a thorough qt study to evaluate the ... - btk inhibitors
TRANSCRIPT
Presented online at the 2020 annual meeting of the American College of Clinical Pharmacy, October 19-30, 2020
INTRODUCTIONBruton Tyrosine Kinase (BTK)• BTK is an enzyme that plays a critical role in immune signaling pathways and is an essential signaling element
downstream of the B-cell, Fc-gamma (Fcγ), and Fc-epsilon (Fcε) receptors (Figure 1)1,2
Figure 1. Role of BTK in Innate and Adaptive Immunity
Megakaryocyte
PlateletsBTK
MicrogliaBTK
Natural killer cellBTK
T CellB cellBTK
Plasma cell
Mast cellBTK
BasophilBTK
NeutrophilBTK
EosinophilBTK
MacrophageBTK
MonocyteBTK
BTK Expression, functional inhibitionBTK Expression, no/limited functional effects
INNATE IMMUNITY ADAPTIVE IMMUNITY
Rilzabrutinib3,4
• Oral, reversible inhibitor targeting BTK and designed for immune diseases (Figure 2)• Covalent binding achieves long BTK target engagement and durable inhibition with limited drug exposure• Clinical advantage of rilzabrutinib’s rapid systemic clearance and long target residence time may prolong efficacy,
while reducing the potential for off-target toxicities
Figure 2. Rilzabrutinib Tailored Covalency™ and Inhibition of BTK4,5
PK E
xpos
ure,
ng/
mL
Time, h
PK/PD: Durable Inhibition With Low Drug Exposure
Rilzabrutinib 40 mg/kg rat2000
1000
0
BTK
Occupancy, %
100
80
60
40
20
00 5 10 15 20 25
COVALENTBINDING SITE
TARGETSITE
OFF-TARGETSITE
NON-COVALENTBINDING REGION
COVALENTBINDING REGION
• Rilzabrutinib plays a critical role in neutralization of processes in immune-mediated diseases, including B and innate immune cells, while sparing T cells (Figure 3)3,4
Figure 3. BTK Inhibition by Rilzabrutinib Within Immune Cells
T cellsB cells, plasma cells
Blocks B-cell receptorInhibits plasma cell differentiation and
antibody production
Monocyte, macrophage
Blocks IgG-mediated FcγR activation, phagocytosisInflammatory mediators
Mast cells, basophils
BTK inhibitor Rilzabrutinib
Blocks IgE-mediated FcεR activation and
degranulation
Neutrophils
Inhibits activation, adhesion, recruitment,
oxidative burst No effect
BTK BTK
BTK
BTK
BTK
BTK
METHODSStudy Objectives • Define a clinically relevant supratherapeutic rilzabrutinib
dose and to evaluate effects of therapeutic and supratherapeutic rilzabrutinib doses on ECG parameters, including Concentation-QTc (C_QTc) analysis in healthy subjects
• In vitro studies suggested that rilzabrutinib is a substrate for the cytochrome P450 enzyme CYP3A; to achieve supratherapeutic exposure, rilzabrutinib was coadministered with the potent CYP3A inhibitor ritonavir5
Two-part Phase 1 Study6,7
• Part A: Randomized, open-label, 3-period, single-dose crossover study with a single dose of rilzabrutinib 100 mg or 1200 mg, or 100 mg + ritonavir (100 mg twice daily [bid]) to define the supratherapeutic dose for Part B
• Part B: Randomized, double-blind, placebo-controlled, 4-way, single-dose crossover study with matched placebo, single dose of rilzabrutinib 400 mg alone or with ritonavir 100 mg bid, or open-label moxifloxacin (400 mg; positive control)
Inclusion Criteria• 18- to 55-year old healthy males and females (nonlactating/
not pregnant)• Body mass index 18.0–30.0 kg/m2 (inclusive) and weight
≥45 kg• Normal 12-lead electrocardiogram (ECG) and blood
pressure (BP) at screening• QTcF interval between >300 and <450 ms (men) or
<470 ms (women)
Exclusion Criteria• History of long or short QT syndrome• Resting systolic B <150 or >90 mm Hg, or diastolic B
<100 or >40 mm Hg• Resting heart rate (HR) >50 or <90 bpm at screening and
baseline (day -1)• Clinically significant medical illness
Primary Endpoints• Part A: Evaluate pharmacokinetic (PK) effects of
rilzabrutinib alone and with a strong CYP3A inhibitor; evaluate safety and tolerability to identify optimal dose for Part B thorough QTc study
• Part B: Assess the effect of therapeutic and supratherapeutic concentration of rilzabrutinib on placebo-corrected, change-from-baseline QTcF ( ΔΔQTcF)
Pharmacokinetic, Cardiac, and Safety Assessments• Fasting blood samples were obtained for plasma PK of
