collective review management of neck injurymedinfo2.psu.ac.th/surgery/collective...
TRANSCRIPT
1
COLLECTIVE REVIEW
MANAGEMENT OF NECK INJURY
15 กรกฎาคม 2552
โดย นพ. ภวสษฏ ตรจกรสงข
ท�ปรกษา : อ.โกเมศวร ทองขาว
ขอบเขตของ Collective review
Introduction
Anatomy
Mechanism
Initial management
Clinical examination
Investigation
Definitive management
Specific organ injuries
Reference
INTRODUCTION 1
การบาดเจบท�คอ เปนเร�องท�ยากในการประเมนและการรกษาอนเน�องมาจากความซบซอนของอวยวะ
และความหนาแนนของจานวนอวยวะสาคญท�มาอยใกลกนในพ �นท�เพยงเลกนอย การประเมนอาการทางคลนก
เปนเร�องทาทายความสามารถของแพทยผ มประสบการณนอยและอาจจะทาใหมการผดพลาดในการวนจฉยการ
บาดเจบได การบาดเจบท�เกดข �นบางคร �งเปน Life threatening condition ศลยแพทยท�รกษาการบาดเจบท�คอควร
มความรอบรเร�อง surgical anatomy และหลกสาคญในการรกษา เพ�อลดภาวะแทรกซอนและอตราการตายใน
ผ ปวยเหลาน �
ANATOMY 2,3,8
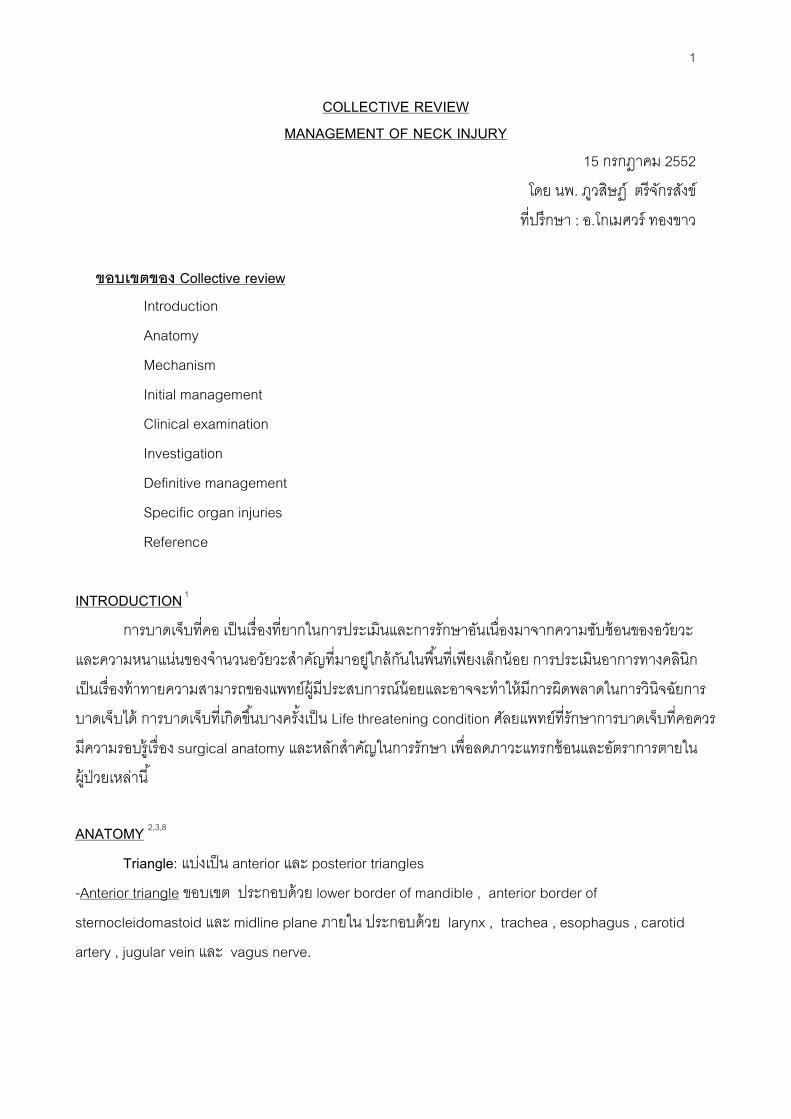
Triangle: แบงเปน anterior และ posterior triangles
-Anterior triangle ขอบเขต ประกอบดวย lower border of mandible , anterior border of
sternocleidomastoid และ midline plane ภายใน ประกอบดวย larynx , trachea , esophagus , carotid
artery , jugular vein และ vagus nerve.
2
-Posterior triangle ขอบเขต ประกอบดวย middle third of clavicle, posterior border of
sternocleidomastoid.
ภายใน ประกอบดวย Spinal accessory nerve, brachial plexus, transverse cervical
vessel, กลามเน �อ levator scapulae และ กลามเน �อ splenius
รปท� 1 แสดง การแบงคอเปน Triangle of neck (จาก Cummings: Otolaryngology: Head & Neck Surgery, 4th ed.)
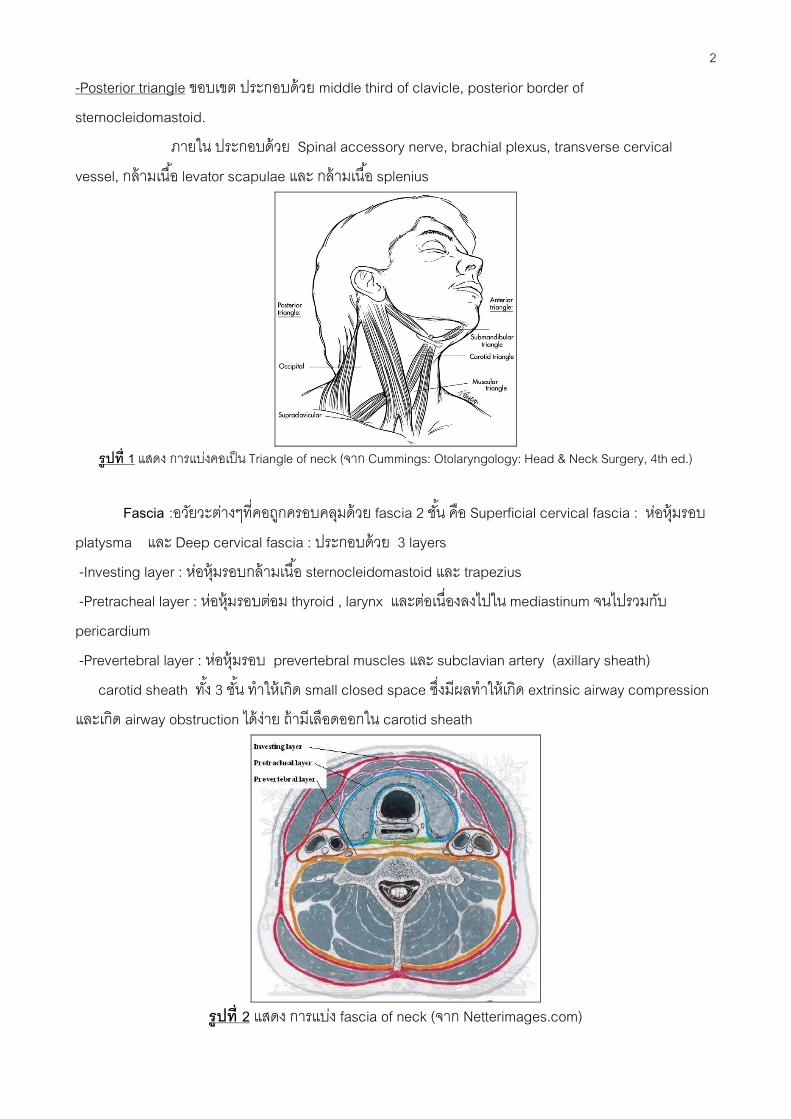
Fascia :อวยวะตางๆท�คอถกครอบคลมดวย fascia 2 ช �น คอ Superficial cervical fascia : หอหมรอบ
platysma และ Deep cervical fascia : ประกอบดวย 3 layers
-Investing layer : หอหมรอบกลามเน �อ sternocleidomastoid และ trapezius
-Pretracheal layer : หอหมรอบตอม thyroid , larynx และตอเน�องลงไปใน mediastinum จนไปรวมกบ
pericardium
-Prevertebral layer : หอหมรอบ prevertebral muscles และ subclavian artery (axillary sheath)
carotid sheath ท �ง 3 ช �น ทาใหเกด small closed space ซ�งมผลทาใหเกด extrinsic airway compression
และเกด airway obstruction ไดงาย ถามเลอดออกใน carotid sheath
รปท� 2 แสดง การแบง fascia of neck (จาก Netterimages.com)

3
Zone : แบงเปน 3 zones (Manson, 1969) 3
Zone I : เร�มจาก suprasternal notch ถง cricoid cartilage
ประกอบดวย common carotid artery, vertebral artery, innominate artery, subclavian artery, jugular vein,
trachea , esophagus , lung , spinal cord , thoracic duct และ cervical nerve trunks
Zone II : อยระหวาง cricoid cartilage และ angle of mandible
ประกอบดวย common , internal และ external carotid arteries , vertebral artery, jugular vein, larynx,
trachea, esophagus และ spinal cord
Zone III : อยระหวาง angle of mandible ข �นไปจนถง base of skull
ประกอบดวย pharynx , distal internal carotid artery , vertebral artery และ jugular vein
รปท� 3 แสดง การแบง Zone of neck (จาก Early care of the injured patient. Moore EE,ed Toronto:BC
Becker,1990:126)
MECHANISM OF INJURY 5,6,8
Penetrating neck injury
สาเหตของ Penetrating neck injuries ตามลาดบดงน �: Firearm 44%, stab wounds 40%, shotguns 4,
และ อาวธอ�นๆ 12% ความรนแรงของการบาดเจบจะข �นอยกบปจจยหลายๆอยาง เชน ชนดของอาวธ ระยะทาง
ระหวางอาวธกบผบาดเจบซ�งย�งใกลความรนแรงกมากข �น การบาดเจบของเน �อเย�อจะเกดจากแรงท�กระทาโดยตรง
หรอเกดจากพลงงานท�กระจายไปทาลายเน �อเย�อรอบๆปากแผลเกดการบาดเจบเปนบรเวณกวาง เราเรยกวาการ
ทาลายลกษณะน �วา temporary cavitation โดยเฉพาะจะเกดกบอาวธท�มความเรวมาก พลงงานท�เกดข �นมสมการ
ดงน � ( M = mass , V = velocity)
KINETIC ENERGY = ½ MV2
จะเหนไดวาความเรวจะเปนปจจยท�มผลทาใหเกดพลงงานไดอยางมาก ดงน �น High-velocity injury จะ
เกด tissue damage ไดมากกวา low-velocity injury สามารถแบงชนดของอาวธดงน �
4
High-velocity weapon คอ อาวธท�มความเรวมากกวา 2,500 ฟต/วนาท เชน อาวธสงคราม, ปน rifle,
shotgun บางชนด
Low-velocity weapon เชน มด, เศษแกว, shotgun, handguns, ice pick, razors เปนตน
อาวธท�มความเรวมากเวลาพงเขาสรางกายจะเกด Temporary cavitation เพราะฉะน �น gunshot wound
(GSW) จะมการบาดเจบของเสนเลอด เสนประสาท หลอดลมและหลอดอาหาร ไดมากกวาบาดแผลถกแทงโดย
