can we prevent postpartum depression? - hkuhknf.hku.hk/day1/gracetienlecture/ppd-hong kong...
TRANSCRIPT

Can We Prevent
Postpartum Depression?
Cindy-Lee Dennis, PhD Professor in Nursing and Psychiatry, University of Toronto
Canada Research Chair in Perinatal Community Health
Shirley Brown Chair in Women’s Mental Health, Women’s College Hospital

Clinical Importance of Depression
• Depression is one the most common health problems women experience
• It is estimated that 20-25% of women will experience depression during their lifetime
• Further, for 30-50% of women who do experience depression, it is estimated to become a chronic recurring condition
Perinatal Depression
• Perinatal depression is an episode of
depression with an onset either during
pregnancy or the first 12 months
postpartum
• Antenatal depression is an episode of
depression with an onset during
pregnancy
• Postpartum depression is an episode of
depression the first 12 months postpartum

Prevalence
Antenatal Depression
• Prevalence across pregnancy: 12.7% (18.4% with minor depression) (Gavin et al, 2005)
Postpartum Depression (PPD)
• Prevalence in the first 12 weeks postpartum: 13% (O’Hara & Swain,
1996)
→ For women with a history of depression, 35% PPD rate
→ For women with depression during pregnancy, 50% PPD rate

Most frequent
form of maternal morbidity
following childbirth

Persistence of PPD
• For the majority of mothers, PPD starts within the first 12
weeks postpartum
• National Canadian data suggest 8% of mothers will
continue to experience PPD past the first 5 months
postpartum and into the following year (Dennis, et al 2012)
→ this rate is more than 4 times the 1.4% point prevalence for
depression among women found in the Canadian Community Health
Survey
Inability to enjoy things that she used
to
Anxiety
Irritability
Worry Inability to sleep, even
when the baby is sleeping
Inability to concentrate or make decisions
Exhaustion
Feeling heavy
Fear of harming self
or baby
Uncontrollable crying
Common Symptoms
Next Steps?
Maternal PPD Risk Factors
• Depression during pregnancy
• Prenatal anxiety
• Previous history of depression
• Childcare stress
• Life stress
• Lack of social support
• Marital dissatisfaction/conflict
• Low self-esteem
• Low socio-economic status
• Single marital status
• Unwanted/unplanned pregnancy

Unfortunately, PPD occurs at a time when the infant is:
− Maximally dependent on parental care
− Highly sensitive to the quality of the interaction
• Given the persistence of PPD and its association with
recurrent depressive episodes (Copper et al 2003; Nylen et al 2010),
concern for child development is warranted as maternal
depression can:
1. Be incompatible with good parenting cognitions and behaviours
2. Cause significant distress for children due to a stressful home
environment (Goodman &Gotlib 1999)
Health Promotion Consequences
• Research suggests maternal health promotion behaviours
are diminished as mothers with PPD are less likely than
non-depressed mothers to:
− Breastfeed
− Attend well-child visits
− Complete immunizations
− Use home safety devices
− Put infants to sleep on their back
− Engage in enriching activities (e.g., reading, singing, outdoor
activities)
(Zajicek-Farber 2009; Cadzow et all 1999)
Child Developmental Consequences
• Mothers with PPD also have children with poorer
developmental trajectories
• Risk transmission through altered maternal-child
interaction (Rishel, 2012)

What are the effects of maternal-child interaction
difficulties on child development?
• Cognitive development
− General consensus that PPD predicts poorer language and IQ
development in children and that this effect is found across
childhood into adolescence
• Behavioural development
− Meta-analysis of 193 studies→ small but significant association
between maternal depression and child behavioural outcomes
• Emotional development
− Meta-analyses → consistent associations between PPD and
insecure attachment and difficulty in establishing effective self-
regulation skills (Martins and Gaffan, 2000; Atkinson et al., 2000; Campbell et al., 2004)

Intergenerational Effect
• Point prevalence rates for psychiatric disorders among
children of depressed mothers are 2 to 5 times above
community populations (Beardslee et al, 1998)
→ signifying a strong intergenerational effect

Costs of Perinatal Mental Health Problems
• 2014 Report released by London School of Economics
and Centre for Mental Health, UK
• This report– for the first time in the published literature –
provides comprehensive estimates of the costs of
perinatal mental health problems, including the adverse
effects on the child as well as the mother

