analysis in to the epidemiology and pathophysiology of respiratory syncytial virus - written - piril...
TRANSCRIPT

An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
1 Piril Erel – UoB 12004723
MPharm Year 3 SSA

Epidemiology of RSVRespiratory Syncytial Virus (RSV) places the heaviest clinical burden on paediatric wards in the UK and the US. It is in fact, a global issue with 3.4 million hospitalisations and approximately 66,000 deaths worldwide per annum (Bush et al., 2007) (Lambert et al., 2014). RSV is the leading cause, especially during the winter months, of severe respiratory infections in infants resulting in a rise in hospital admissions where 0.5-1% of infected babies die from respiratory failure. It is also a significant respiratory concern in the elderly population. (Agoti et al., 2014)
RSV predominantly spreads through airborne particles transmitted either by sneezing and coughing from infected individuals. It is highly contagious virus, and airborne particles remain on surfaces for an extended period of time (Lindsley et al., 2010). Infection takes place if the virus-containing droplets come in contact with the soft mucosa of the nose and eyes of an uninfected individual.
Infants aged two months and younger are most vulnerable to severe RSV and this is further compounded by predisposing factors including prematurity, congenital heart defects, immune deficiencies or lung disease. Interestingly research has demonstrated that healthy infants account for more severe cases of RSV induced bronchiolitis when compared to high-risk babies. (Lambert et al., 2014)
Majority of children are infected with RSV by the age of two (Dawson-Caswell et al., 2011) and may present different clinical outcomes ranging from a mild upper respiratory tract illness to severe lower respiratory tract disease (McNamara et al., 2002). In order to prevent the development of chronic severe illnesses it is critically important to understand the key variances in the immunological response within RSV-infected children. It is the interaction between the human host and the virus that is key in determining the severity of RSV induced respiratory illnesses.
Pathophysiology of RSVRSV is a retrovirus that has 10 genes encoding 11 proteins where each protein holds crucial roles during viral infectivity and pathogenesis (Wu et al., 2012).
Figure 1. A single stranded RNA RSV genome containing 10 genes
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
2 Piril Erel – UoB 12004723
MPharm Year 3 SSA
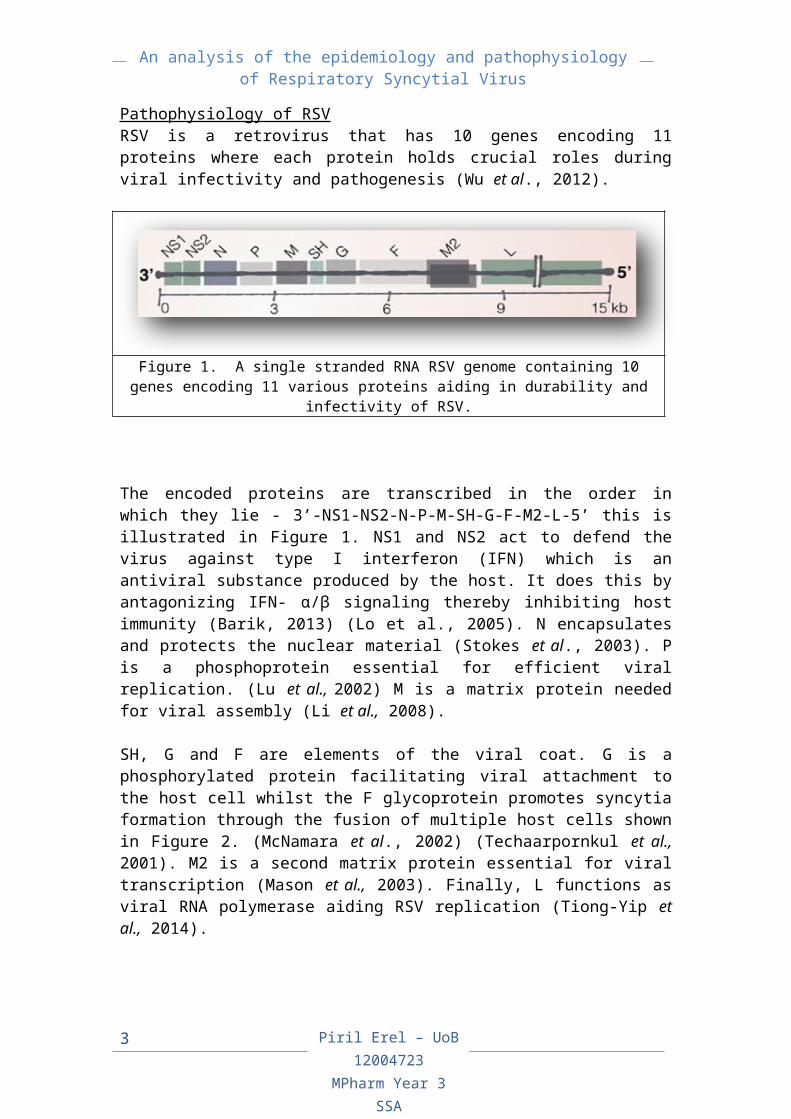
encoding 11 various proteins aiding in durability and infectivity of RSV.
