.93 0.95* 19 2.06 1.06 2.27 1.122.03 0.96*** 20 2.33 1.06 2.39 1.052.52 1.01* 21 2.16 1.06 2.34 1.122.11 0.94** 22 2.35 1.08 2.53 1.111.93 0.93* 23 2.42 0.97 2.50 1.032.59 0.92** 24 2.49 1.02 2.51 1.112.53 0.93* 25 2.73 0.94 2.81 0.892.84 0.78 26 1.97 0.99 2.17 1.081.84 1.04** 27 2.63 0.98 2.93 0.962.98 0.74* 28 2.38 1.06 2.44 1.102.66 0.95** 29 2.11 1.00 2.15 0.991.74 0.94* 30 2.74 0.93 2.86 0.892.81 0.93** 31 2.73 0.95 2.81 1.012.85 0.84**
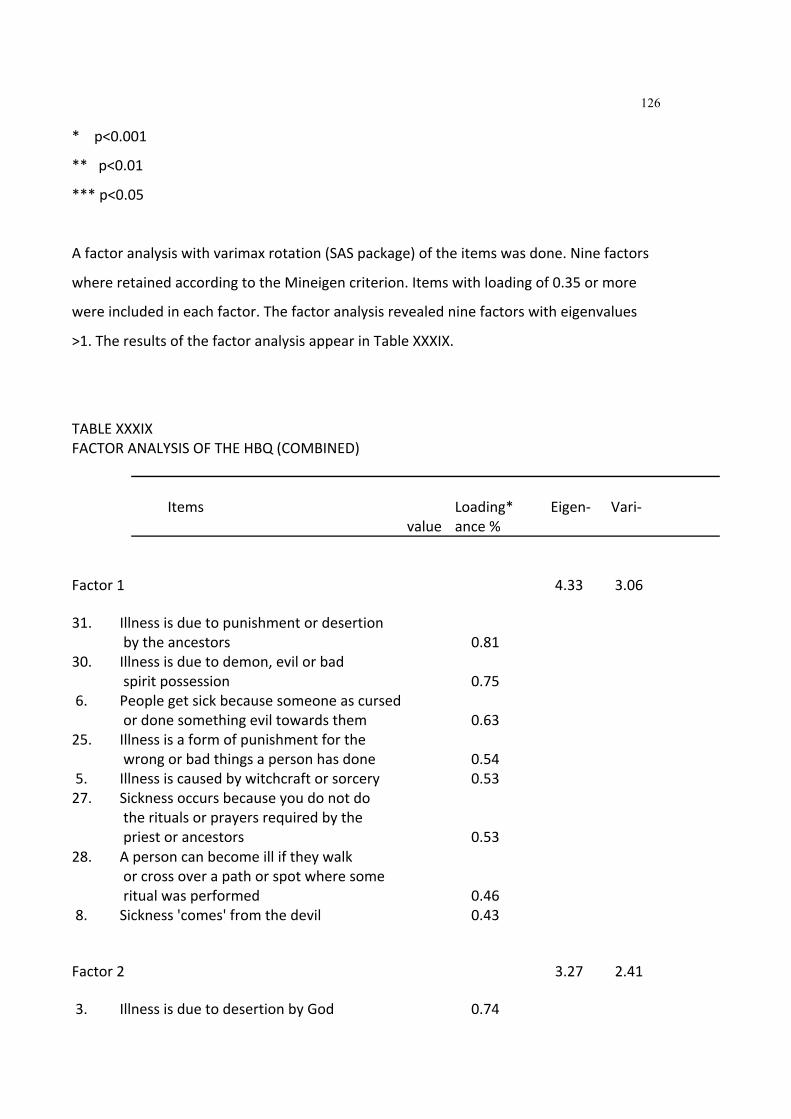
126
*p<0.001
**p<0.01
***p<0.05
Afactoranalysiswithvarimaxrotation(SASpackage)oftheitemswasdone.Ninefactors
whereretainedaccordingtotheMineigencriterion.Itemswithloadingof0.35ormore
wereincludedineachfactor.Thefactoranalysisrevealedninefactorswitheigenvalues
>1.TheresultsofthefactoranalysisappearinTableXXXIX.
TABLEXXXIX FACTORANALYSISOFTHEHBQ(COMBINED)
Items Loading* Eigen‐ Vari‐ value ance% Factor1 4.33 3.06 31. Illnessisduetopunishmentordesertion
bytheancestors 0.81 30. Illnessisduetodemon,evilorbad
spiritpossession 0.75 6. Peoplegetsickbecausesomeoneascursed
ordonesomethingeviltowardsthem 0.63 25. Illnessisaformofpunishmentforthe
wrongorbadthingsapersonhasdone 0.54 5. Illnessiscausedbywitchcraftorsorcery 0.53 27. Sicknessoccursbecauseyoudonotdo
theritualsorprayersrequiredbythe priestorancestors 0.53
28. Apersoncanbecomeilliftheywalk orcrossoverapathorspotwheresome ritualwasperformed 0.46
8. Sickness'comes'fromthedevil 0.43 Factor2 3.27 2.41 3. IllnessisduetodesertionbyGod 0.74

127
1. Peoplegetsickbecausetheyare notstrong 0.60
17. Ifapersongetssickitistheirownfault 0.56 Factor3 1.94 2.08 2. Peoplegetsickbecausetheydonot
eattheproperfoods 0.68 4. Illnessiscausedbyinfection 0.50 12. Peoplegetsickbecausetheydonot
keepthemselvesclean 0.46 14. Peopleinheritillnessesfromtheirparents 0.43 Factor4 1.51 2.01 20. Mostillnessescanbetreatedathome 0.71 24. Whensick,thetreatmentgivenbyelders
orolderpeoplecanreallybehelpful 0.64 21. Olderpeopleknowalotaboutillness
andcanadviseotherswhattodo 0.63 16. Peopleareabletocurethemselves
whentheyaresick 0.49 Factor5 1.25 1.84 29. Sicknessoccursbecauseyourbodyis
notfunctioningproperly 0.66 23. Peoplegetsickbecausetheyarelazy
anddonotworkhardenough 0.58 7. Peoplegetsickbecausetheydonot
exerciseregularly 0.58 26. Peoplegetsickwhensomething
foreigninvadestheirbody 0.50 Factor6 1.18 1.46 10. Doctorsaretheonlyoneswhocan
treatpeoplewhoareill 0.70 11. Thereisnothingapersoncandoto
preventthemselvesfromgettingill 0.61 9. Peoplegotodoctorsonlywhenthey
areseriouslyill 0.41

128
Factor7 1.15 1.45 18. Visitingadoctorforregularcheckups
canpreventapersongettingsick 0.79 15. Ifapersontakesgoodcareof
themselvestheywillnotgetsick 0.60 Factor8 1.07 1.24 22. PeopleshouldpraytoGodtocure
themoftheirillness 0.68 Factor9 1.01 1.19 19. Doctorscanmaketheillnessbetter
buttheycannottreatthecause 0.80 *Itemswithloadingsof0.35ormoreonafactorwereretained.
Theninefactorswhichemergedcouldbedescribedasfollows:
Factor1:Externalevilorancestralinfluence‐cultural(aetiology)
Theitemsthatloadedonthisfactorsuggestthattheaetiologyofillnessistheresultof
'punishmentordesertionbytheancestors';'demon,evilorbadspiritpossession';
'becausesomeonehascursedordonesomethingeviltowardsanother';'formof
punishmentforthewrongorbadthingsapersonhasdone''witchcraftorsorcery';'donot
dotheritualsorprayerrequiredbythepriestorancestors';'theywalkorcrossoverapath
orspotwheresomeritualwasperformed';'comesfromthedevil'.

129
Factor2:Selfblame(aetiology)
Theitemsthatloadedonthisfactorsupportstheaetiologyofillnessasaresultofthe
individualnotbeingstrongenough.IllnessisduetodesertionbyGod;becausepeopleare
notstrong;oritistheindividual'sfault.
Factor3:Medicalreason(aetiology)
Theitemsthatloadedonthisfactorsuggestthatpeoplegetsickbecausetheydonoteat
theproperfoods;illnessiscausedbyinfection;peoplegetsickbecausetheydonotkeep
themselvesclean;peopleinheritillnessesfromtheirparents.
Factor4:Selfmedication(treatment)
Thisfactordealswithtreatment.Theitemsthatloadedheresuggestthatmostillnesses
canbetreatedathome;treatmentgivenbyeldersorolderpeoplecanreallybehelpful;
olderpeopleknowalotaboutillnessandcanadviseotherswhattodoandpeopleare
abletocurethemselveswhentheyaresick.
Factor5:Physicalweaknessorbodymalfunctioning(aetiology)
Thisfactorsuggeststhatsicknessoccursbecausethebodyisnotfunctioningproperly;
peoplegetsickbecausetheyarelazyanddonotworkhardenough;ortheydonot
exerciseregularlyorpeoplegetsickwhensomethingforeigninvadestheirbody.

130
Factor6:Medical(treatment)
Theitemsthatloadedonthisfactorsupportstheviewthatdoctorsaretheonlyoneswho
cantreatpeoplewhoareill,thatthereisnothingapersoncandotopreventthemselves
fromgettingillandthatpeoplegotodoctorsonlywhentheyareseriouslyill.
Factor7:Selfcare(prevention)
Thisfactorrepresentsitemsthatinvolveselfcareasapreventativemeasureagainst
illness.Theitemsthatloadedonthisfactorincludedvisitingadoctorforregularcheckups
topreventapersongettingsick;ifapersontakesgoodcareofthemselvestheywillnot
getsick;
Factor8:Useofprayer(treatment)
Theitemthatloadedonthisfactor'peopleshouldpraytoGodtocurethemoftheir
illness'suggestprayerandtheevokingofGod'sassistanceasamethodoftreatment.
Factor9:Holisticbelief(treatment)
Thisfactorsuggestthatthemedicalmodelisonlypartlyeffectiveasatreatment.Theitem
loadingonthisfactor'doctorscanmaketheillnessbetterbuttheycannottreatthecause'
suggestadditionalmethodstothemedicalmodel.
Factorscoreswerecalculatedforeachoftheninefactorsbyaddingthevaluesoneach
item.Amultivariateanalysis(MANOVA)wasperformedontheninefactorswithmain

131
effects:group,sexandurbanisation(0‐5yearsand>5years).Agewasusedasacovariate.
ThefactorscoresforeachfactorisfoundinTableXL.
TABLEXL MEANFACTORSCORESONTHENINEFACTORSRELATINGTOHEALTHBELIEF Factor Hospital Umlazi KwaMashu
Mean SD Mean SD Mean SD
1 17.83 4.31 18.99 3.86 19.37 4.23 2 8.55 1.80 8.45 1.67 8.77 1.25 3 6.65 1.69 6.69 1.85 6.46 1.53 4 7.90 1.95 7.82 1.92 8.36 2.29 5 7.31 2.03 7.12 1.86 7.00 1.81 6 6.17 1.62 6.61 1.32 6.82 1.44 7 3.52 1.22 3.79 1.08 3.57 1.22 8 1.95 0.80 2.03 0.82 1.74 0.72 9 1.72 0.73 1.83 0.78 1.79 0.71
Onfactor1nomaineffectsorinteractionswerefound.
OnFactor2therewassignificantdifferencesbetweenlivinginanurbanareafor0‐5years
and>5years.(F(1,885)=13.59,p=0.0003).OnFactor3theanalysisrevealedsignificant
differencesinthegroupbyurbaninteraction(p=0.0179),andsignificancewitheffecton
age(p=0.0015).SignificantdifferencesbetweentheHospital,UmlaziandKwaMashu
Groups(p=0.0220),urban(p=0.0355),groupbyurbaninteraction(p=0.0031)werefound
onfactor4.
Onfactor5significantdifferenceswerefoundbetweengroups(p=0.0012),groupsby
urbaninteraction(p=0.0003)andage(p=0.0483)
Forfactor6significantdifferenceswerefoundbetweengroups(p=0.0370)andbetween
groupsbyinteraction(p=0.0370).

132
Significantdifferenceswasfoundonfactor7dependingonthenumberofyearspatients
werelivinginanurbanarea(p=0.0165),ingroupbysex(p=0.0407)andingroupbylivingin
urbanareas(p=0.0250).
Onfactor8thesignificantdifferenceswerebetweengroups(p=0.0146)andbetween
groupbyurbandwelling(p=0.0137).
Onfactor9significantdifferenceswerefoundingroupbyurbandwelling(p=0.0423)and
age(p=0.0106).
5.10SOCIALSUPPORT
ThereliabilityoftheSSQwasdeterminedbysubjectingittotheCronbach'salphatest.A
Cronbach'scoefficientalphaof0.91wasobtained.TableXLIliststhepercentageof
responsesoneachitem.Itwouldappearfromtheresponsesthatthesubjectsinallgroups
weregenerallysatisfiedwiththesocialsupporttheyreceivedandperceivedthemselvesas
asourceofsupportaswell.

133
TABLEXLI COMPARISONSOFSSQITEMSBETWEENGROUPS(in%)
Hospital Umlazi KwaMashu Combined (N=368) (N=360) (N=152) (N=880)
1. Whocanyoureallycount
ontolistentoyouwhen youneedtotalk?
Verysatisfied 60.05 53.31 64.24 58.00 Satisfied 39.13 46.69 35.10 41.54 Dissatisfied 0.82 0.00 0.00 0.34 Verydissatisfied 0.00 0.00 0.66 0.11
2. Whocouldyoureallycount
ontohelpyouinanemerg‐ encyorcrisissituation.
Verysatisfied 52.72 52.50 57.89 53.52 Satisfied 46.26 46.94 40.79 45.57 Dissatisfied0.82 0.28 1.32 0.68 Verydissatisfied 0.27 0.28 0.00 0.23
3. Whohelpsyoufeelthatyou
areagoodandworthwhile person?
Verysatisfied 55.59 52.22 51.66 53.53 Satisfied 42.78 46.39 45.70 44.76 Dissatisfied1.09 0.83 0.66 0.91 Verydissatisfied 0.54 0.56 1.99 0.80

134
4. Whomcanyoureallygoto whenyouareworriedand/ orunderpressure?
Verysatisfied 53.53 52.91 42.38 51.36 Satisfied 44.57 46.26 56.95 47.36 Dissatisfied1.63 0.55 0.66 1.02 Verydissatisfied 0.27 0.28 0.00 0.23
5. Whocanyoucountonwhen
yougenerallyneedhelpfor reasonsotherthanan emergencyorcrisis?
Verysatisfied 48.50 49.58 41.72 47.78 Satisfied 50.14 49.58 54.97 50.74 Dissatisfied1.36 0.83 2.65 1.37 Verydissatisfied 0.00 0.00 0.66 0.11
6. Whocanyoureallycount
ontohelpyouifthingsgo wrong,youhaveamishapor runoutofluck?(eg.fired fromyourjob,meetan accident,etc.)
Verysatisfied 50.95 49.58 47.37 49.77 Satisfied 47.97 50.15 48.68 48.97 Dissatisfied0.81 0.28 3.95 1.13 Verydissatisfied 0.27 0.00 0.00 0.11
7. Whocanyoureallycounton
togiveyouusefuladvice, guidanceorsuggestions thathelpyoutoavoid makingmistakes?
Verysatisfied 48.91 48.20 49.34 48.69 Satisfied 49.46 50.42 49.34 49.83 Dissatisfied1.36 1.39 1.32 1.36 Verydissatisfied 0.27 0.00 0.00 0.11
8. Whodoyoufeelwould
helpifafamilymember

135
orsomeoneveryclose toyoudied?
Verysatisfied 45.11 49.72 42.00 46.47 Satisfied 53.26 47.78 54.67 51.25 Dissatisfied1.36 2.22 2.67 1.94 Verydissatisfied 0.27 0.28 0.67 0.34
9. Whodoyoufeeltruly
lovesyoudeeply?
Verysatisfied 55.83 57.50 70.20 58.98 Satisfied 43.09 41.94 29.80 40.34 Dissatisfied0.54 0.28 0.00 0.34 Verydissatisfied 0.54 0.28 0.00 0.34
10. Whocanyoucountonto
comfort/consoleyouwhen youareveryupset?
Verysatisfied 46.17 48.88 53.33 48.51 Satisfied 51.91 50.84 46.00 50.46 Dissatisfied1.64 0.28 0.67 0.92 Verydissatisfied 0.27 0.00 0.00 0.11
11. Whocanyoureallycount
ontosupportyouinmajor decisionsorplansyoumake?
Verysatisfied 50.68 44.60 52.00 48.41 Satisfied 48.23 54.29 47.33 50.57 Dissatisfied1.09 1.11 0.00 0.91 Verydissatisfied 0.00 0.00 0.67 0.11

136
12. Whodoyouknowwhomyou cantrustwithasecretor informationthatcould getyouintrouble?
Verysatisfied 49.86 45.98 50.34 48.34 Satisfied 48.77 52.91 46.26 50.06
Dissatisfied 0.82 0.83 2.72 1.14 Verydissatisfied 0.54 0.28 0.68 0.46
13. Whodoyoucountonwhen
youareill?
Verysatisfied 49.05 40.28 57.33 46.87 Satisfied 49.05 58.89 41.33 51.76 Dissatisfied1.63 0.56 0.67 1.02 Verydissatisfied 0.27 0.28 0.67 0.34
14. Whocanyoureallycounton
whenyougetintotrouble?
Verysatisfied 48.91 42.46 54.05 47.13 Satisfied 50.55 55.87 45.95 51.95 Dissatisfied0.55 1.40 0.00 0.80 Verydissatisfied 0.00 0.28 0.00 0.11
15. Whodoyouthinkwillcome
toyouiftheyhadaneed orproblem?
Verysatisfied 57.14 48.19 45.27 51.44 Satisfied 41.76 50.97 52.70 47.42 Dissatisfied1.10 0.56 1.35 0.92 Verydissatisfied 0.00 0.28 0.68 0.23
Themeansandstandarddeviationsofthesubjects'responsesforeachitemontheSSQ
arepresentedinTableXLIV.

137
TABLEXLII MEANSANDSTANDARDDEVIATIONSOFSSQITEMSBYGROUPS Item Hospital Umlazi KwaMashu No. Mean SD Mean SD Mean SD
1. 3.59 0.51 3.53 0.50 3.63 0.52 2. 3.51 0.53 3.52 0.52 3.57 0.52 3. 3.53 0.55 3.50 0.55 3.47 0.62 4. 3.51 0.55 3.52 0.53 3.42 0.51 5. 3.47 0.53 3.49 0.52 3.38 0.57 6. 3.50 0.53 3.49 0.51 3.43 0.57 7. 3.47 0.54 3.47 0.53 3.48 0.53 8. 3.43 0.54 3.47 0.56 3.38 0.58 9. 3.54 0.54 3.57 0.52 3.70 0.46 10. 3.44 0.54 3.49 0.51 3.53 0.51 11. 3.50 0.52 3.43 0.52 3.52 0.54 12. 3.48 0.55 3.45 0.53 3.46 0.59 13. 3.47 0.55 3.39 0.52 3.55 0.55 14. 3.48 0.51 3.41 0.54 3.54 0.50 15. 3.56 0.51 3.47 0.53 3.43 0.56
5.10.1 Comparisonsofgroupsonaccessibilityandproximity
Analysisofvariancewasperformedonthevariablesaccessibility(immediateanddelayed)
andproximity(nearbyandfar).Significantdifferenceswerefoundbetweenthethree
groupsonallthesevariables(TableXLII).
TABLEXLIII ANOVAOFACCESSIBILITYANDPROXIMITY
df F p

138
Accessibility:
Immediate 2 98.72 p<0.0001* Delayed 2 71.07 p<0.0001**
Proximity:
Nearby 2 110.30 p<0.0001* Far 2 67.08 p<0.0001**
Duncan'sMultipleRangeTestwasperformedasaposthoctestforpairwisecomparisons.
TheresultsarefoundinTableXLIII.
Themodeinwhichthesubjectsobtainedtheirsupportwasasfollows:HospitalGroup
(N=376),304(80.85%)usedthetelephoneand123(32.71%)wrote;UmlaziGroup
(N=362),20(5.52%)usedthetelephoneand100(27.62%)wrote;withtheKwaMashu
Group(N=154),147(95.45%)telephonedand92(59.74%)wrote.BoththeHospitaland
theKwaMashuGroupsusedthetelephoneasthemainmeansofcommunicationandfor
obtainingsocialsupport.Theotherwaywasbypostalservice.
Afactoranalysisofthesubjects'responsesonthefifteenitemsontheSSQwasdone.The
rotationalvarimaxmethodwasusedandtwofactorsemerged(TableXLV).
TABLEXLIV DUNCAN'SMULTIPLERANGETEST
Duncan's GroupingMean N Group

139
Accessibility(immediate)
A 3.43 154 KwaMashu B 2.03 362 Umlazi C 1.75 376 Hospital
Accessibility(delayed)
A 1.66 154 KwaMashu B 0.69 362 Umlazi B 0.62 376 Hospital
Proximity(Nearby)
A 3.40 154 KwaMashu B 2.00 362 Umlazi C 1.64 376 Hospital
Proximity(Far)
A 1.71 154 KwaMashu B 0.70 362 Umlazi B 0.70 376 Hospital
Thesubjectsreportedobtainingsocialsupportfrommainlyfamilyandfriends.Thefamily
supportwasasfollows:mother(27,78%),spouse(22.53%),friend(7.80%),brother
(7.17%),father(6.59%),sister(5.38%),children(4.16%)andpriest/minister(1.34).No
subjectreportedfathersupportonitem10‐‘Whocanyoucountontocomfortorconsole
youwhenyouareveryupset?’

140
TABLEXLV FACTORANALYSISOFTHESSQ(COMBINED)
Items Loading* Eigen‐ Vari value ance%
Factor1 6.74 4.21 2. Whocouldyoureallycountontohelp
youinanemergencyorcrisissituation? 0.72 4. Whocanyoureallygotowhenyouare
worriedand/orunderpressure? 0.72 5. Whocanyoucountonwhenyougenerally
needhelpforreasonsotherthanan emergencyorcrisis? 0.72
6. Whocanyoureallycountontohelpyou ifthingsgowrong,youhaveamishap orrunoutofluck?(eg.firedfromyour job,meetanaccident,etc.) 0.71
3. Whohelpsyoufeelthatyouareagood andworthwhileperson? 0.70
1. Whocanyoureallycountontolisten toyouwhenyouneedtotalk? 0.65
7. Whocanyoureallycountontogiveyou usefuladvice,guidanceorsuggestions thathelpyoutoavoidmakingmistakes? 0.63
8. Whodoyoufeelwouldhelpifafamily memberorsomeoneveryclosetoyoudied? 0.54
Factor2 1.37 3.90 13. Whodoyoucountonwhenyouareill? 0.78 14. Whocanyoureallycountonwhenyou
getintotrouble? 0.75 15. Whodoyouthinkwillcometoyouif
theyhadaneedorproblem? 0.72 12. Whodoyouknowwhomyoucantrustwith
asecretorinformationthatcouldget youintrouble? 0.71
11. Whocanyoureallycountontosupport youinmajordecisionsorplansyoumake? 0.69
10. Whocanyoucountontocomfort/ consoleyouwhenyouareveryupset? 0.59
9. Whodoyoufeeltrulylovesyoudeeply? 0.56 *Itemswithloadingsof0.35ormoreonafactorwereretained
Factor1

141
Theitemsthatloadedhighonthisfactordealswithsupportinanemergencyorcrisis
situation;whenyouareworriedand/orunderpressure;needhelpforreasonsotherthan
anemergencyorcrisis;helpyouifthingsgowrong,youhaveamishaporrunoutofluck?
(eg.firedfromyourjob,meetanaccident,etc.);helpsyoufeelthatyouareagoodand
worthwhileperson;tolistentoyouwhenyouneedtotalk;togiveyouusefuladvice,
guidanceorsuggestionsthathelpyoutoavoidmakingmistakes;helpifafamilymember
orsomeoneveryclosetoyoudied.
Factor2
Theitemsthatloadedhighonthisfactordealswithsupportwhenill;whenyougetinto
trouble;iftheyhadaneedorproblem;cantrustwithasecretorinformationthatcould
getyouintrouble;inmajordecisionsorplansyoumake;tocomfort/consoleyouwhen
youareveryupset';whoyoufeeltrulylovesyoudeeply.
Factorscoresforeachofthefactorsonthesocialsupportquestionnairewerecalculated
byaddingthevaluesforeachitemonthefactor.A3‐wayMultivariateAnalysisofVariance
(MANOVA)wasperformedonthetwofactorstodeterminewhethertherewere
differencesbetweenthe3groups(Hospital,UmlaziandKwaMashu),betweenmalesand
femalesandbetweenlivinginanurbanareafor0‐5yearsand>5years.(TheMANOVA
testsforwithinsubjecteffectsandrelatedinteractions).Theactualagewasusedasa
covariateintheanalysis.
TheoverallFtestsyieldedsignificanteffectsforbothFactor1(F=2.08,p<0.0162)and
Factor2(F=1.83,p<0.0404).
OnFactor1themaineffects(group,sexandurbandwelling)showednosignificantresults.
Howeverthereweresignificantinteractionsbetweengroupbysex(p=0.0072),groupby
urbandwelling(p=0.0178)andsexbyurbandwelling(p=0.0289).SeeTableXLVI.

