clinical observations on fluothane anaesthesia observations on fluothane anaesthesia* ... producing...
TRANSCRIPT

CLINICAL OBSERVATIONS ON FLUOTHANE ANAESTHESIA*
FmaNAN~ HtroON., M.D., F.ILC.P. ( C ), F F A.'R.C.S., u.D., Fm.C.,.(cT,
MARCEL CLAVET, M.D., a n d JACQUES HOUDE, lVi D ~
THE DEPARTMENT OF ANAESTHESIA at the H6tel-Dieu Hospital m Quebec City has used Fluothane m many different types of anaesthettc machine with various techniques in a total of 1,112 surgical patients of all ages.
Fluothane is a volatile anaesthetic agent; it is a halogenated ethane, 2-bromo- 2-chloro-l-l-l-trlfluoroethane, with the structural formula:
F\ /B~ F C J C C1
F / \ H
PHYSICAL, CHEM_ICAL AND DHAP~ACOLOGICAL PIaOPERTIF_~
It is a clear, colourless liqmd, with a spec~c odour. It is non-inflammable and non-explosive. It is a stable compound but theorehcally, when exposed to air, moisture or light, It may in ttrrte break down into various acids of the halide group. The decomposlbon products may affect certain metals, such as tin and aluminum. Liqmd Fluothane may attack rubber, producing soJ[tening and swel- ling. The rubber reverts to normal when withdrawn from the Fluothane. Clinically, the deeompomtlon pzoducts have no toxic effects even though they are theoretically harmful. Thymol added to Fluothane, in a proportion of 0.01 per cent, protects Fluothane from the effects of light. Storage in a cool place, in amber-coloured bottles, also retards decomposition indefinitely. Fluo- thane is stable in contact with warm or cold soda lune, and it may be used safely m a closed circuit with a CO2 absorber. On the skin, this anaesthetic does not produce the burmng sensation which is felt after the application of ether or chloroform. It is non-irritating t ~ the buccal, laryngeal or tracheal mucosa. It does not cause pulmonary oedetna. Its therapeutic index is twace that of ether, and it is four lames more potent. The anaesthetic ratio is from 1 to g per cent (i--3).
Table I shows the physical and chemacal characteristics of Fluothane as compared with those of chloroform, ether, Vinethene, Vlpamar and Fluoromar.
STATISTICAL DATA
In these studies, Fluothane has been admimstered using various types of anaesthetic apparatus: the Heidbrink No. 7 bottle with the wick atomizer, on
*Fluothane used m this study was plovxded by Ayerst, McKenna & Harnson Ltd., Montreal. Date sent for pubhcatlon April 27, 1957
~D6partrnent of Anaesthesia, H6tel-Dleu Hospital, Quebec Cxty lDoctors Laureat Jean, Jean-Lotus Bolvln, Pmrre-Paul Paquet, Andre McChsh, Jacques
Pelletler and Egbert Da2gle have contnbuted~ their help to t, hls study on Fluothane.
221
Can Anaes Soc J , vol 4, no 3, July, 1957

Ana
esth
etic
Chl
orof
orm
Eth
er
Vin
ethe
ne
Vin
amar
Flu
oram
ar
Flu
otha
ne
Ty
pe
Che
mic
al
form
ula
Mol
ecul
ar
wei
gh t
Boi
ling
po
int
Spe
cifi
c gr
avi t
y-
liqu
id
(wat
er =
1)
Sol
ubil
ity
in
100
part
s w
ater
Sol
ubil
ity
oil-
wat
er
37 ~
C,
Chl
orin
ated
hy
droc
arbo
n
Die
thyl
-eth
er
Div
inyl
-eth
er
Eth
yl-v
inyl
-eth
er
Flu
orin
ated
hy
droc
arbo
n
Hal
ogen
ated
et
hane
CH
CIa
(GH
.02
0
(C2H
a)20
C2t
-I~-
-O--
C2H
a
CF
a--C
H--
O--
C
H--
CH
2
CF
a--C
H--
Br-
- C
1
119.
39
74.1
2
70.9
72.1
0
126.
0
197.
39
61.2
6
34.6
28.3
35
.8
~.7
50.2
1.49
0.71
3
0.77
4
0. 7
59
1.1,
3
1.86
O, 8
22
7.5
4.0
0.4
O. 3
45
100
3.2
41.3
45
94
330
Lim
its
of
flam
mab
ilit
y
Air
O
xyge
n
1.85
- 2
.10
- 36
.5
82.0
1.
7 1.
85
27.0
85
-
-
2.1
.3.0
Non
- in
flam
mab
le
w~t
h 0~
2 0.
5 -.
50.0
Vap
our
tens
ion
at 2
0 ~
C.
ram
. H
g
160.
5
439 4.
85
243

YIUDON et al . :FLUOTHANE 223
inspLralaon and expiralaon, the Marrett and Boyle, in closed and semi-closed clrcmts, the McKesson, E M O, Friedman apparatuses, andlthe M I.E. pacdaatrlc machine. The Fink valve was used for measuring pulmonary ventilation during anaesthesia.