The encoded proteins are transcribed in the order in which they lie - 3’-NS1-NS2-N-P-M-SH-G-F-M2-L-5’ this is illustrated in Figure 1. NS1 and NS2 act to defend the virus against type I interferon (IFN) which is an antiviral substance produced by the host. It does this by antagonizing IFN- α/β signaling thereby inhibiting host immunity (Barik, 2013) (Lo et al., 2005). N encapsulates and protects the nuclear material (Stokes et al., 2003). P is a phosphoprotein essential for efficient viral replication. (Lu et al., 2002) M is a matrix protein needed for viral assembly (Li et al., 2008).
SH, G and F are elements of the viral coat. G is a phosphorylated protein facilitating viral attachment to the host cell whilst the F glycoprotein promotes syncytia formation through the fusion of multiple host cells shown in Figure 2. (McNamara et al., 2002) (Techaarpornkul et al., 2001). M2 is a second matrix protein essential for viral transcription (Mason et al., 2003). Finally, L functions as viral RNA polymerase aiding RSV replication (Tiong-Yip et al., 2014).
Figure 2. RSV particles undergoing syncytial formation with host cell forming a multinucleated cell with infusion bodies containing viral
components
Acute RSV-bronchiolitis is characterized by infiltration of lung tissue by white blood cells such as neutrophils and lymphocytes, which are markers of inflammation (Bush et al., 2007). Once G protein attaches onto epithelial host cells, oedema of the mucosal epithelium begins followed by an increase in mucus secretion eventually forming mucus plugs. The obstruction from mucus secretion narrows the airways and due to a lack of oxygen flow this
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
3 Piril Erel – UoB 12004723
MPharm Year 3 SSA

eventually leads to the shedding of necrotic airway epithelial cells. It is important to note that majority of patients are children and have much softer, less rigid bronchioles and therefore are more predominantly prone to peribronchial lymphocytic hyperinflation or collapse of lung tissue downstream to the blockage (Eckardt-Michael et al., 2008).
Figure 3. The interaction of various factors leading to RSV-related respiratory disease due to RSV infectivity especially in developing
infant lung anatomical structures.
Interestingly severe RSV infection is associated with RSV-related bronchiolitis, RSV-related asthma as well as RSV-related pneumonia (Wu et al., 2012). RSV infections in infants are thought to correlate with individuals developing severe bronchiolitis and are associated with propensity to asthma later in life. Similar adverse conditions may be seen in those individuals who have asthma and other respiratory conditions (McNamara et al., 2002). Some research also implies that airway remodelling after RSV infection may increase susceptibility to asthma. Alternatively, studies have also pointed to a genetic aetiology and have suggested candidate genes associated with both severe RSV infection and asthma. Taking these data together, it seems likely that both mechanisms have a role and act in concert to cause asthma, which is illustrated in Figure 3. However, the underlying mechanisms resulting in later-onset asthma are poorly understood (Wu et al., 2012).
It would be ideal to develop a prophylactic vaccine for RSV however; there are a number of problems with this approach. Primarily most people are infected but not affected by RSV therefore it would be difficult to institute a national vaccination programme. In addition, there are a number of different strains of RSV making it difficult for us to develop a single effective treatment for infants. Notably, in
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
4 Piril Erel – UoB 12004723
MPharm Year 3 SSA

those that are affected, RSV is the most common single viral cause of severe respiratory disease in children and is the major cause of bronchiolitis in infants (Lambert et al., 2014).
Specific viral strains have been identified that are dominant over other strains. These have served to highlight the importance of specific viral proteins. An example of this is RSV genotype ON1. ON1 is characterized by a 72-nucleotide duplication in the gene encoding the G protein, and has been detected in more than 10 countries since first identified in Ontario, Canada, in 2010 (Agoti et al., 2014). Nevertheless, it seems not to be the viral genotype that is the crucial factor in causing severe bronchiolitis, but the host response (Openshaw et al., 2005) (Tregoning et al., 2010).
