attachment & cognitive therapy patricia m. crittenden, ph.d. © patricia m. crittenden, 2005
TRANSCRIPT

Attachment & Cognitive Therapy
Patricia M. Crittenden, Ph.D.
© Patricia M. Crittenden, 2005

Four Growing Points
1. Symptoms: diagnoses & treatment
1. Emphasis on “cognitive” rational & verbal processes
1. Model of psychological functioning & psychopathology
1. Evaluation of harmful effects of psychotherapy
© Patricia M. Crittenden, 2005

Symptoms
• Distress = patient’s perspective
• Diagnosis = professional’s perspective
• Self-protective strategies
• Behaviors can serve many functions
© Patricia M. Crittenden, 2005

Symptoms, con’t
• 50%+ failure rate 1 year post-CT
• Focus on symptom vs. reason for symptom
• Competence with danger vs. competence with safety
• Strengths approach vs. vulnerability© Patricia M. Crittenden, 2005

“Cognition” & Affect
Cognition• Temporal, causal contingencies• Verbal generalizations about contingencies: core
beliefs
Affect• Response to intensity of sensory stimulation• Somatic & psychological feelings: images
© Patricia M. Crittenden, 2005
“Cognitive” Memory Systems
• Procedural Memory– Reflexive, sensorimotor schema– Preconscious– Learned from experienced consequences– Re-active
• Semantic memory– Verbalized procedural contingencies– When/then & if/then and (distorted) absolute forms– Borrowed– Should & ought to do
© Patricia M. Crittenden, 2005

“Affective” Memory Systems
• Imaged memory– Possibility of danger– Fight, flight, freeze– Bodily arousal and feeling anxious– Pro-active
• Connotative language– Brings images to mind– Elicits feeling in listener
© Patricia M. Crittenden, 2005

Integrative Memory Systems
• Episodic memory– Cognitive-affective integration– Learned at about 3 years– Dependent upon a dialogue– Biased by what parents will talk about
• Reflective integration– Permits information to be corrected– Is slow– Done best under safe conditions
© Patricia M. Crittenden, 2005

Memory SystemsTemporal Order
(Cognition)
Procedural
Semantic
Intensity(Affect)
Imaged
Connotative Language
Episodic
Reflective Integration© Patricia M. Crittenden, 2005

Dispositional Representation
• Relation of self to context
• Each different DR disposes behavior differently
• Each highlights some aspect of the problem, but obscures some other
© Patricia M. Crittenden, 2005

Arousal Scale1. Anxiety
• Pain • Sexual Desire• Fear• Anger• Desire for comfort
2. Comfort
3. Depression• Boredom • Tiredness• Sleep• Unconsciousness
© Patricia M. Crittenden, 2005

Transformations
Sensory stimulation
Transformations of information
Dispositional representations
Enacted behavior
© Patricia M. Crittenden, 2005

The only information that we have is information about the past
whereas
The only information that we need is information about the future.
© Patricia M. Crittenden, 2005

Transformations of Information
• True
• Erroneous
• Omitted
• Distorted
• Falsified
© Patricia M. Crittenden, 2005

Ty
pe
of
Tra
ns
form
ati
on
of
Info
rma
tio
n
False
True
Integration of Cognitive and Affective Information AffectiveCognitive
© Patricia M. Crittenden, 2005
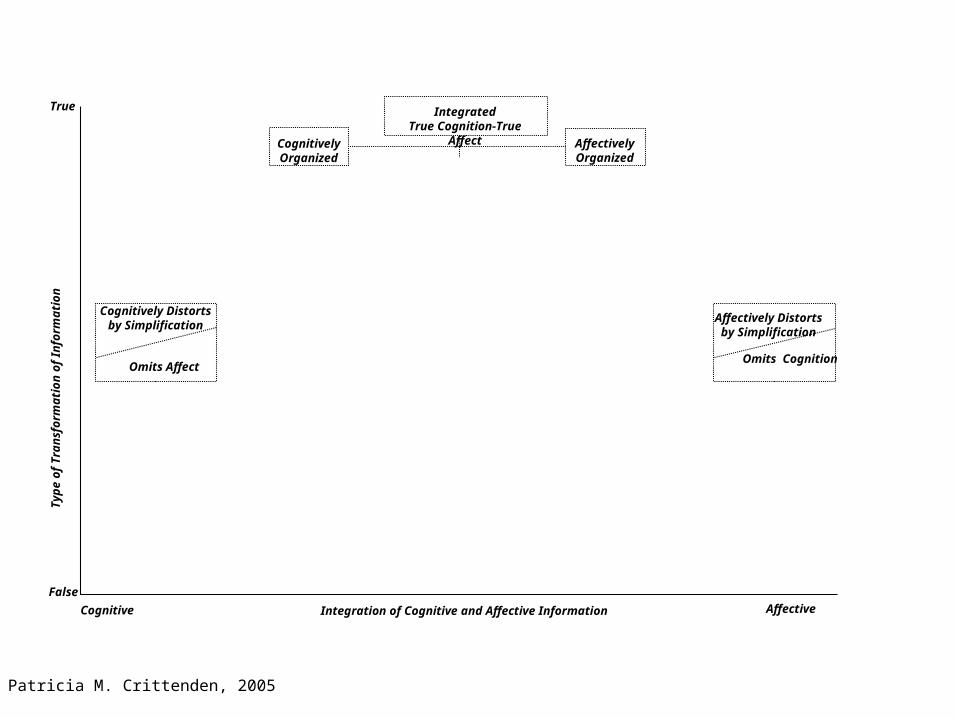
Omits Affect
Cognitively Distortsby Simplification
IntegratedTrue Cognition-True
Affect AffectivelyOrganized
CognitivelyOrganized
Omits Cognition
Affectively Distorts
by Simplification
Ty
pe
of
Tra
ns
form
ati
on
of
Info
rma
tio
n
False
True
Integration of Cognitive and Affective Information AffectiveCognitive
© Patricia M. Crittenden, 2005

