assessment of stroke ischemic vs hemorrhagic stroke · 8/2/2015 2 hemorrhagic stroke 20% of all...
TRANSCRIPT
8/2/2015
1
Assessment of
Ischemic vs Hemorrhagic Stroke
Cynthia Bautista, PhD, RN, CNRN, SCRN, CCNS, ACNS-BC, FNCS
Nursing Brains, LLC
Stroke
In the USA 795,000 new or recurrent strokes
Represents 5th leading cause of death in USA
Copyright Nursing Brains, LLC
Ischemic vs Hemorrhagic
Ischemic stroke is 10x more frequent
Hemorrhagic stroke has higher mortality risk
Common risk factors
Copyright Nursing Brains, LLC
Ischemic Stroke
80% of all strokes Blockage in blood vessel Fatty deposits lining blood vessel wall
Thrombosis (50%)◦ Thrombi formed by plaque
◦ Greater than 50%stenosis
Embolism (30%)◦ Cardiac emboli
◦ Atrial Fibrillation
Copyright Nursing Brains, LLC
Cryptogenic Stroke
30% of ischemic strokes Infarct of undetermined cause Hemispheral infarction Average age 58 No risk factors
Copyright Nursing Brains, LLC
Lacunar Stroke
25% of Ischemic strokes Thrombosis of Lenticulostriate arteries
(small penetrating arteries) Predominate in basal ganglia Caused by hypertension and diabetes No treatment Risk factor management
Copyright Nursing Brains, LLC
8/2/2015
2
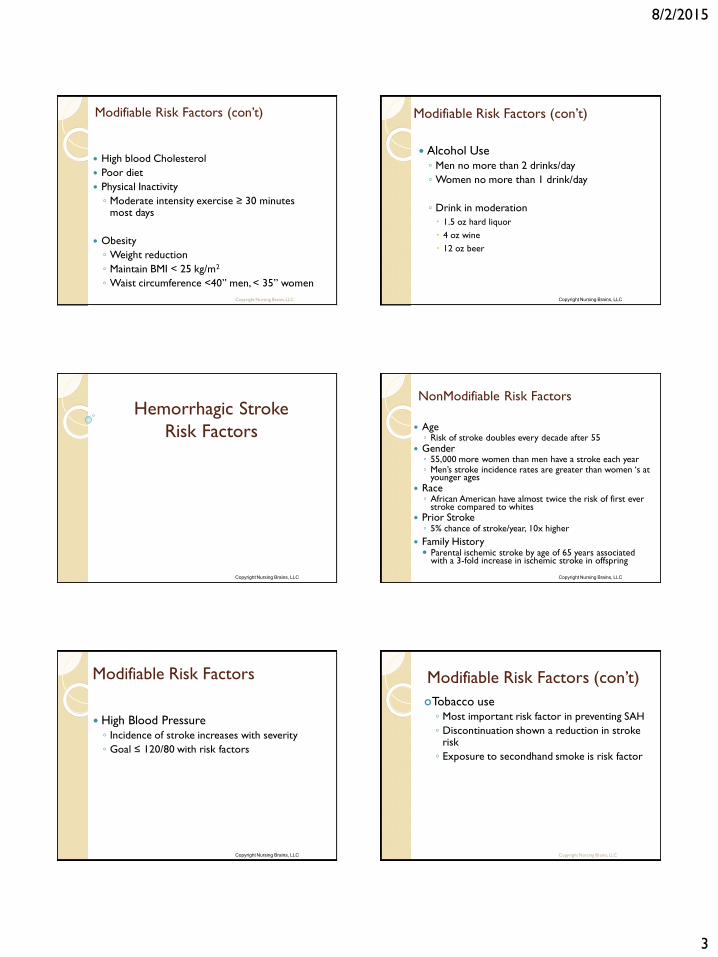
Hemorrhagic Stroke
20% of all strokes
Rupture of leaking blood vessel
Intracerebral (ICH)
◦ High blood pressure
Subarachnoid (SAH)
◦ Cerebral Aneurysm
◦ Arterial Venous Malformation
Intraventricular (IVH)
◦ ICH and/or SAH
Hemorrhagic transformation of ischemic infarct
Copyright Nursing Brains, LLC
Ischemic Stroke
Risk Factors
Copyright Nursing Brains, LLC
NonModifiable Risk Factors
Age◦ Risk of stroke doubles every decade after 55
Gender◦ 55,000 more women than men have a stroke each year◦ Men’s stroke incidence rates are greater than women ‘s at
younger ages
Race◦ African American have almost twice the risk of first ever
stroke compared to whites
Prior Stroke◦ 5% chance of stroke/year, 10x higher
Family History Parental ischemic stroke by age of 65 years associated
with a 3-fold increase in ischemic stroke in offspring
Copyright Nursing Brains, LLC
Modifiable Risk Factors
High Blood Pressure◦ Powerful determinant of risk for both ischemic
stroke and ICH
◦ 77% of first time stroke patients BP > 140/90
◦ Blacks more aware of hypertension than whites
Diabetes◦ Increases ischemic stroke incidence at all ages
◦ Most prominent before 65 years old in blacks & whites
◦ Doubles stroke risk with history of TIACopyright Nursing Brains, LLC
Modifiable Risk Factors (con’t)