rilzabrutinib from 15 min through 24 h post-dose• 12-lead ECGs extracted from continuous Holter recordings
performed on day 1 in each treatment period and on day -1 of period 1
• Safety assessments included treatment-emergent adverse events (TEAEs), ECG, vital signs, and physical examination
Statistical Analysis • For the cardiodynamic ECG assessment, the primary
analysis was based on concentration-QTc modeling of the relationship between rilzabrutinib and placebo-corrected change-from-baseline QTcF (ΔΔQTcF) with the intent to exclude an effect >10 msec at clinically relevant rilzabrutinib plasma concentrations; only timepoints with matching placebo values were included in the modeling
• Categorical outliers analysis was performed for changes in HR, PR, QRS, QTc, T-wave morphology, and U-wave presence
• The effect of rilzabrutinib on ΔΔQTcF was evaluated post-dose by timepoint analysis using the intersection union test
• Assay sensitivity was evaluated using a model similar to the primary analysis
SUBJECTS• Part A included 12 healthy subjects
- 11 completed the study - 1 withdrew due to cannulation difficulty - Mean age was 26.2 y (median was 25.5 y), 67% female, 33% were male, and 75% were Caucasian
• Part B included 39 healthy subjects - 29 subjects completed all 4 treatment periods of the study - 10 subjects withdrew or discontinued from the study - Mean age was 26.9 y (median age was 24 y), 49% female, 51% were male, and 77% were Caucasian
PHARMACOKINETICS AND DRUG-DRUG INTERACTIONPart A Results• A single dose of rilzabrutinib 100 mg was rapidly absorbed under fasting conditions with mean Tmax of 1.1 h, and elimination appeared to be
multiphasic with mean t1/2 of 1.8 h (Table 1)• Combination of rilzabrutinib 100 mg with the CYP3A4 inhibitor ritonavir demonstrated 16.6-fold AUC0-∞ increase and 6.5-fold Cmax increase over
rilzabrutinib 100 mg alone (Table 1, Figure 4A)• Supratherapeutic dose of rilzabrutinib 1200 mg reached mean Tmax at 2.9 h and t1/2 by 3.1 h
- Due to mild-to-moderate gastrointestinal adverse events in 3 of 4 subjects in period 1, the 1200 mg dose of rilzabrutinib was discontinued and removed as a dosing option in periods 2–4 (subjects were able to complete remaining treatment periods and study) - Effects were not related to systemic exposure, since rilzabrutinib exposure at 1200 mg (the median AUC0-∞= 553.14 ng∙h/mL) was only slightly higher than the 400 mg dose (AUC0-∞= 312 ng∙h/mL) based on data5
Part B Results• A similar drug-drug interaction (however, with lower-fold increases in drug exposure) was observed at the 400 mg dose of rilzabrutinib, the dose
selected for QTc studies (Table 1)• Coadministration of rilzabrutinib 400 mg with ritonavir led to 8-fold AUC0-∞ and 5-fold Cmax increases compared with rilzabrutinib 400 mg alone
(Table 1, Figure 4B)• Results from Part A and B confirm the classification of rilzabrutinib as a CYP3A4 substrate
Table 1. Plasma Pharmacokinetics for Rilzabrutinib Without (Therapeutic) and With (Supratherapeutic) Ritonavir
t1/2, h Tmax, h Cmax, ng/mL AUC0-last, h∙ng/mL AUC0-∞, h∙ng/mL
Part A
Rilzabrutinib 100 mg nMean (SD)
121.8 (0.8)
121.1 (0.5)
1234 (31)
1265 (67)
1266 (67)
Rilzabrutinib 100 mg +Ritonavir 100 mg
nMean (SD)
114.0 (0.3)
112.3 (0.5)
11223 (210)
111081 (1198)
111097 (1221)
Rilzabrutinib 1200 mg n*Mean (SD)
43.1 (0.6)
42.9 (1.3)
4569 (888)
42470 (3899)
42474 (3902)
Part B
Rilzabrutinib 400 mg nMean (SD)
313.9 (2.3)
322.1 (0.9)
32144 (124)
32455 (404)
31454 (411)
Rilzabrutinib 400 mg +Ritonavir 100 mg
nMean (SD)
334.5 (0.7)
343.2 (0.8)
34712 (521)
343640 (2800)
333800 (2870)
Moxifloxacin 400 mg(positive control)
nMean (SD)
3511.1 (4.2)
362.2 (1.8)
362360 (681)
3622700 (5240)
3627400 (5250)
*A limited number of patients completed period 1 with the 1200 mg rilzabrutinib dose due to mostly mild to moderate (grade 1 or 2) gastrointestinal-related adverse events and changed dosing for periods 2–4. AUC, area under the plasma concentration-time curve from time 0 to last quantifiable timepoint or infinity (∞); Cmax, maximum peak observed concentration; t1/2, elimination half-life; Tmax, time to maximum observed plasma concentration; SD, standard deviation.
