chronological changes in microanatomy of … in microanatomy of pancreatic tissue in human fetuses:...
TRANSCRIPT
Page 1 of 4
Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY)
FOR CITATION PURPOSES: Patil S, Bhatnagar R, Tandon A, Bandopadhyay D, Pokhrel R, Solanke K. Chronological changes in microanatomy of pancreatic tissue in human fetuses: Current insight. OA Anatomy 2014 Mar 15;2(1):7.
Research study
Co
mp
etin
g in
tere
sts:
No
ne
dec
lare
d.
Co
nfl
ict
of
inte
rest
s: N
on
e d
ecla
red
. A
ll a
uth
ors
co
ntr
ibu
ted
to
co
nce
pti
on
an
d d
esig
n, m
an
usc
rip
t p
rep
ara
tio
n, r
ead
an
d a
pp
rove
d t
he
fin
al m
an
usc
rip
t.
All
au
tho
rs a
bid
e b
y th
e A
sso
cia
tio
n f
or
Med
ica
l Eth
ics
(AM
E) e
thic
al r
ule
s o
f d
iscl
osu
re.
Mic
rosc
opic
A
nato
my
Chronological changes in microanatomy of pancreatic tissue in
human foetuses: Current insight S Patil1, R Bhatnagar1, A Tandon1, D Bandopadhyay1, R Pokhrel2*, K S Solanke1
Abstract Introduction Pancreas is the largest digestive gland and consists of exocrine and endocrine components. The exocrine part is responsible for digestion of lipids, carbohydrates and proteins while the endocrine part (islets of Langerhans) produces various hormones responsible for glucose homeostasis; derangement of which leads to crippling diseases like Diabetes Mellitus. Gene therapy and stem cell therapy are newer frontiers in management of diabetes mellitus especially that of Type I. Our study has been planned to provide an insight into microstructure of pancreas during different stages of foetal development and compare the findings with similar studies available in literature in an attempt to facilitate the incorporation of the new frontiers of therapy. Materials and methods Pancreases were dissected out from thirty aborted foetuses of 12 to 40 weeks of gestation, fixed with 4 % formaldehyde, processed, sectioned by paraffin embedding and stained. Mallory’s phosphotungstic acid and Gordon and Sweet stains were used; in addition to routine Haematoxylin & Eosin stains. Observations were noted under light microscope. All foetuses were obtained from the labour room of our affiliated hospital and any foetus with gross anomalies was excluded from the study. Results Acini, islets and ducts of the gland were all seen to be developing from primitive tubules and later established their separate identity.
Pattern of differentiation of these components was similar to that described by previous researchers. Conclusion Histogenesis of pancreas observed during the present study was by and large comparable with earlier studies. It was also found that foetal pancreas of 22-24 weeks gestational age is most suitable for transplantation.
Introduction Pancreas develops from two endodermal evaginations namely dorsal and ventral pancreatic buds. When duodenum rotates to the right, ventral pancreatic bud moves dorsally and comes to lie immediately below and behind the dorsal bud. Later the parenchyma and duct systems of dorsal and ventral pancreatic bud fuse. The ventral pancreatic bud forms the uncinate process and inferior part of the head of the pancreas. The remaining part of the gland is derived from the dorsal bud1. Pancreas is the largest digestive gland and consists of exocrine and endocrine components. The exocrine pancreas consists of acinar cells and ducts which constitute 80 to 90% of pancreatic mass. The acini are responsible for secretion of enzymes of digestion, pancreatic fluids and electrolytes. Pancreatic islets are ovoid clusters of polyhedral cells, more numerous in the tail region than the head and body. Depending upon immunostaining properties and morphology, the cells in the islets are divided into different types as A, B, D, E and F cells and these cells secrete glucagon, insulin, somatostatin, gherlin and pancreatic polypeptide respectively2. Pancreatic islets were discovered by Paul Langerhan Jr. in 1869 and insulin by Banting and Best in 19213.