Adaptive in SafeContexts, but
Otherwise Maladaptive
Omits Affect
Cognitively Distortsby Simplification
Adaptive in Dangerous
Contexts, but Otherwise
Maladaptive
IntegratedTrue Cognition-True
Affect AffectivelyOrganized
CognitivelyOrganized
Increasing Risk of Mental Health
Problems
Increasing Risk of Mental Health
Problems
Adaptive in SafeContexts, but
Otherwise Maladaptive
Omits Cognition
Affectively Distorts
by Simplification
Adaptive in Dangerous
Contexts, but Otherwise
Maladaptive
Ty
pe
of
Tra
ns
form
ati
on
of
Info
rma
tio
n
False
True
Integration of Cognitive and Affective Information AffectiveCognitive
© Patricia M. Crittenden, 2005

Adaptive in SafeContexts, but
Otherwise Maladaptive
Omits Affect
Cognitively Distorts
by Simplification
Adaptive in Dangerous
Contexts, but Otherwise
MaladaptiveAAnti@ Integrated
False Cognition-False Affect
IntegratedTrue Cognition-True
Affect
Various CoerciveC+ Strategies
Various CompulsiveA+ Strategies
Type CCoercive/
Enmeshed(Anxious Ambivalent)
Type ADefended/
Disengaged(Anxious Avoidant)
Type A+/C+Unintegrated
Cognitive/Affect
Type BBalanced/
Secure
Type A+C+Psychopathy
AffectivelyOrganized
CognitivelyOrganized
ReactiveReserved
Increasing Risk of Mental Health
Problems
Increasing Risk of Mental Health
Problems
Adaptive in SafeContexts, but
Otherwise Maladaptive
Omits Cognition
Affectively Distorts
by Simplification
Adaptive in Dangerous
Contexts, but Otherwise
Maladaptive
Ty
pe
of
Tra
ns
form
ati
on
of
Info
rma
tio
n
False
True
Integration of Cognitive and Affective Information AffectiveCognitive
© Patricia M. Crittenden, 2005

A Dynamic-Maturational Model of Patterns of Attachment in Adulthood
False Affect
Cognition(Type A)
Affect(Type C)
Integrated False Information(Type A+C+)
Integrated True Information(Type B)
True Cognition
Compulsively Caregiving/Compliant
Delusional Idealization/Externally
Assembled Self
Compulsively Promiscuous/Self-Reliant
Socially Facile/Inhibited
ComfortableB3
ReservedB1-2 B4-5
Reactive
A1-2
A3-4
A7-8
A5-6
C7-8
C5-6
C3-4
C1-2Threatening/
Disarming
Aggressive/Feigned Helpless
Punitive/Seductive
Menacing/ParanoidAC
Psychopathy
A/C
True Affect
False Cognition© Patricia M. Crittenden, 2005

Treatment Outcomes
• There could be harmful effects
• Cognitive & affective strategies are psychological opposites
• They might need opposite treatments
© Patricia M. Crittenden, 2005

Ideas from Attachment Theory
• The importance of understanding the self-protective function of symptoms.
• The strategic organization of all persons, patients included.
• The importance of affect.
• The structure of human psychological organization as consisting of two opposite processes and their integration - with patients rarely displaying integration.
© Patricia M. Crittenden, 2005

Ideas from Attachment Theory
• The possibility that treatments may have different effects on people with similar symptoms, but opposite psychological organizations.
• The important of therapists knowing both the organization of each patient and also the effects on psychological functioning of each treatment technique that they employ.
• The importance of the therapist being, uniquely for each patient, a transitional attachment figure who helps to create enough safety and comfort for change to be explored.
© Patricia M. Crittenden, 2005

This talk can be down-loaded from:
www.patcrittenden.com
© Patricia M. Crittenden, 2005