advantages of minimally invasive decompression traditionally the treatment of choice for lumbar...
TRANSCRIPT

Advantages of Minimally Invasive Decompression
Through Laminotomy and Foraminotomy
Introduction
Traditionally, lumbar stenosis is treated with an open decompressive laminectomy with or without facetectomies. This has been a successful treatment for improvement of clinical symptoms but may unintentionally lead to cases of iatrogenic spinal instability, which may result in follow on surgical intervention for stabilization [1]. Radiographic and cadaver studies have shown that open decompressive laminectomies are effective for lumbar stenosis but may also disrupt the normal anatomical structures of the spine (supraspinous ligament, interspinous ligament, spinous process, lamina, facet joints, ligamentum flavum and paraspinal musculature) leading to muscular atrophy [2] and potential long-term spinal instability [3]. Subsequently, minimally invasive spine surgery (MISS) was developed to focally address the diseased structures but minimize disruption of the surrounding normal anatomic structures.
Surgical decompression of lumbar stenosis is one of the most common MISS surgeries. Prospective randomized clinical trials have shown significantly greater improvements in functional outcome and quality of life metrics with surgical intervention compared to conservative medical management. Recent studies have shown similar patient outcomes with MISS approaches for lumbar decompression when these techniques are compared to the traditional open approach. Decreased blood loss, shorter operative time, shorter hospital duration, decreased postoperative narcotic requirement, decreased rate of infection and CSF leak and a decrease in time required for return to work [4,5] have been shown to be additional benefits of MISS approaches. While the open laminectomy has been traditionally the treatment of choice for lumbar stenosis, the MISS approaches have evolved into the modern surgical solution.
The objective of this white paper is to retrospectively examine prospective surgical outcomes, return to work and self-reported pain outcomes preoperatively and 12 months postoperatively among 500 patients who underwent an outpatient MISS laminotomy foraminotomy decompression (LFD) for the treatment of LSS.
Methods
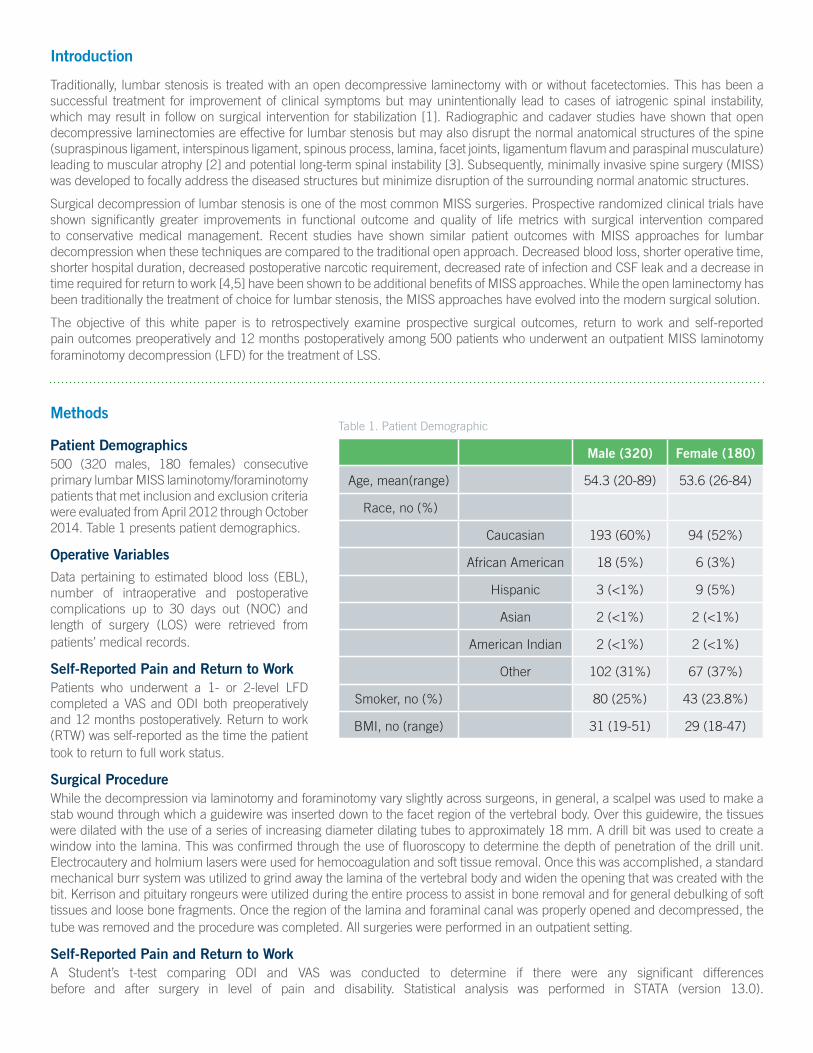
Patient Demographics500 (320 males, 180 females) consecutive primary lumbar MISS laminotomy/foraminotomy patients that met inclusion and exclusion criteria were evaluated from April 2012 through October 2014. Table 1 presents patient demographics.
