abordaje de factores psicosociales en educación para la salud en fisioterapia
TRANSCRIPT

Perspectivas del Abordaje con Educación Para la Salud
en Fisioterapia
@_RaulFerrer
Prof. Raúl Ferrer Peña
#EducFisioLaSalle

EDUCACIÓN PARA LA SALUD
2
“La Educación para la salud (EPS) es una actividad diseñada para
ampliar el conocimiento de la población en relación con la salud y
desarrollar los valores y habilidades personales que promueven la salud”
EDUCACIÓN PARA LA SALUD
2

Salud
Educación Para la Salud

Enfermedad
Salud
Educación Para la SaludPrev. 1ª

Enfermedad
Salud
Educación Para la SaludPrev. 1ª Prev. 2ª
Factores de Riesgo

Enfermedad
Salud
Educación Terapéutica
Educación Para la SaludPrev. 1ª Prev. 2ª Prev. 3ª

BRAINA JOURNAL OF NEUROLOGY
Shape shifting pain: chronification of back painshifts brain representation from nociceptiveto emotional circuitsJaveria A. Hashmi,1 Marwan N. Baliki,1 Lejian Huang,1 Alex T. Baria,1 Souraya Torbey,1
Kristina M. Hermann,1 Thomas J. Schnitzer2 and A. Vania Apkarian1,3,*
1 Department of Physiology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA2 Department of Rheumatology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA3 Departments of Anaesthesia and Surgery, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA
Correspondence to: A. Vania Apkarian, PhD,Department of Physiology,303 E. Chicago,Tarry Bldg. 5-703,Chicago, IL 60611E-mail: [email protected]
Chronic pain conditions are associated with abnormalities in brain structure and function. Moreover, some studies indicate that
brain activity related to the subjective perception of chronic pain may be distinct from activity for acute pain. However, the latter
are based on observations from cross-sectional studies. How brain activity reorganizes with transition from acute to chronic pain
has remained unexplored. Here we study this transition by examining brain activity for rating fluctuations of back pain mag-
nitude. First we compared back pain-related brain activity between subjects who have had the condition for !2 months with no
prior history of back pain for 1 year (early, acute/subacute back pain group, n = 94), to subjects who have lived with back pain
for 410 years (chronic back pain group, n = 59). In a subset of subacute back pain patients, we followed brain activity for back
pain longitudinally over a 1-year period, and compared brain activity between those who recover (recovered acute/sub-acute
back pain group, n = 19) and those in which the back pain persists (persistent acute/sub-acute back pain group, n = 20; based on
a 20% decrease in intensity of back pain in 1 year). We report results in relation to meta-analytic probabilistic maps related to
the terms pain, emotion, and reward (each map is based on 4200 brain imaging studies, derived from neurosynth.org). We
observed that brain activity for back pain in the early, acute/subacute back pain group is limited to regions involved in acute
pain, whereas in the chronic back pain group, activity is confined to emotion-related circuitry. Reward circuitry was equally
represented in both groups. In the recovered acute/subacute back pain group, brain activity diminished in time, whereas in the
persistent acute/subacute back pain group, activity diminished in acute pain regions, increased in emotion-related circuitry, and
remained unchanged in reward circuitry. The results demonstrate that brain representation for a constant percept, back pain, can
undergo large-scale shifts in brain activity with the transition to chronic pain. These observations challenge long-standing
theoretical concepts regarding brain and mind relationships, as well as provide important novel insights regarding definitions
and mechanisms of chronic pain.
Keywords: chronic back pain; fMRI; longitudinal; emotion; reward
Abbreviations: CBP = chronic back pain; SBP = subacute back pain
doi:10.1093/brain/awt211 Brain 2013: 136; 2751–2768 | 2751
Received March 19, 2013. Revised May 16, 2013. Accepted June 14, 2013Published by Oxford University Press on behalf of the Guarantors of Brain 2013. This work is written by US Government employees and is in the public domain in the US.
BRAINA JOURNAL OF NEUROLOGY
Shape shifting pain: chronification of back painshifts brain representation from nociceptiveto emotional circuitsJaveria A. Hashmi,1 Marwan N. Baliki,1 Lejian Huang,1 Alex T. Baria,1 Souraya Torbey,1
Kristina M. Hermann,1 Thomas J. Schnitzer2 and A. Vania Apkarian1,3,*
1 Department of Physiology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA2 Department of Rheumatology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA3 Departments of Anaesthesia and Surgery, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA
Correspondence to: A. Vania Apkarian, PhD,Department of Physiology,303 E. Chicago,Tarry Bldg. 5-703,Chicago, IL 60611E-mail: [email protected]
Chronic pain conditions are associated with abnormalities in brain structure and function. Moreover, some studies indicate that
brain activity related to the subjective perception of chronic pain may be distinct from activity for acute pain. However, the latter
are based on observations from cross-sectional studies. How brain activity reorganizes with transition from acute to chronic pain
has remained unexplored. Here we study this transition by examining brain activity for rating fluctuations of back pain mag-
nitude. First we compared back pain-related brain activity between subjects who have had the condition for !2 months with no
prior history of back pain for 1 year (early, acute/subacute back pain group, n = 94), to subjects who have lived with back pain
for 410 years (chronic back pain group, n = 59). In a subset of subacute back pain patients, we followed brain activity for back
pain longitudinally over a 1-year period, and compared brain activity between those who recover (recovered acute/sub-acute
back pain group, n = 19) and those in which the back pain persists (persistent acute/sub-acute back pain group, n = 20; based on
a 20% decrease in intensity of back pain in 1 year). We report results in relation to meta-analytic probabilistic maps related to
the terms pain, emotion, and reward (each map is based on 4200 brain imaging studies, derived from neurosynth.org). We
observed that brain activity for back pain in the early, acute/subacute back pain group is limited to regions involved in acute
pain, whereas in the chronic back pain group, activity is confined to emotion-related circuitry. Reward circuitry was equally
represented in both groups. In the recovered acute/subacute back pain group, brain activity diminished in time, whereas in the
persistent acute/subacute back pain group, activity diminished in acute pain regions, increased in emotion-related circuitry, and
remained unchanged in reward circuitry. The results demonstrate that brain representation for a constant percept, back pain, can
undergo large-scale shifts in brain activity with the transition to chronic pain. These observations challenge long-standing
theoretical concepts regarding brain and mind relationships, as well as provide important novel insights regarding definitions
and mechanisms of chronic pain.
Keywords: chronic back pain; fMRI; longitudinal; emotion; reward
Abbreviations: CBP = chronic back pain; SBP = subacute back pain
doi:10.1093/brain/awt211 Brain 2013: 136; 2751–2768 | 2751
Received March 19, 2013. Revised May 16, 2013. Accepted June 14, 2013Published by Oxford University Press on behalf of the Guarantors of Brain 2013. This work is written by US Government employees and is in the public domain in the US.
Figure 3 Longitudinal changes in brain activity underlying spontaneous pain when patients transition from acute to chronic back painstate. (A) Plots show the scanning calendar dates of subjects with recovering SBP (SBPr) and persistent SBP (SBPp) for all four visits.Vertical marks represent individual persistent SBP (black) and recovering SBP (grey) subjects. Groups were scanned within the same timewindow (major ticks are years; minor ticks are months). (B) Recovering SBP in contrast to persistent SBP patients exhibited decreased painin time. (C) Group average activation maps (P50.01 uncorrected) for recovering and persistent SBP groups at the four visits. Recoveringand persistent SBP groups show activation within acute pain regions for visits 1 and 2 encompassing bilateral insula, thalamus and anteriorcingulate cortex (ACC). Recovering SBP patients show no significant activity for visits 3 and 4, whereas persistent SBP shows increasedactivation in the medial prefrontal cortex and amygdala at visit 4. (D) Plots show the group average cope (normalized) for pain, emotionand reward masks, for each group (persistent SBP, CBP, recovering SBP), across all visits. Persistent SBP exhibited decreased presentationof their spontaneous pain within the pain mask. This decrease was coupled with an increased activity within the emotion mask. The middlepanel shows CBP activity for all three masks. These values correspond to those we observe in persistent SBP at 1-year scans. In contrast topersistent SBP, the recovering SBP group exhibited decreased activity within all masks in time. (E) Classifier performance applied toindividual persistent SBP activation maps for either pain/emotion or CBP/early SBP, at visits 1 and 4. Persistent SBP activity mainlyclassified as pain or early SBP at visit 1, and as emotion or CBP at visit 4. +P5 0.05, ++P5 0.01, within group comparison to visit 1;**P50.01 comparison between groups at a corresponding time.
2760 | Brain 2013: 136; 2751–2768 J. A. Hashmi et al.
Figure 3 Longitudinal changes in brain activity underlying spontaneous pain when patients transition from acute to chronic back painstate. (A) Plots show the scanning calendar dates of subjects with recovering SBP (SBPr) and persistent SBP (SBPp) for all four visits.Vertical marks represent individual persistent SBP (black) and recovering SBP (grey) subjects. Groups were scanned within the same timewindow (major ticks are years; minor ticks are months). (B) Recovering SBP in contrast to persistent SBP patients exhibited decreased painin time. (C) Group average activation maps (P50.01 uncorrected) for recovering and persistent SBP groups at the four visits. Recoveringand persistent SBP groups show activation within acute pain regions for visits 1 and 2 encompassing bilateral insula, thalamus and anteriorcingulate cortex (ACC). Recovering SBP patients show no significant activity for visits 3 and 4, whereas persistent SBP shows increasedactivation in the medial prefrontal cortex and amygdala at visit 4. (D) Plots show the group average cope (normalized) for pain, emotionand reward masks, for each group (persistent SBP, CBP, recovering SBP), across all visits. Persistent SBP exhibited decreased presentationof their spontaneous pain within the pain mask. This decrease was coupled with an increased activity within the emotion mask. The middlepanel shows CBP activity for all three masks. These values correspond to those we observe in persistent SBP at 1-year scans. In contrast topersistent SBP, the recovering SBP group exhibited decreased activity within all masks in time. (E) Classifier performance applied toindividual persistent SBP activation maps for either pain/emotion or CBP/early SBP, at visits 1 and 4. Persistent SBP activity mainlyclassified as pain or early SBP at visit 1, and as emotion or CBP at visit 4. +P5 0.05, ++P5 0.01, within group comparison to visit 1;**P50.01 comparison between groups at a corresponding time.
2760 | Brain 2013: 136; 2751–2768 J. A. Hashmi et al.
Figure 3 Longitudinal changes in brain activity underlying spontaneous pain when patients transition from acute to chronic back painstate. (A) Plots show the scanning calendar dates of subjects with recovering SBP (SBPr) and persistent SBP (SBPp) for all four visits.Vertical marks represent individual persistent SBP (black) and recovering SBP (grey) subjects. Groups were scanned within the same timewindow (major ticks are years; minor ticks are months). (B) Recovering SBP in contrast to persistent SBP patients exhibited decreased painin time. (C) Group average activation maps (P50.01 uncorrected) for recovering and persistent SBP groups at the four visits. Recoveringand persistent SBP groups show activation within acute pain regions for visits 1 and 2 encompassing bilateral insula, thalamus and anteriorcingulate cortex (ACC). Recovering SBP patients show no significant activity for visits 3 and 4, whereas persistent SBP shows increasedactivation in the medial prefrontal cortex and amygdala at visit 4. (D) Plots show the group average cope (normalized) for pain, emotionand reward masks, for each group (persistent SBP, CBP, recovering SBP), across all visits. Persistent SBP exhibited decreased presentationof their spontaneous pain within the pain mask. This decrease was coupled with an increased activity within the emotion mask. The middlepanel shows CBP activity for all three masks. These values correspond to those we observe in persistent SBP at 1-year scans. In contrast topersistent SBP, the recovering SBP group exhibited decreased activity within all masks in time. (E) Classifier performance applied toindividual persistent SBP activation maps for either pain/emotion or CBP/early SBP, at visits 1 and 4. Persistent SBP activity mainlyclassified as pain or early SBP at visit 1, and as emotion or CBP at visit 4. +P5 0.05, ++P5 0.01, within group comparison to visit 1;**P50.01 comparison between groups at a corresponding time.
2760 | Brain 2013: 136; 2751–2768 J. A. Hashmi et al.
4

BRAINA JOURNAL OF NEUROLOGY
Shape shifting pain: chronification of back painshifts brain representation from nociceptiveto emotional circuitsJaveria A. Hashmi,1 Marwan N. Baliki,1 Lejian Huang,1 Alex T. Baria,1 Souraya Torbey,1
Kristina M. Hermann,1 Thomas J. Schnitzer2 and A. Vania Apkarian1,3,*
1 Department of Physiology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA2 Department of Rheumatology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA3 Departments of Anaesthesia and Surgery, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA
Correspondence to: A. Vania Apkarian, PhD,Department of Physiology,303 E. Chicago,Tarry Bldg. 5-703,Chicago, IL 60611E-mail: [email protected]
Chronic pain conditions are associated with abnormalities in brain structure and function. Moreover, some studies indicate that
brain activity related to the subjective perception of chronic pain may be distinct from activity for acute pain. However, the latter
are based on observations from cross-sectional studies. How brain activity reorganizes with transition from acute to chronic pain
has remained unexplored. Here we study this transition by examining brain activity for rating fluctuations of back pain mag-
nitude. First we compared back pain-related brain activity between subjects who have had the condition for !2 months with no
prior history of back pain for 1 year (early, acute/subacute back pain group, n = 94), to subjects who have lived with back pain
for 410 years (chronic back pain group, n = 59). In a subset of subacute back pain patients, we followed brain activity for back
pain longitudinally over a 1-year period, and compared brain activity between those who recover (recovered acute/sub-acute
back pain group, n = 19) and those in which the back pain persists (persistent acute/sub-acute back pain group, n = 20; based on
a 20% decrease in intensity of back pain in 1 year). We report results in relation to meta-analytic probabilistic maps related to
the terms pain, emotion, and reward (each map is based on 4200 brain imaging studies, derived from neurosynth.org). We
observed that brain activity for back pain in the early, acute/subacute back pain group is limited to regions involved in acute
pain, whereas in the chronic back pain group, activity is confined to emotion-related circuitry. Reward circuitry was equally
represented in both groups. In the recovered acute/subacute back pain group, brain activity diminished in time, whereas in the
persistent acute/subacute back pain group, activity diminished in acute pain regions, increased in emotion-related circuitry, and
remained unchanged in reward circuitry. The results demonstrate that brain representation for a constant percept, back pain, can
undergo large-scale shifts in brain activity with the transition to chronic pain. These observations challenge long-standing
theoretical concepts regarding brain and mind relationships, as well as provide important novel insights regarding definitions
and mechanisms of chronic pain.
Keywords: chronic back pain; fMRI; longitudinal; emotion; reward
Abbreviations: CBP = chronic back pain; SBP = subacute back pain
doi:10.1093/brain/awt211 Brain 2013: 136; 2751–2768 | 2751
Received March 19, 2013. Revised May 16, 2013. Accepted June 14, 2013Published by Oxford University Press on behalf of the Guarantors of Brain 2013. This work is written by US Government employees and is in the public domain in the US.
BRAINA JOURNAL OF NEUROLOGY
Shape shifting pain: chronification of back painshifts brain representation from nociceptiveto emotional circuitsJaveria A. Hashmi,1 Marwan N. Baliki,1 Lejian Huang,1 Alex T. Baria,1 Souraya Torbey,1
Kristina M. Hermann,1 Thomas J. Schnitzer2 and A. Vania Apkarian1,3,*
1 Department of Physiology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA2 Department of Rheumatology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA3 Departments of Anaesthesia and Surgery, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, 60611, USA
Correspondence to: A. Vania Apkarian, PhD,Department of Physiology,303 E. Chicago,Tarry Bldg. 5-703,Chicago, IL 60611E-mail: [email protected]
Chronic pain conditions are associated with abnormalities in brain structure and function. Moreover, some studies indicate that
brain activity related to the subjective perception of chronic pain may be distinct from activity for acute pain. However, the latter
are based on observations from cross-sectional studies. How brain activity reorganizes with transition from acute to chronic pain
has remained unexplored. Here we study this transition by examining brain activity for rating fluctuations of back pain mag-
nitude. First we compared back pain-related brain activity between subjects who have had the condition for !2 months with no
prior history of back pain for 1 year (early, acute/subacute back pain group, n = 94), to subjects who have lived with back pain
for 410 years (chronic back pain group, n = 59). In a subset of subacute back pain patients, we followed brain activity for back
pain longitudinally over a 1-year period, and compared brain activity between those who recover (recovered acute/sub-acute
back pain group, n = 19) and those in which the back pain persists (persistent acute/sub-acute back pain group, n = 20; based on
a 20% decrease in intensity of back pain in 1 year). We report results in relation to meta-analytic probabilistic maps related to
the terms pain, emotion, and reward (each map is based on 4200 brain imaging studies, derived from neurosynth.org). We
observed that brain activity for back pain in the early, acute/subacute back pain group is limited to regions involved in acute
pain, whereas in the chronic back pain group, activity is confined to emotion-related circuitry. Reward circuitry was equally
represented in both groups. In the recovered acute/subacute back pain group, brain activity diminished in time, whereas in the
persistent acute/subacute back pain group, activity diminished in acute pain regions, increased in emotion-related circuitry, and
remained unchanged in reward circuitry. The results demonstrate that brain representation for a constant percept, back pain, can
undergo large-scale shifts in brain activity with the transition to chronic pain. These observations challenge long-standing
theoretical concepts regarding brain and mind relationships, as well as provide important novel insights regarding definitions
and mechanisms of chronic pain.
Keywords: chronic back pain; fMRI; longitudinal; emotion; reward
Abbreviations: CBP = chronic back pain; SBP = subacute back pain
doi:10.1093/brain/awt211 Brain 2013: 136; 2751–2768 | 2751
Received March 19, 2013. Revised May 16, 2013. Accepted June 14, 2013Published by Oxford University Press on behalf of the Guarantors of Brain 2013. This work is written by US Government employees and is in the public domain in the US.
Figure 3 Longitudinal changes in brain activity underlying spontaneous pain when patients transition from acute to chronic back painstate. (A) Plots show the scanning calendar dates of subjects with recovering SBP (SBPr) and persistent SBP (SBPp) for all four visits.Vertical marks represent individual persistent SBP (black) and recovering SBP (grey) subjects. Groups were scanned within the same timewindow (major ticks are years; minor ticks are months). (B) Recovering SBP in contrast to persistent SBP patients exhibited decreased painin time. (C) Group average activation maps (P50.01 uncorrected) for recovering and persistent SBP groups at the four visits. Recoveringand persistent SBP groups show activation within acute pain regions for visits 1 and 2 encompassing bilateral insula, thalamus and anteriorcingulate cortex (ACC). Recovering SBP patients show no significant activity for visits 3 and 4, whereas persistent SBP shows increasedactivation in the medial prefrontal cortex and amygdala at visit 4. (D) Plots show the group average cope (normalized) for pain, emotionand reward masks, for each group (persistent SBP, CBP, recovering SBP), across all visits. Persistent SBP exhibited decreased presentationof their spontaneous pain within the pain mask. This decrease was coupled with an increased activity within the emotion mask. The middlepanel shows CBP activity for all three masks. These values correspond to those we observe in persistent SBP at 1-year scans. In contrast topersistent SBP, the recovering SBP group exhibited decreased activity within all masks in time. (E) Classifier performance applied toindividual persistent SBP activation maps for either pain/emotion or CBP/early SBP, at visits 1 and 4. Persistent SBP activity mainlyclassified as pain or early SBP at visit 1, and as emotion or CBP at visit 4. +P5 0.05, ++P5 0.01, within group comparison to visit 1;**P50.01 comparison between groups at a corresponding time.
2760 | Brain 2013: 136; 2751–2768 J. A. Hashmi et al.
Figure 3 Longitudinal changes in brain activity underlying spontaneous pain when patients transition from acute to chronic back painstate. (A) Plots show the scanning calendar dates of subjects with recovering SBP (SBPr) and persistent SBP (SBPp) for all four visits.Vertical marks represent individual persistent SBP (black) and recovering SBP (grey) subjects. Groups were scanned within the same timewindow (major ticks are years; minor ticks are months). (B) Recovering SBP in contrast to persistent SBP patients exhibited decreased painin time. (C) Group average activation maps (P50.01 uncorrected) for recovering and persistent SBP groups at the four visits. Recoveringand persistent SBP groups show activation within acute pain regions for visits 1 and 2 encompassing bilateral insula, thalamus and anteriorcingulate cortex (ACC). Recovering SBP patients show no significant activity for visits 3 and 4, whereas persistent SBP shows increasedactivation in the medial prefrontal cortex and amygdala at visit 4. (D) Plots show the group average cope (normalized) for pain, emotionand reward masks, for each group (persistent SBP, CBP, recovering SBP), across all visits. Persistent SBP exhibited decreased presentationof their spontaneous pain within the pain mask. This decrease was coupled with an increased activity within the emotion mask. The middlepanel shows CBP activity for all three masks. These values correspond to those we observe in persistent SBP at 1-year scans. In contrast topersistent SBP, the recovering SBP group exhibited decreased activity within all masks in time. (E) Classifier performance applied toindividual persistent SBP activation maps for either pain/emotion or CBP/early SBP, at visits 1 and 4. Persistent SBP activity mainlyclassified as pain or early SBP at visit 1, and as emotion or CBP at visit 4. +P5 0.05, ++P5 0.01, within group comparison to visit 1;**P50.01 comparison between groups at a corresponding time.
2760 | Brain 2013: 136; 2751–2768 J. A. Hashmi et al.
Figure 3 Longitudinal changes in brain activity underlying spontaneous pain when patients transition from acute to chronic back painstate. (A) Plots show the scanning calendar dates of subjects with recovering SBP (SBPr) and persistent SBP (SBPp) for all four visits.Vertical marks represent individual persistent SBP (black) and recovering SBP (grey) subjects. Groups were scanned within the same timewindow (major ticks are years; minor ticks are months). (B) Recovering SBP in contrast to persistent SBP patients exhibited decreased painin time. (C) Group average activation maps (P50.01 uncorrected) for recovering and persistent SBP groups at the four visits. Recoveringand persistent SBP groups show activation within acute pain regions for visits 1 and 2 encompassing bilateral insula, thalamus and anteriorcingulate cortex (ACC). Recovering SBP patients show no significant activity for visits 3 and 4, whereas persistent SBP shows increasedactivation in the medial prefrontal cortex and amygdala at visit 4. (D) Plots show the group average cope (normalized) for pain, emotionand reward masks, for each group (persistent SBP, CBP, recovering SBP), across all visits. Persistent SBP exhibited decreased presentationof their spontaneous pain within the pain mask. This decrease was coupled with an increased activity within the emotion mask. The middlepanel shows CBP activity for all three masks. These values correspond to those we observe in persistent SBP at 1-year scans. In contrast topersistent SBP, the recovering SBP group exhibited decreased activity within all masks in time. (E) Classifier performance applied toindividual persistent SBP activation maps for either pain/emotion or CBP/early SBP, at visits 1 and 4. Persistent SBP activity mainlyclassified as pain or early SBP at visit 1, and as emotion or CBP at visit 4. +P5 0.05, ++P5 0.01, within group comparison to visit 1;**P50.01 comparison between groups at a corresponding time.
2760 | Brain 2013: 136; 2751–2768 J. A. Hashmi et al.
4

