brugada syndrome ecg is highly prevalent in schizophrenia · n e d l e n n e o m a t r n ... c a d...
TRANSCRIPT

DOI: 10.1161/CIRCEP.113.000927
1
Brugada Syndrome ECG Is Highly Prevalent in Schizophrenia
Running title: Blom et al.; Brugada syndrome ECG in schizophrenia
Marieke T. Blom, MA, MSE1; Dan Cohen, MD, PhD2,3; Adrie Seldenrijk, MSc, PhD4,5; Brenda
W.J.H. Penninx, MSc, PhD4,5; Giel Nijpels, MD, PhD6,7; Coen D.A. Stehouwer, MD, PhD8;
Jacqueline M. Dekker, MSc, PhD4,6; Hanno L. Tan, MD, PhD1,9
1Heart Center, 9Department of Cardiology, Academic Medical Center, University of Amsterdam, Amsterdam; 2Department of Community Mental Health, Mental Health Care North Holland
North, Heerhugowaard; 3Department of Epidemiology, University Medical Center Groningen, Groningen; 4Department of Epidemiology and Biostatistics, 5Department of Psychiatry, 6EMGO Institute for Health and Care Research, 7Department of General Practice, VU University Medical
Center, Amsterdam; 8Department of Internal Medicine and Cardiovascular Research Institute Maastricht (CARIM), Maastricht University Medical Centre, Maastricht, the Netherlands
Correspondence:
Hanno L. Tan, MD, PhD
Academic Medical Center
P.O. Box 22660
1100 DD Amsterdam
the Netherlands
Tel: 31-20-5663264
Fax: 31-20-6975458
Email: [email protected]
Journal Subject Codes: [5] Arrhythmias, clinical electrophysiology, drugs, Etiology:[8] Epidemiology
MDMDMD, PhPhPhPhDDDD1,1,1,1,9999
n ed le nn Eo MA tr n
ntttterrrr, 9Departmmem ntnt oooofff f CaCaCaCarddrddioioiolololoogygygyg ,,, AcAcAcadadademmicic MMMMededdediciciccalaa CCCCeneenteteterr,r Unininin vevv rsrsrsitititty y y ofofoff AAAAmmsmsm tedaaaammmm; 2Departmement ooff Coooommmmm unityyy Meennntal HHealtltlth,h,h,h MMMMennntaaal Heaalthhh Careee e NoNoN rtth HoHoHolleerhrhrhhugugugowwowwaaaaaaaarddd; 333Deeeepapapapartmememem ntntnt ooofff f EpEpEpidididemememe ioi lologygygygy, ,,, UnUnUnnivvvererersisisisitytytyt MMMeede icicici alalalal CCCenenene teeer Grronononinn; 4Deeeepap rtmememem nt ooof f f EpEE idemmmmiology and BBBiooostststataaa isticsss,, 5555Departtttmemm nt oooof ff Psycyyy hiatry, 666Eor HeHeHealalala ththth aaandndndd CCCCararree ReReReR sesesearaarchchchch, 77DeDeDeD papapartrrtrtmemeentntnt oooof ff f GeGeGeGenenenerararal ll PrPrPrP acacactititiicececee,, VUVUVUVU UUUUnininiiveveveersrssitititty yyy MAmAmAmstststerererdadadammm;;; 8DeDDeDepapapartrtrtmemementntnt ooofff InInInteteternrnrnalalal MMMedededicicicininineee anananddd CaCaCardrdrddioioiovavavascscsculululararar RRReseseseaeaearcrcrchhh InInInstststricht ((CAAARIRIRIRIM)M)M)M), MaMaMaMaasassastrtrtrricicicichththtt UUUUninninivevevev rsrsrsrsitititityy y y MeMeMeMedidididicacacacalll l CeCeCeCentntntntrererere, MaMaMaMaasasasastrtrtrtricicicchthththt, ttthehehehe NNNNetherlan

DOI: 10.1161/CIRCEP.113.000927
2
Abstract:
Background - The causes of the increased risk of sudden cardiac death (SCD) in schizophrenia
are not resolved. We aimed to establish whether 1) ECG markers of SCD-risk, in particular,
Brugada-ECG pattern, are more prevalent among schizophrenia patients, 2) increased prevalence
of these ECG markers in schizophrenia is explained by confounding factors, notably sodium-
channel blocking medication.
Methods and Results - In a cross-sectional study, we analyzed ECGs of a cohort of 275
schizophrenia patients, along with medication use. We determined whether Brugada-ECG was
present, and assessed standard ECG measures (heart rate, PQ-, QRS- and QT-intervals). We
compared findings with non-schizophrenic individuals of comparable age (NESDA cohort,
N=179), and, to account for assumed increased ageing-rate in schizophrenia, with 20-year older
individuals (Hoorn cohort, n=1168), using multivariate regression models.
Brugada-ECG was significantly more prevalent in the schizophrenia cohort (11.6%) compared
with NESDA controls (1.1%) or Hoorn controls (2.4%). Moreover, schizophrenia patients had
longer QT-intervals (410.9 vs. 393.1 and 401.9 msec, both p<0.05), an increased proportion of
mild or severe QTc-prolongation (13.1% and 5.8% vs. 3.4% and 0.0% [NESDA], vs. 5.1 and
2.8%, [Hoorn]), and higher heart rates (80.8 vs. 61.7 and 68.0 beats per minute, both p<0.05).
Prevalence of Brugada-ECG was still increased (9.6%) when schizophrenia patients without
sodium-channel blocking medication were compared to either control cohort.
Conclusions - Brugada-ECG has increased prevalence among schizophrenia patients. This
association is not explained by use of sodium-channel blocking medication.
Key words: Brugada syndrome, electrocardiography, Schizophrenia
Q )
aaaagegegege ((((NENENENESDSDSDSDA A A A cocococohohohohortrt,,,,
hreniaaaa, ,, , wiwiwiwithththth 22220-0-0-0-yeyeyeyeararaa o
s
C a
D h
-intervals (410.9 vs. 393.1 and 401.9 msec, both p<0.05), an increased proportion
v n
orn]), and higher heart rates (80.8 vs. 61.7 and 68.0 beats per minute, both p<0.0
s (HHHoooooooornrrn ccccohohoho orororrtt,tt n=1168), using multivararariaiaiai tte regression nn moooodddels.
CCCCGGG G was signnnifififi iccanananntltly yy y momomomorrer prprprp eveveve allent tt iiin thehe schchchchiiizi opopopo hrhrhrennniaiaia cccoohorororort t t (1(1(1(11.1.1 6%6%6%%) cocococommpmm a
DAAAA cccontrols s s s (1.11%))) oor HoHoHooroo n coccc ntntntror lsss ((((2.4%4%)... MMMoooro eeoveveveer,r schchizopopopophrennnniaiaia ppaatientntnts h
-interrrvavvv ls ((4141414 0.9 99 vsvsvs. 393..3.111 and 401.9 9 9 msmsmssecececec, both ppp<0.05))),, ananan increreereasededede pppropopp rtion
vere QQQTTcT -ppprolololoongggatiioi n (1(1(13.333 1%1%1%% anddd 5555 88.8% %%% vs. 33.3 4%4%4%4% andddd 0000 0.00%% % [N[N[N[NESESESE DADADAD ],],], vvvvsss.s 555.1 an
oornrn])]), , anand ddd hihihih ghghhherer hhhheaaearttrtt rratateses ((((8080808 .8.88 vvs.s. 66661.1.11 7 77 7 anand dd d 68686868.00.00 bbbbeaeatsttts pperer mmininii ututtte,e, bbbbototh h p<p 0.0.00
DOI: 10.1161/CIRCEP.113.000927
3
Introduction
Patients with severe mental illness have a 14-32 years reduced life expectancy1. Schizophrenia is
associated with increased standardized mortality ratios for all-cause death2, cardiovascular
death3, and sudden cardiac death (SCD)4. The causes for SCD-risk in schizophrenia are
unresolved5. SCD is mostly caused by lethal cardiac arrhythmias resulting from disrupted cardiac
electrophysiology (depolarization and/or repolarization)6. Many researchers ascribe SCD in
schizophrenia to antipsychotics, as antipsychotics may cause such disruptions7. For instance,
increased SCD-risk during use of first-generation antipsychotics (FGA) or second-generation
antipsychotics (SGA) is commonly ascribed to their repolarization-blocking effects, signaled by
QTc-prolongation8,9. However, individual susceptibility is crucial. Co-morbidities that increase
susceptibility may be acquired, e.g., cardiovascular disease; such conditions are more prevalent
among schizophrenic individuals3. The possibility that inherited factors are also relevant has so
far received less recognition.
These considerations prompted us to conduct the present study. We systematically
compared ECGs of a cohort of schizophrenia patients to ECGs of two cohorts of non-
schizophrenia control subjects, and took co-variates for ECG abnormalities into account. Our
primary aim was to establish whether ECG markers of SCD-risk are more prevalent in
schizophrenia patients than in non-schizophrenic controls. This included the Brugada ECG
pattern (Brugada-ECG) and QTc duration. Our secondary aim was to study whether differences
in prevalence of these ECG markers may be explained by use of sodium-channel blockers or
QTc-prolonging drugs and/or presence of cardiovascular risk factors.
