case report melanotic oncocytic metaplasia of the ... · pdf filecase report melanotic...
TRANSCRIPT
Int J Clin Exp Pathol 2015;8(2):2103-2110www.ijcep.com /ISSN:1936-2625/IJCEP0004419
Case Report Melanotic oncocytic metaplasia of the nasopharynx: a case report with a focus on immunohistochemical analyses and literature review
Shogo Tajima1,2, Aki Ohkubo3, Matsumi Yoshida3, Kenji Koda2, Ichirota Nameki3
1Department of Pathology, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan; Departments of 2Pathology, 3Otolaryngology, Fujieda Municipal General Hospital, Shizuoka, Japan
Received December 3, 2014; Accepted January 28, 2015; Epub February 1, 2015; Published February 15, 2015
Abstract: Melanotic oncocytic metaplasia (MOM) of the nasopharynx is an extremely rare lesion, with only 21 cases reported in English literature to date. MOM typically occurs near the Eustachian tube opening in Asian men in their 60 s to 70 s. Here, we present a case of MOM in a 57-year-old Japanese man who is a heavy smoker. The patient did not have complaints; MOM was diagnosed incidentally as 4 flat elevated lesions with brown to black discoloration, ranging from 2 to 3 mm in maximal diameter, were found in the right torus tubarius. On suspecting melanoma, the largest lesion was biopsied. Microscopic examination identified both oncocytic metaplasia and melanin pigmenta-tion of the epithelium in the same gland. Upon immunohistochemical examination, melanocytes displayed reactivity for 3 out of 4 melanocytic markers; immunopositivity for S-100 protein, Melan-A, and MITF and immunonegativity for HMB-45 was observed. Normal melanocytes in the nearby surface respiratory epithelium displayed the same pattern of immunoreactivity. Immunopositivity for S-100 protein and immunonegativity for HMB-45 have been previ-ously reported in MOM. Reduction of stimulation of melanocytes in a longstanding lesion like MOM may explain the immunonegativity for HMB-45. S-100 protein, in conjunction with more specific marker for melanocytes, Melan-A or MITF, could prove the definite presence of melanocytes in this case of MOM. As it has been shown by previous reports that MOM pursues a benign course, it will be sufficient to follow up the patients regularly for the remaining 3 lesions.
Keywords: Melanotic oncocytic metaplasia, nasopharynx, immunohistochemistry
Introduction
Melanotic oncocytic metaplasia (MOM) of the nasopharynx is an extremely rare lesion, first described by Shek et al. in 1995 [1]. There have been only 21 cases reported in English litera-ture to date [1-12]. MOM has typically been diagnosed near the Eustachian tube opening in Asian men in their 60s to 70 s. MOM lesions are usually a few millimeters in size with a slight elevation and show brown to black discolor-ation. Multiple lesions and bilateral involve-ment have sometimes been encountered in patients [5]. The associated representative symptoms such as otitis media and tinnitus may be caused by compression of the Eustachian tube [11].
Although MOM may be macroscopically mis-identified as early nasopharyngeal carcinoma,
malignant melanoma, or nevus, it is microscopi-cally distinct from these three diseases; MOM is characterized by an admixture of both mela-nin pigmentation and oncocytic metaplasia in the same gland [9]. The source of melanin was attributable to the numerous melanocytes found to coexist in MOM. Upon immunohisto-chemical (IHC) analysis, the melanocytes were found to be positive for S-100 protein and nega-tive for HMB-45, both of which are melanocytic markers; only one study on MOM tested for reactivity with Melan-A, another marker of melanocytes, and found a positive result [12].
In this study, we present an additional case of MOM, where the melanocytes stained positive-ly for S-100 protein and negatively for HMB-45, as found by IHC analysis, as was expected. We further analyzed the immunoreactivity of the melanocytes for two additional melanocytic
Nasopharyngeal melanotic oncocytic metaplasia
2104 Int J Clin Exp Pathol 2015;8(2):2103-2110
markers, Melan-A and MITF, and found that the cell showed positive staining for both the markers. This pattern of expression signature of melanocytes in MOM is discussed in this report and extensive review of the literature was conducted to extract characteristics of MOM.