Tobacco use
◦ Ischemic and hemorrhagic stroke
◦ Aggravates atherosclerosis and raises BP
◦ 50% reduction of risk with cessation
◦ Counseling, nicotine products, oral smoking cessation medications
◦ Implement 5 A’s
ASK about tobacco use
ADVISE to quit
ASSESS willingness to attempt to quit
ASSIST in the quit attempt
ARRANGE follow-up
Copyright Nursing Brains, LLC
Modifiable Risk Factors (con’t)
Carotid Disease
Atrial Fibrillation◦ 50% of all embolic strokes
◦ Anticoagulation reduces risk by 68%
Cardiac Disease◦ Routine screening
◦ Aggressive treatment
Sickle Cell Disease
Copyright Nursing Brains, LLC
8/2/2015
3
Modifiable Risk Factors (con’t)
High blood Cholesterol
Poor diet
Physical Inactivity
◦ Moderate intensity exercise ≥ 30 minutes most days
Obesity
◦ Weight reduction
◦ Maintain BMI < 25 kg/m2
◦ Waist circumference <40” men, < 35” women
Copyright Nursing Brains, LLC
Modifiable Risk Factors (con’t)
Alcohol Use◦ Men no more than 2 drinks/day
◦ Women no more than 1 drink/day
◦ Drink in moderation
1.5 oz hard liquor
4 oz wine
12 oz beer
Copyright Nursing Brains, LLC
Hemorrhagic Stroke
Risk Factors
Copyright Nursing Brains, LLC
NonModifiable Risk Factors
Age◦ Risk of stroke doubles every decade after 55
Gender◦ 55,000 more women than men have a stroke each year◦ Men’s stroke incidence rates are greater than women ‘s at
younger ages
Race◦ African American have almost twice the risk of first ever
stroke compared to whites
Prior Stroke◦ 5% chance of stroke/year, 10x higher
Family History Parental ischemic stroke by age of 65 years associated
with a 3-fold increase in ischemic stroke in offspring
Copyright Nursing Brains, LLC
Modifiable Risk Factors
High Blood Pressure◦ Incidence of stroke increases with severity
◦ Goal ≤ 120/80 with risk factors
Copyright Nursing Brains, LLC
Modifiable Risk Factors (con’t)
Tobacco use ◦ Most important risk factor in preventing SAH
◦ Discontinuation shown a reduction in stroke risk
◦ Exposure to secondhand smoke is risk factor
Copyright Nursing Brains, LLC
8/2/2015
4
Modifiable Risk Factors (con’t)
Alcohol Use◦ Men no more than 2 drinks/day
◦ Women no more than 1 drink/day
◦ Drink in moderation
1.5 oz hard liquor
4 oz wine
12 oz beer
Copyright Nursing Brains, LLC
Modifiable Risk Factors (con’t)
Drug Abuse◦ Occurs first time or long-term user
◦ Amphetamines, cocaine, heroin
◦ Hypertension
◦ Intracerebral Hemorrhage
◦ Screen
◦ Rehabilitation
Copyright Nursing Brains, LLC
Ischemic Stroke Presentation
Copyright Nursing Brains, LLC
