course code: c-10134 2 cet points clinical decision making
TRANSCRIPT

Sponsored by:CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔
Detecting glaucomaDue to a lack of obvious earlysymptoms, about 50% of people withglaucoma are actually unaware thatthey are have the condition.4,5 Even toa trained eye, considerableirreversible damage to the retinalnerve fibre layer is likely to haveoccurred before visual field loss isdetectable (about 40% loss),6 or beforeoptic nerve cupping becomes visible(55% loss in rats),7 and thus timelyglaucoma diagnosis remains animportant but elusive clinical issuefor all optometrists.
The College of Optometrists hasproduced guidelines for examiningthe patient at risk from primary angleglaucoma (see www.college-optometrists.org) and broadlyrecommends that: when examining apatient who falls within the at-riskgroups for primary open angleglaucoma, the optometrist has a dutyto carry out the appropriate testsnecessary to determine the likelihood
CONFUSED ABOUT CET REQUIREMENTS? www.cetoptics.com/cetusers/faqs/IMPORTANT INFORMATION
Under the new Vantage rules, all OT CET points awarded will be uploaded to its website by us. All participants must confirm these results on www.cetoptics.comso that they can move their points from the “Pending Points record” into their “Final CET points record”. Full instructions on how to do this are available on their website.
Clinical Decision Making V: IntraocularPressure and Tonometry
COURSE CODE: C-10134 2 CET POINTS
14/1
1/08
CE
T
30
Why is 21mmHg animportant number?21mmHg is purely a statistical marker.The “normal” IOP range is defined bya statistical calculation as twostandard deviations either side of themean value of 15.5mmHg, or betweenapproximately 10mmHg and 21mmHg.Although we do know that the risk ofglaucoma increases as IOP increases,and as such we might expect that mosteyes with glaucoma will have an IOPof more than 21mmHg, this value isnot intended to represent the divisionbetween healthy and unhealthy eyes.Therefore, it is unwise to screen forglaucoma based on IOP measurementsalone.
Variations in IOPIOP changes over time. IOP can varyby several mmHg over a short (a fewseconds), medium (minutes to hours)and long (weeks to months) periods of
of the condition being present. IOPmeasurement is listed as an“appropriate test”, and this articlewill discuss normal and abnormalvariations in IOP, how IOP can beused to identify patients who are atrisk of glaucoma, how best to measureIOP using conventional optometricequipment and new technologicaldevelopments.
Is there a normal IOP?The short answer to this question is“no”. Goldmann and Schmidtoriginally reported that the averageIOP in 400 eyes measured using theGoldmann applanation tonometerwas 15.5±2.5 mmHg.8 Based on thesefigures, about 95% of people have anIOP that falls within the range of10mmHg to 21mmHg. However, it islikely that this range applies only to aCaucasian population, as the meanIOP is known to be closer to 13mmHgin some Asian populations.9-11
Dr Kirsten E. Hamilton, PhD, B.Optom (Hons), MCOptom
The measurement of intraocular pressure (IOP) is perhaps mostcommonly associated with glaucoma. Glaucoma is the name given to agroup of diseases that produce characteristic progressive optic nerveatrophy and associated visual field loss. According to the World HealthOrganisation, glaucoma is the leading cause of irreversible blindnessand currently affects an estimated 61 million people - this number isexpected to rise to almost 80 million by 2020.1,2 On average, around2.1% of people aged 40 years and over have open angle glaucoma(OAG), but this prevalence varies substantially due to age (increasingby several per cent per decade) and racial background (1.4% in eyes ofpeople of Asian origin and 4.2% of people with African origin).3DR