• Taken together, perinatal depression, anxiety and
psychosis carry a total long-term cost to society of about
£8.1 billion for each one-year cohort of births in the UK
• Nearly three-quarters (72%) of this cost relates to adverse
impacts on the child rather than the mother
Postpartum
Depression:
A Family Affair
Paternal PPD Prevalence
• A recent meta-analysis suggests that approximately 10.4% of fathers will experience depression in the first year postpartum
• Growing evidence that PPD in fathers begins later, often following the onset in mothers and with the rate increasing over the first year postpartum
• Risk factor → maternal PPD
(Paulson et al. 2010)
PPD = Major Childhood Adversity
International experts have clearly identified maternal
depression as a major childhood adversity and that effective
interventions to address this condition are one of the most
important public health preventive strategies we can
implement to reduce the long-term negative outcomes
among children
Not only focus on individual treatment
but also include preventive approaches
to the management of PPD
Preventive Approach
• Moving beyond a model where we wait for a mother to
develop major depressive symptoms and then provide
evidence-based treatment
A NEW Philosophy
• FOCUS on the long-term healthy development of mothers and their
children
• PROACTIVELY provide resources to support this healthy
development

Cochrane Systematic Review
Psychosocial and Psychological Interventions for the Prevention of
Postpartum Depression:
An Update
Dennis, C-L., Dowswell, T. (2013). Psychosocial and psychological interventions for preventing postpartum depression. The Cochrane Database of Systematic Reviews, Issue 2.

Primary Objective
• To assess the effects of psychosocial and psychological
interventions compared with usual antepartum,
intrapartum, or postpartum care to reduce the risk of PPD

Secondary Objectives
1. the effectiveness of specific types of psychosocial interventions
2. the effectiveness of specific types of psychological interventions
3. the effects of intervention provider (professionally-based versus lay-based)
4. the effects of intervention mode (e.g. individual versus group-based interventions)
5. the effects of intervention duration (e.g. single-contact
interventions versus multiple-contact interventions)
6. the effects of intervention onset (e.g. antenatal-only,
versus antenatal and postnatal interventions, versus
postnatal-only interventions)
7. the effects of sample selection criteria (e.g. interventions
targeting women with specific risk factors versus the
general population).
Types of Studies
• All published and unpublished studies were eligible if
they fulfilled the following criteria:
− Were a randomised controlled trial
− Evaluated a psychosocial or psychological intervention in which
the primary or secondary aim was a reduction in risk to develop
PPD
• Quasi-randomised trials were excluded from the analysis

Types of Participants
• Pregnant women and new mothers less than 6 weeks
postpartum, including those at no known risk and those
identified as at-risk to develop PPD
• Trials where > 20% of participants were depressed at trial
entry were excluded

Types of Interventions
• A psychosocial or psychological intervention incorporated a variety of non-pharmaceutical strategies including:
−Psycho-educational sessions
−Cognitive behavioural therapy
−Interpersonal psychotherapy
−Non-directive counselling
−Psychological debriefing
−Various supportive interactions
• Excluded interventions that solely evaluated an educational intervention

Electronic Search
• Searched the Cochrane Pregnancy and Childbirth Group Trials
Register by contacting the Trials Search Co-ordinator
• Register contains trials identified from:
−quarterly searches of the Cochrane Central Register of Controlled Trials
(CENTRAL);
−weekly searches of MEDLINE;
−handsearches of 30 journals and the proceedings of major conferences;
−weekly current awareness alerts for a further 44 journals plus monthly BioMed
Central email alerts.
• Trials published in all languages were considered

Risk of Bias Assessment
• Based on recommendations by the Cochrane Collaboration the
following were examined:
− Generation of Allocation Sequence (selection bias)
− classified as low risk if based on computer generated numbers, tables of random
numbers, or similar
− Allocation Concealment (selection bias)
− classified as low risk if based on central randomisation, sealed envelopes, or similar
− Blinding (performance bias)
− classified as low risk if a blinded outcome assessment was conducted
− Completeness of Follow up Data (attrition bias)
• Did not exclude studies based on rate of incomplete data – sensitivity analysis was
completed if a < 80% follow-up rate was achieved

Review Characteristics
• 28 trials
• Almost 17,000 women
• Published between 1995 and 2010
• Conducted primarily in Australia and the UK
• Five trials were conducted in the USA
• One trial was conducted in the follow countries: Canada,
China, Germany, and India
Summary
• Overall psychosocial and psychological interventions
may decreased the risk of developing PPD by
approximately 22%

• There is beginning evidence to suggest the importance of:
1. Additional professional support initiated postnatally
2. Telephone-based peer support initiated postnatally
3. Interpersonal psychotherapy (IPT)
• Interventions are more likely to be beneficial if they are:
− Initiated postnatally
− Individually-based
− Include multiple contacts
− Target ‘at risk’ women