Clinical findings
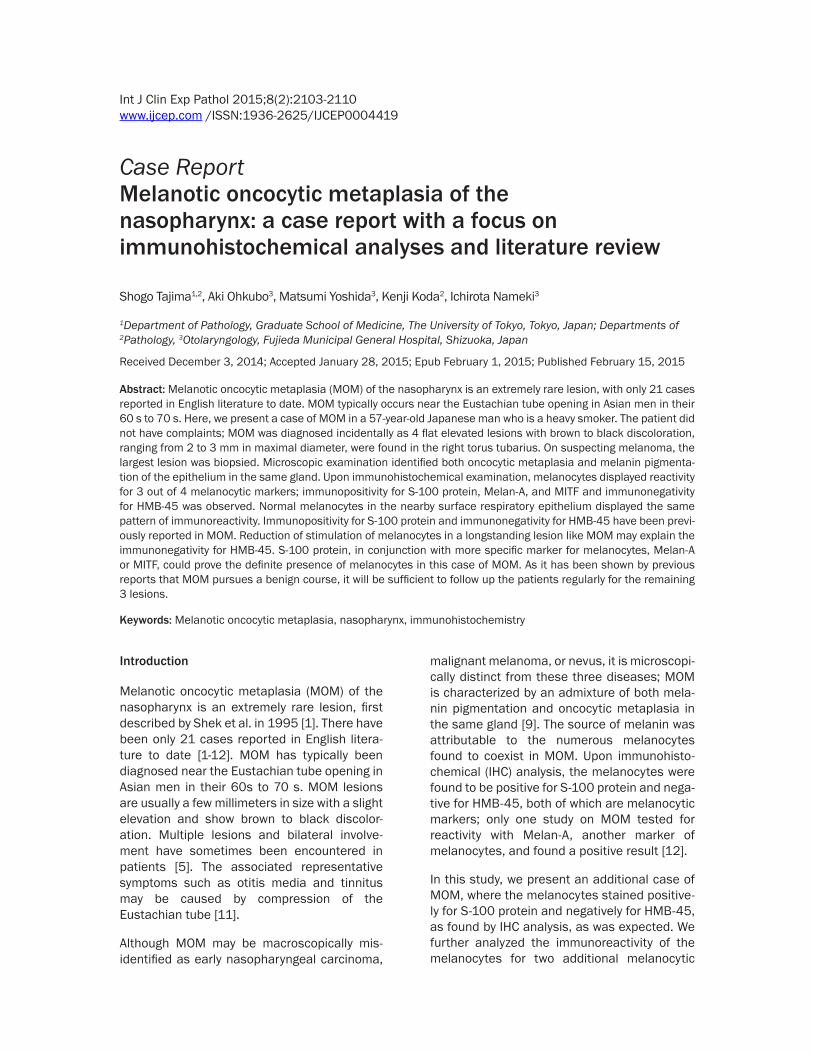
A 57-year-old Japanese man, who was regularly followed up and treated at a local clinic for hypertension and hyperlipidemia, was referred because of elevated carcinoembryonic antigen (CEA: 8.9 ng/ml; normal range: < 5 ng/ml) lev-els and a positive result for fecal occult blood test. He is a heavy smoker with a history of smoking 30 cigarettes per day for the past 40 years (Brinkman index: 1200). Upper and lower endoscopic examination revealed no abnormal-ity. By computed tomography (CT), several nod-ules with central cavities in the bilateral lung were identified. Metastatic or inflammatory lesions were suspected, but the patient refused a TBLB. The head and neck region was exam-ined to search for the origin of a possible meta-static tumor. No palpable mass was found in this region. The patient underwent laryngosco-py, and 4 flat, elevated lesions with brown to black discoloration, ranging from 2 to 3 mm in the maximal diameter, were found in the right torus tubarius (Figure 1A, 1B). Melanoma was
suspected, and a biopsy was collected from the largest lesion; examination revealed MOM. Examination of the nasal cavity, pharynx, and larynx revealed no additional lesions. Sub- sequently, fluorodeoxyglucose positron emis-sion tomography was performed. No abnormal accumulation was found in the lung or any other organs. Six months later, the patient was reex-amined by CT. The lesions that had been ini-tially detected had disappeared and were therefore considered inflammatory lesions. However, the patient’s CEA level was still ele-vated (6.2 ng/ml); the increased CEA level was suspected to be a result of heavy smoking. As the lesions of the right torus tubarius were not enlarged, he was referred back to the local clinic.
Pathological findings
The biopsied tissue was fixed in 10% buffered formalin. The specimen was then embedded in paraffin. Sections were cut for hematoxylin and eosin (H&E) staining (2.5 μm thick sections), Fontana-Masson staining (2.5 μm thick sec-tions), and immunohistochemical analysis (IHC; 4 μm thick sections). IHC analysis was per-formed using an automated slide stainer (Bench-Mark GX; Ventana Medical Systems, Tucson, AZ, USA). Giemsa staining was used as a counterstain for the specimen used for IHC analysis.