มด
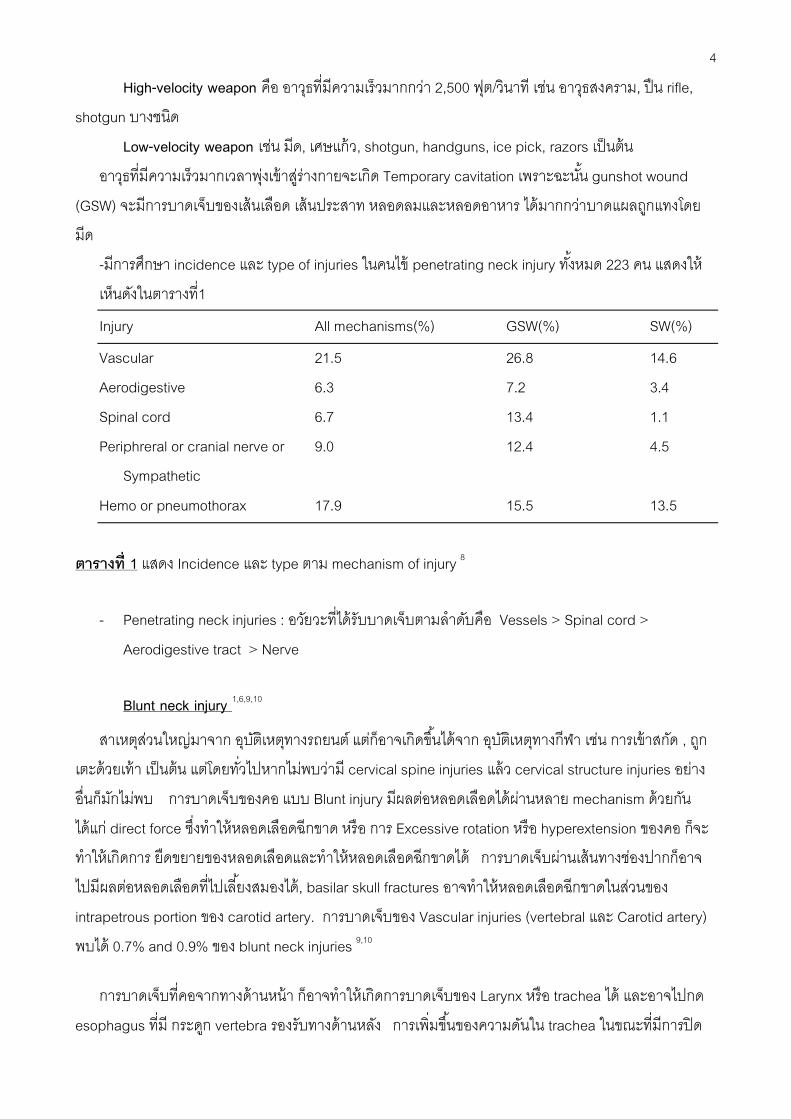
-มการศกษา incidence และ type of injuries ในคนไข penetrating neck injury ท �งหมด 223 คน แสดงให
เหนดงในตารางท�1
Injury All mechanisms(%) GSW(%) SW(%)
Vascular 21.5 26.8 14.6
Aerodigestive 6.3 7.2 3.4
Spinal cord 6.7 13.4 1.1
Periphreral or cranial nerve or 9.0 12.4 4.5
Sympathetic
Hemo or pneumothorax 17.9 15.5 13.5
ตารางท� 1 แสดง Incidence และ type ตาม mechanism of injury 8
- Penetrating neck injuries : อวยวะท�ไดรบบาดเจบตามลาดบคอ Vessels > Spinal cord >
Aerodigestive tract > Nerve
Blunt neck injury 1,6,9,10
สาเหตสวนใหญมาจาก อบตเหตทางรถยนต แตกอาจเกดข �นไดจาก อบตเหตทางกฬา เชน การเขาสกด , ถก
เตะดวยเทา เปนตน แตโดยท�วไปหากไมพบวาม cervical spine injuries แลว cervical structure injuries อยาง
อ�นกมกไมพบ การบาดเจบของคอ แบบ Blunt injury มผลตอหลอดเลอดไดผานหลาย mechanism ดวยกน
ไดแก direct force ซ�งทาใหหลอดเลอดฉกขาด หรอ การ Excessive rotation หรอ hyperextension ของคอ กจะ
ทาใหเกดการ ยดขยายของหลอดเลอดและทาใหหลอดเลอดฉกขาดได การบาดเจบผานเสนทางชองปากกอาจ
ไปมผลตอหลอดเลอดท�ไปเล �ยงสมองได, basilar skull fractures อาจทาใหหลอดเลอดฉกขาดในสวนของ
intrapetrous portion ของ carotid artery. การบาดเจบของ Vascular injuries (vertebral และ Carotid artery)
พบได 0.7% and 0.9% ของ blunt neck injuries 9,10
การบาดเจบท�คอจากทางดานหนา กอาจทาใหเกดการบาดเจบของ Larynx หรอ trachea ได และอาจไปกด
esophagus ท�ม กระดก vertebra รองรบทางดานหลง การเพ�มข �นของความดนใน trachea ในขณะท�มการปด
5
ของ glottis เชน จากการใส seat belt ท�ไมเหมาะสม ในกรณน �กจะเหนรอบจ �าเลอดท�คอ และมผลทาให trachea
injury ได การบาดเจบของ laryngotracheal และ pharyngoesophageal พบไดนอยมาก จาก Blunt neck
injuries คอ เกดประมาณ 0.04% - 0.3% 11,12 ในขณะท�ใน Penetrating neck พบได 5%-15% 13
การบาดเจบแบบ Strangulation เชน เกดจาการแขวนคอ, ผกคอ, ถกบบคอ หรอถกวตถกดทบคอ การท�จะ
เกดการบาดเจบตอ cervical spine หรอ spinal cord ไดอยางมนยสาคญน �นมกเกดไดในการแขวนคอแลวตกลง
มาท�ความสงมากกวาสวนสงของรางกาย การขาดอากาศไมใชสาเหตการตายหลกของการแขวนคอ แตวาการท�ม
cervical spinal disruption มกเปนสาเหตท�ทาใหเกดการเสยชวต
อบตเหตจาก High-velocity crashes เปนสาเหตสวนใหญของการบาดเจบ nerve injuries, การตกจากท�สง
ซ�งทาใหมการดงยดของคอและไหลออกจากกน ทาใหมการ traction ของ brachial plexus ได
INITIAL MANAGEMENT 7,14
เบ �องตนเม�อผ ปวยมาดวยประวตหรออาการบาดเจบบรเวณคอ ตองเร�มจากการดแลตาม ATLS protocol
ในผ ปวย trauma ท�วไปคอ primary survey, secondary survey และ definite treatment
1. Airway : การเปดชองทางหายใจเปนส�งสาคญท�สดส�งแรกท�ตองทา โดยเอาส�งแปลกปลอมท�ขวางทาง
เดนหายใจออก ใช suction ดดเลอด, เสมหะ และอาเจยน ในชองปากออกใหหมด เพ�อปองกน aspiration
ควรใส endotracheal tube กอนถาผ ปวยมอาการของ airway compromise เชน หายใจลาบาก คอบวม
มาก มฟองอากาศออกจากแผล บางคร �งผ ปวยม direct injury โดยตรงตอ larynx หรอ trachea อาจใส ET tube
เบอรเลกผานเขาชองท�เหนโดยตรงไปกอนซ�งอาจตองทา tracheostomy ในภายหลงท�หองผาตด ถาผ ปวยมภาวะ
expanding hematoma จะทาใหเกด tracheal deviation และ elevation of floor of mouth ม sublingual
hematoma ทาใหไมสามารถใส ET tube ไดซ�งอาจจะตองทา emergency cricothyroidotomy
ตองคดถง C - spine injury ทกคนจนกวาจะพสจนไดวาไมใช โดยเฉพาะผ ปวยไมรสกตวจาก brain
injury ตองทา C-spine immobilization ดวย Philadelphia cervical collar หรอใชถงทรายคอยประคองท �งสอง
ขางของคอไมใหเคล�อนท�
2. Breathing: ใน zone 1 อาจมภาวะ hemopneumothorax โดยท�ผ ปวยมอาการแนนหนาอก หายใจ
ลาบาก ตรวจพบ decrease breath sound, subcutaneous emphysema ซ�งถาสงสยตองใส ICD เพ�อปองกน
ภาวะ tension pneumothorax และประเมนเลอดท�ออกจาก pleural cavity ถามเลอดออกจากสาย ICD > 1,500
ccในการใสคร �งแรกหรอเลอดออก 200 cc/hr ตอเน�องเกน 4 ช�วโมงแลวอาจตองทา thoracotomy 43
3. Circulation : อาจมาดวยอาการ hypovolumic shock จากการบาดเจบตอเสนเลอดท�สาคญเชน
common carotid artery ควรจะหามเลอดดวยวธ direct pressure โดยใชน �วมอกดไปตรงท�แผลเลอดออกไมควร
ทา blind artery cramping ในการหยดเลอดออก อาจใช Foley catheter หรอ Fogarty No. 3-8 ใสทาง tract ท�

6
เลอดออก แลว inflate balloon ดวย saline จนเลอดหยดไหล ระหวางน �นก resuscitate ผ ปวยดวย crystalloid
เชน Acetar หรอ Ringer lactate solution เตรยมจองเลอดใหเพยงพอเตรยมพรอมในการผาตด ถาสงสยวาม
