chest tubes · 8/1/14 2 chest tube insertion and placement • air- 2nd intercostal space & mid...
TRANSCRIPT

8/1/14
1
Chest Tubes
Stanley John RT,BS,RRT-NPS,CPFT,CPC,ACCS,AE-C • Assistant Director – NSUH Respiratory Therapy Department
• Vice Chairman – New York State Education Department Respiratory Therapy & Polysomnography Technology Licensure Board
• Adjunct Instructor- Molloy College • Clinical Preceptor- Independence University
2
Disclosure of conflict of interest
I do not have any affiliations with any individual or entities that could be perceived as having a
bearing on my presentation"
2
Chest Tube
Fenestrated drainage hole
• Clear hollow tube • Mostly made of so@ silicon, clear polyvinylchloride (pvc) or a mix of both • Have a radiopaque strip. The strips have gaps that serves to mark the proximal drainage holes
ASTM International
• Name trade mark of manufacturer • ID and OD • Length (depth) in cm • IT Z-‐79 or F 29 • Single use or mulUple use • Radiopaque marker – full length
Pressure Changes in the Thoracic Cavity Pleural space and negative pressure
Parietal Pleura
Visceral Pleura
Serous Fluid
Chest Tube Placement “ InserUon of a silicon or polyvinylchloride (pvc)
tube through the chest wall into the pleural cavity to evacuate the accumulated air/blood/
pus from the pleural space”.
Chest Tube Placement Procedure Chest tube are inserted • At the bedside • In the operating room • or in an interventional radiology suite When-ever possible, informed consent should be
obtained
Indication for Chest Tube Insertion Air
– Pneumothorax (Spontaneous, Traumatic, Iatrogenic) – Tension Pneumothorax (Untreated Pneumothorax)
Fluid (Pleural Effusion) – Hemothorax – Blood – Hydrothorax – Serous fluid – Chylothorax - Lymphatic fluid – Empyema – Pus
Air & Fluid – Hemopneumothorax
Bronchopleural Fistula (BPF) - Post Op, Mechanical Ventilation Pleurodesis

8/1/14
2
Chest Tube Insertion and Placement
• Air- 2nd intercostal space & mid clavicular line • Fluid - 4th-5th intercostal space & mid-axillary line • Chest tube is inserted above the rib (superior border) • Avoiding the vein, artery and nerve –pain receptor which runs
under the rib (inferior border)
Air – mostly in the apices
Fluids (gravity dependent)-‐ bases
Evolution of the Drain Unit The 3 bottle drainage system
Same 3 bottle drain system #1- Collection/Trap Bottle • Collects the pleural drainage • Marked to allow measurement of pleural drainage • Single or multi chamber • Once the collection chamber get filled up the whole drainage
system needs to be changed
#2 – Water Seal Bottle • Middle bottle is the water seal bottle • Prevents air from entering the pleural cavity • Normally, there is no bubbling here. • Continuous bubbling should be reported because this means
there is an active air leak.
#2 - Water-Seal Bottle
• If the water seal should break, submerge chest tube in a glass of water. – If patient is receiving PPV leave tube open to air until a
new system can be set up. Do not clamp the tube – Prevent tension pneumothorax.
• Pulmonary edema may result if there is a malfunction that creates a sudden re-expansion of the lung.
• Water in the water seal bottle must be monitored to prevent any sudden change in pleural pressure
8/1/14
3
#3 - Suction Regulating Bottle
• Apply suction when large amounts of fluid must be drained. • Regulates the amount of negative pressure being applied to
the water seal. • The water height in the suction control bottle will determine
the amount of negative pressure regardless of suction set on the vacuum regulator.