Figure 1. Laryngoscopical examination revealed lesions in the right torus tubarius. (A) One of the 4 flat elevated lesions found in the right torus tubarius. It displayed brown to black discoloration and ranged from 2 to 3 mm in maximal diameter. (B) (A) in higher magnification.
Nasopharyngeal melanotic oncocytic metaplasia
2105 Int J Clin Exp Pathol 2015;8(2):2103-2110
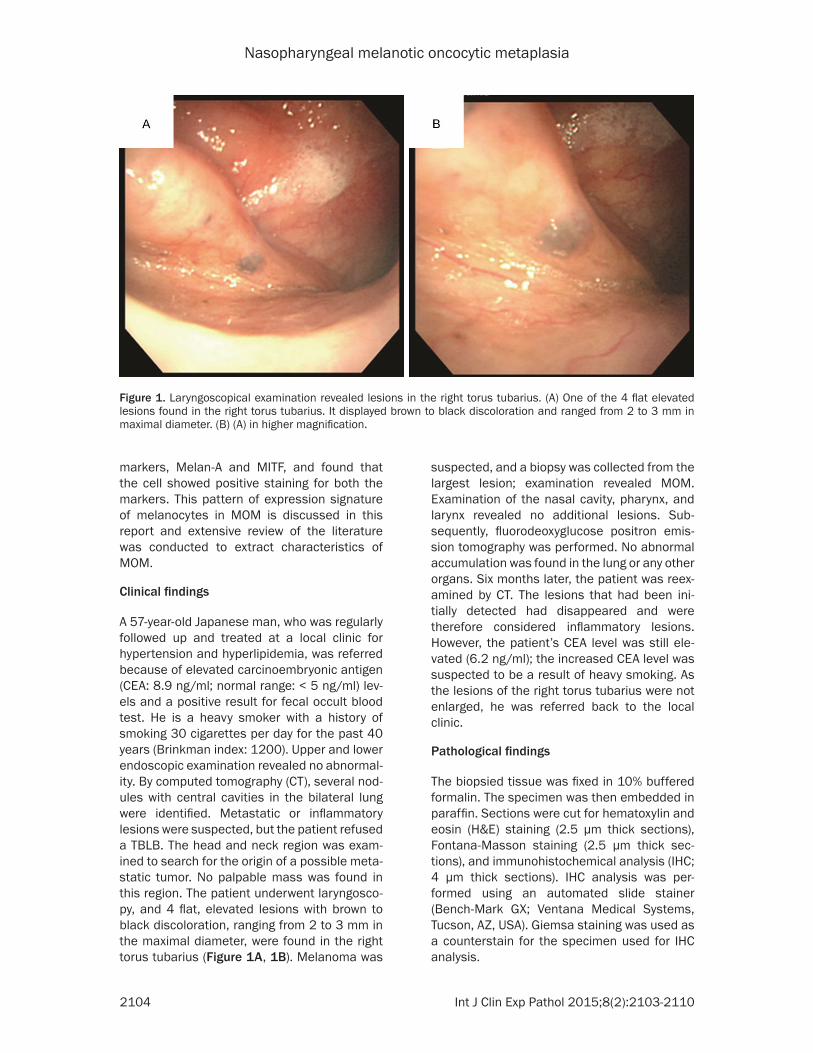
Figure 2. Histopathological findings. A. The surface of the lesion was covered by respiratory epithelium with goblet cells. It was composed of pre-existing seromucous glands with diffuse oncocytic metaplasia (× 20). B. Oncocytes presented abundant eosinophilc granular cytoplasm. Brown pigments were also observed in the cytoplasm of many
Nasopharyngeal melanotic oncocytic metaplasia
2106 Int J Clin Exp Pathol 2015;8(2):2103-2110
Microscopically, the lesion was well demarcat-ed, but was not encapsulated. The surface was covered by respiratory epithelium with goblet cells. The lesion was composed of pre-existing seromucous glands with diffuse oncocytic metaplasia (Figure 2A). Oncocytes presented abundant eosinophilic granular cytoplasm. Brown pigments were also observed in the cytoplasm of many oncocytes (Fig- ure 2B). Upon closer inspection, melano- cytes were found to be hardly discernible. Mitotic figures or atypia of oncocytes were not observed (Figure 2C). The brown pigments were positive for Fontana-Masson staining
(Figure 2C, inset), indicating melanin or li- pofuscin.
