amh ovarian reservemarker dr jyoti bhasker ,dr. sharda jain dr. jyoti agarwal ,
TRANSCRIPT

1
AMH
OVARIAN RESERVEMARKER
DR. JYOTI BHASKARDR. SHARDA JAIN
DR. JYOTI AGARWAL
2
AGE WISE INFERTILITY
20-25 2.8% infertile
30-34 10% infertile
35-39 33% infertile
40-45 86% infertile
3
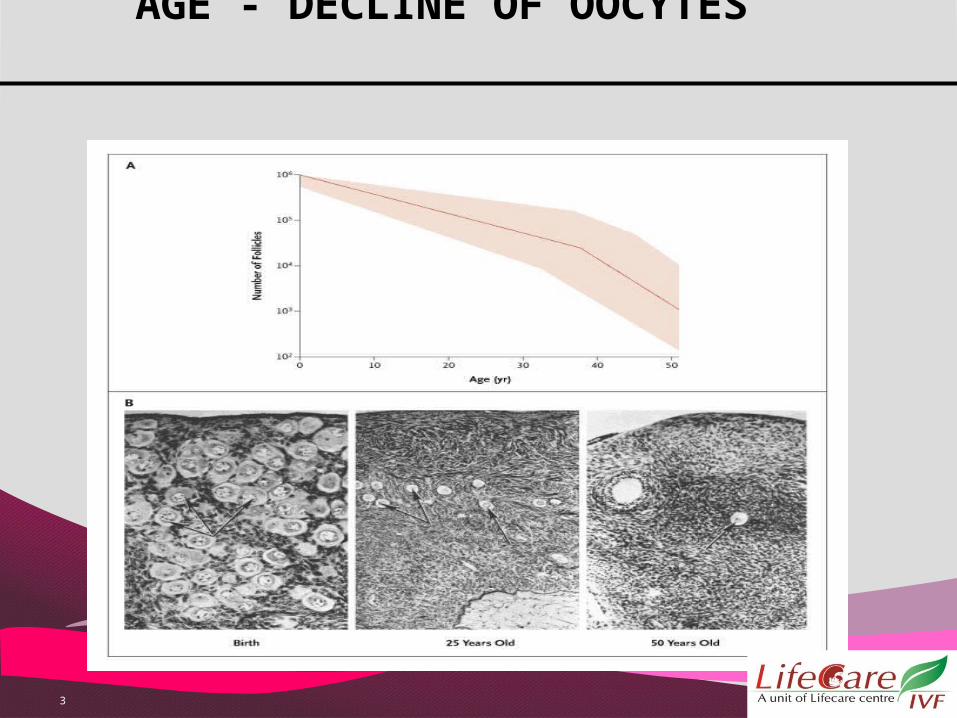
AGE - DECLINE OF OOCYTES

4
MISCARRIAGE RATE
Age 30: 7-15%
Age 31-34: 17-21%
Age 35-39: 17-28%
Age 40: 40-52%
5
ANEUPLOIDY
10% of eggs are aneuploidic in young women
30% at the age of 40
50 % at the age of 43
Nearly all the eggs are aneuploidic at the age of 45
6(teVelde and Pearson 2002)
OVARIAN RESERVE
Age is an important independent determinant of fertitlity and miscarriage
But due to considerable individual variation in the age of menopause and age of subfertility.
Chronological age ALONE is a POOR indicator of reproductive aging, and thus of the ovarian reserve.

7
OFFER -- OVARIAN RESERVE TEST Infertile womenInfertile women
Over 30 years of ageOver 30 years of agewith a history of with a history of exposure to a confirmed exposure to a confirmed
gonadotoxin gonadotoxin i.e., tobacco smoke, i.e., tobacco smoke, chemotherapy, radiation therapy.chemotherapy, radiation therapy.with a strong family history of early with a strong family history of early menopause ormenopause or
premature ovarian failure.premature ovarian failure.women who have had extensive ovarian women who have had extensive ovarian surgery, i.e., cystectomy and unilateral surgery, i.e., cystectomy and unilateral oophorectomyoophorectomy
8
BENEFITS OF ORT IN SUBFERTILE COUPLE
ORT guides in prognosticating ORT guides in prognosticating outcome inoutcome in
individual cases byindividual cases by
Pre-treatment counsellingPre-treatment counsellingChoice of infertility treatmentChoice of infertility treatmentAvoidance of ovarian Avoidance of ovarian hyperstimulationhyperstimulation

9
Ovarian ReserveOvarian Reserve

10
TESTING FOR OVARIAN RESERVE
Hormone analysis
Ultrasound techniques
Dynamic testing

11
HORMONE ANALYSISFollicle Stimulating Hormone (FSH)
Oestradiol
Progesterone
Inhibin B

12
FOLLICLE STIMULATING HORMONE
Usually measured Day 2 or 3 of cycle
Women with > 10 IU/l poor response to ART
Women aged more than 30 with one value
of FSH > 14 IU/l do worse on IVF
13
DISADVANTAGE
Variation from month to month
Lab wise variation in values due to
different techniques.
Spurious fall after hormone therapy.