P. M
ARAZ
ZI/S
CIEN
CE P
HOTO
LIB
RARY
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:00 Page 30
Sponsored by:
CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔
14/1
1/08
CE
T
31
time. Some of these variations arepatient dependent, some areinstrument dependent and some areoperator dependent – all need to betaken into consideration whenattempting to interpret an IOPmeasurement. Table 1 lists some of themost common factors that affect IOP,which have been adapted from areview article published by Whitacreand Stein in 1993.12
IOP and the risk ofglaucomaThe greater the IOP the greater the riskof glaucoma. Even though therequirement for raised IOP to be partof a glaucoma diagnosis has now beenrelegated to old textbooks, andscreening for glaucoma on the basis ofIOP alone is no longer considered tobe acceptable clinical practice, anelevated IOP remains among thestrongest risk factors for thedevelopment of glaucoma.13-15
Additionally, IOP is currently the onlyrisk factor that can be modified andstudies have shown conclusively thatthe risk of glaucomatous damagedecreases following the reduction ofIOP via medication or surgicalmeans.14,16,17
There is no level of IOP that is able toseparate “glaucoma” from “notglaucoma”. An estimated 40% of eyes
with OAG have an IOP that never risesabove 21mmHg (commonly referred toas “normal tension glaucoma”), whileabout 90% of people with an IOPwithin the range of 24mmHg to32mmHg will not develop signs ofglaucomatous damage over a follow-upperiod of five years (commonlyreferred to as “ocular hypertension”).16
This information appears to indicatethat it is the susceptibility ofindividual eyes to a particular IOP thatis linked to glaucoma, not the absoluteIOP itself.18
While there is no minimum thresholdlevel of IOP that guarantees that apatient will be free of glaucoma, thereis an upper level that should beconsidered a cause for concern even inthe absence of other glaucomatoussigns. As a general rule, all patients
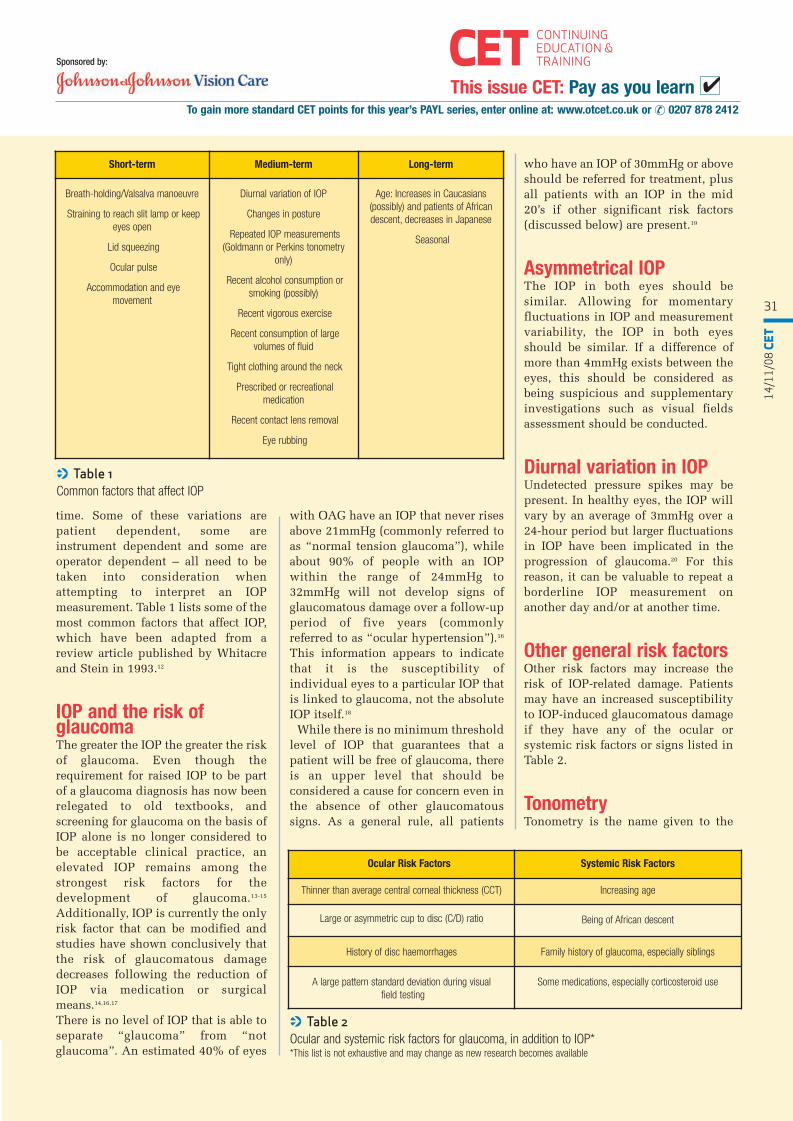
< Table 1 Common factors that affect IOP
Short-term Medium-term Long-term
Breath-holding/Valsalva manoeuvre
Straining to reach slit lamp or keepeyes open
Lid squeezing
Ocular pulse
Accommodation and eyemovement
Diurnal variation of IOP
Changes in posture
Repeated IOP measurements(Goldmann or Perkins tonometry
only)
Recent alcohol consumption orsmoking (possibly)
Recent vigorous exercise
Recent consumption of largevolumes of fluid
Tight clothing around the neck
Prescribed or recreationalmedication
Recent contact lens removal
Eye rubbing
Age: Increases in Caucasians(possibly) and patients of Africandescent, decreases in Japanese
Seasonal
Ocular Risk Factors Systemic Risk Factors
Thinner than average central corneal thickness (CCT) Increasing age
Large or asymmetric cup to disc (C/D) ratio Being of African descent
History of disc haemorrhages Family history of glaucoma, especially siblings
A large pattern standard deviation during visualfield testing
Some medications, especially corticosteroid use
< Table 2 Ocular and systemic risk factors for glaucoma, in addition to IOP* *This list is not exhaustive and may change as new research becomes available