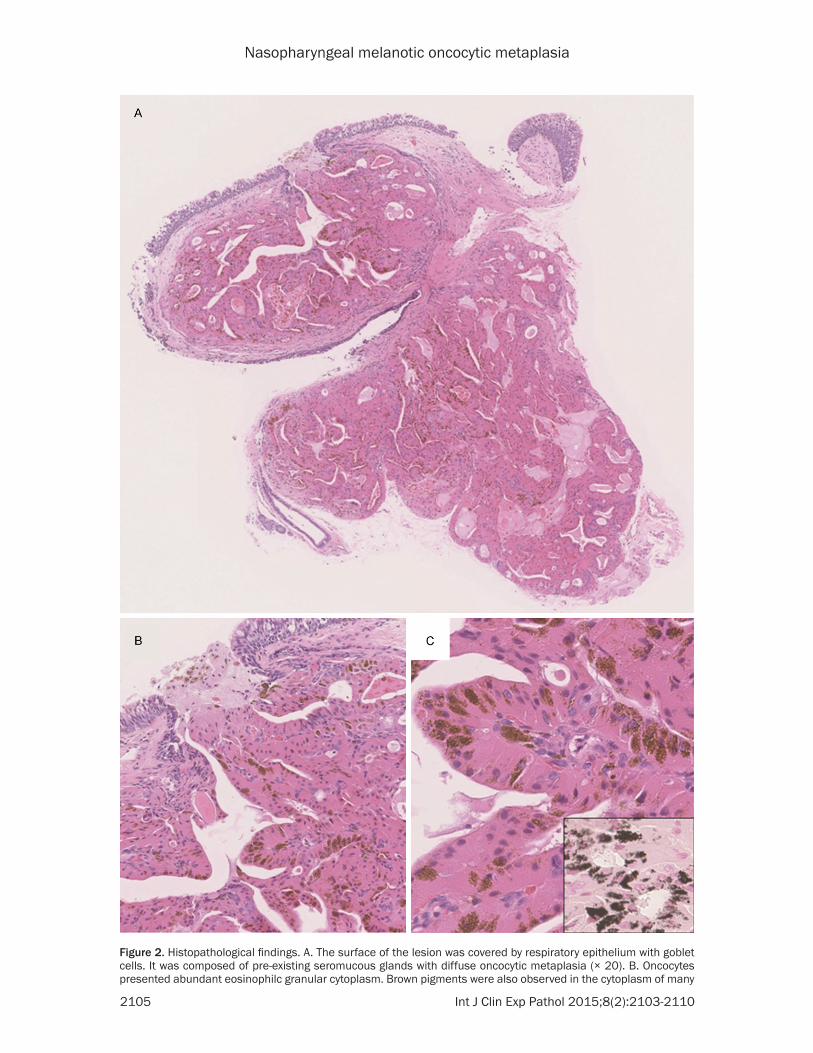
IHC analysis revealed melanocytes in the basal layer and intervening glandular cells. The mela-nocytes were positive for S-100 protein (poly-clonal, 1:1000; Dako, Glostrup, Denmark) (Figure 3A). HMB-45 did not show immunoreac-tivity (HMB-45, 1:100; Dako) (Figure 3B). The melanocytes were found to be immunoreactive to Melan-A (A103, 1:50; Dako) (Figure 3C) and MITF (D5, 1:100; Dako) (Figure 3D). Melano- cytes also existed in the surface respiratory epithelium near the lesion, which showed the
oncocytes (× 200). C. Upon closer inspection, melanocytes were hardly discernible. Mitotic figures or atypia of onco-cytes were not observed. The pigments stained positive with Fontana-Masson staining (inset) (× 400).
Figure 3. Immunohistochemistry of the lesion. Giemsa staining used as a counterstain revealed metachromasia for melanin pigment. Arrows indicate melanocytes. A. Melanocytes stained positive for S-100 protein (× 400). B. Melanocytes stained negative for HMB-45 (× 400). C. Melanocytes were immunoreactive for Melan-A (× 400). D. Melanocytes were immunopositive for MITF (× 400).
