cancer (l. crab) - users.unimi.itusers.unimi.it/minucci/patologialezioni_2018-19/1819...
TRANSCRIPT
Cancer • First-second most common cause of death
in Western world • One in 2-3 Western people will die of
cancer


lezione del dr Cirò
clonal
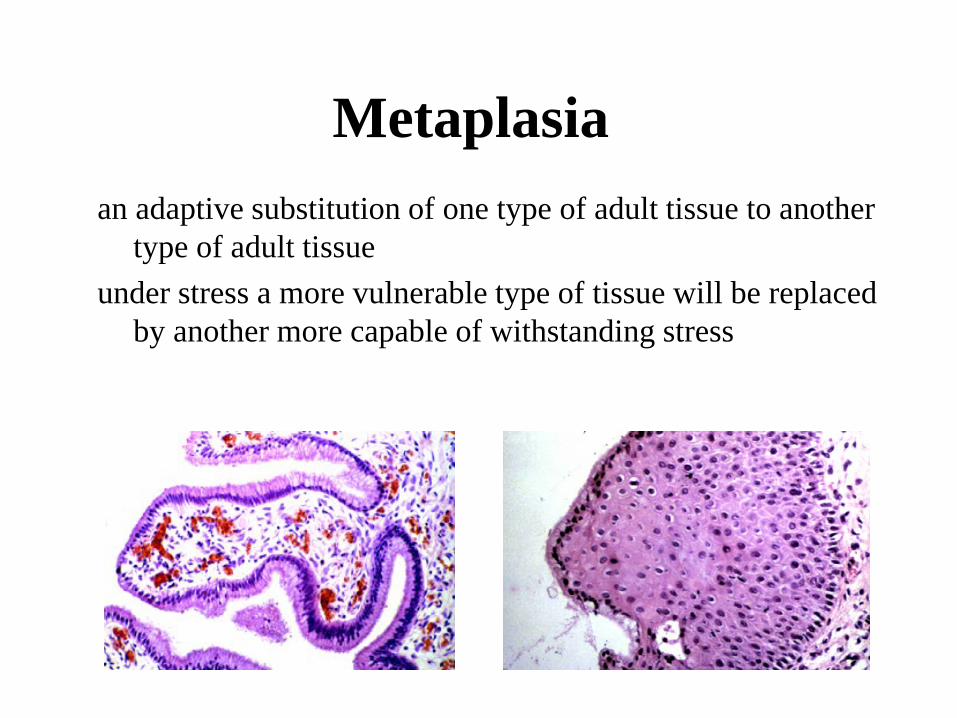
Metaplasia an adaptive substitution of one type of adult tissue to another
type of adult tissue under stress a more vulnerable type of tissue will be replaced
by another more capable of withstanding stress

Dysplasia
An abnormality in cell size, appearance, with or without a disorganized growth pattern

Neoplasia
A disease of cells characterized by alteration of normal growth regulatory mechanisms

Classification-approach Terminology which is used to describe a mass is
based on the clinical, gross and microscopic features-which in combination are a reflection of the predicted/expected biologic behavior
Benign Malignant ?

Neoplastic progression
• Benign or malignant neoplasms can acquire increasingly aggressive features
• Most malignant neoplasms arise de novo • Neoplasms are thought to be preceded by
preneoplastic conditions

Invasion and Metastasis
• Characteristics that are unique to malignant neoplasms (cancer)
• The major cause of morbidity and mortality
Importance of early detection in cancer
Increase of large scale screenings (breast cancer, prostate cancer, colon
cancer…etc)


Core Issues in Screening
• It is difficult to make healthy people better off than they already are. • It is sometimes easy to make healthy people worse off.
• Strong evidence of benefit is important when putting large numbers of healthy people in harm’s way.