who have an IOP of 30mmHg or aboveshould be referred for treatment, plusall patients with an IOP in the mid20’s if other significant risk factors(discussed below) are present.19
Asymmetrical IOPThe IOP in both eyes should besimilar. Allowing for momentaryfluctuations in IOP and measurementvariability, the IOP in both eyesshould be similar. If a difference ofmore than 4mmHg exists between theeyes, this should be considered asbeing suspicious and supplementaryinvestigations such as visual fieldsassessment should be conducted.
Diurnal variation in IOPUndetected pressure spikes may bepresent. In healthy eyes, the IOP willvary by an average of 3mmHg over a24-hour period but larger fluctuationsin IOP have been implicated in theprogression of glaucoma.20 For thisreason, it can be valuable to repeat aborderline IOP measurement onanother day and/or at another time.
Other general risk factorsOther risk factors may increase therisk of IOP-related damage. Patientsmay have an increased susceptibilityto IOP-induced glaucomatous damageif they have any of the ocular orsystemic risk factors or signs listed inTable 2.
TonometryTonometry is the name given to the
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:00 Page 31

CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔Sponsored by:
14/1
1/08
CE
T
32
similarity of corneas of each patientto those used in the originalcalibration sample. Goldmann andSchmidt knew that the results oftheir tonometer would be invalid ifit was used in eyes that differedsignificantly from the eyes that wereused to calibrate the instrument, orunder non-standard conditions(such as in corneas with oedema orscarring),8 but what they did notappear to realise was that cornealproperties varied widely fromperson to person, thus making theirtonometer susceptible tomeasurement errors.
Non-contact TonometryNon-contact tonometry (NCT) wasintroduced by Grohlman in 1972 asan alternative to Goldmann-typetonometers.21 Like Goldmanntonometry, it measures the forcerequired to applanate the cornea,though instead achieves applanationvia the rapid application of acolumnated air-pulse to the cornea.
Due to the fact that NCT wascalibrated to give readings that wereconsistent with Goldmann readings,and are also obtained via a form ofapplanation, it too is sensitive tomost of the corneal factors that affectGoldmann tonometry. Recentresearch suggests that NCT isactually more sensitive to variationsin corneal properties, particularly inthicker corneas. This may bebecause NCT encounters morecorneal resistance since itapplanates a larger area, and becauseit is a more rapid process that islikely to increase viscoelasticresistance compared to the slowerGoldmann process.22
The results of most modern NCTdevices are considered to be roughlyequivalent to the results provided byGoldmann tonometer except at highlevels of IOP, where NCT tends tooverestimate the IOP.23 Additionally,NCT measurements are taken over avery short period of time - they aresensitive to the ocular pulse and thismakes NCT results more variablethan Goldmann readings, though thereliability improves dramatically ifan average of three readings are
< Figure 1 The forces involved in Goldmann tonometry; red arrows are forces acting to resist applanationand green arrows are forces acting to induce applanation
measurement of IOP. Several differenttypes of tonometers are found inclinical practices throughout the UK,with the most common falling intotwo groups – contact (Goldmann andPerkins) and non-contact.