142
TABLEXLVI MANOVAONFACTOR1OFSSQ
df SD F p Group 2 31.06 1.64 0.1940 Sex 1 27.49 2.91 0.0885 Urban 1 3.76 0.40 0.5284 Groupbysex 2 93.86 4.97 0.0072* Groupbyurban 2 76.54 4.05 0.0178** Sexbyurban 1 5.27 4.79 0.0289** Groupbysexbyurban 2 34.30 1.81 0.1636 Age 1 57.92 6.13 0.0135**
*p<0.01
*p<0.05
Asignificantgroupbysexinteractionmeantthatthemalesandthefemalesinthe3
groupsrespondeddifferentlytofactor1.Agealsohadasignificanteffectonthefactor
(p=0.0135).
TableXLVIIshowsthesignificantinteractionsonfactor2betweengroupandsex
(p=0.0465)andgroupbyurbandwelling(p=0.0160).

143
TABLEXLVII MANOVAONFACTOR2OFSSQ
df SD F p Group 2 16.59 1.11 0.3291 Sex 1 17.68 2.37 0.1238 Urban 1 20.43 2.74 0.0981 Groupbysex 2 45.89 3.08 0.0465* Groupbyurban 2 61.98 4.16 0.0160* Sexbyurban 1 5.50 0.74 0.3905 Groupbysexbyurban 2 10.66 0.72 0.0894 Age 1 1.23 0.17 0.6846 *p<0.05
ItisalsoapparentfromtheMANOVAthatthereisagoodcorrelationbetweenFactor1
andFactor2(r=0.670).
5.11SYMPTOMPERCEPTIONS ReliabilitywasdeterminedusingtheCronbach'scoefficientalphatest.Ahighreliabilityof
0.96wasachieved.Thepercentageofsubjectsineachgroupwhohadexperiencedthe
symptomsinthemodifiedsymptominventoryisfoundinTableXLVIII.

144
TABLEXLVIII EXPERIENCEOFSYMPTOMSBYEACHSUBJECTBYGROUP
Symptom HospitalUmlazi KwaMashu Total 1 Headaches 93.86 92.07 93.42 93.12 2 Nervousnessorshakiness
inside 53.98 47.59 66.45 56.01 3 Beingunabletogetrid
ofbadthoughtsorideas 31.52 29.12 36.49 32.38 4 Faintnessordizziness 59.93 43.05 65.3356.10 5 Lossofsexualinterest
orpleasure 25.45 20.28 42.28 29.34 6 Feelingcriticalofothers 29.09 40.00 27.63 32.24 7 Baddreams 65.34 58.13 68.21 63.89 8 Difficultyinspeakingwhen
youareexcited 50.54 55.52 48.00 51.35 9 Troublerememberingthings 48.55 45.33 52.32 48.73 10 Worriedaboutsloppinessor
carelessness 48.73 50.35 51.66 50.25 11 Feelingeasilyannoyedor
irritated 56.52 51.22 63.58 57.12 12 Painsintheheartorchest 40.43 32.17 44.08 38.89 13 Itching 48.55 44.95 81.2158.24 14 Feelinglowinenergyor
sloweddown 56.36 57.04 78.15 63.85 15 Thoughtsofendingyourlife 18.84 30.66 11.8420.44 16 Sweating 71.38 65.97 68.87 68.74 17 Trembling 42.55 37.98 27.81 36.11 18 Feelingconfused 50.36 42.86 51.32 48.18 19 Poorappetite 61.96 63.88 63.58 63.14 20 Cryingeasily 35.87 37.63 26.67 33.39 21 Feelingshyoruneasywith
theoppositesex 37.09 35.44 31.58 34.70 22 Afeelingofbeingtrapped
orcaught 25.82 32.40 18.42 25.55 23 Suddenlyafraidfornoreason 34.55 35.89 33.55 34.66 24 Temperoutburstyoucould
notcontrol 49.82 50.17 46.71 48.90 25 Constipation 52.73 59.16 79.47 63.79 26 Blamingyourselfforthings 50.18 54.86 64.00 56.35 27 Painsinthelowerpartof
yourback 52.19 49.13 54.00 51.77

145
28 Feelingblockedorstymied ingettingthingsdone 35.79 35.44 42.3837.87
29 Feelinglonely 46.91 50.69 72.3756.66 30 Feelingblue 40.22 47.06 59.87 49.05 31 Worryingorstewingabout
things 48.00 54.33 74.17 58.83 32 Feelingnointerestinthings 42.34 38.19 58.94 46.49 33 Feelingfearful 38.77 41.96 47.3342.69 34 Yourfeelingsbeing
easilyhurt 41.82 44.10 51.32 45.75 35 Havingtoaskothers
whatyoushoulddo 51.83 51.21 54.61 52.55 36 Feelingothersdonot
understand 38.69 47.74 49.01 45.15 37 Feelingthatpeopleare
unfriendlyordislikeyou 34.07 48.59 43.71 42.12 38 Havingtodothingsveryslowly
inordertobesureyouare doingthemright 57.86 59.52 61.18 59.52
39 Heartpoundingorracing 44.77 33.80 43.71 40.76 40 Nauseaorupsetstomach 53.99 54.17 72.85 60.34 41 Feelinginferiortoothers 41.30 56.40 36.18 44.63 42 Sorenessofyourmuscles 45.29 43.94 63.16 50.80 43 Loosebowelmovements 63.64 76.82 72.37 70.94 44 Difficultyinfallingasleep
orstayingasleep 50.91 43.94 74.83 56.56 45 Havingtocheckanddouble
checkwhatyoudo 58.39 55.71 75.66 63.25 46 Difficultymakingdecisions 40.88 36.81 60.26 45.98 47 Wantingtobealone 48.18 38.06 52.63 46.29 48 Troublegettingyourbreath 33.45 31.25 26.00 28.23 49 Hotorcoldspells 45.99 40.21 59.73 48.64 50 Havingtoavoidcertain
placesoractivitiesbecause theyfrightenyou 36.86 42.01 46.26 41.71
51 Yourmindgoingblank 24.54 28.13 19.21 23.96 52 Numbnessortinglingin
partsofyourbody 26.37 24.13 23.65 24.72 53 Alumpinyourthroat 29.20 29.72 38.6732.53 54 Feelinghopelessabout
thefuture 35.40 33.33 41.33 36.69 55 Troubleconcentrating 32.12 32.64 37.75 34.17 56 Weaknessinpartsofyourbody 35.77 25.00 20.95 27.24 57 Feelingtenseorkeyedup 30.40 29.51 28.67 29.53 58 Heavyfeelingsinyour

146
armsorlegs 33.94 29.51 27.52 30.32 Additionalitems 59 Fever 79.93 79.44 88.74 82.70 60 Chills 64.47 70.48 75.66 70.20 61 Sorethroat 63.50 69.90 82.00 71.80 62 Achesandpainsallover 62.41 59.16 70.39 63.99 63 Sneezing 66.42 59.93 86.75 71.03 64 Runnynose 51.27 43.55 67.32 54.05 65 Stomachpain 56.93 47.06 73.33 59.12 66 Swelling 34.18 24.31 26.67 28.39 67 Hairloss 21.82 36.24 27.15 28,40 68 Painduringurination 30.55 29.51 40.6733.58 69 Skinrash 42.70 41.96 58.94 47.87 70 Coughing 66.18 61.94 80.00 69.37 71 Blurredvision 32.36 42.51 30.2635.04 72 Slurredspeech 20.36 25.69 18.54 21.53 73 Vomiting 31.64 32.29 48.67 37.53 74 Bloodinstool 17.45 20.07 17.4518.32 75 Coughingblood 21.09 19.10 9.21 16.47 76 Burningsensationsalloveror
incertainpartsofthebody 36.36 35.79 23.49 31.88 77 Lossofweight 41.82 52.26 44.0846.05 78 Swollenglands 21.45 23.26 15.13 19.95 79 Nightsweats 46.91 39.58 36.18 40.89 80 Bleeding 20.07 26.65 24.83 23.85 81 Dischargefromear,noseoreyes 14.18 18.53 15.44 16.05 82 Vaginalorpeniledischarge 17.88 20.83 34.23 24.31 83 Bloodinurine 11.31 16.96 15.5414.60

147
5.12SUBJECTSRATINGOFSEVERITYOFSYMPTOMS
TableXLIXpresentsthemeanandstandarddeviationsofthesubjectsratingofseverityofsymptoms.Theseverityofthesymptomswereratedasfollows:notserious=1;serious=2andveryserious=3.Themeanscoreforeachitemindicatesthattheitemswereratedasbeingeitherseriousorveryseriousbythesubjects.TABLEXLIXMEANANDSTANDARDDEVIATIONOFSEVERITYOFSYMPTOMSItem Hospital Umlazi KwaMashuNo. Mean SD Mean SD Mean SD1. 2.87 0.83 2.63 0.72 2.63 0.772. 2.34 0.87 2.05 0.82 2.45 0.933. 2.07 0.05 1.96 0.88 2.36 0.914. 2.36 0.89 2.04 0.89 2.54 0.845. 2.04 0.87 1.87 0.89 2.74 1.036. 2.09 0.81 2.21 0.97 2.17 0.847. 2.50 0.87 2.41 0.92 2.55 0.788. 2.29 0.84 2.34 0.99 2.49 0.859. 2.25 0.87 2.05 0.85 2.65 0.8810. 2.35 0.93 2.35 1.01 2.46 0.8211. 2.39 0.86 2.47 1.01 2.57 0.8212. 2.19 0.88 1.99 0.89 2.52 0.8213. 2.22 0.88 2.02 0.83 2.37 0.7414. 2.36 0.92 2.21 0.83 2.21 0.6215. 1.99 0.84 1.98 0.93 2.99 1.1516. 2.50 0.92 2.14 0.76 2.26 0.6717. 2.26 0.93 1.97 0.84 2.38 0.8518. 2.28 0.94 2.06 0.90 2.59 0.9019. 2.39 0.95 2.35 0.92 2.36 0.7420. 2.15 0.94 2.12 0.99 2.24 0.8221. 2.04 0.92 1.93 0.93 2.40 0.8122. 1.96 0.86 1.87 0.94 2.41 0.9423. 1.97 0.93 2.03 1.02 2.59 0.9424. 2.18 1.04 2.43 1.09 2.69 0.9025. 2.08 0.93 2.23 0.93 2.49 0.7926. 2.15 0.99 2.23 1.03 2.53 0.8627. 2.18 1.04 2.21 1.03 2.56 0.8428. 2.03 0.99 1.80 0.82 2.59 0.94
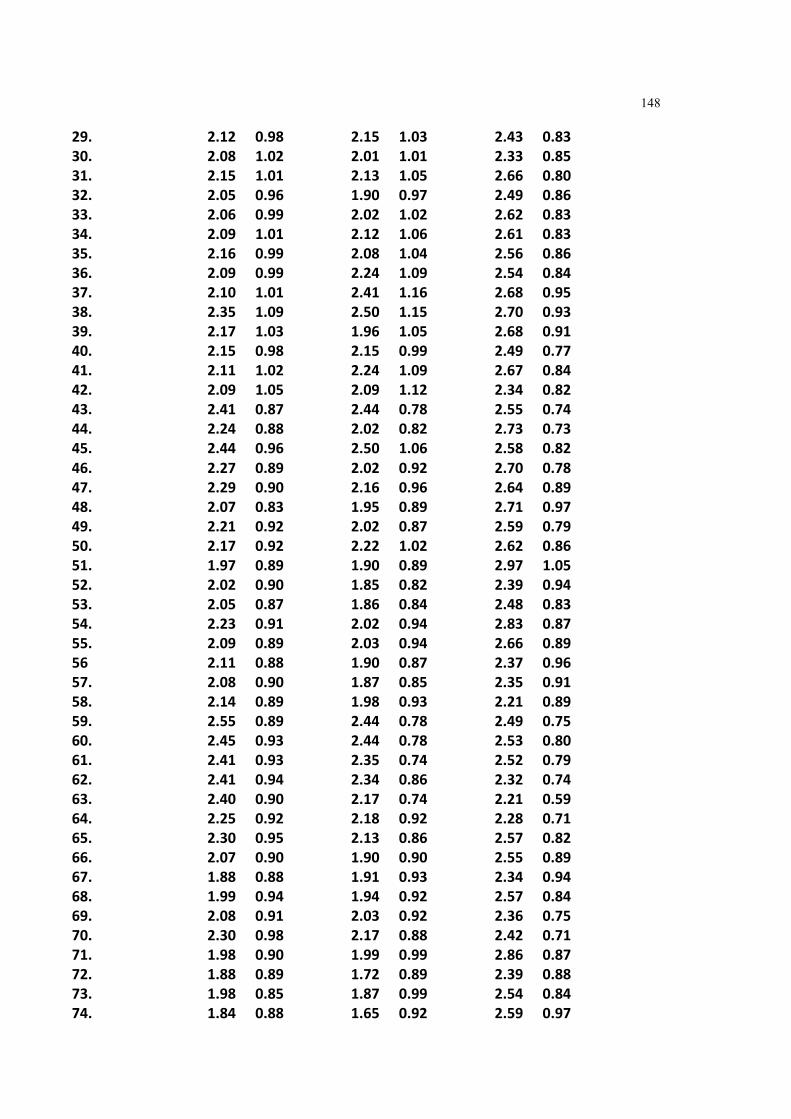
148
29. 2.12 0.98 2.15 1.03 2.43 0.8330. 2.08 1.02 2.01 1.01 2.33 0.8531. 2.15 1.01 2.13 1.05 2.66 0.8032. 2.05 0.96 1.90 0.97 2.49 0.8633. 2.06 0.99 2.02 1.02 2.62 0.8334. 2.09 1.01 2.12 1.06 2.61 0.8335. 2.16 0.99 2.08 1.04 2.56 0.8636. 2.09 0.99 2.24 1.09 2.54 0.8437. 2.10 1.01 2.41 1.16 2.68 0.9538. 2.35 1.09 2.50 1.15 2.70 0.9339. 2.17 1.03 1.96 1.05 2.68 0.9140. 2.15 0.98 2.15 0.99 2.49 0.7741. 2.11 1.02 2.24 1.09 2.67 0.8442. 2.09 1.05 2.09 1.12 2.34 0.8243. 2.41 0.87 2.44 0.78 2.55 0.7444. 2.24 0.88 2.02 0.82 2.73 0.7345. 2.44 0.96 2.50 1.06 2.58 0.8246. 2.27 0.89 2.02 0.92 2.70 0.7847. 2.29 0.90 2.16 0.96 2.64 0.8948. 2.07 0.83 1.95 0.89 2.71 0.9749. 2.21 0.92 2.02 0.87 2.59 0.7950. 2.17 0.92 2.22 1.02 2.62 0.8651. 1.97 0.89 1.90 0.89 2.97 1.0552. 2.02 0.90 1.85 0.82 2.39 0.9453. 2.05 0.87 1.86 0.84 2.48 0.8354. 2.23 0.91 2.02 0.94 2.83 0.8755. 2.09 0.89 2.03 0.94 2.66 0.8956 2.11 0.88 1.90 0.87 2.37 0.9657. 2.08 0.90 1.87 0.85 2.35 0.9158. 2.14 0.89 1.98 0.93 2.21 0.8959. 2.55 0.89 2.44 0.78 2.49 0.7560. 2.45 0.93 2.44 0.78 2.53 0.8061. 2.41 0.93 2.35 0.74 2.52 0.7962. 2.41 0.94 2.34 0.86 2.32 0.7463. 2.40 0.90 2.17 0.74 2.21 0.5964. 2.25 0.92 2.18 0.92 2.28 0.7165. 2.30 0.95 2.13 0.86 2.57 0.8266. 2.07 0.90 1.90 0.90 2.55 0.8967. 1.88 0.88 1.91 0.93 2.34 0.9468. 1.99 0.94 1.94 0.92 2.57 0.8469. 2.08 0.91 2.03 0.92 2.36 0.7570. 2.30 0.98 2.17 0.88 2.42 0.7171. 1.98 0.90 1.99 0.99 2.86 0.8772. 1.88 0.89 1.72 0.89 2.39 0.8873. 1.98 0.85 1.87 0.99 2.54 0.8474. 1.84 0.88 1.65 0.92 2.59 0.97

149
75. 1.89 0.93 1.72 0.96 3.11 1.0276. 2.05 0.94 1.91 0.95 2.35 0.8077. 2.08 0.92 2.09 1.02 2.42 0.7978. 1.89 0.91 1.75 0.95 2.48 0.9579. 2.08 0.96 1.82 0.95 2.57 0.8280. 1.80 0.85 1.79 1.00 3.07 1.0481. 1.81 0.90 1.65 0.91 2.62 0.8982. 1.87 0.93 1.67 0.96 3.20 0.9983. 1.79 0.92 1.64 0.95 2.86 0.915.13EXPERIENCESTRESSORSANDLIFECHANGES TheresponseonthemodifiedLESwassubjectedtotheCronbach'scoefficientAlphatest
andareliabilityof0.71wasobtained.Thissuggeststhatthequestionnairehadgood
constructvalidity.
TheLEScontainedanumberofeventswhichsometimesbringsaboutchangeinthelives
ofindividualsexperiencingthemandwhichnecessitatessocialreadjustment.Thesubjects
wereaskedtoindicatethoseeventstheyhadexperiencedwithinthepastyear.TableL
liststhepercentageofsubjectsineachgroupwhohadexperiencedtheseevents.
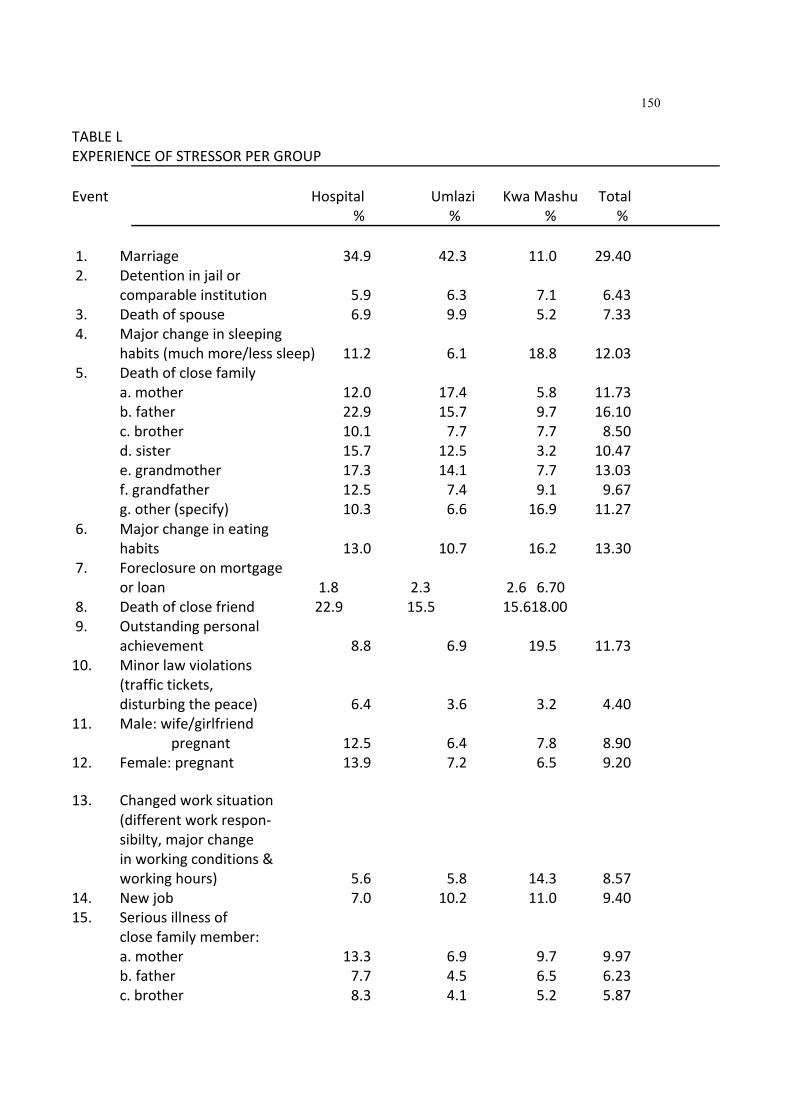
150
TABLEL EXPERIENCEOFSTRESSORPERGROUP Event Hospital Umlazi KwaMashu Total
% % % % 1. Marriage 34.9 42.3 11.0 29.40 2. Detentioninjailor
comparableinstitution 5.9 6.3 7.1 6.43 3. Deathofspouse 6.9 9.9 5.2 7.33 4. Majorchangeinsleeping
habits(muchmore/lesssleep) 11.2 6.1 18.8 12.03 5. Deathofclosefamily
a.mother 12.0 17.4 5.8 11.73 b.father 22.9 15.7 9.7 16.10 c.brother 10.1 7.7 7.7 8.50 d.sister 15.7 12.5 3.2 10.47 e.grandmother 17.3 14.1 7.7 13.03 f.grandfather 12.5 7.4 9.1 9.67 g.other(specify) 10.3 6.6 16.9 11.27
6. Majorchangeineating habits 13.0 10.7 16.2 13.30
7. Foreclosureonmortgage orloan 1.8 2.3 2.6 6.70
8. Deathofclosefriend 22.9 15.5 15.618.00 9. Outstandingpersonal
achievement 8.8 6.9 19.5 11.73 10. Minorlawviolations
(traffictickets, disturbingthepeace) 6.4 3.6 3.2 4.40
11. Male:wife/girlfriend pregnant 12.5 6.4 7.8 8.90
12. Female:pregnant 13.9 7.2 6.5 9.20 13. Changedworksituation
(differentworkrespon‐ sibilty,majorchange inworkingconditions& workinghours) 5.6 5.8 14.3 8.57
14. Newjob 7.0 10.2 11.0 9.40 15. Seriousillnessof
closefamilymember: a.mother 13.3 6.9 9.7 9.97 b.father 7.7 4.5 6.5 6.23 c.brother 8.3 4.1 5.2 5.87

