bi1 part 3b: endobronchial brushing volume 1 bronchoscopy international strategy and planning...
TRANSCRIPT

BIBI 11
Part 3B: Endobronchial BrushingPart 3B: Endobronchial Brushingvolume 1volume 1
Bronchoscopy InternationalBronchoscopy International
Strategy and Planning
Execution

BIBI 22
When to perform endobronchial When to perform endobronchial brushingbrushing
Visible airway mucosal abnormalitiesVisible airway mucosal abnormalities Visible airway nodules or massesVisible airway nodules or masses In case of suspected sarcoidosis (even if In case of suspected sarcoidosis (even if
airway mucosa appears normal)airway mucosa appears normal) In case of abnormal autofluorescence to In case of abnormal autofluorescence to
diagnose intraepithelial lesions (dysplasia, diagnose intraepithelial lesions (dysplasia, metaplasia, carcinoma in-situ)metaplasia, carcinoma in-situ)
BIBI 33
Training is essential in order toTraining is essential in order to
Learn proper techniques and indicationsLearn proper techniques and indications Avoid procedure-related complications.Avoid procedure-related complications. Learn to protect the equipment and the Learn to protect the equipment and the
patientpatient To obtain adequate tissue for diagnosisTo obtain adequate tissue for diagnosis To avoid damaging the working channelTo avoid damaging the working channel To avoid excess patient discomfort (cough, To avoid excess patient discomfort (cough,
anxiety, shortness of breath).anxiety, shortness of breath). To avoid bleeding, that might also prompt To avoid bleeding, that might also prompt
cough and patient agitation.cough and patient agitation.
BIBI 44
Q1: Optimal endobronchial brushing Q1: Optimal endobronchial brushing samples requires correct processingsamples requires correct processing
BIBI 55
Q8: Optimal endobronchial brushing Q8: Optimal endobronchial brushing samples requires correct processingsamples requires correct processing