Genetics of Host ResponseSingle nucleotide polymorphism (SNP) analysis has been used to look for an association of human host genetic variance with disease. By pinpointing the candidate genes involved and analysing the mechanism behind proteins that are encoded by RSV, researchers gain insight into the varying severities. Several genes have been identified in controlling the immune response for example interleukin-4 (IL-4) and the interleukin-4 receptor- chain (IL4R), interleukin-8 (IL-8) (Heinzman et al., 2004), interleukin-9 (IL-9) (Olszewska et al., 2009), C-C chemokine receptor 5 (CCR5) (Hull et al., 2003), and in lung function for example surfactant protein A and surfactant protein B (Bruce et al., 2009) (Wang et al., 1999).
InterleukinsIL-4 is a pleiotropic cytokine that is produced by activated T cells thus forming part of the cell-mediated immune response. Overexpression of IL-4 delays viral clearance and accelerates inflammation. Its gene, IL4R encodes the alpha chain of the receptor protein that binds to IL-4 (Fischer et al, 1997), (Bukreyev et al, 2005). IL4R is upregulated in response to RSV infection (You et al., 2013). It is not difficult to understand that these loci may have a function given the role of leucocytes and neutrophils in lung inflammatory response to RSV.
IL-8 is a predominant inflammatory marker in RSV-bronchiolitis (Fielder et al., 1995). The gene product functions as a chemoattractant and elicits neutrophil accumulation at the site of infection (Patel et al., 1998). Enhanced IL-8 production in RSV-infected epithelial cells shows a strong correlation between the levels of IL-8 mRNA and disease severity in RSV-bronchiolitis (Zhou et al., 2014).
IL-9 expression is elevated in the bronchioles of infants with severe bronchiolitis (McNamara et al., 2004). IL-9 protein has been shown
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
5 Piril Erel – UoB 12004723
MPharm Year 3 SSA
to induce mucus production in bronchial epithelial cells, and this can result in goblet cell hyperplasia and increased chemokine secretion by respiratory epithelial cells and neutrophils (Olszewska et al., 2009). These data indicate that this protein may play a crucial role in the inflammatory cascade in the airways of patients with severe bronchiolitis. Figure 4 exemplifies the activation of IL-4, IL-9 and IL-13 resulting in epithelial-cell damage and goblet cell hyperplasia commonly seen in RSV-induced bronchiolitis and RSV-induced asthma.
Figure 4. Overexpression of IL-4, IL-9 and IL-13 results in goblet cell hyperplasia further complications of IL-4 expression found in asthmatic
patients
The observable signs and symptoms seen in individuals with RSV-bronchiolitis are apparent due to local immunological responses (Smyth et al., 2002), which are in turn governed by subtle host genotype variations or combinations of variance altering the response to infections rather than viral genotype being the major factor.
ChemokinesChemokines are small signaling proteins secreted by various cell types. They have the ability to induce directed chemotaxis in nearby responsive cells thus result in the recruitment of cells like leucocytes and neutrophils to specific areas. Initial research results have shown RSV infection induces the production of a variety of chemokines including CCL3 and CCL5. Studies show that higher expression levels are directly related to increased severity of RSV associated disease. CCL3 and CCL5 both signal via the CCR5 protein product and CCR5 polymorphisms are associated with severe RSV bronchiolitis (Hull et al., 2003).
Surfactant proteinsEpithelial cells in the alveolar tissue of the lung along with bronchiolar epithelial cells secrete surfactant protein A (SP-A). SP-A
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
6 Piril Erel – UoB 12004723
MPharm Year 3 SSA

binds to the RSV viral particles initiating the pathogen for clearance by host defence mechanisms through the stimulation of cellular and humoral immune systems. RSV reduces expression of SP-A by interfering with infected cells involved in the innate immune response. Interestingly, research has shown that RSV does not cause degradation of SP-A and does not interfere with cellular trafficking. However, it does inhibit translation rate, which results in a reduction of SP-A in both types of lung epithelial cells (Bruce et al., 2009). There is elevation of surfactant protein B found within infants with severe RSV bronchiolitis however; the mechanism by which this occurs is yet to be elucidated (Puthothu et al., 2007).SummaryAlthough researchers cannot pinpoint and understand the definitive causes of RSV related illnesses developed with advancing age, it is clear that there is a complex interaction between the host and the environment. Majority of individuals that are affected are infants, and it is imperative to note that there are significant anatomical changes and developments occurring at this age.