Consequences of Screening: The Good
1. Reduced risk of death from the target cancer (compared to no screening)
• Nearly always need a randomized controlled trial to determine this
2. Reassurance (assuming healthy people need reassurance)

Consequences of Screening: The Bad
1. False reassurance when you have cancer
2. False alarms (false positive tests) • Harms of an unnecessary work-up
3. Harms of the test: bleeding, sepsis after biopsy, etc.
4. Detection of a lethal cancer without changing the outcome
• Spend more of your life as a cancer patient
5. Detection of non-lethal cancers (over-diagnosis)
• Unnecessary treatment • Treatment-related deaths of other causes (e.g., heart
disease, secondary cancers)
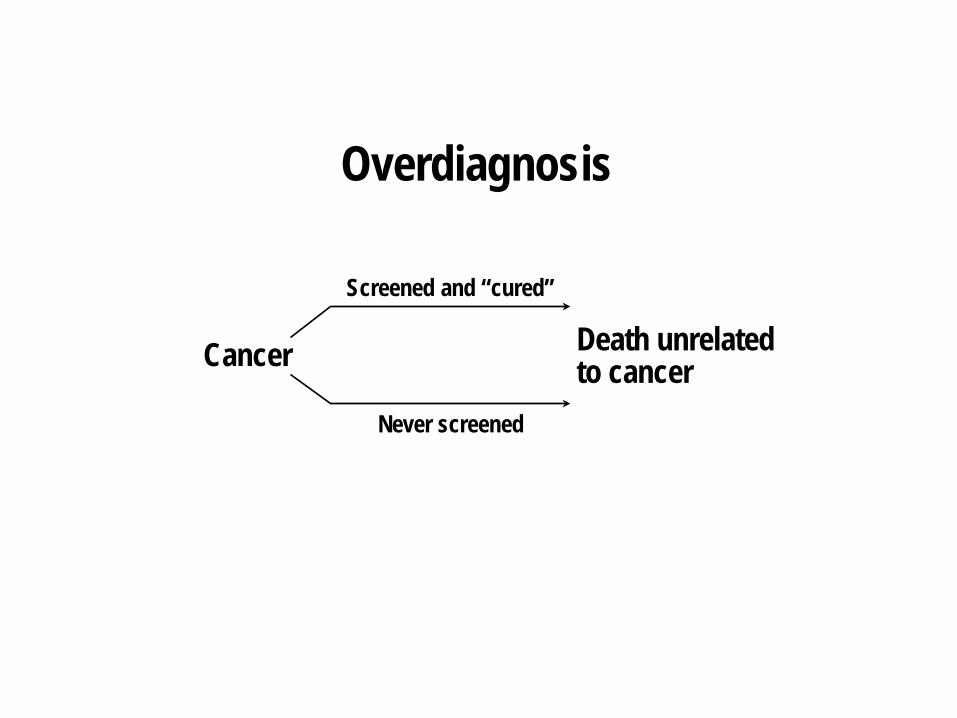
Overdiagnosis
Cancer
Screened and “cured”
Never screened
Death unrelated to cancer
36 Years Ago
Transformation of Philosophy in the Era of “Omics”
• The old days: “You are healthy until proven otherwise.”
• The modern era: “You are sick until proven otherwise.”
Adapted from E. Diamondis & M. Li, Clin Chem Lab Med 2016;54(3):389-396

18
Proportion of
Population Affected
0
100
Risk of Having/Getting Cancer
Symptoms Appear
Asymptomatic Cancer Preneoplasia Risk Factor for
Risk Factor Risk Factor
Consequences of Screening for Cancer Risk

“ The increased vigilance against pre-diseases might also change the way we perceive life itself, slowly transforming life into what can be characterized as pre-death.”
Bjorn Hofmann and John-Arne Skolbekken Surge in Publications on Early Detection, BMJ, 2017
20
Research Strategies to Investigate Overdiagnosis
• Use clinical opportunities to study natural history of indolent lesions • Prostate cancer: active surveillance • Barrett’s esophagus: serial endoscopy/biopsy
• Better animal models of progression of very early lesions
Screening Mammography one real life example

What if you …
were completing 5 years of tamoxifen after a partial mastectomy and breast irradiation,
coping with premature menopause, and undergoing annual mammograms of the other breast,
you learn
that there was a one in three chance of not having had breast cancer
?