ภาวะเลอดออกจาก major venous injury ควรใหผ ปวยอยในทา Trendelenburg เพ�อปองกนภาวะ air embolism
รปท� 4 แสดงการหยดเลอดโดยใช Foley catheter 1
Clinical examination 1, 8
การตรวจรางกายควรตรวจทกระบบและเนนความสาคญไปท�อาการหรออาการแสดงท�บงช �ถงการ
บาดเจบตอ ทางเดนหายใจ,หลอดเลอด,หลอดอาหาร,ไขสนหลง,เสนประสาทและปอด
อาการทางคลนกแบงเปน Hard sign (อาการท�บงช �วามการบาดเจบเกดข �น) และ Soft sign (อาการท�ทา
ใหสงสยวามการบาดเจบแตไมสามารถจะวนจฉยลงไปได)
Evaluation for laryngotracheal injuries
Hard sign: ไดแก Respiratory distress ,air bubbling จากแผล และ major hemoptysis หากมอาการ
เหลาน �เปนขอบงช �ในการผาตดโดยไมจาเปนตองใชการตรวจวนจฉยใดๆ
Soft sign: ไดแก subcutaneous emphysema ,hoarseness และ minor hemoptysis . คนไขเหลาน �
ตองการการตรวจวนจฉยเพ�มเตม เพ�อตรวจหาการบาดเจบท�จาเปนตองเขารบการผาตด (ม 15% ของคนไขกลมน �
ท�ม laryngotracheal injury)8
Evaluation for vascular injuries
Hard sign : ไดแก Severe active bleeding ,large expanding hematoma ,absent หรอ diminished
peripheral pulse, bruit และ unexplained hypotension. (97% ของคนไขในกลมน �ม significant injury)8
Soft sign : ไดแก Stable ,small to moderated size hematoma,minor bleeding ,mild hypotension ท�
ตอบสนองตอการใหสารน �า และ proximity wounds ( 23.5% มความผดปกตท�เหนไดจาก angiogram , ม 3% ท�
ตองไดรบการผาตด)8
Evaluation for pharyngoesophageal tract injuries
Hard sign : ไมม
Soft sign : ไดแก Painfull swallowing ,subcutaneous emphysema และ hematemesis ( ม 18% ท�
พบวามการบาดเจบตอ pharyngoesophageal tract)8
7
Evaluation for nervous system injuries
ใหประเมน Glasgow Coma Scale (GCS) score, Localizing signs, pupils, Cranial nerve (VII,IX-
XII), Spinal cord , Brachial plexus (Median,Ulnar,Radial,Axillary,Musculocutaneous nerve), the phrenic
nerve และ Sympathetic chain (Horner syndrome) บางคร �งหากพบวา GCS ผดปกตอาจจะเปนผลมาจาก
carotid injury หรอ เปนผลมาจาก intracranial missile injury ได
Demetriades D ไดทาการศกษาคนไข penetrating neck injury ท �งหมด 223 คน พบวา มคนไข 160
(71.7%) ไมมอาการแสดงท�บงบอกวาม vascular trauma ซ�งตอมาไมมใครตองไดรบการผาตดเลย (NPV
=100%) มคนไข 127 คนในกลมน �ไดถกตรวจ ดวย angiogram ม 11 คน (8.3%) พบวาม vascular injuries แต
ไมจาเปนตองไดรบการรกษา (angiogram finding พบวาม occlusion of vertebral artery 4 ราย) ใน
การศกษาเดยวกน พบวา มคนไข 152 ราย ไมมอาการแสดง ของ aerodigestive injuries ซ�งตอมาท �งหมดกไมได
ตองการการผาตดรกษาเลย (NPV = 100%)8
INVESTIGATION OF CHOICE IN NECK INJURY 1,8,16,17,18
Chest and neck x-ray
เปนสวนหน�งใน standard investigation ทาทกรายท� hemodynamic stable ซ�งอาจจะเหน foreign
bodies, spinal fracture, hemothorax, pneumothorax อาจพบ tracheal deviation จากการกดของ hematoma
ถาพบ widened mediastinum ท�เกดจาก thoracic outlet vessel injury ใน zone I ควรสง angiogram เพ�มเตม
พบวา 16% ของ คนไข GSW และ 14% ของคนไข stab wound จะม hemopneumothorax 8
Angiography
ถอเปน gold standard ในการประเมน vascular injury ใชในผ ปวย hemodynamic stable zone I, III
neck injury และ asymptomatic zone I neck injury มการศกษาพบวาคนไข penetrating neck injuries ท�ไมม
อาการแตเม�อทา angiogram แลวกพบวาม vascular injury ได ถงแมวาท �งหมดเปนการบาดเจบท�ไมตองการกา
รกษา ดงน �นหากใช clinical examination เพยงอยางเดยวกจะทาให miss minor injuries ได
ขอด : เปน therapeutic diagnosisไดและใหขอมลเก�ยวกบ vascular anatomy สามารถวางแผนการรกษากอน
ผาตดได
ขอเสย : มราคาแพง ตองใชบคลากรจานวนมาก ผ ปวยมความเส�ยงตอการแพ contrast agent อาจเกด local
complication เชน small aneurysm, hematoma, vascular thrombosis, vascular spasm, distal
embolization, arterial dissection
Color flow Doppler ultrasonography (CFD):
ใชในการวนจฉย vascular injury โดยใหขอมลเก�ยวกบ flow , lumen และ vascular wall ของหลอดเลอด
ขอด: ราคาไมแพง และ noninvasive

8
ขอเสย : เปน operator dependentใชเวลานานในการตรวจแมวาอยในมอผ ท�ชานาญแลว ใน zone I, III จะ
ตรวจไดยาก เชน vertebral artery จะถกบงโดย transverse process ถาม hematoma หรอ subcutaneous
emphysema จะประเมนไดลาบาก ผ ปวยอาจจะเจบเพราะตองใช probe ตรวจบรเวณคอท�บาดเจบ
Demetriades et al 15 รายงานเปรยบเทยบการใช CFD กบ angiography พบวาม sensitivity 91%, specificity