RSV has shown to have a willful ability to enter the host resulting in illness both by viral mechanisms and proteins encoded by RSV, dysregulating the synthesis of systemic immune response of the host. Alongside the infiltration of RSV, the heath status and genotype of the host will be a key factor in predetermining disease susceptibility and severity.
It is evident that genetic aspects have been implemented with both RSV and RSV-related illnesses. This may be an area of research to develop prophylactic vaccinations preventing severe RSV infections along with sequelae such as bronchiolitis, late-onset asthma and pneumonia.
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
7 Piril Erel – UoB 12004723
MPharm Year 3 SSA
1. Agoti, C., Otieno, J., Gitahi, C., Cane, P. and Nokes, D. (2014). Rapid Spread and
Diversification of Respiratory Syncytial Virus Genotype ON1, Kenya. Emerg. Infect.
Dis., 20(6), pp.950-959.
2. Barik, S. (2013). Respiratory syncytial virus mechanisms to interfere with type 1
intferons. [online] Ncbi.nlm.nih.gov. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/24362690 [Accessed 4 Jan. 2015].
3. Bruce, S., Atkins, C., Colasurdo, G. and Alcorn, J. (2009). Respiratory syncytial virus
infection alters surfactant protein A expression in human pulmonary epithelial cells by
reducing translation efficiency. AJP: Lung Cellular and Molecular Physiology, 297(4),
pp.L559-L567.
4. Bush, A. and Thomson, A. (2007). Acute bronchiolitis. BMJ, 335(7628), pp.1037-
1041.
5. Eckardt-Michel, J., Lorek, M., Baxmann, D., Grunwald, T., Keil, G. and Zimmer, G.
(2008). The Fusion Protein of Respiratory Syncytial Virus Triggers p53-Dependent
Apoptosis. Journal of Virology, 82(7), pp.3236-3249.
6. Fischer, J., Aung, S., Johnson, T., Johnson, J., Kuli-Zade, R., Parker, R. and
Graham, B. (1997). Overexpression of interleukin-4 delays virus clearance in mice
infected with respiratory syncytial virus.. [online] Ncbi.nlm.nih.gov. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/9343225 [Accessed 4 Jan. 2015].
7. Heinzmann, A., Ahlert, I., Kurz, T., Berner, R. and Deichmann, K. (2004). Association
study suggests opposite effects of polymorphisms within IL8 on bronchial asthma and
respiratory syncytial virus bronchiolitis. Journal of Allergy and Clinical Immunology,
114(3), pp.671-676.
8. Hull, J., Rowlands, K., Lockhart, E., Moore, C., Sharland, M. and Kwiatkowski, D.
(2003). Variants of the Chemokine Receptor CCR5 Are Associated with Severe
Bronchiolitis Caused by Respiratory Syncytial Virus. The Journal of Infectious
Diseases, 188(6), pp.904-907.
9. Lambert, L., Sagfors, A., Openshaw, P. and Culley, F. (2014). Immunity to RSV in
Early-Life. Frontiers in Immunology, 5.
10. Li, D., Jans, D., Bardin, P., Meanger, J., Mills, J. and Ghildyal, R. (2008). Association
of Respiratory Syncytial Virus M Protein with Viral Nucleocapsids Is Mediated by the
M2-1 Protein. Journal of Virology, 82(17), pp.8863-8870.
11. Lindsley, W., Blachere, F., Davis, K., Pearce, T., Fisher, M., Khakoo, R., Davis, S.,
Rogers, M., Thewlis, R., Posada, J., Redrow, J., Celik, I., Chen, B. and Beezhold, D.
(2010). Distribution of Airborne Influenza Virus and Respiratory Syncytial Virus in an
Urgent Care Medical Clinic. Clinical Infectious Diseases, pp.100125140412054-000.
12. Lo, M., Brazas, R. and Holtzman, M. (2005). Respiratory Syncytial Virus
Nonstructural Proteins NS1 and NS2 Mediate Inhibition of Stat2 Expression and
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
BIBLIOGRAPHY
An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
BIBLIOGRAPHYAlpha/Beta Interferon Responsiveness. Journal of Virology, 79(14), pp.9315-9319.
13. Lu, B., Ma, C., Brazas, R. and Jin, H. (2002). The Major Phosphorylation Sites of the
Respiratory Syncytial Virus Phosphoprotein Are Dispensable for Virus Replication In
Vitro. Journal of Virology, 76(21), pp.10776-10784.