151
d.sister 7.0 5.0 6.5 6.17 e.grandmother 12.7 10.2 7.1 10.00 f.grandfather 5.6 5.3 5.1 5.33 g.other(specify) 3.7 3.0 8.4 5.03 h.spouse 4.0 3.3 7.7 5.00
16. Sexualdifficulties 12.0 5.5 7.7 8.40 17. Troublewithemployer
(indangeroflosing job,beingsuspended, demoted,etc.) 4.0 2.8 4.5 3.77
18. Troublewithin‐laws 8.5 9.4 8.4 8.77 19. Majorchangein
financialstatus(alot offoralotworseoff) 8.0 5.0 24.712.57
20. Majorchangein closenessoffamily members(increasedor decreasedcloseness). 14.9 11.6 26.0 17.5
21. Gaininganewfamily member(throughbirth, adoptionorfamily membermovingin) 21.0 23.7 21.4 20.03
22. Changeofresidence 24.2 22.1 23.3 23.20 23. Maritalseparation
frommate(dueto conflict) 2.1 2.7 1.9 2.23
24. Majorchangeinchurch activities(increased ordecreased attendance) 4.5 2.8 6.5 4.60
25. Maritalreconciliation withmate 8.3 3.9 4.5 5.57
26. Majorchangewithnumber
ofargumentswithspouse (alotmoreoralot lessarguments) 4.0 1.7 3.8 3.17
27. Marriedmale:Changein wife'sworkoutsidethe home(beginning/in‐ ceasingwork,changing tonewjobetc.) 1.3 0.6 5.2 2.30
28. Marriedfemale:Changein husband'swork(lossof job,beginningnewjob,

152
retirement,etc.) 4.0 2.0 5.2 3.73 29. Majorchangeinusual
typeand/oramountof recreation 5.6 3.1 6.4 5.03
30. Borrowingmorethan R10000(buyinghome, business,etc.) 3.2 4.1 14.97.40
31. Borrowinglessthan R10000(buyingcar, TV,gettingschool loan,etc.) 3.5 3.0 12.7 6.40
32. Beingfiredfromjob 6.4 3.3 4.5 4.73 33. Male:Wife/girlfriend
havingabortion 3.2 1.1 1.9 2.07 34. Female:Havingabortion 7.5 1.4 5.8 4.90 35. Majorpersonalillness
orinjury 9.8 4.4 11.0 8.40 36. Majorchangeinsocial
activities,e.g,parties, movies,visiting (increasedordecreased participation) 6.1 1.6 13.0 6.90
37. Majorchangeinliving conditionsoffamily (buildingnewhome, remodelling,deterioration ofhomeorneighbourhood)28.2 17.9 17.521.20
38. Divorce 1.6 1.4 4.5 2.50 39. Seriousinjuryorillness
ofclosefriend 10.9 8.0 13.610.83 40. Retirementfromwork 2.4 1.1 2.6 2.03 41. Sonordaughterleaving
home(duetomarriageor college) 6.7 6.4 5.1 6.07
42. Endingofformalschool 8.0 3.0 11.6 7.53 43. Separationfromspouse
(duetoworkortravel) 6.1 4.7 3.6 14.40 44. Engagement 8.5 2.2 8.4 6.37 45. Breakingupwith
boyfriend/girlfriend 20.2 13.2 9.0 14.13 46. Leavinghomeforthe
firsttime 9.1 5.0 9.7 7.93 47. Reconciliationwith
boyfriend/girlfriend 21.3 13.2 11.6 15.37

153
48. Unrestinyourarea* 26.3 18.3 36.3 26.97 49. Boycotts/strikes/
protest* 16.3 13.0 25.3 18.20 50. Housedamaged/burnt
throughunrest* 9.8 6.7 11.0 8.93 *newitemsaddedtotheoriginalscale
TheimpactoftheselifeexperiencesonthesubjectsarefoundinTableLI.Theminussign
indicatesnegativeimpact.
Thereweresignificantdifferences(chi‐squared)inthewaythegroupsperceivedthe
extentortheimpactofthefollowinglifeexperiences:Marriage(item1)wasregarded
positivelywiththeUmlaziGrouphavingmoreofthisexperiencethantheothergroups
(p<0.0001).TheKwaMashuGroupshadtheleastnumberofmarriages.However,the
subjectsgenerallyfoundthemarriageexperienceapositiveexperience.Engagement(item
44)significantlyoccurredmoreinKwaMashuthantheothergroups(p<0.0317).
Engagementsarealsoseenpositively.Reconciliationwithboyfriendorgirlfriend(item47)
hadagreaterimpactintheHospitalandUmlaziGroupthantheKwaZuluGroup.The
impactofmaritalreconciliation(item25)wasmorepositiveintheHospitalGroup.The
impactofoutstandingpersonalachievement(item9)wassignificantlyhigherintheKwa
MashuGroup.Item9seemedtoofhadapositiveimpactforthesubjectsinthisgroup.
Thesignificantnegativeimpactsweredeathofaspouse(item1);changeinsleepinghabits
(item4);deathofmother,father,sister,grandmotherandotherclosefamily(item5);
seriousillnessofotherclosefamilymemberandspouse(item15);troublewithemployer
(item17);changeinthenumberofargumentswithspouse(item26);changeinhusband's
work(item28);changeintheamountofrecreation(item29);borrowingmorethanR10
000(item31);majorpersonalinjury(item35);majorchangesinlivingconditions(item37)
andunrestinyourarea(item48).

154
TABLELI EXTENTOFIMPACTPERGROUP Event Hospital Umlazi KwaMashu p‐value 1. Marriage 0.73 1.08 0.20 0.0001 2. Detentioninjailor
comparableinstitution ‐0.09 ‐0.11 ‐0.15 NS 3. Deathofspouse ‐0.12 ‐0.26 ‐0.19 0.0542 4. Majorchangeinsleeping
habits(muchmore/lesssleep) ‐0.22 ‐0.09 ‐0.21 0.0390 5. Deathofclosefamily
a.mother ‐0.30 ‐0.51 ‐0.21 0.0033 b.father ‐0.57 ‐0.46 ‐0.27 0.0316 c.brother ‐0.20 ‐0.20 ‐0.26 NS d.sister ‐0.40 ‐0.37 ‐0.10 0.0040 e.grandmother ‐0.48 ‐0.41 ‐0.18 0.0130 f.grandfather ‐0.37 ‐0.22 ‐0.27 NS g.other(specify) ‐0.23 ‐0.19 ‐0.51 0.0004
6. Majorchangeineating
habits ‐0.11 ‐0.05 ‐0.01 NS 7. Foreclosureonmortgage
orloan 0.00 ‐0.06 00.06 NS 8. Deathofclosefriend ‐0.45 ‐0.28 ‐0.31 NS 9. Outstandingpersonal
achievement 0.14 0.20 0.40 0.0085 10. Minorlawviolations
(traffictickets, disturbingthepeace) ‐0.01 ‐0.01 ‐0.03 NS
11. Male:wife/girlfriend pregnant 0.20 0.09 0.10 NS
12. Female:pregnant 0.11 ‐0.01 0.07 NS 13. Changedworksituation
(differentworkrespon‐ sibilty,majorchange inworkingconditions, workinghours) 0.04 0.11 0.04 NS
14. Newjob 0.14 0.18 0.16 NS 15. Seriousillnessof
closefamilymember: a.mother ‐0.30 ‐0.19 ‐0.21 NS b.father ‐0.21 ‐0.13 ‐0.16 NS

155
c.brother ‐0.13 ‐0.12 ‐0.07 NS d.sister ‐0.15 ‐0.13 ‐0.20 NS e.grandmother ‐0.24 ‐0.28 ‐0.14 NS f.grandfather ‐0.12 ‐0.15 ‐0.05 NS g.other(specify) ‐0.06 ‐0.09 ‐0.24 0.0059 h.spouse 0.02 ‐0.09 ‐0.25 0.000
16. Sexualdifficulties ‐0.17 ‐0.14 ‐0.14 NS 17. Troublewithemployer
(indangeroflosing job,beingsuspendedor demoted) ‐0.04 ‐0.07 ‐0.16 0.0668
18. Troublewithin‐laws ‐0.12 ‐0.22 ‐0.21 NS 19. Majorchangein
financialstatus(alot offoralotworseoff) ‐0.07 ‐0.03 ‐0.13 NS
20. Majorchangein closenessoffamily members(increasedor decreasedcloseness). ‐0.01 0.09 0.17 NS
21. Gaininganewfamily member(throughbirth, adoptionorfamily membermovingin) 0.34 0.57 0.49 NS
22. Changeofresidence 0.09 0.13 0.24 NS

156
23. Maritalseparation frommate(dueto conflict) 0.00 0.01 ‐0.06 NS
24. Majorchangeinchurch activities(increased ordecreased attendance) 0.04 0.03 ‐0.01 NS
25. Maritalreconciliation withmate 0.18 0.10 0.06 0.0604
26. Majorchangewithnumber ofargumentswithspouse (alotmoreoralot lessarguments) 0.08 ‐0.00 ‐0.07 0.0052
27. Marriedmale:Changein wife'sworkoutsidethe home(beginning/in‐ ceasingwork,changing tonewjobetc.) 0.00 ‐0.01 ‐0.05 NS
28. Marriedfemale:Changein husband'swork(lossof job,beginningnewjobor retirement) 0.02 ‐0.03 ‐0.12 0.0061
29. Majorchangeinusual typeand/oramountof recreation 0.08 ‐0.02 0.04 0.0403
30. Borrowingmorethan R10000(buyinghome, business,etc.) 0.00 ‐0.04 0.12 0.0136
31. Borrowinglessthan R10000(buyingcar, TV,gettingschool loan) 0.04 0.01 0.00 NS
32. Beingfiredfromjob ‐0.12 ‐0.08 ‐0.10 NS 33. Male:Wife/girlfriend
havingabortion ‐0.04 ‐0.03 ‐0.10 NS 34. Female:Havingabortion ‐0.06 ‐0.04 ‐0.06 NS 35. Majorpersonalillness
orinjury ‐0.13 ‐0.08 ‐0.28 0.0336 36. Majorchangeinsocial
activities,e.g,parties, movies,visiting (increasedordecreased participation) 0.01 0.02 0.12 NS
37. Majorchangeinliving conditionsoffamily

157
(buildingnewhome, remodelling,deterioration ofhomeorneighbourhood) ‐0.19 ‐0.19 0.03 0.0402
38. Divorce 0.01 ‐0.02 ‐0.06 NS 39. Seriousinjuryorillness
ofclosefriend ‐0.28 ‐0.18 ‐0.25 NS 40. Retirementfromwork ‐0.01 0.01 0.04 NS 41. Sonordaughterleaving
home(duetomarriageor college) 0.06 0.12 0.01 NS
42. Endingofformalschool 0.14 0.07 0.19 NS 43. Separationfromspouse
(duetoworkortravel) ‐0.10 ‐0.10 ‐0.08 NS 44. Engagement 0.08 0.02 0.19 0.0317 45. Breakingupwith
boyfriend/girlfriend ‐0.30 ‐0.27 ‐0.13 NS 46. Leavinghomeforthe
firsttime ‐0.03 ‐0.03 ‐0.03 NS 47. Reconciliationwith
boyfriend/girlfriend 0.39 0.27 0.14 0.0326 48. Unrestinyourarea* ‐0.53 ‐0.41 ‐0.83 0.0019 49. Boycotts/strikes/
protest* ‐0.30 ‐0.26 ‐0.34 NS 50. Housedamaged/burnt
throughunrest* ‐0.20 ‐0.19 ‐0.22 NS
*newitemsaddedtotheoriginalscale
Amultivariateanalysisofthetotallifeexperiencesbetweenthegroupsshowasignificant
difference(TableXLII).TheDuncan'smultiplerangetestrevealsthatthedifferenceoccurs
intheUmlaziGroup(TableLII),thatistheUmlaziGroupontheaveragehadsignificantly
lesserlifeexperiencesorchangesthantheothergroups.

158
TABLELII MANOVAOFTOTALLIFEEXPERIENCESBETWEENGROUPS
df SD F p Group 2 15209.03 22.68 0.0001
TABLELIII DUNCAN'SMULTIPLERANGETEST
Duncan's GroupingMean N Group
TotalLifeExperiencesA 49.73 376Hospital
A 47.84 154 KwaMashu B 40.88 362 Umlazi
Amultivariateanalysisofthenegativeandpositivelifeexperiencesbetweengroupsalso
showasignificantdifferencebetweengroups(TablesLIVandLVI).TheDuncan'smultiple
rangetestonnegativeandpositivelifeexperiences(TableLVandLVIIrespectively)reveals
thatthesubjectsintheUmlaziGroupexperiencedtheleastamountofchangecompared
totheothergroups.TheseresultssuggestthatalthoughtheHospitalGroupexperienced
morepositiveandnegativelifeexperiences,itwasnotsignificantlydifferenttotheKwa
MashuGroup.Lifeexperiencesare,therefore,notasingulartriggerfactortohelpseeking
behaviour.
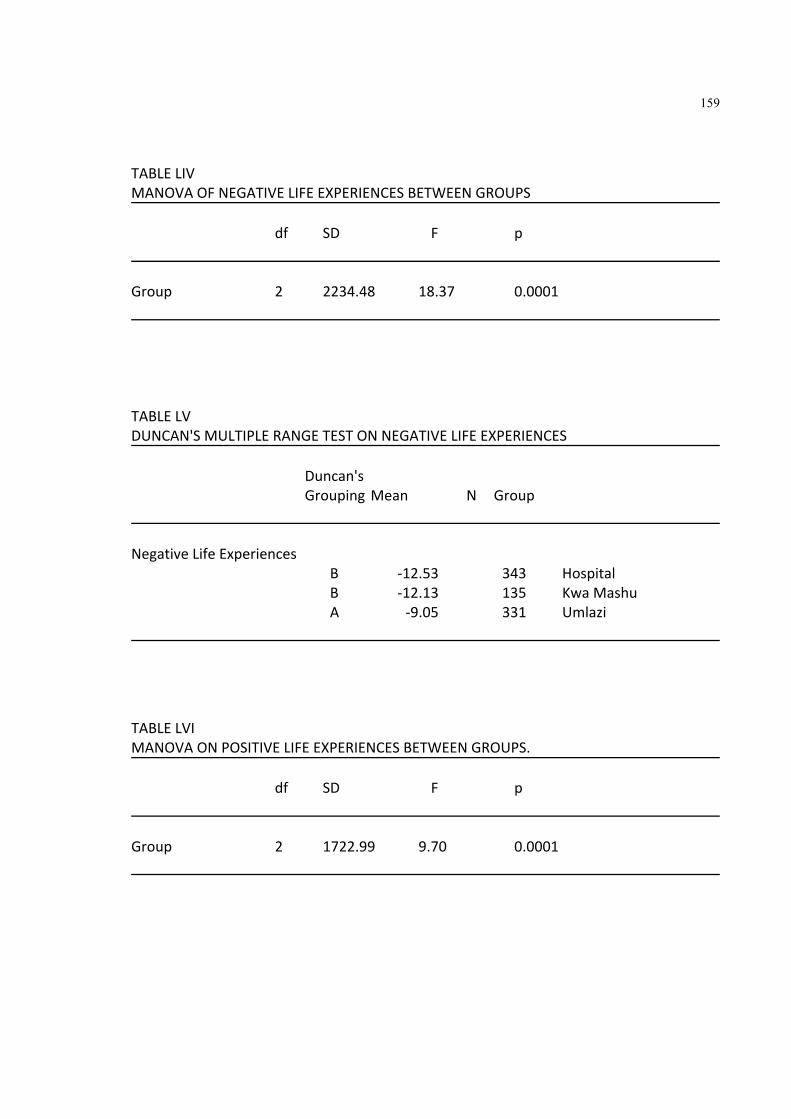
159
TABLELIV MANOVAOFNEGATIVELIFEEXPERIENCESBETWEENGROUPS
df SD F p Group 2 2234.48 18.37 0.0001
TABLELV DUNCAN'SMULTIPLERANGETESTONNEGATIVELIFEEXPERIENCES
Duncan's GroupingMean N Group
NegativeLifeExperiences
B ‐12.53 343 Hospital B ‐12.13 135 KwaMashu A ‐9.05 331 Umlazi
TABLELVI MANOVAONPOSITIVELIFEEXPERIENCESBETWEENGROUPS.
df SD F p Group 2 1722.99 9.70 0.0001

160
TABLELVII DUNCAN'SMULTIPLERANGETESTONPOSITIVELIFEEXPERIENCES
Duncan's Grouping Mean N Group
A 8.76 294 Hospital A 7.87 117 KwaMashu B 5.42 299 Umlazi
Thediscussionoftheseresultsfollowinthenextchapter.

161
CHAPTER6
DISCUSSION
Therewasnosignificantsexoragedifferenceinallthreegroups,althoughtherewere
thirteenpercentmorefemalesthanmalesrepresentedinthesample(TableIand
Figure5).Thisisinkeepingwiththesexratiointhepopulationaccordingtotheofficial
censuscarriedoutin1990.WithregardstotheHospitalGroupthehighernumberof
females(12.76%)iscomparabletootherstudiesonsexdifferencesinhospitalutilisation
whichshowagenerallyhigheruseofmedicalcarefacilitiesbyfemalesthanmales.The
differencesrangefrom30%betweentheages17to44and10to20%over45years
(Nathanson,1977;Verbrugge,1985,1979,Umberson,1992).Themainreasonforhigher
utilisationofmedicalfacilitiesbyfemaleshavebeenattributedbyVerbrugge,(1979)and
HibbardandPope(1983)tothegreaterawarenessamongwomenofsymptoms.
Mostofthesubjectsinthisstudy(90.71%)werebetween20to49yearsold.Itis
interestingthatintheHospitalGroup46.50%werebetweentheages20to29years(Table
III).ThissuggeststhatalmosthalftheAfricanadultpatientsseenatthehospitalareyoung
adults.Thisphenomenonisprobablyrelatedtotheacculturationofthiscommunity,
whereyoungeradultsaremoredisposedtousingmorereadilythemedicalfacilitiesthan
themoreelderlywhostillaremoreinfluencedbythetraditionalideasofillnessand
health.Aswouldbeexpectedthemajorityofthesample(85.09%)wereZulu(TableIV).
TherewasasignificantdifferencebetweenthelevelsofeducationoftheHospitaland
communitygroups(TableV).ThesedifferencesaredepictedinFigure7.Therewasa

162
higherlevelofeducationinthecommunitygroupsthantheHospitalGroup.Ahigher
percentageoftheHospitalGrouphadnoformaleducation(14.10%)orprimaryeducation
(18.88%).Thisdoesnotnecessarilyconflictwiththeavailableliteraturethatsuggeststhat
thereisacorrelationbetweenhighereducationandgreaterutilisationofmedicalfacilities
(Okafor,1983).Thereasonforthisdifferenceisprobablyduetothefactthatthemore
educatedearnbetterand/orareonamedicalaidschemeandmakeuseofprivatehealth
carefacilities.Thosepatientsthatusethestatehospitalsaregenerallythosethatcannot
affordprivatefacilities.
TherewasasignificantdifferencebetweentheHospitalGroupandthecommunitygroup
regardingthenumberofyearsofresidenceinanurbanarea(TableVI).Ahighernumber
ofthesubjectsinthehospitalsamplehadbeenlivinginanurbanareaforlessthan10
years(24.73%)comparedtoUmlazi(10.77%)andKwaMashu(14.95%).Thismaysupport
theviewthatthesubjectsintheHospitalGroupmayhaverecentlymovedintotheurban
areaandthereforemorelikelybeunemployedorwithoutasteadyincome.Theresulting
financialconstraintswouldforcethemtoseektreatmentprovidedbythestatehospitals
whichcostconsiderablyless.
ThesubjectsthatattendedthehospitalwerereferredfromareasthroughoutNatal
(TableVII)althoughthemajorityofthesample(80.31%)wasfromtheareasclosesttothe
hospital.ThereasonsforsuchabroadreferralbaseorcatchmentareaisthatKingEdward
istheonlyteachinghospitalintheprovinceanditisalsoregardedasthehospitalthat
providesthebestserviceforAfricanpeople.Insomeinstances,eventhosethatcanafford
privateservicesprefertoattendKingEdwardtheVIIIHospitalbecauseitisbelievedthat
beingateachinghospital‘specialist’physiciansaremorereadilyavailable.Thisperception
isnotonlyonthepartofthepatientbutisalsofosteredbythelocalclinicswhoreferfor
specialistopinion.Inaddition,thelackofproperlocalfacilitiesfurtherfostersattendance
atthehospital.Krige(1990)pointsoutthatsomeoftheservicesprovidedbylocalclinics
areinadequate;patientsareexpectedtoattendonlyoncertaindays,someservices,such
as,dentalandpsychiatric,arenotprovidedandinsomecasesthedemandforblack
servicescannotbemetandpatientsareturnedaway.

163
However,thefactthatmostofthesampleatthehospitalattendedfromareas,suchas,
UmlaziandKwaMashusupportsthevalidityofcomparisonsbetweensamplesofthe
presentstudysincethesetownshipsarerepresentativeofthecommunityfromwhichthe
HospitalGroupcomes.
Therewasasignificantdifference(p<0.01)intheoccupationsbetweenthethreegroups.
Thesubjectsattendingthehospitalwerefoundtobelessskilledthanthoseinthe
communitygroups(TableVIII).Anoverwhelminglyhighnumberofthesubjectsinthe
hospitalsample(72.34%)wereunskilledcomparedto42.82%intheUmlazigroupand
18.18%intheKwaMashu.Thisagainisinkeepingwiththeviewthatthosewhocannot
affordprivatemedicalhealthfacilitiesorwhodonothavemedicalaidwouldmostlikely
usethestatehealthcarefacilities.Itisalsofoundthat42.60percentofthehospital
samplewereunemployed.Thereareseveralstudiesthatshowthatunemploymenthasa
negativeimpactonanindividualshealth.LeebandRadford(1987a,1987b)andRadford
andLeeb(1986)haveshownthatdismissalfromworkcorrelateswithanxietyanddistress
aftersixmonthswithoutworkandisassociatedwithhelplessnessanddespondency.
Moller(1988)alsohasshownthatunemploymentdirectlyaffectssocio‐psychologicalwell‐
being.
Costs(includingallconstraintsplacedonthepatientsuchastimeorinconvenience)
incurredbypatientshavebeenknowntoaffecttheutilisationoffacilities(Mechanic,
1978).Thepatientsinthisstudyreportedthattheamountpaidintraveltothehospital
rangedfromR1.00toR52.00.Ofcoursetheamountisdependentonthedistancethatthe
patientstravelled.Mostofthepatientsinthestudycamefromareasinandaroundthe
hospital(71.27%)andthereforethecostoftravelonaveragewasR6.27.However,when
oneconsidersthat42.60%wereunemployedandthatthepatientsstillhadtopaya
treatmentfee(minimumofR10.00forthosewithoutincomeandunemployedanda
minimumofR22.50forthoseemployed)thefinancialimplicationsarenotnegligible.In
addition,47.60%hadtotakeoftimeofffromworkinordertoattendthehospitalofwhich

164
23.46%ofthemwillnotbepaid.Fortheseindividualsattendingthehospitalresultsinloss
ofincomeaswell.
Thecostintimevariedgreatlydependingonthedistancetravelled.Somepatientsleft
homeasearlyas2h00toattendthehospital.Theaveragetimespenttravellingtothe
hospitalwasonehourandfortythreeminutes.Inadditiontothetimespenttravellingto
andfromthehospital,timecostsarealsoexperiencedinwaitingfortreatmentatthe
hospital.Althoughthispresentstudydidnotassessthecostoftimeinwaitingfor
treatmentatthehospital,somepatientsdidindicatetheirdispleasurewiththelongdelays
experiencedatthehospital(TableXVIII).Timecostisanimportantfactorsincepatients
leavehomeveryearlyandoftenarrivewellbeforetheMedicalOutpatient'sClinicopens.
Theythereafterwaitinaqueuetobeseenbyadoctor.Afterthisscreeningtheyaremost
oftenreferredtothedispensaryformedicationand/orforspecialinvestigationsand
opinionsfromotherspecialistdepartments.Thisprocesscouldtakethewholeday.
Certainprocedures,forexample,aComputerisedAxialTomography(CAT)Scan,
Electroencephalogram(EEG)orElectrocardiogram(ECG)maynotbeabletobedoneon
thesamedayorinthecaseofotherproceduressuchascertainbloodtestsorlumbar
puncturestheresultsmaynotbeavailablethesameday.Asaresultthepatientmayhave
toreturntothehospitalanotherday.Anotherreasonforpatientshavingtoreturnisthat
sometimesotherdepartmentsinthehospitalmaynotbeabletoseethepatientona
particulardaybecauseoftheirfullclinicprogrammeandgivesthepatientanappointment
foranotherday.Thesefactorsfurtherincreasesthecostforpatients.Accordingto
FitzpatrickandScambler(1984),thosewhoexperiencehighcosts,particularlythrough
lossoftime,beingdependentonpublictransport,orlosewagesfortimetakenofffrom
work,aredemotivatedinseekinghelp.
6.1HELPSEEKINGBEHAVIOUROFHOSPITALSUBJECTS
Thepresentstudyshowsthatthedominantreasonforthechoiceorpreferenceofa
particularmedicalfacilityisthequalityoftheserviceprovided.Inthehospitalsample59%