• Postnatal interventions that were successful
→administered Edinburgh Postnatal Depression Scale
(EPDS) early in the postpartum period to identify
depressive symptomatology
• Secondary preventive interventions

Postpartum Depression
Peer Support Trial (Dennis et al . BMJ 2009)
Funded by Canadian Institutes of Health Research (CIHR)

Purpose
• To evaluate the effect of peer (mother-to-mother) support
on the prevention of PPD among mothers identified as
high-risk

Design Overview
• A randomized controlled trial with stratification based on previous history of depression including PPD was conducted
• Seven Ontario health regions participated in the trial:
− Halton
− Ottawa
− Peel
− Sudbury
− Toronto
− Windsor
− York

Trial Schema
Outcomes at 24 weeks
Outcomes at 12 weeks
Usual Postpartum Care
Outcomes at 24 weeks
Outcomes at 12 weeks
Evaluation of Peer Support
Usual Postpartum Care
Plus Peer Support
Randomization
Eligibility Assessment
Consent
Verbal consent for further contact
Contact details to DCC
EPDS > 9
No further contact
EPDS < 10
PHN Screening

Randomization
• 701 mothers randomized using web-based randomization
(www.randomize.net)
− 349 mothers – intervention group (usual care plus telephone-
based peer support)
− 352 mothers – control group (usual care)
• No significant differences between groups on baseline
variables
Peer Volunteers
• Peer volunteer selection criteria was:
− Ability to speak and understand English
− Self-reported history of and recovery from PPD
− Not currently suffering from depression
• Over 205 peer volunteers were recruited and attended a 4-hour training session
• Provided with a training manual and a list of local community resources for new mothers

Intervention Dosage
• Mothers received a mean of 8.8 (SD=6.0) contacts with
their peer volunteer
• 49.5% were telephone conversations initiated by the peer
volunteer
• The mean duration of these discussions was 14.1 minutes
(SD=18.5)
• 33.4% of contacts were messages were left on mothers’
answering machines
• Only 6.5% contacts were initiated by the mothers
• 2.3% were email interactions
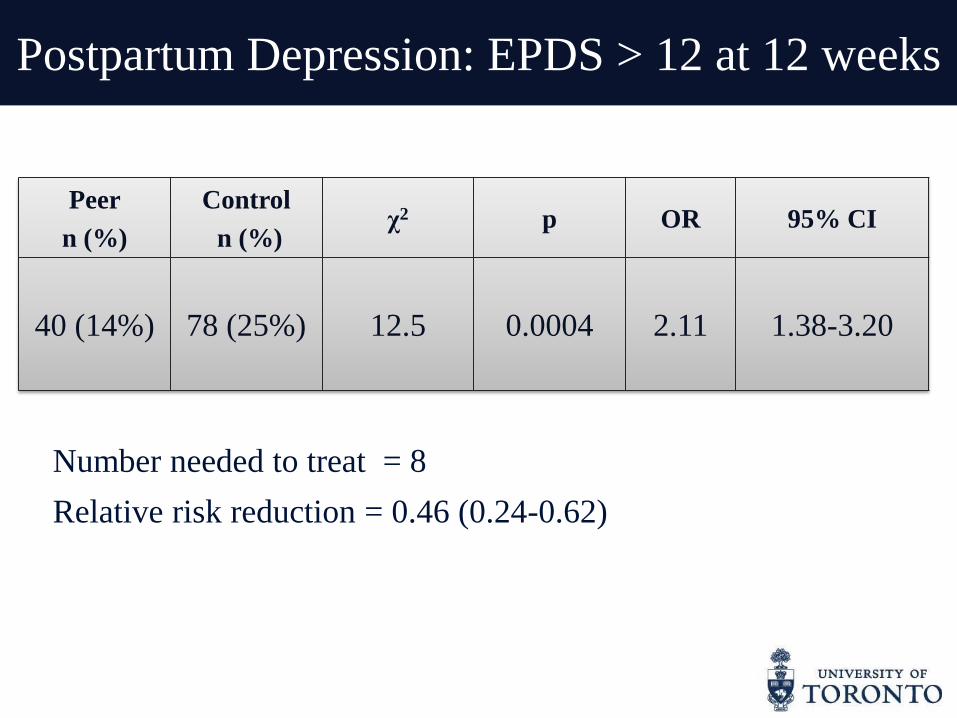
Postpartum Depression: EPDS > 12 at 12 weeks
Peer
n (%)
Control
n (%) χ2 p OR 95% CI
40 (14%) 78 (25%) 12.5 0.0004 2.11 1.38-3.20
Number needed to treat = 8
Relative risk reduction = 0.46 (0.24-0.62)

