clinical documentation and order entry: nursing activity
TRANSCRIPT

Page 1
Clinical Documentation and Order
Entry:
Nursing Activity Guide
(Meditech via Zoom)
Page numbers herein refer to relevant pages in the Clinical
Documentation and Order Entry workbook available online

Page 2
Review the case below and complete the activities, using the information provided. Know
that goal of this Meditech training is to become familiar with Meditech, not create a perfect
case study so don’t get caught up looking for details here to enter into Meditech – if
necessary make it up!
Admission: Mrs. Jones has been admitted to your unit via ED with failure to cope after a
fall. You have completed your assessments and she is now settled. You are ready to document.
CARE PLANNING - SELECTING AN INTERVENTION SET (PAGES 4-7)
1. Add the MED Inpatient intervention set
DOCUMENTING AN INTERVENTION (PAGES 8-18)
2. Document the GEN Med/Surg Admission assessment, which was performed at 7:30 in
the morning, be sure to include:
Past Medical and Surgical History
i. Type 2 diabetes, COPD, Hypertension, previous surgery for breast cancer
Admission Vital Signs
i. BP (right arm, sitting) – 140/90; T – 37.6; HR - 104; RR – 36 on 2l/min via
nasal prongs, O2 sat - 90%,
ii. She has been having pain in her tailbone since the fall. Pain at rest 7,
pain with activity 9.
Height/weight and malnutrition screening
i. She is 165cm and 45kg. She says she has lost about 10 kg over the last 4
to 5 months and is eating less than usual in the last 3 weeks
Functional Status (ADL, diet, toileting etc.)
i. Uses a cane, is continent, previously independent with ADL
Personal/Family Situation;
i. Mrs. Jones relies on help from neighbours, lives in a two story home
Alert for Behavioural Care
i. During your assessment Mrs. Jones was uncooperative and not following
instructions
DOCUMENTING A NOTE (PAGES 31-35)
3. Document your admission note
LINKING A NOTE TO AN ASSESSMENT (PAGES 38-39)
4. At 0900, the patient had a fall in the room. The patient is found on the floor with no
apparent injuries. The patient is put back to bed, the bed alarm is activated and 3 side
Page 3
rails put up. Document a Gen Incident Log intervention and link a fall note to the
intervention.
WORKLIST MANAGEMENT/CARE PLANNING (PAGES 25-30)
5. Change the frequency of the vital sign assessment to q4h (refer to page 7).
6. Complete the Admission assessment from the worklist.
7. Add the GEN Fall Post Monitoring assessment added to the worklist
8. You were unable to do the vital sign assessment because the patient was out of the
room, remove the clocks for the vital sign assessment.
CORRECTING INTERVENTION DOCUMENTATION (PAGES 19-24)
9. Review the admission assessment, notice that the temperature was incorrectly recorded
as 37.6 instead of 36.7, make the correction to the assessment.
CORRECTING A NOTE (PAGES 36-37)
10. Upon review of the Fall note it is seen that 3 side rails were put up but it was really 2.
Amend the note to correct the documentation.
ALLERGY AND HOME MEDICATION DOCUMENTATION (PAGES 43-54)
11. The patient’s POA has allergy information which need to be entered Allergies:
Shell Fish
Penicillins
12. The POA has also bought in a current list of home medications from the patient’s pharmacy. These meds were last taken 2 days ago.
Lasix 40 mg PO Daily
Insulin NPH 10 units in AM and 5 units at HS via insulin pen
Metformin 500 mg PO BID (was prescribed as 1000mg PO BID)
Latanoprost 0.005% eye drops 1 drop in left eye qHS
Milk Thistle 250mg daily (HINT; Additional Information”)
Finished 7 day course of Amoxicillin (started eight days ago)