165
feltthattheservices,facilitiesand/ortreatmentswereverygood,thatthehospitalhad
plentyofdoctorstoattendtotheirneedsandthatthehospitalwasalsowellrecognised
foritsgoodtreatment.Thisviewisconsistentwiththeviewsofthecommunitygroupsas
wellregardingtheirreasonsforthechoiceofservices,suchas,choiceofdoctor,the
choiceofhospitalandthechoiceofapharmacy(seeTablesXI,XIIIandXV).Boththe
communitygroupschooseserviceswhichtheyperceivetobegoodandwhichwere
closesttothem.Coppoetal(1992)havepointedouttheimportanceofunderstandingthe
influencethatdistanceplayonhelp‐seekingbehaviourandcitestudiesthatsuggestthat
thecriticaldistanceisbeyond5kms.
Theotherreasonthatpeopleseekhelporutilizehealthcarefacilitiesarethereferralsby
otherhealthfacilitators,suchas,generalpractitioners(12.00%)andperipheralhospital
andclinics(10.30%)orlayreferrals,suchas,employers,friendsandfamilymembers
(7.00%).Itisinterestingthatthelayreferralsweremadebecausethoseindividualsaswell
believedthatthehospitalprovidedabetterservice.Layreferralswerealsomadeby
employers,friendsandfamily.Suchman(1966)andHouseetal.(1988)haveshownthat
thehealthseekingbehaviourisasocialprocessinvolvingatleastoneotherperson,that
layconsultationinfluencespatternsofhelp‐seekingandthattherewasapreferenceto
consultothers,suchas,thepolice,bystanders,neighboursandfriendsbeforeconsulting
family.
Only2.20%acknowledgedthatthemainreasonforcomingtothisparticularhospitalwas
thatthecostofthetreatmentatthehospitalwasfarlowerthanthatofothermedical
availablefacilities.Ofcoursethecostreferredtohereisthecostoffeesatthehospital
andnotoftime,inconvenienceortransport.Severalstudieshaveshownthatcostisa
crucialdeterminantofhelp‐seekingamongpatients(Lewis,FeinandMechanic,1976;
Mechanic,1986;Mechanic,1992)
Anotherfactorinhelp‐seekingthatisequallyimportanttounderstandiswhatmakesan
individualchooseaparticulartimetoobtaintreatment.Inthisstudy,themajorityofthe
subjectsattendedthehospitalbecausetheybelievedthattheirconditionwas
166
deteriorating(50.34%).Otherreasonsforattendanceonaparticulardaywasavailability
ofappointmentsatthehospital(29.05%);nomoneytoattendearlier(7.77%);
arrangementmadebyotherhealthorganisationsordoctors(7.10%);notime(2.70%)and
notransport(2.4%).Thesefindingsaresignificantsincetheyshowthatthemajorityof
patientswhoseekmedicalhelpmonitortheirstateandonlywhentheybelievethattheir
conditionisgettingoutofcontroldotheyutilisehospitalservices.Hencebarrierssuchas
availabilityofappointments,financialrestraintsandtransportmaypreventtheindividual
fromobtainingmedicalhelpwhentheyactuallybelievetheyneedit.Besidetheundue
stressandanxietythatthiswillcause,itmayevenfurtherdelayaconditionthatshould
havebeenattendedtomuchearlier..Mechanic(1992)hasreportedontheimportanceof
layappraisalofillness,theeffectofvariousbarriers,suchas,money,timeandtransport,
andtherelationshipwiththedoctorininfluencinghelp‐seeking.
Themajorityofthepatients(65.40%)soughthelpfromthehospitalwithinamonthof
suspectingtheywereill.Thisagainsupportstheviewthatindividualsallowaperiodof
timeforselfassessmentbeforeseekingmedicalhelp.Accordingtoourfindingsthisperiod
forselfassessmentismostlikelytotakeplacewithin5.85weeksofthefirstsuspicionof
illness.TableIXandFigure9provideabreakdownofthetimetakenfromthefirst
perceptionsofillnessandtheactualattendanceatahospital.Wecaninferfromthese
resultsthatfollowingself‐assessmentmostindividualswillseekhelpwithinsixweeksof
firstexperiencingtheirsymptoms.
Themostcommonreasongivenbythesubjects(43.50%)fornotattendingearlieror
immediatelyfollowingtheirfirstperceptionsofanillnessisthattheyfeltthattheillness
wasnotseriousenoughtowarrantmedicalhelpseeking,thattheywerenotbotheredby
thesymptoms.Somedidnotattendearlierbecausetheyhadalreadysoughtmedicalhelp
fromageneralpractitioner(19.90%),hadnomoneytoattendthehospital(14.80%),
treatedthemselvesbypurchasingmedicinesfromapharmacy(2.20%),hadnotransport
(1.90%)andbeingtooilltoattend(1.60%).Asmallpercentage(1.90%)wantedtoattend
earlierbutcouldnotgetanearlierappointment.Thesubject'sresponsesforattending

167
earlierareconsistentwiththeearlierresponseswhichendorsetheimportanceofthe
patientsself‐assessmentoftheseriousnessoftheirsymptomswhichprecipitatesmedical
helpseekingbehaviour.Theirresponsesalsoendorsetheseekingofotherservicesbefore
theiruseofthehospital.Pharmaciesandgeneralpractitionersarealsosoughtafterfor
medicalhelp.Forthosewhofeeltheyhavemadenoimprovementhelpissoughtfromthe
hospital.Similarcircumstanceshavebeenfoundtoinfluenceothersocietiesregarding
decision‐makinginhelp‐seekingandtreatmentchoice(Garbo,1986;Good,1986).
Anotherimportantfactortounderstandinmedicalhelpseekingbehaviourconcernsthe
feelingsandexperiencesthatindividualshaveaboutillness.Thesefeelingsand
experiencesarereferredtoassymptomsbymedicalcareproviders.Accordingtothe
respondents63.30%feltthattheywereillbecausetheyexperiencedonlyphysical
symptomswhile20.80%experiencedonlypsychologicalsymptoms.Aboutseventy‐nine
percenthadexperiencedacombinationofphysicalandpsychologicalsymptoms.Itis
interestingthatsubjectsareabletoassociatepsychologicalsymptomswithindicationsof
illness.ItiscommonlybelievedthatAfricanpatientsusuallypresentwithphysical
symptomsandveryrarelypresentwithpsychologicalsymptoms.Apossiblereasonforthis
isthattheymaynothavethepsychologicalvocabularytoreportsuchsymptoms.Another
reasonisthatpatientsreportingpsychologicalsymptomsmaynotbetakenseriouslyand
theirpresentationmaybediscreditedasafactitiousdisorderormalingering.Thelatteris
verylikelytohappeninovercrowded,busyhospitalslikethoseprovidingcareforthe
disenfranchisedinSouthAfrica.Thefailuretotakepsychologicalsymptomatology
seriouslyis,therefore,averycommonphenomenon((Eisenberg,1986;Kellner,1986;
Mayou,1986;Pilowsky,1986).
Themajorityofsubjects(87.00%)wereconcernedorworriedabouttheirsymptomsyet
46.20%didnotknowwhatwaswrongwiththem.However,someattributedtheir
symptomstoainfluenza(13.40%),aformofinfection(12.50%)oraterminalillness
(8.10%).Otherlaydiagnoseswerealsosuggest,suchas,'somethingwrongwiththe
blood',thebladderdirtyandwaterinthehead(5.30%).Culturaldiagnosesofsymptoms
arealsomadeandtheseincludetheworkofthetraditionalhealers,crossingapathwhere

168
someritualwasperformed,inhalingofabadspiritandbeingpoisoned(3.70%).This
seemstosuggestthatalthoughpatientsareabletoperceivesymptomstheyareunableto
accuratelyascribethesefeelingandexperiencestoaparticularcondition.Itisprobably
moretheanxietyexperiencedinordertointerpretthesesymptomsthatprecipitateshelp
seekingbehaviourratherthanthebeliefthattheyhaveaparticulardisorder.Itis,
however,interestingthetypesoflaydiagnosesmade.Thereisanemphasisonorgansor
systemsbeingdirty.Duetothisbeliefitisnotsurprisingthatdetergentsareusedasa
formoftreatment.Acaseinpointisaparasuicide,21years,whichwasreferredfora
psychologicalevaluationfollowinganoverdoseofvinegarandjeyesfluid(cattledip).It
hadbecomesubsequentlyevidentthatthepatienthadnottakenanoverdosebut
believedthatshewaspoisonedbyoneofhercolleagueswhohadgivenhersomefoodto
eatandshehadsubsequentlyfainted.Whenshewasbroughthome,theneighboursand
familygaveherthesesubstancesinordertowashoutthepoison.Theconsequenceof
suchbeliefs,however,mayhavedisastrouseffects.Hereagainweseetheinfluencesof
cultureinattributingmeaningtosymptomsandremainsacrucialdeterminantinhelp‐
seeking.(FreemanandMotsei,1992;SultanaandHunte,1992).
Thereisevidenceofahighlevelofselfdisclosurebypatientsabouttheirsymptoms.
Eighty‐sixpercentreportedthattheydiscussedtheirsymptomswithothers.Mothersand
spousesaremostoftenconfidedin.Itwouldappearthenthesuggestionsand
recommendationsmadebytheseindividualsplayanimportantpartinthedecisionofthe
patientstoseekappropriatehelp.Suchman(1966)andHouseetal.(1988)haveshown
thattheseekingofhealthbehaviourisasocialprocessinvolvingatleastoneotherperson
andthatlayconsultationinfluencespatternsofhelp‐seeking.Peoplemostlikelytobe
consultedarefamily,neighboursandfriends.
6.2USEOFSERVICESBYCOMMUNITYGROUPS

169
Patientsmostoftenchosedoctorsthatweresituatedorlocatednearesttothem(TableX).
Theirmainreasonsforchoosingadoctorwereproximityandthequalityofservice(Table
XI).Asimilarpatternemergedforthechoiceofanhospitalorapharmacy.Subjectschose
toattendthehospitalclosesttothem,forexamplethesubjectsinUmlazichosePrince
MshiyeniMemorialHospital(42.50%)andKingEdwardVIIIHospital(35.30%)andthose
fromKwaMashuchoseKingEdwardVIIIHospital(58.40%).Apossiblereasonforahigher
numberfromUmlazinotattendingPrinceMshiyeniMemorialHospital(whichisinUmlazi)
isthepoliticalaffiliationofthesubjects.ItisgenerallyfeltthatthoseinUmlazihavean
affiliationtotheANCandthatthePrinceMshiyeniMemorialHospitalisadministratedby
theKwaZulugovernmentwhichisaffiliatedtotheIFP.HenceANCsupporterswouldavoid
theuseofsuchahospital.Thisdistrustofmedicalcaresystemshavealsobeenfound
amongstminoritygroupselsewhere,suchas,Jews,PuertoRicansandBlacksintheUSA
(Geertsen,etal.1975;Lendt,1960).
Theresponsesgleanedsuggeststhatthequalityoftheserviceandconvenienceoflocation
playaconsiderablepartintheutilizationofhealthservicesandfacilities.Itis,therefore,
importantthattheseservicesbelocatedwithinthecommunitiestheyareintendedto
serve.Thisisanoverhangofthepoliticalsystemofthecountrywhichprovidedracially
segregatedservicesandwhichnotonlyprovidedinferiorservicesfortheBlackbutalso
relocatedorreservedresidentialareasforthemawayfrombasicandessentialfacilities.As
aresultindividualshavehadtoovercomethesesocio‐economicbarriersinordertoseek
medicalhelpwhichhasdirectlyinfluencedhelp‐seekingbehaviour.Inthisregard,oneof
thehospitalsample'sreasongivenfornotattendingearlier“becausetheydidnotthink
thattheirillnesswasseriousenough”couldalsomeanthattheindividualhadtodecide
whethertheillnesswasseriousenoughtowarrantovercomingthebarriersofdistance
andcost.Lewis,FeinandMechanic(1976)andMechanic(1986)haveemphasized
especiallytheimportanceofaccessibilityofmedicalservicesinhelp‐seeking.
Mostsubjectswerepleasedwiththemedicaltreatmentreceivedfromtheirdoctorsorthe
hospitalstheyattended(TableXVI).However,agreaternumberofthecommunitygroups
werepleasedwiththetreatment(Umlazi83.9%andKwaMashu84.7%),thantheHospital

170
Group(53.2%).Thegreatersatisfactionexpressedbythecommunitygroupswould
probablybeduetotheirabilitytochooseprivatedoctorsandclinicsfortheirtreatment
wherethefacilitiesarebetter,moreaccessibleanddonothavetowaitlongfor
treatment.Hospitalsubjects,ontheotherhand,havenoalternativebuttoacceptthe
servicetheyobtainfromtheovercrowdedstatehospitals.Thewriterdailyobserves
patientsattendingtheKingEdwardVIIIHospitalandspendthewholedaywaitingwithout
grumblingorexpressinganydissatisfactioninordertobetreated.Thesepatientsmost
oftenbelievethattheserviceatthehospitalisaprivilegeandthattheyarenotallowedto
complainorbeassertive.
Thefactorsthatsubjectsusetoassesstheirsatisfactionoftreatmentisthequalityofthe
serviceandcaregiven,andthecuretheyhavehad.Afewassessedtheirsatisfactionby
themethodoftreatment(TableXVII).TableXVIIIliststheaspectsoftreatmentthat
subjectswerenotpleasedwith.Theseincludethequalityofthedoctor‐patient
relationship,thequalityofthefacilities,thetimespenttoobtaintreatment,the
ineffectivenessofthetreatmentandthecostincurred.Itisinterestingthatthecommunity
samplesexpressedmoredissatisfactionwiththequalityofthedoctorpatientrelationship,
thequalitywiththefacilities,timeandcostthanthehospitalsample.Thereasonforthisis
thatthecommunitysamplehaveachoiceofprivatetreatmentandthereforeexpectthe
treatmenttobeofanacceptablestandard.Thehospitalsample,ontheotherhand,
expecttheselimitationsatthestatehospitalbecauseofovercrowdingandover‐utilization
ofthelimitedservicesavailable.Itwouldseemthatchoiceofservicesplaysanimportant
partinpatientsatisfaction.Inaddition,ifpeoplehaveachoicetheywillalsodemand
betterservices.ThisisseenintheresponsebytheHospitalGroupwhoexpressed
dissatisfactionwiththebenefitsofthetreatmentreceived.Inotherwords,peoplewhodo
nothavethechoiceareunabletodemandabetterserviceandhencetheservice
providersarenotpressurizedtoprovideabetterservice.
Awaytorectifythissituationisthathealthshouldbearighttoall,thatpatientsbe
allowedchoiceofservicesandthatthepeoplebeempoweredandeducatedsothatthey
willbeabletodemandareasonablygoodhealthcareandservice.Thiswillalsoleadtoan
171
improvementinthehealthservicesprovidedbytheState.However,areasonforapoor
serviceatthestatehospitalsisthelimitedservicesandbudgetsavailablewhichinturn
leadstoover‐utilisationofcertainstatehospitals.Forexample,inSouthAfricathe
provinceofNatalhasalwaysbeengivenaconsiderablylowerhealthbudgetthanthe
otherprovincesinthecountry.WhileKingEdwardVIIIHospitalhasbeenover‐utilisedand
overcrowded,frequentlyrequiringtheneedforfloorbeds,GreysHospital(constructedfor
whitepatients)hasalwaysbeenunder‐utilised.Againthisimbalancewascreatedbythe
previouspoliticalpolicyofthecountryandpresentpoliticalreforms,itishoped,will
addressthesefundamentalproblemsofinequalityinordertoimprovebothhealthand
illnessbehavioursincethesedirectlyaffectthehealthstatusofthewholesociety.
Mostinterviewees,however,reportedthattheywouldseekmedicaltreatmentinthe
future(92.2%).Thisindicatesthattheurbanpopulationhavecometoseeandacceptthe
needtoobtainmedicaltreatment.Asmallpercentagedidnotwantto(3.1%)orwerenot
sure(4.7%).Itisprobablythissmallgroupthatwouldseekalternateformsoftreatments.
Obviouslytheseindividualsarenottotallyconvincedthatwesternmedicineworks.Such
beliefsmayhavealsoresultedeitherfromtheirnegativeexperiencesofmedical
treatment/sortheirnotexperiencinganybenefitsfromsuchtreatmentsbesidestheir
possibledistrustofwesternmedicine.
Theuseofmedicationisanimportantissuepresentlybecauseofthewidespreadmisuse
orabusethattakesplace.Ofsignificanceisthemisuseofmedicationinsuicidalbehaviour,
agrowingproblemintheAfricancommunity(Schlebusch,1988;Pillay,Naidoo,Tlou,
1992).TableXIXliststhesourcesfromwhichsubjectsobtainedtheirmedication.Most
subjectsobtaintheirmedicationfromprivatedoctors,clinicsorhospitals.Littleself‐
prescribingtakesplace.Self‐medicatingoccurredamong5.1%becausetheyfelttheyhad
thefluand7.7%becausetheyexperiencedpain.Theseresultssuggestaloweruseofover‐
the‐counterdrugsthaninotherpopulations(Schlebusch,1988).However,because
medicationisobtainedfrommedicalpractitionersitisimportantthatthesedoctors
prescriberesponsiblyandeducatepatientsabouttheproperuseofmedications.Since
thesecommunitiesseemnottorelyheavilyonmedication,afactoralsoseeninpatient's

172
dissatisfactionoftreatmentweretheresponse‘nomedication’featuredlow,proper
prescriptionwillalsoteachappropriatemedicatingbehaviour.Thisisimportantsinceonly
40.4%understoodwhytheyweretakingmedicines.Whereas46.8%tookmedication
becauseitwasprescribedwithoutunderstandingthenatureoftheillness.
Therewasasignificantdifference(p=<0,01)inthewaythehospitalandcommunitygroups
respondedtotheperceivedbenefitsofwesternmedicines(TableXX).MoreofHospital
Groupfoundthemlessbeneficialorwerenotsureabouttheirefficacy.Therecouldbe
severalreasonsforthisdiscrepancy.Itisveryunlikelythatthisistheresultofthequality
ofmedicationsbeingusedbythehospitals,sincethestandardofmedicationisequally
goodalthoughthehospitalstendtousegenericmedicationbecauseofthecostof
recognisedtradenamemedicinesThemostlikelyreasonsare,inaccuratemedicationuse
and/ornon‐compliancewiththeprescribedtreatment.Thiscouldbetheresultof
patientsnotbeinggivenproperexplanationsabouttheirillnesses(46.8%didnot
understandwhytheyweretakingmedication),notbeinggivenproperinstructionsonhow
totakethemedication(thewriterhasseennumerouspatientswhohavetaken
suppositoriesorally;vaginalsuppositoriesrectally;eardropsorallyorpatients,whohave
takentabletsprescribedthreetimesdailyonlythreetimes).
Poordoctor‐patientrelationships,sideeffectsofthemedicationandculturalandlanguage
differencesarekeycontributingfactorstothesekindsofmisinterpretations.Thelarge
numbersseenatthehospitals,overcrowding,inabilitytospeakthepatient'slanguage,
lackofunderstandingofthepatient'sperceptionsofillness,orthepatient'sunderstanding
ofillness,andtimeconstraintsdirectlyinfluencethequalityofinstructionandinformation
providedbymedicalpersonnel.Newmethodsofprovidingsuchinformationshouldbe
considered.Thesecouldincludeaudioandvideoeducationwhilepatientsarewaitingat
thehospitals;printedinstructioninAfricanlanguageswiththeuseofstepbystep
graphicalillustrationsotheilliteratewillalsobeabletounderstand;medicalpersonnel
learningthelanguageofthepeopleoremployingskilledinterpreterstodisseminate
information;theestablishmentofinformationcentreserectedinconvenientspots,
mannedbyindividualswhocanspeakthelanguageofthepeopleandarefamiliarwiththe
cultureofthepeople,wherepatientscanobtaininformationandhelpwithoutfeeling

173
intimidated.Implementationofsuchserviceswilltaketheloadoffdoctorsandnurses,
helpimprovecomplianceandlowertheincidenceofpsychologicalproblemsrelatingto
healthandillnessbehaviour.
Theuseofvitaminssupplementsdifferedbetweenthegroups(TableXXI):55.70%ofthe
KwaMashugroupand40.40%oftheUmlazigroupusedsupplements.Thevitamin
supplementswereusedmainlyto'increasestrength',cureortreatanillness,makeone
activeorserveaprotectivefunction.Somealsotookvitaminsupplementsto'strengthen
theblood'orontheadviseofnon‐medicalpersons.Thereisahigheruseofvitamin
supplementsthanmedicines.Thisneedtousesuchsupplementsmaybetheresultofthe
aggressivemediaadvertisementswhichpromotetheuseofvitaminsupplementsaspart
ofthehealth,dietandexercisefadpresentlyinvogue.
Intheearlierchapterstheimportanceofreligiousandculturalbeliefsandtheir
relationshiptohealthbeliefswerediscussed.Ahighpercentageofthesubjects(89.2%)
wereChristian,2,8%belongedtoAfricanreligiousgroupswhile1.4%saidtheybelongedto
bothChristianandtraditionalAfricanreligions.Itisimportant,howevertonotethatthe
largenumberthatclaimedtobeChristianincludesthosethatbelongtoAfrican
independentchurchesaswell.Thesechurches,forexampletheShembeChurch,
integratesbothAfricantraditionsandcultureswiththeChristianfaith.
Mostofthesubjectsdenieduseoftraditionalmedicinesorhealers(55.37%).Subjectsin
thehospitalandUmlazigroupstendtodenytheuseofthesemethodsthanwasthecase
inKwaMashu.Apossibleexplanationforthisisthatgreateracculturationhasprobably
takenplaceamongthethoseattendingthehospitalandintheUmlaziCommunity.Faith
healersareusedmoreoftenthantraditionalhealers.Thisistobeexpectedsinceitwould
bemoreinkeepingwiththerereligiousbeliefs.Wessels(1987,1989)toofoundthatfaith
healerswerebecomingincreasinglypopularintheAfricancommunity.Ourfindingsarein
keepingwithWessels(1987b,1989)studies,regardingthecombinationofmethodsused
inthetreatmentofpatientsbyfaithhealers.Holywaterandherbsareusedmoreoften
thanprayer.Prayerisusuallyobtainedfromwomanprayergroups,family,friendsand

