allograft replacement for infrarenal aortic graft infection
TRANSCRIPT
14° CONGRESS OF ASIAN SOCIETY FOR VASCULAR SURGERY
DANIELE MASOTTIDIVISION OF VASCULAR SURGERY
TREVISO HOSPITAL ITALY

Alexis Carrel reported the use of allograft in animal experiments
Robert Gross was the first to treat aortic coartationon by human arterial allograft
Charles Dubost replaced the infrarenal aorta with a fresh aortic allograft
A BRIEF HISTORY
ABDOMINAL AORTIC GRAFT INFECTION
Abdominal aortic graft infection is rare Operative mortality in patients with infected
aortic aneurysms remains high Abdominal aortic graft infection remains a
major surgical challenge
CLASSIFICATION
By time of apparence Early: < 4 months Late: > 4 months
By extent to post-operative wound infection Grade I: cellulitis involving the wound Grade II: infection involving sottocutaneus tissue Grade III: infection involving the vascular prosthesis
Bandyk
Szilagyi
CLINICAL MANIFESTATIONS
Leukocytosis and an elevated erythrocyte sedimentation rate (in 70% of the cases)
Weight loss The onset is insidiousus, and a low grade of
fever may be present for several months bifore diagnosis
Fever is present in over 70% of the patients
CLINICAL MANIFESTATIONS
Salmonella and gram negative infections have a greater tendency a early rupture and death
Overall mortality from abdominal aortic graft infection is over 50% despite advances in therapy
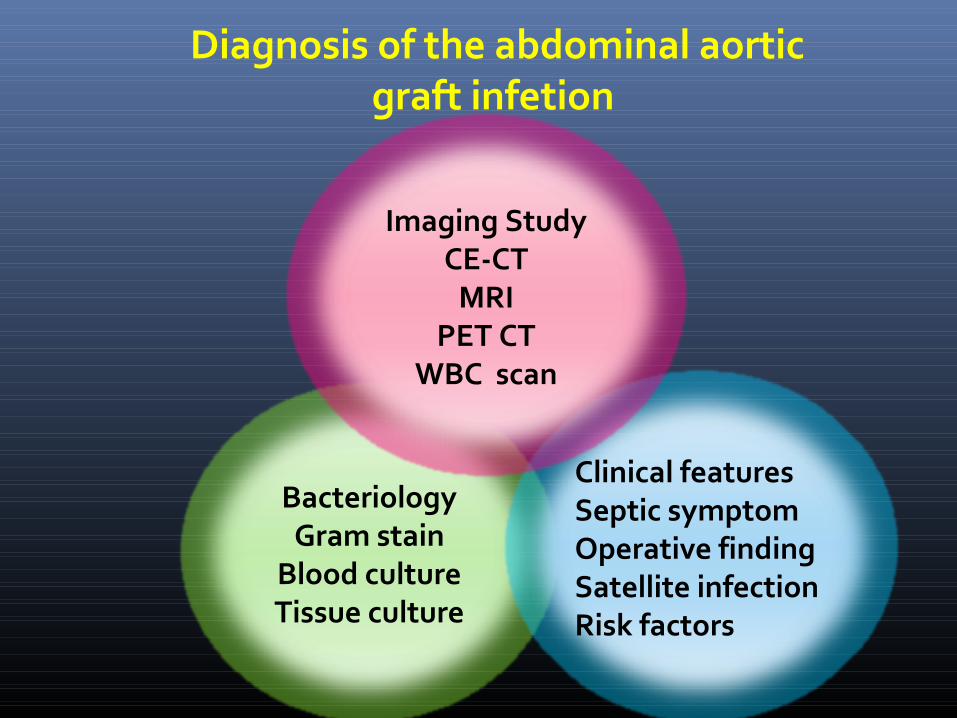
Diagnosis of the abdominal aortic graft infetion
BacteriologyGram stain
Blood cultureTissue culture
Clinical featuresSeptic symptomOperative findingSatellite infectionRisk factors
Imaging StudyCE-CT
MRIPET CT
WBC scan
DIAGNOSIS
Blood culture are helpful in suggesting the diagnosis and identifyng the pathogen (though 25% negative)
Abdominal ultrasnonography CT scan is generally performed preopertively
to assist in surgical planning
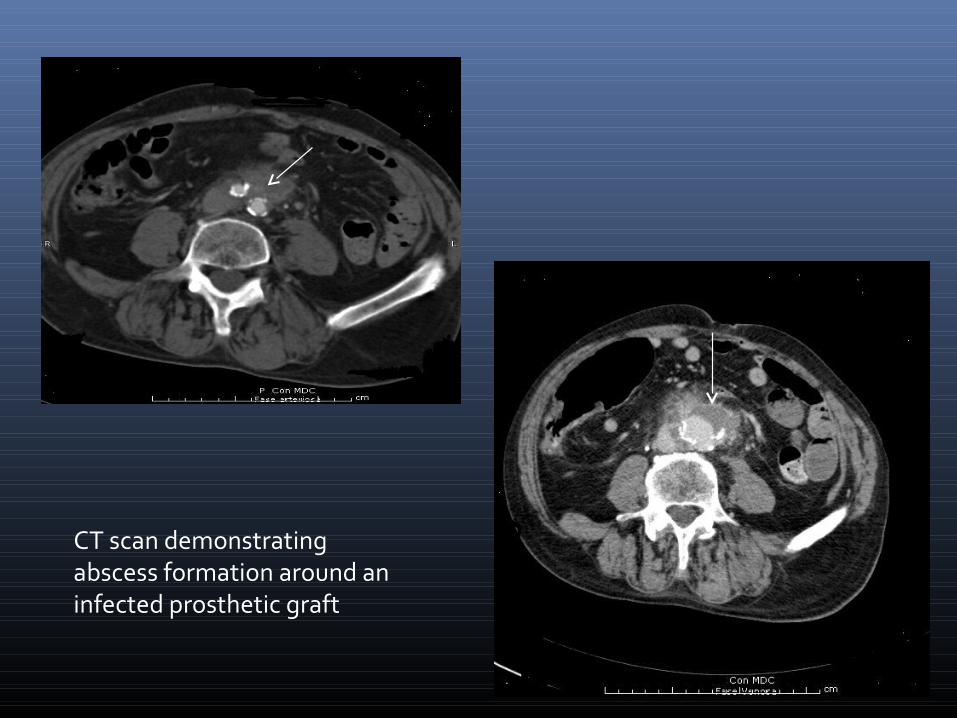
CT scan demonstrating abscess formation around an infected prosthetic graft