Page 4
SPECIAL INDICATORS (Page 42)
13. Add the M-COVID-19 Suspected special indicator. 14. IPAC have cleared the patient as no longer suspected so remove the M-COVID-19
Suspected special indicator
INDIVIDUAL ORDER ENTRY (PAGES 74-79)
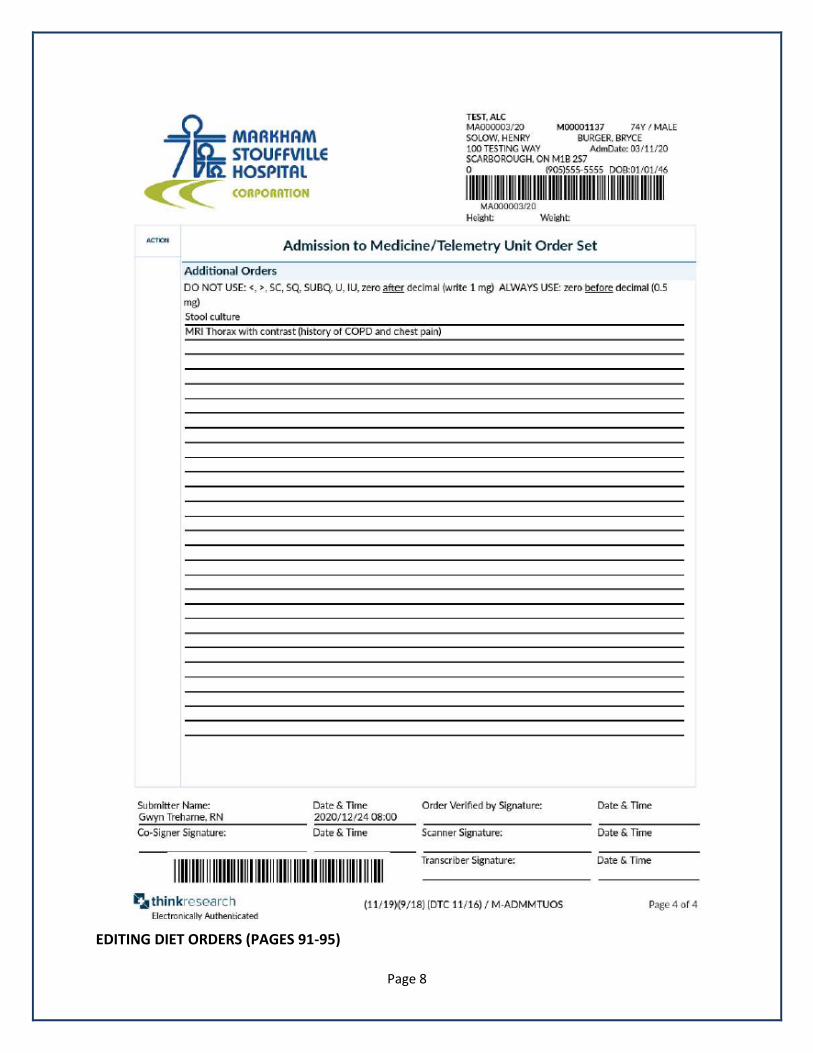
15. Enter the orders on the Medicine/Telemetry Admission order set ON THE NEXT 4 PAGES
(note that on this unit the care provider will collect blood specimens themselves and
stool samples are yet to be collected)
Note that some of these orders will be entered as Orders and some on the Gen
Interprofessional Kardex only.
Remember to note on the order sheet whether the order was entered in Order
Management (OM) or onto the Kardex (K)
There are a total of 10 orders to be entered into the Order Management (OM) system
and several orders that must be entered into the GEN Interprofessional Kardex

Page 5

Page 6

Page 7
Page 8
EDITING DIET ORDERS (PAGES 91-95)

Page 9
CHANGING DIET ORDERS
16. Change the diet order to diabetic diet, honey thick liquids, minced texture and Resource
2.0 Honey with each meal.
17. Change the diet order to enteral feed, Iso-source 1.5 at 50mL per hour for 24 hours
ENTERING MEDICAL DIRECTIVES AND OBTAINING SPECIMENS
18. You implement a medical directive for MRSA/VRE cultures as the patient was at another
hospital in the last month. Enter the orders for this medical directive using the
Multidrug Resistant Organism Screen order set. (You have not yet collected these
samples)
ORDERS AND THE WORKLIST (PAGES 95-96)
19. The patient has now had a bowel movement and the stool sample was taken. Return to
the worklist and document the collection of the stool sample and the MRO swabs
ACKNOWLEDGE ORDERS (PAGES 96-97)
20. Acknowledge the orders entered and sign off the order to indicate that the orders have
been verified.
EDITING/CANCELING ORDERS (PAGES 81-86)
21. The CBC is really for tomorrow, change the start date and time.
22. The physician no longer wants the CXR, cancel this order
23. Edit the clinical history of the MRI order and enter previous breast cancer

Page 10
BONUS ACTIVITIES (only complete if you have completed and are comfortable with all
previous activities)
24. Document another intervention; Document the IPAC Nursing Precautions as Routine
25. Home medications; A letter from the patient’s family physician has now been faxed to
the unit. Update the home medications to reflect the changes below:
Insulin NPH 14 units in AM and 10 units at HS via insulin pen
Flovent 125 mcg 1 puff (HFA) INH BID
Fentanyl 75 mcg patch q72h 26. End of shift documentation;
Document your GEN Shift Handover intervention.
Preview the “Nursing Worksheet by Name” for your patient