Operative VariablesData pertaining to estimated blood loss (EBL), number of intraoperative and postoperative complications up to 30 days out (NOC) and length of surgery (LOS) were retrieved from patients’ medical records.
Self-Reported Pain and Return to WorkPatients who underwent a 1- or 2-level LFD completed a VAS and ODI both preoperatively and 12 months postoperatively. Return to work (RTW) was self-reported as the time the patient took to return to full work status.
Surgical ProcedureWhile the decompression via laminotomy and foraminotomy vary slightly across surgeons, in general, a scalpel was used to make a stab wound through which a guidewire was inserted down to the facet region of the vertebral body. Over this guidewire, the tissues were dilated with the use of a series of increasing diameter dilating tubes to approximately 18 mm. A drill bit was used to create a window into the lamina. This was confirmed through the use of fluoroscopy to determine the depth of penetration of the drill unit. Electrocautery and holmium lasers were used for hemocoagulation and soft tissue removal. Once this was accomplished, a standard mechanical burr system was utilized to grind away the lamina of the vertebral body and widen the opening that was created with the bit. Kerrison and pituitary rongeurs were utilized during the entire process to assist in bone removal and for general debulking of soft tissues and loose bone fragments. Once the region of the lamina and foraminal canal was properly opened and decompressed, the tube was removed and the procedure was completed. All surgeries were performed in an outpatient setting.
Self-Reported Pain and Return to WorkA Student’s t-test comparing ODI and VAS was conducted to determine if there were any significant differences before and after surgery in level of pain and disability. Statistical analysis was performed in STATA (version 13.0).
Table 1. Patient Demographic
Male (320) Female (180)
Age, mean(range) 54.3 (20-89) 53.6 (26-84)
Race, no (%)
Caucasian 193 (60%) 94 (52%)
African American 18 (5%) 6 (3%)
Hispanic 3 (<1%) 9 (5%)
Asian 2 (<1%) 2 (<1%)
American Indian 2 (<1%) 2 (<1%)
Other 102 (31%) 67 (37%)
Smoker, no (%) 80 (25%) 43 (23.8%)
BMI, no (range) 31 (19-51) 29 (18-47)

Results
A significant decrease in VAS (p < 0.001) and ODI scores (p < 0.001) between preoperative and postoperative was observed (Table 2). The average EBL was 48.48 mL and the LOS averaged at 61.17 min. There were no reported intraoperative or postoperative NOC. The average length of time to return to work for patients studied was 1.39 months from the time of their surgery (Table 3). Descriptive statistics for the outcome measures are reported in Table 2 and Table 3.