Jonathan C. Hill and Julie M. Fritz Psychosocial Influences on Low Back Pain, Disability, and Response to Treatment. PHYS THER May 2011 91:712-721
5
Clasificación de factores psicosociales en relación a su influencia en el tratamiento
Mediadores del Tratamiento: representan pasos intermedios en el vínculo entre una intervención y el resultado deseado. (p.e. miedo evitación y exposición graduada para mejorar la función)
Factores Pronóstico para el tratamiento: Ayudan a estimar un resultado probable del paciente con independencia del tratamiento elegido. (p.e. depresión en cronificación de la lumbalgia)
Modificadores o Moduladores del Tratamiento: Medidos al comienzo del tratamiento indican si existe alguna relación entre la intervención específica y el resultado. (p.e. miedo-evitación en manipulación lumbar)
1
2
3

Jonathan C. Hill and Julie M. Fritz Psychosocial Influences on Low Back Pain, Disability, and Response to Treatment. PHYS THER May 2011 91:712-721
5
Clasificación de factores psicosociales en relación a su influencia en el tratamiento
Mediadores del Tratamiento: representan pasos intermedios en el vínculo entre una intervención y el resultado deseado. (p.e. miedo evitación y exposición graduada para mejorar la función)
Factores Pronóstico para el tratamiento: Ayudan a estimar un resultado probable del paciente con independencia del tratamiento elegido. (p.e. depresión en cronificación de la lumbalgia)
Modificadores o Moduladores del Tratamiento: Medidos al comienzo del tratamiento indican si existe alguna relación entre la intervención específica y el resultado. (p.e. miedo-evitación en manipulación lumbar)
1
2
3

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA
Autoeficacia

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA
Autoeficacia Locus de Control

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA
Autoeficacia Locus de Control

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA
Autoeficacia Locus de Control

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA
Autoeficacia Locus de Control
Creencia de gravedad

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA
Autoeficacia Locus de Control
Creencia de gravedad Atribución de causalidad

ALGUNOS FACTORES DEL ÁREA EMOCIONAL A TENER EN CUENTA
Autoeficacia Locus de Control
Creencia de gravedad Atribución de causalidad
Otros factores: Catastrofismo, Kinesiofobia, Miedo-Evitación, Otras Estrategias de Afrontamiento, …
Pérez Jarauta M J, et al. Manual de Educación para la salud. Gobierno de Navarra. 2006.7
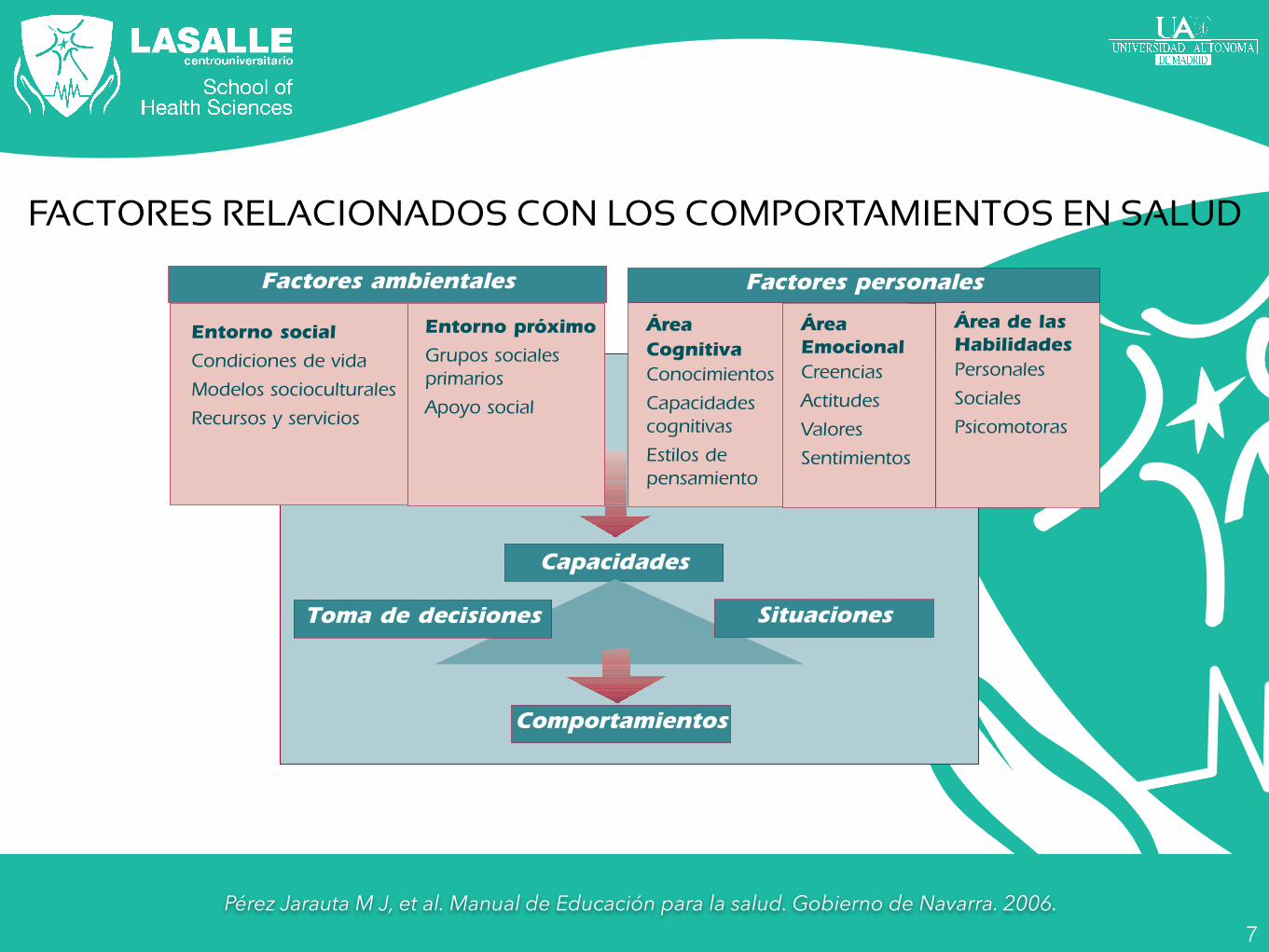
Para cada problema y/o situación de salud es necesario, en las intervenciones educativas,abordar no sólo los comportamientos concretos que se ponen en marcha sino el amplio abanicode factores relacionados con esos comportamientos, priorizando los principales bloques de conte-nidos según las necesidades e intereses de la persona o grupo con el que trabajemos y la dispo-nibilidad de recursos (tiempo del que se dispone, personal…).
Distintos autores (Bartoli, Green…), diferentes teorías psicológicas, pedagógicas… y distintosmodelos de análisis de comportamientos (modelo de creencias, clarificación de valores, PRECE-DE, aprendizaje social…) han realizado importantes aportaciones en este campo.
En este Manual consideramos, además de la dimensión biológica, tres tipos de factores: a) fac-tores del entorno social, de la sociedad en la que vive, b) factores del entorno próximo (su grupofamiliar, de trabajo y otros) y c) factores personales, del área cognitiva (lo que sabe), del áreaemocional (lo que cree y siente) y del área de las habilidades (lo que sabe hacer).
FACTORES RELACIONADOS CON LOS COMPORTAMIENTOS EN SALUD
El conjunto de los factores relacionados con los comportamientos configura las capacidades:capacidades para manejar la hipertensión arterial, el asma o el infarto agudo de miocardio; paradejar de fumar, alimentarse de forma saludable, favorecer el desarrollo psicoevolutivo y la estimu-lación psicomotriz, auditiva y táctil de los hijos e hijas, para afrontar el parto, la parentalidad, elduelo migratorio o el envejecimiento, etc.
Unas mismas capacidades permiten la puesta en marcha de una amplia gama de comporta-mientos. Las decisiones se toman respondiendo a las diferentes situaciones que se dan. Así, unapersona activa físicamente que acude con regularidad a clases de baile, puede no acudir respon-diendo a distintas situaciones: una visita de un amigo al que no ha visto hace tiempo, una enfer-medad de su madre… Los comportamientos son dúctiles.
La dimensión biológica hace referencia al cuerpo y a la corporeidad, a su funcionamiento,los procesos biofisiológicos, la condición física de la persona, la presencia o ausencia de enferme-dades y los autocuidados del cuerpo. Es más saludable una relación armónica del propio cuerpoconsigo mismo y con el entorno.
34
Comportamientos
Capacidades
Entorno próximoGrupos socialesprimariosApoyo social
ÁreaCognitivaConocimientosCapacidadescognitivasEstilos depensamiento
Entorno socialCondiciones de vidaModelos socioculturalesRecursos y servicios
Factores ambientales
ÁreaEmocionalCreenciasActitudesValoresSentimientos
Área de lasHabilidadesPersonalesSocialesPsicomotoras
Factores personales
FACTORES RELACIONADOS
Toma de decisiones Situaciones
FACTORES RELACIONADOS CON LOS COMPORTAMIENTOS EN SALUD

Pérez Jarauta M J, et al. Manual de Educación para la salud. Gobierno de Navarra. 2006.7
Para cada problema y/o situación de salud es necesario, en las intervenciones educativas,abordar no sólo los comportamientos concretos que se ponen en marcha sino el amplio abanicode factores relacionados con esos comportamientos, priorizando los principales bloques de conte-nidos según las necesidades e intereses de la persona o grupo con el que trabajemos y la dispo-nibilidad de recursos (tiempo del que se dispone, personal…).
Distintos autores (Bartoli, Green…), diferentes teorías psicológicas, pedagógicas… y distintosmodelos de análisis de comportamientos (modelo de creencias, clarificación de valores, PRECE-DE, aprendizaje social…) han realizado importantes aportaciones en este campo.
En este Manual consideramos, además de la dimensión biológica, tres tipos de factores: a) fac-tores del entorno social, de la sociedad en la que vive, b) factores del entorno próximo (su grupofamiliar, de trabajo y otros) y c) factores personales, del área cognitiva (lo que sabe), del áreaemocional (lo que cree y siente) y del área de las habilidades (lo que sabe hacer).
FACTORES RELACIONADOS CON LOS COMPORTAMIENTOS EN SALUD
El conjunto de los factores relacionados con los comportamientos configura las capacidades:capacidades para manejar la hipertensión arterial, el asma o el infarto agudo de miocardio; paradejar de fumar, alimentarse de forma saludable, favorecer el desarrollo psicoevolutivo y la estimu-lación psicomotriz, auditiva y táctil de los hijos e hijas, para afrontar el parto, la parentalidad, elduelo migratorio o el envejecimiento, etc.
Unas mismas capacidades permiten la puesta en marcha de una amplia gama de comporta-mientos. Las decisiones se toman respondiendo a las diferentes situaciones que se dan. Así, unapersona activa físicamente que acude con regularidad a clases de baile, puede no acudir respon-diendo a distintas situaciones: una visita de un amigo al que no ha visto hace tiempo, una enfer-medad de su madre… Los comportamientos son dúctiles.
La dimensión biológica hace referencia al cuerpo y a la corporeidad, a su funcionamiento,los procesos biofisiológicos, la condición física de la persona, la presencia o ausencia de enferme-dades y los autocuidados del cuerpo. Es más saludable una relación armónica del propio cuerpoconsigo mismo y con el entorno.
34
Comportamientos
Capacidades
Entorno próximoGrupos socialesprimariosApoyo social
ÁreaCognitivaConocimientosCapacidadescognitivasEstilos depensamiento
Entorno socialCondiciones de vidaModelos socioculturalesRecursos y servicios
Factores ambientales
ÁreaEmocionalCreenciasActitudesValoresSentimientos
Área de lasHabilidadesPersonalesSocialesPsicomotoras
Factores personales
FACTORES RELACIONADOS
Toma de decisiones Situaciones
FACTORES RELACIONADOS CON LOS COMPORTAMIENTOS EN SALUD

Pérez Jarauta M J, et al. Manual de Educación para la salud. Gobierno de Navarra. 2006.7
Para cada problema y/o situación de salud es necesario, en las intervenciones educativas,abordar no sólo los comportamientos concretos que se ponen en marcha sino el amplio abanicode factores relacionados con esos comportamientos, priorizando los principales bloques de conte-nidos según las necesidades e intereses de la persona o grupo con el que trabajemos y la dispo-nibilidad de recursos (tiempo del que se dispone, personal…).
Distintos autores (Bartoli, Green…), diferentes teorías psicológicas, pedagógicas… y distintosmodelos de análisis de comportamientos (modelo de creencias, clarificación de valores, PRECE-DE, aprendizaje social…) han realizado importantes aportaciones en este campo.
En este Manual consideramos, además de la dimensión biológica, tres tipos de factores: a) fac-tores del entorno social, de la sociedad en la que vive, b) factores del entorno próximo (su grupofamiliar, de trabajo y otros) y c) factores personales, del área cognitiva (lo que sabe), del áreaemocional (lo que cree y siente) y del área de las habilidades (lo que sabe hacer).
FACTORES RELACIONADOS CON LOS COMPORTAMIENTOS EN SALUD
El conjunto de los factores relacionados con los comportamientos configura las capacidades:capacidades para manejar la hipertensión arterial, el asma o el infarto agudo de miocardio; paradejar de fumar, alimentarse de forma saludable, favorecer el desarrollo psicoevolutivo y la estimu-lación psicomotriz, auditiva y táctil de los hijos e hijas, para afrontar el parto, la parentalidad, elduelo migratorio o el envejecimiento, etc.
Unas mismas capacidades permiten la puesta en marcha de una amplia gama de comporta-mientos. Las decisiones se toman respondiendo a las diferentes situaciones que se dan. Así, unapersona activa físicamente que acude con regularidad a clases de baile, puede no acudir respon-diendo a distintas situaciones: una visita de un amigo al que no ha visto hace tiempo, una enfer-medad de su madre… Los comportamientos son dúctiles.
La dimensión biológica hace referencia al cuerpo y a la corporeidad, a su funcionamiento,los procesos biofisiológicos, la condición física de la persona, la presencia o ausencia de enferme-dades y los autocuidados del cuerpo. Es más saludable una relación armónica del propio cuerpoconsigo mismo y con el entorno.
34
Comportamientos
Capacidades
Entorno próximoGrupos socialesprimariosApoyo social
ÁreaCognitivaConocimientosCapacidadescognitivasEstilos depensamiento
Entorno socialCondiciones de vidaModelos socioculturalesRecursos y servicios
Factores ambientales
ÁreaEmocionalCreenciasActitudesValoresSentimientos
Área de lasHabilidadesPersonalesSocialesPsicomotoras
Factores personales
FACTORES RELACIONADOS
Toma de decisiones Situaciones
FACTORES RELACIONADOS CON LOS COMPORTAMIENTOS EN SALUD

ALGUNOS MODELOS DE EDUCACIÓN PARA LA SALUD
• Modelo Preventivista: basado en conocimientos sobre normas adecuadas
• Modelo Educativista: basado en el cambio a estilos de vida saludables.
• Modelo de Desarrollo Personal: Basado en hacer al sujeto responsable de su salud
Pérez Jarauta M J, et al. Manual de Educación para la salud. Gobierno de Navarra. 2006.

ALGUNOS MODELOS DE EDUCACIÓN PARA LA SALUD
• Modelo Preventivista: basado en conocimientos sobre normas adecuadas
• Modelo Educativista: basado en el cambio a estilos de vida saludables.
• Modelo de Desarrollo Personal: Basado en hacer al sujeto responsable de su salud
Pérez Jarauta M J, et al. Manual de Educación para la salud. Gobierno de Navarra. 2006.

Características:
JAMA. 2002;288(19):2469-2475 9

Lo que enseña: Habilidades en como actuar ante los problemas
Características:
JAMA. 2002;288(19):2469-2475 9

Lo que enseña: Habilidades en como actuar ante los problemas
Características:
JAMA. 2002;288(19):2469-2475
Cómo se formulan los problemas: El paciente identifica los problemas que pueden estar o no relacionados con su salud
9

Lo que enseña: Habilidades en como actuar ante los problemas
Relación entre la educación y la enfermedad: La educación ofrece habilidades de resolución relevantes relativas a las consecuencias de los problemas
Características:
JAMA. 2002;288(19):2469-2475
Cómo se formulan los problemas: El paciente identifica los problemas que pueden estar o no relacionados con su salud
9

Lo que enseña: Habilidades en como actuar ante los problemas
Relación entre la educación y la enfermedad: La educación ofrece habilidades de resolución relevantes relativas a las consecuencias de los problemas
Cuál es la teoría propuesta: Más confianza del paciente en su autoeficacia redunda en mejores resultados
Características:
JAMA. 2002;288(19):2469-2475
Cómo se formulan los problemas: El paciente identifica los problemas que pueden estar o no relacionados con su salud
9

Lo que enseña: Habilidades en como actuar ante los problemas
Relación entre la educación y la enfermedad: La educación ofrece habilidades de resolución relevantes relativas a las consecuencias de los problemas
Cuál es la teoría propuesta: Más confianza del paciente en su autoeficacia redunda en mejores resultados
Cuál es el objetivo: Mejorar la autoeficacia para mejorar los resultados
Características:
JAMA. 2002;288(19):2469-2475
Cómo se formulan los problemas: El paciente identifica los problemas que pueden estar o no relacionados con su salud
9

Lo que enseña: Habilidades en como actuar ante los problemas
Relación entre la educación y la enfermedad: La educación ofrece habilidades de resolución relevantes relativas a las consecuencias de los problemas
Cuál es la teoría propuesta: Más confianza del paciente en su autoeficacia redunda en mejores resultados
Cuál es el objetivo: Mejorar la autoeficacia para mejorar los resultados
Quién es el educador: Un profesional sanitario, un paciente experto o un líder semejante, a menudo en grupos.
Características:
JAMA. 2002;288(19):2469-2475
Cómo se formulan los problemas: El paciente identifica los problemas que pueden estar o no relacionados con su salud
9

Copyright 2015 American Medical Association. All rights reserved.
Effect of Primary Care–Based Education on Reassurancein Patients With Acute Low Back PainSystematic Review and Meta-analysisAdrian C. Traeger, MPhty; Markus Hübscher, PhD; Nicholas Henschke, PhD; G. Lorimer Moseley, PhD;Hopin Lee, MPhty; James H. McAuley, PhD
IMPORTANCE Reassurance is a core aspect of daily medical practice, yet little is known on howit can be achieved.
OBJECTIVE To determine whether patient education in primary care increases reassurance inpatients with acute or subacute low back pain (LBP).
DATA SOURCES Medline, EMBASE, Cochrane Central Register for Controlled Trials, andPsychINFO databases were searched to June 2014.
DESIGN Systematic review and meta-analysis of randomized and nonrandomized clinicaltrials.
STUDY SELECTION To be eligible, studies needed to be controlled trials of patient educationfor LBP that were delivered in primary care and measured reassurance after the intervention.Eligibility criteria were applied, and studies were selected by 2 independent authors.
MAIN OUTCOMES AND MEASURES The primary outcomes were reassurance in the short andlong term and health care utilization at 12 months.
DATA EXTRACTION AND SYNTHESIS Data were extracted by 2 independent authors andentered into a standardized form. A random-effects meta-analysis tested the effects ofpatient education compared with usual care on measures of reassurance. To investigate theeffect of study characteristics, we performed a preplanned subgroup analysis. Studies werestratified according to duration, content, and provider of patient education.
RESULTS We included 14 trials (n = 4872) of patient education interventions. Trials assessedreassurance with questionnaires of fear, worry, anxiety, catastrophization, and health careutilization. There is moderate- to high-quality evidence that patient education increasesreassurance more than usual care/control education in the short term (standardized meandifference [SMD], −0.21; 95% CI, −0.35 to −0.06) and long term (SMD, −0.15; 95% CI, −0.27to −0.03). Interventions delivered by physicians were significantly more reassuring thanthose delivered by other primary care practitioners (eg, physiotherapist or nurse). There ismoderate-quality evidence that patient education reduces LBP-related primary care visitsmore than usual care/control education (SMD, −0.14; 95% CI, −0.28 to −0.00 at a 12-monthfollow-up). The number needed to treat to prevent 1 LBP-related visit to primary care was 17.
CONCLUSIONS AND RELEVANCE There is moderate- to high-quality evidence that patienteducation in primary care can provide long-term reassurance for patients with acute orsubacute LBP.
JAMA Intern Med. doi:10.1001/jamainternmed.2015.0217Published online March 23, 2015.
Invited Commentary
Supplemental content atjamainternalmedicine.com
Author Affiliations: NeuroscienceResearch Australia, Sydney, Australia(Traeger, Hübscher, Moseley, Lee,McAuley); School of MedicalSciences, University of New SouthWales, Sydney, Australia (Traeger,Lee, McAuley); Institute of PublicHealth, University of Heidelberg,Heidelberg, Germany (Henschke);Sansom Institute for Health Research,University of South Australia,Adelaide, South Australia, Australia(Moseley).
Corresponding Author: James H.McAuley, PhD, NeuroscienceResearch Australia, Barker Street,Randwick, NSW 2031, Australia([email protected]).
Research
Original Investigation | LESS IS MORE
(Reprinted) E1
Copyright 2015 American Medical Association. All rights reserved.
JAMA Intern Med.Published online March 23. 2015 10