Left (Dominant Hemisphere)
Left gaze preference Right visual field deficit Right hemiparesis Right hemisensory loss
Copyright Nursing Brains, LLC
Right (Nondominant Hemisphere)
Right gaze preference Left visual field deficit Left hemiparesis Left hemisensory loss◦ Neglect (left hemi-inattention)
Copyright Nursing Brains, LLC
Brainstem Stroke Syndrome
Decreased consciousness Diplopia, dysconjugate gaze, gaze palsy Hemiparesis or quadriplegia Sensory loss in hemibody or all 4 limbs Dysarthria Dysphagia Vertigo, tinnitus Nausea/vomiting Abnormal respirations
Copyright Nursing Brains, LLC
8/2/2015
5
Cerebellum Stroke Syndrome
Gait ataxia Limb ataxia Neck stiffness Nystagmus
Copyright Nursing Brains, LLC
Warning Signs of Stroke
Think F-A-S-T
F = FACE numbness or weakness especially one side of body
A = ARM numbness or weakness one side of body
S = SPEECH slurred or difficulty speaking or understanding
T = TIME to immediately call 9-1-1 and note time symptoms started or last time person was seen normal
Copyright Nursing Brains, LLC
Hemorrhagic Stroke
Presentation
Copyright Nursing Brains, LLC
Hemorrhage Stroke Syndromes
Decreased level of consciousness Focal neurological deficits Headache Neck pain Light intolerance Nausea, vomiting
Copyright Nursing Brains, LLC
Level of Consciousness
Glasgow Coma Scale
Eye Opening
◦ 4 - Spontaneous
◦ 3 - To Speech
◦ 2 - To Pain
◦ 1 - None
Verbal Response
◦ 5 - Oriented
◦ 4 - Confused
◦ 3 - Inappropriate Words
◦ 2 - Inappropriate Sounds
◦ 1 - None
Motor Response
◦ 6 - Obeys Commands
◦ 5 - Localizes
◦ 4 - Withdraws
◦ 3 - Abnormal Flexion
◦ 2 - Abnormal Extension
◦ 1 -None
Copyright Nursing Brains, LLC
Ischemic Stroke Imaging
Copyright Nursing Brains, LLC
8/2/2015
6
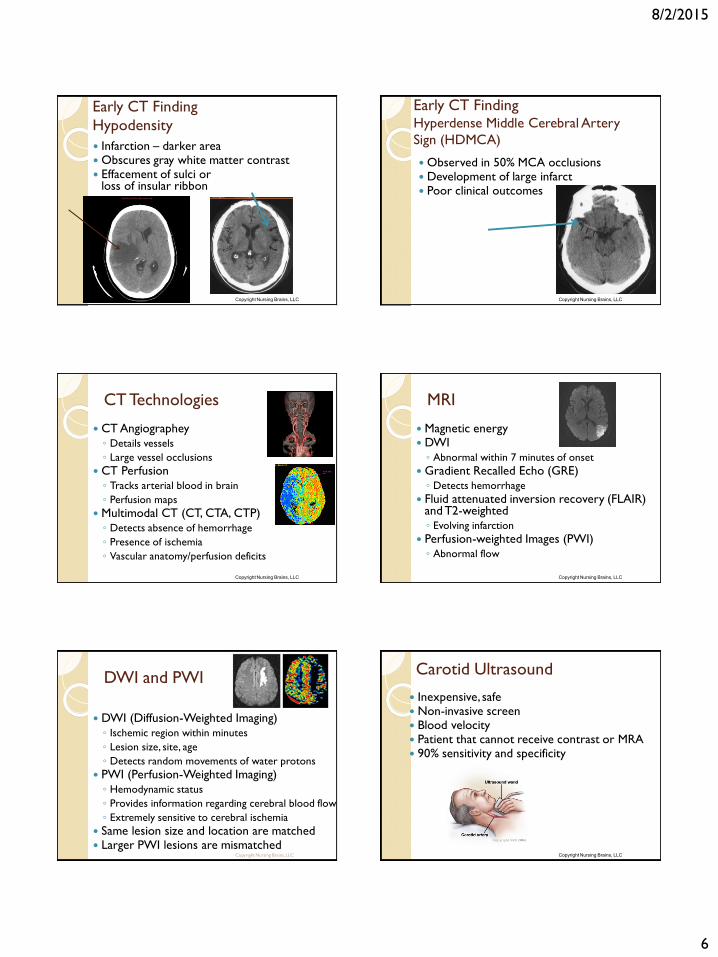
Early CT Finding
Hypodensity
Infarction – darker area Obscures gray white matter contrast Effacement of sulci or
loss of insular ribbon
Copyright Nursing Brains, LLC
Early CT FindingHyperdense Middle Cerebral Artery
Sign (HDMCA)
Observed in 50% MCA occlusions Development of large infarct Poor clinical outcomes
Copyright Nursing Brains, LLC
CT Technologies
CT Angiographey◦ Details vessels
◦ Large vessel occlusions
CT Perfusion◦ Tracks arterial blood in brain
◦ Perfusion maps
Multimodal CT (CT, CTA, CTP)◦ Detects absence of hemorrhage
◦ Presence of ischemia
◦ Vascular anatomy/perfusion deficits
Copyright Nursing Brains, LLC
MRI
Magnetic energy DWI◦ Abnormal within 7 minutes of onset
Gradient Recalled Echo (GRE)◦ Detects hemorrhage