Compare overdiagnosis risk with benefit of screening

The Treatment and Cost of Breast Cancer Overdiagnosis
• mastectomy or lumpectomy + radiation • anti-hormone therapy for 5-10 years • HER2/neu+: trastuzumab IV q 3 wks x 1 yr • Triple neg: chemotherapy Overtreatment antidotes • Premature menopause: supportive care • Osteopenia: biphosphonate, etc. Cost • Financial, physical, emotional, …

Randomized Trials of Screening Mammography 30 to 50 Years Ago
Trial Country Mortality Benefit Problem(s)
Health Insurance Plan of New York, 1963 U.S. Screening arm included MD Exam
Benefit only in 50-59 y/o’s
Malmo Study Sweden
Two-County Trial Sweden
Gothenburg Breast Screening Trial Sweden
Stockholm Trial Sweden
Edinburgh Trial Scotland
Canadian Natl. Breast Screening Trial 1
Canada None Actually worse in screened subjects
Canadian Natl. Breast Screening Trial 2
Canada None
Cochrane Analysis
• One biased trial excluded 600,000 women in analyses
• Three trials with adequate randomization did not show a significant reduction in breast cancer mortality at 13 years (RR=0.90, CI 0.79-1.02)
• 4 trials with suboptimal randomization showed a significant reduction in BrCa mortality with an RR=0.75 (CI 0.67-0.83)
• The RR for all 7 trials combined was 0.81 (CI 0.74-0.87)
Cochrane Analysis • Breast cancer mortality was an unreliable
outcome biased in favor of screening, mainly because of differential misclassification of cause of death
• Trials with adequate randomization did not find an effect of screening on cancer mortality: • Either breast cancer, after 10 years
(RR=1.02, 95% CI 0.95-1.10), or • All-cause mortality after 13 years
(RR=0.99, 95% CI 0.95 to 1.03)
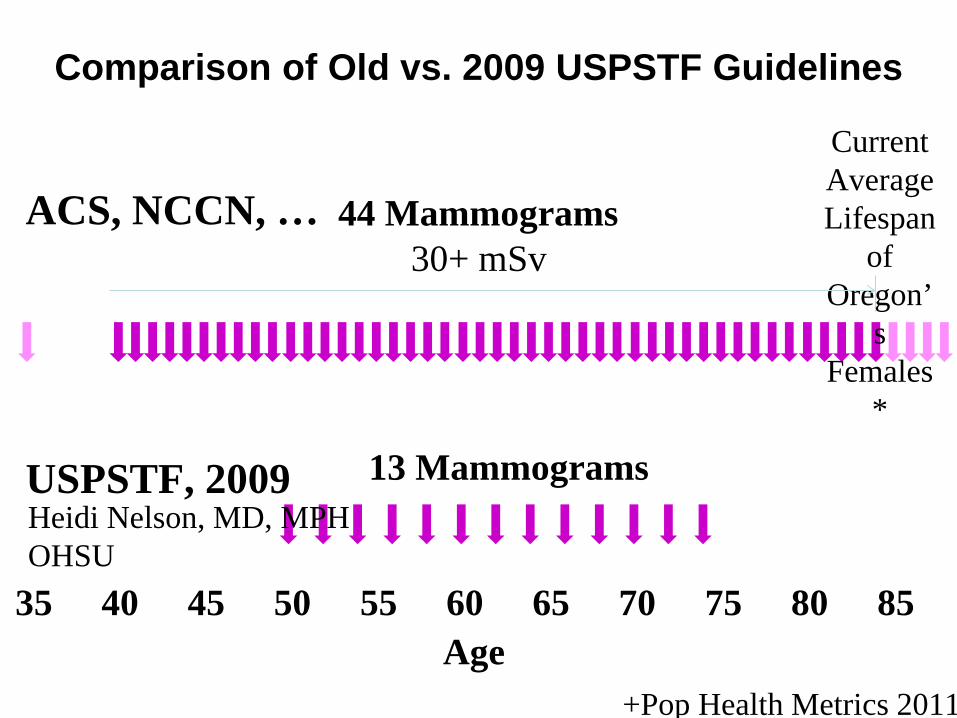
Comparison of Old vs. 2009 USPSTF Guidelines
Current Average Lifespan
of Oregon’
s Females
*
44 Mammograms
+Pop Health Metrics 2011
35 40 45 50 55 60 65 70 75 80 85 Age
13 Mammograms USPSTF, 2009 Heidi Nelson, MD, MPH OHSU
ACS, NCCN, … 30+ mSv

To the extent that screening mammograms result in the
diagnosis of ‘cancer’ that either does not need to be diagnosed or detected when it is, it can be said that
they cause breast cancer.
How Screening Mammograms ‘Cause’ Breast Cancer (and not from the radiation of mammograms)
These women undergo the same diagnostic interventions and treatment
(including surgery, radiation, and hormonal therapy and in some chemotherapy) and the associated adverse
physical, emotional, and financial effects of women who develop breast cancer without being screened.