Contact TonometryGoldmann applanation tonometry(GAT) was introduced approximately50 years ago, and since that time it hasbeen elevated to the status of the “goldstandard” instrument for the clinicalmeasurement of IOP.8 For thepurposes of this discussion, thePerkins tonometer will be consideredequivalent to GAT.
GAT operates via the Imbert–Fickprinciple – this principle states thatthe IOP can be estimated indirectlyvia measuring the force required toapplanate or “flatten” a given area ofthe cornea. Strictly speaking, theImbert-Fick principle should only beused to determine the pressure withinany spherical object whilst it alsoassumes that the surface of that objectis dry, elastic and infinitely thin.
However, in reality, the cornea meetsnone of these conditions as it isactually elliptical, covered by a wettear film, exhibits viscoelastic ratherthan elastic behaviour and has anaverage thickness of 540µm. In order tocompensate for the mismatch betweentheory and reality, the Goldmanntonometer was calibrated inexperiments against directly measuredintracameral readings of IOP, where aneedle was placed in the anteriorchamber of the eye. Goldmann andSchmidt then selected an applanationdiameter for their tonometer whichmost closely matched the intracameralIOP;8 it was at this point that theybelieved that the resistance of thecornea and the attractive capillaryforces of the tear film were equal andopposite (shown as red and greenarrows in Figure 1, respectively) andthus were able to cancel each other outand provide an accurate IOP reading.
However, due to the fact that theGoldmann tonometer was calibratedagainst measurements obtained in realeyes, its accuracy depends on the
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 32
Sponsored by:
CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔
14/1
1/08
CE
T
33
taken for each eye. For these reasons, itis suggested that borderline or highNCT readings are verified with aGoldmann tonometer.
The importance ofTonometer CalibrationTonometers need to be checkedregularly to ensure that they arecalibrated. The accuracy of tonometersdecreases over time. In a recent surveyconducted, almost 70% of respondentschecked the calibration of theirGoldmann tonometers at less than therecommended monthly frequency,24
and an estimated 40-50% areinaccurate by more than ±2.5mmHg atany given time.25 Goldmann andPerkins tonometers should be checkedmonthly and returned to the supplierfor re-calibration if found to beinaccurate by 2.5mmHg or more; fornon-contact tonometers it is advisedthat practitioners contact their supplierfor the recommended service interval.
The problem of cornealthickness for tonometersFollowing the introduction of accuratecorneal pachymetry (corneal thicknessmeasurement) some years after theintroduction of the Goldmanntonometer, it was realised that therewas a much greater variability incorneal properties throughout thepopulation than had originally beenanticipated. Though averaging 540µmin most people, corneal thickness canvary by 60µm either side of this valuein perfectly healthy eyes, and evenmore in extreme cases.26
The impact of this inter-patientvariability in central corneal thickness(CCT) on IOP measurement wasunknown until 1975, when Ehlers etal. performed a study where theycompared the Goldmann IOP to theintracameral IOP in 29 patients whowere about to undergo cataractsurgery.27 They found that GoldmannIOP was underestimated in eyes withthin corneas and overestimated in eyeswith thick corneas, with the effectamounting to approximately ±5mmHgover the range of corneal thicknessesthat are likely to be encountered inroutine clinical practice. A similar
conclusion has been reached in manysimilar studies since that time, albeitthat the effect has not always beenreported to be as large or asconsistent.26 This effect also appears tobe present in all other tonometers thatrely on corneal manipulation toestimate IOP, including non-contactand Perkins tonometry, as well as theTonoPen.22
The potential influence of cornealthickness-induced errors in IOPmeasurements on glaucomamanagement were highlighted by Coptet al., who estimated that 31% of eyesdiagnosed with normal tensionglaucoma have statistically elevatedIOP when corrected for the effects ofCCT, while 55% of eyes classified ashaving ocular hypertension have astatistically normal IOP.28 A furtherstudy by Shih et al. of 188 subjectswith glaucoma or ocular hypertensionindicates that 43% of eyes require anadjustment in IOP of at least ±3mmHgfollowing CCT measurement, with19% of the subjects requiring a changein glaucoma therapy following cornealthickness correction.29 This means thatthere are some patients with glaucomawho may be under-treated (or notdetected at all by glaucoma screeningprograms based on IOP), and otherswho are being monitored unnecessarily
for glaucoma.