A) ) or second-geg neerarararatititt o
ockinng g g efefffffeffe tcttcts,s, ssigigignanananalele
n 8 9 r
i a
i a
d
ese considerations prompted s to cond ct the present st d We s stematicall
ngggatatatatioioioi nnn8,8,8,999.... HoHoHowweww ver, individual susceptibibibibililililiity is cruciall. Coooo-mmmom rbidities that incr
itttyt may be acququirededed, e.gg.g , cardrdrddiooovasculullar ddiiseaaaseseee;;; suuchhh conddiitioooonns areeee mmmorore prrreeeva
izophphphhrerereninininic indididi iiviiduddd llals3. ThThThTheee posssibibibibiliililittitity y thththt tttat inhnhnhnheritititi eedede fffacacaca tottt rs are aaaalslslslso relell vanttt hhhha
d less recogngg ititittioioioion.
e isidde titi tpt ded tto dd tct tthhe tnt tt dd WW tst tatiic lalll
DOI: 10.1161/CIRCEP.113.000927
4
Methods
Schizophrenia cohort
In a cross-sectional study, all outpatients at the Department of Severe Mental Illness, Mental
Health Care Center-North Holland North (n=603), typically in psychiatric care for >10 years,
were asked to participate in yearly metabolic screening in February 2008 - January 2011. Among
387 patients who agreed to participate, 275 with DSM-IV classification 295.xx (schizophrenia,
schizoaffective disorder, schizophreniform disorder) were included in the study cohort
(Schizophrenia cohort). This study was conducted according to the principles expressed in the
Declaration of Helsinki. Written informed consent was obtained from all participants who
underwent ajmaline testing10. The Ethics Committee of the Academic Medical Center approved
this study.
Control cohorts
We compared the patients of the Schizophrenia cohort with age-comparable control persons from
the Netherlands Study of Depression and Anxiety (NESDA), an ongoing longitudinal cohort
study in the Netherlands11. We used data from 179 individuals, selected randomly from a large
sample of control volunteers in the NESDA study without psychiatric disorder, of whom ECG
and cardiovascular measurements were made (cardiovascular subsample)12.
Since several studies suggested that schizophrenic patients have higher biologic age
relative to their calendar age with commensurately increased prevalence of cardiovascular and
metabolic disorders13,14, we studied a second control cohort ~20 years older than the study
cohort: the Hoorn Study cohort, in which participants, selected randomly from the population
registry of the town of Hoorn, have been followed since 1989 15. After excluding 7 participants
nciplp es exppressedddd iiiin nnn
all pparar itititiciiicipapanttnttss whwhwhwhoooo
10
r n
lands St d of Depression and An iet (NESDA) an ongoing longit dinal coho
ajmamamamalilililinenenee tttesee tiiingngngn 10. The Ethics Committeeeeee oof the Academee iccc MMMMedical Center appr
horttttss
red hthhe papp tiiiennntstststs of ff thhhe ScSS hihihihizophphphreniiia cohhhort witiithhh h aggge-cocooomppparararr babbbllel controlololol pppperererrson
lla dnd StSt dd fof DD iio dd AAn ii tet (N(NESESDADA)) iin llo itit ddiin lal hoh
DOI: 10.1161/CIRCEP.113.000927
5
whose medication data were missing, and 4 participants who used antipsychotics, we studied
ECGs of 1168 participants (Hoorn cohort).
ECG analysis
To ensure consistent classification, all ECGs were analyzed by one cardiologist (HLT), who was
blinded to cohort status. Brugada-ECG was defined as type-1 or type-2/3 Brugada-ECG
according to the Brugada Syndrome (BrS) consensus criteria (Figure 1)10. Prolongation of QTc-
interval (Bazett rate correction) was defined as mild (male 431-450 msec, female 451-470 msec)
or severe (male >450 msec, female >470 msec)16.
Brugada-ECG and Brugada Syndrome
The diagnosis BrS requires typical ST-segment elevations in right precordial ECG leads (type-1
Brugada-ECG) and events suggestive of cardiac arrhythmia or a family history of BrS or SCD.
In most BrS patients, the baseline ECG is only suspicious for BrS (type-2/3 Brugada-ECG). To
confirm or refute this suspicion, they must undergo provocation testing with a sodium channel-
blocking drug (Figure 1)10. Accordingly, schizophrenia patients with baseline type-2/3 Brugada-
ECG were invited for ajmaline testing in the Academic Medical Center. All patients with type-1
Brugada-ECG (at baseline or after ajmaline testing) underwent DNA screening of SCN5A17.
SCN5A encodes -subunit of the cardiac sodium-channel18 which drives depolarization.
Moreover, family screening was offered. In the NESDA and Hoorn cohorts, ajmaline testing
could not be performed. Therefore, the prevalences of baseline Brugada-ECG (type-1 or type-
2/3) were compared between cohorts.
Confounders
Risk factors for cardiovascular disease and SCD (previous myocardial infarction, hypertension,
hypercholesterolemia, diabetes mellitus, body mass index) were derived from patient files
o y
C
S )
refute this suspicion, they must undergo provocation testing with a sodium chan
r g (Fig re 1)10 Accordingl schi ophrenia patients ith baseline t pe 2/3 Br
osis s s s BrBrBB SSS rererer quqq irrreesee typical ST-segment elevevevatations in righttt prececececordial ECG leads (ty
CCCCGGGG) and evenntss suguugggestttivivivve ofofoff caaarddiacc aarrhyhythmimimim a a a a orr aaa fffamilyy hihihiiststtory ofofof BBrrS ooor S
S patitititienenentstststs, thhhhe bbbaseliililine EEEECGCGCGCG is onnnnlylylyly sssuspipii iiciiouousss fffof r rr BBBrB SSSS (t(t(t( ypype-2/3333 BrBrBrBruggaddda-ECECECECGGGG)
reffffute hhthiisi susususspipipipi iicion, hhtheyyy must undeddd rgggo prpp ovocattioii n teeeestinii g g g iiwii hthh a s ddoddiuiuiuium mmm chccc an
(F(Fiig 1)1)101010 AAc drdiin lgl hchii hhr iia tatiie tnt iithth bb leliin tt 22/3/3 BB
DOI: 10.1161/CIRCEP.113.000927
6
(Schizophrenia cohort) or from medication use and patient files (control cohorts)12,15. Drug use
during ECG recording or ajmaline testing was derived from patient records (Schizophrenia
cohort), questionnaire (Hoorn cohort), or drug container inspection (NESDA cohort). We
assessed use of sodium-channel blockers19, QTc-prolonging drugs20, FGA, SGA, antidepressants,
cardiovascular drugs (nitrates, -blockers, calcium channel antagonists, antithrombotics), and
lipid lowering drugs.
Statistical analysis
To analyze differences between cohorts in prevalence of co-morbidities and medication use, we
used 2 statistics (Pearson/Fisher Exact where appropriate) for categorical variables and analyses
of variance for continuous variables. We performed multivariate logistic regression analyses to
assess differences between cohorts in Brugada-ECG, correcting for sex and factors that were
significantly (p<0.05) different between cohorts. Multivariate linear and logistic regression
analyses were performed to investigate differences in quantitative ECG parameters, correcting
for sex and factors that were significantly (p<0.05) different between cohorts. To evaluate the
association between sodium-channel blocker use and ECG outcomes, we compared
schizophrenic patients with or without sodium-channel blockers, and performed separate
analyses with patients from the Schizophrenia cohort who used no sodium-channel blockers
during ECG recording, employing the statistical methods described above. All statistics were
performed in SPSS (version 20.0 for Mac, Chicago IL, USA).
Results
Cohort characteristics
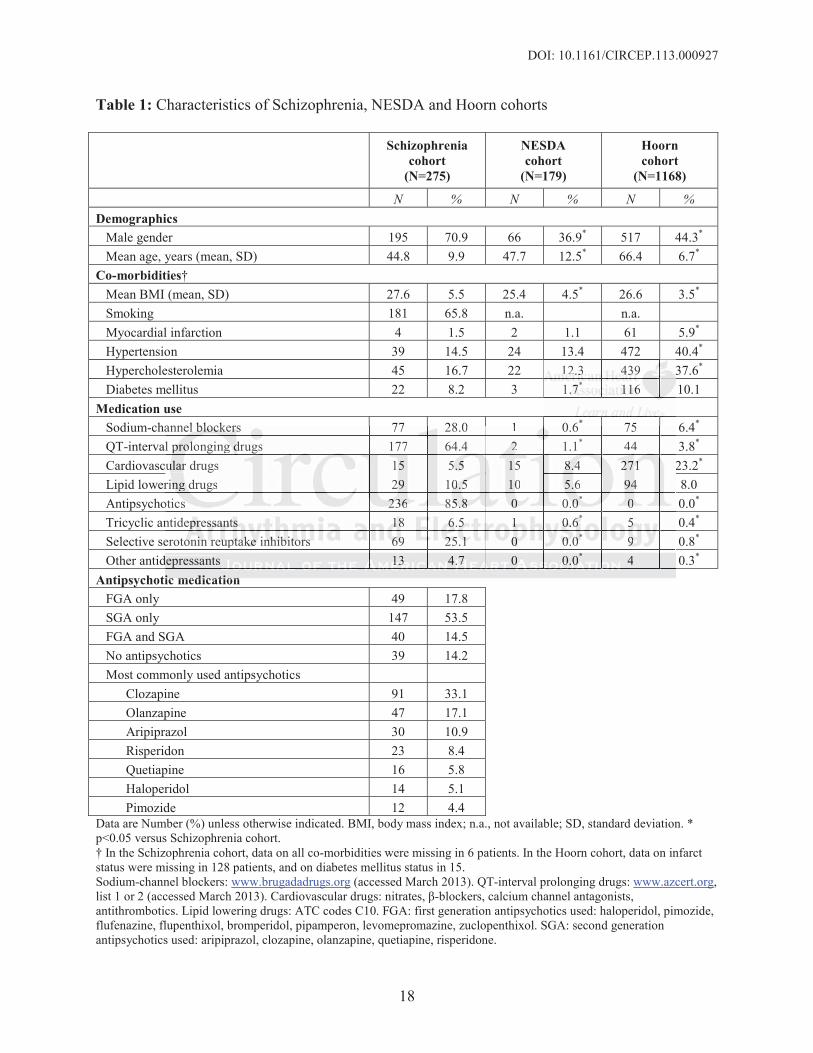
Table 1 shows patient characteristics. Compared with NESDA controls, schizophrenia patients
were slightly younger and more often male. They had higher body mass index (27.6 vs. 25.4, p
es and medication n usususu e
ricall vavariiri bbabablelell ss anand ddd anan
e for continuous variables. We erformed multivariate logistic r ression anal e
e r
ly <0.0 different between cohorts. Multivariate linear and lo stic regression
ere performed to investigate differences in quantitative ECG parameters, correct
d f h i ifi l ( 0 05) diff b h T l
e fofoforr rr cococc ntnttininini uuousususus variables. We performedddd mmultivariate loll giststststiici regression analyse
errrer nnncn es betweenen cohoohortsss iiin BrBB ugggada-ECGG, correreerectctctctinng fooor seexx annnddd facttttooro s thhat wwwer
ly (pp<0<0<0 000.05)5)5) dddififfferent bbetween cohhortsts. MuMuM ltltiiivariiai te llinear andd logigigi tsticic regressiion
ere pepp rformed ddd to investigagg te differences in quqq antitativee ECGGG ppparameters,s,s, ccccorororrect
d f h i ifi l ( 0 05) diff b h T l
DOI: 10.1161/CIRCEP.113.000927
7
<0.05), higher prevalence of diabetes mellitus (8.0 vs. 1.7%, p<0.05) and a trend towards higher
lipid lowering drug use (10.5 vs. 5.6% p=0.07). Antidepressants use was significantly more
frequent among schizophrenia patients (tricyclic antidepressants: 6.5%, selective serotonin
receptor inhibitors: 25.1%, other antidepressants: 4.7%); one participant of the NESDA cohort
used low-dose amitriptyline (10 mg OD) for neuralgy. Higher antidepressants and antipsychotics
use caused higher use of sodium-channel blockers (28.0 vs. 0.6%) and QTc-prolonging drugs
(64.4 vs. 1.1%).