Nasopharyngeal melanotic oncocytic metaplasia
2107 Int J Clin Exp Pathol 2015;8(2):2103-2110
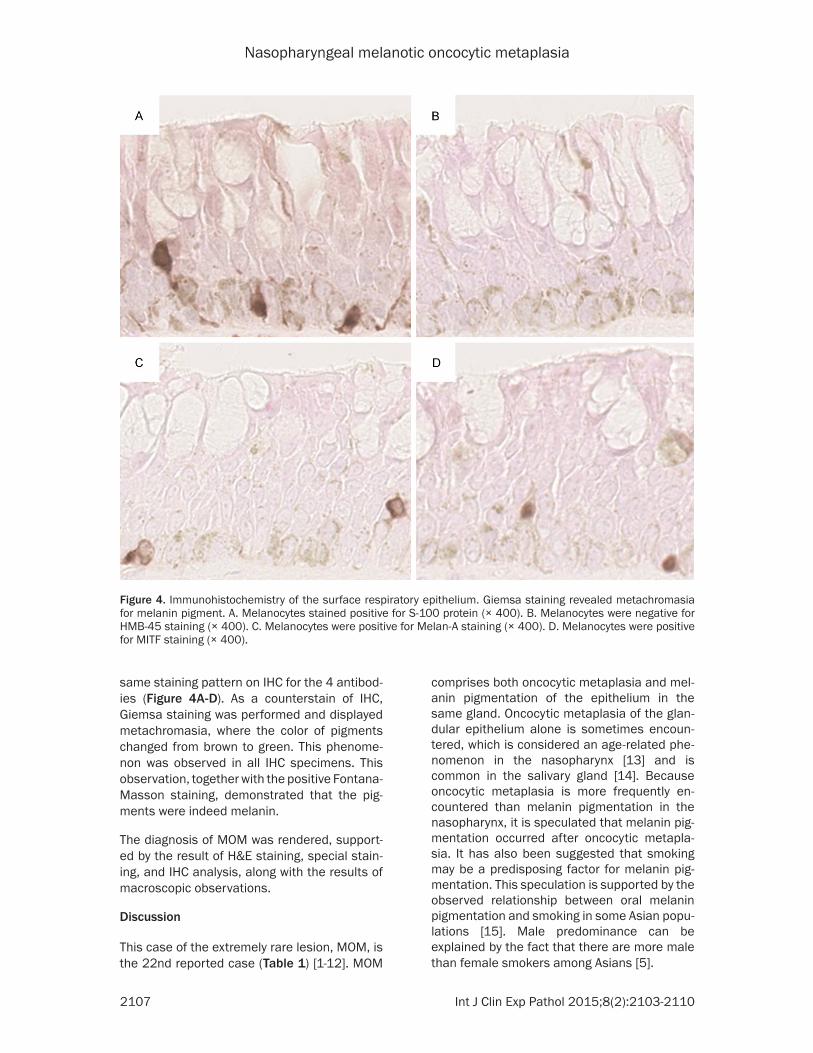
same staining pattern on IHC for the 4 antibod-ies (Figure 4A-D). As a counterstain of IHC, Giemsa staining was performed and displayed metachromasia, where the color of pigments changed from brown to green. This phenome-non was observed in all IHC specimens. This observation, together with the positive Fontana-Masson staining, demonstrated that the pig-ments were indeed melanin.
The diagnosis of MOM was rendered, support-ed by the result of H&E staining, special stain-ing, and IHC analysis, along with the results of macroscopic observations.
Discussion
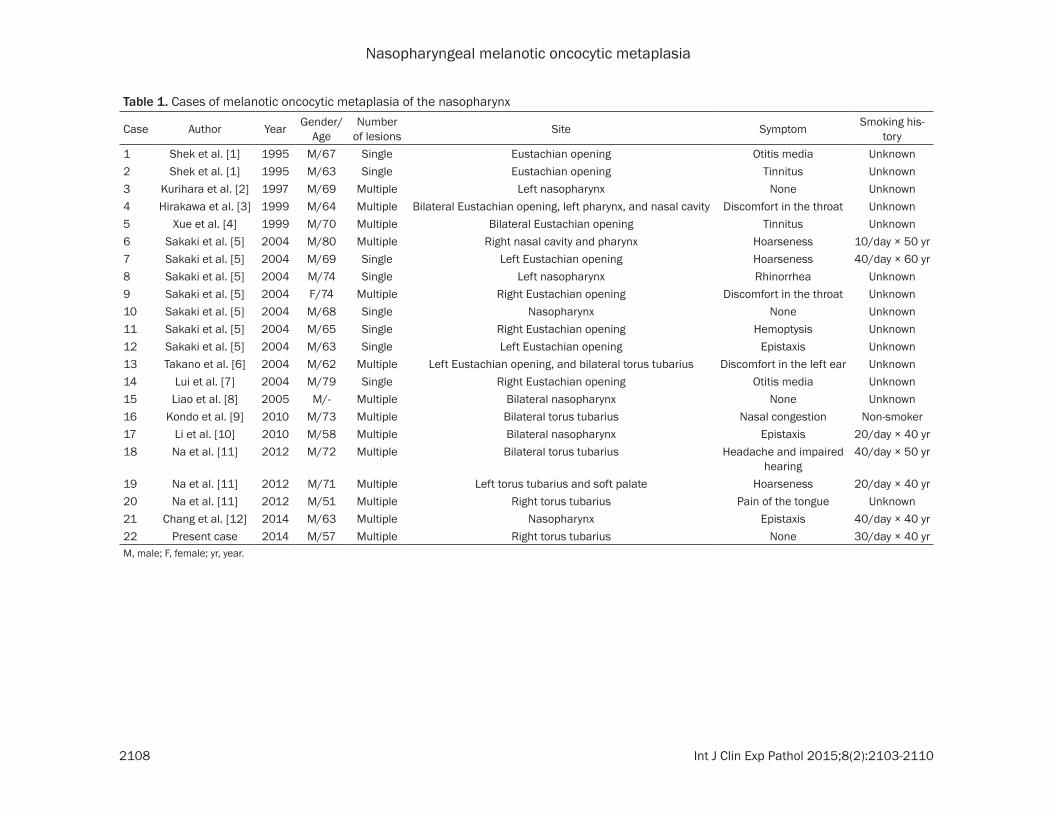
This case of the extremely rare lesion, MOM, is the 22nd reported case (Table 1) [1-12]. MOM
comprises both oncocytic metaplasia and mel-anin pigmentation of the epithelium in the same gland. Oncocytic metaplasia of the glan-dular epithelium alone is sometimes encoun-tered, which is considered an age-related phe-nomenon in the nasopharynx [13] and is common in the salivary gland [14]. Because oncocytic metaplasia is more frequently en- countered than melanin pigmentation in the nasopharynx, it is speculated that melanin pig-mentation occurred after oncocytic metapla-sia. It has also been suggested that smoking may be a predisposing factor for melanin pig-mentation. This speculation is supported by the observed relationship between oral melanin pigmentation and smoking in some Asian popu-lations [15]. Male predominance can be explained by the fact that there are more male than female smokers among Asians [5].
Figure 4. Immunohistochemistry of the surface respiratory epithelium. Giemsa staining revealed metachromasia for melanin pigment. A. Melanocytes stained positive for S-100 protein (× 400). B. Melanocytes were negative for HMB-45 staining (× 400). C. Melanocytes were positive for Melan-A staining (× 400). D. Melanocytes were positive for MITF staining (× 400).
Nasopharyngeal melanotic oncocytic metaplasia
2108 Int J Clin Exp Pathol 2015;8(2):2103-2110