98.6% ในการวนจฉย vascular injury
CT/Helical CT angiography (HCTA)
CT มกนใชอยางแพรหลายท �งในผ ปวย penetrating และblunt neck injury ท� extremity, mediastinum,
abdomen โดยปจจบนมโปรแกรมสรางเปน 3 –dimension ชวยทาใหมความละเอยดแมนยามากข �น
ขอด : ใชเวลาทานอย มประโยชนมากในการด bullet trajectory ซ�งชวยประเมนถงความจาเปนของ
angiogram. สามารถ ใชวนจฉย vascular injury ไดด ในกรณของ HCTA ม 90% sensitivity, 100%
specificity, 100% PPV, and 98%NPV จากการศกษาของ Munera 16
ขอเสย : Bullet fragment, metallic foreign body อาจจะรบกวนภาพเหนเปน artifacts ในรายท� HCTA แปลผล
ลาบากหรอไมอานผล อาจจะตองทา angiography อยด lesion เลกๆเชน intimal flap, small aneurysm อาจ
มองเหนไดไมชดเจน
Esophageal studies
ใชในการตรวจคนไขท�มอาการสงสย Esophageal injuries หรอในกรณท�ม bullet trajectory
ใกลกบ Esophagus
# Contrast esophagography
ขอด : ทาไดงาย
ขอเสย : ไมสามารถทาในหองผาตดไดหรอถาคนไขไมรสกตว
มขอกงวลวาการทา esophagogram เพยงอยางเดยวจะทาให Miss small esophageal injuries ได
เน�องจากมการศกษาของ Armstrong 17 พบม perforation diagnosis ไดจาก esophagography 62% แตถาเปน
rigid esophagoscopy พบ 100% แต มขอโตแยงวาอาจจะม false negative เปนผลไดจากเทคนคการตรวจ
โดยแนะนาวาเร�มแรกใหใช water soluble contrast กอน เชน gastrographin ถาหากไมเหนการ leakage ให
ทาซ �าดวย thin barium 1; พบวาการใช gastrographin อยางเดยวจะทาให miss small injuries ได 18
# Esophagoscopy (Rigid or flexible)
ขอด : มประโยชนในการด cervical esophagus
High accuracy : Flexible esophagoscopy ม NPV 100% ,PPV 33% 19,20
สามารถทาในคนไขท�ไมรสกตว และตรวจใน intraoperative ได
ขอเสย : Operator dependent
9
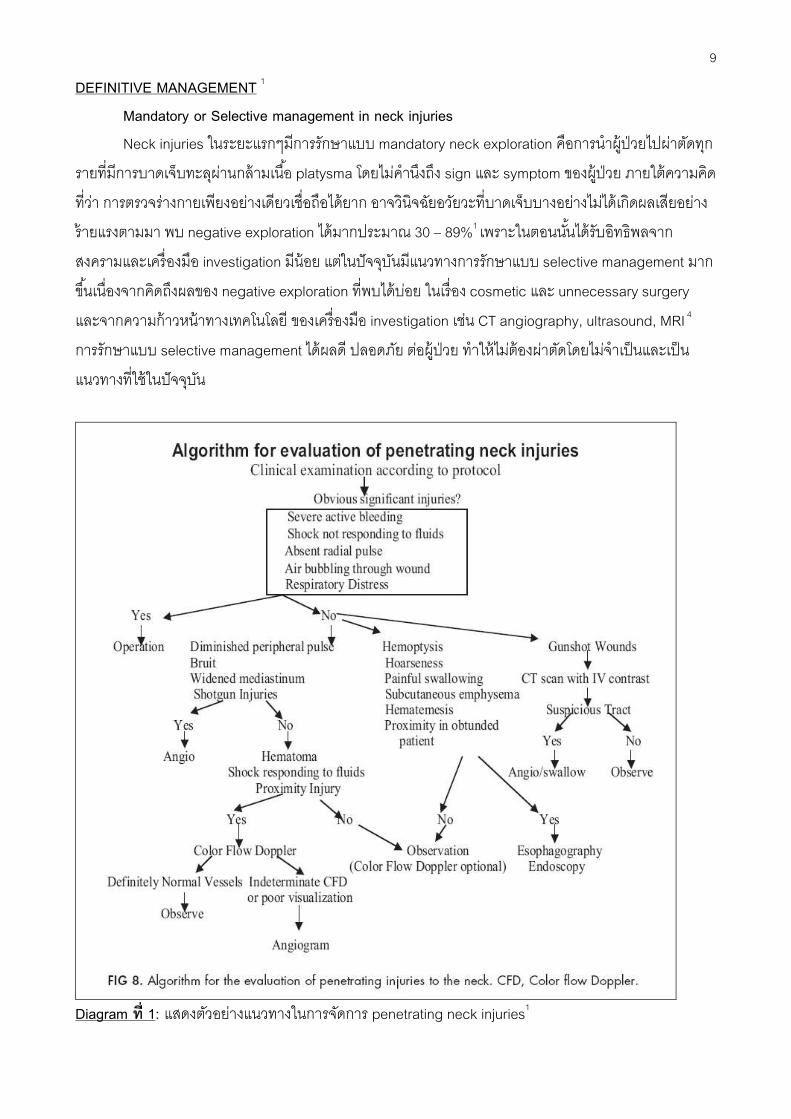
DEFINITIVE MANAGEMENT 1
Mandatory or Selective management in neck injuries
Neck injuries ในระยะแรกๆมการรกษาแบบ mandatory neck exploration คอการนาผ ปวยไปผาตดทก
รายท�มการบาดเจบทะลผานกลามเน �อ platysma โดยไมคานงถง sign และ symptom ของผ ปวย ภายใตความคด
ท�วา การตรวจรางกายเพยงอยางเดยวเช�อถอไดยาก อาจวนจฉยอวยวะท�บาดเจบบางอยางไมไดเกดผลเสยอยาง
รายแรงตามมา พบ negative exploration ไดมากประมาณ 30 – 89%1 เพราะในตอนน �นไดรบอทธพลจาก
สงครามและเคร�องมอ investigation มนอย แตในปจจบนมแนวทางการรกษาแบบ selective management มาก
ข �นเน�องจากคดถงผลของ negative exploration ท�พบไดบอย ในเร�อง cosmetic และ unnecessary surgery
และจากความกาวหนาทางเทคโนโลย ของเคร�องมอ investigation เชน CT angiography, ultrasound, MRI 4
การรกษาแบบ selective management ไดผลด ปลอดภย ตอผ ปวย ทาใหไมตองผาตดโดยไมจาเปนและเปน
แนวทางท�ใชในปจจบน
Diagram ท� 1: แสดงตวอยางแนวทางในการจดการ penetrating neck injuries1

10
Surgical approach3
การจดทาของการผาตดมความสาคญ หากจดทาไมเหมาะสมจะทาใหเกดความลาบากในการผาตด และ
ตองคานงถง extension ของ incision ดวย ดงตวอยางรปท� 4 แสดงการจดทา neck exploration โดยท�วไป การ
ลงมอทา neck exploration ทกคร �งตองเตรยมเคร�องมอ vascular set ใหพรอมและอาจตองเตรยมขาสาหรบ vein
graft ดวย การแบงคอเปน 3 zone เพ�อการ differential diagnosis และ การ approach ท�ตางกน
Zone I : การผาตดเขาสบรเวณน �ใช supraclavicular incision อาจจาเปนตองทา clavicular head resection,
median sternotomy หรอ anterolateral thoracotomy (trapdoor or book thoracotomy) อาจใช collar
incision ในกรณท�มการบาดเจบท �งสองขาง
Zone II : การผาตดเขาสบรเวณน � สามารถทาไดโดยงาย โดยใช standard sternocleidomastoid incision
(anterior to sternomastoid muscle)
Zone III : การผาตดเขาสบรเวณน �ใช extension ของ sternocleidomastoid incision อาจจาเปนตองทา
mandibular ramus osteotomy , subluxation of mandible , division of posterior belly digastric muscle ,
resection of styloid หรอ craniotomy
รปท� 4 แสดง Position สาหรบ neck exploration (จาก DSTC)
รปท� 5 แสดง Incision ตางๆสาหรบ Neck exploration (DSTC)
11
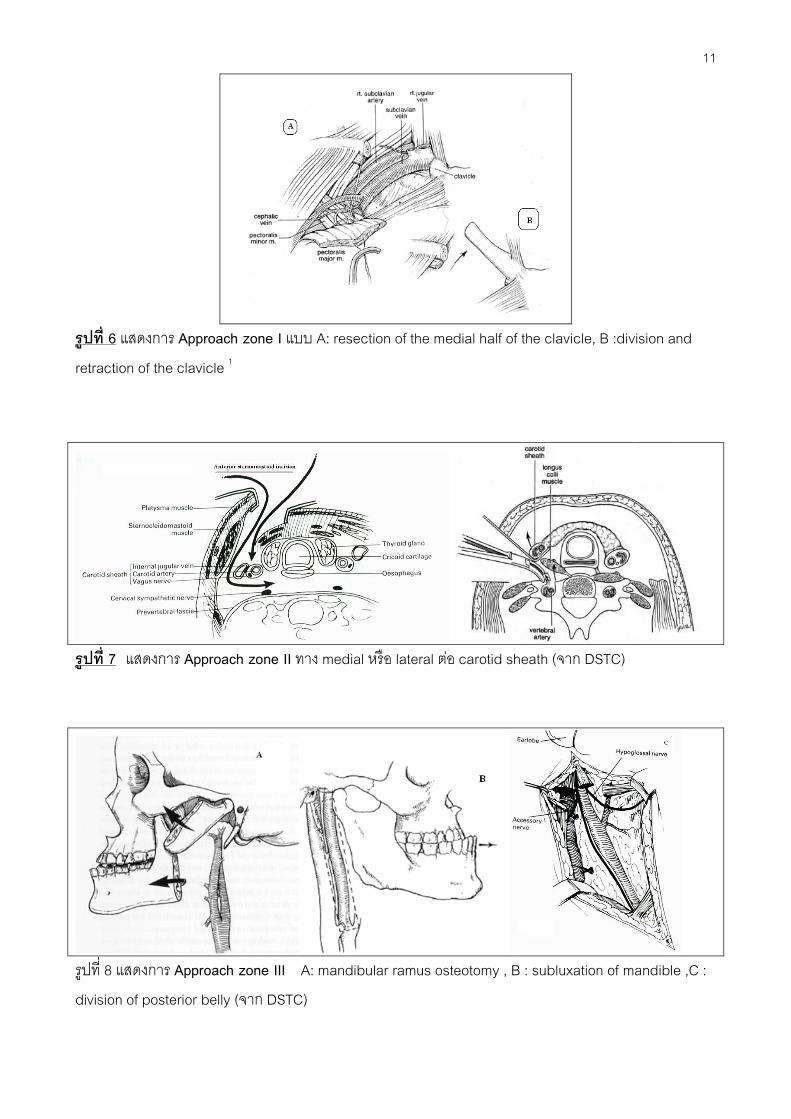
รปท� 6 แสดงการ Approach zone I แบบ A: resection of the medial half of the clavicle, B :division and
retraction of the clavicle 1
รปท� 7 แสดงการ Approach zone II ทาง medial หรอ lateral ตอ carotid sheath (จาก DSTC)
รปท� 8 แสดงการ Approach zone III A: mandibular ramus osteotomy , B : subluxation of mandible ,C :
division of posterior belly (จาก DSTC)
12