BIBI 66
TRUETRUE. Brushing samples must be processed . Brushing samples must be processed correctly and according to the needs and correctly and according to the needs and preferences of your institution’s cytology preferences of your institution’s cytology
and microbiology laboratories.and microbiology laboratories.
Other ways to potentially increase Other ways to potentially increase diagnostic yield includediagnostic yield include Using brushes with longer bristlesUsing brushes with longer bristles Brushing vigorously and for a longer period of Brushing vigorously and for a longer period of
time.time. Making sure that all parts of the brush are in Making sure that all parts of the brush are in
contact with the mucosal abnormality.contact with the mucosal abnormality. Using the pirouette technique (rotation) in Using the pirouette technique (rotation) in
combination with long-axis motion.combination with long-axis motion.
BIBI 77
Bronchial brushing:Bronchial brushing:
Originally done under fluoroscopy without Originally done under fluoroscopy without bronchoscopybronchoscopy
Common indications:Common indications: Visible endobronchial tumors or mucosal abnormalityVisible endobronchial tumors or mucosal abnormality Peripheral tumors (+/- fluoroscopy)Peripheral tumors (+/- fluoroscopy) Peripheral infection – pneumonia, abscess, cavityPeripheral infection – pneumonia, abscess, cavity
Brush samples larger surface area of lesionBrush samples larger surface area of lesion
BIBI 88
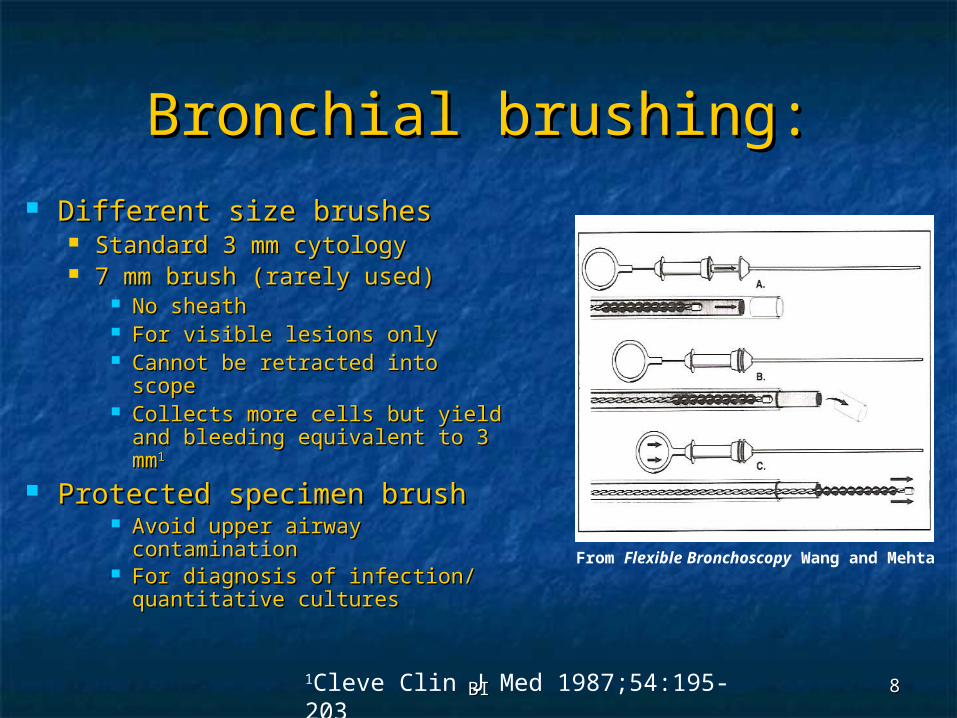
Bronchial brushing:Bronchial brushing: Different size brushesDifferent size brushes
Standard 3 mm cytology Standard 3 mm cytology 7 mm brush (rarely used)7 mm brush (rarely used)
No sheathNo sheath For visible lesions onlyFor visible lesions only Cannot be retracted into scopeCannot be retracted into scope Collects more cells but yield Collects more cells but yield
and bleeding equivalent to 3 and bleeding equivalent to 3 mmmm11
Protected specimen brushProtected specimen brush Avoid upper airway Avoid upper airway
contaminationcontamination For diagnosis of infection/ For diagnosis of infection/
quantitative culturesquantitative cultures
1Cleve Clin J Med 1987;54:195-203
From Flexible Bronchoscopy Wang and Mehta

BIBI 99
Bronchial brushing:Bronchial brushing:
Technique:Technique: Advance catheter into desired segment Advance catheter into desired segment
– then extend brush (up to 5 cm)– then extend brush (up to 5 cm) Make sure brush extension doesn’t push Make sure brush extension doesn’t push
back the scope or catheterback the scope or catheter Move back and forth over the visible Move back and forth over the visible
lesion or blindly in distal airway (5-10 lesion or blindly in distal airway (5-10 times) +/- rotationtimes) +/- rotation
Cells collected in brush bristlesCells collected in brush bristles