Table 2. Self-Reported Pain Outcomes
VAS ODI
Preop Postop A Preop Postop A
All 6.2 3.3 2.9** 27.4 11.4 16**
Male 6.3 3.2 3.1** 28.4 10.7 17.7***
Female 6.1 3.4 2.7** 26.8 11.9 14.9**
Table 3. Operative Variables
RTW (mths) EBL (ml) LOS (min)
All 1.39 48.48 61.17
Male 1.35 47.76 60.11
Female 1.44 49.21 62.23
Conclusion
Results indicate that MISS for the treatment of LSS is associated with short operative times, low complication rates, reduced return to work times and minimal average EBL. Results also indicate that patients who underwent MIS also reported less pain and disability postoperatively than preoperatively. These findings support the current literature that MIS using endoscopy may be both a safe and effective treatment for LSS. Table 4 presents a meta-analysis of existing studies who have investigated similar variables for MISS procedures with operative and patient outcomes. The current analysis reports quantitatively and statistically similar results in all variables investigated.
Table 4. Meta-Analysis of Patient and Operative Outcomes in MISS Procedures
Study Patients Age Functional Outcome Scores Follow-Up EBL LOS
Khoo, 2002 25 68 No functional outcomes 12 68 109
Ikuta, 2003 47 66 VAS ^70.6% 22 68 124
Ikuta, 2003 30 69 No functional outcomes 16 44 98
Rahman, 2003 126 68 No functional outcomes NR 50 108
Castro, 2005 50 56 VAS ^6.02, ODI ^30.23 48 NR 94.3
Ikuta, 2005 114 67 VAS ^38% 28 NR NR
Rosen, 2005 57 80 VAS ^2.4, ODI ^21 10 NR NR
Ikuta, 2006 37 69 VAS ^43% 38 NR NR
Asgarzadie, 2007 48 64 ODI ^20 48 26 55
Pao, 2007 53 62 ODI ^47.6 15 104.5 126.7
Current analysis 500 53 VAS ^2.7 (^44%) ODI ^14.9 (^56%) 3 - 36 months 48.48 61.17
Minimally invasive surgery is an important means of reducing tissue trauma and patient morbidity. This may prove to be essential in improving pain and reducing postoperative stress responses and delayed sequelae that can lead to unfortunate complications after otherwise uneventful procedures. MISS laminotomy and foraminotomy can be used to decompress the spinal canal as effectively as an open laminotomy and may prove to be beneficial in decreasing the complications and morbidity of standard treatments for lumbar stenosis. Although any patient can experience a variety of complications from surgery, our analysis provides evidence that MISS procedures result in fewer complications and improved patient outcomes regardless of patient demographics. Additionally, this analysis demonstrates that the MISS procedures produce sufficient decompression that reduces levels of pain and disability with no complications and minimal blood loss.
(^represents a reduction in the function outcome score)
**=p<0.05, ***=p<0.001

4948-020817-AM© 2017 Laser Spine Institute, LLC
References
[1] Bassewitz H, Herkowitz H. Lumbar Stenosis with Spondylolisthesis: Current Concepts of Surgical Treatment. Clinical Orthopaedics and Related Research. 2001;384:54-60.
[2] Yagi M, Okada E, Ninomiya K, Kihara M. Postoperative Outcome After Modified Unilateral-Approach Microendoscopic Midline Decompression for Degenerative Spinal Stenosis. Journal of Neurosurgery: Spine. 2009;10(4):293-299.
[3] Bresnahan L, Ogden AT, Natarajan RN, Fessler RG. A Biomechanical Evaluation of Graded Posterior Element Removal for Treatment of Lumbar Stenosis: Comparison of a Minimally Invasive Approach with Two Standard Laminectomy Techniques. Spine. 2009;34(1):17-23.
[4] O’Toole JE, Eichholz KM, Fessler RG. Surgical Site iInfection Rates After Minimally Invasive Spinal Surgery. Journal of Neurosurgery: Spine. 2009;11(4):471-476.
[5] Lawton C, Smith ZA, Barnawi A, Fessler RG. The Surgical Technique of Minimally Invasive Transforaminal Lumbar Interbody Fusion. Journal of Neurosurgical Sciences. 2011;55(3):259-264.