174
neighbours(TableXXVIII).AhighernumberintheKwaMashugrouprespondedthatthey
hadusedprayerasamethodoftreatmentfortheirillness.
Ontheaverage,thesubjectsfrequentedtraditionalhealersthreetimesandthereafter
theirattendanceoffaithhealingdeclined(TableXXIV).Thisisoddbecausetherewas
generalconsensusamongthosethatsoughtsuchtreatmentthatthetraditionalhealing
washelpful(60.9%).Infactmoreinthecommunityperceivedthiskindoftreatmentto
bebeneficialthanthosewhoattendedthehospital.Apossiblereasonforthisdeclineis
eitheracculturationoranawarenessthatconsultingtraditionalhealersisnotregardedas
acceptablebehaviourandasaresultthereisareluctancetoreportsuchbeliefs.
Ontheaverage21.00%reportedconsultinganherbalist.Itwouldappearfromtheresults
thatsubjectsinthecommunityconsultedherbalistmoreoftenthanthosewhoattendthe
hospitals(TableXXIX).Apossiblereasonforthisisthatthosewhoattendthehospitalmay
haveagreaterbeliefintheefficacyinwesternmedicinesoralternativelybelievethatthe
illnessrequiresmedicalintervention.
Nevertheless,itisimportanttobearinmindthatahighpercentage(60.9%)dobelievein
theefficacyoftraditionaltreatmentandasignificantnumber(23.3%)wereambiguous
aboutitsefficacy.Inaddition,47.40%indicatedthattheywillcontinuewithtraditional
treatments(TableXXVII).Thissuggestthattraditionaltreatmentwillstillbesoughtand
thataconsiderableamountofhealthbehaviourtakesplaceoutsideofthemedicalsystem.
Thereforethissituationhastobecarefullyconsideredwhenplanningandprovidinghealth
servicestourbanAfricans.Failuretoacknowledgetheirunderstandingandbeliefsin
traditionalhealerswillresultinadualistapproachtothetreatmentoftheirillness.
Individualswillusemedicalservicesbutwillprobablyalsosecretlyattendtraditional
healers.Thefearofappearingignorantorprimitiveiftheyexpressadesiretosee
traditionalhealersmayleadtoadelayinhelp‐seekingbehaviourandmaybe
counterproductiveifdoctorsarenotawareofothertreatmentspatientsmaybetakingor,
especially,iftheyareaskedtostopmedicaltreatmentbytraditionalorreligioushealers.
Theauthorhasseenseveralcaseswerepatientshavebeenaskedbyreligioushealersto

175
stoptakingmedicationbecausetheirtakingofmedicationindicatesalackoffaithinGod
tohealthem.Therehavealsobeenothercaseswherepatientshavebeengivenherbsand
othersubstances,suchas,intelezi,thathavevariouspsychological,psychiatricand
physicalsymptoms.Ifpatientsdonotfeelcomfortablesharingtheirbeliefsabout
traditionalandreligiousmethodsoftreatment,thedoctorwillnotbeabletoassistthe
patientpromptlyorefficiently.Ifpatientsdonotfeelthatthedoctorunderstandstheir
beliefsorthattheirbeliefswillbefrowneduponandridiculed,thepatientwillnotshare
thisinformationandthiswillleadtonon‐compliancewithtreatmentsprescribedbythe
doctor.
Subjectsalsoreportedtheuseofseverallayorfolkmedicines(TableXXIX).Laxativesor
purgativeareusedveryfrequently(88%).Warmwaterorseawaterisoftenusedto
inducevomiting.AreasonforthisisthatthereisbeliefamongAfricansinthecleaningof
thebodyanditssystems.Thebeliefisthateithertheorgansaredirty,thebloodnotclean
orthatsomethingpoisonoushasbeeningested.However,thedangersoftheuseof
purgativesuchasepsomsalts,castoroilandotherlaxativehavebeenfrequentlyobserved
inblackhospitals.Thecaseofthe21yearoldparasuicidecitedearlierdemonstratesbelief
thatcleansingisneeded.‘Strengtheningmedicines’areespeciallypopularbecausethey
protecttheindividualfromvariousomens(Wessels,1989).
6.3HEALTHANDILLNESSBELIEFS(QUALITATIVE)
Thesubjectsusedavarietyofsymptomsorlackofsymptomsandfeelingstoexplaintheir
understandingandmeaningofbeingillorwell(TableXXXI,XXXII,XXXIIIandXXXIV).In
mostcasesbeingillmeansthatonedoesnotfeelgoodorwellphysicallyand
psychologically,i.e.onedoesnotfeelnormal,isworried,feelsuncomfortableandnot
relaxed.Associatedwiththisispain.ItisworthnotingthatpainratedlowerintheHospital
Group(15.7%)thanthecommunitygroups(32%and39%).Thisprobablyisaresultof

176
desensitisationtopainorthatthoseattendthehospitalbearpainstoically.Hencetheydo
notusepainasasignofillnessbutrathergeneralwellbeing.
Illnessisalsoassociatedwithbeingineffectiveorbeingunproductive,havingadysphoric
mood,lookingillphysically,psycho‐motorretardation,symptomaticandbeing
dependent.Sleepandappetiteareusedtoassessillnessaswell.
‘Wellness’isconsideredtheoppositeofthe‘ill’condition.Anindividualwhoiswellis
expectedtofeelgoodandnormalbothphysicallyandpsychologically.Hisorhermoodis
expectedtobeelated,painfree,productiveandefficient,lively,active,lookinggood
physicallyorhealthyasymptomaticandindependent.Thisviewofhealthandillnessis
similartothoseinotherculturesaswell;forexample,Diaz‐Guerrero(1984)studywhich
includedthirtydifferentcultures.Thereiscross‐culturalagreementthathealthis
characterisedas“good”,“potent”and“active”(Diaz‐Guerrero,1984).However,hedoes
pointoutthatadjectivesvaryfromoneculturetoanother.
Itisveryclearfromtheresponsesofthoseinterviewedthattheyadoptaholisticconcept
ofhealthandillness.Thisisveryimportantsincethereisastrongmovementinwestern
medicineaswelltoadoptanholisticapproachtohealthandillnessespeciallyinviewof
thedichotomousrelationbetweenthemindandbodyassumedbythemedicalmodel
(Engel,1977;Engel,1980;Schlebusch,1990).Ifhealthworkersdonotrecogniseand
promotethisholisticconceptthattheAfricanpossessthentheyruntheriskofteaching
themanarrowviewofillnessandhealthoutofkeepingwiththeirtraditionalworld‐view
whichlastsbeyondseveralgenerationsofacculturation.Unfortunately,theover‐
utilisationofservices,lackoffacilities,overcrowdingandtimeconstrainsandpoordoctor‐
patientcaremayactuallypromoteabiologicalmodelofillnesswhichmayhavetobe
unlearnedlater.Further,doctorswillhavetounderstandandtreatAfricanpeople
holistically,otherwisetheirpatientswillnotcomplywiththetreatmentsprescribed.
Theholisticunderstandingofhealthandillnessisalsoseeninthereasonsprovidedbythe
subjectswhypeoplegetsick(TableXXXV).Themostprominentreasonsarepoornutrition
anddiets;socialstresssuchaspoorlivingconditions,poverty,infectionanddiseases,

177
alcoholandsubstanceabuses;psychologicalstress;environmentalstress,suchas,
violence,warunrestandoccupationalstresses;inheritedillnesses;bodymalfunctioningor
atrophy;preventativemeasures,suchas,checkups;andtraditionalideas,suchas,
bewitchment,badtermswithneighboursandfamily,seasonalandweatherchanges,and
dirtyorgans.
Althoughallgroupsindicatedthattheywouldgotoadoctor,someoftheillness
behaviourssignificantlyvariedamongthegroups;.Thesewereforhospitalattendance
(p=<0.05),useofapharmacy(p=<0.01),useofprayer(p=<0.05),denial(p=<0.01),self
medication(p=<0.01)andreadingaboutillnesses(p=<0.01).TheKwaMashugroupwas
lesslikelytoattendthehospitalthantheothergroupsbutmorelikelythantheother
groupstogotoapharmacy,self‐medicateordenytheillness.Thisisprobablytheresultof
therenotbeingahospitalnearKwaMashuwhereasUmlazihasthePrinceMshiyeni
MemorialHospital,theKingEdwardVIIIandClairwoodHospitalscloseby.Thisagain
endorsestheviewthatthelackoffacilitiesforceindividualstoseekalternateillness
behaviours.Further,theHospitalGroupendorsedprayermorethanthecommunity
groupsasaformoftreatment.TheUmlazigroupreportedthattheyreadaboutillnessin
ordertounderstandtheirillness.Ontheotherhand,theHospitalGrouprespondedthe
leasttoreadingabouttheirillness.Thisisunderstandableintermsofthelowerlevelof
educationandlowersocio‐economiclevelsoftheHospitalGroup.
6.4THEHEALTHANDILLNESSBELIEF(QUANTITATIVE)
Thereliabilityofthisquestionnaire,whichwasdevelopedtomeasurehealthandillness
beliefsforanAfricanpopulation,was0.76.Thissuggeststhatthemeasurementhashigh
internalconsistencyandisreliableforinterpretivepurposes.Acomparisonofthemeans
foreachoftheitemsshowthatthereweresignificantdifferencesinthewayeachofthe
groupsrespondedtoitems1,3,4,5,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,
24,26,27,28,29,30,and31.
178
Item1assessedthebeliefthatapersongetssickbecausetheyarenotstrong.Onthisitem
theHospitalGroupagreedmorethanthecommunitygroups.Therewasasignificant
differencebetweenthethreegroups(p<0.001).Overalltherespondentsdidagreeor
sometimesagreethatifapersonisnotstrongenoughheorshewillgetsick.Wecould,
therefore,assumethatbeingillmeansthatapersonisnotstrongenoughandvulnerable
andthatthisviewwillinfluencehowtheyaccepttheirillnessandhowothersrespondto
them.Anindividualwhoperceiveshimselforherselfasstrongandwhogetsillmay
thereforedenyhis/hersymptomsforalongtimeandmay,asaresult,delayseekinghelp.
Othersassociatingwiththepersonwhoisillmaytreathimasweak.Thismayleadtoand
fosteradependentroleinthepatientormayleadtothepatientresistingthesupportof
thosearoundhim.TherewasalsostatisticallysignificantdifferencesbetweentheHospital
GroupandtheUmlaziGroup(p<0.01),andtheHospitalGroupandKwaMashuGroup
(p<0.001)Thissuggeststhatthose,whoattendthehospitalshaveastrongerbeliefthat
thosewhoareillarenotstrong.Thereweresomewhodisagreedwiththisviewranging
from22.6%intheHospitalGroupto37.7%inthecommunitygroup.
Therewasgeneralagreementbyallgroupsthataperson'sdietmayleadtoillness(item
2).Thisisinkeepingwiththereasonsthesubjectsofferedwhypeoplegetsick?
TheintervieweestendedtodisagreewiththeviewthatillnessisduetodesertionbyGod
(item3).Thethreegroupsstatisticallydifferedsignificantlyonthisbelief(p<0.001),
especiallythoseintheKwaMashuGroup(71.4%)whodifferedfromtheHospitalGroup
(p<0.001).Althoughthereisagreementsometimesthatitcouldbetrue,itwouldsuggest
thatthegeneralcommunitybelievesthismorethanthosewhoattendthehospital.
Thebeliefthatillnessiscausedbyinfectionwasoverwhelminglyendorsedbyallsubjects
(item4).Itisapparent,therefore,thattheviewofinfectionasacauseofillnessiswell
accepted.Howevertherewasasignificantdifferencebetweenthegroups'responseon
thisitem(p<0.05).Therewasalsosignificantdifferencesintheendorsementsbetween
theHospitalGroupandtheUmlaziGroup(p<0.05),andtheHospitalGroupandtheKwa

179
MashuGroup(p<0.05).TheKwaMashuGroupendorsedthisitemoverwhelminglyhigher
thantheothergroups.
Item5whichrequiredthesubjectstorespondtothebeliefthatillnesswascausedby
witchcraftorsorceryyieldedmixedresponses.Therewassignificantdifferencesbetween
thethreegroups(p<0.05)aswellbetweentheHospitalGroupandtheUmlaziGroup
(p<0.05),andtheHospitalandKwaMashuGroup(p<0.05).Halfofthesubjectseither
agreed/sometimesagreeordisagreed/sometimesdisagreed.Althoughthebeliefisnota
dominantone,itisobviouslyanimportantbeliefininterpretingandunderstandingones
illness.Withitem6,thatdealswiththebeliefthatsicknessisduetoacurseor
bewitchmentbyothers,mixedresponseswerealsoobtained.Althoughtherewasa
slightlyhighertendencytodisagreewithsuchabelief.
Thereisgeneralbeliefthatlackoforinadequateregularexerciseleadstoillhealth(item
7).Asmallgroupdisagreesorarenotsureofthebenefitsofregularexercise.
Mostsubjectsdisagreedwiththebeliefthatsicknesscamefromthedevil(item8).Onthe
average,25.62%werenotsure.Asimilarpercentageagreedorsometimesagreed.
Thevisitingofdoctorsastheonlyhelp‐seekingbehaviourwhenseriouslyill(item9)wasa
dominantbelief.Although,thereweresignificantdifferencesbetweenthethreegroupsin
theiragreement(p<0.001).Allgroupsoverwhelminglyendorsedthisstatement.
Mostofthesubjectsdisagreedwiththebeliefthatonlydoctorscantreatpeoplewhoare
ill(item10),thisbeingmoresointhecommunitygroupsthantheHospitalGroup.There
wassignificantdifferencebetweenHospitalGroupandUmlaziGroupofp<0.001and
betweentheHospitalGroupandKwaMashuGroupofp<0.001.Ofthosewhoagreed,this
beliefwasmorecommonintheHospitalGroup.Thiscouldexplainwhypeopleseek
medicalhelpandmaybeausefulbelieftoconsiderincompliance.
180
Item11whichassessedthebeliefthatthereisnothingapersoncandotopreventhimself
fromgettingillalsoelicitedmixedresponses.Astatisticalsignificanceofp<0001was
obtainedbetweenthethreegroups.Whilealargenumberdisagreed,16.74%agreed,
21.91%sometimesagreedand17.19%werenotsure.Thiswouldindicatethatthereare
manywhobelievethattheyhavenointernallocuscontrolinpreventingthemselvesfrom
gettingill(WallstonandWallston,1984).
Sicknessasaresultofpoorselfcareand/orhygienewasendorsedbymostofthesubjects
(item12).Asignificantdifferencewasfoundbetweenthegroups(p<0.05).Thisbeliefisin
keepingwiththesubjectsresponsesto“Whypeoplegetill”
Thesubjectsagree/sometimesagreedthatsomeillnesscannotbetreatedbymedical
doctors(item13).Thiswouldsuggestthenthatifindividualsdonotbelievethatdoctors
cantreatallillnessesthenwecouldassumethattheywouldseekhelpwheretheymay
feeltheywouldobtainappropriatetreatment.Thisbeliefmayaccountforthevaried
responsetoitem10andmayleadtoselectivehelp‐seekingbehaviour.
Thesubjectsalsoendorsedthebeliefthatsometimesillnessesareinherited(item14).The
threegroupsrespondeddifferentlyonthisitem(p<0.001).TheKwaMashuGroupagreed
lesswiththisitembutendorsed“sometimesagree”moreoften.
Item15whichlookedatselfcarebyindividualspreventingillness,wasgenerallyendorsed
bythesubjects.19,21%disagreedand15.03%werenotsure.Againtheissueofinternal
locusofcontrolinhealthbehaviourmustbeconsidered(WallstonandWallston,1984).
Thesubjectsfeltthattheywereabletoeffectacurethemselveswhenill(item16).27.36%
disagreedand16.78%werenotsure.However,theydidnotseethemselvesasculpable
forillnesses(item17).Althoughtheysometimesagreedthattheirillnesscouldbetheir
fault.Responsessignificantlydifferedbetweengroups(p<0.001).Hereagaintheconcept
ofinternallocusofcontrolmaybeacentralissuetoconsider.
181
'Visitingadoctorforregularcheckupscanpreventapersongettingsick'(item18)was
agreed/sometimesagreedbymostrespondentsHowever,14.09%disagreedand16.46%
werenotsure.Asignificantdifferenceofp<0.001betweenthethreegroupswasobtained.
Inaddition,theintervieweesexpressedthebeliefthatdoctorscantreatsymptomsbutnot
thecause(item19).Hereagaintheinfluenceofculturaland/ortraditionalbeliefsof
illnessmaybediscerned.
Therewasageneralisedresponsetothebeliefthatmostillnesscanbetreatedathome
(item20).Asignificanceofp<0.001wasobtainedbetweenthegroups.24.49%agreed,
30.70agreedsometimes,26.41%disagreedand18.40%werenotsure.TheKwaMashu
Groupoverwhelminglydisagreedwiththisview.Respondentsalsobelievedthatolder
peopleknowatlotaboutillnessandthattheycanprovideappropriateadvice(item21).
Theresponsesshowthat29.91%agreedand30.70%sometimesagreedwiththis
statement.
Item22dealtwiththebeliefthatpeopleshouldpraytoGodtocurethemoftheirillness.
Theresponsevariedfrom27.64%agreeing,29.44%agreeingsometimes,22.70%
disagreeingand20.22%notsure.Thethreegroupssignificantlydifferedintheirresponses
(p<0.001).
Item23assessedthebeliefthatpeoplearelazyanddonotworkhardenough.Mostofthe
subjectssometimesagreed(35.85%).Asignificanceofp<0.05betweenthegroupswas
obtained.
Beliefsaboutthetreatmentgivenbyeldersorolderpeoplewasassessedbyitem24.The
mostcommonresponsewas'sometimesagree'(37.02%).Thesecondhighestresponse
was'notsure'(23.59%).Ontheaverage18.17%agreedand21.22%disagreed.
Asmuchas49.21%ofthesubjectsdisagreedwiththebeliefthatillnessisaformof
punishmentforthewrongorbadthingsthatapersonhasdone.However,19.41%agreed
sometimes,11.17%agreedand20.20%werenotsure.

182
Thebeliefthatapersonmaygetsickasaresultofsomethinginvadingtheirbody(item25)
wasanacceptedbeliefbysubjectseitheragreeing(39.37%)orsometimesagreeing
(31.79%).Only13,46%werenotsureand15.38%disagreedwiththestatement.TheKwa
MashuGroupshowedhighestagreementwiththestatement(49.4%)andlowest
disagreement(10.4%)
Item27assessedthebeliefthatsicknessoccurredasaresultofnotperformingthe
requiredritualsorprayerstoancestorsorpriest.Thegroupssignificantlydiffered
(p<0.001).Although43.53%disagreedwiththisbelief,12.04%agreed,20.25%agreed
sometimesand24.18%werenotsure.TheKwaMashuGroupleastagreedwiththe
statement(5.2%)andshowedhighestdisagreement(59.7%).
Avariedresponsewasobtainedforthebeliefthatapersoncanbecomeilliftheywalkor
crossoverapathorplacewheresomeritualwasperformed(item28).Asignificant
differencebetweengroupswasobtained(p<0.05)'Sometimesagree'wasthemost
commonresponse(22.57%),while22.57%agreedand21.33%werenotsure.25.17%
disagreedwiththebelief.TheKwaMashugroupdemonstratedlowestagreementwith
thisbelief.
Thebeliefthatsicknessistheresultofmalfunctioningorimproperfunctionofthebody
(item29)appearstobeacommonbeliefoftherespondents.Thosethatresponded'agree'
were34.76%and'sometimesagree',36.23%.TheKwaMashuhighestagreementwiththe
statement(50.0%)andlowestdisagreement(5.8%)
Therewasahighdisagreementwiththestatementthatillnessisduetodemon,evilorbad
spiritpossession(48.48%).Ap<0.05significancewasobtainedbetweenthethreegroups.
Boththecommunitygroupsshowedlowagreement.Umlazi9.9%andKwaMashu9.7%.
AlthoughtheHospitalGroupdemonstratedmoreagreementwiththebelief(14.9%),they
alsorespondedwiththehighestdisagreement(51.9%).

183
Thelastitemassessedthebeliefthatillnessisduetopunishmentordesertionbythe
ancestors.Therespondentsshowedhighdisagreementwiththisbelief(47.18%).Although
22.86%werenotsure,14.53%agreedand15.43%sometimesagreedwiththebelief.The
KwaMashugroupindicatedthelowestagreementwiththisbelief.
Whiletherehasbeensignificantdifferencesinthewaytheintervieweesrespondedon
eachitem,therewasnoconsistentdifferenceinthewayeachgroupresponded.This
suggestthattheHospitalGroupbeliefsofhealthandillnessarenotsignificantlydifferent
tothatofthecommunity.
However,itappearsthatcertaindominantbeliefsareendorsedbytherespondentsthese
are:peoplegetillbecausetheydonoteattheproperfoods;illnessiscausedbyinfection,
peoplegetsickbecausetheydonotexerciseregularly;peoplegotodoctorsonlywhen
theyareseriouslyill,peoplegetsickbecausetheydonotkeepthemselvesclean;thereare
someillnessesthatdoctorscannottreat;peopleinheritillnessfromtheirparents;if
peopletakegoodcareofthemselvestheywillnotgetill;peopleareabletocure
themselves;visitingadoctorforregularcheck‐upscanpreventapersongettingsick;
doctorscanmaketheillnessbetterbuttheycannottreatthecause;olderpeopleknowa
lotaboutillnessandcanadviseotherswhattodo;peoplegetsickbecausetheyarelazy
anddonotworkhardenough;peoplegetsickwhensomethingforeigninvadestheir
bodiesandsicknessoccurswhenthebodyisnotfunctioningproperly.Inaddition,
respondentsgenerallydisagreedwiththefollowing:illnessisduetodesertionbyGod;
sicknesscomesfromthedevil;doctorsaretheonlyonesthatcantreatpeoplewhoareill;
thereisnothingapersoncandotopreventthemselvesfromgettingill,ifapersongetsill
itistheirownfault;illnessisaformofpunishmentforthewrongorbadthingsaperson
hasdone;sicknessoccursbecauseyoudonotperformtheritualsorprayerrequiredby
thepriestorancestors;illnessisduetodemon,evilorbadspiritpossession;andillnessis
duetopunishmentordesertionbytheancestors.
Thebeliefsthatwerelessclearwere:peoplegetsickbecausetheyarenotstrong;illnessis
causedbywitchcraftorsorcery;peoplegetsickbecausesomeonehascursedordone

184
somethingeviltothem;mostillnessescanbetreatedathome;peopleshouldpraytoGod
tocurethemoftheirillness;treatmentgivenbyeldersorolderpeoplecanreallybe
helpful;andapersoncanbecomeilliftheywalkorcrossoverapathorspotwheresome
ritualwasperformed.
Oftheninefactorsthatemerged,fourdealtwithaetiology,fouraddressedbeliefs
regardingtreatmentandoneillnessprevention.Theaetiologiesofillnessforurban
Africansaccordingtotheseresponsesareexternalevilandancestral,self‐blame,medical
andbodymalfunctionorweakness.Themaintreatmentbeliefsareselfmedication,
medicaltreatments,prayerandanholistictreatmentapproach.Self‐careisseenasa
methodforpreventingillnesses.
Thereweresignificantdifferencesoncertainfactors(TableXXXIX).Onfactor2,boththose
livinginanurbanareaforlessthan5yearsandgreaterthan5yearsendorsedthe
aetiologicalbeliefofself‐blame(p=0.0003)butthosewhowerelivinginaurbanareafor
lessthan5yearsendorsedthebeliefofself‐blamemorethanthosewhowerelivingfor
greaterthan5years.Apossiblereasonforthiscouldbethatthosewholivedforlessthan
fiveyearswouldhaveonlyrecentlylefttheruralareasandthereforeweremorelikelyto
attributetheirillnesstohavingabandonedtheirculturalrootsandbeliefs.
Onfactor3therewasasignificantdifferenceamongthegroups(p=0.0003)inthe
interactionwithurbanisation.Themoreurbanisedtheindividualthemorelikelyheorshe
wastoadoptamedicalaetiologyofillness.Therewasalsosignificantageeffect
(p=0.0015).Theyoungertheadultthemorelikelywasheorshetoadoptamedicalreason
forillness.Thisisprobablyduetotheprocessofeducation.
Beliefsinself‐medication(factor4)significantlydifferedbetweenthe3groups(p=0.0220).
Thesebeliefsalsovariedwithurbanisation(i.e.thenumberofyearslivinginanurban
area).Urbanisationalsoinfluencedthegroup'sbeliefsonbodymalfunctionandphysical
weaknessetiology(factor5).Thisbeliefwasalsoaffectedbytheageoftheindividuals.
Theoldertheindividualthelesslikelythebelief.Self‐careaspreventativebeliefwas

185
differentbetweengroupsandwasalsoinfluencedbyurbanisationandtheageofthe
individuals.Thissuggeststhaturbanisationandyoungeradultsbelievethatself‐carewill
preventillnesses.Theuseofprayer(factor8)variedbetweenthegroupsandwas
influencedbyurbanisationaswell.Bothurbanisationandagealsoinfluencedtheholistic
treatmentbelief(factor9).
Factor6whichdealswithmedicaltreatmentvariedbetweenthegroups.Thecommunity
groupsstronglybelievedinmedicaltreatment.Thiswouldsuggestthatahigherlevelof
education,acculturationandurbanisationcontributestothebeliefsoftheefficacyof
medicaltreatments.
Theseresultssuggestthereforethatthehospitalattendersdonothaveasetofbeliefsof
healthandillnessdifferentfromthoseofthegeneralpopulation.Nevertheless,thereare
severalhealthandillnessbeliefsheldbythiscommunity.Thesebeliefsarestrongly
influencedbyurbanisationandtheageoftheindividual.Itwould,therefore,seemthat
healthandillnessbeliefsvaryandarestronglyinfluencedbyurbanisationandageofthe
individuals.
6.5SOCIALSUPPORTANDHEALTH
Thisquestionyieldedaveryhighlevelofreliability(0.91).Hereagain,thismeasurement
hadhighinternalconsistency.
Theresponsesofthesubjectsshowthattheyweregenerallysatisfiedwithallaspectsof
socialsupport(TableXLI).Regardingaccessibility,therewasasignificantdifferenceamong
thegroupsastowhethertheaccessibilitywasimmediate(p=0.0001)ordelayed
(p=0.0001).Ofthosethatindicatedthattheyhadimmediateaccessibility,theKwaMashu
Groupscoredhighest,followedbytheUmlaziGroupandthentheHospitalGroup.For
thosethatindicatedthattheiraccessibilitywasdelayed,thoseinKwaMashureported
moredelaysthantheothergroups.