Fluothane has been used alone with a nitxous oxide-oxygen mixture and in various other comblnataons.
Combzned A naesthetzcs
N.~O +O._+Fluothane 817 Neraval 4-N20 +O2 +Fluothane 92 Pentothal-kN.~O +O~ +Fluothane 181 N20+O2 q-Fluothane+C~ H6 7 N.oO+O2 -kFluothane+(C2 H~)_~O 4 Fluothane +local (kn,~e) 1 Fluothane+brachaal ~ock 4 Fluothane +spinal 3 Fluothane +caudal 1 Fluothane +Vmdrfl 2
1,112
Fluothane has been employed in 1,112 surgical cases for different lengths of tame, in patients of all ages and of both sexes (514 male, 598 female). Several patients were anaesthetized with Fluothane more than once, the intervals between anaesthesia varying from a few days to a few weeks (57 twice, 5 three times, and one four times ).
Many pataents received no pre-anaesthetac medication, for others, premedicataon did not,differ from that currently used wath other methods of general anaesthesia.
Preoperatwe clinical examanatmns demonstrated certain disease processes in some pataents, pulmonary emphysema, pulmonary sclerosis, bronchitis, asthma, mltral stenosls, chrome endocarditts, coronary sclerosis, old infarct, bronchial obstructmn, ventrlcular strain, diabetes, and vascular disorders of the extremities
CLINICAL STUDIES
Studies of the effect of armesthesla and of the aclaon of Fluothane on the autonomic and central nervous systems, as well as on the cardio-respiratory and renal systems, give quite a clear concept of the ~ehnical value of this new, volatlIe, anaesthetac agent.
Induc twn and Maintenance of Anaesthesia
Induction with Fluothane and nitrous oxide-oxygen (5.5 litres or 3.g hixes, accorchng to the apparatus and the technique employed) should be slow and gradual rather than rapid, so that the concetitration is kept within 1-4 per cent and adequate pulmonary ventalatlon mamtamed, whale the pulse and blood pressure are kept under observalaon Because a percentage"cahbrated vaporizer was not available, an ether vaporizer bottle No 7 with wicks was used m the Heldbrlnk machine The control is opened gradually up to No. 4 and, for maintenance, it is turned back to Nos 2 or g With both the Marrett and Boyle's
224 CANADIAN ANAESTHETISTS' SC~;EETY JOUI~'q'.A_L
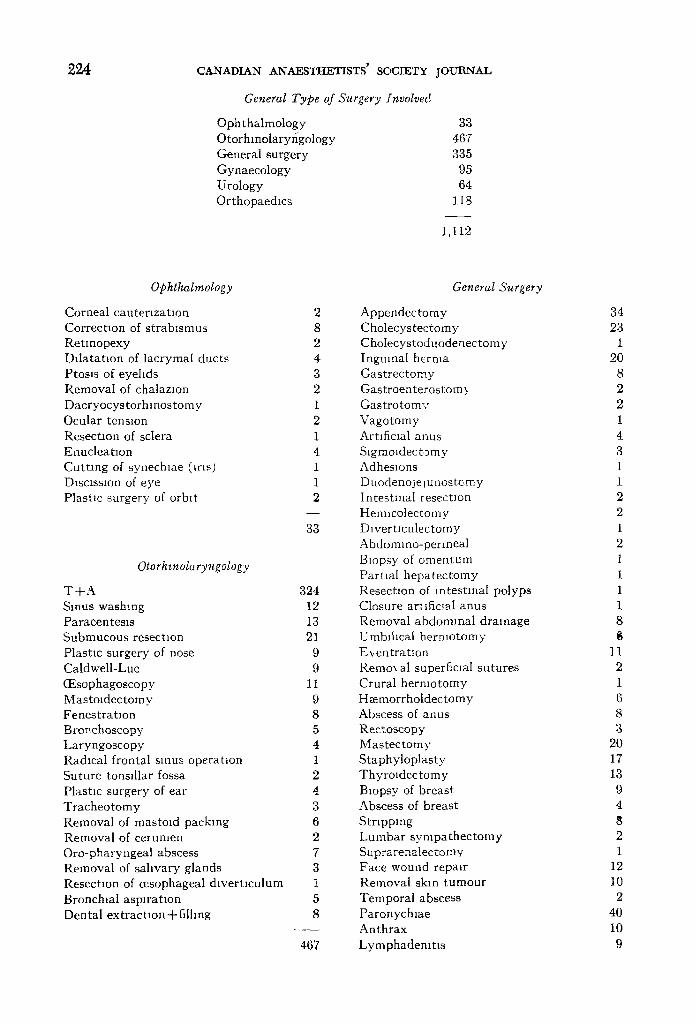
General Type of Surgery fnvolved
Ophthalmology 3,3 Otorhmolaryr~gology 467 General surgery 335 Gynaecology 95 Urology 64 Orthopaedics 118
1,112
Ophthalmology
Corneal cautenza tmn 2 Correctxon of strabismus 8 Retmopexy 2 Dda ta tmn of lacrymal ducts 4 Ptoms of eyelids 3 Removal of chalazIon 2 Dacryocystorhlnostomy 1 Ocular tensmn 2 Resectaon of sclera 1 Enucleatlon 4 Cutt ing of synechme (Lr~s) 1 Dmctssmn of eye 1 Plasnc surgery of orblt 2
33
Otorhznolaryngology