14
SERUM OESTRADIOL
E2 alone of little value to asses ovarian
reserve
Combined E2 and FSH levels – better than E2 alone.
E2 of > 80 pg/ml day 3 pre IVF cycle- higher cancellation rate
15
PROGESTERONE
Doesn’t have any independent role in assessment of ovarian reserve
Early LH surge and elevation of P4 suggested sign of poor ovarian reserve
16
INHIBIN B
Hetero dimeric protein similar to AMH
Levels >45 pg/ml – poor response to induction
High false positive rate
Not widely used nowadays.
17
CLOMIPHENE CHALLENGE TESTBaseline FSH, LH & E2 followed by CC 100mg/day
from Days 5 to 9
Measure E2, FSH and LH on Day 9 to 11
Exaggerated FSH after CC bad prognostic sign
Along with other tests like FSH or GNRH agonist stimulation test no better inference than basal
values

18
ANTRAL FOLLICULAR COUNT
Count of total follicles measuring 2 to 5mm in both ovaries on Day 2/3 of periods.
Can be done in any day of the cycle
To be done by Trans Vaginal Ultrasound

19
ANTRAL FOLLICULAR COUNT
NORMAL AFC COUNT – 10-18
POOR RESPONDER - < 7
HYPERRESPONDER - > 20
20
DRAWBACKS OF AFCDRAWBACKS OF AFC
Accurate assessment of AFC requires an Accurate assessment of AFC requires an experienced sonographerexperienced sonographer and can be limited in and can be limited in patients who have had pelvic surgery or patients who have had pelvic surgery or
uterine uterine fibroids and in those who are obesefibroids and in those who are obese
Moderate interobserver and intercycle Moderate interobserver and intercycle variabilityvariability of of
AFC determinations limits its reproducibility. AFC determinations limits its reproducibility.

21
FACTORS AFFECTING AFCFACTORS AFFECTING AFC
Oral contraceptive use (decreases)Oral contraceptive use (decreases)
Polycystic ovary syndrome (PCOS) Polycystic ovary syndrome (PCOS) (increases).(increases).
22
AFC
So far, assessment of antral follicle count by
ultrasonography, best predicts the quantitative aspect of
ovarian reserve.
Most cost effective SINGLE predictor of
ovarian reserve -- IS AFC
(Scheffer, et al., 2003)

23
ANTI-MULLERIAN HORMONE

24
AMHAMH is a glycoprotein
Originally known as Mullerian Inhibiting Substance(MIS)
Appears in females at puberty
Produced by granulosa cells of pre-antral and small antral follicles of 4-6 mm
AMH is not expressed in atretic follicles and theca cells.

25

26
AMH is produced by the small growing (primary and AMH is produced by the small growing (primary and preantral) follicles in the postnatal ovary and has two preantral) follicles in the postnatal ovary and has two sites of action. It inhibits initial sites of action. It inhibits initial follicle recruitment (1) and inhibits FSH-dependent follicle recruitment (1) and inhibits FSH-dependent growth and selection of preantral and small antral growth and selection of preantral and small antral follicles (2).follicles (2).
Model of AMH action in the ovary.Model of AMH action in the ovary.

27
The intrafollicular concentrations of AMH in normal human antral follicles show a gradual reduction as the diameter of the follicle increases, and a sharp decline is observed around 8mm
Physiological function- prevent excessive follicle recruitment. Acts as a Gatekeeper
28
AMH - unaffected
Not cycle dependant-can be measured any day
Less cycle to cycle variation than FSH.Not altered after down regulation with
GNRH agonist.Pregnancy
AMH – factors that Increase Polycystic ovaries