186
Theproximityofthesubjects'socialsupportsignificantlyvariedforthegroups
(TableXLIII).Eachgrouprespondedsignificantlydifferentlyregardingtheproximityof
theirsupport.TheKwaMashuGroupmostlyindicatedsupportnearbyfollowedbythe
UmlaziGroupandthentheHospitalGroup.However,ofthosethatindicatedthattheir
supportwasfar,theKwaMashuGrouphadgreateramountofsupportfurtherawaythan
boththeHospitalorUmlaziGroups.
Regardingthemodeofsupport,boththeHospital(80.85%)andKwaMashu(95.45%)
groupsusedthetelephoneextensivelytoobtainsupport:Supportthroughletterwriting
orpostalserviceswasobtainedby32.71%intheHospitalGroup,27.62%intheUmlazi
groupand59.74%intheKwaMashugroup.Itwouldseemthatthosewhoattendedthe
hospitalandthoselivingintheKwaMashuareahavelessphysicalcontactwiththosewho
providesocialsupportalthoughtheseindividualsdonotliveveryfaraway.Thisisin
keepingwiththeearlierresultsthatshowedthat79.26%ofthehospitalsubjectswere
unaccompanied.Thiscouldbeduetovarioussocio‐economicfactorssuchashavingtolive
separately,inrelatives'homesorbecausethosethatprovidesocialsupporteitherlive
withtheiremployers,asinthecaseofdomestics,orinhostelsprovidedbyemployers.
Withinthiscontext,theuseofthetelephoneorpostalservicesbecomepractical.The
Umlazicommunity,ontheotherhand,havemorepersonalsupportandrepresents
familieslivingtogether.Thefactthatthesubjectsdescribedtheirsocialsupportasbeing
satisfactorydespitethevariationinthetypeofsocialsupport,suggeststhatitisnothow
socialsupportisobtainedbutrathertheavailabilityandtheperceptionofsupportbythe
individualthatisimportant.Theperceptionsofsupportareprobablyinfluencedbythe
individual'sexpectationsaswell.Inthecontextwheretheconceptoffamilyhas
deterioratedtotheextentithasamongAfricansinSouthAfrica,theindividual's
expectancyofsocialsupportisprobablynotcommensuratewiththoseofindividualsin
moreprivilegedcommunities.
Supportismostoftenprovidedbyamother,family,friendsandneighbours.Thisisin
keepingwiththehospitalsubjectsqualitativeresponseswithregardstobeing

187
accompaniedtothehospital.Ofthoseaccompanied,mostwereaccompaniedbyclose
familyandfriends.Suchman(1966)andHouseetal.(1988)haveshownthattheseeking
ofhealthbehaviourisasocialprocessinvolvingfamily,neighboursandfriends.
Thefactoranalysisoftheresponsesonthesocialsupportquestionnaireyieldedtwo
factors.Factor1dealswithgeneralsocialsupportorsupportinthetimeofacrisis.Factor
2dealswithaclose,confidentialtypeofsupport.Itisinterestingthatonfactor1theway
subjectsrespondeddependedontheirsex,thelengthofstayinanurbanareaandage
(TableXLVI).Therewasnosignificantdifferencesbetweenthegroupssuggestingthat
socialsupportdidnotinfluencehelp‐seekingbehaviourintheHospitalGroup.
FemalesintheHospitalGroupsignificantlyendorsedthesupportoffactor1morethanthe
males(p=0.0072).Malesendorsedthistypeofsupportinthecommunitygroupsmore.
ThismaysuggestthatfemalesintheHospitalGrouparemoresatisfiedgenerallywith
socialsupportorsocialsupportincrisesthanthoseinthecommunity.Inaddition,those
livinglessthanfiveyearsintheurbanareaweresignificantlymoresatisfiedwiththetype
ofsocialsupportinfactor1exceptinthecaseoftheUmlaziGroup(p=0.0178).Thismay
suggestthatthosenewintheurbanareaaresatisfiedwiththesocialsupport.Asthey
residelongerinanurbanareathefactor1typesocialsupportisperceivedasbeingless
satisfactoryorthesocialsupportactuallydwindles.Anotherreasonforthoselivinginan
urbanarealessthanfiveyearsfindingthesocialsupportsatisfactory,isthattheymay
havecomefromruralareaswherethequalityofsocialsupporthadbeenpoorornon‐
existent.Therewerealsosignificantdifferencesinthewaylivinginanurbanareaaffected
male'sandfemale'sperceptionoffactor1socialsupport(p=0.0289).Thelengthofstayin
anurbanareadoesnotseemtoaffectthemalesperceptionoffactoronesocialsupport.
Afterfiveyearsresidenceinanurbanarea,thefemalesperceptionimproved.Thiswould
suggestthatfemales'levelofsocialsupport(factor1type)oratleasttheirperceptionofit
improveswhentheymoveintoanurbanarea.
Onfactor2thereweresignificantdifferenceswithregardstolengthofstayinanurban
areabetweenthegroups(p=0.0160)andthesexofthesubjectsbetweenthegroups

188
(p=0.0160).Thesedifferencesweresimilartofactor1suggestingthatthefemalesinthe
HospitalGrouparemoresatisfiedgenerallywithsocialsupportorsocialsupportincrises
thanthoseinthecommunity(exceptintheHospitalGroup)andthatthosenewinthe
urbanareaaresatisfiedwiththesocialsupport.However,astheyresidelongerinan
urbanareathefactor2typesocialsupportisperceivedasbeinglesssatisfactoryorthe
socialsupportactuallydwindles.Hereagain,anotherreasonforthoselivinginanurban
arealessthanfiveyearsfindingthesocialsupportsatisfactoryisthattheymayhavecome
fromruralareaswherethequalityofsocialsupporthadbeenpoor.However,the
perceptionofUmlaziGroup'ssocialsupport(factor2type)improvedwiththeirresidence
inanurbanarea.
Overall,theresultsshowthatthereissatisfactionwiththeavailablesocialsupports.
Femalesseemtoperceiveandexperiencebettersocialsupportthanmen.The
improvementofthefemales'satisfactionwithsocialsupportonfactor1,aswellasthe
males'perceptionsnotdeclining,appearstohavepositiveimplicationsregardingsocial
supportandurbanisationinAfricansbecausesatisfactorysocialsupportisdirectlyrelated
tophysicalandpsychologicalwell‐beingandactsasabufferbetweenstressfullifeevents
andsymptoms(Zimetetal.,1988).Ontheotherhand,theexperienceandperceptionsof
socialsupportonageneralscaleseemtodeclinewithlongerresidenceinanurbanarea.
Thisaspectraisesconcernforthefuture.Thepositiveeffectsofgoodsocialsupportin
healthandhealthbehaviourhasbeenwelldocumented(CohenandSyme,1985;
Geertsen,1988;Ritter,1988;Sarason,etal.1985).However,inthisstudytherewasno
significantdifferencesbetweenthegroups.Thissuggeststhatsocialsupportdidnot
influencehelp‐seekingbehaviourintheHospitalGroup.
6.6SYMPTOMPERCEPTIONS
Averyhighreliabilitywasalsoobtainedinthisquestionnaire(0.96).Thissuggestthatthe
measurementhashighinternalconsistency.

189
TheHospitalGroupdidnotexperiencemoresymptomsorratetheirsymptomasmore
seriousthantheothergroups.Generally,theKwaMashuGroupexperiencedmore
symptomsthantheothergroups.Thesubjectsendorsedtheirexperienceofpsychological
andpsychiatricsymptomatology,suchas,depressionandanxietytogetherwithphysical
symptoms.ThisiscontrarytothepopularbeliefthatAfricanpatientsdonotgenerally
presentwithdepressiveoranxietysymptomatologybutmainlyphysicalsymptoms.Itis
possiblethattheseindividualsperceivethemedicaldoctorasbeinginterestedinphysical
symptomsandthereforeonlyreportphysicalsymptomstohimorher.Thisisa
fundamentalproblemwiththemedicalmodel;itfocusesonlyonthebiological.Asa
result,patientsaretaughttopresenttheirillnessinthismanner.Mechanic(1992)points
outtheinfluenceofdoctorsviewsandpracticesonhealthandillnessbehaviours.The
failuretoaddresstheotherdimensionsofhealthandillness,ortheself‐understanding
withinAfricanworld‐viewwillperpetuatetheseekingofalternatetreatment,thedelayin
medicalhelp‐seekingbehaviourand/orobtainingtreatmentfromothersourcesthatwill
addressthedifferentdimensions(FreemanandMotsei,1992).Thefocusonphysical
symptomatologywillalsocontributetotheviewthatpsychological,psychiatricandsocial
symptomsarelessimportantandthetreatmentofthesesymptomsarealuxury.Sucha
viewresultsintheindividualnotbeingtakenseriouslyorcontributestohisorherlearning
tosomatizeinordertoobtainhelp.
6.7STRESSANDHELPSEEKINGBEHAVIOUR
ThereliabilityobtainedinthemodifiedversionoftheLifeexperienceSurveywas0.71.
Hereagaintheinternalconsistencywashigh.Thissuggeststhatthequestionnairehas
goodconstructvalidity.
Thereweresignificantdifferencesinthewaythegroupsperceivedtheextentorimpactof
thefollowinglifeexperiences:Marriage(item1)wasregardedpositivelywiththeUmlazi
Group.Itssamplerecordedthemostmarriages(p=0.0001).TheKwaMashuGroup
reportedtheleastnumberofmarriages.However,thesubjectsgenerallyfoundmarriagea

190
positiveexperience.Engagements(item44)wererecordedinlargernumbersintheKwa
MashuGroupthantheothergroups(p=0.0317).Engagementstooaredescribedas
positiveexperiences.Reconciliationwithboyfriendorgirlfriend(item47)hadagreater
impactintheHospitalandUmlaziGroupthantheKwaMashuGroup.Theimpactof
maritalreconciliation(item25)wasmorepositiveintheHospitalGroup.Theimpactof
outstandingpersonalachievement(item9)wassignificantlyhigherintheKwaMashu
Group.Thistoohadapositiveimpact.Thesignificantnegativeimpactswereduetodeath
ofaspouse(item1);changeinsleepinghabits(item4);deathofmother,father,sister,
grandmotherandotherclosefamilymembers(item5);seriousillnessofotherclose
familymembersandspouse(item15);troublewithemployer(item17);changeinthe
numberofargumentswithspouse(item26);changeinhusband'swork(item28);change
intheamountofrecreation(item29);borrowingmorethanR10000(item31);major
personalinjury(item35);majorchangesinlivingconditions(item37)andunrestinthe
areaofresidence(item48).
Amultivariateanalysisofthetotallifeexperiencesbetweenthegroupsshowasignificant
difference(p<0.001—TableLIII).TheDuncan'smultiplerangetestrevealsthatthe
differenceoccurredintheUmlaziGroup(TableL).suggestingthattheUmlaziGroupon
theaveragehadsignificantlylesserthreateningorenhancinglifeexperiencesorchanges
thantheothergroups.Amultivariateanalysisofthenegativeandpositivelifeexperiences
betweengroupsalsoshowasignificantdifferencebetweengroups(TablesLIVandLVI).
TheDuncan'smultiplerangetestonnegativeandpositivelifeexperiences(TableLIIand
LIV,respectively)revealsthatthesubjectsintheUmlaziGroupexperiencedtheleast
amountofchangecomparedtotheothergroups.Theseresultssuggestthatalthoughthe
HospitalGroupexperiencedmorepositiveandnegativelifeexperiences,itwasnot
significantlydifferenttotheKwaMashugroup.Itmaybeinferredthenthatlife
experiencesarethereforenotasingularlytriggerfactorforhelp‐seekingbehaviourinthe
hospital.However,thefactthatthesubjectsintheHospitalGrouphadmostlifechanging
experiencesmaylendsomesupporttotherelationthatsomehavearguedforbetween
stressandillness(Feuerstein,etal.,1987;HolmesandRahe,1967;RaheandLind,1971;
Selye,1956;Steptoe,1991;TurtonandChalmers,1990).

191
Thisstudyshowsthatthosethatattendthehospitaldonothaveadistinctivelydifferent
setofhealthbeliefstoothersintheirsociety.Whatemergesisthatthereareseveral
healthbeliefsabouttheaetiology,treatmentandprevention.Inthisstudythefollowing
mainbeliefsemerged:aetiologicalbeliefs(externalancestral/evil,self‐blame,medical,
physicalweaknessorbodymalfunction);treatmentbeliefs(selfmedication,medical,
prayer,holistictreatment)andthepreventativebelief(selfcare).Age,sex,educationand
urbanisationstronglyinfluencethebeliefsthatapersonadopts.FortheAfricanpatient,
health,illnessanddiseaseareviewedholistically.Thebodyandmindareinseparablefrom
thedimensionsofthesocial,culturalandreligious.Medicalbeliefsarealsowellintegrated
intotheirconceptualisationofhealthandillness.Thereis,however,amuchlesser
emphasisonculturalbeliefs,whichisprobablyaresultofacculturationinthiscommunity.
However,thisdoesnotmeanthatthemedicalviewofillnessisreadilyaccepted.There
existsabeliefthatwesternmedicinetreatsthesymptomsbutnotthecause.Depending
ontheindividual'sbeliefofwhatthecausemaybe,theappropriatehelp‐seekingtakes
place.Thismayincludeself‐medication,seekingthehelpoffamily,traditionalhealers,
faithhealers,herbalistsorprayer.ThisstudyalsoshowedthattheHospitalGroupdidnot
significantlydifferfromtheothergroupsintheexperienceandperceptionofsocial
support,theexperiencesandseverityofsymptomsandthenumberoflifeinfluencing
experiences.
6.8ACOMPARISONOFTHERESULTSWITHOTHERHEALTHANDILLNESSMODELS
Theresultsofthisstudysupportmanyofthecomponentsorconceptsproposedbysome
ofthemorepopularmodelsofhealthandillness.(Areviewofthepopularmodelshas
beenpresentedinchaptertwo).Thoserelevantaspectsthatemergedfromthisstudyand
allowinferencestobemadewillbebrieflydiscussedhere.However,itmustbenotedthat
thisstudywasnotdesignedtotestthesemodels.Possibleinferencesaredrawnfromthe
resultstosupportorvalidateaspectsoftheseothermodelswherethismaybevalidly
done..

192
Theresultofthepresentstudysupportstheviewthattheperceptionofsymptomsplays
animportantpartintheseekingofhelp.AccordingtotheHBM,symptomsactasan
internaldecisionmakingprocessthatactasa'cuetoaction'.KaslandCobb'sModel
(1966a)onillnessandsickrolebehaviourshypothesizesthatbehaviourundertakeninthe
presenceofsymptomsisinfluenceddirectlybytheindividual'sperceptionofthedisease
andthebeliefconcerninghealthaction.Suchman(1965a;1965b)alsopointsoutthat
symptomexperiencesalerttheindividualthatsomethingiswrongwhichisthen
interpretedandresultsintheassumptionofthesickrole.Fabrega'sModel(1973)also
suggestthattherecognitionandevaluationofsymptomsleadstorealisationofthe
presenceofillnessandinturnleadstobehaviourstoalleviatethem.Thisisalsocommon
toMechanic'sModel(1978)aswell.Inthepresentstudytooitwasfoundthatthe
presenceofsymptomsalertstheindividualthatsomethingiswrongandprecipitatesthe
processofhelpseeking.
Theseverityofsymptomsisalsoacomponentofmanyofthesemodels.Inkeepingwith
theHBM,Suchman'sModel(1965a,1965b)andMechanic'sModel(1978),theextentto
whichsymptomsareperceivedasseriouswillaffecthelp‐seeking.Thisvariablewasalso
foundtobeoneofthesixcategoriestoemergefromtheCummings,BeckerandMaile
(1980)studytoidentifycommonvariablesamongthehealthmodels.Inthisstudy,
severityofsymptomsplayedamajorpartinprecipitatinghelp‐seekingandsubjectsalso
reportedthatdelayinseekinghelpwasaresultofthemnotperceivingtheirsymptomsas
serious.
'Benefits'or'costofaction'and'barriers'isacomponentthatfeaturesfrequentlyinthe
healthmodels(HBM;KaslandCobb,1966a;1966b;Mechanic,1978).Hereagain,subjects
inthisstudysoughthelpiftheybelievedthatsuchactionwouldalleviatetheirsymptoms.
Thisstudyalsoshowedtheusageofseveralothertreatmentsinadditiontomedicalhelp‐
seeking.Thesecomponentssuchasshopping,selfmedication,homeremediesand/or
culturaltreatmentsarealsocommontoSuchman'sModel(1965a,1965b),Fabrega's
Model(1973)andYoung'smodel(1980)

193
Ahighpercentageinthisstudyreportedseekingthehelpandadviceofsignificant
individualsintheirenvironment.Suchman(1965a,1965b),Fabrega(1973),Mechanic
(1978),Young(1980)andCummings,BeckerandMaile(1980)allemphasizethe
importanceofsocialsupportandsocialnetworksintheutilizationofhealthfacilities,
Consistentwithallthesemodels,healthattitudes,valuesandbeliefshavebeenfoundto
playanimportantroleintheperception,experienceandunderstandingofsymptoms,the
choiceoftreatments,thedecisiontoseektreatmentandthebenefitsoftreatments.This
studyisinkeepingwiththesemodelsalsosupportstheviewthatdemographicvariables
playsaroleintheseekingofhelp.
Theaccessibilityofservices,astheHBM,Anderson'sModel(1968)andYoung(1980)also
found,contributestotheutilizationofhealthservices.Responsestoitemssuchas5,7,10,
11,15,17,18,1924and30ontheHBQ,supportsconceptssuchas'healthlocusof
control','internalhealthlocusofcontrol','powerfulothershealthlocusofcontrol'and
'chancehealthlocusofcontrol'(WallstonandWallston,1984)
Thefactthattheseresultsvalidatesomeofthefundamentalaspectsofthecommon
healthandillnessmodelssuggeststhatthesewesternmodelsmaybeadaptedforusein
theAfricancontext.Localresearch,likethispresentone,canbeintegratedintoalready
existingmodelstoprovidemoreusefulworkingmodelsforlocalusage.
6.9TOWARDSAMODELOFHEALTHANDILLNESS
BasedonthefindingsofthisstudyitispossibletoconstructahelpfulmodelofAfrican
helpseekingbehaviourvalidatleastforcommunitiessimilartotheurbanAfrican
communitiesstudiedhere.AgraphicalrepresentationofthemodelispresentedinFigure
12.Theexperiencesofsymptomsalertstheindividualofchangestakingplaceand
commencestheprocessofhelpseeking.Thesymptomsexperiencedbythepatientsare

194
bothpsychologicalandphysical.Asmuchas63%experiencephysicalsymptomsandabout
20%psychologicalsymptoms.Thesesymptomsthatareexperiencedareevaluatedinthe
contextoftheindividual'spersonalconceptionofhealthandillness.Thisstudyhas
uncoveredfurtherevidencefortheviewthattheurbanAfrican'sconceptionofhealthand
illnessisholistic.
Healthisviewedasfeelinggood,well,comfortable,freeinbodyandmindandinvolves
thefeelingofcontentmentwithlife.Theindividual'smoodindicatesthatthepersonis
well;thereisnopain;theindividualisactiveandproductive;thereisnormalvegetative
functioningandtheindividualsocializesappropriately.Changesinanyofthesewill
constituteillness.

195

196
Thesechanges,thatisthephysicalandpsychologicalchanges,aswellasthecognitive
evaluationofthechanges,alerttheindividualthatallisnotwell(thismaybereferredto
asthestageofalertness).Theindividualwilldisclosethisexperienceorfeelingtoothers.
Aboutasmanyas86%willsharethisinformationwithothers.Thissharingofsymptomsis
referredtoasillnessdisclosure.Thepurposeofillnessdisclosureistohelptheindividual
makesenseofhisorhersymptoms.Illnessdisclosuremayalsobealearnedresponsein
theindividual'sinitialassumptionofillnessbehaviourandsickrolebehaviour.Thesupport
anddisclosureismostoftentomother,familyandfriends.Thisisprobablybecause
mothersaregenerallytheonesclosesttotheindividualfrombirth.Theexperienceof
symptoms,istherefore,associatedwiththecaringandnursingofamotherormother
figureandhencesupportwillbesoughtfromsuchindividuals.Theviewthatolderfolk
knowalotaboutdiseaseswillalsoleadtotheseekingofhelporsupportfromthem.
Duringthestageofalertnesstheindividualtriestounderstandorattachmeaningtothe
symptoms.Inaddition,theviewsofothers(towhomtheindividualhasdisclosedhis
illnessto),theindividualbeliefsandpastexperienceswillalsoplayacrucialrolein
establishingmeaningforthesymptoms.
Beliefsmaybecategorisedintofourmainareas;Theseare,cultural,self‐blame,medicalor
bodymalfunction(TableXXXIX‐factors1,2,3,and5).TableXXXVprovidesexamplesof
thesebeliefs.Theexperiencesthatassistintheunderstandingofthesymptomsreferto
thoseillnessexperiencestheindividualhasexperiencedinthepastanditsconsequences,
aswellasexperiencesofotherswhowereillorexperiencesofillnessviaothermeanssuch
astelevision,newspaper,stories,oraltraditions,formaleducationandothermedia.
Onthebasisofthemeaningorunderstandingofthesesymptomsactivehelp‐seeking
begins.However,asmuchas46%willstillnotknowwhatiswrongwiththemotherthan
realisethattheyareillandrequirehelp.Theunderstandingormeaningsascribedto
symptomsmaybecategorizedintothreebroadareas,namely,medical,layand/orcultural
(TableXXXIX).