Figure 4. Concentration-Time Profiles (Mean ± SD) of Rilzabrutinib After a Single Dose ± Ritonavir
Part A: Rilzabrutinib 100 mg ± Ritonavir Part B: Rilzabrutinib 400 mg ± Ritonavir
-10
20
140
260
380
500
4 8 120
Nominal Time, h
16 20 24
Mea
n R
ilzab
rutin
ib P
lasm
a C
once
ntra
tion,
ng/
mL
Mea
n R
ilzab
rutin
ib P
lasm
a C
once
ntra
tion,
ng/
mL
-500
0
500
1000
1500
4 8 120
Nominal Time after dose, h
16 20 24
100 mg Rilzabrutinib
100 mg Rilzabrutinib + 100 mg Ritonavir
400 mg Rilzabrutinib
400 mg Rilzabrutinib + 100 mg Ritonavir
CARDIODYNAMIC EVALUATION• Mean change-from-baseline QTcF (ΔQTcF) values for both rilzabrutinib and placebo were negative at all timepoints except 16 h post-dose (Figure 5)• During the first 3 h post-dose, mean ΔQTcF on rilzabrutinib was somewhat more negative than on placebo, and thereafter, followed the placebo pattern• The upper limit of 90% CIs for placebo-corrected ΔQTcF (ΔΔQTcF) was <10 ms at all evaluated rilzabrutinib doses and post dose time points• The C-QTc relationship on rilzabrutinib was shallow and slightly negative with a slope of -0.01 ms per ng/mL (90% CI, -0.016, -0.0010) with a small intercept
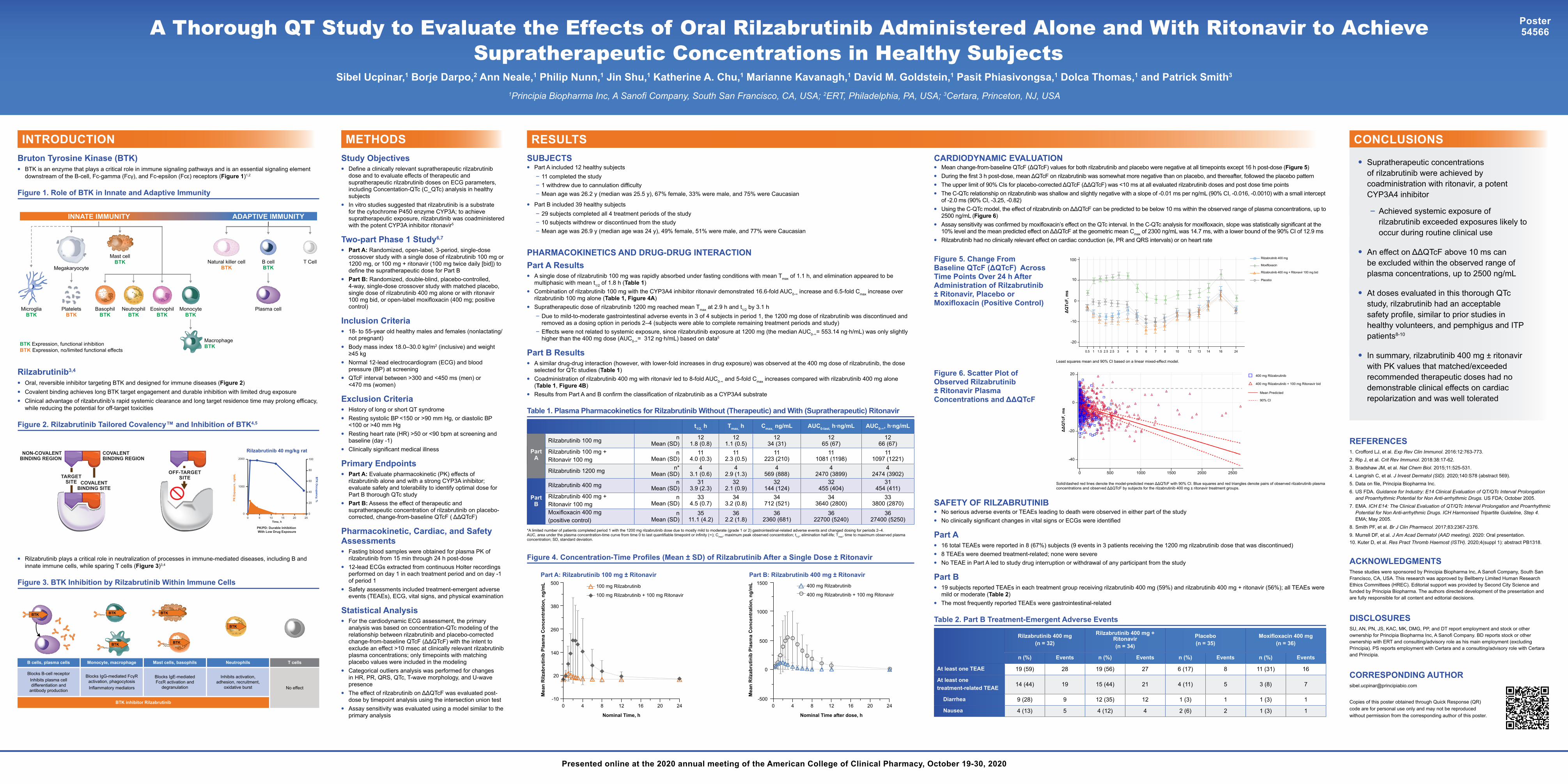
of -2.0 ms (90% CI, -3.25, -0.82)• Using the C-QTc model, the effect of rilzabrutinib on ΔΔQTcF can be predicted to be below 10 ms within the observed range of plasma concentrations, up to
2500 ng/mL (Figure 6)• Assay sensitivity was confirmed by moxifloxacin’s effect on the QTc interval. In the C-QTc analysis for moxifloxacin, slope was statistically significant at the
10% level and the mean predicted effect on ΔΔQTcF at the geometric mean Cmax of 2300 ng/mL was 14.7 ms, with a lower bound of the 90% CI of 12.9 ms• Rilzabrutinib had no clinically relevant effect on cardiac conduction (ie, PR and QRS intervals) or on heart rate