Table 1. Cases of melanotic oncocytic metaplasia of the nasopharynx
Case Author Year Gender/Age
Number of lesions Site Symptom Smoking his-
tory1 Shek et al. [1] 1995 M/67 Single Eustachian opening Otitis media Unknown2 Shek et al. [1] 1995 M/63 Single Eustachian opening Tinnitus Unknown3 Kurihara et al. [2] 1997 M/69 Multiple Left nasopharynx None Unknown4 Hirakawa et al. [3] 1999 M/64 Multiple Bilateral Eustachian opening, left pharynx, and nasal cavity Discomfort in the throat Unknown5 Xue et al. [4] 1999 M/70 Multiple Bilateral Eustachian opening Tinnitus Unknown6 Sakaki et al. [5] 2004 M/80 Multiple Right nasal cavity and pharynx Hoarseness 10/day × 50 yr7 Sakaki et al. [5] 2004 M/69 Single Left Eustachian opening Hoarseness 40/day × 60 yr8 Sakaki et al. [5] 2004 M/74 Single Left nasopharynx Rhinorrhea Unknown9 Sakaki et al. [5] 2004 F/74 Multiple Right Eustachian opening Discomfort in the throat Unknown10 Sakaki et al. [5] 2004 M/68 Single Nasopharynx None Unknown11 Sakaki et al. [5] 2004 M/65 Single Right Eustachian opening Hemoptysis Unknown12 Sakaki et al. [5] 2004 M/63 Single Left Eustachian opening Epistaxis Unknown13 Takano et al. [6] 2004 M/62 Multiple Left Eustachian opening, and bilateral torus tubarius Discomfort in the left ear Unknown14 Lui et al. [7] 2004 M/79 Single Right Eustachian opening Otitis media Unknown15 Liao et al. [8] 2005 M/- Multiple Bilateral nasopharynx None Unknown16 Kondo et al. [9] 2010 M/73 Multiple Bilateral torus tubarius Nasal congestion Non-smoker17 Li et al. [10] 2010 M/58 Multiple Bilateral nasopharynx Epistaxis 20/day × 40 yr18 Na et al. [11] 2012 M/72 Multiple Bilateral torus tubarius Headache and impaired
hearing40/day × 50 yr
19 Na et al. [11] 2012 M/71 Multiple Left torus tubarius and soft palate Hoarseness 20/day × 40 yr20 Na et al. [11] 2012 M/51 Multiple Right torus tubarius Pain of the tongue Unknown21 Chang et al. [12] 2014 M/63 Multiple Nasopharynx Epistaxis 40/day × 40 yr22 Present case 2014 M/57 Multiple Right torus tubarius None 30/day × 40 yrM, male; F, female; yr, year.