Copyright 2015 American Medical Association. All rights reserved.
Effect of Primary Care–Based Education on Reassurancein Patients With Acute Low Back PainSystematic Review and Meta-analysisAdrian C. Traeger, MPhty; Markus Hübscher, PhD; Nicholas Henschke, PhD; G. Lorimer Moseley, PhD;Hopin Lee, MPhty; James H. McAuley, PhD
IMPORTANCE Reassurance is a core aspect of daily medical practice, yet little is known on howit can be achieved.
OBJECTIVE To determine whether patient education in primary care increases reassurance inpatients with acute or subacute low back pain (LBP).
DATA SOURCES Medline, EMBASE, Cochrane Central Register for Controlled Trials, andPsychINFO databases were searched to June 2014.
DESIGN Systematic review and meta-analysis of randomized and nonrandomized clinicaltrials.
STUDY SELECTION To be eligible, studies needed to be controlled trials of patient educationfor LBP that were delivered in primary care and measured reassurance after the intervention.Eligibility criteria were applied, and studies were selected by 2 independent authors.
MAIN OUTCOMES AND MEASURES The primary outcomes were reassurance in the short andlong term and health care utilization at 12 months.
DATA EXTRACTION AND SYNTHESIS Data were extracted by 2 independent authors andentered into a standardized form. A random-effects meta-analysis tested the effects ofpatient education compared with usual care on measures of reassurance. To investigate theeffect of study characteristics, we performed a preplanned subgroup analysis. Studies werestratified according to duration, content, and provider of patient education.
RESULTS We included 14 trials (n = 4872) of patient education interventions. Trials assessedreassurance with questionnaires of fear, worry, anxiety, catastrophization, and health careutilization. There is moderate- to high-quality evidence that patient education increasesreassurance more than usual care/control education in the short term (standardized meandifference [SMD], −0.21; 95% CI, −0.35 to −0.06) and long term (SMD, −0.15; 95% CI, −0.27to −0.03). Interventions delivered by physicians were significantly more reassuring thanthose delivered by other primary care practitioners (eg, physiotherapist or nurse). There ismoderate-quality evidence that patient education reduces LBP-related primary care visitsmore than usual care/control education (SMD, −0.14; 95% CI, −0.28 to −0.00 at a 12-monthfollow-up). The number needed to treat to prevent 1 LBP-related visit to primary care was 17.
CONCLUSIONS AND RELEVANCE There is moderate- to high-quality evidence that patienteducation in primary care can provide long-term reassurance for patients with acute orsubacute LBP.
JAMA Intern Med. doi:10.1001/jamainternmed.2015.0217Published online March 23, 2015.
Invited Commentary
Supplemental content atjamainternalmedicine.com
Author Affiliations: NeuroscienceResearch Australia, Sydney, Australia(Traeger, Hübscher, Moseley, Lee,McAuley); School of MedicalSciences, University of New SouthWales, Sydney, Australia (Traeger,Lee, McAuley); Institute of PublicHealth, University of Heidelberg,Heidelberg, Germany (Henschke);Sansom Institute for Health Research,University of South Australia,Adelaide, South Australia, Australia(Moseley).
Corresponding Author: James H.McAuley, PhD, NeuroscienceResearch Australia, Barker Street,Randwick, NSW 2031, Australia([email protected]).
Research
Original Investigation | LESS IS MORE
(Reprinted) E1
Copyright 2015 American Medical Association. All rights reserved.
JAMA Intern Med.Published online March 23. 2015 10
Consuelo, Alivio…

Copyright 2015 American Medical Association. All rights reserved.
Effect of Primary Care–Based Education on Reassurancein Patients With Acute Low Back PainSystematic Review and Meta-analysisAdrian C. Traeger, MPhty; Markus Hübscher, PhD; Nicholas Henschke, PhD; G. Lorimer Moseley, PhD;Hopin Lee, MPhty; James H. McAuley, PhD
IMPORTANCE Reassurance is a core aspect of daily medical practice, yet little is known on howit can be achieved.
OBJECTIVE To determine whether patient education in primary care increases reassurance inpatients with acute or subacute low back pain (LBP).
DATA SOURCES Medline, EMBASE, Cochrane Central Register for Controlled Trials, andPsychINFO databases were searched to June 2014.
DESIGN Systematic review and meta-analysis of randomized and nonrandomized clinicaltrials.
STUDY SELECTION To be eligible, studies needed to be controlled trials of patient educationfor LBP that were delivered in primary care and measured reassurance after the intervention.Eligibility criteria were applied, and studies were selected by 2 independent authors.
MAIN OUTCOMES AND MEASURES The primary outcomes were reassurance in the short andlong term and health care utilization at 12 months.
DATA EXTRACTION AND SYNTHESIS Data were extracted by 2 independent authors andentered into a standardized form. A random-effects meta-analysis tested the effects ofpatient education compared with usual care on measures of reassurance. To investigate theeffect of study characteristics, we performed a preplanned subgroup analysis. Studies werestratified according to duration, content, and provider of patient education.
RESULTS We included 14 trials (n = 4872) of patient education interventions. Trials assessedreassurance with questionnaires of fear, worry, anxiety, catastrophization, and health careutilization. There is moderate- to high-quality evidence that patient education increasesreassurance more than usual care/control education in the short term (standardized meandifference [SMD], −0.21; 95% CI, −0.35 to −0.06) and long term (SMD, −0.15; 95% CI, −0.27to −0.03). Interventions delivered by physicians were significantly more reassuring thanthose delivered by other primary care practitioners (eg, physiotherapist or nurse). There ismoderate-quality evidence that patient education reduces LBP-related primary care visitsmore than usual care/control education (SMD, −0.14; 95% CI, −0.28 to −0.00 at a 12-monthfollow-up). The number needed to treat to prevent 1 LBP-related visit to primary care was 17.
CONCLUSIONS AND RELEVANCE There is moderate- to high-quality evidence that patienteducation in primary care can provide long-term reassurance for patients with acute orsubacute LBP.
JAMA Intern Med. doi:10.1001/jamainternmed.2015.0217Published online March 23, 2015.
Invited Commentary
Supplemental content atjamainternalmedicine.com
Author Affiliations: NeuroscienceResearch Australia, Sydney, Australia(Traeger, Hübscher, Moseley, Lee,McAuley); School of MedicalSciences, University of New SouthWales, Sydney, Australia (Traeger,Lee, McAuley); Institute of PublicHealth, University of Heidelberg,Heidelberg, Germany (Henschke);Sansom Institute for Health Research,University of South Australia,Adelaide, South Australia, Australia(Moseley).
Corresponding Author: James H.McAuley, PhD, NeuroscienceResearch Australia, Barker Street,Randwick, NSW 2031, Australia([email protected]).
Research
Original Investigation | LESS IS MORE
(Reprinted) E1
Copyright 2015 American Medical Association. All rights reserved.
JAMA Intern Med.Published online March 23. 2015
Copyright 2015 American Medical Association. All rights reserved.
Pooled effect sizes remained stable when we accounted fordifferences in study quality, comparison group, symptom dura-tion, use of dichotomous data transformations or, if studies mea-sured more than 1 dimension of reassurance, our choice of effectsize used in the meta-analysis (Table 2). Effect size estimateschanged when results were stratified according to outcome mea-sure. Pooled effect size estimates were larger on measures of fear(SMD, −0.34; 95% CI, −0.54 to −0.14) than on measures of worry(SMD, 0.01; 95% CI, −0.30 to 0.32), anxiety (SMD, −0.07; 95% CI,−0.24 to 0.10), and catastrophizing (SMD, −0.05; 95% CI, −0.31to 0.22) (Table 2 and eFigure 2 in the Supplement).
Subgroup analysis demonstrated that education was sig-nificantly more effective when delivered by a physician (SMD,−0.38; 95% CI, −0.62 to −0.14) rather than a nurse (SMD, −0.12;95% CI, −0.40 to 0.17) or a physiotherapist (SMD, 0.00; 95%CI, −0.15 to 0.14) (Figure 2). All other subgroup analyses didnot reach significance (eTable 2 in the Supplement; see alsoeFigures 3-6 in eAppendix 4 in the Supplement).
Health Care UtilizationSeven studies53,55,59-61,63 measured LBP-related visits at a 12-month follow-up. We found moderate-quality evidence (7 stud-ies, limitations in design) that education reduces LBP-relatedprimary care visits more than usual care/control education
(SMD, −0.14; 95% CI, −0.28 to 0.00) (Figure 3). The mean rateof any primary care consultation from 3 control groups55,61,64
(ie, the “Patient’s Expected Event Rate”) was 35% at 12 months.The estimated “number needed to educate” to prevent 1 LBP-related primary care visit over 12 months was 17.
DiscussionMain FindingsThis systematic review and meta-analysis provides moderate-to high-quality evidence that patient education provided by pri-mary care practitioners can reassure patients with acute LBP.These effects are maintained for up to 12 months. Patient edu-cation is also associated with reduced LBP-related health carevisits. Preplanned subgroup analyses suggest that patient edu-cation is more reassuring when provided by physicians thanwhen provided by nurses or physiotherapists.
Strengths and LimitationsWe have used a clear definition of reassurance that is consis-tent with contemporary models21 and with previous reviewsin the field.15,31 The methods used to conduct this review werein line with those recommended by the Cochrane Back Re-
Figure 1. Effects of Patient Education vs Usual Care/Control Education on Reassurance
Favors(experimental)
–2 20 1SMD (IV, Random, 95% CI)
–1
Weight, %Favors(control)SMD (SE)Source
Short term
SMD(IV, Random, 95% CI)
7.1–0.89 (0.19)Burton et al,57 1999 –0.89 (–1.26 to –0.52)5.0–0.76 (0.26)Storheim et al,65 2003 –0.76 (–1.27 to –0.25)5.0–0.38 (0.26)Hill et al,55 2011 –0.38 (–0.89 to 0.13)5.0–0.31 (0.26)Roberts et al,54 2002 –0.31 (–0.82 to 0.20)
12.1–0.30 (0.07)Leonhardt et al,56 2008 –0.30 (–0.44 to –0.16)10.5–0.23 (0.11)Jellema et al,62 2005 –0.23 (–0.45 to –0.01)
6.8–0.18 (0.20)Bücker et al,51 2010 –0.18 (–0.57 to 0.21)8.3–0.15 (0.16)Deyo et al,60 1987 –0.15 (–0.46 to 0.16)
10.9–0.12 (0.10)Hagen et al,52 2000 –0.12 (–0.32 to 0.08)10.9–0.01 (0.10)Hay et al,61 2005 –0.01 (–0.21 to 0.19)
Heterogeneity: τ2 = 0.04; χ 2 = 35.60 (P < .001); I 2 = 69%100.00Subtotal (95% CI)
11
–0.21 (–0.36 to –0.07)
9.60.08 (0.13)Pengel et al,53 2007 0.08 (–0.17 to 0.33)8.70.17 (0.15)Cherkin et al,59 1996 0.17 (–0.12 to 0.46)
Test for overall effect: z = 2.90 (P = .004) Long term
8.4–0.56 (0.18)Burton et al,57 1999 –0.56 (–0.91 to –0.21)22.3–0.25 (0.07)Leonhardt et al,56 2008 –0.25 (–0.39 to –0.11)
4.7–0.22 (0.26)Hill et al,55 2011 –0.22 (–0.73 to 0.29)5.0–0.16 (0.25)Roberts et al,54 2002 –0.16 (–0.65 to 0.33)
15.5–0.13 (0.11)Jellema et al,62 2005 –0.13 (–0.35 to 0.09)8.4–0.09 (0.18)Pengel et al,53 2007 –0.09 (–0.44 to 0.26)
18.7–0.04 (0.09)Hagen et al,52 2000 –0.04 (–0.22 to 0.14)17.10.04 (0.10)Hay et al,61 2005 0.04 (–0.16 to 0.24)
Heterogeneity: τ2 = 0.01; χ2 = 12.55 (P = .08); I 2 = 44%100.00Subtotal (95% CI)
7
–0.15 (–0.27 to –0.03)
Test for overall effect: z = 2.46 (P = .01)
IV indicates inverse variance; SMD, standardized mean difference.
Research Original Investigation Reassurance in Patients With Acute Low Back Pain
E6 JAMA Internal Medicine Published online March 23, 2015 (Reprinted) jamainternalmedicine.com
Copyright 2015 American Medical Association. All rights reserved.
Copyright 2015 American Medical Association. All rights reserved.
suggests that effective reassurance involves a shift in a pa-tient’s cognitive appraisal of their health problem. Reap-praisal of the problem then reduces health-seeking behaviorin spite of ongoing symptoms.21 For nonspecific conditions,where ongoing symptoms are likely and the risk of excessivehealth care use is high, reassurance is a particularly relevantoutcome in primary care.
InterpretationOur data suggest that when practitioners are trained to de-liver structured patient education interventions, the reassur-ance this provides to patients is superior to usual care. A re-cent survey of Australian general practice activity found thatonly 20% of primary care physicians report giving advice andeducation of this type in the treatment of LBP.34 Patient edu-
Figure 2. Differences in Short-term Effects of Patient Education Interventions on Reassurance, When Interventions Are StratifiedAccording to the Deliverer of the Intervention
Favors(experimental)
–2 20 1SMD (IV, Random, 95% CI)
–1
Weight, %Favors(control)SMD (SE)Source
Physiotherapist
SMD(IV, Random, 95% CI)
5.3–0.28 (0.25)Hill et al,55 2011 –0.28 (–0.77 to 0.21)10.9–0.01 (0.10)Hay et al,61 2005 –0.01 (–0.21 to 0.19)
9.50.08 (0.13)Pengel et al,53 2007 0.08 (–0.17 to 0.33)
Heterogeneity: τ2 = 0.00; χ2 = 1.64 (P = .44); I 2 = 0%25.7Subtotal (95% CI)
2
–0.00 (–0.15 to 0.14)
Test for overall effect: z = 0.06 (P = .96) Physician
7.1–0.89 (0.19)Burton et al,57 1999 –0.89 (–1.26 to –0.52)5.0–0.76 (0.26)Storheim et al,65 2003 –0.76 (–1.27 to –0.25)5.0–0.31 (0.26)Roberts et al,54 2002 –0.31 (–0.82 to 0.20)
10.4–0.24 (0.11)Jellema et al,62 2005 –0.24 (–0.46 to –0.02)6.8–0.18 (0.20)Bücker et al,51 2010 –0.18 (–0.57 to 0.21)
10.9–0.12 (0.10)Hagen et al,52 2000 –0.12 (–0.32 to 0.08)
Heterogeneity: τ2 = 0.06; χ2 = 16.65 (P = .005); I 2 = 70%45.2Subtotal (95% CI)
5
–0.38 (–0.63 to –0.14)
Test for overall effect: z = 3.06 (P = .002) Nurse
12.2–0.30 (0.07)Leonhardt et al,56 2008 –0.30 (–0.44 to –0.16)8.3–0.15 (0.16)Deyo et al,60 1987 –0.15 (–0.46 to 0.16)8.70.17 (0.15)Cherkin et al,59 1996 0.17 (–0.12 to 0.46)
Heterogeneity: τ2 = 0.05; χ2 = 8.21 (P = .02); I 2 = 76%29.1Subtotal (95% CI)
2
2
–0.11 (–0.40 to 0.17)
Test for overall effect: z = 0.78 (P = .44)
Heterogeneity: τ2 = 0.04; χ 2 = 35.26 (P <.001); I 2 = 69%100.00Total (95% CI)
11
–0.21 (–0.35 to –0.07)
Test for overall effect: z = 2.87 (P = .004) Test for subgroup differences: χ2 = 6.69 (P = .04); I 2 = 70.1%
IV indicates inverse variance; SMD, standardized mean difference.
Figure 3. Effects of Patient Education vs Usual Care/Control Education on the Number of Primary Care Visits in the 12 Months After Intervention
Favors(experimental)
–2 20 1SMD (IV, Random, 95% CI)
–1
Weight, %Favors(control)SMD (SE)Source
SMD(IV, Random, 95% CI)
7.0–0.41 (0.27)Hill et al,55 2011 –0.41 (–0.94 to 0.12)15.7–0.33 (0.18)Pengel et al,53 2007 –0.33 (–0.68 to 0.02)11.6–0.21 (0.21)Deyo et al,60 1987 –0.21 (–0.62 to 0.20)19.9–0.15 (0.16)Roland et al,64 1989 –0.15 (–0.46 to 0.16)14.1–0.06 (0.19)Cherkin et al,59 1996 –0.06 (–0.43 to 0.31)14.10 (0.19)Karjalainen et al,63 2003 0.00 (–0.37 to 0.37)17.60.03 (0.17)Hay et al,61 2005 0.03 (–0.30 to 0.36)
Heterogeneity: τ2 = 0.00; χ2 = 3.95 (P = .68); I 2 = 0%100.00Total (95% CI)
6
–0.14 (–0.28 to 0.00)
Test for overall effect: z = 1.93 (P = .05)
IV indicates inverse variance; SMD, standardized mean difference.
Research Original Investigation Reassurance in Patients With Acute Low Back Pain
E8 JAMA Internal Medicine Published online March 23, 2015 (Reprinted) jamainternalmedicine.com
Copyright 2015 American Medical Association. All rights reserved.
14 estudios. (n=4872)
10
Número de visitas:
Efecto a corto y largo plazo:

Copyright 2015 American Medical Association. All rights reserved.
Effect of Primary Care–Based Education on Reassurancein Patients With Acute Low Back PainSystematic Review and Meta-analysisAdrian C. Traeger, MPhty; Markus Hübscher, PhD; Nicholas Henschke, PhD; G. Lorimer Moseley, PhD;Hopin Lee, MPhty; James H. McAuley, PhD
IMPORTANCE Reassurance is a core aspect of daily medical practice, yet little is known on howit can be achieved.
OBJECTIVE To determine whether patient education in primary care increases reassurance inpatients with acute or subacute low back pain (LBP).
DATA SOURCES Medline, EMBASE, Cochrane Central Register for Controlled Trials, andPsychINFO databases were searched to June 2014.
DESIGN Systematic review and meta-analysis of randomized and nonrandomized clinicaltrials.
STUDY SELECTION To be eligible, studies needed to be controlled trials of patient educationfor LBP that were delivered in primary care and measured reassurance after the intervention.Eligibility criteria were applied, and studies were selected by 2 independent authors.
MAIN OUTCOMES AND MEASURES The primary outcomes were reassurance in the short andlong term and health care utilization at 12 months.
DATA EXTRACTION AND SYNTHESIS Data were extracted by 2 independent authors andentered into a standardized form. A random-effects meta-analysis tested the effects ofpatient education compared with usual care on measures of reassurance. To investigate theeffect of study characteristics, we performed a preplanned subgroup analysis. Studies werestratified according to duration, content, and provider of patient education.
RESULTS We included 14 trials (n = 4872) of patient education interventions. Trials assessedreassurance with questionnaires of fear, worry, anxiety, catastrophization, and health careutilization. There is moderate- to high-quality evidence that patient education increasesreassurance more than usual care/control education in the short term (standardized meandifference [SMD], −0.21; 95% CI, −0.35 to −0.06) and long term (SMD, −0.15; 95% CI, −0.27to −0.03). Interventions delivered by physicians were significantly more reassuring thanthose delivered by other primary care practitioners (eg, physiotherapist or nurse). There ismoderate-quality evidence that patient education reduces LBP-related primary care visitsmore than usual care/control education (SMD, −0.14; 95% CI, −0.28 to −0.00 at a 12-monthfollow-up). The number needed to treat to prevent 1 LBP-related visit to primary care was 17.
CONCLUSIONS AND RELEVANCE There is moderate- to high-quality evidence that patienteducation in primary care can provide long-term reassurance for patients with acute orsubacute LBP.
JAMA Intern Med. doi:10.1001/jamainternmed.2015.0217Published online March 23, 2015.
Invited Commentary
Supplemental content atjamainternalmedicine.com
Author Affiliations: NeuroscienceResearch Australia, Sydney, Australia(Traeger, Hübscher, Moseley, Lee,McAuley); School of MedicalSciences, University of New SouthWales, Sydney, Australia (Traeger,Lee, McAuley); Institute of PublicHealth, University of Heidelberg,Heidelberg, Germany (Henschke);Sansom Institute for Health Research,University of South Australia,Adelaide, South Australia, Australia(Moseley).
Corresponding Author: James H.McAuley, PhD, NeuroscienceResearch Australia, Barker Street,Randwick, NSW 2031, Australia([email protected]).
Research
Original Investigation | LESS IS MORE
(Reprinted) E1
Copyright 2015 American Medical Association. All rights reserved.
JAMA Intern Med.Published online March 23. 2015
Copyright 2015 American Medical Association. All rights reserved.
suggests that effective reassurance involves a shift in a pa-tient’s cognitive appraisal of their health problem. Reap-praisal of the problem then reduces health-seeking behaviorin spite of ongoing symptoms.21 For nonspecific conditions,where ongoing symptoms are likely and the risk of excessivehealth care use is high, reassurance is a particularly relevantoutcome in primary care.
InterpretationOur data suggest that when practitioners are trained to de-liver structured patient education interventions, the reassur-ance this provides to patients is superior to usual care. A re-cent survey of Australian general practice activity found thatonly 20% of primary care physicians report giving advice andeducation of this type in the treatment of LBP.34 Patient edu-
Figure 2. Differences in Short-term Effects of Patient Education Interventions on Reassurance, When Interventions Are StratifiedAccording to the Deliverer of the Intervention
Favors(experimental)
–2 20 1SMD (IV, Random, 95% CI)
–1
Weight, %Favors(control)SMD (SE)Source
Physiotherapist
SMD(IV, Random, 95% CI)
5.3–0.28 (0.25)Hill et al,55 2011 –0.28 (–0.77 to 0.21)10.9–0.01 (0.10)Hay et al,61 2005 –0.01 (–0.21 to 0.19)
9.50.08 (0.13)Pengel et al,53 2007 0.08 (–0.17 to 0.33)
Heterogeneity: τ2 = 0.00; χ2 = 1.64 (P = .44); I 2 = 0%25.7Subtotal (95% CI)
2
–0.00 (–0.15 to 0.14)
Test for overall effect: z = 0.06 (P = .96) Physician
7.1–0.89 (0.19)Burton et al,57 1999 –0.89 (–1.26 to –0.52)5.0–0.76 (0.26)Storheim et al,65 2003 –0.76 (–1.27 to –0.25)5.0–0.31 (0.26)Roberts et al,54 2002 –0.31 (–0.82 to 0.20)
10.4–0.24 (0.11)Jellema et al,62 2005 –0.24 (–0.46 to –0.02)6.8–0.18 (0.20)Bücker et al,51 2010 –0.18 (–0.57 to 0.21)
10.9–0.12 (0.10)Hagen et al,52 2000 –0.12 (–0.32 to 0.08)
Heterogeneity: τ2 = 0.06; χ2 = 16.65 (P = .005); I 2 = 70%45.2Subtotal (95% CI)
5
–0.38 (–0.63 to –0.14)
Test for overall effect: z = 3.06 (P = .002) Nurse
12.2–0.30 (0.07)Leonhardt et al,56 2008 –0.30 (–0.44 to –0.16)8.3–0.15 (0.16)Deyo et al,60 1987 –0.15 (–0.46 to 0.16)8.70.17 (0.15)Cherkin et al,59 1996 0.17 (–0.12 to 0.46)
Heterogeneity: τ2 = 0.05; χ2 = 8.21 (P = .02); I 2 = 76%29.1Subtotal (95% CI)
2
2
–0.11 (–0.40 to 0.17)
Test for overall effect: z = 0.78 (P = .44)
Heterogeneity: τ2 = 0.04; χ 2 = 35.26 (P <.001); I 2 = 69%100.00Total (95% CI)
11
–0.21 (–0.35 to –0.07)
Test for overall effect: z = 2.87 (P = .004) Test for subgroup differences: χ2 = 6.69 (P = .04); I 2 = 70.1%
IV indicates inverse variance; SMD, standardized mean difference.
Figure 3. Effects of Patient Education vs Usual Care/Control Education on the Number of Primary Care Visits in the 12 Months After Intervention
Favors(experimental)
–2 20 1SMD (IV, Random, 95% CI)
–1
Weight, %Favors(control)SMD (SE)Source
SMD(IV, Random, 95% CI)
7.0–0.41 (0.27)Hill et al,55 2011 –0.41 (–0.94 to 0.12)15.7–0.33 (0.18)Pengel et al,53 2007 –0.33 (–0.68 to 0.02)11.6–0.21 (0.21)Deyo et al,60 1987 –0.21 (–0.62 to 0.20)19.9–0.15 (0.16)Roland et al,64 1989 –0.15 (–0.46 to 0.16)14.1–0.06 (0.19)Cherkin et al,59 1996 –0.06 (–0.43 to 0.31)14.10 (0.19)Karjalainen et al,63 2003 0.00 (–0.37 to 0.37)17.60.03 (0.17)Hay et al,61 2005 0.03 (–0.30 to 0.36)
Heterogeneity: τ2 = 0.00; χ2 = 3.95 (P = .68); I 2 = 0%100.00Total (95% CI)
6
–0.14 (–0.28 to 0.00)
Test for overall effect: z = 1.93 (P = .05)
IV indicates inverse variance; SMD, standardized mean difference.
Research Original Investigation Reassurance in Patients With Acute Low Back Pain
E8 JAMA Internal Medicine Published online March 23, 2015 (Reprinted) jamainternalmedicine.com
Copyright 2015 American Medical Association. All rights reserved.
11

Copyright 2015 American Medical Association. All rights reserved.
Effect of Primary Care–Based Education on Reassurancein Patients With Acute Low Back PainSystematic Review and Meta-analysisAdrian C. Traeger, MPhty; Markus Hübscher, PhD; Nicholas Henschke, PhD; G. Lorimer Moseley, PhD;Hopin Lee, MPhty; James H. McAuley, PhD
IMPORTANCE Reassurance is a core aspect of daily medical practice, yet little is known on howit can be achieved.
OBJECTIVE To determine whether patient education in primary care increases reassurance inpatients with acute or subacute low back pain (LBP).
DATA SOURCES Medline, EMBASE, Cochrane Central Register for Controlled Trials, andPsychINFO databases were searched to June 2014.
DESIGN Systematic review and meta-analysis of randomized and nonrandomized clinicaltrials.
STUDY SELECTION To be eligible, studies needed to be controlled trials of patient educationfor LBP that were delivered in primary care and measured reassurance after the intervention.Eligibility criteria were applied, and studies were selected by 2 independent authors.
MAIN OUTCOMES AND MEASURES The primary outcomes were reassurance in the short andlong term and health care utilization at 12 months.
DATA EXTRACTION AND SYNTHESIS Data were extracted by 2 independent authors andentered into a standardized form. A random-effects meta-analysis tested the effects ofpatient education compared with usual care on measures of reassurance. To investigate theeffect of study characteristics, we performed a preplanned subgroup analysis. Studies werestratified according to duration, content, and provider of patient education.
RESULTS We included 14 trials (n = 4872) of patient education interventions. Trials assessedreassurance with questionnaires of fear, worry, anxiety, catastrophization, and health careutilization. There is moderate- to high-quality evidence that patient education increasesreassurance more than usual care/control education in the short term (standardized meandifference [SMD], −0.21; 95% CI, −0.35 to −0.06) and long term (SMD, −0.15; 95% CI, −0.27to −0.03). Interventions delivered by physicians were significantly more reassuring thanthose delivered by other primary care practitioners (eg, physiotherapist or nurse). There ismoderate-quality evidence that patient education reduces LBP-related primary care visitsmore than usual care/control education (SMD, −0.14; 95% CI, −0.28 to −0.00 at a 12-monthfollow-up). The number needed to treat to prevent 1 LBP-related visit to primary care was 17.
CONCLUSIONS AND RELEVANCE There is moderate- to high-quality evidence that patienteducation in primary care can provide long-term reassurance for patients with acute orsubacute LBP.
JAMA Intern Med. doi:10.1001/jamainternmed.2015.0217Published online March 23, 2015.
Invited Commentary
Supplemental content atjamainternalmedicine.com
Author Affiliations: NeuroscienceResearch Australia, Sydney, Australia(Traeger, Hübscher, Moseley, Lee,McAuley); School of MedicalSciences, University of New SouthWales, Sydney, Australia (Traeger,Lee, McAuley); Institute of PublicHealth, University of Heidelberg,Heidelberg, Germany (Henschke);Sansom Institute for Health Research,University of South Australia,Adelaide, South Australia, Australia(Moseley).
Corresponding Author: James H.McAuley, PhD, NeuroscienceResearch Australia, Barker Street,Randwick, NSW 2031, Australia([email protected]).
Research
Original Investigation | LESS IS MORE
(Reprinted) E1
Copyright 2015 American Medical Association. All rights reserved.
JAMA Intern Med.Published online March 23. 2015
Copyright 2015 American Medical Association. All rights reserved.
suggests that effective reassurance involves a shift in a pa-tient’s cognitive appraisal of their health problem. Reap-praisal of the problem then reduces health-seeking behaviorin spite of ongoing symptoms.21 For nonspecific conditions,where ongoing symptoms are likely and the risk of excessivehealth care use is high, reassurance is a particularly relevantoutcome in primary care.
InterpretationOur data suggest that when practitioners are trained to de-liver structured patient education interventions, the reassur-ance this provides to patients is superior to usual care. A re-cent survey of Australian general practice activity found thatonly 20% of primary care physicians report giving advice andeducation of this type in the treatment of LBP.34 Patient edu-
Figure 2. Differences in Short-term Effects of Patient Education Interventions on Reassurance, When Interventions Are StratifiedAccording to the Deliverer of the Intervention
Favors(experimental)
–2 20 1SMD (IV, Random, 95% CI)
–1
Weight, %Favors(control)SMD (SE)Source
Physiotherapist
SMD(IV, Random, 95% CI)
5.3–0.28 (0.25)Hill et al,55 2011 –0.28 (–0.77 to 0.21)10.9–0.01 (0.10)Hay et al,61 2005 –0.01 (–0.21 to 0.19)
9.50.08 (0.13)Pengel et al,53 2007 0.08 (–0.17 to 0.33)
Heterogeneity: τ2 = 0.00; χ2 = 1.64 (P = .44); I 2 = 0%25.7Subtotal (95% CI)
2
–0.00 (–0.15 to 0.14)
Test for overall effect: z = 0.06 (P = .96) Physician
7.1–0.89 (0.19)Burton et al,57 1999 –0.89 (–1.26 to –0.52)5.0–0.76 (0.26)Storheim et al,65 2003 –0.76 (–1.27 to –0.25)5.0–0.31 (0.26)Roberts et al,54 2002 –0.31 (–0.82 to 0.20)
10.4–0.24 (0.11)Jellema et al,62 2005 –0.24 (–0.46 to –0.02)6.8–0.18 (0.20)Bücker et al,51 2010 –0.18 (–0.57 to 0.21)
10.9–0.12 (0.10)Hagen et al,52 2000 –0.12 (–0.32 to 0.08)
Heterogeneity: τ2 = 0.06; χ2 = 16.65 (P = .005); I 2 = 70%45.2Subtotal (95% CI)
5
–0.38 (–0.63 to –0.14)
Test for overall effect: z = 3.06 (P = .002) Nurse
12.2–0.30 (0.07)Leonhardt et al,56 2008 –0.30 (–0.44 to –0.16)8.3–0.15 (0.16)Deyo et al,60 1987 –0.15 (–0.46 to 0.16)8.70.17 (0.15)Cherkin et al,59 1996 0.17 (–0.12 to 0.46)
Heterogeneity: τ2 = 0.05; χ2 = 8.21 (P = .02); I 2 = 76%29.1Subtotal (95% CI)
2
2
–0.11 (–0.40 to 0.17)
Test for overall effect: z = 0.78 (P = .44)
Heterogeneity: τ2 = 0.04; χ 2 = 35.26 (P <.001); I 2 = 69%100.00Total (95% CI)
11
–0.21 (–0.35 to –0.07)
Test for overall effect: z = 2.87 (P = .004) Test for subgroup differences: χ2 = 6.69 (P = .04); I 2 = 70.1%
IV indicates inverse variance; SMD, standardized mean difference.
Figure 3. Effects of Patient Education vs Usual Care/Control Education on the Number of Primary Care Visits in the 12 Months After Intervention
Favors(experimental)
–2 20 1SMD (IV, Random, 95% CI)
–1
Weight, %Favors(control)SMD (SE)Source
SMD(IV, Random, 95% CI)
7.0–0.41 (0.27)Hill et al,55 2011 –0.41 (–0.94 to 0.12)15.7–0.33 (0.18)Pengel et al,53 2007 –0.33 (–0.68 to 0.02)11.6–0.21 (0.21)Deyo et al,60 1987 –0.21 (–0.62 to 0.20)19.9–0.15 (0.16)Roland et al,64 1989 –0.15 (–0.46 to 0.16)14.1–0.06 (0.19)Cherkin et al,59 1996 –0.06 (–0.43 to 0.31)14.10 (0.19)Karjalainen et al,63 2003 0.00 (–0.37 to 0.37)17.60.03 (0.17)Hay et al,61 2005 0.03 (–0.30 to 0.36)
Heterogeneity: τ2 = 0.00; χ2 = 3.95 (P = .68); I 2 = 0%100.00Total (95% CI)
6
–0.14 (–0.28 to 0.00)
Test for overall effect: z = 1.93 (P = .05)
IV indicates inverse variance; SMD, standardized mean difference.
Research Original Investigation Reassurance in Patients With Acute Low Back Pain
E8 JAMA Internal Medicine Published online March 23, 2015 (Reprinted) jamainternalmedicine.com
Copyright 2015 American Medical Association. All rights reserved.
11

12
¿Estamos preparados para identificar factores psicosociales?

12
¿Estamos preparados para identificar factores psicosociales?
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004

12
¿Estamos preparados para identificar factores psicosociales?
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Overmeer et al., 2004). In addition there is also evidence that re-lates various psychosocial factors directly to development ofdisability in various musculoskeletal conditions (Pincus et al., 2002;Burton et al., 2004; Åsenlof and Soderlund, 2010).
Although there has been an increased interest in the psychoso-cial aspect of disability, amajor difficulty in exploring this area is thevaried description and lack of consensus regarding the definition ofthe psychosocial construct in the literature (Martikainen et al.,2002; Egan et al., 2008). In the pain, particularly chronic pain liter-ature, psychosocial factors have been described as the combinationof the individual's cognitive (e.g. attitudes, beliefs) and emotional(e.g. mood state) status and the cultural, family and work circum-stances (e.g. support, cohesion, control and efficacy, security andautonomy) that together influence their thoughts, behaviours andtheir biomedical health condition (Pincus et al., 2002; Egan et al.,2008; Nicholas et al., 2011). However, literature on therapies forpain has tended to focus more on physiological mechanisms andclinical aspects of its management (Sim and Smith, 2004) with lessexplicit attention to psychosocial, and in particular social, de-terminants of health. Musculoskeletal chronic pain patients oftenexpress some of their psychosocial ‘barriers to recovery’ in the formof altered cognition, behaviours and physical symptoms, includingpain sensitivity, somatisation, symptoms magnification and poorparticipation with physiotherapy (Gatchel and Wright, 2002). Psy-chosocial factors not only impact on the patient's disability (i.e. pain,impairments in structure and function, activity and participationrestrictions) but their disability experience in turn reciprocally af-fects their psychosocial status (WHO, 2001). The increasing under-standing of the contribution from psychosocial factors tomusculoskeletal conditions has added to the growing calls forphysiotherapists to adopt a more holistic biopsychosocial approachto their assessment that includes psychosocial factors along withphysical factors for all musculoskeletal conditions (Jones andEdwards, 2006; Green et al., 2008; Laisn!e et al., 2012).
1.1. Study context
Physiotherapists in Australia have been primary contact practi-tioners for over 30 years. Historically physiotherapists working inmusculoskeletal oriented private practice have followed a pre-dominantly biomedical model (Sanders et al., 2013). However, withthe increasing prominence of the more contemporary bio-psychosocial model, clinicians are increasingly challenged throughthe literature and through professional development education, tobroaden their practice approach. Current physiotherapy standardsindicate that all physiotherapists should be well educated in theassessment of physical and environmental factors that contributeto and are influenced by patients' pain and disability (AustralianPhysiotherapy Council 2006, p. 51). Additionally there is long-standing evidence in favour of assessing various psychosocial fac-tors while assessing any musculoskeletal presentation. Forexample, the Australian Acute Musculoskeletal Pain GuidelinesGroup (2004) and WorkCover (2007) recognised various psycho-social factors such as attitudes and beliefs about pain, emotion andbehaviour that can influence musculoskeletal presentationsalthough the social influence on disability is notably absent. Inaddition to the evidence of close links between chronic musculo-skeletal oriented pain and psychosocial factors, there is also evi-dence that psychosocial factors play a role in acute musculoskeletalpain, possibly contributing to the transition of acute to chronicpresentations (Linton, 2000; Pincus et al., 2002a; Burton et al.,2004; Blyth et al., 2007; Heneweer et al., 2007; Jensen et al.,2011; Laisn!e et al., 2012).
Given themounting evidence on the importance of psychosocialfactors to disability (Laisn!e et al., 2012; Sanders et al., 2013),
physiotherapists have been encouraged to assess patients' psy-chosocial status. However, while a number of resources coveringbiopsychosocial theory and application to practice exist (e.g.Schultz et al., 2002; French and Sim, 2004; Main et al., 2010) it isreported that physiotherapists' understanding and assessment ofpatients' psychosocial status is often less developed and lessstructured (Haggman et al., 2004; Overmeer et al., 2004; Main andGeorge, 2011) than their assessment of physical problems (Sanderset al., 2013). It was demonstrated that physiotherapists had diffi-culty identifying patients with severe psychosocial issues byHaggman et al. (2004) through a study involving 68 physiothera-pists and 232 patients. A two-item screening test for depressiontaken from Primary Care Evaluation of Mental Disorder Procedure(PRIME-MD) was found to be much more accurate than physio-therapists' judgement of the depressive state of patients with lowback pain. Similarly a survey of 102 physiotherapists revealed thatalthough most physiotherapists recognised the importance ofpsychosocial factors, they had difficulty in identifying which factorsare clinically relevant. Furthermore there is limited research onhow physiotherapists actually assess a patient's psychosocial status(Overmeer et al., 2004). The present research aims to address thisgap by exploring physiotherapists' assessment of a patient's psy-chosocial status.
2. Methods
Given the limited research in physiotherapists' understandingand practice of psychosocial assessment in musculoskeletal ori-ented private practice, a qualitative descriptive (QD) researchdesign (Sandelowski, 2000) was used to explore this issue andprovide further understanding to guide future research. As theemphasis in this research was to explore different aspects ofphysiotherapists' psychosocial assessment to inform current prac-tice and future research, rather than develop new theory, adescriptive research design was selected over grounded theory.Ethical approval was obtained from the Human Research and EthicsCommittee (HREC), University of South Australia. With the aim ofexploring this issue through semi-structured interviews, nine par-ticipants were recruited through purposeful sampling(Sandelowski, 2000; Neergaard et al., 2009).
2.1. Participant selection and recruitment
Potential participants were invited to participate through lettersor phone calls in various private physiotherapy practices in Ade-laide. The principal inclusion criteria were that participants wereregistered physiotherapists with a minimum of six months expe-rience, working in private physiotherapy practice and dealingpredominantly with patients with musculoskeletal problems. Thecriterion of minimum work experience was deemed necessary sothat participants had sufficient clinical experience on which to
Table 1Profile of participants.
Name Age Qualification Experience
Catharine 27 BPT 8 monthsEthan 32 BPT, MPT 11 yearsJoshua 25 BPT 3 yearsLachlan 36 BPT, MPT 10 yearsMax 34 BPT, MPT 11 yearsNoah 33 BPT, MPT 11 yearsOliver 53 BPT, MPT 29 yearsRobin 25 BPT, pursuing MPT 2 yearsWilliam 27 BPT, MPT 3 years
Abbreviations; BPT ¼ Bachelors of Physiotherapy, MPT ¼ Masters of Physiotherapy.
M. Singla et al. / Manual Therapy 20 (2015) 328e334 329