Tq-A 324 Sinus washing 12 Paracentesis 13 Submucous resectmn 21 Plastm surgery of nose 9 Caldwell-Luc 9 (Esophagoscopy 11 Mastoldectomy 9 Fenestratmn 8 Bronchoscopy 5 Laryngoscopy 4 Radical frontal smus operanon 1 Suture tonsdlar fossa 2 Plastic surgery of ear 4 Tracheotomy 3 Removal of rnastoxd packing 6 Removal of cerumen 2 Oro-pharyngeal abscess 7 Removal of sahvary glands 3 Resectmn of oesophageal dlvertmulum 1 Bronchtal asplratmn 5 Dental extractmn +fi lhng 8
467
General Surgery
Appendectomy Cholecystectomy Cho[ecystoduodeaectomy Ingmnal herma Gast rec tomy Gastroente:rostom3 Gas t ro tomv Vagotomy Artxficlal anus Slgmoldectomy Adhesions Duodenojelunostomy Intestinal r esectlon Hemmolectomy Dlvertmulectomy Abdommo-permeal Biopsy of omentum Parual hepatec tomy Resection of intestinal polyps Closure ar~ ificlaI anus Removal abdominal drainage Umblhcal he rmotomy E~entrat lon Remox al superficJal sutures Crural hermotomy Haemorrholdectomy Abscess of anus Rectoscopy Mastec tomy Staphyloplasty Thyroxdectomy Biopsy of breast Abscess of breast Stripping Lumbar sympa thec tomy Suprarenatectomv Face wound repair Removal skin tumour Temporal abscess Paronychlae Anthrax Lymphademt ts
34 23
1 20
8 2 2 1 4 3 1 1 2 2 1 2 1 1 1 1 8
11 2 1 6 8 3
20 17 13 9 4 8 2 1
12 10
2 4O 10
9

mJllON et al.: FLUOTHANE 225
General Surgery (conhnued)
Btopsy gland of neck 6 Radical exc,smn of neck 5 Cyst of neck 1 Ltgatton ocmpttal ar tery 1 Biopsy of tongue 2 Pdomdal cyst 2 Skm graft 5
335
Gynaecology
G.vnaeco[ogmal e,mmmatxon and uterine curettage 47
Hys terec tomy 29 Colpopermeorraphy 10 Werthetm 2 Vulvectom.x 1 Oophorectomy 3 Bar thohman abscess 1 Cotte 's operatmn 1 Salpmgo-oaphorectomy 1
95
Urology
Cystos tomy 3 Castrat ion 1 Cystectomy 1 Inverston of tumca vagmahs (hydrocele 3
repair) Ureterostgmoldostomy 1 Pros ta tec tomy 3 Nephrectomy 2 Pyelotomy 1 Pylography 1 Lumbo tomy 1 Cystoscopy 23 Ctrcumctsmn 24
64
Orthopae&cs
Bone marrow punlzture Bursectomy Cos to tomy thoracic drainage Open reduction Club foot stretching of tendons Finger repair TorUcoll,s ResecUon of bone Leg cast S:y novlal cyst (wrist) Dislocation of mamlla Memsec tomy of knee Saucensauon of femur AmputaUons Removal K1rschner wire Plaster corset L a m m e e t o m y Hallux valgus Wound dgbndement
0 - 6 m o 6 m o - 1 year 1-5 5-10
10-15 15-25 25-35 35-45 45-65 65-75 75-85
Age
Duratwn of Anaesthesta
0-30 minutes 30-45 45760
122 hours 2-3 3-4 4-5 5-6
3 5 4
31 9 5 1
12 9 4 1 7 1 8 5 2 1 1 9
118
7 23
134 154
56 161 144 133 220
70 10
1,112
246 378 128 233
84 28 10
5
1,112

226 CANADIAN ANAESTHETISTS' SOCIETY JOUItNAL
machine, Fluothane is placed m the Tnlene bottle, this is opened to approximately the same figures, the plunger in the Trdene bottle wtth the Boyle apparatus being completely withdrawn.