Compared with Hoorn controls, schizophrenia patients were more often male and ~20
years younger (by design). Prevalence of diabetes mellitus was comparable (8.2 vs. 10.1%), but
schizophrenia patients had lower prevalence of previous myocardial infarction, hypertension, and
hypercholesterolemia (1.5, 14.2, and 16.7% vs. 5.9, 40.4, and 37.6%, all p<0.05). Accordingly,
they used less often cardiovascular drugs (5.5 vs. 23.2%, p<0.05), but had comparable use of
lipid lowering drugs. They used antidepressants more often than Hoorn controls (TCA: 6.5
vs.0.4%; SSRI: 25.1 vs 0.8%, other: 4.7 vs. 0.3%, all p<0.05). Antipsychotics were only used by
schizophrenia patients. FGAs were used by 18%, SGAs by 54%, and both SGAs and FGAs by
15%; 14% used no antipsychotics. Sodium-channel blockers and QTc-prolonging drugs were
used more frequently by schizophrenia patients (28.0 vs. 6.4% and 64.4 vs. 3.8%).
Brugada-ECG in schizophrenia cohort
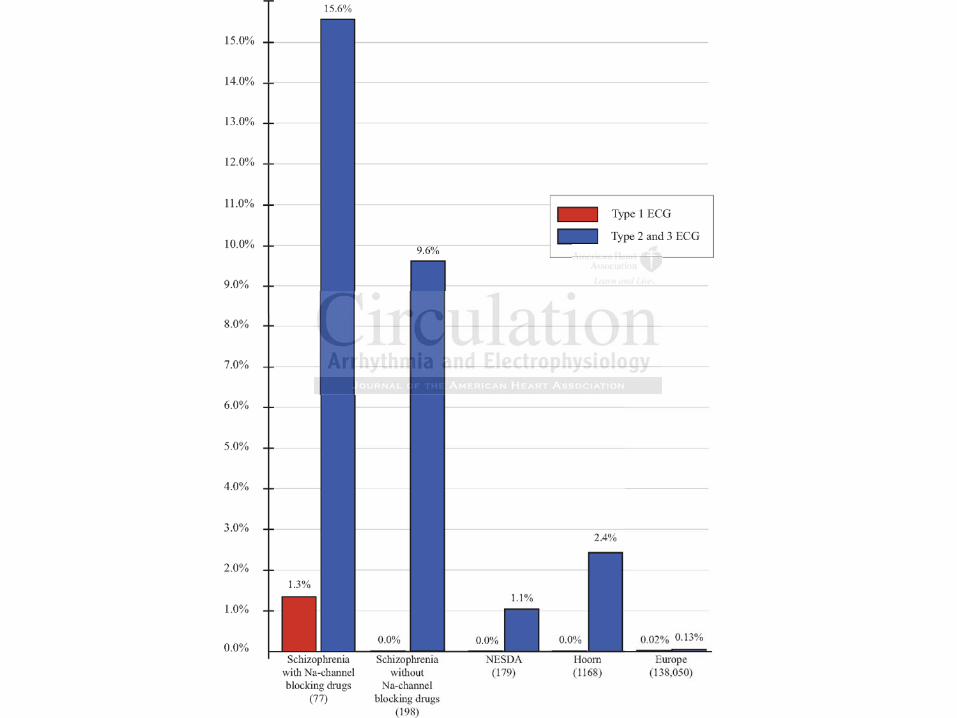
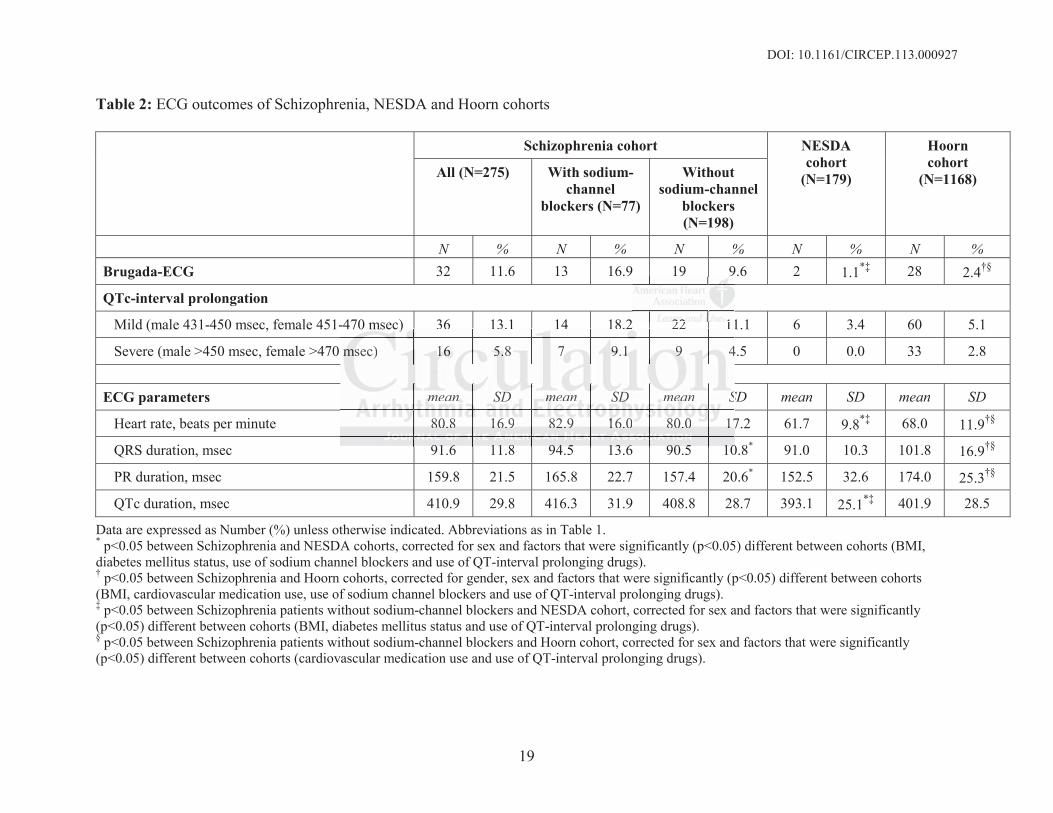
In the Schizophrenia cohort, 32 patients (11.6%) had Brugada-ECG at baseline: one had type-1
Brugada-ECG, while 31 had type-2/3 Brugada-ECG (Table 2). This was significantly more than
among NESDA or Hoorn controls, where no patient had type-1 Brugada-ECGs, while 2 (1.1%)
and 28 (2.4%, both p<0.05 vs. Schizophrenia cohort), respectively, had type-2/3 Brugada-ECG.