• Normally set at -20cm H20 • Higher negative pressure can help speed the re-exapansion
process but it can also damage the tissue and prolong healing
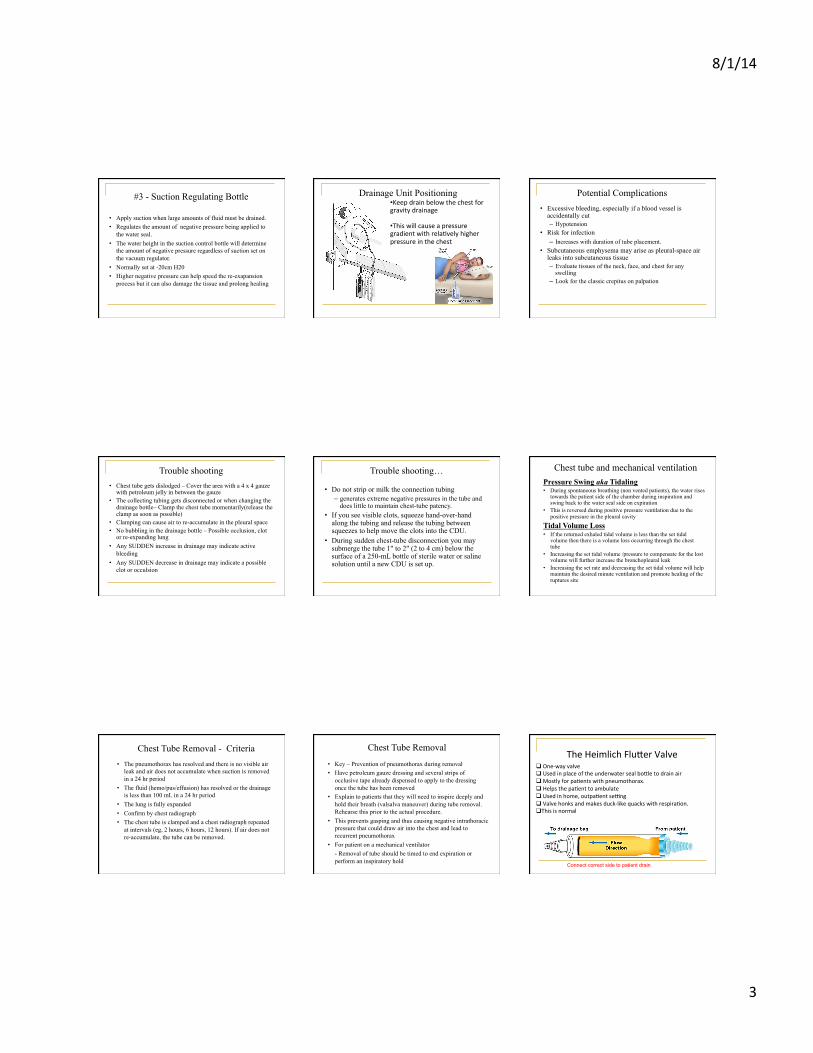
Drainage Unit Positioning • Keep drain below the chest for gravity drainage • This will cause a pressure gradient with relaUvely higher pressure in the chest
Potential Complications • Excessive bleeding, especially if a blood vessel is
accidentally cut – Hypotension
• Risk for infection – Increases with duration of tube placement.
• Subcutaneous emphysema may arise as pleural-space air leaks into subcutaneous tissue – Evaluate tissues of the neck, face, and chest for any
swelling – Look for the classic crepitus on palpation
Trouble shooting • Chest tube gets dislodged – Cover the area with a 4 x 4 gauze
with petroleum jelly in between the gauze • The collecting tubing gets disconnected or when changing the
drainage bottle– Clamp the chest tube momentarily(release the clamp as soon as possible)
• Clamping can cause air to re-accumulate in the pleural space • No bubbling in the drainage bottle – Possible occlusion, clot
or re-expanding lung • Any SUDDEN increase in drainage may indicate active
bleeding • Any SUDDEN decrease in drainage may indicate a possible
clot or occulsion
Trouble shooting…
• Do not strip or milk the connection tubing – generates extreme negative pressures in the tube and
does little to maintain chest-tube patency. • If you see visible clots, squeeze hand-over-hand
along the tubing and release the tubing between squeezes to help move the clots into the CDU.
• During sudden chest-tube disconnection you may submerge the tube 1" to 2" (2 to 4 cm) below the surface of a 250-mL bottle of sterile water or saline solution until a new CDU is set up.
Chest tube and mechanical ventilation Pressure Swing aka Tidaling • During spontaneous breathing (non vented patients), the water rises
towards the patient side of the chamber during inspiration and swing back to the water seal side on expiration
• This is reversed during positive pressure ventilation due to the positive pressure in the pleural cavity
Tidal Volume Loss • If the returned exhaled tidal volume is less than the set tidal
volume then there is a volume loss occurring through the chest tube
• Increasing the set tidal volume /pressure to compensate for the lost volume will further increase the bronchopleural leak
• Increasing the set rate and decreasing the set tidal volume will help maintain the desired minute ventilation and promote healing of the ruptures site
Chest Tube Removal - Criteria • The pneumothorax has resolved and there is no visible air
leak and air does not accumulate when suction is removed in a 24 hr period
• The fluid (hemo/pus/effusion) has resolved or the drainage is less than 100 mL in a 24 hr period
• The lung is fully expanded • Confirm by chest radiograph • The chest tube is clamped and a chest radiograph repeated
at intervals (eg, 2 hours, 6 hours, 12 hours). If air does not re-accumulate, the tube can be removed.
Chest Tube Removal
• Key – Prevention of pneumothorax during removal • Have petroleum gauze dressing and several strips of
occlusive tape already dispensed to apply to the dressing once the tube has been removed
• Explain to patients that they will need to inspire deeply and hold their breath (valsalva maneuver) during tube removal. Rehearse this prior to the actual procedure.