12
¿Estamos preparados para identificar factores psicosociales?
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
SPINE Volume 30, Number 11, pp 1316–1322©2005, Lippincott Williams & Wilkins, Inc.
Do Physical Therapists in the United KingdomRecognize Psychosocial Factors in Patients With AcuteLow Back Pain?
Annette Bishop, MSc, and Nadine E. Foster, DPhil
Study Design. A cross-sectional, descriptive vignettesurvey of practicing, musculoskeletal physical therapists.
Objectives. The aim of this study was to determine ifmusculoskeletal physical therapists, in the United King-dom, recognize when patients with low back pain (LBP)are at risk of chronicity due to psychosocial factors. Asecondary aim was to explore the advice they give topatients about work and activities.
Summary of Background Data. Psychosocial factorshave been shown to be important in the progression fromacute LBP to chronic disability. Early identification of in-dividuals at risk of developing chronic disability is impor-tant to enable targeted intervention.
Methods. Three vignettes were written based on acuteLBP patients attending for physical therapy and incorpo-rated into a self-completed postal questionnaire sent to asimple random sample of musculoskeletal physical thera-pists in the United Kingdom (n ! 900). After one reminder,20% of nonresponders were sent a further questionnaire(n ! 80). Data were analyzed using the Statistical Packagefor the Social Sciences (SPSS version 11).
Results. The response rate was 57.7% (n ! 518) with453 meeting all inclusion criteria. The sample consisted ofphysical therapists working in the musculoskeletal fieldacross all practice settings. Most correctly rated the chro-nicity risk of the low- and high-risk patient vignettes. Ad-vice to restrict work and activity was common.
Conclusions. Most physical therapists recognize whenpatients are at high risk of developing chronicity, yetmany recommend the patient limit their activity levelsand not work. Advice to “not work” is associated withmore severe perceived spinal pathology, suggesting per-sistence of the biomedical model for LBP.
Key words: low back pain, physical therapy, recom-mendations, vignettes. Spine 2005;30:1316–1322
Low back pain (LBP) and disability in particular, con-tinue to be significant healthcare problems in developedsocieties. LBP is a common condition with a lifetimeprevalence of around 58%.1,2 Traditional thinking, thatepisodes of LBP resolve rapidly, has been challenged, andthe course of LBP may be one that takes many weeks to
settle and is prone to relapse and recurrence.3,4 The eco-nomic burden of LBP was estimated to be £10,668 mil-lion pounds in the United Kingdom in 1998.5 Figuresfrom the United States estimate LBP to have had a totalimpact in the industrial setting alone in excess of $170billion6; furthermore, treatment costs for LBP are risingby at least 7% per year.7
LBP disability and costs of work loss and sicknessbenefits rose dramatically toward the end of the 20thcentury.8 In response to the increasing disability associ-ated with LBP, the appropriateness of the biomedicalmodel has been questioned and a biopsychosocial modelhas been proposed to try to improve outcomes for pa-tients with LBP.8–10 The biopsychosocial model is con-structed from the key elements of physical functioning,beliefs and coping, distress, illness behavior, and socialinteractions and has been adopted by the World HealthOrganisation in the international classification of func-tioning, disability, and health.11 This model presents auseful framework to improve the understanding of per-sistent back pain.12 Early identification of individuals atrisk of developing chronic problems is paramount, as therisk of long-term incapacity increases with time and itallows for early use of specific interventions to minimizebarriers to recovery.8,13,14 Available guidelines forhealthcare professionals involved in the management ofLBP have been published in many countries and givebroadly similar recommendations. Recommendationsinclude advising early return to work and continuationof normal activities.15,16 Bed rest should be avoided as itoffers no improvement on staying active and may exac-erbate physical deconditioning and passive coping strat-egies.17–19 Moreover, physical activity programs havebeen shown to be beneficial for LBP.20,21
In the United Kingdom, physical therapists see manypatients with LBP, with estimates varying from 9% to50%5,22 of LBP patients seeking health care. By recog-nizing risk factors to poor outcome and using interven-tions that target physical and psychosocial factors, phys-ical therapists are well placed to identify and addressbarriers to recovery early in the patient’s pain experi-ence. Failure to recognize key psychosocial factors couldinadvertently encourage chronicity. To date, no large-scale studies have been carried out to investigate whethermusculoskeletal physical therapists in the United King-dom have embraced the biopsychosocial model for themanagement of LBP, although a survey in the Nether-lands and a qualitative study in the United Kingdom have
From the Department of Physiotherapy Studies and Primary Care Sci-ences Research Centre, Keele University, Staffordshire, UK.Acknowledgment date: March 9, 2004. First revision date: May 28,2004. Second revision date: July 12, 2004. Acceptance date: July 12,2004.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Annette Bishop, MSc,Primary Care Sciences Research Centre, Keele University, Stafford-shire, ST5 5BG, United Kingdom; E-mail: [email protected]
1316
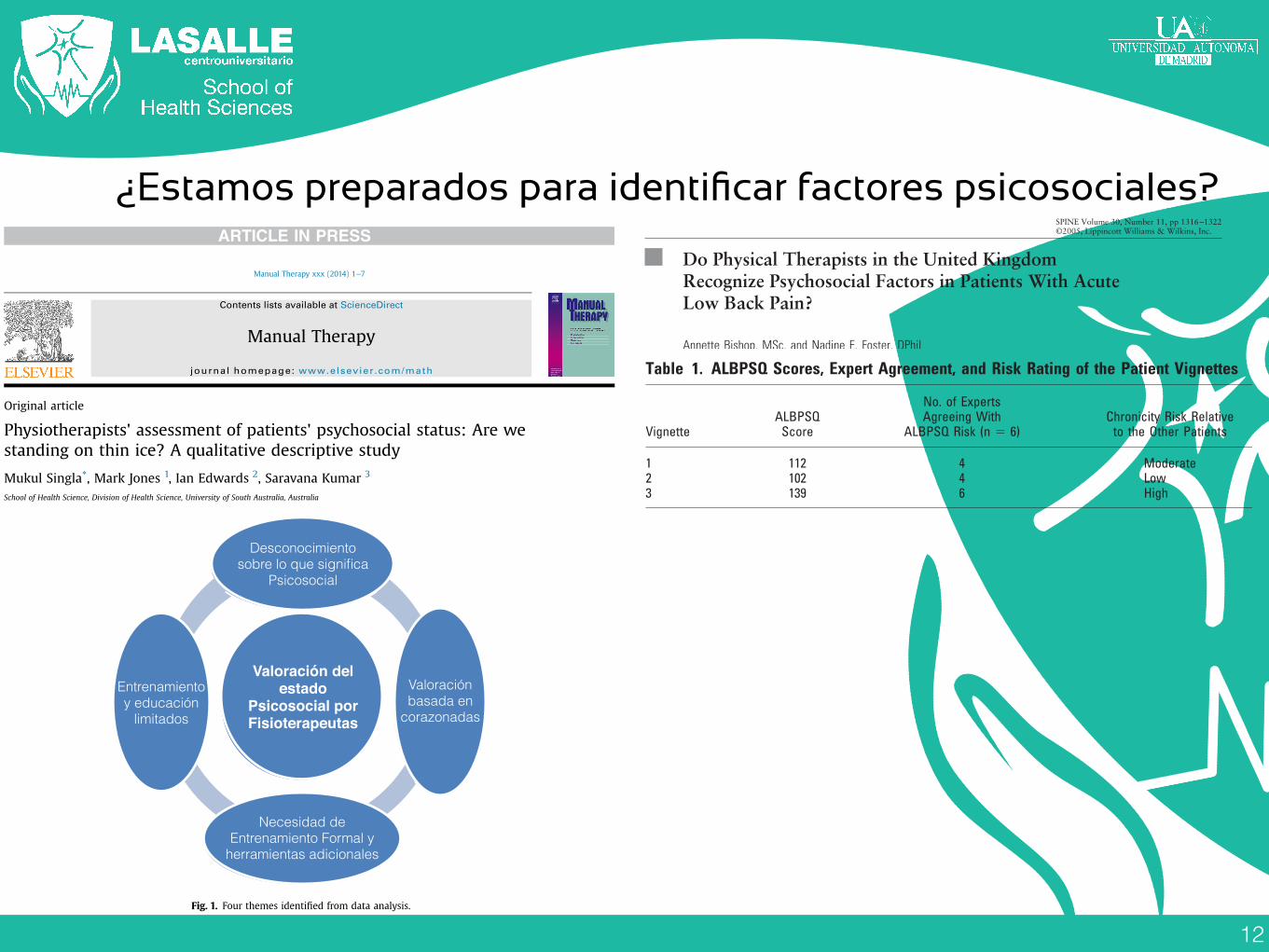
12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
SPINE Volume 30, Number 11, pp 1316–1322©2005, Lippincott Williams & Wilkins, Inc.
Do Physical Therapists in the United KingdomRecognize Psychosocial Factors in Patients With AcuteLow Back Pain?
Annette Bishop, MSc, and Nadine E. Foster, DPhil
Study Design. A cross-sectional, descriptive vignettesurvey of practicing, musculoskeletal physical therapists.
Objectives. The aim of this study was to determine ifmusculoskeletal physical therapists, in the United King-dom, recognize when patients with low back pain (LBP)are at risk of chronicity due to psychosocial factors. Asecondary aim was to explore the advice they give topatients about work and activities.
Summary of Background Data. Psychosocial factorshave been shown to be important in the progression fromacute LBP to chronic disability. Early identification of in-dividuals at risk of developing chronic disability is impor-tant to enable targeted intervention.
Methods. Three vignettes were written based on acuteLBP patients attending for physical therapy and incorpo-rated into a self-completed postal questionnaire sent to asimple random sample of musculoskeletal physical thera-pists in the United Kingdom (n ! 900). After one reminder,20% of nonresponders were sent a further questionnaire(n ! 80). Data were analyzed using the Statistical Packagefor the Social Sciences (SPSS version 11).
Results. The response rate was 57.7% (n ! 518) with453 meeting all inclusion criteria. The sample consisted ofphysical therapists working in the musculoskeletal fieldacross all practice settings. Most correctly rated the chro-nicity risk of the low- and high-risk patient vignettes. Ad-vice to restrict work and activity was common.
Conclusions. Most physical therapists recognize whenpatients are at high risk of developing chronicity, yetmany recommend the patient limit their activity levelsand not work. Advice to “not work” is associated withmore severe perceived spinal pathology, suggesting per-sistence of the biomedical model for LBP.
Key words: low back pain, physical therapy, recom-mendations, vignettes. Spine 2005;30:1316–1322
Low back pain (LBP) and disability in particular, con-tinue to be significant healthcare problems in developedsocieties. LBP is a common condition with a lifetimeprevalence of around 58%.1,2 Traditional thinking, thatepisodes of LBP resolve rapidly, has been challenged, andthe course of LBP may be one that takes many weeks to
settle and is prone to relapse and recurrence.3,4 The eco-nomic burden of LBP was estimated to be £10,668 mil-lion pounds in the United Kingdom in 1998.5 Figuresfrom the United States estimate LBP to have had a totalimpact in the industrial setting alone in excess of $170billion6; furthermore, treatment costs for LBP are risingby at least 7% per year.7
LBP disability and costs of work loss and sicknessbenefits rose dramatically toward the end of the 20thcentury.8 In response to the increasing disability associ-ated with LBP, the appropriateness of the biomedicalmodel has been questioned and a biopsychosocial modelhas been proposed to try to improve outcomes for pa-tients with LBP.8–10 The biopsychosocial model is con-structed from the key elements of physical functioning,beliefs and coping, distress, illness behavior, and socialinteractions and has been adopted by the World HealthOrganisation in the international classification of func-tioning, disability, and health.11 This model presents auseful framework to improve the understanding of per-sistent back pain.12 Early identification of individuals atrisk of developing chronic problems is paramount, as therisk of long-term incapacity increases with time and itallows for early use of specific interventions to minimizebarriers to recovery.8,13,14 Available guidelines forhealthcare professionals involved in the management ofLBP have been published in many countries and givebroadly similar recommendations. Recommendationsinclude advising early return to work and continuationof normal activities.15,16 Bed rest should be avoided as itoffers no improvement on staying active and may exac-erbate physical deconditioning and passive coping strat-egies.17–19 Moreover, physical activity programs havebeen shown to be beneficial for LBP.20,21
In the United Kingdom, physical therapists see manypatients with LBP, with estimates varying from 9% to50%5,22 of LBP patients seeking health care. By recog-nizing risk factors to poor outcome and using interven-tions that target physical and psychosocial factors, phys-ical therapists are well placed to identify and addressbarriers to recovery early in the patient’s pain experi-ence. Failure to recognize key psychosocial factors couldinadvertently encourage chronicity. To date, no large-scale studies have been carried out to investigate whethermusculoskeletal physical therapists in the United King-dom have embraced the biopsychosocial model for themanagement of LBP, although a survey in the Nether-lands and a qualitative study in the United Kingdom have
From the Department of Physiotherapy Studies and Primary Care Sci-ences Research Centre, Keele University, Staffordshire, UK.Acknowledgment date: March 9, 2004. First revision date: May 28,2004. Second revision date: July 12, 2004. Acceptance date: July 12,2004.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Annette Bishop, MSc,Primary Care Sciences Research Centre, Keele University, Stafford-shire, ST5 5BG, United Kingdom; E-mail: [email protected]
1316
found a persistence of a biomedical model in the practiceof many physical therapists.23,24
Available practice guidelines recommend clinical as-sessment to identify psychosocial factors in the first in-stance, with the use of validated questionnaires beingreserved for patients who do not make adequate progressafter initial intervention,13,15 as these can be unwieldyand time-consuming and are not commonly used byphysical therapists, particularly in acute patients or inprimary care situations.22,25,26
The current study aimed to investigate if physical ther-apists working in the musculoskeletal field, in the UnitedKingdom, can identify patients with acute LBP at risk ofdeveloping chronicity from psychosocial factors in com-mon clinical scenarios. Second, the study aimed to ex-plore whether the advice that physical therapists provideto acute LBP patients related to work and activity isconsistent with current published best evidence guide-lines.
Materials and Methods
The design was a cross-sectional, descriptive survey of clini-cally active physical therapists working in the musculoskeletalfield, between July and October 2002, registered with the Char-tered Society of Physiotherapy in the United Kingdom. Ethicalapproval was obtained from the West Midlands MulticenterResearch Ethics Committee in the United Kingdom, in June2002. Written consent was not sought from each participant,but consent of respondents was assumed if they completed andreturned the questionnaire.
Survey Instrument
Patient Vignettes or Case Scenarios. Three vignettes (casescenarios) of patients with acute LBP were constructed (Appen-dix A, available for viewing on ArticlePlus only). The vignettesincluded descriptions of history, symptoms, and relevant phys-ical findings and did not attempt to describe in detail any test-ing procedures that may not be used by all physical therapists.The vignettes were based on actual patients attending a physi-cal therapy clinic in the West Midlands, in the United Kingdom.Before usual assessment and treatment, patients consented tothe use of their case as a vignette and completed the Acute LowBack Pain Screening Questionnaire (ALBPSQ).27 The ALBPSQwas developed to screen patients with pain of less than 12weeks’ duration, at risk of poor outcome from psychosocialrisk factors, and its utility and cutoff points for high risk havebeen previously investigated in Sweden and Northern Ire-land.27,28 The patient population of the current study was sim-ilar to the Northern Ireland population, in that there was a mixof working and nonworking patients and all had been referred
to physical therapy. As a result, a cutoff point for poor outcomeof 112, described by Hurley et al28 was used to categorise thepatients in this study. Three patients were chosen for the vi-gnettes, one patient each at low and high risk and one patientwith a borderline score.
In line with recommendations,29 –31 the vignettes weretested by a panel of U.K. experts (identified through publica-tion history or clinical expertise, by the authors) (n ! 6), toensure the vignettes were realistic and to test that they demon-strated examples of patients at low, moderate, and high risk ofchronicity. The experts consisted of one consultant physicaltherapist, one senior physical therapy clinician, and four mus-culoskeletal researchers (three physical therapists and one os-teopath). The cutoff scores, expert agreement, and risk rating ofthe patients and the percentage of respondents agreeing withthe ALBPSQ risk are summarized in Table 1. Of the six experts,two commented that Patient 1 had more psychosocial risk fac-tors and Patient 2 had more physical risk factors. As a result,some minor modifications were made to the low-risk patientvignette (Patient 2) to reduce the physical risk factors, in orderto aid differentiation with the borderline risk case (Patient 1).
The vignettes were then incorporated into a postal, self-completed questionnaire, which sought demographic details ofthe respondents and responses to questions about the patientvignettes. The questions asked about each vignette can befound in Appendix B (available for viewing on ArticlePlusonly). The questions on work recommendation and activityadvice were taken from a previously successful questionnairesent to physicians.32
Sample. A simple random sample of Chartered Physiother-apists working in the musculoskeletal field in the United King-dom was used. The professional body generated the samplefrom a database of physical therapists who had previously self-reported the musculoskeletal field as their speciality, based ondata gathered in the year 2000. Although the database was 2years out of date, it was considered to be the best samplingframe available at the time. Further inclusion criteria were thatthe physical therapist was involved in the treatment of LBP andhad treated at least one case of acute LBP in the previous 12months. Filter questions at the beginning of the questionnaireascertained whether these two criteria were met and, if not, therespondent was asked to return the questionnaire without com-pleting the rest of the items.
A pilot study (n ! 50) demonstrated that the questionnairegenerated a response rate in keeping with other postal surveysof physical therapists,22,24,33 and levels of missing data werelow. Missing data constituted less than 1% for all but 5 ques-tionnaire items, and the maximum level of missing data for anysingle item was 3.3%. Given the estimation from the pilotstudy, that there would be approximately 52% of applicableresponses, and that less than 5% error in the key survey esti-mates was desirable, it was estimated that approximately 900
Table 1. ALBPSQ Scores, Expert Agreement, and Risk Rating of the Patient Vignettes
VignetteALBPSQ
Score
No. of ExpertsAgreeing With
ALBPSQ Risk (n ! 6)Chronicity Risk Relative
to the Other Patients% of Respondents Agreeing
With ALBPSQ Risk
1 112 4 Moderate 25.42 102 4 Low 56.63 139 6 High 89.1
1317Physical Therapists in UK • Bishop and Foster

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
SPINE Volume 30, Number 11, pp 1316–1322©2005, Lippincott Williams & Wilkins, Inc.
Do Physical Therapists in the United KingdomRecognize Psychosocial Factors in Patients With AcuteLow Back Pain?
Annette Bishop, MSc, and Nadine E. Foster, DPhil
Study Design. A cross-sectional, descriptive vignettesurvey of practicing, musculoskeletal physical therapists.
Objectives. The aim of this study was to determine ifmusculoskeletal physical therapists, in the United King-dom, recognize when patients with low back pain (LBP)are at risk of chronicity due to psychosocial factors. Asecondary aim was to explore the advice they give topatients about work and activities.
Summary of Background Data. Psychosocial factorshave been shown to be important in the progression fromacute LBP to chronic disability. Early identification of in-dividuals at risk of developing chronic disability is impor-tant to enable targeted intervention.
Methods. Three vignettes were written based on acuteLBP patients attending for physical therapy and incorpo-rated into a self-completed postal questionnaire sent to asimple random sample of musculoskeletal physical thera-pists in the United Kingdom (n ! 900). After one reminder,20% of nonresponders were sent a further questionnaire(n ! 80). Data were analyzed using the Statistical Packagefor the Social Sciences (SPSS version 11).
Results. The response rate was 57.7% (n ! 518) with453 meeting all inclusion criteria. The sample consisted ofphysical therapists working in the musculoskeletal fieldacross all practice settings. Most correctly rated the chro-nicity risk of the low- and high-risk patient vignettes. Ad-vice to restrict work and activity was common.
Conclusions. Most physical therapists recognize whenpatients are at high risk of developing chronicity, yetmany recommend the patient limit their activity levelsand not work. Advice to “not work” is associated withmore severe perceived spinal pathology, suggesting per-sistence of the biomedical model for LBP.
Key words: low back pain, physical therapy, recom-mendations, vignettes. Spine 2005;30:1316–1322
Low back pain (LBP) and disability in particular, con-tinue to be significant healthcare problems in developedsocieties. LBP is a common condition with a lifetimeprevalence of around 58%.1,2 Traditional thinking, thatepisodes of LBP resolve rapidly, has been challenged, andthe course of LBP may be one that takes many weeks to
settle and is prone to relapse and recurrence.3,4 The eco-nomic burden of LBP was estimated to be £10,668 mil-lion pounds in the United Kingdom in 1998.5 Figuresfrom the United States estimate LBP to have had a totalimpact in the industrial setting alone in excess of $170billion6; furthermore, treatment costs for LBP are risingby at least 7% per year.7
LBP disability and costs of work loss and sicknessbenefits rose dramatically toward the end of the 20thcentury.8 In response to the increasing disability associ-ated with LBP, the appropriateness of the biomedicalmodel has been questioned and a biopsychosocial modelhas been proposed to try to improve outcomes for pa-tients with LBP.8–10 The biopsychosocial model is con-structed from the key elements of physical functioning,beliefs and coping, distress, illness behavior, and socialinteractions and has been adopted by the World HealthOrganisation in the international classification of func-tioning, disability, and health.11 This model presents auseful framework to improve the understanding of per-sistent back pain.12 Early identification of individuals atrisk of developing chronic problems is paramount, as therisk of long-term incapacity increases with time and itallows for early use of specific interventions to minimizebarriers to recovery.8,13,14 Available guidelines forhealthcare professionals involved in the management ofLBP have been published in many countries and givebroadly similar recommendations. Recommendationsinclude advising early return to work and continuationof normal activities.15,16 Bed rest should be avoided as itoffers no improvement on staying active and may exac-erbate physical deconditioning and passive coping strat-egies.17–19 Moreover, physical activity programs havebeen shown to be beneficial for LBP.20,21
In the United Kingdom, physical therapists see manypatients with LBP, with estimates varying from 9% to50%5,22 of LBP patients seeking health care. By recog-nizing risk factors to poor outcome and using interven-tions that target physical and psychosocial factors, phys-ical therapists are well placed to identify and addressbarriers to recovery early in the patient’s pain experi-ence. Failure to recognize key psychosocial factors couldinadvertently encourage chronicity. To date, no large-scale studies have been carried out to investigate whethermusculoskeletal physical therapists in the United King-dom have embraced the biopsychosocial model for themanagement of LBP, although a survey in the Nether-lands and a qualitative study in the United Kingdom have
From the Department of Physiotherapy Studies and Primary Care Sci-ences Research Centre, Keele University, Staffordshire, UK.Acknowledgment date: March 9, 2004. First revision date: May 28,2004. Second revision date: July 12, 2004. Acceptance date: July 12,2004.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Annette Bishop, MSc,Primary Care Sciences Research Centre, Keele University, Stafford-shire, ST5 5BG, United Kingdom; E-mail: [email protected]
1316