MANAGEMENT
Abdominal aortic gaft infection is treated with intravenous antibiotics and surgical exicision
Antibiotic therapy must be continued post-operatively for at least 6 weeks

MANAGEMENT
The standard surgical approach involves:
Resection of infected aortic aneurysm and infected retroperitoneal tissueOwersewing of the native aorta as stumpsRestoration of distal perfusion
ALLOGRAFT
The aim of this prospective , observational study was the evaluate the safety and efficacy of cryopreserved arterial allograft reconstruction in the treatment of abdominal aortic infection

ALLOGRAFT
Cryopreserved in liquid nitrogen
Expensive
Delay
ALLOGRAFT
Technical points
Unfreeze and rinse just before implantation
Ligature of side branches
Coverage of the graft
6 weeks of antibiotics
STUDY DESIGN IN PATIENTS WITH ABDOMINAL AORTIC GRAFT INFECTION
STUDY DESIGN 19 patients with abdominal aortic graft
infection presenting to our institution over a recent 8-years period were studied
INITIAL SURGERY
All patients were referred from other hospitals.
8 aortobifemoral bypasses 4 aorto-aortic grafts4 aortobiliac bypasses2 aortofemoral bypasses1 endoprosthesis
RESULTS
19 patient with infected aortic graft were treated with surgery with cryopreserved allograft
(November 1999-February 2007)
90% were febrile, 90% had leukocytosis and 30% were emodinamically unstable
The most common responsible pathogens were Staphylococcus aureus (31%)
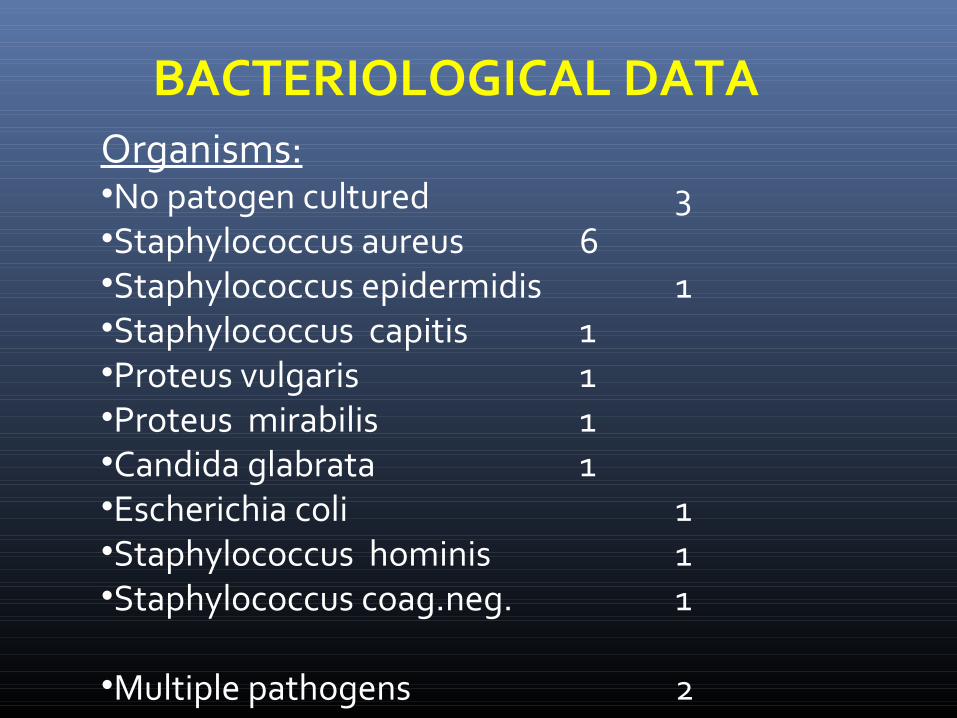
BACTERIOLOGICAL DATAOrganisms:•No patogen cultured 3•Staphylococcus aureus 6•Staphylococcus epidermidis 1•Staphylococcus capitis 1•Proteus vulgaris 1•Proteus mirabilis 1•Candida glabrata 1•Escherichia coli 1•Staphylococcus hominis 1•Staphylococcus coag.neg. 1
•Multiple pathogens 2