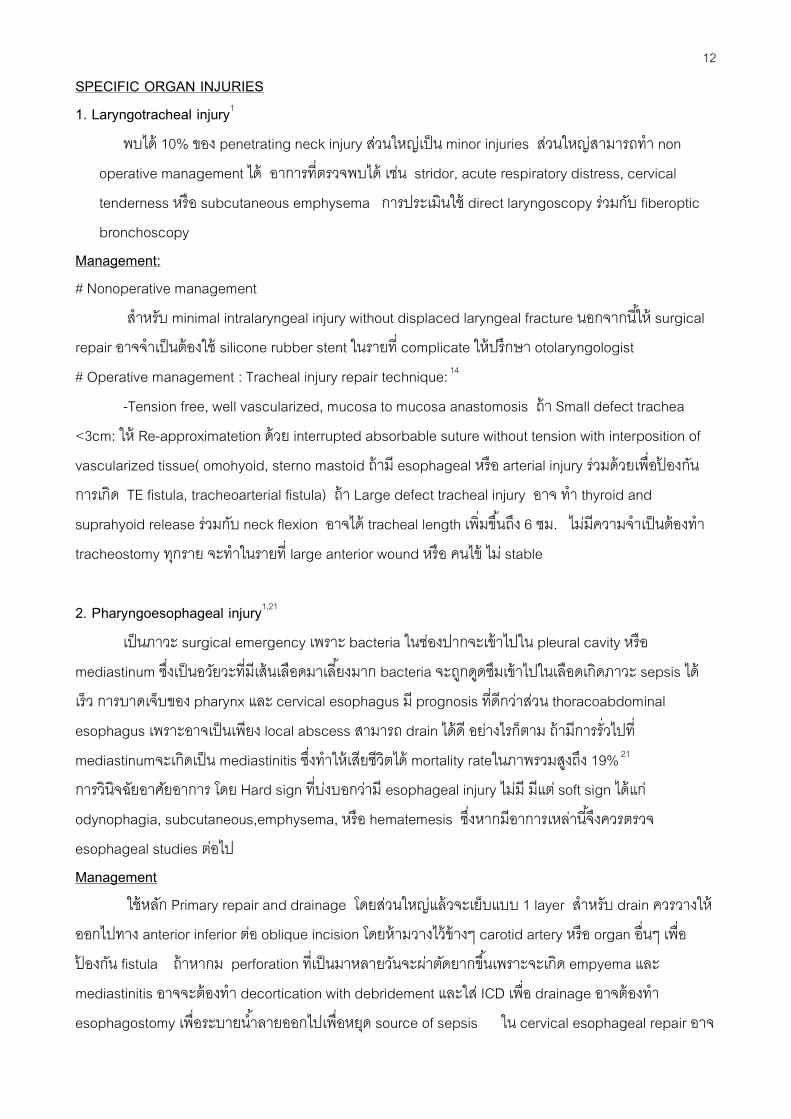
SPECIFIC ORGAN INJURIES
1. Laryngotracheal injury1
พบได 10% ของ penetrating neck injury สวนใหญเปน minor injuries สวนใหญสามารถทา non
operative management ได อาการท�ตรวจพบได เชน stridor, acute respiratory distress, cervical
tenderness หรอ subcutaneous emphysema การประเมนใช direct laryngoscopy รวมกบ fiberoptic
bronchoscopy
Management:
# Nonoperative management
สาหรบ minimal intralaryngeal injury without displaced laryngeal fracture นอกจากน �ให surgical
repair อาจจาเปนตองใช silicone rubber stent ในรายท� complicate ใหปรกษา otolaryngologist
# Operative management : Tracheal injury repair technique: 14
-Tension free, well vascularized, mucosa to mucosa anastomosis ถา Small defect trachea
<3cm: ให Re-approximatetion ดวย interrupted absorbable suture without tension with interposition of
vascularized tissue( omohyoid, sterno mastoid ถาม esophageal หรอ arterial injury รวมดวยเพ�อปองกน
การเกด TE fistula, tracheoarterial fistula) ถา Large defect tracheal injury อาจ ทา thyroid and
suprahyoid release รวมกบ neck flexion อาจได tracheal length เพ�มข �นถง 6 ซม. ไมมความจาเปนตองทา
tracheostomy ทกราย จะทาในรายท� large anterior wound หรอ คนไข ไม stable
2. Pharyngoesophageal injury1,21
เปนภาวะ surgical emergency เพราะ bacteria ในชองปากจะเขาไปใน pleural cavity หรอ
mediastinum ซ�งเปนอวยวะท�มเสนเลอดมาเล �ยงมาก bacteria จะถกดดซมเขาไปในเลอดเกดภาวะ sepsis ได
เรว การบาดเจบของ pharynx และ cervical esophagus ม prognosis ท�ดกวาสวน thoracoabdominal
esophagus เพราะอาจเปนเพยง local abscess สามารถ drain ไดด อยางไรกตาม ถามการร�วไปท�
mediastinumจะเกดเปน mediastinitis ซ�งทาใหเสยชวตได mortality rateในภาพรวมสงถง 19% 21
การวนจฉยอาศยอาการ โดย Hard sign ท�บงบอกวาม esophageal injury ไมม มแต soft sign ไดแก
odynophagia, subcutaneous,emphysema, หรอ hematemesis ซ�งหากมอาการเหลาน �จงควรตรวจ
esophageal studies ตอไป
Management
ใชหลก Primary repair and drainage โดยสวนใหญแลวจะเยบแบบ 1 layer สาหรบ drain ควรวางให
ออกไปทาง anterior inferior ตอ oblique incision โดยหามวางไวขางๆ carotid artery หรอ organ อ�นๆ เพ�อ
ปองกน fistula ถาหากม perforation ท�เปนมาหลายวนจะผาตดยากข �นเพราะจะเกด empyema และ
mediastinitis อาจจะตองทา decortication with debridement และใส ICD เพ�อ drainage อาจตองทา
esophagostomy เพ�อระบายน �าลายออกไปเพ�อหยด source of sepsis ใน cervical esophageal repair อาจ
13
ใช sternocleidomastoid muscle หรอ strap muscle เปน flap คอยปดบรเวณท�เยบซอมไวเพ�อปองกนการเกด
esophageal fistula กบอวยวะขางเคยง เชน trachea , carotid artery การผาตดม complication เชน wound
infection 8% ,esophageal fistula 5% , neck abscess 4%, mediastinitis 4%, trachoesophageal fistula
1.4% 21
3. Carotid artery injury1,22
เปนการบาดเจบท�พบไมบอยแตมความรนแรงมากและมอตราตายกอนมาถงโรงพยาบาลประมาณ 66%
ขณะท� mortality ของผ ปวยท�มชวตรอดหลง admission ท� 10-%20% 22 สาเหตสวนใหญมาจาก penetrating
neck injuries (90%) , โดยพบวา incidence ของ carotid artery injuries ใน penetrating neck injuries ม
ประมาณ 4%-15%1 ผ ปวยจะมาดวยอาการ shock, active external or intraoral bleeding, expanding
hematoma คลา carotid pulseไมได ซ�งอาการเหลาน �ตองรบนาผ ปวยไปผาตดทนท บางคร �งอาจมอาการของ
neurological deficit รวมดวยเชน hemiplegia, aphasia จนถง coma จากภาวะ ischemic cerebral infarction
ซ�งจะพบไดมากข �นใน hypovolemic shock, internal carotid artery injury, complete vessel transection และ
arterial ligation ถาผ ปวยมภาวะ hemodynamic stable อาจสง investigation เพ�มเตมซ�ง gold standard ยงคง
เปน angiography แตในปจจบนมรายงานการใช HCTA แทน angiography กนมากข �นและม sensitivity และ
specificity ท�สงสามารถใชเปนทางเลอกอกทางหน�งได
Management 1,23
หลกการเลอกวธการรกษาท�เหมาะสมข �นอยกบปจจยหลายอยาง ไดแก Hemodynamic stability
, mechanism of injury (blunt vs. penetrating), nature and severity of the vascular injury, anatomical site
,neurological status, และ associated injuries
Mechanism of injury: มหลกการรกษาท�แตกตางกน penetrating carotid injury มแนวโนมรกษาดวย
การผาตด แตวา ใน blunt carotid injury มแนวโนมรกษาแบบ Nonoperative management
Penetrating carotid injuries1,23 .