There seems to be no analgesic period. The second phase differs from that of ether, there being no mental confusion, dehrium, tears, cries, coughing, sneezing, eructat/on, nausea, vomiting, salivary or tracheo-bronehial secretions or con- vulsions noted. Surgmal anaesthesm resulted in four to eight minutes Intubation could be done easily without producing coughing or ]bucking movements and, usually, without using a relaxant
_Premed~catzon
None Atropine on13 Codeine +atropine Morphine ~-atroplne Morphine ~-atroplne + Benadr31 Morphine +atropine + Pacatal Morphine +atropine +Stemetll Demerol only Demerol +atropine Demerol +atropine + BenadrF 1 Levodromoran only Lex odromoran +atropine Levodromoran +atropine + Benadr 51 Levodromoran +atropine + Pacatal Levodromoran +atroplne + Sparlne
111 16 2
417 13
6 1 3
459 3 1
16 43 20
1
1,112
When Pentothal or Neraval is used, with or without I elaxants, for the inductmn of anaesthesia, Fluothane should not be admmlstered unM the blood pressure has stabilized and the respiratory rate has become regular and adequate for proper inhalatmn of the anaesthehe.
On the basis of certain obvious anaesthetic signs, it would seem that Fluothane has some "ganghoplegm" activity Whether or not 'the patient has received premedicahon, the pupds remain small and do not ddate progressively as they do during deep anaesthesia with ether The conlunctlvae become cbngested There is absolutely no persplrataon and salivary and traeheo-bronehlal secretaons are inhabited The skin is warm and dry and the peripheral vaso-chlatataon is present (4). There are no hiccoughs and no spasm of the larynx or of the bronchi. Stndor of the larynx has occurred in a non-intubated pahent under deep anaesthesia for osteosynthesis of the hbia. When the concentration of the anaesthetm was reduced, this symptom disappeared, l~'luothane did not produce
No mtubatlon 377 Intubatlon wxth N.O+O2+Fluothane 486 Intubatlon with N20+O2+Fluothane-t-
relaxa n t 249
1,112
rFCDON et al. : FLUOTHANE 227
Inccoughs which somelames occur during gastrectomy under anaesthesia with the thlobarbiturate-curare-nltrous oxide-oxygen combination.
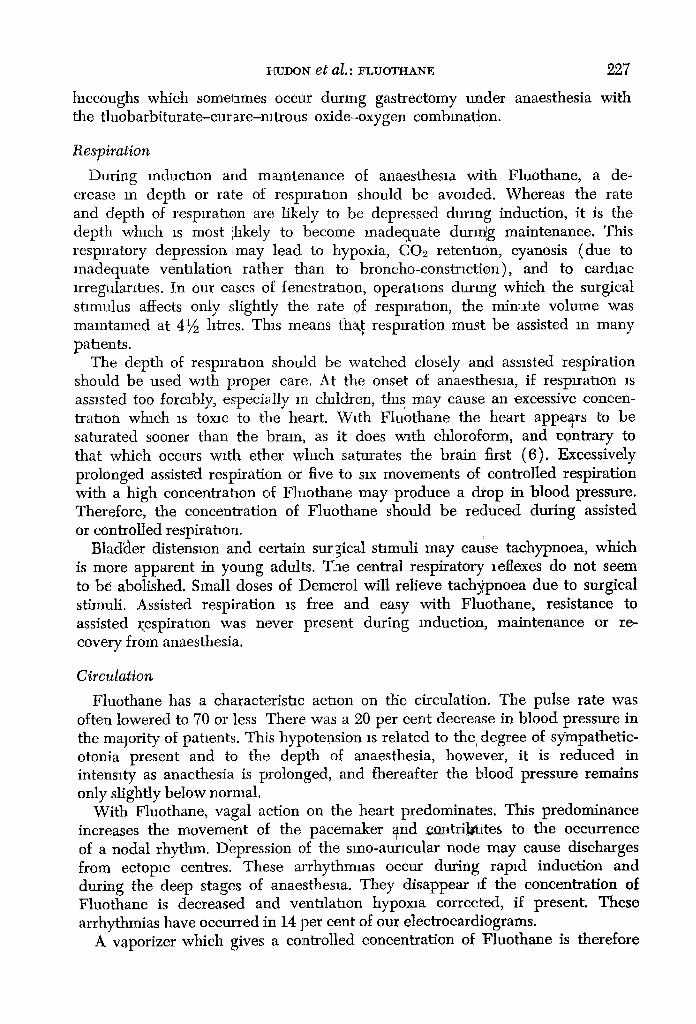
Respirat ion
During mduchon and maintenance of anaesthesm with Fluothane, a de- crease m depth or rate of resplrahon should be avoided. Whereas the rate and depth of respiration are; likely to be depressed during induction, it is the depth whmh xs most ihkely to become inadequate during maintenance. This respiratory depression I may lead to hypoxia, CO2 retention, cyanosis (due to inadequate venhlation rather than to broncho-constrmtion), and to cardmc lrregularlhes. In our cases of fenestration, operahons during which the surgical stimulus affects only slightly the rate of resprratlon, the minute volume was maintained at 4�89 htres. This means tha~ resprration must be assisted m many pahents.