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
SPINE Volume 30, Number 11, pp 1316–1322©2005, Lippincott Williams & Wilkins, Inc.
Do Physical Therapists in the United KingdomRecognize Psychosocial Factors in Patients With AcuteLow Back Pain?
Annette Bishop, MSc, and Nadine E. Foster, DPhil
Study Design. A cross-sectional, descriptive vignettesurvey of practicing, musculoskeletal physical therapists.
Objectives. The aim of this study was to determine ifmusculoskeletal physical therapists, in the United King-dom, recognize when patients with low back pain (LBP)are at risk of chronicity due to psychosocial factors. Asecondary aim was to explore the advice they give topatients about work and activities.
Summary of Background Data. Psychosocial factorshave been shown to be important in the progression fromacute LBP to chronic disability. Early identification of in-dividuals at risk of developing chronic disability is impor-tant to enable targeted intervention.
Methods. Three vignettes were written based on acuteLBP patients attending for physical therapy and incorpo-rated into a self-completed postal questionnaire sent to asimple random sample of musculoskeletal physical thera-pists in the United Kingdom (n ! 900). After one reminder,20% of nonresponders were sent a further questionnaire(n ! 80). Data were analyzed using the Statistical Packagefor the Social Sciences (SPSS version 11).
Results. The response rate was 57.7% (n ! 518) with453 meeting all inclusion criteria. The sample consisted ofphysical therapists working in the musculoskeletal fieldacross all practice settings. Most correctly rated the chro-nicity risk of the low- and high-risk patient vignettes. Ad-vice to restrict work and activity was common.
Conclusions. Most physical therapists recognize whenpatients are at high risk of developing chronicity, yetmany recommend the patient limit their activity levelsand not work. Advice to “not work” is associated withmore severe perceived spinal pathology, suggesting per-sistence of the biomedical model for LBP.
Key words: low back pain, physical therapy, recom-mendations, vignettes. Spine 2005;30:1316–1322
Low back pain (LBP) and disability in particular, con-tinue to be significant healthcare problems in developedsocieties. LBP is a common condition with a lifetimeprevalence of around 58%.1,2 Traditional thinking, thatepisodes of LBP resolve rapidly, has been challenged, andthe course of LBP may be one that takes many weeks to
settle and is prone to relapse and recurrence.3,4 The eco-nomic burden of LBP was estimated to be £10,668 mil-lion pounds in the United Kingdom in 1998.5 Figuresfrom the United States estimate LBP to have had a totalimpact in the industrial setting alone in excess of $170billion6; furthermore, treatment costs for LBP are risingby at least 7% per year.7
LBP disability and costs of work loss and sicknessbenefits rose dramatically toward the end of the 20thcentury.8 In response to the increasing disability associ-ated with LBP, the appropriateness of the biomedicalmodel has been questioned and a biopsychosocial modelhas been proposed to try to improve outcomes for pa-tients with LBP.8–10 The biopsychosocial model is con-structed from the key elements of physical functioning,beliefs and coping, distress, illness behavior, and socialinteractions and has been adopted by the World HealthOrganisation in the international classification of func-tioning, disability, and health.11 This model presents auseful framework to improve the understanding of per-sistent back pain.12 Early identification of individuals atrisk of developing chronic problems is paramount, as therisk of long-term incapacity increases with time and itallows for early use of specific interventions to minimizebarriers to recovery.8,13,14 Available guidelines forhealthcare professionals involved in the management ofLBP have been published in many countries and givebroadly similar recommendations. Recommendationsinclude advising early return to work and continuationof normal activities.15,16 Bed rest should be avoided as itoffers no improvement on staying active and may exac-erbate physical deconditioning and passive coping strat-egies.17–19 Moreover, physical activity programs havebeen shown to be beneficial for LBP.20,21
In the United Kingdom, physical therapists see manypatients with LBP, with estimates varying from 9% to50%5,22 of LBP patients seeking health care. By recog-nizing risk factors to poor outcome and using interven-tions that target physical and psychosocial factors, phys-ical therapists are well placed to identify and addressbarriers to recovery early in the patient’s pain experi-ence. Failure to recognize key psychosocial factors couldinadvertently encourage chronicity. To date, no large-scale studies have been carried out to investigate whethermusculoskeletal physical therapists in the United King-dom have embraced the biopsychosocial model for themanagement of LBP, although a survey in the Nether-lands and a qualitative study in the United Kingdom have
From the Department of Physiotherapy Studies and Primary Care Sci-ences Research Centre, Keele University, Staffordshire, UK.Acknowledgment date: March 9, 2004. First revision date: May 28,2004. Second revision date: July 12, 2004. Acceptance date: July 12,2004.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Annette Bishop, MSc,Primary Care Sciences Research Centre, Keele University, Stafford-shire, ST5 5BG, United Kingdom; E-mail: [email protected]
1316
(n=453)questionnaires needed to be distributed.34 This represented20% of the total sampling frame of 4,247 physical therapists,registered with the Chartered Society of Physiotherapy andworking within the musculoskeletal field at the time of sam-pling.
The questionnaire package consisted of the questionnairewith the three vignettes, a covering letter, and a stamped ad-dressed envelope. Three weeks after distribution of the mainquestionnaire, postcard reminders were sent to all nonre-sponders. Finally, 6 weeks after the second mailing, a sample of20% (n ! 80) of the nonresponders was sent a further ques-tionnaire. Of these, 30 were returned, which permitted someassessment of nonresponse bias.
Data Analysis. Data analyses were carried out using the Sta-tistical Package for Social Scientists for Windows (SPSS Inc.,Chicago, IL, version 11). The questionnaires were precodedand an SPSS datafile created. After data input, the file waschecked for errors and some variables were recoded to enhancethe analyses. The perceived spinal pathology and chronicityrisk questions were analyzed by combining the lower two andhigher two response options, resulting in “mild,” “moderate,”and “severe” categories for the spinal pathology question and“low,” “moderate,” and “high” categories for the chronicityrisk question. The work and activity recommendation ques-tions were taken from a previous questionnaire,32 but somerespondents noted some difficulty in answering these questionsbecause of the mix of the two constructs of pain and exertion.The work recommendation question was therefore recoded toform a dichotomous response of “work” or “no work” toovercome this difficulty. It should be noted, however, that the“work” response included the “work as normal,” “work full-time, avoiding pain,” “work full-time, light duties,” and “workpart-time, light duties” response options. Advice for patients tofollow restricted duties may not be in keeping with best evi-dence as actively restricting work may be giving the patientnegative messages about work and their back pain. However,returning someone to work in any capacity may be a positivestep in the patient’s rehabilitation. To capture any positiveresponses about return to work, all of the options other than“no work” were included in the “work” response. Data wereanalyzed using descriptive statistics and crosstabulations and!2 tests were carried out to test for significant associationsbetween key survey variables.35 A significance level of P " 0.01was used throughout due to the multiple tests being carriedout.36
Results
Survey ResponseA total of 900 questionnaires were distributed and 518responses were received (response rate, 57.5%). Of the518 respondents, 453 met the inclusion criteria (involvedin the treatment of LBP and had seen at least one case ofacute LBP in the preceding 12 months) and completedthe questionnaire. The results presented here summarizethe responses of these 453 physical therapists.
NonrespondersThe sample of nonresponders (n ! 30) were very similarto the responders, in terms of their experience, worksetting, and clinical grade. They also gave similar chro-nicity ratings for all 3 patients and similar work recom-
mendations for Patients 1 and 2; however, nonre-sponders were more likely to advise the high-risk Patient3 to “not work” than responders (52% vs. 34.5%) andto rate the spinal pathology as “severe” (50% vs.37.6%).
Characteristics of Physical TherapistsAs expected, the respondents were physical therapistsworking in the musculoskeletal field with 42.5% (n !192) having completed at least one formal postgraduateeducation program, where their knowledge or skill hadbeen tested by examination or formal evaluation. Themean postgraduate practice time was 18 years (# SD 9.5years); and as expected, there were no recently qualifiedphysical therapists in the sample (minimum practicetime, 3 years). The majority of respondents workedwholly or partially within the U.K. National Health Ser-vice (61.3%).
Responses to the Vignette Questions
Therapists’ Rating of Patients’ Risk of ChronicityThe majority of therapists agreed with the chronicity riskestablished by the ALBPSQ for Patients 2 and 3, with56.6% and 89.1% stating a risk of low and high, respec-tively. The borderline Patient 1 was assessed as moderateby 25.5% of respondents, with the majority (68.9%)rating this patient as at low risk of chronicity. There wereno statistical differences in the chronicity ratings betweenthose therapists seeing at least one acute LBP patient aweek compared with those who see less than one patienta week. For example, the percentage of respondents rat-ing Patient 1 as low risk was 68.3% for those seeingmore than one patient with acute LBP a week and 69.8%for those seeing less than one patient a week.
Perceived Severity of Spinal PathologyThe majority of respondents rated the spinal pathologyas moderate in all 3 patients. A summary of the physicaltherapists’ perceived level of spinal pathology of eachpatient can be found in Table 2.
Advice on Work and ActivityThe respondents’ work recommendations are summa-rized in Figure 1. This shows that advice to “not work”was recommended by 28.6%, 11.5%, and 34.5% of re-spondents for Patients 1, 2, and 3, respectively; however,normal work was advised by only a small proportion ofrespondents (3.4%, 5.8%, and 5.6% respectively). Sim-ilarly, 95%, 88.6%, and 85.8% of physical therapists
Table 2. Summary of Perceived Level of SpinalPathology of Each Patient
Perceived Levelof Pathology
Patient 1$% (no.)%
Patient 2$% (no.)%
Patient 3$% (no.)%
Mild 38.9 (175) 33.1 (148) 17.5 (77)Moderate 54.4 (245) 60.4 (270) 44.9 (198)Severe 6.6 (30) 6.4 (29) 37.6 (166)Total 100 (450) 100 (447) 100 (441)
1318 Spine • Volume 30 • Number 11 • 2005

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
SPINE Volume 30, Number 11, pp 1316–1322©2005, Lippincott Williams & Wilkins, Inc.
Do Physical Therapists in the United KingdomRecognize Psychosocial Factors in Patients With AcuteLow Back Pain?
Annette Bishop, MSc, and Nadine E. Foster, DPhil
Study Design. A cross-sectional, descriptive vignettesurvey of practicing, musculoskeletal physical therapists.
Objectives. The aim of this study was to determine ifmusculoskeletal physical therapists, in the United King-dom, recognize when patients with low back pain (LBP)are at risk of chronicity due to psychosocial factors. Asecondary aim was to explore the advice they give topatients about work and activities.
Summary of Background Data. Psychosocial factorshave been shown to be important in the progression fromacute LBP to chronic disability. Early identification of in-dividuals at risk of developing chronic disability is impor-tant to enable targeted intervention.
Methods. Three vignettes were written based on acuteLBP patients attending for physical therapy and incorpo-rated into a self-completed postal questionnaire sent to asimple random sample of musculoskeletal physical thera-pists in the United Kingdom (n ! 900). After one reminder,20% of nonresponders were sent a further questionnaire(n ! 80). Data were analyzed using the Statistical Packagefor the Social Sciences (SPSS version 11).
Results. The response rate was 57.7% (n ! 518) with453 meeting all inclusion criteria. The sample consisted ofphysical therapists working in the musculoskeletal fieldacross all practice settings. Most correctly rated the chro-nicity risk of the low- and high-risk patient vignettes. Ad-vice to restrict work and activity was common.
Conclusions. Most physical therapists recognize whenpatients are at high risk of developing chronicity, yetmany recommend the patient limit their activity levelsand not work. Advice to “not work” is associated withmore severe perceived spinal pathology, suggesting per-sistence of the biomedical model for LBP.
Key words: low back pain, physical therapy, recom-mendations, vignettes. Spine 2005;30:1316–1322
Low back pain (LBP) and disability in particular, con-tinue to be significant healthcare problems in developedsocieties. LBP is a common condition with a lifetimeprevalence of around 58%.1,2 Traditional thinking, thatepisodes of LBP resolve rapidly, has been challenged, andthe course of LBP may be one that takes many weeks to
settle and is prone to relapse and recurrence.3,4 The eco-nomic burden of LBP was estimated to be £10,668 mil-lion pounds in the United Kingdom in 1998.5 Figuresfrom the United States estimate LBP to have had a totalimpact in the industrial setting alone in excess of $170billion6; furthermore, treatment costs for LBP are risingby at least 7% per year.7
LBP disability and costs of work loss and sicknessbenefits rose dramatically toward the end of the 20thcentury.8 In response to the increasing disability associ-ated with LBP, the appropriateness of the biomedicalmodel has been questioned and a biopsychosocial modelhas been proposed to try to improve outcomes for pa-tients with LBP.8–10 The biopsychosocial model is con-structed from the key elements of physical functioning,beliefs and coping, distress, illness behavior, and socialinteractions and has been adopted by the World HealthOrganisation in the international classification of func-tioning, disability, and health.11 This model presents auseful framework to improve the understanding of per-sistent back pain.12 Early identification of individuals atrisk of developing chronic problems is paramount, as therisk of long-term incapacity increases with time and itallows for early use of specific interventions to minimizebarriers to recovery.8,13,14 Available guidelines forhealthcare professionals involved in the management ofLBP have been published in many countries and givebroadly similar recommendations. Recommendationsinclude advising early return to work and continuationof normal activities.15,16 Bed rest should be avoided as itoffers no improvement on staying active and may exac-erbate physical deconditioning and passive coping strat-egies.17–19 Moreover, physical activity programs havebeen shown to be beneficial for LBP.20,21
In the United Kingdom, physical therapists see manypatients with LBP, with estimates varying from 9% to50%5,22 of LBP patients seeking health care. By recog-nizing risk factors to poor outcome and using interven-tions that target physical and psychosocial factors, phys-ical therapists are well placed to identify and addressbarriers to recovery early in the patient’s pain experi-ence. Failure to recognize key psychosocial factors couldinadvertently encourage chronicity. To date, no large-scale studies have been carried out to investigate whethermusculoskeletal physical therapists in the United King-dom have embraced the biopsychosocial model for themanagement of LBP, although a survey in the Nether-lands and a qualitative study in the United Kingdom have
From the Department of Physiotherapy Studies and Primary Care Sci-ences Research Centre, Keele University, Staffordshire, UK.Acknowledgment date: March 9, 2004. First revision date: May 28,2004. Second revision date: July 12, 2004. Acceptance date: July 12,2004.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Annette Bishop, MSc,Primary Care Sciences Research Centre, Keele University, Stafford-shire, ST5 5BG, United Kingdom; E-mail: [email protected]
1316
(n=453)questionnaires needed to be distributed.34 This represented20% of the total sampling frame of 4,247 physical therapists,registered with the Chartered Society of Physiotherapy andworking within the musculoskeletal field at the time of sam-pling.
The questionnaire package consisted of the questionnairewith the three vignettes, a covering letter, and a stamped ad-dressed envelope. Three weeks after distribution of the mainquestionnaire, postcard reminders were sent to all nonre-sponders. Finally, 6 weeks after the second mailing, a sample of20% (n ! 80) of the nonresponders was sent a further ques-tionnaire. Of these, 30 were returned, which permitted someassessment of nonresponse bias.
Data Analysis. Data analyses were carried out using the Sta-tistical Package for Social Scientists for Windows (SPSS Inc.,Chicago, IL, version 11). The questionnaires were precodedand an SPSS datafile created. After data input, the file waschecked for errors and some variables were recoded to enhancethe analyses. The perceived spinal pathology and chronicityrisk questions were analyzed by combining the lower two andhigher two response options, resulting in “mild,” “moderate,”and “severe” categories for the spinal pathology question and“low,” “moderate,” and “high” categories for the chronicityrisk question. The work and activity recommendation ques-tions were taken from a previous questionnaire,32 but somerespondents noted some difficulty in answering these questionsbecause of the mix of the two constructs of pain and exertion.The work recommendation question was therefore recoded toform a dichotomous response of “work” or “no work” toovercome this difficulty. It should be noted, however, that the“work” response included the “work as normal,” “work full-time, avoiding pain,” “work full-time, light duties,” and “workpart-time, light duties” response options. Advice for patients tofollow restricted duties may not be in keeping with best evi-dence as actively restricting work may be giving the patientnegative messages about work and their back pain. However,returning someone to work in any capacity may be a positivestep in the patient’s rehabilitation. To capture any positiveresponses about return to work, all of the options other than“no work” were included in the “work” response. Data wereanalyzed using descriptive statistics and crosstabulations and!2 tests were carried out to test for significant associationsbetween key survey variables.35 A significance level of P " 0.01was used throughout due to the multiple tests being carriedout.36
Results
Survey ResponseA total of 900 questionnaires were distributed and 518responses were received (response rate, 57.5%). Of the518 respondents, 453 met the inclusion criteria (involvedin the treatment of LBP and had seen at least one case ofacute LBP in the preceding 12 months) and completedthe questionnaire. The results presented here summarizethe responses of these 453 physical therapists.
NonrespondersThe sample of nonresponders (n ! 30) were very similarto the responders, in terms of their experience, worksetting, and clinical grade. They also gave similar chro-nicity ratings for all 3 patients and similar work recom-
mendations for Patients 1 and 2; however, nonre-sponders were more likely to advise the high-risk Patient3 to “not work” than responders (52% vs. 34.5%) andto rate the spinal pathology as “severe” (50% vs.37.6%).
Characteristics of Physical TherapistsAs expected, the respondents were physical therapistsworking in the musculoskeletal field with 42.5% (n !192) having completed at least one formal postgraduateeducation program, where their knowledge or skill hadbeen tested by examination or formal evaluation. Themean postgraduate practice time was 18 years (# SD 9.5years); and as expected, there were no recently qualifiedphysical therapists in the sample (minimum practicetime, 3 years). The majority of respondents workedwholly or partially within the U.K. National Health Ser-vice (61.3%).
Responses to the Vignette Questions
Therapists’ Rating of Patients’ Risk of ChronicityThe majority of therapists agreed with the chronicity riskestablished by the ALBPSQ for Patients 2 and 3, with56.6% and 89.1% stating a risk of low and high, respec-tively. The borderline Patient 1 was assessed as moderateby 25.5% of respondents, with the majority (68.9%)rating this patient as at low risk of chronicity. There wereno statistical differences in the chronicity ratings betweenthose therapists seeing at least one acute LBP patient aweek compared with those who see less than one patienta week. For example, the percentage of respondents rat-ing Patient 1 as low risk was 68.3% for those seeingmore than one patient with acute LBP a week and 69.8%for those seeing less than one patient a week.
Perceived Severity of Spinal PathologyThe majority of respondents rated the spinal pathologyas moderate in all 3 patients. A summary of the physicaltherapists’ perceived level of spinal pathology of eachpatient can be found in Table 2.
Advice on Work and ActivityThe respondents’ work recommendations are summa-rized in Figure 1. This shows that advice to “not work”was recommended by 28.6%, 11.5%, and 34.5% of re-spondents for Patients 1, 2, and 3, respectively; however,normal work was advised by only a small proportion ofrespondents (3.4%, 5.8%, and 5.6% respectively). Sim-ilarly, 95%, 88.6%, and 85.8% of physical therapists
Table 2. Summary of Perceived Level of SpinalPathology of Each Patient
Perceived Levelof Pathology
Patient 1$% (no.)%
Patient 2$% (no.)%
Patient 3$% (no.)%
Mild 38.9 (175) 33.1 (148) 17.5 (77)Moderate 54.4 (245) 60.4 (270) 44.9 (198)Severe 6.6 (30) 6.4 (29) 37.6 (166)Total 100 (450) 100 (447) 100 (441)
1318 Spine • Volume 30 • Number 11 • 2005