197
Thehelp‐seekingbehaviourswillvary.Help‐seekingmaybeseparatedintofourbroad
areas,namely,self‐help,prayer,culturaland/ormedical.Selfhelpwillincludetheuseof
substancesavailableathome,fromsignificantothers,shopsandpharmacies.About32%
(TableXXXVI)willmedicatethemselves.Thesubstancesusedmayvaryfromhomemade
concoctionstomedicaltreatments(TableXXX).
Prayerasamethodofhelp‐seekingisbasedonthereligiousviewthattheycouldbe
healedbyGodwhohasthepowertodoso.Usuallyprayerisobtainedfrommembersof
churchesorotherreligiousorganisations.Culturaltreatmentsareobtainedfromthe
traditionalhealer,thefaithhealerandherbalist.
Theuseofmedicalservicesisthefourthtypeoftreatment.However,onlyabout20
percentwillvisitadoctorimmediately.About40%willmonitortheirsymptomsandatthe
pointthattheythinkthatitisseriousenoughwilltheyvisitadoctor.Insomeinstancesthe
delayinvisitingadoctormaybeduetootherbarrierssuchasfinancialconstraints,lackof
transport,availabilityofappointments,sickleaveandpersonalproblemssuchasnobaby
sittersornoonetoaccompanythepersonfortreatment.
Medicalhelp‐seekingisprobablytheresultoflearnedbehaviour,sanctionedsocially
acceptedbehaviourandtheresultofwesterninfluencesabouttheunderstandingof
illnessandhealth.Theinitialreason,thatismedicalhelpseekingisalearnedresponse,is
duetoseveralwaysinwhichthebehaviourcouldhavebeenreinforced.Thesedays,more
andmoreAfricanbabiesarebeingborninthehospitalandnot,asinthepast,athomeby
midwives.Asaresult,theindividualisexposedfrombirthtohospitals,doctorsandclinics.
Evenpregnancy,anormaldevelopmentalprocessismedicalisedbecauseofthe
developmentofspecialisedobstetriccareandthefactthatapregnancyistreatedasa
“disease”wherethemotherisrequiredtoattendante‐natalclinics.Thefollowupcareat
clinicsafterbirthtomonitorbirthweightandtheimmunizationofchildrenfurther
reinforcesthisview.Visitstothedoctorandtheinteractionwiththedoctorleadstoa
learnedresponsebytheindividualespeciallyinamannerthatisacceptabletothedoctor.
Inthisregard,patientsareinfluencedtopresentsymptomstotheirdoctorsinaparticular

198
way.Thisprocessoflearningtakesplacesthroughtheassociationofsymptomswith
doctors,thereinforcedbenefitsoftreatmentandmodelling.
Otheraspectsthatinfluencesthechoiceandselectionofmedicalservicesarethelocation
andqualityoftheserviceprovided.Individualswilluseserviceslocatedclosesttothemor
wheretheybelievegoodservicesareprovided.Hereagain,theopinionsofsignificant
othersplayanimportantroleindeterminingwheregoodservicesexist.
Itisimportanttonotethatthevarioussourcesoftreatment,namely,self‐help,prayer,
culturalandmedicalarenotnecessarilymutuallyexclusivetreatments.Individualstendto
usethemconcurrently.However,certaintreatmentsmaybecomesociallysanctioned
morethanothers.Forexample,withacculturationmedicalhelpseekingismoresocially
acceptedthanculturaltreatments.Yettheutilizationofaparticulartreatmentmaynot
representcompleteortotaltreatmentbecausetheremayexistthebeliefthatdoctorscan
treatsymptomsbutnotthecauseorthatdoctorsarenottheonlyoneswhocantreat
peoplewhoareill(HBQitem10and19respectively).Alternativetreatmentsmaythenbe
soughtbutifthesearenotsociallysanctioneditwouldtakeplaceclandestinely.
6.10SUMMARYANDCONCLUSIONS
Thisstudyhasdemonstratedthefollowing:
1 UrbanAfricanshaveapersonalconceptionofillness,healthanddiseasethat
influencestheirmannerofhelp‐seeking.Healthisviewedasfeelinggood,well,
comfortable,freeinbodyandmindandinvolvesonefeelingcontentwithlife.The
individual'smoodindicatesthatthepersoniswell,thereisnopain,theindividual
isactiveandproductive,thereisnormalvegetativefunctioningandtheindividual
socializesappropriately.Theirpersonalorphenomenologicaldefinitionofhealth,
illnessanddiseaseisholisticandisstronglyinfluencedbytheirtraditionaland
culturalcontextandexperience.Withwesternisationandurbanisationtheprocess

199
ofacculturationisrapidlytakingplaceresultingintheintegrationofwesternviews
onhealth,illnessanddiseasewiththeirexistingview.
2 Therearecertainattitudesandbeliefsthatdirectlyinfluencebothpositiveand
negativehealthbehaviour.Whatemergesareseveralhealthbeliefsaboutthe
aetiology,treatmentandprevention.Inthisstudythefollowingbeliefsemerged:
aetiologicalbeliefs(externalancestral/evil,self‐blame,medical,physical
weaknessorbodymalfunction);treatmentbeliefs(selfmedication,medical,
prayer,holistictreatment)andthepreventativebelief(selfcare).Failuretotake
thesebeliefsintoaccountwillresultinnegativehealthbehaviours.Someofthese
beliefs,suchas,bewitchment,demonpossessionandbodyfunctioningattributed
to“somethingwrongwiththeirblood”,“dirtyorgans”and“waterinthehead”may
alsocontributetodelaysinmedicalhelp‐seekingorthetakingofsubstancesthat
couldbefataltotheindividual.Self‐medicatingandseekingofprayercanalso
delaytheseekingofmedicaltreatment.
Otherattitudesandbeliefsthatcontributedtohelp‐seekingofmedicalservices
werethatthehospitalprovidedthebestservicesforAfricans,thetreatmentwas
goodanditprovidedthebestfacilities.Thebeliefsthatthehospitalisbusyand
crowded,illnessisnotseriousenough,thatonemaygetbetterwithout
interventionanddenialofillnessalsocontributetodelaysinseekinghelp.
3 TheHospitalGroupdidnotsignificantlydifferfromtheothergroupsonhealth
beliefs,socialsupport,symptomperceptionorlifeexperiences.Thissuggestthat
thosewhoseekmedicalhelpdonothaveapeculiarprofile.Rather,thereare
severalhealthbeliefswhichinteractinacomplexwayandmayleadtomedical
help‐seeking.
4 Healthactionwasfoundtobeinfluencedbysignificantindividualsinthesubject's
environment.Theyareusuallymothers,spouses,friends,familyaswellas

200
employersanddoctors.Theseindividualsplayanimportantpartinhelpingthe
individualunderstandhisorhersymptomsaswellastheseekingofhelp.
5 Demographicvariables,suchas,age,sex,educationandurbanisationstrongly
influencethehealthandillnessbeliefs.Youngeradults,withhighereducationand
whohavelivedlongerinurbanenvironmentstendtousewesternmodesof
treatmentsmorereadily.Withregardstosexitwasfoundthatmorefemales
attendedthehospital.Thehospitalattendersalsohadlowereducation,moved
recentlytourbanareasandhadasignificantlyhighernumberofunemployedor
unskilled.
6 Theseresultsvalidatedsomeofthefundamentalaspectsofthecommonwestern
healthandillnessmodels.Thissuggeststhatthesemodelsmaybeadaptedforuse
intheAfricancontext.Localresearchlikethisonecan,therefore,beintegrated
intoresearchalreadydoneinordertobeusedlocally.
7 Theuseofservicesandfacilitiesaredeterminedbythelocation,accessibilityand
thequalityofservices.Individualswilluseservicesandfacilitiesthatareclosestto
themandwhichtheyperceiveasprovidingagoodservice.Generally,subjects
werepleasedwiththetreatmenttheyreceivedatthehospitals.Theaspectsthat
subjectswerenotpleasedaboutweredoctor‐patientrelationships,pooror
inadequatefacilities,timedelaysandillnessnotcured.
8 Therewerecertainbarriersthatnegativelyaffectedhelp‐seeking.Thesewere
financialcosts,time,transport,lackofcommunitysupports(suchas,creches,lack
ofplacestoleavechildreninordertoattendthehospitalandnoonetoaccompany
thosethatareveryill),noearlyappointmentsavailableatthehospitalsandother
priorities,suchas,workandschool.
9 Symptomshavebeenidentifiedasa“triggerfactor”orprecipitantofhelp‐seeking.
Bothphysicalandpsychologicalsymptomatologyareexperiencedandrecognised.
Almost50percentwerenotabletoassociatethesymptomswithadisorder.
201
10 Patientsusedmedicationsthattheyobtainedfromdoctorsorapharmacy.The
subjectsalsoacknowledgedtheuseofvitaminsupplementsforincreasingtheir
strength,toimprovetheirhealth,makethemactive,protectthemfromillnesses
anddiseasesandasabloodsupplement.
11 Individualsuseotherformsoftreatmentsindependentofmedicaltreatments.A
significantlyhighnumberareChristianwhouseprayerandsoconsulttraditional
healersand/orfaithhealersaswell.Traditionalorculturaltreatmentscost
betweenR68.23toR95.29.Subjectsgenerallyconsulttraditionalhealersforabout
threetimesandthereafterthereisadeclineinattendance.Ofthosethatused
thesetreatmentsbetween40to80percentfoundthembeneficialandindicated
thattheywillcontinuetraditionaltreatment.
12 Amodelofhelp‐seekingforurbanAfricans.Thismodelexplainstheprocess
involvedintheseekingofhelpwhenill.
Theseresultsdemonstratetheimportanceofstudyofhealthandillnessbehaviourwithin
theSouthAfricancontext.Itisobviousthatoneoftheimportantrolesoftheclinical
psychologistinSouthAfricaistheresearchandpracticeofpsychologyinhealthsettings.
Thisisespeciallyimportantsincethehealthsystemofthecountryispresentlybeing
dismantledbecausetheexistinghealthstructures,whichweredevelopedonracial
segregation,havenowbeenrejected.WiththeannouncementoftheStatePresidentthat
healthistobecomeafunctionofgeneralaffairsfromthe1April1993(DailyNews,30
January1993),itisessentialthatinthedevelopmentandre‐structuringofanhealth
systemthattheperspectivesofclinicalpsychologistsaretakenintoaccount.Clinical
psychologistscanplayanimportantfunctioninbothpolicy‐makingandinthestructuring
andplaningofhealthcarefacilities(fromwhichtheyhavebeenleftoutinthepast)by
applyingtheirknowledgeandskillsinhealthpsychology.Suchanapproachisadoptedat
theSub‐DepartmentofMedicallyAppliedPsychology,DepartmentofPsychiatry,Faculty

202
ofMedicine,UniversityofNatal,Durban,wherethepsychologists,aspartofthere
functionattheMedicalSchool,areinvolvedinpolicymaking.Itishopedthatsucha
situationisexpandedtootherpartsofthecountry.
Clinicalpsychologistscanalsoplayanimportantfunctioningeneralhospitalsandmedical
schools.Inotherpartsoftheworldtherehasbeenanincreaseintheemploymentof
psychologistsinhealthrelatedfields(GentryandMatarazzo,1981;Horwardetal.,1986;
Millon,1982;Sweetetal.1991).WhilethisisstilltobecomeatrendinSouthAfrica,the
roleofpsychologyinthiscountryisalsoundergoingcriticalreview.AttherecentPASA
annualgeneralmeetingtherewasarecommendationthattheorganisationdisbands
becauseofinter aliaitslackofrelevanceforthepresentcontextofachangingsociety.
Whiletherelevanceofthetraditionalroleofpsychologistmaybequestionedthereis
evidenceinthispresentresearchthatpsychologistsinthiscountrymayhaveaspecialrole
toplayinthefieldofhealth.
Thispresentresearchsupportstheviewthat,althoughdifficult,cross‐culturalresearchin
healthpsychologycanandmustbeundertaken.Moreresearchofthisnaturecanonly
helptoprovidebettercareandtreatmenttothemanyinourcountrythathavebeen
disenfranchised.Inaddition,researchofthiskindwillcontributetorapidlyequalisethe
imbalancesthatpresentlyexist.Studiesofthiskindwillalsohelpinthedevelopmentof
newaswellasthestandardisingof,researchinstrumentsinhealthpsychologywithinthe
SouthAfricancontext.
Itishopedthatthispresentresearchwillcreateinterestintheareaofpsychologyasitis
appliedtohealthandillnessinSouthAfrica.Specificareasofhealthandillnesscanbe
selectedandstudiedwithintightlycontrolledresearchdesignsthusprovidinginsightsfor
thetreatmentofAfricansinthiscountry.

203
REFERENCES

204
Aday,L.A.&Anderson,R.(1974).Aframeworkforthestudyofaccesstomedicalcare.
Health Services Research,9,pp.208‐220.
Adepoju,A.(1974).Migrationandsocio‐economiclinksbetweenurbanmigrantsandtheir
homecommunitiesinNigeria.Africa,64,pp.383‐396.
Anderson,R.(1968).A Behavioural Model of Families' Use of Health Services.Chicago:
UniversityofChicago.
Andersson,N.&Marks,S.(1988).Apartheidandhealthinthe1980's.Social Science and
Medicine,27,pp.667‐681.
Belloc,N.B.&Breslow,L.(1972).Relationshipofphysicalhealthstatusandhealth
practices.Preventative Medicine,1,pp.409‐421.
Berkanovic,E.&Reeder,L.G.(1974).Canmoneybuytheappropriateuseofservices?
Somenotesonthemeaningofutilizationdata.Journal of Health and Social Behaviour,15,
pp.93‐99.
Berkanovic,E.&Telesky,C.(1985).Mexican‐American,Black‐AmericanandWhite‐
Americandifferencesinreportingillness,disabilityandphysicianvisitsforillness.Social
Science and Medicine,20,pp.567‐577.
Berki,S.E.&Ashcraft,M.L.(1979).Ontheanalysisofambulatoryutilization:An
investigationoftherolesofneed,accessandpriceaspredictorsofillnessand
preventativevisits.Medical Care,17,1163‐1181.
Biesheuvel,S.(1959).The Development of Personality in African Cultures.Confidential
Report.Johannesburg;NationalInstituteforPersonalResearch.

205
Billings,A.G.&Moos,R.H.(1981).Theroleofcopingresponsesandsocialresponsesin
attenuatingtheimpactofstressfullifeevents.Journal of Behavioural Medicine,4,pp.139‐
157.
Bishop,G.D.(1984).Gender,roleandillnessbehaviorinamilitarypopulation.Health
Psychology,3,pp.519‐534.
Bishop,G.D.&Converse,S.A.(1986).Illnessrepresentations:Aprototypeapproach.
Health Psychology,5(2),pp.95‐114.
Braunstein,J.J.(1981).Conceptsofhealth,illnessanddisease.InBraunsteinJ.J.,Toister
R.P.(Eds). Medical Applications of the Behavioural Sciences.YearBookMedical
Publishers:Chicago.
Brennan,J.F.(1986).History and systems of psychology.(2ndeds)EnglewoodCliffs,New
Jersey:SimonandSchuster.
Briscoe,M.H.(1990).A researcher's guide to scientific and Medical Illustrations.New
York:SpringerVerlag.
Brislin,R.W.(1980).Translationandcontentanalysisoforalandwrittenmaterial.InT.
TriandisandT.W.Berry(Eds),Handbook of Cross‐cultural Psychology. Vol II,Methodology.
Boston:Allyn&BaconInc.
Buch,E.(1987).CurrentfacilitiesinthehealthsectorinSouthAfrica.InC.P.Owen(Ed),
Towards a National Health Service. Proceedingsofthe1987NAMDAAnnualConference.
CapeTown:NAMDAPublications.
Cheetam,R.W.S&Cheetam,R.J.(1976).Conceptsofmentalillnessamongsttherural
XhosapeopleinSouthAfrica.Australian and New Zealand Journal of Psychiatry,10,pp.
39‐45.

206
Cheetham,R.W.S.&Griffiths,J.A.(1980).ChangingpatternsofpsychiatryinAfrica.
South African Medical Journal,51,pp.166‐168.
Chetty,K.(1990).TheprovisionofhospitalsandclinicsinSouthAfrica:Somestepsto
redresstheproblems.AreportontheMaputoConference,April1990.Critical Health,31,
pp.21‐23.
Christie,D.&Lawrence,L.(1978).Patientsandhospitals:Astudyoftheattitudesofstroke
patients.Social Science and Medicine,12,pp.49‐51.
Christman,N.J.&Kleinman,A.(1983).Popularhealthcare,socialnetworksandcultural
meanings:Theorientationofmedicalanthropology.InD.Mechanic(Ed).Handbook of
Health, Health Care and the Health Professions.NewYork:FreePress.
Clymer,R.,Baum,A.&Krantz,D.S.(1984).PreferenceforSelf‐Careandinvolvementin
HealthCare.Handbook of Psychology and Health, 4,NewJersey:LawrenceErlbaumAssoc.
Cohen,S.&McKay,G.(1984).Socialsupport,stressandbufferinghypothesis:A
theoreticalanalysis.InA.Baum,J.E.Singer&S.E.Taylor(Eds). Handbook of Psychology
and Health,4,NewJersey:LawrenceErlbaumAssoc.
Cohen,S.&Syme,S.L.(1985).Social Support and Health.London:AcademicPress.
Coppo,P.,Pisani,L.&Keita,A.(1992).Perceivedmorbidityandhealthbehaviourina
dogonecommunity.Social Science and Medicine,34,pp.1227‐1235.
Cott,A.(1986).Thedisease‐illnessdistinction:Amodelforeffectiveandpractical
integrationofbehaviouralandmedicalsciences.InS.McHugh&T.M.Vallis(Eds).Illness
Behaviour. A Mulitidisciplinary Model.NewYork:PlenumPress.

207
Cummings,K.M.,Becker,M.H.&Maile,M.C.(1980).Bridgingthemodelstogether:An
empiricalapproachtocombiningvariablesusedtoexplainhealthaction.Journal of
Behavioural Medicine,3(2),pp.123‐145.
Davis,D.L.(1984).Medicalmisinformation:Communicationbetweenoutput
Newfoundlandwomenandtheirphysicians. Social Science and Medicine,18,pp.273‐278.
Dawes,A.(1990).Theeffectsofpoliticalviolenceonchildren:aconsiderationofSouth
Africanandrelatedstudies. International Journal of Psychology,25,pp.13‐31.
DeBeer,F.E.(1980).Meerdoelige opname onder swartes in stedelike gebiede, 1978.
Besoek aan toordokters.Pretoria:HumanScienceResearchCouncilPublication.
DeBeer,C.(1984).The South African disease: Apartheid, Health and Health
Services.Johannesburg:SouthAfricanResearchServices.
Diaz‐Guerrero,R.(1984)Behaviouralhealthacrosscultures.InJ.D.Matarazzo,J.A.Herd,
N.E.Miller&S.M.Weiss(Eds.), Behavioural Health: A Handbook of Health Enhancement
and Disease Prevention.NewYork:Wiley.
Dyer,C.,Adams,E.B.,Seedat,A.M.&Morfopoulos,J.(1986).FiftyyearsatKingEdward
VIIIHospital,Durban.South African Medical Journal,70,pp.684‐687
Edwards,S.D.,Grobbelaar,P.W.,Nene,L.M.,Makunga,N.V.,Kunene,S.T.&Sibaya,P.
T.(1983).Reaction to Illness and Concepts of Mental Illness among Representative
Samples of Rural, Urban and University Educated Black People.Publicationseriesofthe
UniversityofZululand,SeriesB,No26.
Eisenberg,L.(1986).Arepsychiatricdisorders“real”?InS.McHughandM.Vallis(Eds),
Illness Behaviour. A Multidisciplinary Model.NewYork:PlenumPress.

208
Engel,G.L.(1977).Theneedforanewmedicalmodel:achallengeforbiomedicine.
Science,196,pp.129‐136.
Engel,G.L.(1980).Theclinicalapplicationofthebiopsychosocialmodel.American Journal
of Psychiatry,137,pp.535‐544.
Fabrega,H.(1973).Towardamodelofillnessbehaviour.Medical Care,11,pp.470‐484
Farge,E.J.(1978).MedicalorientationamongaMexican‐Americanpopulation:Anoldand
anewmodelreviewed.Social Science and Medicine,12,pp.277‐282.
Feuerstein,M.,Labbé,E.E.&Kuczmierczyk.,A.R.(1987).Health psychology. A
Psychobiological Perspective.NewYork:PlenumPress.
Fiore,M.,Novotny,T.E.,Pierce,J.P.,Hatziandreu,E.J.,Patel,K.M.&Davis,R.M.(1989).
TrendsincigarettesmokingintheUnitedStates.Journal of American Medical Association,
261,pp.49‐55.
Fitzpatrick,R.&Scambler,G.(1984).Socialclass,ethnicityandillness.InR.Fitzpatrick,J.
Hinton,S.Newman,G.Scambler&J.Thompson(Eds),The Experience of Illness.NewYork:
TavistockPublicationsLtd.
Franks,P.,Campbell,T.L.&Sheilds,C.G.(1992).Socialrelationshipsandhealth.The
relativerolesoffamilyfunctioningandsocialsupport. Social Science and Medicine,34,pp.
779‐788.
Freeman,M.&Motsei,M.(1992).PlanninghealthcareinSouthAfrica—istherearole
fortraditionalhealers?Social Science and Medicine,34,pp.1183‐1190.
Garro,L.(1986).Decision‐makingmodelsoftreatmentchoice.InS.McHughandM.Vallis
(Eds),Illness Behaviour. A Multidisciplinary Model.NewYork:PlenumPress.

209
Geersten,R.,Klauber,M.R.,Rindflesh,M.,Kane,R.L.&Gray,R.(1975).Are‐examination
ofSchuman'sviewonsocialfactorsinhealthcareutilization. Journal of Health and Social
Behaviour,16,pp.226‐237.
Geertsen,R.(1988).Socialgroupcharacteristicsandhealthbehaviour.InD.S.Gochman
(Ed),Health Behaviour. Emerging Research Perspectives.NewYork:PlenumPress.
Gentry,W.D.&Matarazzo,J.D.(1981).Medicalpsychology:Threedecadesofgrowthand
development.InC.K.ProkopandL.A.Bradly(Eds), Medical Psychology. Contributions to
Behavioural Medicine.NewYork:AcademicPress.
Gochman,D.S.(1982).Labels,systemsandmotives:Someperspectivesforfuture
research.InD.S.&G.S.Parcel(Eds.),Children'shealthbeliefsandhealthbehaviours
[Specialissue].Health Education Quarterly,9,pp.167‐174.
Gochman,D.S.(1988).Health Behaviour. Emerging Research Perspectives.NewYork:
PlenumPress.
Good,B.(1986).Explanatorymodelsandcare‐seeking.InS.McHughandM.Vallis(Eds),
Illness Behaviour. A Multidisciplinary Model.NewYork:PlenumPress.
Gore,S.(1978).Theeffectofsocialsupportinmoderatinghealthconsequencesof
unemployment.Journal of Health and Social Behaviour,19,pp.157‐165.
Guttmucher,S.&Elinson,J.(1971).Ethno‐religiousvariationsinperceptionsofillness:The
useofillnessasanexplanationfordeviantbehaviour.Social Science and Medicine,5,
pp.117‐125.
Haefer,D.P.(1974).Thehealthbeliefmodelandpreventivedentalbehaviours.Health
Education Monographs,2(4),pp.420‐432.

210
Harris,D.M.&Guten,S.(1979).Healthprotectivebehaviour:Anexploratorystudy.
Journal of Health and Social Behaviour,20,pp.17‐29.
Henderson,S.,Duncan‐Jones,P.,McAulley,M.&Ritchie,K.(1978).Thepatient'sprimary
group.British Journal of Psychiatry,132,pp.74‐86.
Henderson,S.,Byrne,D.G.,Duncan‐Jones,P.,Scott,R.&Adcock,S.(1980).Social
relationships,adversityandneurosis:Astudyofassociationsinageneralhospitalsample.
British Journal of Psychiatry,136,pp.574‐583.
Hershey,J.C.,Luft,H.S.&Gianaris,J.M.(1975).Makingsenseoutofutilizationdata.
Medical Care,13,pp.838‐853.
Hibbard,J.H.&Pope,C.R.(1983).Genderroles,illnessorientationandtheuseofmedical
services.Social Science and Medicine,17,pp.129‐137.
Hochbaum,G.(1958).Publicparticipationinmedicalscreeningprograms:Asociological
study.Public Health Service Publications No.572.WashingtonD.C.
Holmes,T.H.&Rahe,R.H.(1967).Thesocialreadjustmentratingscale.Journal of
Psychosomatic Research.11,pp.213‐218.
House,J.S.,Landis,K.R.&UmbersonD.(1988).Socialrelationship.Health Science,241,
pp.540‐544.
Howard,A.,Pion,G.,Gottfriedson,G.,Flattau,P.,Oskamp,S.,Pfafflin,S.,Bray,D.and
Burstein,A.(1986).ThechangingfaceofAmericanpsychology:Areportfromthe
committeeonEmploymentandHumanResources.American Psychologist,41,pp.13311‐
1327.