Figure 2 shows Brugada-ECG prevalences in the study cohorts, and reported prevalences21. In
ore often male andnddd ~~~
arablee ((((88.88 2222 vsvs. 110101 .1.111%)%%%)
nia patients had lower prevalence of previous myocardial infarction, hypertensio
esterolemia 1.5, 14.2, and 16.7% vs. 5.9, 40.4, and 37.6%, all p<0.0 . Accordin
ess often cardiovascular drugs (5.5 vs. 23.2%, p<0.05), but had comparable use
r
SRI: 25 1 s 0 8% other: 4 7 s 0 3% all p<0 05) Antips chotics ere onl s
nia a a a papapapatititit enenenntststs hadadadd lower prevalence of preeevivivivioous myocardidd al iiinfnfnfarction, hypertensio
esssts eeere olemia (1..5, 1444.222, aaandndndnd 16.666 7%7%7% vs. 555.9, 40.4444, anananand 3777.666%, alll ppp<<0< .05)5)55 ... AcAccordrdrdin
ess ooftftfftennenen cardididid ovascular drdrdrdruuugs (5555 55.55 vvvsss. 22223.33 2%2%2%2%, p<p<p<p<0.000 00050 )))), bbbuttt hhhhad comomomompap rablblblle use
ring gg ddrd ugggs. TTTheheheey yy us dedd antidididdepppressantts more offften hththan HHHHoornnn controls (T(T(T(TCACACACA::: 6.5
SRSRII: 2255 11 00 88%% thth 44 77 00 3%3% lalll <p<00 0505)) AA tntiip hch totiic lnl
DOI: 10.1161/CIRCEP.113.000927
8
the Schizophrenia cohort, ajmaline testing was offered to the 31 patients with type-2/3 Brugada-
ECG, accepted by 23, and found positive in 10. Thus, at least 11 patients had type-1 Brugada-
ECG at baseline or after ajmaline testing (4% of all schizophrenia patients, 6 men, age 48.1±10.2
years). One patient had a mutation in SCN5A (c.3956G>T). Family screening was offered to all
11 patients with type-1 Brugada-ECG, but only conducted in 5 relatives of 4 patients, because
other relatives were unavailable or declined investigation; no investigated relatives had Brugada-
ECG. Supplemental Table 1 shows ECG parameters, co-morbidities, and medication use of all
patients with type-1 Brugada-ECG. Four schizophrenia patients with type-2/3 Brugada-ECG
who declined ajmaline testing provided additional medical and family history; none had suffered
syncope, dizziness or palpitations. No SCD at age <45 years had occurred in the family, and no
family members suffered from schizophrenia.
Analysis of QTc-interval and other ECG variables
Compared to NESDA controls, schizophrenia patients had higher heart rate (80.8 vs. 61.7 beats
per minute, p<0.05) and longer QTc-interval (410.9 vs. 393.1 msec, p<0.05). They also had
higher proportion of mild or severe QTc-prolongation (13.1% and 5.8% vs. 3.4% and 0.0%), but
not when corrected for relevant covariates (BMI, diabetes mellitus status, use of sodium-channel
blockers or QTc-prolonging drugs). Compared to Hoorn controls, schizophrenia patients had
higher heart rate (80.8 vs. 68.0 beats per minute, p<0.05), but shorter QRS-interval (91.6 vs.
101.8 msec, p<0.05) and PR-interval (159.8 vs. 174.0 msec, p<0.05). QTc-interval was not
different (410.9 vs. 401.9 msec, p=0.251). The proportion of mild or severe QTc-prolongation
was higher in the schizophrenia cohort (13.1% and 5.8% vs. 5.1 and 2.8%), but not significantly
different when corrected for relevant covariates (BMI, cardiovascular medication use, use of
sodium-channel blockers or QTc-prolonging drugs).
ypype-2/3 Bruggada-ECECECECG
histooryry;; nononene hhhhadaddd ssssufuf
izziness or palpitations. No SCD at age <45 years had occurred in the family, an
m
f
to NESDA controls, schizophrenia patients had higher heart rate (80.8 vs. 61.7 b
p<0 05) and longer QTc inter al (410 9 s 393 1 msec p<0 05) The also had
izzizizinenenenesssss oooorr r papaalplplpitations. No SCD at age <4<4<455 years had ocoo cuuuurrrrrrr ed in the family, an
mmmmbeeeers sufferedd ffrommm schhhizizizzophrhrhrh ennniaa.
f QTTTTccc i-intntnttervalll and dd ttother ECECECECG vaaaaririririabababbllell s
to NENENEN SDSDSDAA A cooontntntn rolsll , schihihizophphphreniiia papp tiients hhhh daddd hhhhigigighehh r r heheheh arrt tt rratte (((8080808 88.8 vs.sss 666111.1 7 b
<p<00 0505)) dd llo QQTTc ii tnt ll (4(41010 99 339393 11 <0<0 005)5) ThTh lls hhadd
DOI: 10.1161/CIRCEP.113.000927
9
Effects of sodium-channel blockers on ECG parameters
To study whether use of sodium-channel blockers affected prevalence of Brugada-ECG and ECG
parameters in schizophrenia, we compared schizophrenia patients who used sodium-channel
blockers (n=77) to those who did not (n=198) (Table 2). The groups differed in PR and QRS
duration (165.8 vs. 157.4 and 94.5 vs. 90.5 msec, both p<0.05), but were otherwise similar.
Prevalence of Brugada-ECG was not different (16.9 vs. 9.6%, p=0.091).
To study whether ECG differences between the Schizophrenia and control cohorts may
be attributed to use of sodium-channel blockers, we compared ECG parameters between
schizophrenia patients who used no sodium-channel blockers with both control cohorts.
Compared with NESDA controls, this schizophrenia subset had more Brugada-ECG (9.6 vs
1.1%, p<0.05), higher heart rate (80.0 vs. 61.7, p<0.05), and longer QTc-duration (408.8 vs.
393.1, p<0.05). Mild or severe QTc-prolongation was more prevalent in this schizophrenia
subset (11.1 and 4.5% vs. 3.4 and 0.0%, p<0.05), but not significantly when corrected for
relevant covariates (sex, BMI, QT-prolonging drugs and diabetes).
Similarly, compared with Hoorn controls, this schizophrenia subset had higher
prevalence of Brugada-ECG (9.6 vs. 2.4%, p<0.05), higher heart rate, and shorter QRS- and PR-
interval. Mild or severe QTc-prolongation was more prevalent in this schizophrenia subset (11.1
and 4.5% vs. 5.1 and 2.8%, p<0.05), but not significantly when corrected for relevant covariates
(sex, BMI, QT-prolonging drugs and diabetes).
Discussion
We found that Brugada-ECG has higher prevalence in schizophrenia patients than in similarly
aged or ~20 years older non-schizophrenic controls. Importantly, the prevalence was also
significantly increased in schizophrenia patients who used no sodium-channel blocking drugs
arameters betweennnn
h cononttrtrt olllol ccohohhhorortss.
s
s
o ariates (se BMI QT prolonging dr gs and diabetes)
wiiiththhth NNNNESESESSDADADA ccccontrols, this schizophrennniaiaiaia ssubset had momm reee BBBBrugada-ECG (9.6 v
00050 ))),) higher heearrt raatttte (8080800.0 vvss. 6661.7, p<<0.055), anannnddd d longeeer QQTTc-dd-dduuratioiooonn n ((4008.8 vs
.05))). MiMiMiMildldldld or severe QQQQTc-ppprrorolongggatatata ioiioion was momomorererere ppprrrrevaaalelelelenttt iiin thisisiss sssschchhhizophhhrh eniiiia
1 anddd 444.555%%% vsvsvss. 3.333 444 anddd 0.00 0%0%0%0 , p<pp 00.0 05050505),),), bbbbut not sigigignififificaaaantntntn lylyly wwwwhehhh n correcteteteteddd d fofff r
iiatte ((s BMBMII QQTT llo iin ddr dd didi bab tet ))
DOI: 10.1161/CIRCEP.113.000927
10
(notably antipsychotics). In contrast, while we also found, in accordance with previous
studies7,22,23, that schizophrenia is associated with QTc-prolongation, QTc-prolongation was
largely explained by confounding factors, including use of QTc-prolonging (antipsychotics)
drugs.
Schizophrenia and Brugada-ECG
As many as 4% of schizophrenia patients had type-1 Brugada-ECG compared to an estimated
prevalence in the general population of 0.05%21. This suggests a higher prevalence of BrS in
schizophrenia. This could partly explain the increased SCD risk in schizophrenia. Indeed, the
yearly SCD incidence in our Schizophrenia cohort (19/8561 patient years = 0.2%, not shown) is
higher than the incidence in the general population in the Netherlands (0.1%)24. Schizophrenia
patients with BrS would be vulnerable to the arrhythmia-causing effects of sodium-channel
blocking medication, which include many antipsychotics25, particularly in combination with the
increased prevalence of cardiovascular risk factors that increase SCD-risk. Still, it must be noted
that type-1 Brugada-ECG per se is not sufficient for the diagnosis BrS if associated signs are
absent. We did not find such signs in the Schizophrenia cohort. However, these signs are difficult
to ascertain or obtain in schizophrenia patients. For instance, unexplained syncope (a presumed
symptom of cardiac arrhythmias in BrS) is non-specific in these patients, often resulting from the
blood pressure lowering effects of antipsychotics. Moreover, we had little opportunity to obtain a
family history, as most patients had sparse contact with their relatives, and most available
relatives declined investigation. Therefore, although the association between schizophrenia and
Brugada-ECG suggested that BrS is more prevalent in schizophrenia, we could not prove this. It
could be argued that use of antipsychotics may provoke a Brugada-ECG, thereby facilitating
easier detection by ECG analysis. This may especially apply to sodium-channel blockers25, 26.
hizopphrenia. Indeededdd,, , , tht
ears == 0000.2%2%2%2%, nonot t shshshshooowow
n 24 e
l
m t
p
Br gada ECG is not s fficient for the diagnosis BrS if associated signs a
n thhhee ee ininininciciciidedededennce ee e inii the general population nn ininini the Netherlanaa dsss (((0.1%)24. Schizophre
thhh h BBBrB S would be vvulululnerararabblbb e tottto thehhe arrrhhhythhmmiaa c-cauauauausiinggg eeeffecctts ooof f f sodidiiiumumm-ccchannnnnnel
medicatataatioioioionn, whihihih hhchh iiiinclull de mmmmany anannntitititipspspsycchohh titititicss252552 , papapaparticicculululu arllly iiiin cocooombmbmbmbin ttatiiion iiwit
prpp ev lallence offf caccc rddddiiiovascullllar risiii kkk ffaf cttors hhthat iiincrease SCSCCCDDD-riririri kkskk. SSStilililill,l iiit t mumumumustststt be
BBr dad ECECGG ii tt ffffiiciie tnt ff tthhe ddiia iis BB SrS iiff ici tat ded iig
DOI: 10.1161/CIRCEP.113.000927
11
Still, >50% of patients with Brugada-ECG used no sodium-channel blockers (Supplemental
Table 1), and differences remained significant when correcting for and stratifying according to
use of sodium-channel blockers. Furthermore, it is unlikely that use of sodium-channel blockers
alone results in Brugada-ECG when an innate factor is absent27. Therefore, the high prevalence
of Brugada-ECG found here can probably not be solely attributed to use of sodium-channel
blocking antipsychotics.