Fluid attenuated inversion recovery (FLAIR) and T2-weighted ◦ Evolving infarction
Perfusion-weighted Images (PWI)◦ Abnormal flow
Copyright Nursing Brains, LLC
DWI and PWI
DWI (Diffusion-Weighted Imaging) ◦ Ischemic region within minutes
◦ Lesion size, site, age
◦ Detects random movements of water protons
PWI (Perfusion-Weighted Imaging) ◦ Hemodynamic status
◦ Provides information regarding cerebral blood flow
◦ Extremely sensitive to cerebral ischemia
Same lesion size and location are matched Larger PWI lesions are mismatched
Copyright Nursing Brains, LLC
Carotid Ultrasound
Inexpensive, safe Non-invasive screen Blood velocity Patient that cannot receive contrast or MRA 90% sensitivity and specificity
Copyright Nursing Brains, LLC
8/2/2015
7
Digital Subtraction Angiography
(DSA)
Gold Standard for cerebral vasculature Degree of stenosis Provides interventions◦ Thrombolytics
◦ Thrombectomy
◦ Angioplasty and stenting
Copyright Nursing Brains, LLC
Echocardiogram
Transthoracic
Noninvasive utilizing sound waves
Transesophageal
Combines ultrasonography & endoscopy
Image posterior of the heart
Heart structures
Clots, valves, PFO, LV function
Copyright Nursing Brains, LLC
Hemorrhagic Stroke Imaging
Copyright Nursing Brains, LLC
Early CT Finding
Hyperdensity
Hemorrhage appears white Petechial is scattered hyperdense points Hematoma is solid, homogenously
hyperdense legion
Copyright Nursing Brains, LLC
Predicting ICH Expansion
Spot sign on CTA
Copyright Nursing Brains, LLC
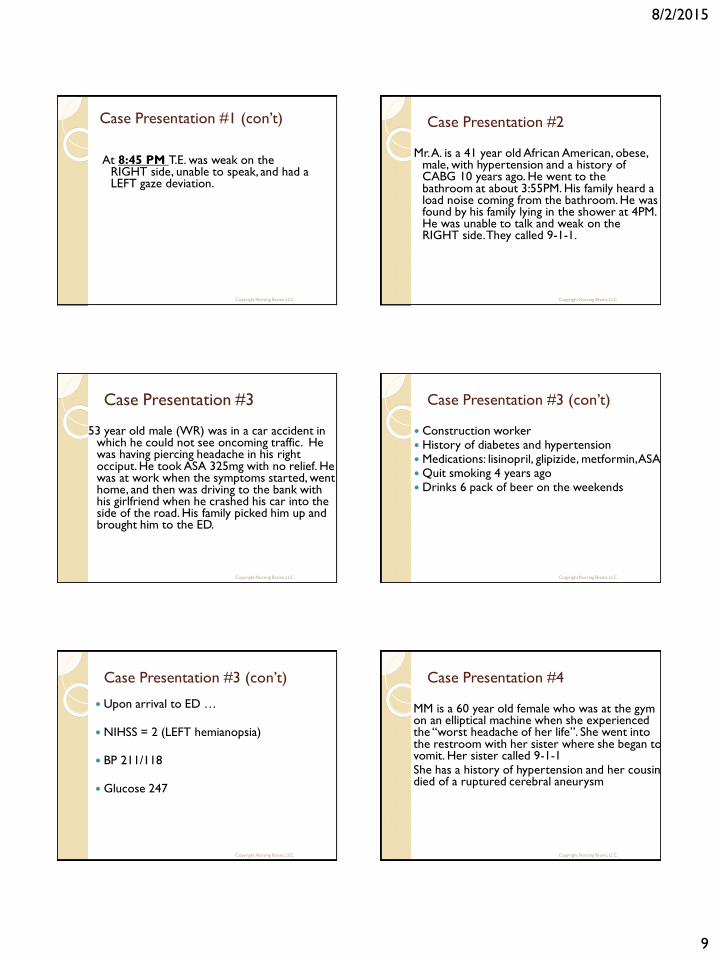
CT Scan in SAH
Copyright Nursing Brains, LLC

8/2/2015
8
MRA
Extracranial & intracranial cerebral circulation abnormalities
86% sensitivity 98% specificity Aneurysm detection 95% sensitivity
Copyright Nursing Brains, LLC
CT Scan in
Intraventricular Hemorrhage
Copyright Nursing Brains, LLC
CT Scan in
Hemorrhagic Transformation of
Ischemic Stroke
Copyright Nursing Brains, LLC
Transcranial Doppler (TCD)
Safe, inexpensive Flow of blood through arteries of the brain High frequency sound waves pass through
tissue Detects, monitors stenosis, vasospams,
reperfusion Concern with
◦ Velocity of >120
◦ Lindegaard ration > 3
Copyright Nursing Brains, LLC
Stroke Case Studies
Copyright Nursing Brains, LLC
Case Presentation #1
T.E. is a 39 year old Caucasian man who works in construction. Ten years ago he had a myocardial infarction, EF 45% with apical akenesis and an intraventricular thrombus (was on warfarin). Has a history of TIAs, hypercholesterolemia and smokes 2-3 packs per day.