- หลกการคอควรทา Revascularization ทกราย ไมวาจะม neurological deficit กอนมาถงหรอตอน
มาถงแลวม depress mental status เพราะอาจจาก hypovolemic shock หรอจาก intoxication23 การซอม
หลอดเลอดถาdefect มขนาดเลกควรทา transverse arteriorhaphy เยบดวย prolene 6-0 interupt suture ถา
defect อยใกลกบ bifurcation of common carotid artery. ควรใช thin wall PTFE patch หรอ saphenous vein
patch เยบดวย prolene 6-0 continuous suture สวน larger perforation หรอ segmental defect ใน common
carotid artery. อาจทา resection and insertion of interposition saphenous vein หรอใช PTFE graft ถาเปน
ท�ตาแหนง internal carotid ใช interposition saphenous vein. graft ม patency ดกวา การ repair carotid
artery. ถาม esophageal repair รวมดวยควรใช sternal head of SCM เปน flap มาก �นระหวางกลางเพ�อลด
อบตการการเกด leakageในชวงหลงผาตด สาหรบการ control bleeding ถาทา direct pressure แลวยง
14
control hemorrhageไมไดอาจใช Fogarty catheter No.3-4 ผานทาง small arteriotomy ท� common carotid
artery. แลว inflate balloon จนเลอดหยด หรอ ใช balloon Foley catheter ใสทางแผลท�เลอดออกแลว balloon
ถาเลอดหยดไหลแลวตองตดสนใจตอวาจะทาอะไร เชน continuing balloon ตอจน 48-72 ช�วโมง หรอทา
angiographic intervention หรอ high cervical exploration การทา balloon occlusion of the high internal
carotid arteryเหมอนกบการทา ligation ควร monitor EEG,ICP ถา EEG สงสยวาม ipsilateral cerebral
ischemia หลงจากใส balloon ควรทา saphenous by pass graft จาก internal carotid artery ไป petrous
portion of internal carotid artery ผานทาง small temporal craniotomy โดยท�วไปการ check stump pressure
หากพบวาต�ากวา 40มม. ปรอท การทาshunt จะมประโยชน การทา high cervical exploration จะทากตอเม�อ
manual pressure หรอ balloon temponade ไมสามารถ control hemorrhage ไดหรอ ไมมเคร�องมอและ
radiologist ท�เช�ยวชาญ หรอทา embolization แลวแตยง control hemorrhageไมได
Operative management of carotid artery injury with associated neurological deficit or coma
ผ ปวย symptomatic carotid artery. injury ทกคนควรไดรบการผาตด revascularization ไมวาจะม
หรอไมม preoperative neurological deficit แตถาม preoperative coma และ Glasgow Coma Scale score <
8 ซ�งไมสมพนธกบ hemorrhagic shock, hypothermia, intoxication จะมผลการรกษาท�แย prognosisไม
เปล�ยนแปลงไมวาจะทา revascularization หรอ ligation ซ�งถาผ ปวยมาถงดวยอาการ coma มา > 3-4 ช�วโมง
แลวควรทา CT scan ถาพบ ischemic infarction การ revascularization ถอเปน contraindication เพราะ อาจ
ทาใหผ ปวยเสยชวตไดจาก hemorrhagic infraction เพราะ ischemic infarctionจะมภาวะ severe cerebral
edema ทาใหม vascular fragility เกดเปน hemorrhagic infarction แทน
ในปจจบนมการรายงานการรกษาโดยการใช endovascular therapy ในการรกษา hemodynamic
stable carotid artery injury มากข �นและไดผลการรกษาท�ด 24-27 โดยมหลกการคอ preservation of normal
patency cerebral arteries โดยท�เปน selective elimination of the fistulous communication, aneurysm or
stenosis เพราะการผาตดรกษา vascular injury บรเวณ zone I และzone III ทาไดยากและอนตรายกวาท�จะได
adequate proximal and distal control ซ�งม morbidity และ mortality สง
ผ ปวย stable symptomatic zone I,III หรอ asymptomatic ใน zone I ถาสงผ ปวยไปทา imaging study
แลวพบ abnormal study มแนวทางการรกษาดงน �
1. Intramural hematoma, intimal defect, dissection with intact distal flow อาจใชการสงเกตอาการและทา
angiogram ซ �าใน 1-2 อาทตย การผาตดมท�ใชนอยลงเร�อยๆ ซ�งถามการตบแคบของ lumen มากข �น
endovascular stent มประโยชนถา lesion อยใน internal carotid artery การใช systemic heparinization ถา
ผ ปวยไมม brain injury หรอมภาวะ coagulopathy มการศกษาพบวาสามารถเพ�ม survival rateได
2. Pseudoaneurysm ถามขนาดใหญข �นเร�อยๆจนเกด compressive symptom การผาตดไดผลดโดยเฉพาะ
ตาแหนง zone II หรอใช arteriographic embolization with or without stent โดยเฉพาะ lesion ท�อยบรเวณ
base of skull (zone III) เพ�อหลกเล�ยงการทา subluxation of TMJ or vertical ramus osteotomy of mandible
15
ในการ approach distal extracranial internal carotid artery สวน aneurysm ขนาดเลกใชการสงเกตอาการเปน