Future studies are required to establish the causes for the increased prevalence of
Brugada-ECG (or BrS) in schizophrenia. Emerging evidence indicates that schizophrenia and
acute psychosis may impact on cardiac electrophysiology22. Accordingly, genetic studies suggest
that the pathobiology of schizophrenia involves various voltage-gated ion channels28-30. Because
these proteins also control cardiac electrophysiology, variants in their encoding genes (KCNH2,
CACNA1C) may increase arrhythmia and SCD-risk. We did not screen KCNH2, CACNA1C in
the patients with Brugada-ECG, but only SCN5A, because SCN5A is the only gene routinely
screened at our institution in BrS patients17. Nevertheless, our observations lend support to the
more general notion that (nonstructural) brain disease and (electrical) heart disease share
common underlying pathomechanisms. For instance, in epilepsy, too, the increased incidence of
SCD31 may stem from expression of the same (mutant) ion channel in brain and heart32,33.
Furthermore, a recent study34 showed that Neuregulin1, related with both epilepsy and
schizophrenia, is also associated with SCD. Autonomic dysregulation may also explain the
association between BrS and schizophrenia, being reported in both conditions. However, while
reduced vagal tone exists in schizophrenia patients (including those not using antipsychotics)35
increased vagal tone may unmask Brugada-ECG and cause SCD in BrS26.
s that schizophp reniniiia a a a aa
gly, ggenenettetticicii ssttutut didiidieseseses ssu
t 28 30
N
C C
s
t o r instit tion in BrS patients17 Ne ertheless o r obser ations lend s pport to
thooobibiibiolololologogggy y y ofofof sssschcc izophrenia involves vaaririririouus voltage-gaggg ted ddd ioii n channels28-30. Be
insnsnsns also controoll cardrdrdiac eleee ectrtttrophyhhysioologyy, varrriaiaiantntntntss innn tthheirr eencccodoo ing g g ggeg nenes (KCKCKCN(
C) may y y inininincrease arrhhhyhythtt miiiiaaa a aaand CC SCSCSCSCDDDD- iiriri kkskk. WWWeW ddddidididi nnnnoot ssscrcrcrc een KCKCKCK NHNHNHNH222, CCCCACACACCNANANAN 111C1
s witiii h hh BrBB ugggadadadaaaa-EEEECGCGCG, bbbut onlylyly SCSCSCN5N5N5N5AAA, bebb cause SCSCSCS N5N5N55AA iiis thehehee o lnlly yy gegg ne rorororoututututiiini el
tt o ii tititt titi ii BBrSS titi tts171717 NNe trthhelle bob tatiio ll dd tt tto
DOI: 10.1161/CIRCEP.113.000927
12
Schizophrenia and sudden cardiac death risk
If proven in future studies that increased prevalence of Brugada-ECG in schizophrenia reflects
increased prevalence of BrS, this finding could contribute to a better understanding of excess
SCD-risk in schizophrenia patients, especially those using (antipsychotic or non-antipsychotic)
medication that blocks cardiac depolarization. The risk for lethal cardiac arrhythmias in BrS is
mediated by dysfunctional (impaired) depolarizing ion channels, notably, the cardiac sodium-
channel. BrS-patients, through their innately impaired cardiac sodium-channels (reduced
depolarization reserve), are particularly vulnerable to additional sodium-channel block exerted
by some antipsychotics (and other drugs). BrS-patients may also be more vulnerable to the
depolarization-blocking effects of concomitant conditions36. In particular, acute myocardial
ischemia/infarction (more likely to occur in schizophrenic patients, given their higher prevalence
of diabetes) impairs cardiac depolarization37. BrS-patients may have particularly increased risk to
suffer lethal cardiac arrhythmias during acute myocardial ischemia/infarction. Thus, the
combined effects of higher prevalence of Brugada-ECG and concomitant factors that impair
cardiac depolarization such as drug use or (risk factors for) ischemic heart disease may partly
explain the increased incidence of SCD in schizophrenia.
Similarly, we found increased prevalence of QTc-prolongation in schizophrenia patients.
While mostly mild and not hazardous per se, this QTc-prolongation may identify individuals at
increased risk for lethal cardiac arrhythmias and SCD if concomitant factors that cause further
QTc-prolongation (e.g., cardiac hypertrophy or heart failure caused by hypertension or heart
disease) are also present. However, QTc-prolongation observed in schizophrenia patients was
largely explained by confounding factors, suggesting that QTc-prolongation is not strongly
associated with schizophrenia per se, in contrast with the occurrence of Brugada-ECG. We used
m-channel block exexexexere
ore vuvullnlnl ererababbbllelle tto ththththee
t 36 l
n a
a
effects of higher pre alence of Br gada ECG and concomitant factors that impai
tionnnn-b-b-bblololoockckckckininining efefefffects of concomitant connndidididitit ons36. In paraa ticucucuulall r, acute myocardia
nffffarrrrction (morre likkkellly too o oooccuurr innn schhizzzophrhrennicicici ppppatatata ienntntsss, giivenenn thheh ir hhhhiigi heher prerereva
) imppppaiiaiairssrsrs cardididid ac ddddepolarizizizzattatation3737373 . BrBrBrB SSSS-papatititiientstststs mayyayay hhhhavavavave pa tttrticululululararararlllyly iincreas ddded
al cardddiiai c arrhrhrhytytyty hmhhh iiai s dudd iriiinggg acute myoyy carddddiiiall iiisi hhchemiaiaaa/i/i/infnfnfararararcttiioi n. TTThuhh s,sss tttthehehee
ffff tts ff hihi hgh lle fof BB dda EECGCG dnd itit tt ffa tct thth tat ii iai
DOI: 10.1161/CIRCEP.113.000927
13
Bazett’s formula for heart rate correction, since this method is most widely employed and allows
for easy comparison with other studies. Although Bazett’s formula may overestimate QTc-
duration at higher heart rates when compared to other rate correction methods, it is not resolved
which method best captures co-variates of QT duration38.
Strengths and Limitations
A major strength of our study is that it involved a large group of schizophrenia patients with data
on medication use and relevant co-morbidities during ECG recording. While it is difficult to
gather these data in patients with severe mental illness, the newly introduced yearly
cardiovascular screening among schizophrenic patients enabled us to perform this study.
Moreover, we compared our findings with two well-defined control cohorts.
Our study has some limitations. We were unable to perform ajmaline testing in both
control cohorts, and 8 schizophrenia patients declined ajmaline testing. Furthermore, data on
family history of SCD in the Schizophrenia cohort was limited due to disturbed family relations,
precluding a firm diagnosis of BrS. Clinical implications of type-2/3 Brugada-ECG are not well-
defined. Nonetheless, the difference in prevalence of type-2/3 Brugada-ECG seems sufficient to
warrant further research (e.g., replication of our findings in a separate cohort of schizophrenia
patients) and prudence with drug prescription.
Conclusion
We found a strongly elevated prevalence of Brugada-ECG in schizophrenia patients. Further
studies are required to elucidate whether this increased prevalence reflects an association of BrS
and schizophrenia, and the underlying causes. If confirmed, our findings warrant ECG recording
as part of periodic cardiovascular screening in schizophrenia patients, and prudent prescription of
sodium-channel blockers, to minimize SCD-risk39.
oduced yyearly y
perfororm m ththththisisii sstuttut dydyydy..
r h
h o
o a
a firm diagnosis of BrS Clinical implications of t pe 2/3 Br gada ECG are not
weee cccommomompapapaparrer d dd oouoo r findings with two welllllll -d-dddefined contrrrol cccohohohorts.
r stutuuudy has somem limimimitatttioioioons. WWWWeee wwerre unabble totooo ppppeerfooormmm ajmjmallllininine testststs inii gg in bbboooth
horts,, aaandndndnd 88 schhhiiizopophhhhrenia ppppaatientttssss dededede lclclliineddd ajmamamamalililiinenenene tesesessttttiiing. FFFFurththththererere more, daddd ttta o
oryyy offf SCSCSCD DD inininn thehhh SSSchhhizii oppphhrhh eniiia cohhhhort was lllimitiited ddddueueee to didididistturbbeb dd d faff mimimim lylylyl relad
fifi didi isi fof BB SrS ClCliiniic lal ii lili titi fof tt 22//33 BBr dad ECECGG tt

DOI: 10.1161/CIRCEP.113.000927
14
Acknowledgments: The authors wish to express their gratitude to Jan Peetoom, internist, who performed the initial ECG analysis in the schizophrenia cohort, Remco Boerman, nurse practitioner, who recorded all ECGs in the schizophrenia cohort, and Irene Beems, who contributed to data collection. The authors greatly appreciate the contributions of Paulien Homma and Loes Bekkers for data collection and data entry, Julien Barc and Leander Beekman for DNA analysis, and thank Patrick Souverein for his help in analyzing medication data.