The depth of resprrahon should be watched closely and assisted respiration should be used with propeI care. At the onset of anaesthesm, if resprrahon is assisted too forcibly, especivlly m c/~uldren, th~s may cause an excessive concen- trahon winch is toxin to the heart. With Fluothane the heart appears to be saturated sooner than the brain, as it does w~th chloroform, and contrary to that which occurs with ether which saturates the brain first (6). Excessively prolonged assisted respiration or five to sax movements of controlled respiration with a high concentrahon of Fluothane may produce a drop in blood pressure. Therefore, the concentration of Fluothane should be reduced during assisted or controlled respirahon.
Bladkler distensmn and certain surgical shmuli may cause tachypnoea, which is more apparent in young adults. T_ae central respiratory leflexes do not seem to be abolished. Small doses of Demerol will relieve tachypnoea due to surgical stimuli. Assisted respiration xs free and easy with Fluothane, resistance to assisted ~espiratlon was never present during reduction, maintenance or re- covery from anaesthesia.
Circulation
Fluothane has a characterishc aclaon on the circulation. The pulse rate was often lowered to 70 or less There was a 20 per cent decrease in blood pressure in the malority of patients. This hypotension is related to the degree of sympathetic- otonia present and to the depth of anaesthesia, however, it is reduced in intenmty as anaethesia is prolonged, and thereafter the blood pressure remains only slightly below normal.
With Fluothane, vagal action on the heart predominates. This predominance increases the movement of the pacemaker and ~trihCtites to the occurrence of a nodal rhythm. Depression of the smo-aurlcular node may cause discharges from eetopm centres. These arrhythmms occur during rapid induction and during the deep stages of anaesthesia. They disappear Jf the concentration of Fluothane is decreased and venhlahon hypoxm corrected, if present. These arrhythmias have occurred in 14 per cent of our electrocardiograms.
A vaporizer which gives a controlled concentration of Fluothane is therefore

228 CANADIAN ANAESTHETISTS" SOCIETY IOUt~NAL
not only useful but essential. The concentration sh~ as a maximum (5). The following arrhythmias 1,112 patients: nodal, superior nodal, slight br~ geminal pulse and extrasystoles of ventricular or
Our patients with old infarcts, cor-pulmonale al not appear to be adversely affected by the admini
told be limited to 8.5 per cent were found in our series of idycardia, bigeminal and tri- [gin. kd coronary artery disease did ~tration of Fluothane. Patients
with emphysema accompanied by venous hypertension seemed to improve tempo- rarily while under anaesthesia and for some time after.
ECG tracings were taken during prolonged anaesthesia with Fluothane, that is, during the fenestralaon operations.
A report on the "Summary of findings from 30 EICG's taken during anaesthesia with Fluothane, by Drs. Georges Saulnier and J~an Beaudoin, cardiologists in the Department of Medicine at Hotel-Dieu Hospital, :s presented here:
1 Graphs taken preoperatively I. 21 strictly normal graphs.
II 9 abnormal graphs, distributed as follows (a) 1 case sinus tachycard:a rate 142 (b) 1 case extrasystole (c) 1 case deeper P wave, possibly hypertrophy of t:ght attr:cle (d) 6 cases non-spec:fic changes of terrmnal phase, ~lvmg so-called '%orderhne"
graphs
2 Graphs taken dunng surgery I. A moderate slowing of card:ae rhythm was found m most cases
II. The abnormal graphs were not modafied during anaesthesia. III. Four electrical modlficat:ons are worthy of mentaon
(a) Development of a nodal rhythm, 58/minute, 10 minutes after onset of anaes- thesia. A graph taken 20 minutes after onset of anaesthesia shows that everything rs back to normal ( Fig 1 )
Fmwrm 1 FictmE 2

230 CANADIAN ANAESTHETISTS" SOCIETY JOURNAL
traction on the bladder (distension), Fowler's positaon, and hyperventilation Capillary oozmg is markedly reduced, even after a three-hour permd of anaes- thesia with Fluothane. The use of adrenalin is dangerous and must be avoided durmg anaesthesia with Fluothane. Bladder dIstensmn may cause a blood pressure rise of 80-50 mflhmetres of mercury.
Adiuvant Medication
Various drugs have been used to counteract the side effects of Fluothane on the circulation and carchac rhythm (hypotension, exh asystoles ); these drugs were central vagolytacs and tranquilizers, that is, Pacatal, Benadryl, Centrine, atropine and Demerol
Supporting Med~catzon None 905 Demerol 23 Atropme ',38 Benadryl 78 Pacatal 55 Arfonad 4 Dlparcol 3 Centrme 4 Benatrol 2
1,112
With the exceplaon of atropine and Benadryl given intravenously, which increased blood pressure and heart rate but did not enlarely control pulse irregularities, adluvant medication did not give the expected results Demerol has decreased the respiratory rate, this depression is partly compensated ,for by an increase m depth but the compensation remains inadequate. Such medi- cation is not an adequate substitute for proper anaesthetic techmque. In some patients, pulse trregulanties were controlled only by reducing the concentration or briefly stopping the administration of Fluothane.