Pancreatic islets of Langerhans develop in the third month of foetal life from parenchymatous tissue and scatter throughout the pancreas. Insulin secretion begins at approximately the fifth month of intrauterine life4. There is persistent need for gaining insight into the embryology and histogenesis of pancreatic islets because the pancreatic beta cell may be a primary site of pathology in diabetes and the numbers of functioning beta cells affect the initiation or outcome of disease5. We aim to carry out a light microscopic study in order to determine the sequence of histologic differentiation of exocrine and endocrine components of pancreas in an attempt to facilitate the incorporation of the new frontiers of therapy.
Materials and methods This work conforms to the values laid down in the Declaration of Helsinki (1964). The protocol of this study has been approved by the relevant ethical committee related to our institution in which it was performed. Informed written consent was obtained from the parents of foetuses. Thirty foetuses of 12 to 40 weeks with no obvious congenital anomaly were obtained from the labour room of our affiliated hospital. These foetuses included spontaneous abortions and stillborn preterm babies. Foetuses were grouped under five groups based on their gestational age (see results). Gestational age of foetus was obtained from the case sheet of the hospital and further confirmed by measurements of crown rump length using reference from Hamilton and Boyd’s text book of embryology6. The foetuses were fixed in 4% formaldehyde within two to six hours
*Corresponding author Email: [email protected]
1 Department of Anatomy, Armed Forces Medical
College, Pune, India
2 Department of Anatomy, Nepal Army Institute of
Health Sciences, Kathmandu, Nepal
Page 2 of 4
Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY)
FOR CITATION PURPOSES: Patil S, Bhatnagar R, Tandon A, Bandopadhyay D, Pokhrel R, Solanke K. Chronological changes in microanatomy of pancreatic tissue in human fetuses: Current insight. OA Anatomy 2014 Mar 15;2(1):7.
Research study
Co
mp
etin
g in
tere
sts:
No
ne
dec
lare
d.
Co
nfl
ict
of
inte
rest
s: N
on
e d
ecla
red
. A
ll a
uth
ors
co
ntr
ibu
ted
to
co
nce
pti
on
an
d d
esig
n, m
an
usc
rip
t p
rep
ara
tio
n, r
ead
an
d a
pp
rove
d t
he
fin
al m
an
usc
rip
t.
All
au
tho
rs a
bid
e b
y th
e A
sso
cia
tio
n f
or
Med
ica
l Eth
ics
(AM
E) e
thic
al r
ule
s o
f d
iscl
osu
re.
(mean 2.25 hour) by both injection and immersion methods. The pancreas was then dissected out using abdominal incision and similarly fixed in 4% formaldehyde for at least 48 hours after which it was divided perpendicular to its long axis into tissue pieces of approximately 5mm size. Each bit of tissue was stored in a separate labelled container. Tissues were then routinely processed, embedded in paraffin and slides were prepared. Staining was done using haematoxylin and eosin (H & E), Mallory’s phosphotungstic acid and Gordon and Sweet stain. Observations were noted under a light microscope.
Results The foetuses were grouped into five groups. Observations as per the groups of foetuses were as following: 12 to 13 week stage (1 foetus): branched tubules with wide lumen were seen embedded in the mesenchymal tissue. Budding was seen at the ends of these tubules forming primitive acini and islets. Parenchyma began to organize into lobes and lobules. Islets were small and spherical (Figure 1 and Figure 2). 13.1-18 week stage (5 foetuses): Lobes and lobules were more established in parenchyma. Size of islets had increased. Cells in islets were more evenly distributed. Some undifferentiated mesenchymal tissues were seen (Figure 3, Figure 4, Figure 5 and Figure 6). 18.1-24 week stage (6 foetuses): Parenchyma was well organized into lobes and lobules and tubules differentiated into interlobular and intralobular ducts. Islets were increased in size, well encapsulated with the islet cells closely packed. Islets were better differentiated with Gordon and Sweet stain and Mallory’s phosphotungstic acid. (Figure 7, Figure 8 and Figure 9). 24.1 to 30 week stage (7 foetuses): Ducts were numerous and better formed, surrounded by connective tissue condensation. The islets were
markedly increased in number and distributed in the substance of the pancreas. Fully formed acini were arranged in groups separated by connective tissue. (Figure 10, Figure 11 and Figure 12) 30.1 to 40 week stage (11 foetuses): A well-defined architecture of pancreatic tissue was seen at all stages. Some amount of undifferentiated mesenchymal tissue was still observed above 34 weeks. The acini and ductal system was better formed. Islets were larger and prominent concentrated towards the tail region. (Figure 13, Figure 14, Figure 15, Figure 16 and Figure 17).