Summary
• Telephone-based peer support may be effective in
preventing PPD among high-risk mothers
• Mothers who received peer support were at half the risk
to develop PPD

Underlying Mechanisms of Peer Support
• Peer support can:
− Increase social networks
− Reinforce help-seeking behaviours
− Decrease barriers to care
− Encourage effective coping
− Promote social comparisons
− Increase self-efficacy
− Aid self-esteem

NICE Guideline for Depression

Management
of Perinatal
Depression

Case Identification
• The first step in the management of PPD is case
identification
• Research consistently demonstrates that informal
surveillance is imprecise with less than 50% of mothers
with perinatal depression identified despite various
interactions with health professionals (Yawn et al 2012; Goodman &
Tyer-Viola, 2010)
Antenatal Screening
• You can screen antenatally but most effective if it is to
identify women with current depressive symptoms
needing intervention → decreased predictive validity
when trying to identify asymptomatic women at risk
of developing PPD
• Flag women at high risk to develop PPD − History of depression
− Elevated anxiety
− History of abuse
− Migrant status
− Poor marital relationship

Postnatal Screening
Edinburgh Postnatal Depression Scale
(EPDS)
• 10-item self-report instrument
• Scores range from 0 to 30
• Cut-off 12/13 (> 12) – probable PPD
• Cut-off 9/10 (> 9) – possible PPD
• Widely available and free

EPDS
• Validated for antenatal use
• Translated and psychometrically tested in many non-
English populations – over 30 different languages
• Surveys of large samples of perinatal women have found
acceptability to be high (80-90%)
• Critical factor
• Provides a common language
• Enables comparability of clinical and research results
Does perinatal depression screening
increase the number of mothers
who recover?

Research is Clear
Screening alone is insufficient
to ensure the provision of appropriate treatment
and thus ultimately improving clinical outcomes

• The U.S. Preventive Services Task Force recommends screening adults for depression in clinical practices that have systems in place to assure:
1. Accurate diagnosis
2. Effective treatment
3. Follow-up

Effective Treatment Tools
Pharmacological
Psychological
−Interpersonal psychotherapy
(IPT)
−Cognitive behavioural therapy
(CBT)
−Mindfulness-based strategies
Psychosocial
−Peer support /support groups
−Non-directive counselling
Alternative
−Relaxation/Massage
−Exercise
−Yoga
−Bright light therapy
• Pharmacological interventions are a very effective
treatment
• Many mothers are reluctant to take antidepressant
medication due to concerns about breast milk transmission
or potential side-effects

Maternal Treatment Preferences
• The majority of mothers prefer “talking therapies” → especially if they are breastfeeding
• Interpersonal psychotherapy (IPT) is a common and effective ‘talking therapy’ for depression
• IPT is a brief, highly structured, manual-based psychotherapy that addresses interpersonal issues in depression such as: conflict, role disputes, social isolation, prolonged grief
• Intervention teaches:
− More effective communication with family and friends
− Skills for obtaining social support
− Effective coping techniques to use during times of need and during life
changes

• Unfortunately, IPT is not widely available, especially in rural
and remote areas
• There are often long wait-times to receive IPT from a trained
psychiatrist or psychologist
• Therapy is typically provided face-to-face in a clinic/hospital
setting
• PPD treatment has unique barriers (e.g. childcare issues) and high
attrition rates in group or clinic-based PPD treatment programs

Telepsychiatry
• To improve access to care, telepsychiatry has been introduced and includes the provision of psychiatric/mental health services via telephone
• Telepsychiatry can play an important adjunct role within an integrated health care system
• It is predicted to become an increasingly acceptable alternative to traditional face-to-face services
• The provision of IPT by trained nurses can also increase the clinical utility and feasibility of this treatment option

Interpersonal Psychotherapy Trial
Telephone-Based Interpersonal Psychotherapy for the
Treatment of Postpartum Depression
Funding: Canadian Institutes of Health Research

Design Overview
• Randomized controlled trial to evaluate the effect of telephone-based IPT by trained nurses among clinically depressed mothers (SCID positive)
• 36 health regions across Canada from 6 provinces:
− Nova Scotia
− Ontario
− Manitoba
− Saskatchewan
− Alberta
− British Columbia
Randomization
• 241 mothers randomized using web-based randomization
(www.randomize.net)
• 120 mothers → IPT group
• 121 mothers → Control group (standard care)
• No significant differences between groups on baseline
variables