29
AMH – factors that decrease
Increasing age Increasing age Race and EthinictyRace and Ethinicty Obesity Obesity Smoking, Alcohol IntakeSmoking, Alcohol Intake Administration of Gonadotropins Administration of Gonadotropins Administration of chemotherapy or Administration of chemotherapy or radiation radiation Surgical removal of one or both ovaries Surgical removal of one or both ovaries Contraceptive PillsContraceptive Pills
30
AMH BLOOD LEVEL
High (often PCOS) Over 3.5 ng/ml
Normal Over 1.4 ng/ml
Low Normal Range 0.7 – 1.3 ng/ml
Low 0.3 - 0.6 ng/ml
Very Low Less than 0.3 ng/ml
31
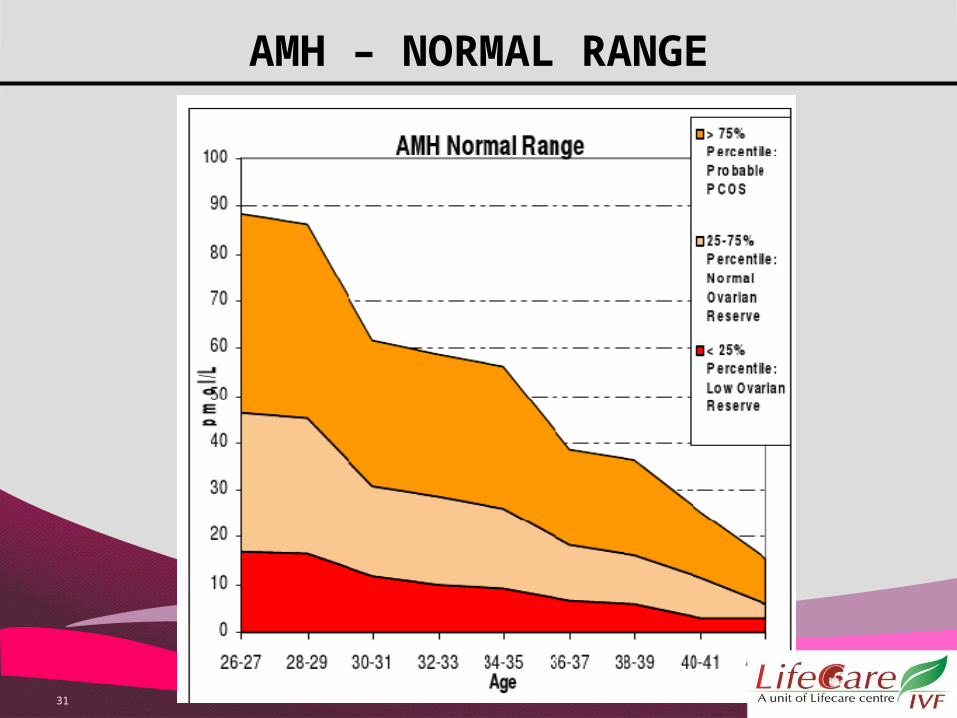
AMH – NORMAL RANGE
32
AMH BLOOD LEVEL
AMH of less than 1.36 ng/ml has a sensitivity of 75.5% and specificity of 74.8% in prediction of poor response.
AMH > 3.5 ng/ml has a sensitivity of 88% and
67% specificity in prediction of hyperstimulation
33
WE DO HAVE EXCEPTIONS IN REALITY !!!
42 YRS OLD LADY, WITH AMH OF 0.5 , SPONTANOUS CONCEPTION--- NOW 28 WEEKS. NO MISCARRIAGE, NO ANEUPLOIDY
THESE CUTOFFS ARE GUIDELINES WHICH HELP IN:1. COUNSELLING
2. SELECTING THE OPTIMAL PROTOCOL.DECISION HAS TO BE COLLECTIVE –
WOMAN’S CHOICE GETS THE PRIORITY

34
Understanding AMH measurement methods
AMH is measurable in serum
TWO METHODS AVAILABLE ARE Diagnostic system Lab ( DSL) (ng/ml) Immunotech Beckman Coulter ( IBL) assay.
( pmol/l)
NEW METHOD : AMH Generation II assay

35
AMH
Increasing age means a decreasing AMH level
Lower AMH levels at any given time irrespective of age predicts a poor
response to ART.
High AMH levels – candidates prone for OHSS.

36
ADVANTAGE OVER OTHER ORT MARKERS
It is the earliest marker to change with ageIt shows the least intercycle and intracycle
variabilityIt can be randomly measured during the cycleIt shows no modifications during GnRHaIt needs no modification in hypothalamic
amenorrheaIt is both more convenient and informative
than basal FSH

37
INDIVIDUALISED AMH TAILORED COH
Improves embryo transfer rates, the incidence of fertilization, pregnancy and live birth rates.
Reduces incidence of adverse outcomes,
such as OHSS and failed fertilization

38
PROPOSED AMH BASED PROTOCOLS
Low AMH (< 1.4 ng/ml) Cycle cancellation or poor response a. Inform the patient about the cycle
cancellation or no transfer b. Low possibility of pregnancy c. Avoid long suppression d. Antagonist cycle e. Use of HMG for stimulation Normal AMH (1.4-3.5 ) Normal
Response a. Standard protocol
39
PROPOSED AMH BASED PROTOCOLS
HIGH AMH (> 3.5 ng/ml) a. Inform about the risk of OHSSb. Avoid depot GnRHac. Low FSH dosed. Antagonist cycle preferrede. Agonist Triggerf. Blastocyst transfer or Freeze all
embryos and transfer later.
40
CONCLUSION Anti mullerian hormone (AMH) alone
or best in combination with antral follicular count (AFC)
is the BETTER INDICATOR
of ovarian reserve than any other hormonal or
sonographic markers available at present.

41

ADDRESS 11 Gagan Vihar, Near Karkari
Morh Flyover, Delhi - 51
CONTACT US 9650588339 (Helpline)
011-22414049,22058865 WEBSITE :
www.drshardajain.in
www.lifecarecenreivf.com E-MAIL ID
[email protected] [email protected]
ISO 14001:2004 (EMS) …..Caring hearts, healing
hands
ISO 9001:2008
ISO 9001:2008 www.globalstemgenn.com , Helpline: 9599044357
www.lifecarecentre.in
Helpline:9599044257