Renal System
Experiments in rats have shown that renal f u n c t i o n was not impaired by the repeated administration of Fluothane (2) In eight cases of s which were kept under Fluothane anaesthesxa for approximately 4�89 hours, urinalyses made on the day of the operation and on the third postoperatave day have shown no sign of any patholog, cal condition that is, albumin, casts, or abnormal specafic gravity.
Muscular Relaxation
Fluothane gives good muscular relaxataon for lower abdominal operations. In upper abdominal operations, the relaxalaon obtained is not always satisfactory and, with Fluothane alone, adequate relaxation may occasionally be secured only at the cost of marked hypotension or cardiac arrhythmla. Twenty to forty mllhgrams of Flaxedll are usually needed, this dose changes pulmonary ventilation

HUDON et al.. FLUOTHANE 231
very shghtly or not at all, and it provides adequate relaxataon without increasing concentration of Fhiothane.
Rela.xants
None ,837 Anectme 47 Anectlne-4-s~ ncurme 29 Brevldtl 37 Brevldfl --[-s 3 ncurme 20 Syncurme 2 Tubo curare 11 Flaxedfl 129
1,112
It is not always necessary to repeat this dose in closing the peritonemn. Experience should determine the proper administration of a relaxant, as reqmred. Tubo-curare, which has 'ganghoplegi~' actwlty, is not recommended. Succinyl- choline and decamethonium, having no hypotenswe actlwty, are well suited to anaesthesia with Fluothane, with the understan&ng, however, that they should be used in small doses, either to increase muscular relaxation or to facilitate intubation.
Recovery
Consciousness returned from five to twenty minutes postoperatively. The patients awakehed quietly, nausea was infrequent and might have been due to various other factoxs. The blood pressure remained exactly as ff the patients had not been anaesthettzed. The postoperalave crrculation was better than that observed after the use of other anaesthetacs. This may be due to the fact that with'other anaesthetics a depression in circulation follows the circulatory stimula- taon concurrent with anaesthesia, or it may 15e attributed to postoperative blood accumulation in the splanchnic area. On the other hand, with the use of Fluothane, there may be bettm circulation an the smaller blood vessels or the drug may have a superior action on the autonomic nervous system. There is no cyanosas of the extremitaes, no shivering or anything else which might resemble cyclo-shock The blood pressure and peripheral circulation tend to remain normal; these facts support the statement that Fluothane has anti-shock a c t i v i t y ( 4 ) .
If excessive muscular relaxation persists after the anaesthesia, and especially if 80 milligrams or more of Flaxe&l have been used, 1 milligram of prostigmine and 0 4 milligram of atropine should be given, and whale assssted respiration is maintained, Fhiothane is eliminated.
Postoperative Period
It is our impression that postoperative pulmo~3~ z, omplications are less and that respiratory function in emphysema is improved in t_he beginning of anaes- thesia. It is generally considered that the postoperative pulmonary complications which occur during the first few days have really started soon after awakening and may be due to the retentaon of respiratory secretions caused by the

28~ CANADIAN ANAESTHETISTS' SOCIETY JOUJRNAL
anaesthetics, a muscarinic effect of the relaxants, the parasympathomimetic drugs, or paxnful reflexes On the other hand, Fluothane depresses the cough and broncho- constrictor reflexes, even those generally reduced by the induction of a laryngoscope or endotracheal tube. This beneficial effect is seen dtmng bronchial aspiration carried out during Fluothane anaesthesia. Smce sahvary and tracheo-bronchial secretions are minimal with Fluothane, even without premedicaUon, it is easy to understand that postoperative pulmonary atelectas~s should be decreased Our study of 1,112 cases would seem to substantxate this impression.
Ten paUents, who had another type of anaesthetic a ~ew days previously, had a bronchial asp~ratmn under Fluothane anaesthesia As soon as the aspiration was completed and the irritation caused by the catheter had subsided, the pataents returned spontaneously to normal respiration, there was no cough. spasm, or any production of fresh secretions. This procedure, which completely oxygenates the patient before aspiration, facilitates the tec~anque to such an extent that in our Department of Anaesthesm it is preferred to all other methods used previously, including trans-trachea], thiobarbxturates, N90-Oo.-Cz Ha, and topical anaesthesia.
No postoperative mental depression occurred m our series of pati6nts Ratients who had been anaesthelazed twice for fenestraUons, once with t 'entothal- nitrous oxide--oxygen and once with nitrous oxide-oxygen-Fluothane, stated that with Fluothane they felt less depressed the next day This reaction might indicate a lower degree of toxicity-a sympathetacotonic state which might explain the anti-shock effect and the improvement in pulmonary function.
Cardiac Arres t
Two cases of cardiac arrest occurred early in this ,series but, with the use of appropriate therapeutic measures, recovery was complete.