14. Marin, D. and Herbet, M. (2011). Respiratory Syncytial Virus Infection in Children. 1st
ed. [ebook] New Orleans, Louisiana: American Family Physician, p.141. Available at:
http://www.aafp.org/afp/2011/0115/p141.pdf [Accessed 4 Jan. 2015].
15. Mason, S., Aberg, E., Lawetz, C., DeLong, R., Whitehead, P. and Liuzzi, M. (2003).
Interaction between Human Respiratory Syncytial Virus (RSV) M2-1 and P Proteins Is
Required for Reconstitution of M2-1-Dependent RSV Minigenome Activity. Journal of
Virology, 77(19), pp.10670-10676.
16. McNamara, P. (2002). The pathogenesis of respiratory syncytial virus disease in
childhood. British Medical Bulletin, 61(1), pp.13-28.
17. Olszewska, W. and Openshaw, P. (2009). Emerging drugs for respiratory syncytial
virus infection. Expert Opinion on Emerging Drugs, 14(2), pp.207-217.
18. Openshaw, P. and Tregoning, J. (2005). Immune Responses and Disease
Enhancement during Respiratory Syncytial Virus Infection. Clinical Microbiology
Reviews, 18(3), pp.541-555.
19. Patel, J., Jiang, Z., Nakajima, N. and Kunimoto, M. (1998). Autocrine regulation of
interleukin-8 by interleukin-1alpha in respiratory syncytial virus-infected pulmonary
epithelial cells in vitro. Immunology, 95(4), pp.501-506.
20. Puthothu, B., Forster, J., Heinze, J., Heinzmann, A. and Krueger, M. (2007).
Surfactant protein B polymorphisms are associated with severe respiratory syncytial
virus infection, but not with asthma. BMC Pulm Med, 7(1), p.6.
21. Smyth, R., Mobbs, K., O'Hea, U., Ashby, D. and Hart, C. (2002). Respiratory syncytial
virus bronchiolitis: Disease severity, interleukin-8, and virus genotype. Pediatr.
Pulmonol., 33(5), pp.339-346.
22. Stokes, H. (2003). Chimeric pneumovirus nucleocapsid (N) proteins allow
identification of amino acids essential for the function of the respiratory syncytial virus
N protein. Journal of General Virology, 84(10), pp.2679-2683.
23. Techaarpornkul, S., Barretto, N. and Peeples, M. (2001). Functional Analysis of
Recombinant Respiratory Syncytial Virus Deletion Mutants Lacking the Small
Hydrophobic and/or Attachment Glycoprotein Gene. Journal of Virology, 75(15),
pp.6825-6834.
24. Tiong-Yip, C., Aschenbrenner, L., Johnson, K., McLaughlin, R., Fan, J., Challa, S.,
Xiong, H. and Yu, Q. (2014). Characterization of a Respiratory Syncytial Virus L
Protein Inhibitor. Antimicrobial Agents and Chemotherapy, 58(7), pp.3867-3873.
25. Tregoning, J. and Schwarze, J. (2010). Respiratory Viral Infections in Infants:
Causes, Clinical Symptoms, Virology, and Immunology. Clinical Microbiology
Reviews, 23(1), pp.74-98.
9 Piril Erel – UoB 12004723
MPharm Year 3 SSA

An analysis of the epidemiology and pathophysiology of Respiratory Syncytial Virus
BIBLIOGRAPHY26. Wang, S., Doyle, I., Nicholas, T. and Forsyth, K. (1999). Plasma Surfactant Protein-B
Is Elevated in Infants with Respiratory Syncytial Virus-Induced Bronchiolitis. Pediatr
Res, 46(6), pp.731-731.
27. Wu, P. and Hartert, T. (2011). Evidence for a causal relationship between respiratory
syncytial virus infection and asthma. Expert Review of Anti-infective Therapy, 9(9),
pp.731-745.
28. You, D., Marr, N., Saravia, J., Shrestha, B., Lee, G., Turvey, S., Brombacher, F.,
Herbert, D. and Cormier, S. (2013). IL-4RÂ on CD4+ T cells plays a pathogenic role
in respiratory syncytial virus reinfection in mice infected initially as neonates. Journal
of Leukocyte Biology, 93(6), pp.933-942.
29. Zhou, Y., Yang, J., Deng, H., Xu, H., Zhang, J., Jin, W., Gao, H., Liu, F. and Zhao, D.
(2014). Respiratory syncytial virus infection modulates interleukin-8 production in
respiratory epithelial cells through a transcription factor activator protein 1 signaling
pathway. Molecular Medicine Reports.
10 Piril Erel – UoB 12004723
MPharm Year 3 SSA