Nasopharyngeal melanotic oncocytic metaplasia
2109 Int J Clin Exp Pathol 2015;8(2):2103-2110
Melanocytes are consistently present in MOM as a source for melanin pigmentation in onco-cytes [1-12]. Melanocytes have been reported to exist in the epithelium and stroma of the nasal cavity [16] and are postulated to colonize in MOM. Ultrastructurally, oncocytes in MOM lack premature melanosomes, in which mela-nin is produced [3]. Hence, the melanin pig-ment in MOM is believed to be passed on from the adjacent melanocytes via their dendrites [3].
Upon IHC examination of previous reports, there were some cells in MOM consistently found to be positive for S-100 protein and neg-ative for HMB-45, both of which are melano-cytic markers. Only one previous study con-firmed the presence of melanocytes in MOM using a third melanocytic marker, Melan-A [12]. As S-100 protein is the most sensitive marker for melanocytes [17], positive staining for S-100 was expected. However, positive staining for S-100 protein does not conclusively identify cells as melanocytes due to its lack of specific-ity [17]. Although HMB-45 is a more specific marker for melanocytes than S-100 protein [17], it stains premelanosome glycoprotein abundant in adult melanocytes during stimula-tion and normal adult skin melanocytes are not stained [18]. This is a likely explanation for why HMB-45 staining was not observed in previous studies. It may also be presumed that melano-cytes in MOM are not in a highly stimulated state at the time of biopsy, indicating a previ-ously developed and longstanding nature of MOM. In contrast, we speculate that melano-cytes were stimulated during MOM develop-ment, judging by the abundant melanin pig-mentation. Another melanocytic marker, Melan-A, which is the same as MART-1, a trans-membrane protein of melanocytes [19], is more sensitive than HMB-45 [20]. Melan-A/MART-1 stains normal skin melanocytes [19], explaining the positive staining of melanocytes in MOM for Melan-A. MITF is an integral transcriptional reg-ulator in melanocytes and expression of this gene is required [21]. This fact may explain the finding that melanocytes in MOM are positive for MITF.
All the reported cases of MOM followed a benign clinical course; there have not been any cases of recurrence or progression of MOM [11]. Simple excision, including excisional biop-sy, is a suitable treatment of choice for MOM [6].
In conclusion, this is the 22nd reported case of MOM occurring in an Asian man who is a heavy smoker. Asian ethnicity and the history of heavy smoking are likely related to the development of MOM. In addition to 2 frequently used mela-nocytic markers, S-100 protein and HMB-45, 2 additional melanocytic markers with high spec-ificity, Melan-A and MITF, were used in this case. The use of these additional markers increases the accuracy of the diagnosis, as S-100 is less specific as a marker for melano-cytes and HMB-45, a more specific marker, hardly recognizes melanocytes not being stimu-lated. Some cells of MOM in this case were shown to stain positively for Melan-A and MITF, which indicated the definite presence of mela-nocytes. Using S-100 protein and HMB-45 alone would not be sufficient for evaluating benign and dormant melanocytic lesions. Since MOM pursues a benign course, it will be suffi-cient to follow up regularly with the patient to evaluate progression of the remaining 3 lesions that were not biopsied.
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Shogo Tajima, Department of Pathology, Graduate School of Medicine, The University of Tokyo, 7-3-1 Hongo, Bunkyo-Ku, Tokyo 113-0033, Japan. Tel: +81-3-5841-3341; Fax: +81-3-3815-8379; E-mail: [email protected]
References
[1] Shek TW, Luk IS, Nicholls JM and Fok KO. Mel-anotic oncocytic metaplasia of the nasophar-ynx. Histopathology 1995; 26: 273-275.