Funding Sources: Dr. Tan was supported by the Netherlands Organization for Scientific Research (NWO, grant ZonMW Vici 918.86.616), the Dutch Medicines Evaluation Board (MEB/CBG), the European Community's Seventh Framework Programme (FP7, grant 241679, ARITMO), and Biobanking and Biomolecular Research Infrastructure The Netherlands (BBMRI-NL). The infrastructure for the NESDA study (www.nesda.nl) is funded through the Geestkracht program of the Netherlands Organisation for Health Research and Development (Zon-Mw, grant 10-000-1002) and supported by participating universities and mental health care organizations (VU University Medical Center, GGZ inGeest, Arkin, Leiden University Medical Center, GGZ Rivierduinen, University Medical Center Groningen, Lentis, GGZ Friesland, GGZ Drenthe, Scientific Institute for Quality of Healthcare (IQ healthcare), Netherlands Institute for Health Services Research (NIVEL), and Netherlands Institute of Mental Health and Addiction (Trimbos Institute). Additional cardiovascular measurements were supported by the Netherlands Heart Foundation (Grant Number 2006B258). The Hoorn Study was funded by the EMGO Institute VUmc, and has received grants from the Netherlands Diabetes Research Foundation and the Netherlands Organization for Health Research and Development.
Conflict of Interest Disclosures: None.
References:
1. Tiihonen J, Lönnqvist J, Wahlbeck K, Klaukka T, Niskanen L, Tanskanen A, Haukka J. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study). Lancet. 2009;374:620-627.
2. Saha S, Chant D, McGRath J. A systematic review of mortality in schizophrenia. Arch Gen Psychiatry. 2007;64:1123-1131.
3. De Hert M, Correll CU, Bobes J, Cetkovich-Bakmas M, Cohen D, Asai I, Detraux J, Gautam S, Möller HJ, Ndetei DM, Newcomer JW, Uwakwe R, Leucht S. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10:52-77.
4. Appleby L, Thomas S, Ferier N, Lewis G, Shaw J, Amos T. Sudden unexplained death in psychiatric in-patients. Brit J Psychiatry. 2000;176:405-406.
p ( ,heheeealalalalthththth ccccarararare e e e ororororgagagaganinininizazazazatitititiooiity MMMMededededicicicicalalalal CCCCenenenentetett r,r,r,r, GGGGeslandddd,,,, GGGGGGGGZ Z Z Z DrDrDrDrenenenenththtt e
Institute for Quality of Healthcare (IQ healthcare), Netherlands Institute for Healesearch (NIVEL), and Netherlands Institute of Mental Health and Addiction (TriAdditional cardiovascular measurements were supported by the Netherlands Hean
Study was funded by the EMGO Institute VUmc, and has received grants from dan
f Interest Disclos res: None
Instituuutetete fffororor QQuauauuality of Healthcare (IQ heaaaltltlthcare), Netherlaaaandnnn s Institute for Healessseaeaearch (NNNNIIVELELEE ), and Netherlands Instituutee of Mentallll HHHHealtltltlth and Addiction (TrAAAdA dddid tional cararar idid ovvvvasssscucucuculalalaar rr memeeeaasaa uruureemenennts wwereee e ssus ppppppp orteteteddd bybybyb ttheee NNNNetttheheheherlllrlananandsdsdsds HHHean (((GGGrG ant Numbbeer 2220006BBB22252 8).
StSttududududy y y wawawawas sss fufufufunddddedededed bbbby yyy thhhe eee EMEMEMMGOOOO IIInsnsnsn tititititututuuttet VVVVUmUmUmUmc,c,c,c, aaaandndndnd hhhhasasasa rececececeieieiveveveveddd d grgrgg ananana tsss fffrororor mmm mds Diiiabaaa etess RRReseaeaearcrcrch Founuuundation andddd theeee NNNNetherlrlrlanaa ds Orgrgrgganananizatioooon fofofofor Health nd DDDDevevevelelelopopopmememeentntntnt.
ff IInttere tst DDiis lclos res: NNo
DOI: 10.1161/CIRCEP.113.000927
15
5. Koponen H, Alaräisänen A, Saari K, Pelkonen O, Huikuri H, Raatikainen MJ, Savolainen M, Isohanni M. Schizophrenia and sudden cardiac death: a review. Nord J Psychiatry. 2008;62:342-345.
6. Myerburg RJ, Castellanos A. Emerging paradigms of the epidemiology and demographics of sudden cardiac arrest. Heart Rhythm. 2006;3:235-239.
7. Timour Q, Frassati D, Descotes J, Chevalier P, Christé G, Chahine M. Sudden death of cardiac origin and psychotropic drugs. Front Pharmacol. 2012;3:76.
8. Ray WA, Chung CP, Murray KT, Hall K, Stein CM. Atypical antipsychotic drugs and the risk of sudden cardiac death. N Engl J Med. 2009;360:225-235.
9. Haddad PM, Anderson IM. Antipsychotic-related QTc prolongation, torsade de pointes and sudden death. Drugs. 2002;62:1649-1671.
10. Wilde AA, Antzelevitch C, Borggrefe M, Brugada J, Brugada R, Brugada P, Corrado D, Hauer RN, Kass RS, Nademanee K, Priori SG, Towbin JA. Proposed diagnostic criteria for the Brugada syndrome: consensus report. Circulation. 2002;106:2514-2519.
11. Penninx BW, Beekman AT, Smit JH, Zitman FG, Nolen WA, Spinhoven P, Cuijpers P, De Jong PJ, Van Marwijk HW, Assendelft WJ, Van Der Meer K, Verhaak P, Wensing M, De Graaf R, Hoogendijk WJ, Ormel J, Van Dyck R; NESDA Research Consortium. The Netherlands Study of Depression and Anxiety (NESDA): rationale, objectives and methods. Int J Methods Psychiatr Res. 2008;17:121-140.
12. Seldenrijk A, van Hout HP, van Marwijk HW, de Groot E, Gort J, Rustemeijer C, Diamant M, Penninx BW. Carotid atherosclerosis in depression and anxiety: associations for age of depression onset. World J Biol Psychiatry. 2011;12:549-558.
13. Kirkpatrick B, Messias E, Harvey PD, Fernandez-Egea E, Bowie CR. Is schizophrenia a syndrome of accelerated aging? Schizophr Bull. 2008;34:1024-1032.
14. Jeste DV, Wolkowitz OM, Palmer BW. Divergent trajectories of physical, cognitive, and psychosocial aging in schizophrenia. Schizophr Bull. 2011;37:451-455.
15. De Vegt F, Dekker JM, Jager A, Hienkens E, Kostense PJ, Stehouwer CD, Nijpels G, Bouter LM, Heine RJ. Relation of impaired fasting and postload glucose with incident type 2 diabetes in a Dutch population: The Hoorn Study. JAMA. 2001;285:2109-2113.
16. Committee for Proprietary Medicinal Products. Points to consider: the Assessment of the Potential for QT Interval Prolongation by Non-Cardiovascular Medicinal Products. London, 1997.
17. Hofman N, Tan HL, Alders M, Kolder I, de Haij S, Mannens MM, Lombardi MP, Dit Deprez RH, van Langen I, Wilde AA. Yield of molecular and clinical testing for arrhythmia
Brugaadaddda PPPP, CCCoCorrrradadddooo o DDdiagnnnnosososostitititicccc crcrcrcrititititererereriaiaiaia fffoor
y
x BW, Beekman AT, Smit JH, Zitman FG, Nolen WA, inhoven P, Cui ers Pan Marwi HW, Assendelft WJ, Van Der Meer K, Verhaak P, Wensi M, De Gdijk WJ, Ormel J, Van Dyck R; NESDA Research Consortium. The Netherlands
oR
rijk A an Ho t HP an Mar ijk HW de Groot E Gort J R stemeijer C Diam
yndddrorororomemmem ::: cocconsssenenene sus report. Circulation. 2220000 2;106:251444-251515119.9
xxx x BBBWB , Beekmmann ATATAT, Smmmmit JH,HHH ZZZittmaannn FGG, Noooolelelennn n WAWAA, Spininhohoooveen P,P,, CCCuuijjperrrs Pannn MMMarwijkkjkk HHWW, AAAsssennndededelft WJWJWJW , VaVaVann n Deer MeMeeeeeer KKKK,, VVVerrrhr aaak k P, WWWWensisisis ngnng MM, DeDD Gdijk kk WJWWJWJ, OOOrmelll J,J,JJ VVVVan DDDDycycycy kkkk R; NNNNESESESESDADADADA RRReseaeaeaearrrrch hhh CoCoCoConsnsnssortititium. ThThThTheee e NNethththerlall dddndsepreeeesssssss ioioioi n n n ananannd d d d AnAnAnA xixixix etetetty y y y (N(N(NNESEEE DADADADA):)::): rrrataata ionananan lele,,,, obobobo jejejej ctcctiviviviveseseses aaaandndndd mmmmetetetthohohohodsdsdsds. InInInInt t t J J J J MeMeMeMetho
Res. 2220000008;88 171717:1:1:1121212121-111404040.
irijkjk AA HHo tt HHPP MM iijkjk HHWW dd GGr tt EE GG tt JJ RR tte ijij CC DiDi
DOI: 10.1161/CIRCEP.113.000927
16
syndromes: report of 15 years' experience. Circulation. 2013;128:1513-1521.