ระยะ
3. Carotid artery – jugular vein arteriovenous fistula พบไดไมบอยและมกเกดจาก internal carotid artery.
ถาขนาดใหญมากอาจทาใหเกด high output cardiac failure ได ตองทาการผาตด repair หรอทา coil
embolization มประโยชนโดยเฉพาะบรเวณ base of skull
4. Occlusion ในผ ปวย asymptomatic ท�มการอดตนท� internal carotid artery. พบไดนอย อาจใช
heparinization เพ�อลดการเกด emboli ไป intracranial circulation
Management of blunt carotid injuries 1,28-31
ประมาณ 3 – 10% ของ carotid artery injury ท �งหมด mechanism of injury พบได 4 รปแบบ คอ
cervical hyperextension / rotation (whip lash) ซ�งพบไดบอยท�สด, direct blow to the neck, intraoral trauma
และ fracture base of skull สวนมากมก involve internal carotid artery สวนปลาย (90%) พบการบาดเจบ
ท �งสองขางไดประมาณ 20 – 50% โดยมผ ปวยประมาณคร�งหน�ง ไมพบวาม sign ของ cervical trauma หรอ
neurodeficit ขณะแรกรบผ ปวย 28 การวนจฉยทาไดยาก เพราะผ ปวยสวนมากมกม significant intracranial
lesion หรอ อาจม alcohol, drug intoxication จากรายงานของ Cogbill 31 พบวามผ ปวยเพยง 37% ท�ม
Glasgow Coma Score นอยกวา 8 และมผ ปวยถง 49% ท�ม normal neurologic examination (GCS > 12) และ
มผ ปวยมากกวาคร�งท�ม neurodeficit ภายหลง 12 ช�วโมงไปแลว Fabian และคณะ 29 รายงานวา มผ ปวยถง
43% ท�ไมสามารถวนจฉย blunt carotid artery injury ไดจนกระท�งผ ปวยม neurodeficit โดยเฉล�ยแลวระยะเวลา
ท� delay diagnosis ประมาณ 53 ช�วโมง และการวนจฉยผ ปวยไดรวดเรว ทาใหม outcome ท�ด ตาแหนงท�พบ
การบาดเจบไดบอยคอ distal internal carotid artery ซ�งประเมนไดยากจากการใช Doppler Ultrasonography
ผ ปวยท�ม neurodeficit และม CT brain ปกต หรอมอาการไมสอดคลองกบ CT findings หรอม severe cervical
soft tissue injury (contusion, hematoma, bruit), neurodeficit in lucid patients, cranial nerve deficit
,Hornor’s syndrome และผ ปวยท�ม high-risk mechanism(direct cervical blow,significant whiplash ),
combine head-neck-chest trauma ควรนาผ ปวยไปทา diagnostic angiography 30 โดยสวนใหญการรกษา
ใช non operative management เปนหลก โดย ให heparin และ ตามดวย coumadin 3-6 เดอน 29-31
ไมวาจะ
เปน dissection หรอ occlusion Fabian 29 รายงาน non operative management พบวา 62% ของ carotid
dissection สามารถกลบเปนปกตได และอก 29% กลายเปน pseudoaneurysm ผ ปวยท�ม pseudoaneurysm
ใหทา repair ถาสามารถทาได ในกรณท�ไมสามารถ repair ได ใหทา proximal ligation รวมกบการให heparin
และอาจพจารณาทา extracranial/intracranial bypass สาหรบ carotid cavernous sinus fistula (CCF) รกษา
โดย balloon occlusion technique mortality rate ในผ ปวยกลมน �ประมาณ 5-43% และมgood neurologic
outcome เพยง 20-63% 29-31
16
4. Subclavian artery injury 32-36
เปนการบาดเจบท�พบไมบอยแตมความทาทายศลยแพทยมาก ผ ปวยจะมาดวยอาการ pulsatile
massive bleeding จน hypovolemic shock และอาจใชมอกดบรเวณจดเลอดออกเพ�อ control bleeding ไดยาก
เพราะมกระดก clavicle ขวางอย สาเหตมกเกดจากGSW มากกวา stab wound ม mortality ประมาณ 39% และ
มกพบ associate injury รวมดวย ทเชน subclavian vein 45%, brachial plexus 30% morbidityและ mortality
จะข �นอยกบ hemodynamic instability และ associate injury ถามรวมดวยต �งแต 3 ข �นไป mortality rate สงถง
83% การผาตด subclavian artery. ถกแบงเปน Proximal portion โดยท� middle และ distal portion จะอย
หลงตอ anterior scalene muscle มกลง incision เหนอหรอใตตอ clavicleแลวแตตาเเหนงท�บาดเจบ อาจตอง
ตดกระดก clavicle รวมดวยเพ�อ control hemorrhageและ surgical exposure ท�เหมาะสม โดยท�
• Proximal right subclavian injury มกจะลง incision เปน median sternotomy อาจทา right supraclavicular
extension เพ�อ distal control
• Left proximal subclavian a. injury ลง incision เปน median sternotomy with anterolateral thoracotomy
อาจตองทา supraclavicular extension รวมดวยเปน trapdoor incision
• Middle subclavian a. injury ลง incision เหนอ clavicle อาจตองทา disarticulation of sternoclavicular joint
and clavicular resection ดวยโดยเฉพาะ middle subclavian artery injury ท�ขนาด > 2cm ข �นไป
• Distal subclavian a. injury มกลง incision เปน infraclavicular incision with separation of pectoralis
major and division of the pectoralis minor insertion
โดยท�วไปควรทา primary repair by resection with end to end anastomosis อาจมทางเลอกอ�นๆเชน
artery reconstruction with saphenous vein interposition graft หรอใชวสดสงเคราะห เชน PTFE ในกรณท�
saphenous vein มขนาดเลกไมพอเหมาะ ligation มท�ใชถา control hemorrhage ไมไดผ ปวย hemodynamic
unstable ม multiple injury รวมดวย การผก subclavian อาจเกดภาวะ claudication จาก limb ischemia หรอ
เกด subclavian steal syndrome ถาทา ligation proximal ตอ
vertebral artery สวน endovascular stent graft อาจใชในผ ปวยท�ม subclavian artery injury อยางเดยวไม
ม associate injury อ�นๆรวมดวยและ hemodynamic stable ในปจจบนมความกาวหนาทาง endovascular
technology โดยการใช stent, coil embolization ม case report จานวนมากข �นท�รายงานการรกษา
pseudoaneurysm, AV fistura, arterial intimal flap, focal arterial laceration , first-order branch vessel
injury ใน penetrating subclavian artery injury ในภาวะท� hemodynamic stable
5. Vertebral artery injury
เปนการบาดเจบท�พบไดนอย ~ 1% ของ neck vascular injury ท �งหมด ม mortality ประมาณ 4% สวน
ใหญไมมอาการ มกจะวนจฉยไดโดยบงเอญจากการทา angiography ซ�ง penetrating trauma อาจทาใหเกด
arterial lesion เชน AV fistula, pseudoaneurysm, arterial dissection อาการอาจตรวจพบ bruit, thrill,
17
enlarging hematoma อาจจะม neurological symptom จาก emboli ทาใหเกด cerebrovascular accident
หรอเกดภาวะ transient ischemic attack ได จากรายงานของ Reid และ Weigelt 34 พบวา ผ ปวย 72% ท�ม
penetrating vertebral artery injury ตรวจรางกายไมพบความผดปกต และ 88% ของผ ปวยม normal GCS
ในขณะตรวจรางกายแรกรบ Thomas 36 รายงานวา การทา unilateral vertebral artery ligation ทาใหเกด brain
stem ischemia ได 3.1% ในขางซาย และ 1.8% ในขางขวา วนจฉย จาก Four-vessle multiplane
angiography เปนการบาดเจบท�ยากตอการรกษาเพราะ anatomy ท�เตมไปดวย bone structure ของ cervical
spine และ mandible Complication: จะเกด pseudoaneurysm, artery occlusion, active bleeding, AV
fistula ซ�ง AV fistula อาจทาใหเกดภาวะ vascular steal syndrome ทาใหอวยวะท�อย distal คอ brain เกด
ischemia ตามมาได การรกษา แบงเปน
Surgical approach: ยากและเส�ยงตอการบาดเจบตออวยวะขางเคยงท�สาคญ เชน spinal cord, esophagus
สามารถทา ligation ไดเลยเพราะม incident การเกดภาวะ brain stem ischemia หลงผกนอยมาก การ repair
vertebral artery จะทาในกรณท�พบวา angiogram ม collateral circulation ท�ไมเพยงพอ.
Endovascular repair37 อาจทา coil embolization and temporary balloon occlusion ในการรกษา AV fistula
หรอใส endovascular stent with coil คอใส stent กอนแลวคอยทา coil embolization เพ�อปองกนภาวะ coil
herniation into the parent artery ในการรกษา pseudoaneurysm การทา endovascular therapy มขอดกวา
surgical approach เชน การรกษาทาไดทนทหลงทา angiography เชนการใส stent และ embolization , เปน
local anesthesia, short recovery time, และการหลกเล�ยงการบาดเจบในอวยวะขางเคยงเชน esophagus,
trachea
6. Spine and spinal cord injury 38-40
ใน GSW neck injury ประมาณ 18%จะม spine injury และคร�งนงตองไดรบการผาตด ผ ปวยท�ม GSW
บรเวณใบหนาม C-spine injury ประมาณ 7% อาจพบ associated injury เชน vertebral artery ,tracheaรวมไป
ถง esophagus มกจะมาดวยอาการ unstable spine injury เชน ปวดบรเวณตนคอ หรอม neurological deficit
เชน quadriplegia และ 10% อาจจะไมพบอาการทาง clinic ไดโดยเฉพาะผ ปวยท�ม brain injury รวมดวย ตอง
immobilization C-spine เสมอจนกวาจะวนจฉยแยกไดโดย radiologic investigation เพราะอาจเกด iatrogenic
spinal cord injuryได การทา airway management ตองทาดวยความระมดระวง มรายงานการบาดเจบของ C-
spine injury แตไมม spinal cord injury ซ�งไมมอาการ neurologic symptom เลยจงไมไดทา C-spine
immobilization
7. Major venous injury
พบใน penetrating neck injury ประมาณ 4-15% ของผ ปวย ปกตถามการบาดเจบเพยงขางเดยวของ
brachiocephalic , internal jugular ,subclavian vein สามารถทา ligation ไดเลย โดยเฉพาะในผ ปวยท�
unstable ถามการบาดเจบท �ง 2 ขางควรทา primary repair ดานใดดานหน�ง เพ�อปองกนภาวะ acute cerebral

18
edema การทา lateral venorrhaphy จะทาในรายท�ถาทาแลวม lumen >50%จากของเดม หลงการทาอาจจะม
lumen ท�แคบ เกด thrombosis ไดงายใหระวง pulmonary embolism
8. Thyroid and parathyroid
ถาการบาดเจบเกด Superficial อาจเยบปดแผลดวย simple interrupt suture เลอดท�ออกมกจะหยดเอง
หรออาจทารวมกบ ligation of inferior thyroid artery ถาบาดแผลกวางมากอาจตองทา lobectomy การบาดเจบ
ตอ parathyroid gland พบไดนอยมากมกเกดจาก major resection of thyroid ซ�งอาจเกดภาวะ hypocalcemia
ไดชวงหลงผาตด
9. Thoracic duct injury
พบไดนอยมากและ มกพบรวมกบการบาดเจบของ left subclavian vein ถาผาตดแลวพบวาม thoracic
duct injury ควรจะทา ligation แตสวนใหญมกจะวนจฉยไมไดและเกด complication ผ ปวยจะมาดวยเร�อง chyle
leakage ผานทาง drain ท�วางไว หรอเกด subcutaneous fistula อาจพบเปน subcutaneous tissue mass เปน
chylocele ได
สรป
การบาดเจบบรเวณคอเปนภาวะฉกเฉน การตดสนใจของศลยแพทยสาคญมากในระยะแรกเพ�อใหผ ปวย
พนระยะวกฤตไปได มการแบงคอเปน 3 zone เพ�อการวนจฉยและจดการแตกตางกนไปในผ ปวยแตละคน ใน
ปจจบนนยมเปน selective management มากกวา mandatory management การวนจฉยท�ลาชาจะทาใหเกด
morbidity และ mortality ท�สงข �นตามมาภายหลงได สามารถใช HCTA เปนทางเลอกแทนการใช routine
angiography ได มรายงานการใช endovascular therapy ใน symptomatic stable penetrating neck injury ท�
เปน pseudoaneurysm, AV fistula กนมากข �นเร�อยๆ ในอนาคตเช�อวานาจะเปนstandard treatment เพราะ
ปลอดภยและเปน minimal invasive surgery ซ�งยงคงตองรอการศกษาดผลภาวะแทรกซอนในระยะยาวกนตอไป