Discussion Changes in organization of lobes, lobules and acini Manupati S. reported that at 8-10 weeks of gestation parenchyma begins to organize into lobes and lobules with abundant mesenchymal tissue. At 16-18 weeks, acini are better formed and at 28-30 weeks, they were separated by connective tissue7. Gupta et al. observed that, in the early weeks of foetal maturation, primitive tubules exhibit budding of cells, which differentiate into acini, islets or ducts. At 12 weeks, organization of parenchyma began to form lobes and lobules, at 14-15 weeks the organization was well defined8. In the present study, it was seen that at 12-13 weeks parenchyma began to organize into lobes and lobules. Budding at the ends of branched tubules resulting in the formation of primitive acini. At 13-18 weeks, more branched tubules with more established lobes and lobules were seen. At 18-24 weeks, it was found that parenchyma was well organized into lobes and lobules. There was acinar proliferation. At 31-40 weeks, acini were better formed. Presence of mesenchymal tissue In the early weeks of maturation, parenchyma were composed of mesenchymal tissue around lobes and lobules. Undifferentiated mesenchymal tissue was seen upto 40
weeks of age. As maturity increased mesenchymal tissue decreased due to acinar proliferation. This was in accordance with earlier studies available in the literature7, 8.
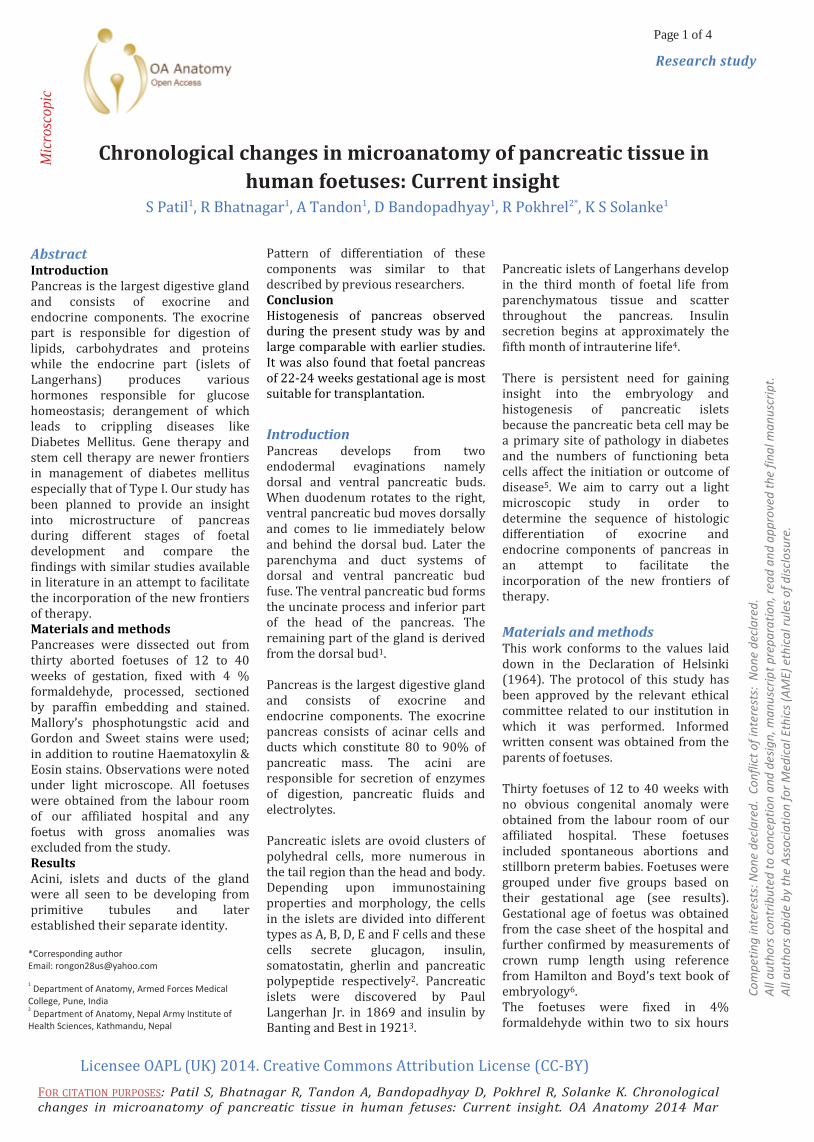
Figure 1: (100X) Photomicrograph of 12th week pancreas. H & E Stain showing mesenchymal tissue.
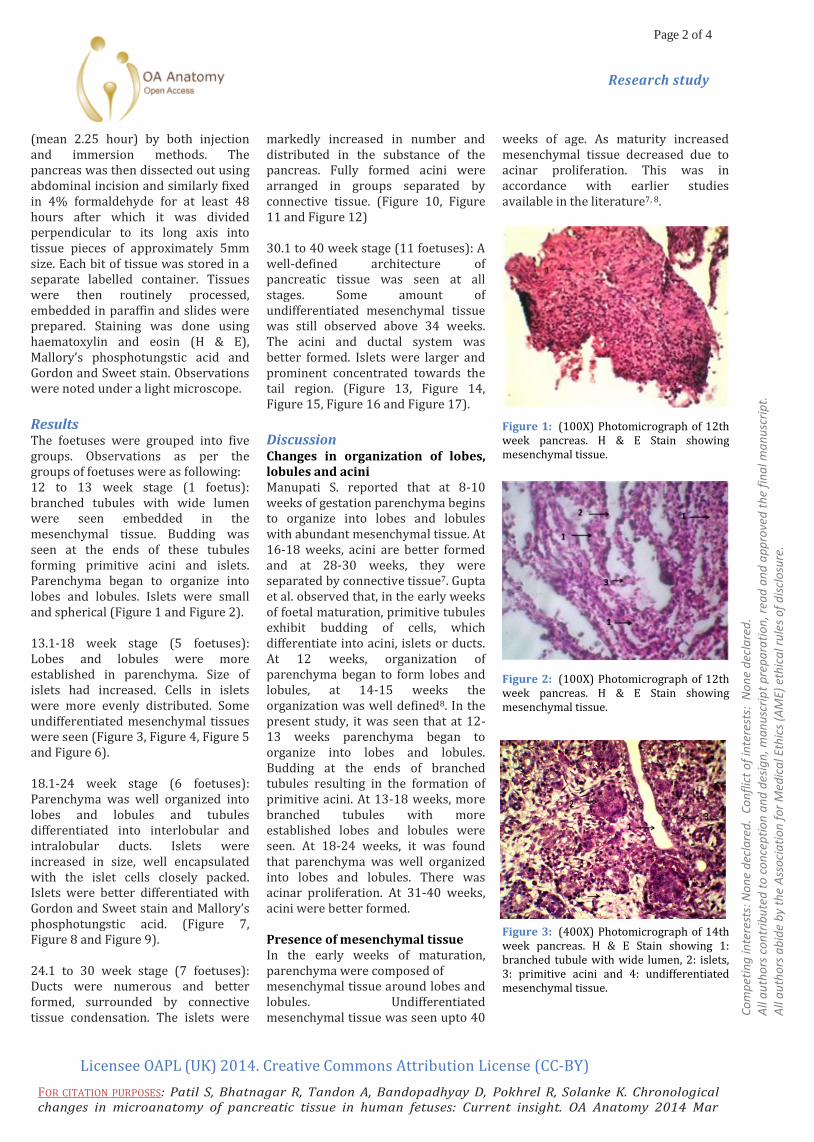
Figure 2: (100X) Photomicrograph of 12th week pancreas. H & E Stain showing mesenchymal tissue.