CONCLUSIONS
• Supratherapeutic concentrations of rilzabrutinib were achieved by coadministration with ritonavir, a potent CYP3A4 inhibitor
- Achieved systemic exposure of rilzabrutinib exceeded exposures likely to occur during routine clinical use
• An effect on ΔΔQTcF above 10 ms can be excluded within the observed range of plasma concentrations, up to 2500 ng/mL
• At doses evaluated in this thorough QTc study, rilzabrutinib had an acceptable safety profile, similar to prior studies in healthy volunteers, and pemphigus and ITP patients8-10
• In summary, rilzabrutinib 400 mg ± ritonavir with PK values that matched/exceeded recommended therapeutic doses had no demonstrable clinical effects on cardiac repolarization and was well tolerated
REFERENCES1. Crofford LJ, et al. Exp Rev Clin Immunol. 2016:12:763-773.2. Rip J, et al. Crit Rev Immunol. 2018:38:17-62. 3. Bradshaw JM, et al. Nat Chem Biol. 2015;11:525-531. 4. Langrish C, et al. J Invest Dermatol (SID). 2020;140:S78 (abstract 569). 5. Data on file, Principia Biopharma Inc.6. US FDA. Guidance for Industry: E14 Clinical Evaluation of QT/QTc Interval Prolongation
and Proarrhythmic Potential for Non Anti-arrhythmic Drugs. US FDA; October 2005.7. EMA. ICH E14: The Clinical Evaluation of QT/QTc Interval Prolongation and Proarrhythmic
Potential for Non Anti-arrhythmic Drugs. ICH Harmonised Tripartite Guideline, Step 4. EMA; May 2005.
8. Smith PF, et al. Br J Clin Pharmacol. 2017;83:2367-2376. 9. Murrell DF, et al. J Am Acad Dermatol (AAD meeting). 2020: Oral presentation.10. Kuter D, et al. Res Pract Thromb Haemost (ISTH). 2020;4(suppl 1): abstract PB1318.