Intervention
• Mothers received 12 weekly 1-hour IPT sessions at a
regularly scheduled time based on maternal convenience
• IPT nurse and mother never met
• Nurses completed an activity log per participant to
document all IPT session details
• All telephone sessions were digitally recorded and
emailed to the trial coordinator
−Guide supervision
−Ensure intervention fidelity

IPT Nurses
• 7 Toronto-based nurses hired and trained by two
psychiatrists (Ravitz & Grigoriadis) to provide IPT
– 3 nurses with psychiatric experience
– 2 public health nurses
– 1 pediatric nurse
– 1 ER nurse

Clinical Depression:
SCID Positive
Weeks
Follow-up
IPT
Group
n (%)
Control
Group
n (%)
χ2 p OR 95% CI
12 weeks
(N = 204)
11
(10.6)
35
(35) 17.41 <.001 4.55 2.16-9.62
24 weeks
(N = 202)
11
(10.9)
34
(33.7) 15.13 <.001 4.15 1.96-8.79
Maternal Evaluation
• Mothers felt the IPT nurses were competent and well-trained
• Telephone-based IPT was convenient and met their needs
• There was only one negative comment – would like more sessions
• Overall, mothers were highly satisfied and would recommend it to
a friend

Conclusion
• Mothers who received IPT were significantly more likely to have a
reduction in depressive symptoms
• Nurses can effectively deliver telephone-based IPT among
clinically depressed mothers
• The remission remained across time to 6 months post-treatment
• Significant ↓ in anxiety and ↑ in relationship quality with partner

• Technology plays a
major role in the
development and
evolution of our lives
• It has percolated into
all aspects including
education, banking,
and business
management

E-Health
• The implementation of technology in
the health sector, popularly known
as eHealth, is emerging as one of the
most rapidly growing areas in
healthcare today
• It encompasses a whole range of
purposes from purely administrative
through to health care delivery
E-Mental Health
• E-Mental health has tremendous potential to address the gap
between the identified need for mental health services and the
limited capacity to provide conventional care
• Applications can address four areas of mental health service
delivery:
1. Information provision
2. Screening, assessment, and monitoring
3. Intervention
4. Social support
• Primarily based on its ability to improve “reach”

Technologies Transforming Mental Health
Foster Collaboration
Increase Access to Services
Engage Individuals
Internet-based
Treatment
Online Peer Support Groups Telepsychiatry
Mobile Therapy
Outstanding Clinical Problem
While effective treatment tools exists for PPD……
Adequate treatment = treatment to remission

Maternal treatment preference
History of psychiatric treatment
Severity
Cultural
Factors
Barrier to treatment
accessibility
New treatment approaches are
required to address the GAP
between the existence and uptake of
effective PPD treatment tools

Collaborative Care
• “Collaborative care” is an approach
to treatment that is highly effective
for the management of general
depression
• In a collaborative care model, case
identification occurs at the
primary care level
• A depression care manager directs
individuals to appropriate treatment
and monitors progress – all in
collaboration with a mental health
specialist

Treatment Follow-Up
• Part of the success of this approach is that it actively
promotes treatment initiation and adherence while
addressing patient preferences and perceived barriers
• Also ensures appropriate follow-up and treatment to
remission

Evaluating Collaborative Care for Postpartum
Depression in Primary Care Settings
Funded by CIHR

Design Overview
• Randomized controlled trial
• Telephone-based collaborative care intervention for PPD
• Diverse maternal and infant outcomes
• Mothers between 0 to 6 months postpartum with
depressive symptomatology (EPDS >9)
• Identified during well-child visits in eight primary care
practices across Toronto

1. A multi-professional approach to care
2. Structured management plan
3. Scheduled patient follow-ups
4. Enhanced inter-professional communication

Summary
• Importance of clinical depression for women
• Prevalence and risk factors
• Impact on child development - cost
• Postpartum depression is a family affair
• Need to be proactive – prevent first then treatment if necessary
• Psychosocial and psychological interventions for prevention
• Peer support a simple yet effective secondary intervention
• Identification (screening) and treatment (talking therapy)
• Nurse-provided telephone-based IPT and the use of technology
• New approach to management – collaborative care
• Ensure treatment to remission to improve child development

Cindy-Lee Dennis, PhD Professor and Canada Research Chair
University of Toronto
www.cindyleedennis.ca