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
SPINE Volume 30, Number 11, pp 1316–1322©2005, Lippincott Williams & Wilkins, Inc.
Do Physical Therapists in the United KingdomRecognize Psychosocial Factors in Patients With AcuteLow Back Pain?
Annette Bishop, MSc, and Nadine E. Foster, DPhil
Study Design. A cross-sectional, descriptive vignettesurvey of practicing, musculoskeletal physical therapists.
Objectives. The aim of this study was to determine ifmusculoskeletal physical therapists, in the United King-dom, recognize when patients with low back pain (LBP)are at risk of chronicity due to psychosocial factors. Asecondary aim was to explore the advice they give topatients about work and activities.
Summary of Background Data. Psychosocial factorshave been shown to be important in the progression fromacute LBP to chronic disability. Early identification of in-dividuals at risk of developing chronic disability is impor-tant to enable targeted intervention.
Methods. Three vignettes were written based on acuteLBP patients attending for physical therapy and incorpo-rated into a self-completed postal questionnaire sent to asimple random sample of musculoskeletal physical thera-pists in the United Kingdom (n ! 900). After one reminder,20% of nonresponders were sent a further questionnaire(n ! 80). Data were analyzed using the Statistical Packagefor the Social Sciences (SPSS version 11).
Results. The response rate was 57.7% (n ! 518) with453 meeting all inclusion criteria. The sample consisted ofphysical therapists working in the musculoskeletal fieldacross all practice settings. Most correctly rated the chro-nicity risk of the low- and high-risk patient vignettes. Ad-vice to restrict work and activity was common.
Conclusions. Most physical therapists recognize whenpatients are at high risk of developing chronicity, yetmany recommend the patient limit their activity levelsand not work. Advice to “not work” is associated withmore severe perceived spinal pathology, suggesting per-sistence of the biomedical model for LBP.
Key words: low back pain, physical therapy, recom-mendations, vignettes. Spine 2005;30:1316–1322
Low back pain (LBP) and disability in particular, con-tinue to be significant healthcare problems in developedsocieties. LBP is a common condition with a lifetimeprevalence of around 58%.1,2 Traditional thinking, thatepisodes of LBP resolve rapidly, has been challenged, andthe course of LBP may be one that takes many weeks to
settle and is prone to relapse and recurrence.3,4 The eco-nomic burden of LBP was estimated to be £10,668 mil-lion pounds in the United Kingdom in 1998.5 Figuresfrom the United States estimate LBP to have had a totalimpact in the industrial setting alone in excess of $170billion6; furthermore, treatment costs for LBP are risingby at least 7% per year.7
LBP disability and costs of work loss and sicknessbenefits rose dramatically toward the end of the 20thcentury.8 In response to the increasing disability associ-ated with LBP, the appropriateness of the biomedicalmodel has been questioned and a biopsychosocial modelhas been proposed to try to improve outcomes for pa-tients with LBP.8–10 The biopsychosocial model is con-structed from the key elements of physical functioning,beliefs and coping, distress, illness behavior, and socialinteractions and has been adopted by the World HealthOrganisation in the international classification of func-tioning, disability, and health.11 This model presents auseful framework to improve the understanding of per-sistent back pain.12 Early identification of individuals atrisk of developing chronic problems is paramount, as therisk of long-term incapacity increases with time and itallows for early use of specific interventions to minimizebarriers to recovery.8,13,14 Available guidelines forhealthcare professionals involved in the management ofLBP have been published in many countries and givebroadly similar recommendations. Recommendationsinclude advising early return to work and continuationof normal activities.15,16 Bed rest should be avoided as itoffers no improvement on staying active and may exac-erbate physical deconditioning and passive coping strat-egies.17–19 Moreover, physical activity programs havebeen shown to be beneficial for LBP.20,21
In the United Kingdom, physical therapists see manypatients with LBP, with estimates varying from 9% to50%5,22 of LBP patients seeking health care. By recog-nizing risk factors to poor outcome and using interven-tions that target physical and psychosocial factors, phys-ical therapists are well placed to identify and addressbarriers to recovery early in the patient’s pain experi-ence. Failure to recognize key psychosocial factors couldinadvertently encourage chronicity. To date, no large-scale studies have been carried out to investigate whethermusculoskeletal physical therapists in the United King-dom have embraced the biopsychosocial model for themanagement of LBP, although a survey in the Nether-lands and a qualitative study in the United Kingdom have
From the Department of Physiotherapy Studies and Primary Care Sci-ences Research Centre, Keele University, Staffordshire, UK.Acknowledgment date: March 9, 2004. First revision date: May 28,2004. Second revision date: July 12, 2004. Acceptance date: July 12,2004.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Annette Bishop, MSc,Primary Care Sciences Research Centre, Keele University, Stafford-shire, ST5 5BG, United Kingdom; E-mail: [email protected]
1316
(n=453)questionnaires needed to be distributed.34 This represented20% of the total sampling frame of 4,247 physical therapists,registered with the Chartered Society of Physiotherapy andworking within the musculoskeletal field at the time of sam-pling.
The questionnaire package consisted of the questionnairewith the three vignettes, a covering letter, and a stamped ad-dressed envelope. Three weeks after distribution of the mainquestionnaire, postcard reminders were sent to all nonre-sponders. Finally, 6 weeks after the second mailing, a sample of20% (n ! 80) of the nonresponders was sent a further ques-tionnaire. Of these, 30 were returned, which permitted someassessment of nonresponse bias.
Data Analysis. Data analyses were carried out using the Sta-tistical Package for Social Scientists for Windows (SPSS Inc.,Chicago, IL, version 11). The questionnaires were precodedand an SPSS datafile created. After data input, the file waschecked for errors and some variables were recoded to enhancethe analyses. The perceived spinal pathology and chronicityrisk questions were analyzed by combining the lower two andhigher two response options, resulting in “mild,” “moderate,”and “severe” categories for the spinal pathology question and“low,” “moderate,” and “high” categories for the chronicityrisk question. The work and activity recommendation ques-tions were taken from a previous questionnaire,32 but somerespondents noted some difficulty in answering these questionsbecause of the mix of the two constructs of pain and exertion.The work recommendation question was therefore recoded toform a dichotomous response of “work” or “no work” toovercome this difficulty. It should be noted, however, that the“work” response included the “work as normal,” “work full-time, avoiding pain,” “work full-time, light duties,” and “workpart-time, light duties” response options. Advice for patients tofollow restricted duties may not be in keeping with best evi-dence as actively restricting work may be giving the patientnegative messages about work and their back pain. However,returning someone to work in any capacity may be a positivestep in the patient’s rehabilitation. To capture any positiveresponses about return to work, all of the options other than“no work” were included in the “work” response. Data wereanalyzed using descriptive statistics and crosstabulations and!2 tests were carried out to test for significant associationsbetween key survey variables.35 A significance level of P " 0.01was used throughout due to the multiple tests being carriedout.36
Results
Survey ResponseA total of 900 questionnaires were distributed and 518responses were received (response rate, 57.5%). Of the518 respondents, 453 met the inclusion criteria (involvedin the treatment of LBP and had seen at least one case ofacute LBP in the preceding 12 months) and completedthe questionnaire. The results presented here summarizethe responses of these 453 physical therapists.
NonrespondersThe sample of nonresponders (n ! 30) were very similarto the responders, in terms of their experience, worksetting, and clinical grade. They also gave similar chro-nicity ratings for all 3 patients and similar work recom-
mendations for Patients 1 and 2; however, nonre-sponders were more likely to advise the high-risk Patient3 to “not work” than responders (52% vs. 34.5%) andto rate the spinal pathology as “severe” (50% vs.37.6%).
Characteristics of Physical TherapistsAs expected, the respondents were physical therapistsworking in the musculoskeletal field with 42.5% (n !192) having completed at least one formal postgraduateeducation program, where their knowledge or skill hadbeen tested by examination or formal evaluation. Themean postgraduate practice time was 18 years (# SD 9.5years); and as expected, there were no recently qualifiedphysical therapists in the sample (minimum practicetime, 3 years). The majority of respondents workedwholly or partially within the U.K. National Health Ser-vice (61.3%).
Responses to the Vignette Questions
Therapists’ Rating of Patients’ Risk of ChronicityThe majority of therapists agreed with the chronicity riskestablished by the ALBPSQ for Patients 2 and 3, with56.6% and 89.1% stating a risk of low and high, respec-tively. The borderline Patient 1 was assessed as moderateby 25.5% of respondents, with the majority (68.9%)rating this patient as at low risk of chronicity. There wereno statistical differences in the chronicity ratings betweenthose therapists seeing at least one acute LBP patient aweek compared with those who see less than one patienta week. For example, the percentage of respondents rat-ing Patient 1 as low risk was 68.3% for those seeingmore than one patient with acute LBP a week and 69.8%for those seeing less than one patient a week.
Perceived Severity of Spinal PathologyThe majority of respondents rated the spinal pathologyas moderate in all 3 patients. A summary of the physicaltherapists’ perceived level of spinal pathology of eachpatient can be found in Table 2.
Advice on Work and ActivityThe respondents’ work recommendations are summa-rized in Figure 1. This shows that advice to “not work”was recommended by 28.6%, 11.5%, and 34.5% of re-spondents for Patients 1, 2, and 3, respectively; however,normal work was advised by only a small proportion ofrespondents (3.4%, 5.8%, and 5.6% respectively). Sim-ilarly, 95%, 88.6%, and 85.8% of physical therapists
Table 2. Summary of Perceived Level of SpinalPathology of Each Patient
Perceived Levelof Pathology
Patient 1$% (no.)%
Patient 2$% (no.)%
Patient 3$% (no.)%
Mild 38.9 (175) 33.1 (148) 17.5 (77)Moderate 54.4 (245) 60.4 (270) 44.9 (198)Severe 6.6 (30) 6.4 (29) 37.6 (166)Total 100 (450) 100 (447) 100 (441)
1318 Spine • Volume 30 • Number 11 • 2005
advised some restriction of physical activities, for Pa-tients 1, 2, and 3, respectively. Again, there were nostatistical differences between those therapists seeing pa-tients with acute LBP more often (at least one case aweek) or less often (less than one case a week), with70.3% and 73.4%, respectively, advising Patient 1 to“work.”
Chronicity Rating and Work RecommendationThe therapists’ assessments of each patient’s chronicityrisk were not consistently associated with their workrecommendations. There was no significant associationbetween the reported chronicity risk and work recom-mendation for Patient 1 (!2 ! 1.7, P ! 0.421). However,there was a significant association between these vari-ables for Patient 2 with those rating this patient as at“high risk” of chronicity being more likely to recom-mend the patient to “not work” (!2 ! 21.8, P " 0.001).It should be noted that the numbers in the high-riskcrosstabulation cell were small. !2 tests were not possiblefor Patient 3 because of a low cell count in some cells ofthe cross-tabulation.
Perceived Spinal Pathology and Work RecommendationThe perceived severity of each patient’s spinal pathologyappeared to be associated with the therapists’ work rec-ommendations. There were significant associations be-tween work recommendation and perceived level of spi-nal pathology for all 3 patients (!2 ! 13.2, P ! 0.001;!2 ! 20.6, P " 0.001; !2 ! 45, P " 0.001, respectively),with the recommendation to “not work” being morelikely when pathology was perceived by the therapist tobe more severe.
Practice Setting and Work RecommendationRespondents working in the National Health Service(NHS) were more likely to report advising all 3 patients“to work” than those working in non-NHS settings, al-though this did not reach a statistically significant levelfor Patient 2 (Patient 1, !2 ! 11.1, P ! 0.001; Patient 3,!2 ! 18.9, P " 0.001).
Discussion
This survey is the first nationwide survey in the UnitedKingdom to explore whether physical therapists workingin the musculoskeletal field have adopted a biopsychoso-cial approach to the management of LBP. The responsesto questions about work and activity levels, and per-ceived severity of spinal pathology provide insights intothe therapists’ ability to recognize patients who are atrisk of chronicity and their recommendations for workand activity.
Clinical vignettes were used as this allows data to begathered about a specific situation from a large samplewhen obtaining this information in real life is impracti-cal. The advantages of using vignettes include the abilityto control and manipulate variables easily, the sugges-tion of reduced Hawthorne effects,37 reduced social de-sirability and observer bias,37,38 and the way in whichresponses are not hindered by problems of recall.29 Dis-advantages are that vignettes tend to elicit attitudes andopinions rather than measuring actual behavior in real sit-uations.29,39,40 Use of a simple random sample, a large sam-ple size, basing the vignettes on actual patients with aknown psychosocial risk and expert testing, were all in-cluded to enhance the external validity of the results. Vi-gnettes have previously been used successfully to exploreclinical decision-making in survey research with physicians,chiropractors, and physical therapists.32,41–44
Experience and Postgraduate Education ofRespondents
As expected, the therapists were very experienced interms of the number of years in clinical practice, withonly 30% of the therapists having been qualified for lessthan 10 years. In the current study, 55% of therapistswere seeing at least one patient with acute LBP a week,which may reflect the waiting lists for therapy that arecommon in the U.K. healthcare system. Despite thelengthy practice time of the therapists, 51.8% had notcompleted any postgraduate training where their knowl-
Figure 1. Summary of work rec-ommendations for the three pa-tient vignettes. Patient one, mod-erate risk; Patient two, low risk;Patient three, high risk.
1319Physical Therapists in UK • Bishop and Foster

12
¿Estamos preparados para identificar factores psicosociales?
reflect. Physiotherapists working in fields other than private prac-tice or currently working in a capacity other than a clinical practi-tioner (e.g. clinical educator, clinical supervisor, and clinicaladministration) were excluded from the study. Nine physiothera-pists working in private practice of varying age (25e53 years) andclinical experience (8 monthse29 years were recruited in thisstudy). A brief description of the participants is presented in Table 1.
2.2. Data collection
Following informed consent (Liamputtong and Ezzy, 2005),semi-structured interviews, which aid in gaining independentunderstanding of participant views (Hansen, 2006), were con-ducted at the participants' workplace. Open-ended questions wereused to minimise biasing participants' responses (Daykin andRichardson, 2004). An interview guide (refer to Appendix A)based on existing physiotherapy psychosocial assessment researchand theory was developed to ensure standardisation of questionsregarding key issues identified in the literature. Five pilot in-terviews were conducted to refine the interview guide. Partici-pants' age, gender, average working hours, years of experience andqualifications were recorded. The principal researcher conductedall interviews, which were continuously recorded and then tran-scribed verbatim.
2.3. Data analysis
Verbatim transcripts were produced from recording of semi-structured interviews. The data analysis was primarily informedby Tesch (1990) methods of coding. This method involved readingthe initial transcripts and identifying key ideas presented in eachinterview. Once various ideas were gathered, similar ideas weregrouped together and identified as codes. These codes were used tofurther identify additional segments within all transcripts. In thisprocess, common codes were recognised and grouped together toform themes (Liamputtong and Ezzy, 2005). These themesdescribed the key messages from the data gathered and variousheadings capturing the essence of those messages were given tothese themes.
Organisation of data from initial ideas to eventual themesthrough the analysis of the transcripts was assisted through the useof NVivo software. Thematic data analysis was an iterative processwhere data collection and analysis were conducted simultaneously(Liamputtong and Ezzy, 2005; Hansen, 2006) enablingmodificationof the interview guide in response to evolving analysis andemerging themes. For example, after analysing the initial threeinterview transcripts it became apparent that inquiring aboutactual strategies for assessment of psychosocial issues often ledparticipants to discuss the difficulties they faced in conducting apsychosocial assessment. This led to inclusion of a separate ques-tion in the interview guide pertaining to the barriers in conductionpsychosocial assessment as perceived by participants.
Rigour in the research process was facilitated through severalstrategies. To establish respondent validation the key summarypoints at the end of the interview (as noted by the researcher) werechecked with participants (Liamputtong and Ezzy, 2005). Cross-checking was conducted to evaluate inter-rater reliability of cod-ing (Creswell, 2009). For this two other researchers and the prin-cipal researcher coded a section of interview transcript and resultswere compared for inter-coder agreement. Coding consistency wasconducted by coding sections of interview transcripts four weeksapart and the results were found to be consistent. To promotereflexivity an effort was made to present the principal researcher asa ‘researcher interested in participants views’ and not as a ‘clinician’to minimise any perception of his own clinical views. In addition to
this, an effort was also made to minimise researcher bias byreflecting on personal clinical views during data collection as wellas data analysis. Throughout the analysis the researcher reflectedon discussions held during the interviews, and his own perceptionon how to interpret the deeper meaning of what participants hadsaid. The combination of interview notes (Merriam, 2009), andNVivo notes along with discussion with supervisors also aided thisprocess.
3. Findings
Four main interrelated themes (see Fig. 1) emerged from dataanalysis that describe various aspects of the physiotherapists' un-derstanding of and approaches towards psychosocial assessment inclinical practice. These themes were: “unclear about what psy-chosocial means”; assessment based on ‘gut feeling’; limitedtraining and education; and need for formal training and additionaltools. Each of the four main themes are described and con-textualised below with participants' own words.
3.1. Theme 1: “unclear about what psychosocial means”
Although most participants initially felt that they could recog-nise patients' psychosocial factors immediately, on further discus-sion it appeared they had limited understanding of whatpsychosocial factors entail. Many participants in this researchlimited their description of psychosocial factors to the factors thatcause delay in recovery or the chronicity of the condition. Somerelated psychosocial factors only to the compensable state of pa-tients such as WorkCover or insurance. While describing psycho-social factors in their patients, five out of nine participantscategorised their patients as either having or not having psycho-social factors. They often implied that patients belonging to acertain group were likely to have psychosocial factors, or if theyhave psychosocial factors then they likely belong to a certain group(e.g. WorkCover, insurance case or chronic condition).
Fig. 1. Four themes identified from data analysis.
M. Singla et al. / Manual Therapy xxx (2014) 1e7 3
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
Entrenamiento y educación
limitados
Valoración basada en
corazonadas
Valoración del estado
Psicosocial por Fisioterapeutas
Desconocimiento sobre lo que significa
Psicosocial
Necesidad de Entrenamiento Formal y
herramientas adicionales
Original article
Physiotherapists' assessment of patients' psychosocial status: Are westanding on thin ice? A qualitative descriptive study
Mukul Singla*, Mark Jones 1, Ian Edwards 2, Saravana Kumar 3
School of Health Science, Division of Health Science, University of South Australia, Australia
a r t i c l e i n f o
Article history:Received 30 January 2014Received in revised form25 June 2014Accepted 7 October 2014
Keywords:PsychosocialYellow flagsPhysiotherapyPhysical therapy
a b s t r a c t
Pain is a complex problem and one that confronts many physiotherapists' working in private practice ona daily basis. While physiotherapists' understanding of pain has matured a great deal in recent times,especially the role of psychosocial (PS) factors, it is unclear if and how, physiotherapists assess theirpatients' psychosocial status in clinical practice. The aim of this study was to explore private practicephysiotherapists' assessment of patients' psychosocial status.
A qualitative descriptive research design was used in this study. Participants were recruited throughpurposeful sampling and potential informants were invited to participate through letters or phone callsand data was collected via semi-structured interviews. Nine semi-structured interviews were conductedat the participants' workplaces. Data collection and analysis were conducted simultaneously and com-mon concepts and themes were recognised, coded and grouped together into themes.
Analysis of the data resulted in identification of various themes related to physiotherapists' assessmentof patients' PS status. These themes relate to; physiotherapists capacity to conduct PS assessment, thebarriers they face while conducting PS assessment and the suggestions they have provided to overcomethese barriers.
In general the physiotherapists' in this study demonstrated and acknowledged a poor understandingof the role of PS factors in their patients' clinical presentation. They were also unclear about theassessment of psychosocial factors. The barriers to assessment of psychosocial factors ranged from in-dividual shortcomings to limitations in professional networks and time constraints. The most consistentbarrier highlighted was participants' lack of formal education in PS theory and assessment.
© 2014 Published by Elsevier Ltd.
1. Introduction
Physiotherapists in private practice work with a wide variety ofpatient problems incorporating a combination of interview, ques-tionnaire and physical assessment procedures to guide their man-agement. There is increasing evidence that psychosocial factors playan important role in musculoskeletal presentations/conditions,particularly in the maintenance of musculoskeletal symptoms anddisability (Burton et al., 2004; Heneweer et al., 2007;Menezes Costaet al., 2009; Main et al., 2010; Raymond et al., 2011; Laisn!e et al.,2012). The World Health Organisation's (WHO) International
Classification of Functioning, Disability and Health (ICF) recognisesthat pain and associated disability can be influenced by a combi-nation of biomedical (i.e. health condition: diseases, disorders, in-juries), personal and environmental factors (WHO, 2001).
In the context of the ICF framework psychosocial factors areconceptualised as contextual factors with personal factors repre-senting intrinsic individual characteristics such as social back-ground, coping styles, education, past and current experiences andthe meaning they hold, all of which influence how disability isexperienced by the individual. Environmental factors are broadlycomprised of the physical, social and attitudinal environment inwhich people conduct their lives that also influence an individual'sdisability experience. There is well documented evidence of thelink between the experience of disability being influenced byvarious psychosocial factors that may include but are not limited tocognitive factors (e.g. fear avoidance beliefs, attitudes), social fac-tors (e.g. unemployment, workers compensation, social support,work relations, work satisfaction) and physical factors (e.g. musclestrength, age, physical condition) (Linton, 2000; Ariens et al., 2001;
* Corresponding author. Tel.: þ61 0421885399 (mobile).E-mail addresses: [email protected], [email protected]
(M. Singla), [email protected] (M. Jones), [email protected](I. Edwards), [email protected] (S. Kumar).
1 Tel.: þ61 08 8302 2549.2 Tel.: þ61 08 8302 2570.3 Tel.: þ61 08 8302 2085.
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier .com/math
http://dx.doi.org/10.1016/j.math.2014.10.0041356-689X/© 2014 Published by Elsevier Ltd.
Manual Therapy xxx (2014) 1e7
Please cite this article in press as: Singla M, et al., Physiotherapists' assessment of patients' psychosocial status: Are we standing on thin ice? Aqualitative descriptive study, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.10.004
SPINE Volume 30, Number 11, pp 1316–1322©2005, Lippincott Williams & Wilkins, Inc.
Do Physical Therapists in the United KingdomRecognize Psychosocial Factors in Patients With AcuteLow Back Pain?
Annette Bishop, MSc, and Nadine E. Foster, DPhil
Study Design. A cross-sectional, descriptive vignettesurvey of practicing, musculoskeletal physical therapists.
Objectives. The aim of this study was to determine ifmusculoskeletal physical therapists, in the United King-dom, recognize when patients with low back pain (LBP)are at risk of chronicity due to psychosocial factors. Asecondary aim was to explore the advice they give topatients about work and activities.
Summary of Background Data. Psychosocial factorshave been shown to be important in the progression fromacute LBP to chronic disability. Early identification of in-dividuals at risk of developing chronic disability is impor-tant to enable targeted intervention.
Methods. Three vignettes were written based on acuteLBP patients attending for physical therapy and incorpo-rated into a self-completed postal questionnaire sent to asimple random sample of musculoskeletal physical thera-pists in the United Kingdom (n ! 900). After one reminder,20% of nonresponders were sent a further questionnaire(n ! 80). Data were analyzed using the Statistical Packagefor the Social Sciences (SPSS version 11).
Results. The response rate was 57.7% (n ! 518) with453 meeting all inclusion criteria. The sample consisted ofphysical therapists working in the musculoskeletal fieldacross all practice settings. Most correctly rated the chro-nicity risk of the low- and high-risk patient vignettes. Ad-vice to restrict work and activity was common.
Conclusions. Most physical therapists recognize whenpatients are at high risk of developing chronicity, yetmany recommend the patient limit their activity levelsand not work. Advice to “not work” is associated withmore severe perceived spinal pathology, suggesting per-sistence of the biomedical model for LBP.
Key words: low back pain, physical therapy, recom-mendations, vignettes. Spine 2005;30:1316–1322
Low back pain (LBP) and disability in particular, con-tinue to be significant healthcare problems in developedsocieties. LBP is a common condition with a lifetimeprevalence of around 58%.1,2 Traditional thinking, thatepisodes of LBP resolve rapidly, has been challenged, andthe course of LBP may be one that takes many weeks to
settle and is prone to relapse and recurrence.3,4 The eco-nomic burden of LBP was estimated to be £10,668 mil-lion pounds in the United Kingdom in 1998.5 Figuresfrom the United States estimate LBP to have had a totalimpact in the industrial setting alone in excess of $170billion6; furthermore, treatment costs for LBP are risingby at least 7% per year.7
LBP disability and costs of work loss and sicknessbenefits rose dramatically toward the end of the 20thcentury.8 In response to the increasing disability associ-ated with LBP, the appropriateness of the biomedicalmodel has been questioned and a biopsychosocial modelhas been proposed to try to improve outcomes for pa-tients with LBP.8–10 The biopsychosocial model is con-structed from the key elements of physical functioning,beliefs and coping, distress, illness behavior, and socialinteractions and has been adopted by the World HealthOrganisation in the international classification of func-tioning, disability, and health.11 This model presents auseful framework to improve the understanding of per-sistent back pain.12 Early identification of individuals atrisk of developing chronic problems is paramount, as therisk of long-term incapacity increases with time and itallows for early use of specific interventions to minimizebarriers to recovery.8,13,14 Available guidelines forhealthcare professionals involved in the management ofLBP have been published in many countries and givebroadly similar recommendations. Recommendationsinclude advising early return to work and continuationof normal activities.15,16 Bed rest should be avoided as itoffers no improvement on staying active and may exac-erbate physical deconditioning and passive coping strat-egies.17–19 Moreover, physical activity programs havebeen shown to be beneficial for LBP.20,21
In the United Kingdom, physical therapists see manypatients with LBP, with estimates varying from 9% to50%5,22 of LBP patients seeking health care. By recog-nizing risk factors to poor outcome and using interven-tions that target physical and psychosocial factors, phys-ical therapists are well placed to identify and addressbarriers to recovery early in the patient’s pain experi-ence. Failure to recognize key psychosocial factors couldinadvertently encourage chronicity. To date, no large-scale studies have been carried out to investigate whethermusculoskeletal physical therapists in the United King-dom have embraced the biopsychosocial model for themanagement of LBP, although a survey in the Nether-lands and a qualitative study in the United Kingdom have
From the Department of Physiotherapy Studies and Primary Care Sci-ences Research Centre, Keele University, Staffordshire, UK.Acknowledgment date: March 9, 2004. First revision date: May 28,2004. Second revision date: July 12, 2004. Acceptance date: July 12,2004.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).No funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.Address correspondence and reprint requests to Annette Bishop, MSc,Primary Care Sciences Research Centre, Keele University, Stafford-shire, ST5 5BG, United Kingdom; E-mail: [email protected]
1316
(n=453)questionnaires needed to be distributed.34 This represented20% of the total sampling frame of 4,247 physical therapists,registered with the Chartered Society of Physiotherapy andworking within the musculoskeletal field at the time of sam-pling.
The questionnaire package consisted of the questionnairewith the three vignettes, a covering letter, and a stamped ad-dressed envelope. Three weeks after distribution of the mainquestionnaire, postcard reminders were sent to all nonre-sponders. Finally, 6 weeks after the second mailing, a sample of20% (n ! 80) of the nonresponders was sent a further ques-tionnaire. Of these, 30 were returned, which permitted someassessment of nonresponse bias.
Data Analysis. Data analyses were carried out using the Sta-tistical Package for Social Scientists for Windows (SPSS Inc.,Chicago, IL, version 11). The questionnaires were precodedand an SPSS datafile created. After data input, the file waschecked for errors and some variables were recoded to enhancethe analyses. The perceived spinal pathology and chronicityrisk questions were analyzed by combining the lower two andhigher two response options, resulting in “mild,” “moderate,”and “severe” categories for the spinal pathology question and“low,” “moderate,” and “high” categories for the chronicityrisk question. The work and activity recommendation ques-tions were taken from a previous questionnaire,32 but somerespondents noted some difficulty in answering these questionsbecause of the mix of the two constructs of pain and exertion.The work recommendation question was therefore recoded toform a dichotomous response of “work” or “no work” toovercome this difficulty. It should be noted, however, that the“work” response included the “work as normal,” “work full-time, avoiding pain,” “work full-time, light duties,” and “workpart-time, light duties” response options. Advice for patients tofollow restricted duties may not be in keeping with best evi-dence as actively restricting work may be giving the patientnegative messages about work and their back pain. However,returning someone to work in any capacity may be a positivestep in the patient’s rehabilitation. To capture any positiveresponses about return to work, all of the options other than“no work” were included in the “work” response. Data wereanalyzed using descriptive statistics and crosstabulations and!2 tests were carried out to test for significant associationsbetween key survey variables.35 A significance level of P " 0.01was used throughout due to the multiple tests being carriedout.36
Results
Survey ResponseA total of 900 questionnaires were distributed and 518responses were received (response rate, 57.5%). Of the518 respondents, 453 met the inclusion criteria (involvedin the treatment of LBP and had seen at least one case ofacute LBP in the preceding 12 months) and completedthe questionnaire. The results presented here summarizethe responses of these 453 physical therapists.
NonrespondersThe sample of nonresponders (n ! 30) were very similarto the responders, in terms of their experience, worksetting, and clinical grade. They also gave similar chro-nicity ratings for all 3 patients and similar work recom-
mendations for Patients 1 and 2; however, nonre-sponders were more likely to advise the high-risk Patient3 to “not work” than responders (52% vs. 34.5%) andto rate the spinal pathology as “severe” (50% vs.37.6%).
Characteristics of Physical TherapistsAs expected, the respondents were physical therapistsworking in the musculoskeletal field with 42.5% (n !192) having completed at least one formal postgraduateeducation program, where their knowledge or skill hadbeen tested by examination or formal evaluation. Themean postgraduate practice time was 18 years (# SD 9.5years); and as expected, there were no recently qualifiedphysical therapists in the sample (minimum practicetime, 3 years). The majority of respondents workedwholly or partially within the U.K. National Health Ser-vice (61.3%).
Responses to the Vignette Questions
Therapists’ Rating of Patients’ Risk of ChronicityThe majority of therapists agreed with the chronicity riskestablished by the ALBPSQ for Patients 2 and 3, with56.6% and 89.1% stating a risk of low and high, respec-tively. The borderline Patient 1 was assessed as moderateby 25.5% of respondents, with the majority (68.9%)rating this patient as at low risk of chronicity. There wereno statistical differences in the chronicity ratings betweenthose therapists seeing at least one acute LBP patient aweek compared with those who see less than one patienta week. For example, the percentage of respondents rat-ing Patient 1 as low risk was 68.3% for those seeingmore than one patient with acute LBP a week and 69.8%for those seeing less than one patient a week.
Perceived Severity of Spinal PathologyThe majority of respondents rated the spinal pathologyas moderate in all 3 patients. A summary of the physicaltherapists’ perceived level of spinal pathology of eachpatient can be found in Table 2.
Advice on Work and ActivityThe respondents’ work recommendations are summa-rized in Figure 1. This shows that advice to “not work”was recommended by 28.6%, 11.5%, and 34.5% of re-spondents for Patients 1, 2, and 3, respectively; however,normal work was advised by only a small proportion ofrespondents (3.4%, 5.8%, and 5.6% respectively). Sim-ilarly, 95%, 88.6%, and 85.8% of physical therapists
Table 2. Summary of Perceived Level of SpinalPathology of Each Patient
Perceived Levelof Pathology
Patient 1$% (no.)%
Patient 2$% (no.)%
Patient 3$% (no.)%
Mild 38.9 (175) 33.1 (148) 17.5 (77)Moderate 54.4 (245) 60.4 (270) 44.9 (198)Severe 6.6 (30) 6.4 (29) 37.6 (166)Total 100 (450) 100 (447) 100 (441)
1318 Spine • Volume 30 • Number 11 • 2005
advised some restriction of physical activities, for Pa-tients 1, 2, and 3, respectively. Again, there were nostatistical differences between those therapists seeing pa-tients with acute LBP more often (at least one case aweek) or less often (less than one case a week), with70.3% and 73.4%, respectively, advising Patient 1 to“work.”
Chronicity Rating and Work RecommendationThe therapists’ assessments of each patient’s chronicityrisk were not consistently associated with their workrecommendations. There was no significant associationbetween the reported chronicity risk and work recom-mendation for Patient 1 (!2 ! 1.7, P ! 0.421). However,there was a significant association between these vari-ables for Patient 2 with those rating this patient as at“high risk” of chronicity being more likely to recom-mend the patient to “not work” (!2 ! 21.8, P " 0.001).It should be noted that the numbers in the high-riskcrosstabulation cell were small. !2 tests were not possiblefor Patient 3 because of a low cell count in some cells ofthe cross-tabulation.
Perceived Spinal Pathology and Work RecommendationThe perceived severity of each patient’s spinal pathologyappeared to be associated with the therapists’ work rec-ommendations. There were significant associations be-tween work recommendation and perceived level of spi-nal pathology for all 3 patients (!2 ! 13.2, P ! 0.001;!2 ! 20.6, P " 0.001; !2 ! 45, P " 0.001, respectively),with the recommendation to “not work” being morelikely when pathology was perceived by the therapist tobe more severe.
Practice Setting and Work RecommendationRespondents working in the National Health Service(NHS) were more likely to report advising all 3 patients“to work” than those working in non-NHS settings, al-though this did not reach a statistically significant levelfor Patient 2 (Patient 1, !2 ! 11.1, P ! 0.001; Patient 3,!2 ! 18.9, P " 0.001).
Discussion
This survey is the first nationwide survey in the UnitedKingdom to explore whether physical therapists workingin the musculoskeletal field have adopted a biopsychoso-cial approach to the management of LBP. The responsesto questions about work and activity levels, and per-ceived severity of spinal pathology provide insights intothe therapists’ ability to recognize patients who are atrisk of chronicity and their recommendations for workand activity.
Clinical vignettes were used as this allows data to begathered about a specific situation from a large samplewhen obtaining this information in real life is impracti-cal. The advantages of using vignettes include the abilityto control and manipulate variables easily, the sugges-tion of reduced Hawthorne effects,37 reduced social de-sirability and observer bias,37,38 and the way in whichresponses are not hindered by problems of recall.29 Dis-advantages are that vignettes tend to elicit attitudes andopinions rather than measuring actual behavior in real sit-uations.29,39,40 Use of a simple random sample, a large sam-ple size, basing the vignettes on actual patients with aknown psychosocial risk and expert testing, were all in-cluded to enhance the external validity of the results. Vi-gnettes have previously been used successfully to exploreclinical decision-making in survey research with physicians,chiropractors, and physical therapists.32,41–44
Experience and Postgraduate Education ofRespondents
As expected, the therapists were very experienced interms of the number of years in clinical practice, withonly 30% of the therapists having been qualified for lessthan 10 years. In the current study, 55% of therapistswere seeing at least one patient with acute LBP a week,which may reflect the waiting lists for therapy that arecommon in the U.K. healthcare system. Despite thelengthy practice time of the therapists, 51.8% had notcompleted any postgraduate training where their knowl-
Figure 1. Summary of work rec-ommendations for the three pa-tient vignettes. Patient one, mod-erate risk; Patient two, low risk;Patient three, high risk.
1319Physical Therapists in UK • Bishop and Foster