[2] Kurihara K and Nakagawa K. Pigmented vari-ant of benign oncocytic lesion of the pharynx. Pathol Int 1997; 47: 315-317.
[3] Hirakawa E, Miki H, Ohmori M, Kobayashi S, Haba R and Nagai Y. Melanin pigmented onco-cytic metaplasia of the nasopharynx. Virchows Arch 1999; 434: 455-457.
[4] Xue WC and Hui YZ. Melanotic oncocytic meta-plasia of the nasopharynx. Histopathology 1999; 35: 481-482.
[5] Sakaki M, Shek TW, Hirokawa M, Kashima K, Daa T, Gamachi A and Sano T. Melanotic onco-cytic metaplasia of the nasopharynx: a report of seven cases and review of the literature. Vir-chows Arch 2004; 444: 345-349.
[6] Takano K, Sato J, Shirasaki H, Yamazaki N, Hoki K and Himi T. Melanin pigmented onco-cytic metaplasia of the nasopharynx. Auris Na-sus Larynx 2004; 31: 161-163.
Nasopharyngeal melanotic oncocytic metaplasia
2110 Int J Clin Exp Pathol 2015;8(2):2103-2110
[7] Lui PC, Chan AB, Chan KF, Choi CH and Tse GM. Melanocytic and non-melanocytic onco-cytic metaplasia of the nasopharynx. Patholo-gy 2004; 36: 504-505.
[8] Liao CT and Kuo TT. Images in pathology. Mela-notic oncocytic metaplasia of the nasophar-ynx. Int J Surg Pathol 2005; 13: 279.
[9] Kondo T, Mori K, Oka S and Morinaka S. Mela-notic oncocytic metaplasia of the nasopharynx as a benign mimicker of malignant melanoma: a case report. Diagn Pathol 2010; 5: 5.
[10] Li Y, Lu ZH, Lu W and Chen J. Images for diag-nosis. Melanotic oncocytic metaplasia of naso-pharynx: a case report with review. Chin Med J (Engl) 2010; 123: 1230-1232.
[11] Na JY, Kim YH, Choi YD and Lee JS. Melanotic oncocytic metaplasia of the nasopharynx: a re-port of three cases and review of the literature. Korean J Pathol 2012; 46: 201-204.
[12] Chang IW, Wang CC, Liu KW, Lan CH and Hung CH. Melanotic oncocytic metaplasia of the na-sopharynx. Pol J Pathol 2014; 65: 162-164.
[13] Morin GV, Shank EC, Burgess LP and Heffner DK. Oncocytic metaplasia of the pharynx. Oto-laryngol Head Neck Surg 1991; 105: 86-91.
[14] Hartwick RW and Batsakis JG. Non-Warthin’s tumor oncocytic lesions. Ann Otol Rhinol Laryn-gol 1990; 99: 674-677.
[15] Hedin CA and Axell T. Oral melanin pigmenta-tion in 467 Thai and Malaysian people with special emphasis on smoker’s melanosis. J Oral Pathol Med 1991; 20: 8-12.
[16] Uehara T, Matsubara O and Kasuga T. Melano-cytes in the nasal cavity and paranasal sinus. Incidence and distribution in Japan. Acta Pathol Jpn 1987; 37: 1105-1114.
[17] Clarkson KS, Sturdgess IC and Molyneux AJ. The usefulness of tyrosinase in the immuno-histochemical assessment of melanocytic le-sions: a comparison of the novel T311 anti-body (anti-tyrosinase) with S-100, HMB45, and A103 (anti-melan-A). J Clin Pathol 2001; 54: 196-200.
[18] Smoller BR, McNutt NS and Hsu A. HMB-45 recognizes stimulated melanocytes. J Cutan Pathol 1989; 16: 49-53.
[19] Fetsch PA, Fetsch JF, Marincola FM, Travis W, Batts KP and Abati A. Comparison of melano-ma antigen recognized by T cells (MART-1) to HMB-45: additional evidence to support a common lineage for angiomyolipoma, lymph-angiomyomatosis, and clear cell sugar tumor. Mod Pathol 1998; 11: 699-703.
[20] Busam KJ and Jungbluth AA. Melan-A, a new melanocytic differentiation marker. Adv Anat Pathol 1999; 6: 12-18.
[21] Widlund HR and Fisher DE. Microphthalamia-associated transcription factor: a critical regu-lator of pigment cell development and survival. Oncogene 2003; 22: 3035-3041.