BIBI 1010
Bronchial brushing:Bronchial brushing:
Yield:Yield: 94% endoscopically visible/peripheral 94% endoscopically visible/peripheral
78%78%11
92% central and peripheral with fluoro92% central and peripheral with fluoro22
77% endoscopically visible/20% 77% endoscopically visible/20% peripheral with fluoroperipheral with fluoro33
1CHEST 1973;63:889-892
1Am Rev Respir Dis 1974;109:63-66
2CHEST 1974;65:616-619
3CHEST 1976;69:752-757
BIBI 1111
Bronchial brushing:Bronchial brushing:
Complications:Complications: BleedingBleeding PneumothoraxPneumothorax
BIBI 1212
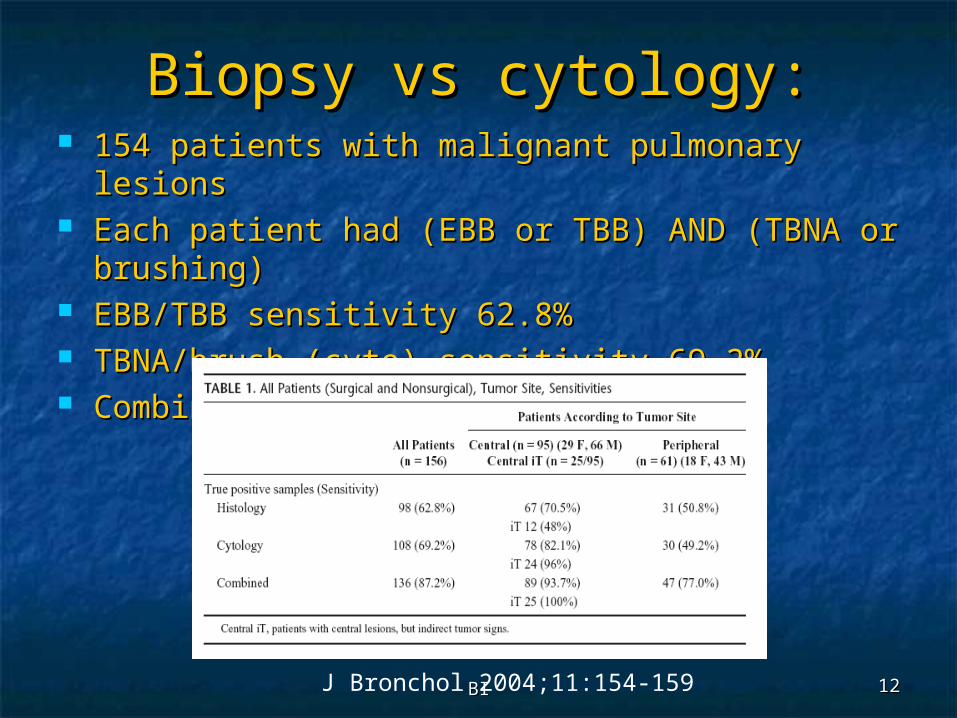
Biopsy vs cytology:Biopsy vs cytology: 154 patients with malignant pulmonary lesions154 patients with malignant pulmonary lesions Each patient had (EBB or TBB) AND (TBNA or Each patient had (EBB or TBB) AND (TBNA or
brushing)brushing) EBB/TBB sensitivity 62.8%EBB/TBB sensitivity 62.8% TBNA/brush (cyto) sensitivity 69.2%TBNA/brush (cyto) sensitivity 69.2% Combined sensitivity 87.2%Combined sensitivity 87.2%
J Bronchol 2004;11:154-159

BIBI 1313
Additional literature:Additional literature:
J Bronchol 2004;11:154-159
BIBI 1414
Endobronchial BrushingEndobronchial Brushing
Brush samples large area of mucosal Brush samples large area of mucosal abnormalityabnormality
May be done under direct May be done under direct visualization, or with fluoroscopic visualization, or with fluoroscopic guidanceguidance
Brushes may be bare of within Brushes may be bare of within a covering sheatha covering sheathBrush Video

BIBI 1515
Indications and brushing Indications and brushing techniquestechniques
IndicationsIndications Visible airway mucosal abnormalityVisible airway mucosal abnormality Peripheral lesion (lung nodule, abcess etc)Peripheral lesion (lung nodule, abcess etc) Peripheral lung infiltratePeripheral lung infiltrate
TechniquesTechniques Extend catheter into target segmentExtend catheter into target segment Extend brush “Brush out”. Be certain extended Extend brush “Brush out”. Be certain extended
brush does not cause pain or pneumothorax, nor brush does not cause pain or pneumothorax, nor push bronchoscope proximally.push bronchoscope proximally.
Brush forcefully and gently and frequently (5-10 Brush forcefully and gently and frequently (5-10 times) with and without brush rotation so that all times) with and without brush rotation so that all parts of brush touch the lesion.parts of brush touch the lesion.
Retract brush “Brush in”.Retract brush “Brush in”. Remove the catheter-brush from the working Remove the catheter-brush from the working
channel.channel.