1 Female patient, 40 years of age, m a state of severe vagotoma, scheduled for racheal mastectomy Premedmataon levo-dromoran 2 mflhgrams, atropine 0 4 milhgram Induction: Pentothal 250 rndhgrams, succmylchohne 60 milligrams Intubalaon followed by controlled respiration w~th N20-O2-Fluothane The patient was placed m the reverse Trendelenburg position Suddenly, the heart stopped beating Four minutes later, eardmc massage was earned out through a thoraeotomy The heart had stopped m the chastohc phase Heart beats were resumed with the first massage movements Some mdmatmn of corlaeal xrntat~on was present Treatment consisted of hypertomc glucose solutmn, repeated stellar infiltrataons, and plasma. Consemusness reamed during the evening, mental alertness did not seem 1raptured, with the exceptmn of some mental confusion of 24-hour duratmn, and loss of memory for recent events whmh returned m a few days
Seven days later, the pataent was operated on for radmal mastectomy, the operataon lasted two hours and was uneventful Preme&catmn levo-dromoran 2 mllhgrams, atropine 0 4 rmlhgram, Pacatal 25 mllhgrams Supporting medmatmn Paeatal 50 rmlhgrams, Benadryl 50 rmlligrams Induetmn and maintenance N~O-O_~-Fluothane-suecmylehohne 40 rmlhgrams Postoperative period, normal
2 Female patient, 10 years of age, obese, presented for emergency appendectomy Pre- mecheataon Demerol 50 mllhgrams, atropine 0 8 mflhgram Induction Pentothal 250 milli- grams, sueelnylchohne 60 mllhgrams Maintenance mtubataon, No O-Oa-Fluothane under controlled resplratmn w~th hyperventdatmn When the caecum was drawn out, the blood pressure whmh was 120/80 fell suddenly and the heart stopped beating Since marked resistance to resptratmn was present, the anaesthetist had lust given 0 2 milligram atropine
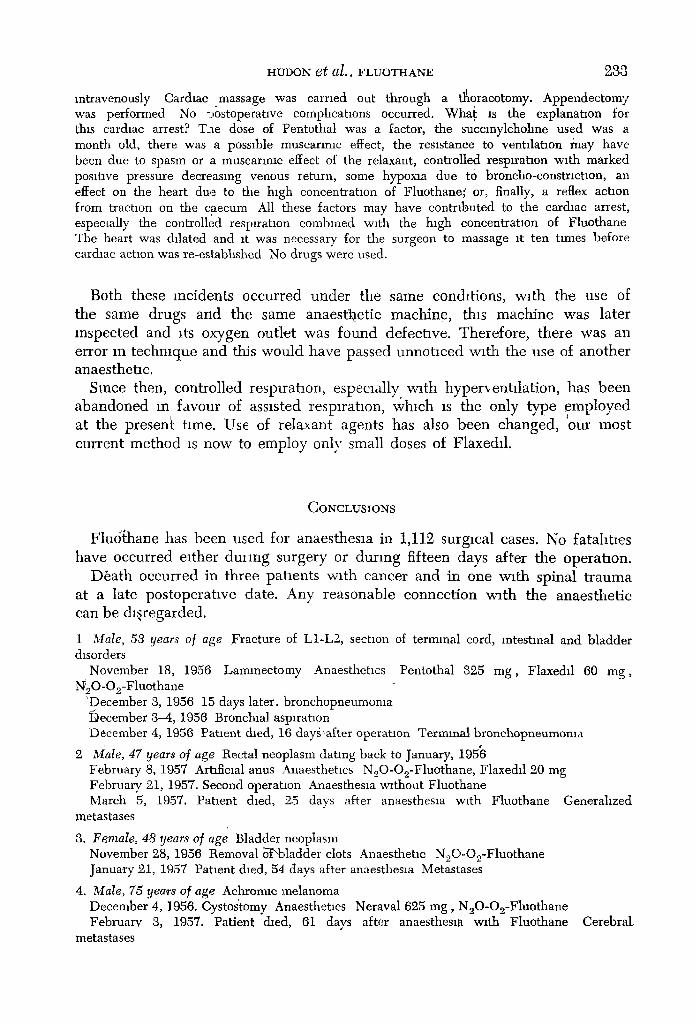
HUDON et al.. FLUOTHANE 288
intravenously Cardiac massage was carried out through a tl~oracotomy. Appendectomy was performed No =.ostoperatlve complications occurred. Wha~ is the explanatmn for this cardiac arrest? T_-te dose of Pentothal was a factor, the suecmylchohne used was a month old, there was a possible muscarmm effect, the resistance to ventilation fiaay have been due to spasm or a muscarmm effect of the relaxant, controlle d resplratmn with marked positive pressure decreasing venous return, some hypoxm due to broncho-constriction, an effect on the heart due to the high coneentratmn of Fluothane; or, finally, a reflex action from tractmn on the caecum All these factors may have contributed to the cardiac arrest, especmlly the controlled respiration combined with the high coneentratmn of Fluothane The heart was dilated and it was necessary for the surgeon to massage it ten times before cardiac aetmn was re-estabhshed No drugs were used.