INDICATION FOR CRYOPRESERVED AORTIC
ALLOGRAFT
→ 15 were patients for primary graft infection
(78,9%)
→ 1 patient for mycotic aneurism (5,3%)
→ 2 patients for aortoenteric fistulas (10,5%)
→ 1 patient for endoprostesis infection (5,3%)
RESULTS
Early postoperative mortality was 36,8% (7 patients) including 3 (15,79%) allograft related deaths from rupture of the allograft
Four deaths were not allograft related There were six (31,58%) non lethal allograft
complication (rupture n = 2, thromboses, which were successfully treated at repeat operation, n = 4
Amputation n = 1 One patient need dialitic treatment Four patients (21,05%) were lost to follow-up Mean follow-up was 24 months Late mortality was 10,53% (2 patients)
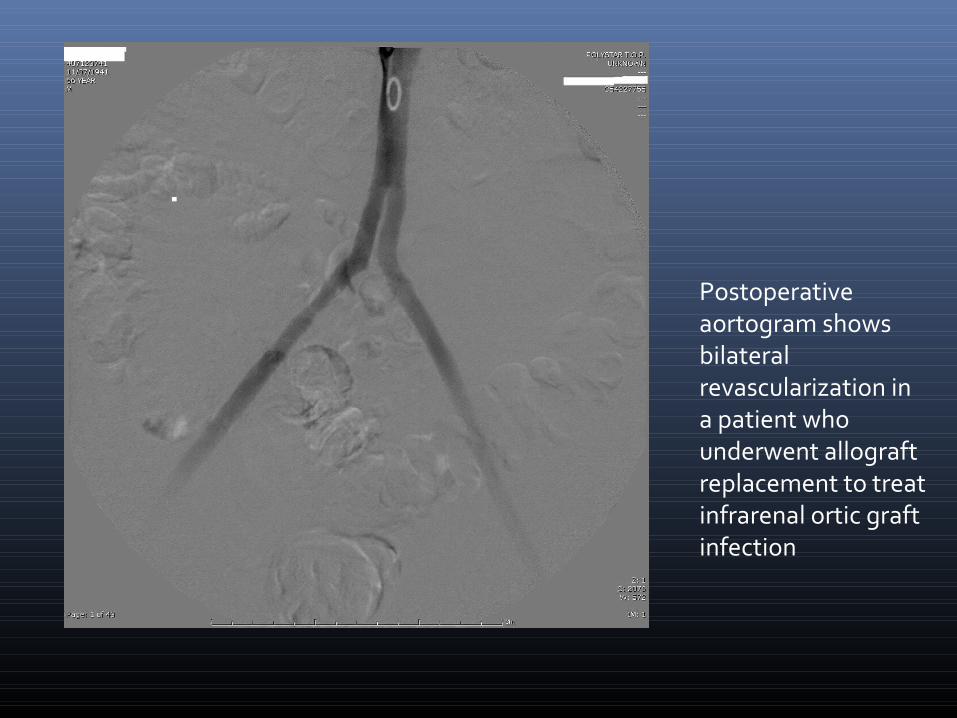
Postoperative aortogram shows bilateral revascularization in a patient who underwent allograft replacement to treat infrarenal ortic graft infection

AORTOENTERIC FISTULA
Direct communication between the aorta and the GI tract.
Aortoenteric Fistula (AEF) is a rare, lifethreatening disease process.
Most commonly a complication of repair of abdominal aortic aneurysms.
Occurs in approximately 0.3-2% of patients with open AAA repairs.

PROGNOSIS
Prognosis is poor Mortality rate of 100% if no surgical
intervention done. Mortality rate between 60-90% with surgical
intervention
CONCLUSION
Our experience with cryopreserved arterial allograft in the management of abdominal aortic infection suggests that this tecnique seems to be a useful option for treating one of the most dreaded vascular complications