211
Hunt,S.(1988)Measuringhealthinclinicalcareandclinicaltrials.InTeelingSmith,G.
(Eds.),Measuring Health: A Practical Approach.Chichester:Wiley.
Irvine,S.H.(1969).FactorAnalysisofAfricanabilitiesandattainments:constructsacross
culture.Psychological Bulletin,71(1),pp.20‐32.
Janz,N.K.&Becker,M.H.(1984).Thehealthbeliefmodel:Adecadelater.Health
Education Quarterly,11(1),pp.1‐47.
Kasl,S.V.,&Cobb,S.(1966b).Healthbehaviour,illnessbehaviourandsickrolebehaviour
II.Archives of Environmental Health,12,pp.531‐541.
Kasl,S.V.,&Cobb,S.(1966a).Healthbehaviour,illnessbehaviourandsickrolebehaviour
I.Archives of Environmental Health,12,pp.246‐266.
Kellner,R.(1986).Thetreatmentofsomatization.InS.McHughandM.Vallis(Eds),Illness
Behaviour. A Multidisciplinary Model.NewYork:PlenumPress.
Kessler,C.R.&McLoed,J.D.(1985).Socialsupportandmentalhealthincommunity
samples.InS.Cohen&S.L.Syme(Eds),Social Support and Health.London:Academic
Press.
Kimble,G.&Schlesinger,K.(1985a).Topics in the History of Psychology, Vol I.Hillsdale,
NewJersey:Erlbaum
Kimble,G.,&Schlesinger,K.(1985b).Topics in the History of Psychology, Vol II.Hillsdale,
NewJersey:Erlbaum
Kleinman,S(1986).IllnessMeaningsandIllnessBehaviour.InS.McHugh&T.M.Vallis
(Eds).Illness Behaviour. A Mulitidisciplinary Model.NewYork:PlenumPress.

212
Kleinman,A.&Sung,L.H.(1979).Whydoindigenouspractitionerssuccessfullyheal?
Social Science and Medicine,13,pp.7‐26.
Knowles,J.H.(1977).Doing Better and Feeling Worse:Health in the United States.New
York:Nortan.
Koss,M.P.&Woodruff,W.J.(1991).Emergingissuesinwomen'shealth.InJ.J.Sweet,R.
H.Rozensky&S.M.Tovain(Eds), Handbook of Clinical Psychology in Medical Settings.
NewYork:PlenumPress.
Krige,D.(1990).Thebasicneedsapproachtodevelopment:Thequestionofhealthcare
forblackpeopleinNatal.Development Southern Africa,7(1),pp.53‐66.
Kuhn,T.S.(1962).The Structure of Scientific Revolutions.Chicago:UniversityofChicago
Press.
Lave,J.R.,Lave,L.B.,Leinhardt,S.&Nagin,D.(1979).Characteristicsofindividualswho
identifyaregularsourceofmedicalcare.American Journal of Public Health,69,pp.261‐
267.
Laventhall,H.,Meyer,D.&Narenz,D.(1980).Thecommonsenserepresentationofillness
danger.InS.Rachman(Ed),Contributions to Medical Psychology, Vol. 2.Oxford:Pergamon
Press.
LeRoux,G.(1973).PsychopathologyinBantuCulture.South Africa Medical Journal,47,
pp.2077‐2086.
Leeb,W.andRadford,J.(1987a).ResearchintheBlackTownshipofMpophomeni:Isthere
hope?Reality,19(1),pp.17‐20

213
Leeb,W.andRadford,J.(1987b)The Sarmcol Struggle and the Effects of Job Loss in the
Community of Mpophomeni.UniversityofNatal,Pietermaritzburg:DepartmentofAdult
EducationandPsychology.
Lendt,L.A.(1960).A Social History of Washington Heights, New York City.NewYork:
Columbia‐WashingtonHeightsCommunityMentalProject.
Levenstein,J.H.(1990).Symptominterpretation:Thecruxoftheclinicalcompetence.
South African Family Practice,Feb,pp.54‐56.
Leventhal,H.(1986).Symptomreporting:afocusonprocess.InMcHugh,S.&Vallis,T.M.
(Eds). Illness Behaviour. A Multidisciplinary Model. NewYork:PlenumPress.
Levi,L.(1972).Introduction:Psychosocialstimuli,psychophysiologicalreactions,and
disease.InL.Levi(Ed),Stress and Distress in Response to Psychosocial Stimuli.Oxford:
PergamonPress.
Lewis,C.E.,Fein,R.&Mechanic,D.(1976).A Right to Health: the Problem of Access to
Primary Medical Care.NewYork:Wiley‐Interscience.
Li,V.C.,Wong,G.C.,Qiu,S.Cao,F.,Li,P.&Sun,J.(1990).Characteristicsofwomenhaving
abortionsinChina.Social Science and Medicine,31,pp.445‐453.
Luft,H.S.,Hershey,J.C.&Morrell,J.(1976).Factorsaffectingtheuseofphysicianservices
inaruralcommunity.American Journal of Public Health,66,pp.865‐871
Maforah,N.F.(1988).ThechangingRoleoftheBlackFamilyanditsAdaptationtopresent
Needs. Journal of Social Work,38,pp.262‐269.
Manganyi,N.C.(1977).Alienation and the Body in a Racial Society.USA:NokPublishers.
214
Matarazzo,J.D.(1982).Behaviouralhealth'schallengetoacademic,scientificand
prefessionalpsychology.American Psychologist,371(1),pp.1‐14.
Matthews,K.A.,Siegel,J.M.,Kuller,L.H.,Thompson,M.&Varat,M.(1983).
Determinantsofdecisionstoseekmedicaltreatmentbypatientswithacutemyocardinal
infarctionsymptoms.Journal of Personality and Social Psychology,44,pp.1144‐1156.
Mayou,R.(1986).Theuseofillnessbehaviourconceptsinpsychiatry.InS.McHughandM.
Vallis(Eds),Illness Behaviour. A Multidisciplinary Model.NewYork:PlenumPress.
McClain,C.(1977).Adaptioninhealth:ModernandtraditionalmedicineinaWest
Mexicancommunity.Social Science and Medicine,11,pp.341‐347.
McFarlane,A.H.,Neale,K.A.,Norman,G.R.,Roy,R.G.&Streiner,D.L.(1981).
Methodologicalissuesindevelopingascaletomeasuresocialsupport.Schizophrenia
Bulletin,7,pp.90‐100.
Mechanic,D.(1992).HealthandIllnessbehaviourandpatient‐practitionerrelationships.
Social Science and Medicine,34,pp.1345‐1350.
Mechanic,D.(1983).Theexperienceandexpressionofdistress.Thestudyofillness
behaviorandmedicalutilization.InD.Mechanic(Ed)Handbook of Health, Health Care and
the Health Professionals.NewYork:FreePress.
Mechanic,D.(1978).Medical Sociology.(2nded.).NewYork:FreePress
MechanicD.(1976a).The growth of Bureaucratic Medicine: An inquiry into the Dynamics
of Patient Behavior and the Organization of Medical Care.NewYork:Wiley‐Interscience.
MechanicD.(1976b)Sex,illnessbehaviourandtheuseofhealthservices.Journal of
Human Stress,2,pp.29‐40.

215
MechanicD.(1976c).Stress,illnessandillnessbehaviour.Journal of Human Stress,2,pp.
2‐6.
Mechanic,D.(1986).Illnessbehaviour:Anoverview.InS.McHugh&T.M.Vallis,(Eds.),
Illness Behaviour. A Multidisciplinary Model.NewYork:Plenum.
MillonT.(1982).OnthenatureofClinicalHealthPsychology.InT.Millon,C.J.Green&R.
B.Meager(Eds), Handbook of Clinical Health Psychology.NewYork:Plenum.
Mills,J.(1983).Health, Healing and Dis‐ease in a South African Township.UnpublishedM
AThesis.UniversityofCapeTown.
Mills,J.(1985).ThePossessionstateofIntwaso:AnAnthropologicalRe‐appraisal.South
African Journal of Sociology,16,pp.9‐13.
Moller,V.(1988)UnemploymentandIll‐Being.Con‐text,1,pp.81‐96.
Msengi,N.P.&Daynes,G.(1981).CommunityresponsetomentalillnessinTranskei.
South African Medical Journal,59,47‐49.
Murabak,K.,Shafqat,S.,Malik,U.andQureshi,A.F.(1990).Health,attitudesandbeliefs
ofworkingwomen. Social Science and Medicine,31,pp.1029‐1033).
Nathanson,C.(1977).Sex,IllnessandMedicalCare:AReviewofdata,theoryandmethod.
Social Science and Medicine,11,pp.13‐26.
NationalMedicalandDentalAssociation(1987)Towards a National Health Service.Annual
Conference.

216
Ngubane,H.(1977)Body and Mind in Zulu Medicine: An Ethnography of Health and
Disease in Nyuswa‐Zulu Thought and Practice.London:AcademicPress.
Nicholas,K.(1983).Psychologicaltherapyandpersonalcrises—thecareofphysicallyill
people.InD.Pilgram(Ed). Psychology and Psychotherapy. Current Trends and Issues.
London:RoutledgeandKeaganPaul.
Okafor,S.I.(1983).Factorsaffectingthefrequencyofhospitaltripsamonga
predominantlyruralpopulation.Social Science and Medicine,17,pp.591‐595.
Oosthuizen,G.C.(1986).Religion Alive. Studies in the new Movements and the Indigenous
Church in Southern Africa.Johannesburg:Hodder&Stoughton.
Östergren,P.‐O.,Hanson,S.‐O.&Trjler,L.(1991).Socialnetwork,socialsupportand
acutechestcomplaintsamongyoungandmiddle‐agedpatientsinanemergency
department—casecontrolstudy. Social Science and Medicine,33,pp.257‐267.
Parsons,T.(1951).The Social System.Illinois:FreePress.
Pennebaker,J.W.(1982).The Psychology of Physical Symptoms.NewYork:Springer‐
Verlag.
Pillay,B.J.,Naidoo,P.&Tlou,E.(1992).AstudyofsuicidalBehaviourataGeneral
Hospital.InL.Schlebusch(Ed),Suicidal Behaviour 2.ProceedingsoftheSecondSouthern
AfricanConferenceonSuicidology,IllovoBeach,SouthAfrica.
Pillay,B.J.,Schlebusch,L.andLouw,J.(1992).Illnessbehaviourinliverelatedandcadaver
renaltransplantrecipients.South African Medical Journal,81,pp.411‐415.

217
Pilowsky,I.(1986).Abnormalillnessbehaviour:areviewoftheconceptandits
implications.InS.McHughandM.Vallis(Eds),Illness Behaviour. A Multidisciplinary Model.
NewYork:PlenumPress.
Popper,K.R.(1959).LogicofScientificDiscovery.London:Hutchinson.
Rosenstock,I.M.(1974).Historicaloriginsofthehealthbeliefmodel.Health Education
Monographs,2(4),pp.328‐335.
Price,M.(1988).Theconsequenceofhealthserviceprivatisationforequalityandequityin
healthcareinSouthAfrica.Social Science and Medicine,27,pp.703‐716.
Radford,E.J.,andLeeb,W.(1986).An Investigation into the Effects of Job Loss on the
African Township of Mpophomeni.UniversityofNatal,Pietermaritzburg:Departmentof
Psychology.
Rahe,R.H.&Lind,E.(1971).Psychosocialfactorsandsuddencardiacdeath:Apilotstudy.
Journal of Psychosomatic Research,15,pp.19‐24.
Rahe,R.H.&Arthur,R.J.(1978).Lifechangesandillnessstudies:pasthistoryandfuture
directions. Journal of Human Stress,4(1),pp.3‐15.
Reddy,J.(1990).Dental health policy in South Africa. Health Priorities for the 1990's.
ProceedingsoftheNationalMedicalandDentalAssociation7thNationalConference,July
1990.
Reeder,L.G.&Berkanovic,E.(1973).Sociologicalconcomitantsofhealthorientations:a
partialreplicationofSchuman.Journal of Health and Social behaviour,14,pp.134‐143.
Remple,H.(1971).Therural‐to‐urbanimmigrantinKenya.African Urban Notes,6,pp.
53‐72.

218
Retief,A.(1988).Method and Theory in Cross‐cultural Psychological Assessment.Human
ScienceResearchCouncil.InvestigationintoResearchMethodology.Researchreport
series:6.
Richardson,A.(1980).Attitudes.InJ.C.Coleman(Ed), Introduction to Psychology. A Text
book for Health Students.RoutledgeandKeaganPaul:London.
Ritter,C.(1988).Socialsupports,socialnetworks,andhealthbehaviours.InD.S.Gochman
(Ed),Health Behaviour. Emerging Research Perspectives.NewYork:PlenumPress.
Roghman,K.J.&Haggerty,R.J.(1972).Thediaryasaresearchinstrumentinthestudyof
healthandillnessbehavior.Medical Care,10,pp.143‐163.
Rosenstock,I.M.(1974).Thehealthbeliefmodelandpreventionhealthbehaviour.Health
Education Monographs,2,pp.354‐386.
Rotter,J.B.,Chance,J.&Phares,E.J.(1972).Application of Social Learning Theory of
Personality.NewYork:Holt,Rinehart&Winston.
Rotter,J.B.(1966).Generalizedexpectanciesforinternalversusexternalcontrolof
reinforcement.Psychological Monographs,80(1),pp.247‐355.
Sarason,I.G.,Johnson,J.H.&Siegel,J.M.(1978).Assessingtheimpactoflifechanges:
DevelopmentoftheLifeExperienceSurvey.Journal of Consulting and Clinical Psychology,
46(5),pp.932‐946.
Sarason,I.G.,Sarason,B.R.,Potter,E.H.&Antoni,M.H.(1985).Lifeevents,social
supportandillness.Psychosomatic Medicine,47,pp.156‐163.
Schaefer,C.,Coyne,J.C.&Lazarus,R.S.(1981).Thehealth‐relatedfunctionsofsocial
support.Journal of Behavioural Medicine,4,pp.381‐406.
219
Schlebusch,L.(1989). Mind‐body Synthesis. The Interactive Health Care Equation.
UniversityofNatalPress:Pietermaritzburg.
Schlebusch,L.,Pillay,B.J.&Louw,J.(1989).Depressionandself‐reportdisclosureafter
liverelatedandcadaverrenaltransplants.South African Medical Journal,75,pp.490‐493.
Schlebusch,L.(1990).PsychologicalConceptsinDiseaseandHealth.InL.Schlebusch(Ed),
Clinical Health Psychology. A Behavioural Perspective.SouthernBookPublishers:Halfway
House.
Schlebusch,L.Wessels,W.H.&Rzadkowolsky,A.(1990).Cross‐culturalindicatorsofhelp‐
seekingbehaviourinaggressivegeneralhospitalpatients.South African Journal of
Psychology,20(4),pp.223‐234.
Schlebusch,L.(1987).MedicalpsychologyinSouthAfrica:Futureconcernsinthegeneral
teachinghospital.South African Journal of Psychology,17,pp.110‐113.
Schlebusch,L.&Simpson,M.A.(1987).MedicalPsychology.Itsgrowthanddevelopment
inmedicalschoolsinsouthernAfrica.South African Medical Journal,20,pp.413‐416.
Schlebusch,L.(1983b).Thetrainingofinternsinmedicalpsychologyonaconsultation
serviceinageneralhospital,Psychotherapeia,28,pp.18‐21.
Schlebusch,L.(1983a).Consultation‐liasonclinicalpsychologyinmoderngeneralhospital
practice.South African Medical Journal,64,pp.781‐786.
Schlebusch,L.(1988).Parasuicide:across‐culturalcomparison.InLSchlebusch(Ed)
Suicidal Behaviour.ProceedingsofthefirstSouthernAfricanConferenceonSuicidology.
Durban:Sub‐Dept.ofMedicallyAppliedPsychology,FacultyofMedicine,Universityof
Natal,Durban.

220
Schlebusch,L.&Wessels,W.H.(1986).Establishmentofthefirstdepartmentofmedically
appliedpsychologyataSouthAfricanmedicalschool.Educationinnovationswithinthe
SouthAfricanmedicalschools,1980‐1985.SouthernAfricanAssociationMedical
Education Newsletter,4,p.29.
Schlemmer,L.&Stopforth,P.(1979).A Guide to the Coding of Occupations in SouthAfrica.
UniversityofNatal:CentreforAppliedSocialSciences.
Selye,H.(1956).The stress of life.NewYork:McGraw‐Hill.
ShadowoftheGallows.30January1993.Daily News
Steptoe,A.(1991).Invitedreview:Thelinksbetweenstressandillness.Journal of
Psychosomatic Research,35(6),pp.633‐644.
Stone,G.C.(1979).Psychologyandthehealthsystem.InG.C.Stone,F.Cohen,&N.E.
Adler(Eds),Health Psychology.SanFrancisco:Jossey‐bass.
Suchman,E.A.(1965b)Stagesofillnessandmedicalcare. Journal of Health and Social
Behaviour,6,pp.114‐128
Suchman,E.A.(1966).Healthorientationandmedicalcare.American Journal of Public
Health,56,pp.97‐105.
Suchman,E.A.(1965a).Socialpatternsofillnessandmedicalcare.Journal of Health and
Social Behaviour,6,pp.2‐16.
Suchman,E.A.(1972).Stagesofillnessandmedicalcare.InE.G.Jaco(Ed),Patients,
Physicians and Illness: A Sourcebook in Behavioural Science and Health.NewYork:Free
Press.

221
Sultana,F.&Hunte,P.A.(1992).Health‐seekingbehaviourandthemeaningofmedication
inBalochistan,Pakistan.Social Science and Medicine,34,pp.385‐1397.
Sundkler,B.G.M.(1976).BantuProphetsinSouthAfrica.London:OxfordUniversityPress.
Svarstad,B.L.,Cleary,P.D.,Mechanic,D.&Robers,P.A.(1987).Genderdifferencesinthe
acquisitionofofprescribeddrugs:Anepidemiologicalstudy. Medical Care,25,pp.1089‐
1098.
Sweet,J.J.,Rozensky,R.H.&Tovain,S.M.(1991).ClinicalPsychologyinMedicalsettings.
PastandPresent.InJ.J.Sweet,R.H.Rozensky&S.M.Tovain(Eds).Handbook of Clinical
Health Psychology in Medical Settings.NewYork:PlenumPress.
Tardy,C.H.(1985).Socialsupportmeasurement.American Journal of Comunity
Psychology,54,416‐423.
TheHealthSystemsettoCrumbleinNatal.9March1990.Daily News
Titkow,A.(1983).Illnessbehaviourandaction:Thepatient‐role.Social Science and
Medicine,17,637‐646.
Turner,R.J.(1981).Socialsupportasacontingencyinpsychologicalwell‐being.Journal of
Health and Social Behaviour,22,pp.357‐367.
Turton,R.W.&Chalmers,B.E.(1990).Apartheid,stressandillness:thedemographic
contextofdistressreportedbySouthAfricanAfricans.Social Science and Medicine,31,pp.
1191‐1200.
Umberson,D.(1992).Gender,mentalstatusandsocialcontrolofhealthbehaviour.Social
Science and Medicine,34,pp.907‐917.

222
Uyanga,J.(1983).Rural‐urbanmigrationandsicknesshealthcarebehaviour.AStudyof
EasternNigeria. Social Science and Medicine,17,pp.579‐583.
Verbrugge,L.M.(1985).Genderandhealth:anupdateonhypothesesandevidence.
Journal of Health and Social Behaviour,26,pp.156‐182.
.
Verbrugge,l.(1979)Femaleillnessratesandillnessbehaviour,testinghypothesisabout
sexdifferencesinhealth.Woman Health,4,p.61.
Vilakazi,A.(1962).Zulu transformations: a Study of the Dynamics of Social Change.
Pietermaritzburg:UniversityofNatalPress.
Wallston,B.S.&Wallston,K.A.(1984).Socialpsychologicalmodelsofhealthbehaviour:
Anexaminationandintergration.Handbook of Psychology and Health,4,pp.23‐53.
Wallston,K.A.&Wallston,B.S.(1981).HealthLocusofControlScales.InH.M.Lefcourt
(Ed)Research with Locus of Control Construct. Vol I. Assessment methods.London:
AcademicPress.
Wallston,B.S.,Wallston,K.A.,Kaplan,G.D.&Maides,S.A.(1976).Developmentand
validationoftheHealthLocusofControlScale. Journal of Consulting and Clinical
Psychology,44(4),pp.580‐585.
Wan,T.T.H.(1976).Predictingself‐assessedhealthstatus:Amultivariateapproach.
Health Services Research,11,pp.464‐477.
Watts,H.L.(1980).SomereactionstoillnessinUrbanblacksandIndianfamiliesinDurban
‐asumaryofanexploratorystudy.South African Medical Journal,57,pp.589‐591.
Weissman,M.M.(1975).Theassessmentofsocialadjustment:areviewoftechniques.
Archives of General Psychiatry,32,pp.357‐365.
223
Wessels,W.H.(1985c).Thetraditionalhealerandpsychiatry. Australian and New Zealand
Journal of Psychiatry,19,pp.283‐286.
Wessels,W.H.(1985b).Culturalpsychiatry:theoryandpractice.Continuing Medical
Education,3,pp.23‐26.
Wessels,W.H.(1987a).HealingwithintheAfricancontext.Psychiatric Insight,4(3),p.34.
Wessels,W.H.(1987b).NewdevelopmentsinAfricanhealingpractices.Psychiatric
Insight,4(3),p.35.
Wessels,W.H.(1984b).Transculturalaspectsofpsychiatry.InH.A.Shapiro(Ed),Medicine
and Health in Developing South Africa.CapeTown:CollegeofMedicineofSouthAfrica.
Wessels,W.H.(1985a).Understandingculture‐specificsyndromesinSouthAfrica—the
Westerndilemma.Modern Medicine of South Africa,10(9),pp.51‐63.
WesselsW.H.(1984a)TransculturalaspectsofPsychiatry.ProceedingsofInterdisplinary
SymposiumoftheCollegeofMedicineofSouthAfrica.5‐6July.
Wessels,W.H.(1983).Histeriesepsigosebyswartpasiente.Psychotherapeia,August,
pp.22‐25.
Wessels,W.H.(1989).HealingpracticesintheAfricanIndependentChurches.InG.C.
Oosthuizen,S.D.Edwards,W.H.Wessels&I.Hexham(Eds), Afro‐Christian Religion and
Healing in Southern Africa,AfricanStudiesVol.8.,Lewiston:EdwinMellenPress.
Wortman,C.B.&Conway,T.L.(1985).Theroleofsocialsupportintheadaptationand
recoveryfromphysicalillness.InS.Cohen&S.L.Syme(Eds), Social Support and Health.
London:AcademicPress.

224
Young,J.(1980).Medical Choice in a Cultural Context: Treatment Decision‐Making in a
Mexican Town.NewJersey:RutgersUniversityPress.
Zadoraznyj,M.&Svarstad,B.L.(1990).Gender,employmentandmedicationuse.Social
Science and medicine,31,pp.971‐978.
Zimet,G.D.,Dahlem,N.W.,Zimet,S.G.&Farley,G.K.(1988).Themultidimensionalscale
ofperceivedsocialsupport.Journal of Personality Assessment,52(1),pp.30‐41
Zwarenstein,M.&Bradshaw,D.(1990).An overview of health status and health care in
South Africa. The Case for a National Health Service.Aseriesoflecturesorganizedby
extra‐muralstudiesandNationalMedicalandDentalAssociation(WesternCape).
UniversityofWesternCape.
Zwi,A.,Marks,S.&AnderssonN.(1988).Health,apartheidandthefrontlinestates.Social
Science and Medicine,27,pp.661‐665.
225
APPENDIX