13
Identificación de “banderas” (factores)Clínicas:
Psicosociales:
Patología grave Patología Mental
Factores Psicológicos (negativos)
Kendall, N., Linton, S.J., and Main, C.J. 1997 Guide to assessing psychosocial yellow flags in acute low back pain: Risk factors for long term disability and work loss. Accident rehabilitation and Compensation Insurance of New Zealand and the National Health Committee, Wellington, New Zealand
Factores Laborales
Factores Sociales y Políticos
Factores Psicológicos (positivos)

• Catastrofismo
• Experiencias dolorosas insoportables, dolor extremo desproporcionado
• Creencias desadaptativas sobre el dolor
• Preocupación excesiva por la salud, exceso de ansiedad, angustia y bajo estado de ánimo
• El miedo a una nueva lesión (kinesiofobia)
• La incertidumbre acerca de lo que pasará en el futuro
• Contar con otras personas para resolver los problemas (ser pasivo en el proceso)
• Visitas a varios profesionales sin mejoría.
• …
Factores Psicológicos (negativos)
14

15
REVIEW
Identification of prognostic factors for chronicity in patientswith low back pain: a review of screening instruments
M. Melloh & A. Elfering & C. Egli Presland & C. Roeder &
T. Barz & C. Rolli Salathé & O. Tamcan & U. Mueller &
J. C. Theis
Received: 15 September 2008 /Revised: 17 October 2008 /Accepted: 31 October 2008 / Published online: 8 January 2009# Springer-Verlag 2008
Abstract Low back pain (LBP) is currently the mostprevalent and costly musculoskeletal problem in modernsocieties. Screening instruments for the identification ofprognostic factors in LBP may help to identify patients withan unfavourable outcome. In this systematic reviewscreening instruments published between 1970 and 2007were identified by a literature search. Nine differentinstruments were analysed and their different items groupedinto ten structures. Finally, the predictive effectiveness ofthese structures was examined for the dependent variablesincluding “work status“, “functional limitation”, and“pain“. The strongest predictors for “work status” werepsychosocial and occupational structures, whereas for“functional limitation” and “pain” psychological structures
were dominating. Psychological and occupational factorsshow a high reliability for the prognosis of patients withLBP. Screening instruments for the identification ofprognostic factors in patients with LBP should includethese factors as a minimum core set.
Résumé La lombalgie (LBP) est un problème importantnotamment sur le poste des dépenses dans nos sociétésmodernes. Sur le plan évolutif, il est primordial de pouvoirdépister des facteurs pronostics négatifs de ces patients. entre1970 et 2007, un certain nombre d’éléments permettant cetteanalyse ont été identifiés dans la littérature. Ces instrumentsd’analyse nous semblent importants de façon à déterminer lalimitation fonctionnelle, les possibilités de travail et la douleur.
International Orthopaedics (SICOT) (2009) 33:301–313DOI 10.1007/s00264-008-0707-8
M. Melloh : J. C. TheisDepartment of Medical and Surgical Sciences,Section of Orthopaedic Surgery, Dunedin School of Medicine,University of Otago,Private Bag 1921,Dunedin 9001, New Zealand
M. Mellohe-mail: [email protected]
J. C. Theise-mail: [email protected]
A. Elfering :C. Egli Presland (*) : C. Rolli SalathéDepartment of Work and Organizational Psychology,Institute of Psychology, University of Berne,Uni-Tobler, Muesmattstrasse 45,3000 Berne 9, Switzerlande-mail: [email protected]
A. Elferinge-mail: [email protected]
C. Rolli Salathée-mail: [email protected]
C. Roeder :O. Tamcan :U. MuellerDepartment of Evaluative Clinical Research,Institute for Evaluative Research in Orthopaedic Surgery,MEM Research Center, University of Berne,Stauffacherstrasse 78,3014 Berne, Switzerland
C. Roedere-mail: [email protected]
O. Tamcane-mail: [email protected]
U. Muellere-mail: [email protected]
T. BarzDepartment of Orthopaedic Surgery,Asklepios Klinikum Uckermark,Auguststrasse 23,16303 Schwedt/Oder, Germanye-mail: [email protected]
1.Acute Low Back Pain Screening Questionnaire (ALBPSQ)
2.Vermont Disability Prediction Questionnaire (VDPQ)
3.Örebro Musculoskeletal Pain Questionnaire (ÖMPSQ)
4.Screening Questionnaire for Predicting Outcome in Acute and Subacute Back Pain
5.HFK-R 10
6.Fear-Avoidance Beliefs Questionnaire (FABQ)
7.LBP Patient Perception Scale (PPS)
8. INTERMED Questionnaire
9.Chronic Pain Coping Inventory (CPCI)

15
REVIEW
Identification of prognostic factors for chronicity in patientswith low back pain: a review of screening instruments
M. Melloh & A. Elfering & C. Egli Presland & C. Roeder &
T. Barz & C. Rolli Salathé & O. Tamcan & U. Mueller &
J. C. Theis
Received: 15 September 2008 /Revised: 17 October 2008 /Accepted: 31 October 2008 / Published online: 8 January 2009# Springer-Verlag 2008
Abstract Low back pain (LBP) is currently the mostprevalent and costly musculoskeletal problem in modernsocieties. Screening instruments for the identification ofprognostic factors in LBP may help to identify patients withan unfavourable outcome. In this systematic reviewscreening instruments published between 1970 and 2007were identified by a literature search. Nine differentinstruments were analysed and their different items groupedinto ten structures. Finally, the predictive effectiveness ofthese structures was examined for the dependent variablesincluding “work status“, “functional limitation”, and“pain“. The strongest predictors for “work status” werepsychosocial and occupational structures, whereas for“functional limitation” and “pain” psychological structures
were dominating. Psychological and occupational factorsshow a high reliability for the prognosis of patients withLBP. Screening instruments for the identification ofprognostic factors in patients with LBP should includethese factors as a minimum core set.
Résumé La lombalgie (LBP) est un problème importantnotamment sur le poste des dépenses dans nos sociétésmodernes. Sur le plan évolutif, il est primordial de pouvoirdépister des facteurs pronostics négatifs de ces patients. entre1970 et 2007, un certain nombre d’éléments permettant cetteanalyse ont été identifiés dans la littérature. Ces instrumentsd’analyse nous semblent importants de façon à déterminer lalimitation fonctionnelle, les possibilités de travail et la douleur.
International Orthopaedics (SICOT) (2009) 33:301–313DOI 10.1007/s00264-008-0707-8
M. Melloh : J. C. TheisDepartment of Medical and Surgical Sciences,Section of Orthopaedic Surgery, Dunedin School of Medicine,University of Otago,Private Bag 1921,Dunedin 9001, New Zealand
M. Mellohe-mail: [email protected]
J. C. Theise-mail: [email protected]
A. Elfering :C. Egli Presland (*) : C. Rolli SalathéDepartment of Work and Organizational Psychology,Institute of Psychology, University of Berne,Uni-Tobler, Muesmattstrasse 45,3000 Berne 9, Switzerlande-mail: [email protected]
A. Elferinge-mail: [email protected]
C. Rolli Salathée-mail: [email protected]
C. Roeder :O. Tamcan :U. MuellerDepartment of Evaluative Clinical Research,Institute for Evaluative Research in Orthopaedic Surgery,MEM Research Center, University of Berne,Stauffacherstrasse 78,3014 Berne, Switzerland
C. Roedere-mail: [email protected]
O. Tamcane-mail: [email protected]
U. Muellere-mail: [email protected]
T. BarzDepartment of Orthopaedic Surgery,Asklepios Klinikum Uckermark,Auguststrasse 23,16303 Schwedt/Oder, Germanye-mail: [email protected]
1.Acute Low Back Pain Screening Questionnaire (ALBPSQ)
2.Vermont Disability Prediction Questionnaire (VDPQ)
3.Örebro Musculoskeletal Pain Questionnaire (ÖMPSQ)
4.Screening Questionnaire for Predicting Outcome in Acute and Subacute Back Pain
5.HFK-R 10
6.Fear-Avoidance Beliefs Questionnaire (FABQ)
7.LBP Patient Perception Scale (PPS)
8. INTERMED Questionnaire
9.Chronic Pain Coping Inventory (CPCI)

16
RESEARCH Open Access
Spanish version of the screening ÖrebroMusculoskeletal Pain Questionnaire: across-cultural adaptation and validationAntonio Ignacio Cuesta-Vargas1,2* and Manuel González-Sánchez1
Abstract
Background: Spanish is one of the five most spoken languages in the world. There is currently no publishedSpanish version of the Örebro Musculoskeletal Pain Questionnaire (OMPQ). The aim of the present study is todescribe the process of translating the OMPQ into Spanish and to perform an analysis of reliability, internalstructure, internal consistency and concurrent criterion-related validity.
Methods: Design: Translation and psychometric testing. Procedure: Two independent translators translated theOMPQ into Spanish. From both translations a consensus version was achieved. A backward translation was made toverify and resolve any semantic or conceptual problems. A total of 104 patients (67 men/37 women) with a meanage of 53.48 (±11.63), suffering from chronic musculoskeletal disorders, twice completed a Spanish version of theOMPQ. Statistical analysis was performed to evaluate the reliability, the internal structure, internal consistency andconcurrent criterion-related validity with reference to the gold standard questionnaire SF-12v2.
Results: All variables except “Coping” showed a rate above 0.85 on reliability. The internal structure calculationthrough exploratory factor analysis indicated that 75.2% of the variance can be explained with six components withan eigenvalue higher than 1 and 52.1% with only three components higher than 10% of variance explained. In theconcurrent criterion-related validity, several significant correlations were seen close to 0.6, exceeding that value inthe correlation between general health and total value of the OMPQ.
Conclusions: The Spanish version of the screening questionnaire OMPQ can be used to identify Spanish patientswith musculoskeletal pain at risk of developing a chronic disability.
Keywords: Musculoskeletal pain, Reliability, Validity, Outcome, Factor analysis, Clinimetric, Measurement
BackgroundChronic musculoskeletal conditions have a negative impact,affecting the well-being, independence and physical andpsychological health of those who suffer [1]. The incidenceof such diseases is very high, with an estimated overallprevalence in the general adult population of a personsuffering a low back pain (LBP) episode in his/her lifetimeranging between 60% and 85% [2], with a high impact onsocio-economic cost [1,3].
Clinical practice guidelines in primary care basedon musculoskeletal evidence show the importance ofidentifying indicators of poor outcomes need to beconsidered when achieving the rehabilitative process[4]. Several studies have been published showing theinteraction between the patient’s psychosocial statusand the probability increase for a musculoskeletal problembecoming chronic [5]. These psychological factors havebeen shown as good predictors of long-term disabilities[6], developing a correlation in which the experience ofpain is associated with disability. Biomedical professionalsspend a considerable amount of time with their patientsand are aware of the importance that psychosocial factorshave. Nevertheless, the ways to face these factors are
* Correspondence: [email protected] de psiquiatría y fisioterapia, Instituto de InvestigaciónBiomédico de Málaga (IBIMA), Universidad de Málaga, C/ ArquitectoFrancisco Peñalosa, Ampliación Campus Teatinos, 29071 Malaga, Spain2School of Clinical Sciences, Faculty of Health at the Queensland Universityof Technology, Queensland, Australia
© 2014 Cuesta-Vargas and González-Sánchez; licensee BioMed Central Ltd. This is an Open Access article distributed under theterms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricteduse, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative CommonsPublic Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available inthis article, unless otherwise stated.
Cuesta-Vargas and González-Sánchez Health and Quality of Life Outcomes 2014, 12:157http://www.hqlo.com/content/12/1/157
http://goo.gl/nKrvj6
25 (21) ítems
0 - 210 puntos
6 Dimensiones:• “Pain” • “Distress” • “Work Return Expectancy”
• “General Health” • “Social Functioning” • “Physical Function”
• “Coping”,• “Function”• ”Fear Avoidance”

17
• La Educación Para la Salud es eficaz en el manejo de factores psicosociales
• Es importante realizar una evaluación sistemática de los mismos
• Hay que tenerlos en cuenta antes, durante y después del tratamiento
Conclusiones

Muchas Gracias
@_RaulFerrer