Reference
1. Demetriades D.Neck injuries. Curr Probl Surg 2007;44:13-87.
2. Asensio JA, Valenziano CP, Falcone RE .Management of penetration neck injuries.The controvery surrounding
zone II injuries.Surg Clin North Am 1991;71:267-294
3. Monson DO, Saletta JD, Freeark RJ. Caroid vertebral trauma. Trauma 19699;987-999 .
4. Thompson EC,Porter JM,Fernandez LG. Penetrating neck trauma. An overview of management .J Oral Maxillofac
Surg 2002; 60:918-923.
5. Asensio JA, Valenziano CP, Falcone RE. Management of penetration neck injuries.The controvery surrounding
zone II injuries.Surg Clin North Am 1991;71:267-294
6. David B levy ,Brian S gruber. Neck Trauma.Emedicine 2008;1-2.
19
7. American college of surgeons, Advanced trauma life support: Program for doctor:1997;59-
85,St.Clair,Chicago,IL.
8. Demetriades D, Theodorou D, Cornwell EE, et al. Evaluation of penetrating injuries of the neck: prospective
study of 223 patients. World J Surg 1997;21:41
9. Clothren CC, Moore EE, Biffl WL, et al. Cervical spine fracture patterns predictive of blunt vertebral artery injury.
J Trauma 2003;55:811-3.56.
10. Clothren CC, Moore EE, Biffl WL, et al. Anticoagulation is the gold standard therapy for blunt carotid injuries to
reduce stroke rate. Arch Surg 2004;139:540-6.
11. Gussack GS, Jurkovich GJ, Luterman A. Laryngotracheal trauma: a protocol approach to a rare injury.
Laryngoscope 1986;96:660-5.
12. Minard G, Kudsk KA, Croce MA, Butts JA, Cicala RS, Fabian TC. Laryngotracheal trauma. Am Surg
1992;58:181-7.
13. Atkins BZ, Abbate S, Fischer SR, Vaslef SN. Current management of laryngotracheal trauma: case report and
literature review. J Trauma 2004;56:185-90.
14. Demetriades D, Asensio JA, Velmahos G, Thal E. Complex problems in penetrationg neck trama. Surg Clin North
Am 1996;76:661-683.
15. Demetriades D ,Theodorou D, Cornwell E ,Velmahos G, Yellin,Berne TV,Weaver F. Penetrating injuries of the
neck in patients in stable condition.Arch Surg 1995;130:971-975.
16. Munera F, Soto JA, Palacio D, Velez SM, Medina E. Diagnosis of arterial injuries caused by penetrating trauma to
the neck: comparison of helical CT angiography and conventional angiography. Radiology 2000;216:356-62.
17. Armstrong WB, Detar TR, Standley RB. Diagnosis and management of external penetrating cervical esophageal
injuries. Ann Otol Rhinol Laryngol 1994;103:863-71.
18. Fan ST, Lau WY, Yip WC, et al. Limitations and dangers of gastrografin swallow after esophageal and upper
gastric operations. Am J Surg 1988;153:495-7.
19. Srinivasan R, Haywood T, Horwitz B, et al. Role of flexible endoscopy in the evaluation of possible esophageal
trauma after penetrating injuries. Am J Gastroenterol 2000;95:1725-9.
20. Flowers JL, Graham SM, Ugarte MA, et al. Flexible endoscopy for the diagnosis of esophageal trauma. J Trauma
1996;40:261-5.
21. Asensio JA, Chahwan S , Forno W ,et al. Penetrating esophageal injuries:Multicenter study of the American
association for the surgery of trauma.J Trauma 2001; 50:289-296.
22. Demetriades D. Carotid artery injuries: experience with 124 cases. J Trauma 1989;29:91-4.
23. David V. Feliciano . Management of penetrating injuries to carotid artery.World J Surg 2001;25:1028-1035.
24. Ramsay DW, McAuliffe W. Traumatic pseudoaneurysm and high flow arteriovenous fistula involving internal
jugular vein and common carotid artery. Treatment with covered stent and embolization. Australasian radiology
2003;47:177-180.
20
25. Blattman SB , Landis GS, Knight M, Panetta TF, Sclafani SJ, Burack JH .Combined endovascular and open
repair of a penetrating innominate artery and tracheal injury.Ann Thorac Surg 2002;74:237-239.
26. McNeil CJ, Chiou MA,Gunlock MM, et al . Successful endovascular therapy of a penetrating zone III internal
carotid injury. J Vasc Surg 2002; 36:187-190.
27. Joo YJ, AhnJY, Chung YS, Chung SS, Kim SH, et al . Therapeutic endovascular treatments for traumatic carotid
artery injuries.J Trauma 2005;58:1159-1166.
28. Ballard JL, Mcintyre WB. Cervicothoracic Vascular Injuries, in Rutherford RB, Vascular Surgery 5th edition 2000 :
893-901,
29. Fabian TC, Patton JH, Croce MA, et al. Blunt carotid injury: Importance of early diagnosis and anticoagulant
therapy: Ann Surg 1996. 223:513-525.
30. Cogbill TH, Moore EE, Meissner M, et a. The spectrum of blunt injury to the carotid artery: A multicenter
perspective. J Trauma 1994; 37:473-479.
31. Parikh AA, Luchett FA, Valente JF, et al. Blunt carotid artery injuries. J Am Coll Surg 1997; 185:80-86,
32. Lin PH , Koffron AJ, Guske PJ, Lujan HJ, Heilizer TJ, Yario RF ,Tatooles CJ. Penetrating injuries of the subclavian
artery . Am J Surg 2003;185:580-584.
33. Kalakuntla V,Patel V,Tagoe A,Weaver W. Six-year experience with management of subclavian artery injuries.The
American Surgeon 2000;66:927-931.
34. Danetz JS, Cassano AD, Stoner MC, Ivatury RR , Levy MM .Feasibility of endovascular repair in penetrating
axillosubclavian injuries : A retrospective review. J Vasc Surg 2005; 41:246-254.
35. Strauss DC, Toit DF, Warren BL. Endovascular repair of occluded subclavian arteries following penetrating
trauma. J Endovasc Ther 2001;8:529-533.
36. Maskovic J, Radonic V, Jankovic S Cambj-Sapunar L, Mimica Z, Bacic A. Traumatic false aneurysm of the
subclavian artery treated by insertion of Memotherm stent. European journal of radiology 2001;38:205-208.
37. Albuquerque FC, Javedan SP , Mcdougall CG . Endovascular management of penetrating vertebral artery
injuries.J Trauma 2002 ;53:574-580.
38. Klein Y, Cohn SM, Soffer D, Lynn M, Shaw CM, Hasharoni A. Spine injuries are common among asymptomatic
patients after gunshot wounds.J Trauma 2005;58:833-836.
39. Platz A , Kossmann T , Payne B ,Trentz O . Stab wounds to the neck with partial transsection of the spinal cord
and penetrating injury to the esophagus. J Trauma 2003;54:612-614.
40. Apfelbaum JD, Cantrill SV , Waldman N.Unstable cervical spine without spinal cord injury in penetrating neck
trauma. Am J Emer Med 1999;18:55-57.
41. Reid JD, Weigelt JA. Forty three cases of vertebral artery trauma. J Trauma 1988; 28:1007-1012.
42. Thomas GI, Anderson KN, Hain RF. The significance of anomalous vertebral-basilar artery communications in
operations on the heart and great vessels. Surgery1959; 46:747-757.
43. Peitzman AB, Rhodes M, Schwab CW, et al. The Trauma Manual. Lippincott-Raven.Publications 2000.
44. Asher Hirshberg ,Kenneth L.Mattox .Safari in tiger country .Top knife 2005:199-213