Both these incidents occur red unde r t h e same condit ions, w~th the use of the same drugs and the same a n a e s ~ e t i c mach ine , this mach ine was later respec ted and its oxygen out le t was found defeelave. Therefore , there was an error m techn ique and tiffs w o u l d have passed u n n o t m e d wi th the use of ano ther anaesthetic .
Since then, control led respirat ion, especially, w~th hypep , entdat ion , has been a b a n d o n e d m favour of assisted respl rahon, wh ich is the only type e m p l o y e d at the presen~ time. Use of relaxant agents has also been changed , our mos t cur rent m e t h o d is now to employ only small doses of Flaxedi1.
CONCLUSIONS
Flud thane has been used for anaesthesia in 1,112 surgmal cases. No fatahtaes have occurred either dulang surgery or dur ing fifteen days after the operat ion.
D6a th occurred in three pat ients wi th cancer and in one wi th spinal t r auma at a late pos topera t ive date. Any reasonable connec t ion wi th the anaes thet ic can be d isregarded.
1 Male, 53 gears of age Fracture of L1-L2, section of terminal cord, intestinal and bladder &sorders
November 18, 1956 Lamlneetomy Anaesthetms Pentothal g25 rag, Flaxedd 69 rag, N20-O2-Fluothane
'December 3, 1956 15 days later, bronchopneumoma December 8-4, 1956 Bronchial aspiration December 4, 1956 Patmnt dmd, 16 day"after operation Terminal bronchopneumoma
L �9
2 Male, 47 years of age Rectal neoplasm dating back to January, 1956 February 8, 1957 Artificial anus Anaesthetms N20-O2-Fluothane, Flaxedi1 20 mg February 2i, 1957. Second operatmn Anaesthesia without Fluothane March 5, 1957. Patient died, 25 days after anaesthesia with Fluothane Generahzed
metastases
8. Female, 48 years of age Bladder neoplasm November 28, 1956 Removal o-'~.ladder clots Anaesthetic N~O-Oo-Fluothane January 21, 1957 Patmnt died, 54 days after anaesthesm Metastases
4. Male, 75 yea~s of age Aehromte melanoma December 4, 1956. Cystos'tomy Anaesthetms Neraval 625 mg, N20-O2-Fluothane February 3, 1957. Patient dmd, 61 days after anaesthesm w~th Fluothane Cerebral
metastases

284 CANADIAN ANAESTHETISTS' SOCIETY JOURNAL
The following conclusions may be drawn ]Erom this study of 1,112 cases of anaesthesia with Fluothane:
Fluothane has many advantages. Its disadvantages are easily controlled. It is a potent, volatile anaesthetac, its actaon is easily reversible, it is non-explosive and non-mflammable (it can even put out a flame). [t produces smooth and easy induction, and is well tolerated by the pataent. Induction should be slow, gradual and progressive. The patient should be maintained quietly without hyperventila- tion and without sudden increases m concentrataon; a properly calibrated vaporizer should be used. This is the best way to avoid a sudden hypotension, cardaac arrhythmlas and respiratory depression which this anaesthetic may produce (7).
The fact that there is no broncho-constriction and no laryngospasm, and that tracheo-bronchlal secrelaons are diminished, facilitates I pulmonary ventilation and contributes somewhat to less postoperative pulmonary atelectasis. Fluothane may be used with soda lime It decreases capillary oozing and blood loss during surgery. It appears to have anti-shock activity, in the manner of the "ganglio- plegic'" agents. It has a mild postoperative ataraxic effect. Clinically~ it seems to be non-toxic; there are no urinary disorders, fatigue or anorexia.
Possibly Fluothane is the equal of ether and cyclopropane, but has advantages which are lacking in both these agents', non-exp][osibilffy, non-inflammability, inhlbltaon of tracheo-bronchial secretaons, anti-shock, potency, and easy reversi- bxl ty.
REFERENCES
1. BlaYcE-SMaTH, R & O'Bamrr H D Fluothane, a Non-Explosive Volatile Anaesthetic Agent Bnt Med j , 989 (October 27, 1956)
2 R_~vE~rros, J The Action of Fluothane, a New Volatile Anaesthetic Brit, j Pharmacol, 11(4) 894 409 (1956)
8. GOODALL, R R Estimation of Fluothane m Blood Brit. J Pharmacol, 11(4) 409-11 (1956).
4. JOHNSTONE, M The Human Cardlo-Vascular Response to Fluothane Anaesthesia Bnt J Anaesth, 28(9). 892-411 (1956).
5 HIt.L, E. FALXNFm Percentages of Fluothane Vapour Dehvered from a Tnlene Bottle. Brit, J. Anaesth, 29 (1) 12-16 (1957).
6 H_MmIs, T A B The Mode of Achon of Anaesthetics Pp 177 Pp 577 Edinburgh E &S Livingstone (1951).
7 JOHNSTONE, M Correspondence Bnt J Anaesth,29(B) 135-6 (1957)