He left his house about 8:15PM and was found lying on the sidewalk. People passing by called 9-1-1.
Copyright Nursing Brains, LLC
8/2/2015
9
Case Presentation #1 (con’t)
At 8:45 PM T.E. was weak on the RIGHT side, unable to speak, and had a LEFT gaze deviation.
Copyright Nursing Brains, LLC Copyright Nursing Brains, LLC
Case Presentation #2
Mr. A. is a 41 year old African American, obese, male, with hypertension and a history of CABG 10 years ago. He went to the bathroom at about 3:55PM. His family heard a load noise coming from the bathroom. He was found by his family lying in the shower at 4PM. He was unable to talk and weak on the RIGHT side. They called 9-1-1.
Case Presentation #3
53 year old male (WR) was in a car accident in which he could not see oncoming traffic. He was having piercing headache in his right occiput. He took ASA 325mg with no relief. He was at work when the symptoms started, went home, and then was driving to the bank with his girlfriend when he crashed his car into the side of the road. His family picked him up and brought him to the ED.
Copyright Nursing Brains, LLC
Case Presentation #3 (con’t)
Construction worker History of diabetes and hypertension Medications: lisinopril, glipizide, metformin, ASA Quit smoking 4 years ago Drinks 6 pack of beer on the weekends
Copyright Nursing Brains, LLC
Case Presentation #3 (con’t)
Upon arrival to ED …
NIHSS = 2 (LEFT hemianopsia)
BP 211/118
Glucose 247
Copyright Nursing Brains, LLC
Case Presentation #4
MM is a 60 year old female who was at the gym on an elliptical machine when she experienced the “worst headache of her life”. She went into the restroom with her sister where she began to vomit. Her sister called 9-1-1She has a history of hypertension and her cousin died of a ruptured cerebral aneurysm
Copyright Nursing Brains, LLC
8/2/2015
10
Case Presentation #5
D.B. is a 75 year old Caucasian man in good health. He quit smoking over 30 years ago and has no family history of stroke. He has not seen a physician in over 40 years. He was taking his family to McDonalds for lunch. After leaving the drive thru window he began to drive erratically over curbs and islands. D.B. had a sudden onset of right facial droop, right arm weakness, and difficulty speaking.
His daughter got him to stop the car and she called 9-1-1.
Case Presentation #6
A 57-year-old female (CB) last spoke to her relatives on Sunday. She did not answer her phone on Monday. The landlady entered her apartment on Thursday and found her lying face down on floor of living room covered in vomit and feces. Landlady called 9-1-1
Case Presentation #6
Pre Hospital◦ Vital signs 149/94 – 79 – 20, 99.3, pulse
oxygenation 98%
◦ Not moving right side
Emergency Room◦ 162/83 – 87 – 20
◦ Pupils equal react to light
◦ Opens eyes, difficult to remain awake
Case Presentation #6
History of chronic atrial fibrillation Coumadin started in 2007 Noncompliant Sub therapeutic INR Patient on ASA only
Case Presentation #7
83 year old man (JP) fell at home x2 last night. He was able to getup on his own after the first fall, unable to getup after 2nd
fall. According to wife, JP began acting abnormal (asking strange questions, using inappropriate words). Wife dragged JP from living room to bedroom. They slept together on the floor in the bedroom.
Case Presentation #7 (con’t)
In the morning the wife was unable to wake JP up and called 9-1-1
JP had right sided weakness, right facial droop
History of TIA, CAD, hypertension Pre Hospital
◦ 198/80 – 93 – 20 Pulse oxygenation 95%