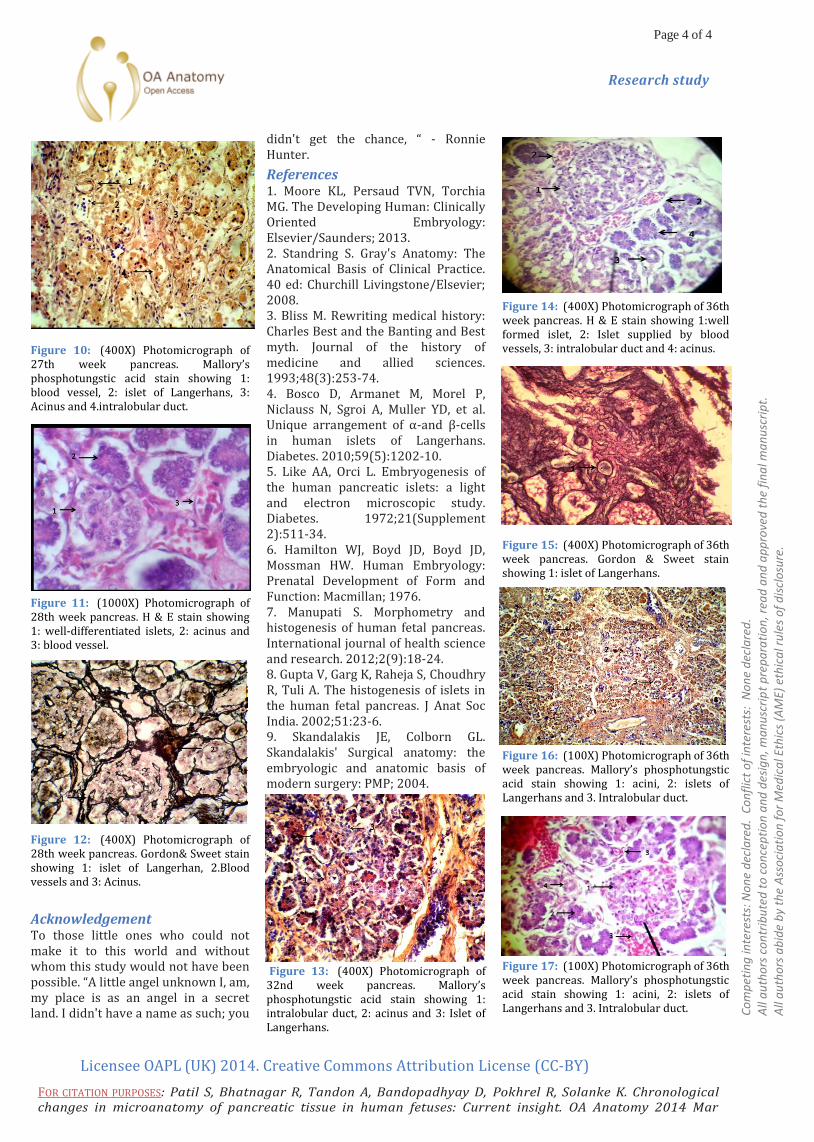
Figure 3: (400X) Photomicrograph of 14th week pancreas. H & E Stain showing 1: branched tubule with wide lumen, 2: islets, 3: primitive acini and 4: undifferentiated mesenchymal tissue.