18. Chen Q, Kirsch GE, Zhang D, Brugada R, Brugada J, Brugada P, Potenza D, Moya A, Borggrefe M, Breithardt G, Ortiz-Lopez R, Wang Z, Antzelevitch C, O'Brien RE, Schulze-Bahr E, Keating MT, Towbin JA, Wang Q. Genetic basis and molecular mechanism for idiopathic ventricular fibrillation. Nature. 1998;392:293-296.
19. www.brugadadrugs.org, accessed March 2013.
20. www.azcert.org, accessed March 2013.
21. Postema PG. About Brugada syndrome and its prevalence. Europace. 2012;14:925-928.
22. Hatta K, Takahashi T, Nakamura H, Yamashiro H, Yonezawa Y. Prolonged QT interval in acute psychotic patients. Psychiatry Res. 2000;94:279-285.
23. Suvisaari J, Perälä J, Saarni SI, Kattainen A, Lönnqvist J, Reunanen A. Coronary heart disease and cardiac conduction abnormalities in persons with psychotic disorders in a general population. Psychiatry Res. 2010;175:126-132.
24. De Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, van Ree JW, Daemen MJ, Houben LG, Wellens HJ. Out-of-hospital cardiac arrest in the 1990's: a population-based study in the Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol.1997;30;1500-1505.
25. Postema PG, Wolpert C, Amin AS, Probst V, Borggrefe M, Roden DM, Priori SG, Tan HL, Hiraoka M, Brugada J, Wilde AA. Drugs and Brugada syndrome patients: review of the literature, recommendations, and an up-to-date website (www.brugadadrugs.org). Heart Rhythm.2009;6:1335-1341.
26. Meregalli PG, Wilde AAM, Tan HL. Pathophysiological mechanisms of Brugada syndrome: depolarization disorder, repolarization disorder or more? Cardiovasc Res. 2005;67:367-378.
27. Yap YG, Behr ER, Camm AJ. Drug-induced Brugada syndrome. Europace. 2009;11:989-994.
28. Atalar F, Acuner TT, Cine N, Oncu F, Yesilbursa D, Ozbek U, Turkcan S. Two four-marker haplotypes on 7q36.1 region indicate that the potassium channel gene HERG1 (KCNH2, Kv11.1) is related to schizophrenia: a case control study. Behav Brain Funct. 2010;6:27.
29. Casamassima F, Hay AC, Benedetti A, Lattanzi L, Cassano GB, Perlis RH. L-type calcium channels and psychiatric disorders: A brief review. Am J Med Genet B Neuropsychiatr Genet.2010;153B:1373-1390.
30. Askland K, Read C, O'Connell C, Moore JH. Ion channels and schizophrenia: a gene set-based analytic approach to GWAS data for biological hypothesis testing. Hum Genet.
en AA. CoCoCC roronanaryryyy hhhheaeaeaearrrtrt c disorororordedededersrsrsrs iiiinnnn aaaa gegegegennner
.
e MG ts5
ma PG, Wolpert C, Amin AS, Probst V, Borggrefe M, Roden DM, Priori SG, TanBr gada J Wilde AA Dr gs and Br gada s ndrome patients: re ie of the
. PsPsPsPsycycycychihihih atatata ryryry RRResesese . 2010;175:126-132.
eeeede eeee-Swagemaakkersss JJJJ, GGGooorgelslslsl AAAPP, DDuuuboiis--Arrrrbobobouwuuwu WWWIII, vanan RRReeeee JWW,WW DDDaeaemeeenn n MG, WWWellenss HHHJJ. OOuttt-of-hohohohospspspitalalalal cccaarardiacacac arrreest ininin thhhhee 199999909 's: aa poooopupupup latitititiooon-b-baseeded ststrichchchhttt arrararea on iiinciiiidddence, cccchahhaharactttererereriisistitiitics a ddndd surururur iiviivavavaval. JJJJ AAAmA CCCColl ll CaCaCaCardiolll.500-1-1-115050505.5.5
ma PG, WoWoolplplplpererere t t t t C,C,CC, AAAAmimimimin n n ASASAS, , , , PrPPP obobobobstststs VVVV,,,, BoBoBoBorgrgrgrggrgrgrefeffefe eee M,MM,M, RRRododododenenenen DDDDM,M,MM, PPPPririiriorororori iii SG, TanBB dda JJ WiWildld AAAA DD dnd BB dda ddr titi tts ii ff thth

DOI: 10.1161/CIRCEP.113.000927
17
2012;131:373-391.
31. Bardai A, Lamberts RJ, Blom MT, Spanjaart AM, Berdowski J, van der Staal SR, Brouwer HJ, Koster RW, Sander JW, Thijs RD, Tan HL. Epilepsy is a risk factor for sudden cardiac arrest in the general population. PLoS One. 2012;7:e42749.
32. Surges R, Thijs RD, Tan HL, Sander JW. Sudden unexpected death in epilepsy: risk factors and potential pathomechanisms. Nat Rev Neurol. 2009;5:492-504.
33. Johnson JN, Hofman N, Haglund CM, Cascino GD, Wilde AA, Ackerman MJ. Identification of a possible pathogenic link between congenital long QT syndrome and epilepsy. Neurology.2009;72:224-231.
34. Huertas-Vazquez A, Teodorescu C, Reinier K, Uy-Evanado A, Chugh H, Jerger K, Ayala J, Gunson K, Jui J, Newton-Cheh C, Albert CM, Chugh SS. A Common Missense Variant in the Neuregulin1 Gene is associated with Both Schizophrenia and Sudden Cardiac Death. Heart Rhythm. 2013;10:994-998.
35. Bär KJ, Wernich K, Boettger S, Cordes J, Boettger MK, Löffler S, Kornischka J, Agelink MW. Relationship between cardiovagal modulation and psychotic state in patients with paranoid schizophrenia. Psychiatry Res. 2008;157;255-257.
36. Bardai A, Amin AS, Blom MT, Bezzina CR, Berdowski J, Langendijk PN, Beekman L, Klemens CA, Souverein PC, Koster RW, de Boer A, Tan HL. Sudden cardiac arrest associated with use of a non-cardiac drug that reduces cardiac excitability: evidence from bench, bedside, and community. Eur Heart J. 2013;34:1506-1516.
37. Shaw RM, Rudy Y. Electrophysiologic effects of acute myocardial ischemia: a theoretical study of altered cell excitability and action potential duration. Cardiovasc Res. 1997;35:256-272.
38. Malik M, Hnatkova K, Kowalski D, Keirns JJ, van Gelderen EM. QT/RR Curvatures in Healthy Subjects: Sex Differences and Covariates. Am J Physiol Heart Circ Physiol.2013;305:H1798-H1806.
39. Schneeweiss S, Avorn J. Antipsychotic agents and sudden cardiac death: how should we manage the risk? N Engl J Med. 2009;360:294-296.
Missense Variannt t t t ininininCaCaCaCardrdrdrdiaiaiaiac c cc DeDeDeDeatatatath.h.hh HeHeHeHearararrttt
, Wernich K, Boettger S, Cordes J, Boettger MK, Löffler S, Kornischka J, Agelitionship between cardiovagal modulation and psychotic state in patients with parn
A, Amin AS, Blom MT, Bezzina CR, Berdowski J, Langendijk PN, Beekman LC af a non-cardiac drug that reduces cardiac excitability: evidence from bench, bedsu
, WeWeWeWernrnrnr icicicch hh h K,KK BBBBooeo ttger S, Cordes J, Boettttttgegeg r MK, Löfflel r S,S,S,S, Kornischka J, Agelitiiiononononship betetetetweweweeneee cccararardididiiovovoovagagaggalalalal mmmodododulululatatatioii n aand pspsspsycycycychoohotitititic c c c stststatattate ee in ppppatatatatieieiei ntnn sss wiwiwiw thththh ppparnnnin aaa.a Psychiatryry Resess. 200808088;157575757;2555-25777.
A, AmAmAmAmininnin AAAS,SSS BBBlolll m MTMMM , BeBeBeBezzina a CRCRCRCR, BBBeB ddrddowowowskskskski JJJ, LLLLanananngege ddnddijijii k PNPNPNPN, Beekkkman LLLCA, SoSoSoSouvuvuvererereieieiin nnn PCPCPCP , KoKoKoKoststststereer RRRRW,W,W,W, dddde e e BoBoBoBoer AAAA, TaTaTaTan n nn HLHLHLH .. . SuSuSuSuddddddddenenenn ccccarararardidididiacacacc aaarrrrrresesese t t t t asasassosososociaf a non-cardddiaiaiacccc drddd uggg thahh t reddud ces carddddiac exciiitat bibibib lililil tytyty: evvvvidididennnceccc ffffrom bebb ncccchhh,h bbbbedsunity. Eurr rr HeHeHeHearararrt t t t J.JJ.J. 22201101013;;3;3 343434:11:1:1505050506-6-6-6-151515151616616.. .