“One in every 8 women will develop breast cancer
in her lifetime”
If 31% of all breast cancer is overdiagnosed, the actual risk is one in every 11 women

How much of the reported improvement in overall breast cancer survival is
an artifact of overdiagnosis ?
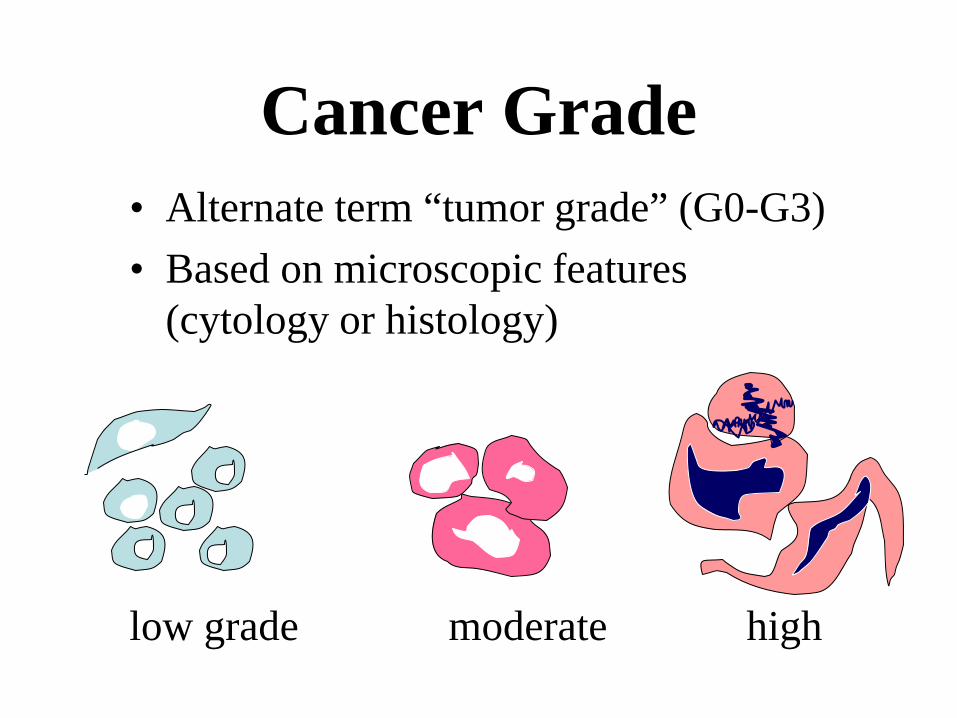
Cancer Grade • Alternate term “tumor grade” (G0-G3) • Based on microscopic features
(cytology or histology)
low grade moderate high

Cancer Stage • Reflects degree of spread, for an individual cancer
patient • Assigned at the time of diagnosis, may be updated
as patient progresses T Tumor characteristics N Nodal involvement M Metastasis

Epidemiologia dei tumori




Il cancro è una malattia genetica
La componente “ambientale” gioca però un ruolo fondamentale:
Sociologia dei tumori