Page 3 of 4
Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY)
FOR CITATION PURPOSES: Patil S, Bhatnagar R, Tandon A, Bandopadhyay D, Pokhrel R, Solanke K. Chronological changes in microanatomy of pancreatic tissue in human fetuses: Current insight. OA Anatomy 2014 Mar 15;2(1):7.
Research study
Co
mp
etin
g in
tere
sts:
No
ne
dec
lare
d.
Co
nfl
ict
of
inte
rest
s: N
on
e d
ecla
red
. A
ll a
uth
ors
co
ntr
ibu
ted
to
co
nce
pti
on
an
d d
esig
n, m
an
usc
rip
t p
rep
ara
tio
n, r
ead
an
d a
pp
rove
d t
he
fin
al m
an
usc
rip
t.
All
au
tho
rs a
bid
e b
y th
e A
sso
cia
tio
n f
or
Med
ica
l Eth
ics
(AM
E) e
thic
al r
ule
s o
f d
iscl
osu
re.
Figure 4: (400X) Photomicrograph of 17th week pancreas. H &E Stain showing 1: small spherical islets, 2: intralobular duct and 3: Primitive acinus.
Figure 5: (100X) Photomicrograph of 18th week of pancreas. Gordon & Sweet stain showing 1: well established lobes and lobules.
Figure 6: (400X) Microphotograph of 18th week of pancreas. Gordon & Sweet stain showing 1: islet with distinct capsule and 2: acinus.
Formation of duct system Gupta et al. described that ducts were differentiated into intralobular and interlobular by 18-24 weeks8. Parenchyma consisted of a collection of branched tubules lined by cuboidal cells which proliferated to form primitive islets, acini and ducts8. Similar findings were observed in the present study.
Appearance of islets of Langerhans In the third month of foetal life, the islets of Langerhans develop from the collecting tubules to form isolated groups of cells in which secretory granules can be identified. By the fourth month the islet tissue constitutes approximately a third of the total pancreatic mass6. Two different populations of endodermal cells develop: those that form ducts and acini, and those that form islet cells. Ducts and acini form first, but islet primordial bud off ducts as soon as they are formed9. In the present study it was found that at 12-13 weeks of age, islets were small and spherical. As the age of foetus increased, size and number of islets also increased. Islets were well encapsulated. In older foetuses with age group 31-40 weeks, islets were larger and prominent and they were more concentrated towards the tail region as compared to the head and body.
Conclusion There was no local variation in the normal histogenesis observed during the present study and all findings were by and large comparable with earlier studies. The human infant and foetal pancreas is a potential source of pancreatic islets for transplantation for the patients with insulin dependent diabetes mellitus, carcinomas of pancreas, chronic pancreatitis etc. It was noted that foetal pancreas of 22-24 weeks is a suitable donor for transplantation, but it also requires more detailed biochemical and ultrastructural analysis for accurate staging. Thus successful foetal pancreas transplant requires the knowledge of its development, morphology, its insulin producing capacity and its response to glucose at various stages of islet genesis. An understanding of normal histogenesis of the pancreas along with some common variations is a stepping-stone towards this correlation. However a study group involving a larger sample size and the use of electron microscopy with special staining techniques will add to
this understanding and aid in the early definitive diagnosis of certain pancreatic diseases.
Figure 7: (400 X) Photomicrograph of 22ndweek pancreas. H &E Stain showing 1: well-encapsulated islets, 2: acinus and 3: intralobular duct.
Figure 8: (400X) Photomicrograph of 22nd week of pancreas. Gordon & Sweet stain showing 1: typical islet of Langerhans.
Figure 9: (400X) Microphotograph of 22nd week pancreas. Mallory’s phosphotungstic acid stain showing 1: mesenchymal tissue, 2: intralobular duct and 3: islet of Langerhans.
Page 4 of 4
Licensee OAPL (UK) 2014. Creative Commons Attribution License (CC-BY)
FOR CITATION PURPOSES: Patil S, Bhatnagar R, Tandon A, Bandopadhyay D, Pokhrel R, Solanke K. Chronological changes in microanatomy of pancreatic tissue in human fetuses: Current insight. OA Anatomy 2014 Mar 15;2(1):7.