BIBI 1616
Brushing YieldBrushing Yield Greatest when Greatest when
cancer is cancer is presentpresent 94% in case of 94% in case of
central lesion, central lesion, 78% in case of 78% in case of peripheral peripheral lesions. But lesions. But yields can also yields can also be as low as 20 be as low as 20 % for peripheral % for peripheral lesions.lesions.
Chest 1973;63:889, Chest 1976;69:752, J Bronchol 2004;11:154*
**

BIBI 1717
Brushing-related Brushing-related ComplicationsComplications
BleedingBleeding PneumothoraxPneumothorax Perforation of lung Perforation of lung
abscessabscess
BIBI 1818
Bleeding risk if Bleeding risk if Thrombocytopenia: Thrombocytopenia:
<50,000<50,000 Risk of bleeding: 0-26% (TBBx, post Risk of bleeding: 0-26% (TBBx, post
transfusion) transfusion) (1)(1)
Brushing with mean platelet count of 30,000:Brushing with mean platelet count of 30,000:Bleed: 16% , Death: 4% Bleed: 16% , Death: 4% (2) (2)
What to do? Transfuse 6 packs before & What to do? Transfuse 6 packs before & during bronchoscopy, no need to recheck during bronchoscopy, no need to recheck platelets platelets (3)(3)
Platelet half-life 6 hours!Platelet half-life 6 hours!
(1) Weiss S, Chest, 1993;104:1025(1) Weiss S, Chest, 1993;104:1025(2) Papin T, Chest, 1985; 88:54(2) Papin T, Chest, 1985; 88:54(3)Wahidi M, Respiration 2005;72:285(3)Wahidi M, Respiration 2005;72:285

BIBI 1919
Combined procedures have Combined procedures have greatest greatest
yield for malignancyyield for malignancy Arch Bronchoneumol. 2006;42(6):278-82 75 patients underwent bronchial washing 75 patients underwent bronchial washing
before (pre) and after (post) endobronchial before (pre) and after (post) endobronchial biopsy and brushingbiopsy and brushing

BIBI 2020
This presentation is part of a This presentation is part of a comprehensive curriculum for comprehensive curriculum for
Flexible Bronchoscopy. Our Flexible Bronchoscopy. Our goals are to help health care goals are to help health care
workers become better at what workers become better at what they do, and to decrease the they do, and to decrease the burden of procedure-related burden of procedure-related
training on patients.training on patients.
BIBI 2121
BRONCHATLAS©
Step by Step©
Bronchoscopy.org

BIBI 2222
All efforts are made by Bronchoscopy All efforts are made by Bronchoscopy International to maintain currency of online International to maintain currency of online information. All published multimedia slide information. All published multimedia slide
shows, streaming videos, and essays can be shows, streaming videos, and essays can be cited for reference as:cited for reference as:
Bronchoscopy International: Art of Bronchoscopy, an Bronchoscopy International: Art of Bronchoscopy, an Electronic On-Line Multimedia Slide Presentation. Electronic On-Line Multimedia Slide Presentation. http://www.Bronchoscopy.org/Art of Bronchoscopy/htm. http://www.Bronchoscopy.org/Art of Bronchoscopy/htm. Published 2007 (Please add “Date Accessed”).Published 2007 (Please add “Date Accessed”).
Thank you
BIBI 2323
Prepared with the expert assistance of Udaya Prepared with the expert assistance of Udaya Prakash M.D. (Mayo Clinic, USA), and Atul Mehta Prakash M.D. (Mayo Clinic, USA), and Atul Mehta M.D. (Cleveland Clinic, USA), and Wes Shepherd M.D. (Cleveland Clinic, USA), and Wes Shepherd M.D. (Virginia Commonwealth University, USA)M.D. (Virginia Commonwealth University, USA)
www.bronchoscopy.org