ACKNOWLEDGMENTSThese studies were sponsored by Principia Biopharma Inc, A Sanofi Company, South San Francisco, CA, USA. This research was approved by Bellberry Limited Human Research Ethics Committees (HREC). Editorial support was provided by Second City Science and funded by Principia Biopharma. The authors directed development of the presentation and are fully responsible for all content and editorial decisions.
DISCLOSURESSU, AN, PN, JS, KAC, MK, DMG, PP, and DT report employment and stock or other ownership for Principia Biopharma Inc, A Sanofi Company. BD reports stock or other ownership with ERT and consulting/advisory role as his main employment (excluding Principia). PS reports employment with Certara and a consulting/advisory role with Certara and Principia.
CORRESPONDING [email protected]
Copies of this poster obtained through Quick Response (QR) code are for personal use only and may not be reproduced without permission from the corresponding author of this poster.
RESULTS
SAFETY OF RILZABRUTINIB• No serious adverse events or TEAEs leading to death were observed in either part of the study • No clinically significant changes in vital signs or ECGs were identified
Part A• 16 total TEAEs were reported in 8 (67%) subjects (9 events in 3 patients receiving the 1200 mg rilzabrutinib dose that was discontinued)• 8 TEAEs were deemed treatment-related; none were severe• No TEAE in Part A led to study drug interruption or withdrawal of any participant from the study
Part B• 19 subjects reported TEAEs in each treatment group receiving rilzabrutinib 400 mg (59%) and rilzabrutinib 400 mg + ritonavir (56%); all TEAEs were
mild or moderate (Table 2)• The most frequently reported TEAEs were gastrointestinal-related
Table 2. Part B Treatment-Emergent Adverse Events
Rilzabrutinib 400 mg(n = 32)
Rilzabrutinib 400 mg + Ritonavir(n = 34)
Placebo(n = 35)
Moxifloxacin 400 mg(n = 36)
n (%) Events n (%) Events n (%) Events n (%) Events
At least one TEAE 19 (59) 28 19 (56) 27 6 (17) 8 11 (31) 16
At least one treatment-related TEAE 14 (44) 19 15 (44) 21 4 (11) 5 3 (8) 7
Diarrhea 9 (28) 9 12 (35) 12 1 (3) 1 1 (3) 1
Nausea 4 (13) 5 4 (12) 4 2 (6) 2 1 (3) 1
Figure 5. Change From Baseline QTcF (ΔQTcF) Across Time Points Over 24 h After Administration of Rilzabrutinib ± Ritonavir, Placebo or Moxifloxacin (Positive Control)
Figure 6. Scatter Plot of Observed Rilzabrutinib ± Ritonavir Plasma Concentrations and ΔΔQTcF
Least squares mean and 90% CI based on a linear mixed-effect model.
-20
-10
0
10
100
0.5 1 1.5 2.5 2.5 3 4 5 6 7 8 10 12 13 14 16 24
ΔQ
TcF,
ms
Time, h
Rilzabrutinib 400 mg
Moxifloxacin
Rilzabrutinib 400 mg + Ritonavir 100 mg bid
Placebo
Solid/dashed red lines denote the model-predicted mean ΔΔQTcF with 90% CI. Blue squares and red triangles denote pairs of observed rilzabrutinib plasma concentrations and observed ΔΔQTcF by subjects for the rilzabrutinib 400 mg ± ritonavir treatment groups.
-40
0
ΔΔ
QTc
F, m
s
Rilzabrutinib Concentration, ng/mL
-20
0
20 400 mg Rilzabrutinib
400 mg Rilzabrutinib + 100 mg Ritonavir bid
Mean Predicted
90% CI
500 1000 1500 2000 2500
P P
A Thorough QT Study to Evaluate the Effects of Oral Rilzabrutinib Administered Alone and With Ritonavir to Achieve Supratherapeutic Concentrations in Healthy Subjects
Sibel Ucpinar,1 Borje Darpo,2 Ann Neale,1 Philip Nunn,1 Jin Shu,1 Katherine A. Chu,1 Marianne Kavanagh,1 David M. Goldstein,1 Pasit Phiasivongsa,1 Dolca Thomas,1 and Patrick Smith3
1Principia Biopharma Inc, A Sanofi Company, South San Francisco, CA, USA; 2ERT, Philadelphia, PA, USA; 3Certara, Princeton, NJ, USA
Poster54566