Research study
Co
mp
etin
g in
tere
sts:
No
ne
dec
lare
d.
Co
nfl
ict
of
inte
rest
s: N
on
e d
ecla
red
. A
ll a
uth
ors
co
ntr
ibu
ted
to
co
nce
pti
on
an
d d
esig
n, m
an
usc
rip
t p
rep
ara
tio
n, r
ead
an
d a
pp
rove
d t
he
fin
al m
an
usc
rip
t.
All
au
tho
rs a
bid
e b
y th
e A
sso
cia
tio
n f
or
Med
ica
l Eth
ics
(AM
E) e
thic
al r
ule
s o
f d
iscl
osu
re.
Figure 10: (400X) Photomicrograph of 27th week pancreas. Mallory’s phosphotungstic acid stain showing 1: blood vessel, 2: islet of Langerhans, 3: Acinus and 4.intralobular duct.
Figure 11: (1000X) Photomicrograph of 28th week pancreas. H & E stain showing 1: well-differentiated islets, 2: acinus and 3: blood vessel.
Figure 12: (400X) Photomicrograph of 28th week pancreas. Gordon& Sweet stain showing 1: islet of Langerhan, 2.Blood vessels and 3: Acinus.
Acknowledgement To those little ones who could not make it to this world and without whom this study would not have been possible. “A little angel unknown I, am, my place is as an angel in a secret land. I didn't have a name as such; you
didn't get the chance, “ - Ronnie Hunter.
References 1. Moore KL, Persaud TVN, Torchia MG. The Developing Human: Clinically Oriented Embryology: Elsevier/Saunders; 2013. 2. Standring S. Gray's Anatomy: The Anatomical Basis of Clinical Practice. 40 ed: Churchill Livingstone/Elsevier; 2008. 3. Bliss M. Rewriting medical history: Charles Best and the Banting and Best myth. Journal of the history of medicine and allied sciences. 1993;48(3):253-74. 4. Bosco D, Armanet M, Morel P, Niclauss N, Sgroi A, Muller YD, et al. Unique arrangement of α-and β-cells in human islets of Langerhans. Diabetes. 2010;59(5):1202-10. 5. Like AA, Orci L. Embryogenesis of the human pancreatic islets: a light and electron microscopic study. Diabetes. 1972;21(Supplement 2):511-34. 6. Hamilton WJ, Boyd JD, Boyd JD, Mossman HW. Human Embryology: Prenatal Development of Form and Function: Macmillan; 1976. 7. Manupati S. Morphometry and histogenesis of human fetal pancreas. International journal of health science and research. 2012;2(9):18-24. 8. Gupta V, Garg K, Raheja S, Choudhry R, Tuli A. The histogenesis of islets in the human fetal pancreas. J Anat Soc India. 2002;51:23-6. 9. Skandalakis JE, Colborn GL. Skandalakis' Surgical anatomy: the embryologic and anatomic basis of modern surgery: PMP; 2004.
Figure 13: (400X) Photomicrograph of 32nd week pancreas. Mallory’s phosphotungstic acid stain showing 1: intralobular duct, 2: acinus and 3: Islet of Langerhans.
Figure 14: (400X) Photomicrograph of 36th week pancreas. H & E stain showing 1:well formed islet, 2: Islet supplied by blood vessels, 3: intralobular duct and 4: acinus.
Figure 15: (400X) Photomicrograph of 36th week pancreas. Gordon & Sweet stain showing 1: islet of Langerhans.
Figure 16: (100X) Photomicrograph of 36th week pancreas. Mallory’s phosphotungstic acid stain showing 1: acini, 2: islets of Langerhans and 3. Intralobular duct.
Figure 17: (100X) Photomicrograph of 36th week pancreas. Mallory’s phosphotungstic acid stain showing 1: acini, 2: islets of Langerhans and 3. Intralobular duct.