• This prevents gasping and thus causing negative intrathoracic pressure that could draw air into the chest and lead to recurrent pneumothorax
• For patient on a mechanical ventilator - Removal of tube should be timed to end expiration or perform an inspiratory hold
The Heimlich Flu_er Valve q One-‐way valve q Used in place of the underwater seal bo_le to drain air q Mostly for paUents with pneumothorax. q Helps the paUent to ambulate q Used in home, outpaUent seang q Valve honks and makes duck-‐like quacks with respiraUon. q This is normal
Connect correct side to patient drain
8/1/14
4
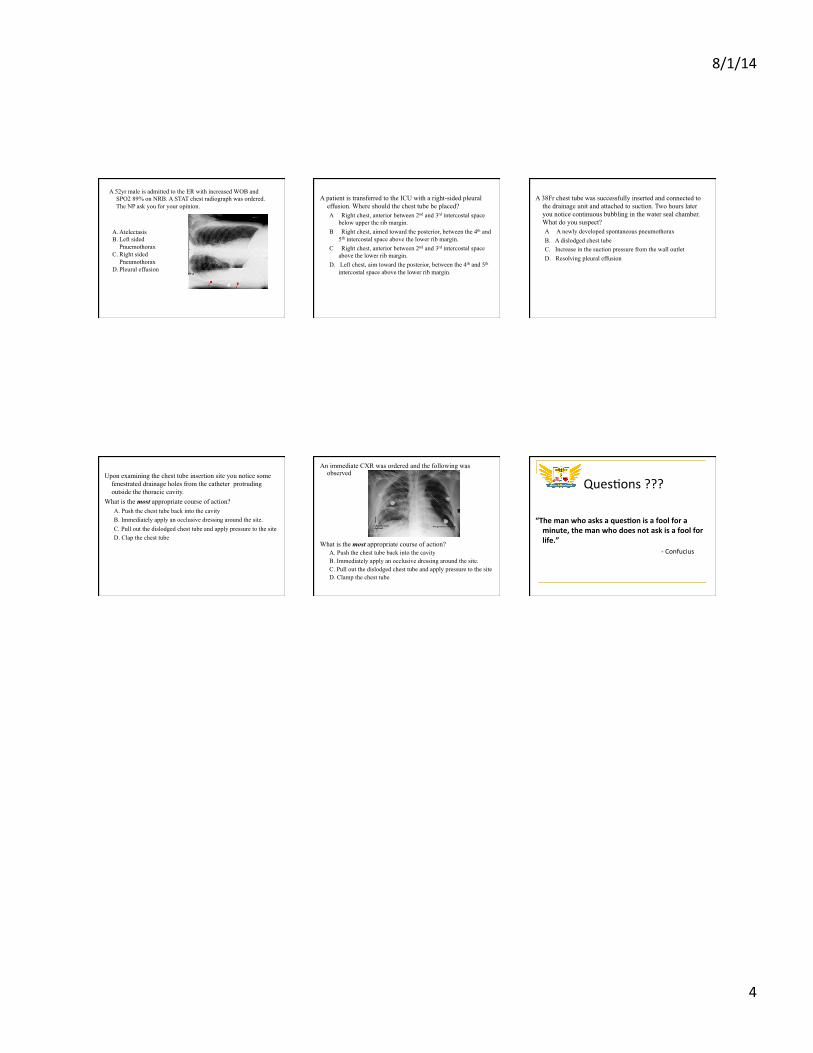
A 52yr male is admitted to the ER with increased WOB and SPO2 89% on NRB. A STAT chest radiograph was ordered. The NP ask you for your opinion.
A. Atelectasis B. Left sided
Pnuemothorax C. Right sided
Pneumothorax D. Pleural effusion
A patient is transferred to the ICU with a right-sided pleural effusion. Where should the chest tube be placed? A Right chest, anterior between 2nd and 3rd intercostal space
below upper the rib margin. B Right chest, aimed toward the posterior, between the 4th and
5th intercostal space above the lower rib margin. C Right chest, anterior between 2nd and 3rd intercostal space
above the lower rib margin. D. Left chest, aim toward the posterior, between the 4th and 5th
intercostal space above the lower rib margin.
A 38Fr chest tube was successfully inserted and connected to the drainage unit and attached to suction. Two hours later you notice continuous bubbling in the water seal chamber. What do you suspect? A A newly developed spontaneous pneumothorax B. A dislodged chest tube C. Increase in the suction pressure from the wall outlet D. Resolving pleural effusion
Upon examining the chest tube insertion site you notice some fenestrated drainage holes from the catheter protruding outside the thoracic cavity.
What is the most appropriate course of action? A. Push the chest tube back into the cavity B. Immediately apply an occlusive dressing around the site. C. Pull out the dislodged chest tube and apply pressure to the site D. Clap the chest tube
An immediate CXR was ordered and the following was observed
What is the most appropriate course of action?
A. Push the chest tube back into the cavity B. Immediately apply an occlusive dressing around the site. C. Pull out the dislodged chest tube and apply pressure to the site D. Clamp the chest tube
QuesUons ???
“The man who asks a ques/on is a fool for a minute, the man who does not ask is a fool for life.” -‐ Confucius