Ereditarietá dei tumori • Una componente ereditaria é piú o meno facilmente
identificable sia per la predisposizione, che per la insorgenza di diversi tipi di tumori;
• Tumori ereditari: retinoblastoma, adenomatosi familiare del colon, piccola frazione dei tumori mammari/ovarici
• Tumori familiari: manifestazione familiare di tumori esistenti anche in forma sporadica
• Sindromi da difetti nel sistema di riparazione del DNA
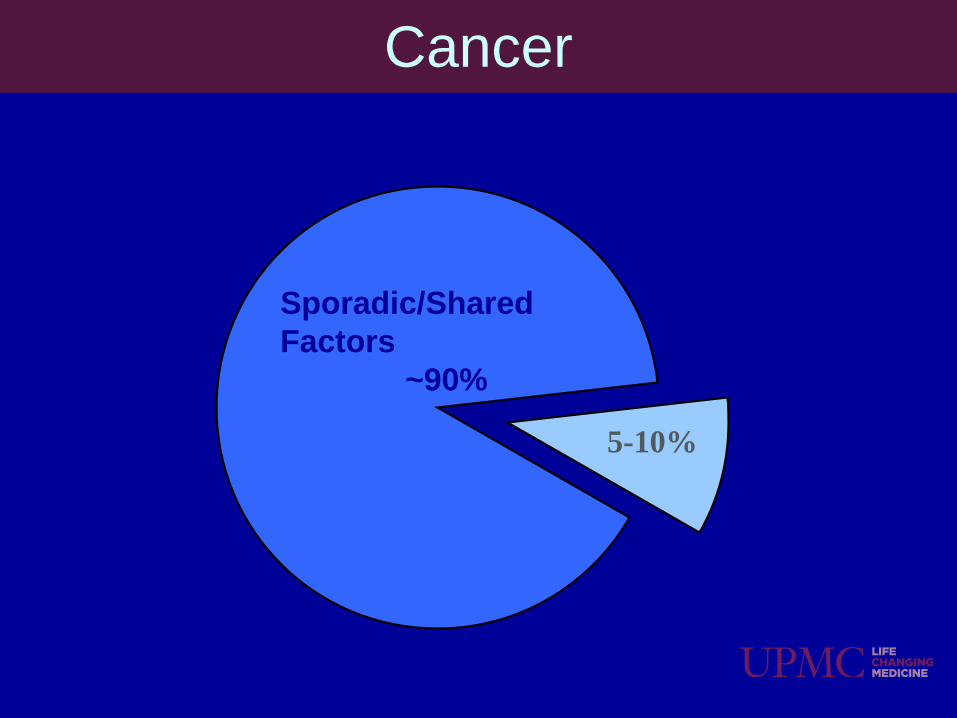
5-10%
Hereditary Susceptibility
Sporadic/Shared Factors
~90%
Cancer

Types of Genetic Testing
• Evaluation of a blood or saliva specimen to identify inherited genetic mutations
• Aid in determining treatment • OncotypeTM (breast)
• May enable personalized therapy that is targeted to a specific gene pathway • EGFR mutations (lung)
• Can sometimes identify hereditary cancer predispositions
Germline Studies
Genomic Tumor Studies

Genome Medicine/Precision Medicine
• The use of knowledge from genetic testing of tumor (somatic) or germline to direct a patient’s cancer care
• Next Generation Sequencing (NGS) the ability to analyze
multiple genes or DNA fragments simultaneously-- faster and at less cost (gene panels)

Implications of Identifying a Mutation
48
b r ca d x 4 8
79 78
BSO 3 5
60 29
ch ild birth
63 57
50
76 48
b r ca d x 4 5
75
45
50
b r ca d x 4 7
45
ov ca dx 45
br ca dx50
BRCA2 Cancer Risks (lifetime) • 60% Breast Cancer Risk (Avg) • 30-40% Second Breast Cancer • 16-27% Ovary Cancer Risk • 5% Pancreas Cancer • 39% Prostate Cancer • 5% Melanoma

Cancer Gene Panel High-Risk Genes
Moderate-Risk Genes
Newer Genes
• Well studied
• Lifetime risk of cancer >50%
• May be related to more than 1 type of cancer
• Guidelines for screening and prevention established
• Well studied • Lifetime risk of
developing breast cancer 24-49%
• Guidelines for
screening available • Guidelines for
prevention not established
• Not as well studied
• Data based on small numbers of patients
• Cancer risks not yet determined
• May increase risks for breast and other cancers
• Guidelines for care not established

Possible Genetic Test Results Pathogenic Variant
Detected or
Positive Result
No Pathogenic Variant Detected
or Negative Result
Variant of Uncertain Significance (VUS)
• Increased Cancer Risks • Apply Management
Guidelines if available • Test other family members
if actionable
• Assess result based on family history
• Screen based on family history No genetic testing for unaffected family members
• Subtle DNA change • Unknown if benign variant
(normal) or disease causing • Follow based on family history • More info may become available

49
Another reason to consider updated/additional genetic testing is a change in personal or cancer family history (new diagnoses)

Summary • Testing technology changes and updated testing may be a
consideration • Personal and family cancer histories change and additional
testing may be considered • NGS multigene panels provide additional information, but
not all pathogenic variants (mutations) identified will result in a change in clinical management (new genes)
• Testing more genes means there is a greater chance to identify a VUS
• Testing not be completely covered by insurance due to lack of evidence regarding medical interventions for some genes evaluated