DOI: 10.1161/CIRCEP.113.000927
18
Table 1: Characteristics of Schizophrenia, NESDA and Hoorn cohorts
Schizophrenia cohort
(N=275)
NESDAcohort
(N=179)
Hoorncohort
(N=1168)
N % N % N %Demographics
Male gender 195 70.9 66 36.9* 517 44.3*
Mean age, years (mean, SD) 44.8 9.9 47.7 12.5* 66.4 6.7*
Co-morbidities†Mean BMI (mean, SD) 27.6 5.5 25.4 4.5* 26.6 3.5*
Smoking 181 65.8 n.a. n.a.Myocardial infarction 4 1.5 2 1.1 61 5.9*
Hypertension 39 14.5 24 13.4 472 40.4*
Hypercholesterolemia 45 16.7 22 12.3 439 37.6*
Diabetes mellitus 22 8.2 3 1.7* 116 10.1Medication use
Sodium-channel blockers 77 28.0 1 0.6* 75 6.4*
QT-interval prolonging drugs 177 64.4 2 1.1* 44 3.8*
Cardiovascular drugs 15 5.5 15 8.4 271 23.2*
Lipid lowering drugs 29 10.5 10 5.6 94 8.0Antipsychotics 236 85.8 0 0.0* 0 0.0*
Tricyclic antidepressants 18 6.5 1 0.6* 5 0.4*
Selective serotonin reuptake inhibitors 69 25.1 0 0.0* 9 0.8*
Other antidepressants 13 4.7 0 0.0* 4 0.3*
Antipsychotic medicationFGA only 49 17.8SGA only 147 53.5FGA and SGA 40 14.5No antipsychotics 39 14.2Most commonly used antipsychotics
Clozapine 91 33.1Olanzapine 47 17.1Aripiprazol 30 10.9Risperidon 23 8.4Quetiapine 16 5.8Haloperidol 14 5.1Pimozide 12 4.4
Data are Number (%) unless otherwise indicated. BMI, body mass index; n.a., not available; SD, standard deviation. * p<0.05 versus Schizophrenia cohort.† In the Schizophrenia cohort, data on all co-morbidities were missing in 6 patients. In the Hoorn cohort, data on infarct status were missing in 128 patients, and on diabetes mellitus status in 15. Sodium-channel blockers: www.brugadadrugs.org (accessed March 2013). QT-interval prolonging drugs: www.azcert.org,list 1 or 2 (accessed March 2013). Cardiovascular drugs: nitrates, -blockers, calcium channel antagonists, antithrombotics. Lipid lowering drugs: ATC codes C10. FGA: first generation antipsychotics used: haloperidol, pimozide, flufenazine, flupenthixol, bromperidol, pipamperon, levomepromazine, zuclopenthixol. SGA: second generation antipsychotics used: aripiprazol, clozapine, olanzapine, quetiapine, risperidone.
12121212.3.3.3.3 434343439999 331...7777** 111111116666
d
annel blockers 77 28 0 1 0 6 75l
2r
one
ic medication
annel blblblococockekk rsrr 77 28.0 1 0.6 75l pppproooolllonging ddrd ugs 177 64.4 222 1.1* 44uuulu arrrr drugs 15 555.5 555 15 8.88.8 444 272727271111 2riinngng drugs 229 1000.5.5.55 10 5..6 944
otics 2323232 6666 858585.8.8.88 0000 0.0000** 000ntideprprprp essssasasantntntsss 181181 6.666 555 111 0.0.00.6666*** 5555erotoooonininiinn n rerereupupuptatatakekekek inhnhnhhibibibibititittorororsss 6969696 2525252 1.111 0000 00.00 000** 9999
depressants 1313 4..77 0 0.0.0 000*** 4iiic medididicatitition
DOI: 10.1161/CIRCEP.113.000927
19
Table 2: ECG outcomes of Schizophrenia, NESDA and Hoorn cohorts
Schizophrenia cohort NESDAcohort
(N=179)
Hoorncohort
(N=1168)All (N=275) With sodium-channel
blockers (N=77)
Without sodium-channel
blockers (N=198)
N % N % N % N % N %Brugada-ECG 32 11.6 13 16.9 19 9.6 2 1.1*‡ 28 2.4†§
QTc-interval prolongation
Mild (male 431-450 msec, female 451-470 msec) 36 13.1 14 18.2 22 11.1 6 3.4 60 5.1
Severe (male >450 msec, female >470 msec) 16 5.8 7 9.1 9 4.5 0 0.0 33 2.8
ECG parameters mean SD mean SD mean SD mean SD mean SD
Heart rate, beats per minute 80.8 16.9 82.9 16.0 80.0 17.2 61.7 9.8*‡ 68.0 11.9†§
QRS duration, msec 91.6 11.8 94.5 13.6 90.5 10.8* 91.0 10.3 101.8 16.9†§
PR duration, msec 159.8 21.5 165.8 22.7 157.4 20.6* 152.5 32.6 174.0 25.3†§
QTc duration, msec 410.9 29.8 416.3 31.9 408.8 28.7 393.1 25.1*‡ 401.9 28.5
Data are expressed as Number (%) unless otherwise indicated. Abbreviations as in Table 1. * p<0.05 between Schizophrenia and NESDA cohorts, corrected for sex and factors that were significantly (p<0.05) different between cohorts (BMI, diabetes mellitus status, use of sodium channel blockers and use of QT-interval prolonging drugs). † p<0.05 between Schizophrenia and Hoorn cohorts, corrected for gender, sex and factors that were significantly (p<0.05) different between cohorts (BMI, cardiovascular medication use, use of sodium channel blockers and use of QT-interval prolonging drugs). ‡ p<0.05 between Schizophrenia patients without sodium-channel blockers and NESDA cohort, corrected for sex and factors that were significantly (p<0.05) different between cohorts (BMI, diabetes mellitus status and use of QT-interval prolonging drugs). § p<0.05 between Schizophrenia patients without sodium-channel blockers and Hoorn cohort, corrected for sex and factors that were significantly (p<0.05) different between cohorts (cardiovascular medication use and use of QT-interval prolonging drugs).
22222222 111
1094 511 891 6
470 msec) 36 13.1 14 18.2 22 11
4
S
7
90 513 6
470 msec) 36 13.1 14 18.2 22 11
msmsmsm ec) 16161616 5.5.5.5 8 777 9.9 1111 9999 4
mem annn SD memm an SDDD meeeanaa S
8080 8.8 1616 9.9 8282 9.9 161161 0.0 8080 0.0 1717
9191 66 1111 88 9494 55 1313 66 9090 55 1010

DOI: 10.1161/CIRCEP.113.000927
20
Figure Legends
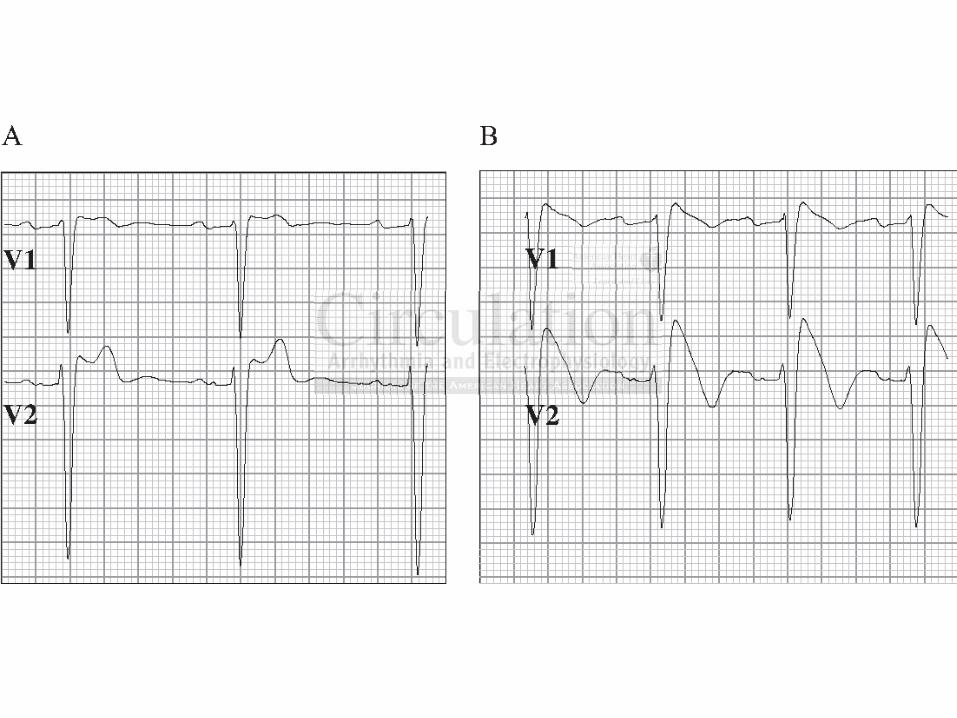
Figure 1: Example of Brugada-ECG and ajmaline test. Precordial ECG leads (25 mm/s, 10
mm/mV) are shown. Panel A (baseline ECG) shows “saddle-back” type ST elevations in V1 (1
mm) and V2 (3 mm) suggestive of Brugada syndrome. After 30 mg ajmaline infusion (panel B),
>2 mm “coved-type” ST elevations occur (type-1 Brugada-ECG), fulfilling the diagnostic
criteria for Brugada syndrome10.
Figure 2: Prevalence of type-1 and type-2/3 Brugada-ECG at baseline in schizophrenia with
antipsychotics, schizophrenia without antipsychotics, NESDA and Hoorn cohorts (this study),
compared with combined published prevalences in Europe21. Supplemental Table 2 provides
details of prevalence per country.
e in sschhchhizizii opophrhrhh eneniaiaaa wwwwitit
tics, schizophrenia without antipsychotics, NESDA and Hoorn cohorts (this stud
w e
p
ticsscscs, scscscs hihihiizozozoz phphphrerererenia without antipsychoticscscs, NESDA and dd Hooooooroo n cohorts (this stud
wwwwittthhh h combinedd ppubbbliiishedededd preevav lennces in EEuuropppeeee21. Suuupppppplemementttalalal Tabbbbleee 22 pprovivivide
prevalelellenccncnce peper countttry.