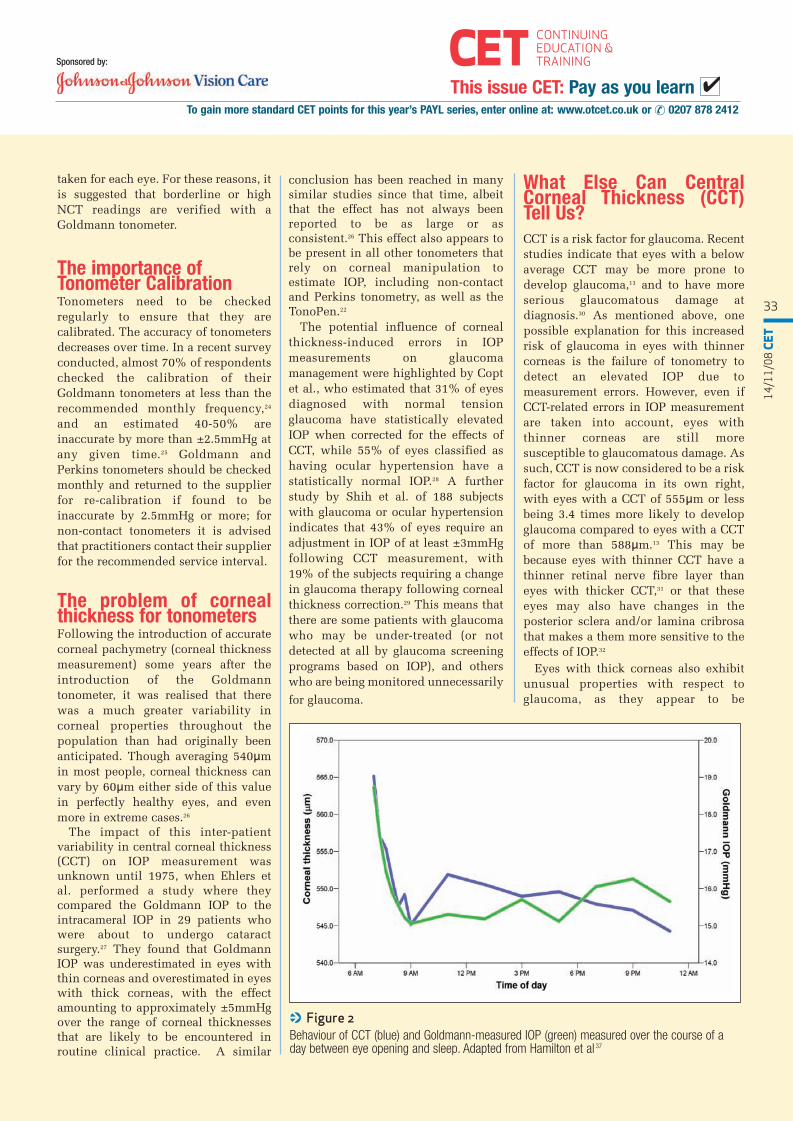
< Figure 2Behaviour of CCT (blue) and Goldmann-measured IOP (green) measured over the course of aday between eye opening and sleep. Adapted from Hamilton et al 37
What Else Can CentralCorneal Thickness (CCT)Tell Us?CCT is a risk factor for glaucoma. Recentstudies indicate that eyes with a belowaverage CCT may be more prone todevelop glaucoma,13 and to have moreserious glaucomatous damage atdiagnosis.30 As mentioned above, onepossible explanation for this increasedrisk of glaucoma in eyes with thinnercorneas is the failure of tonometry todetect an elevated IOP due tomeasurement errors. However, even ifCCT-related errors in IOP measurementare taken into account, eyes withthinner corneas are still moresusceptible to glaucomatous damage. Assuch, CCT is now considered to be a riskfactor for glaucoma in its own right,with eyes with a CCT of 555µm or lessbeing 3.4 times more likely to developglaucoma compared to eyes with a CCTof more than 588µm.13 This may bebecause eyes with thinner CCT have athinner retinal nerve fibre layer thaneyes with thicker CCT,31 or that theseeyes may also have changes in theposterior sclera and/or lamina cribrosathat makes a them more sensitive to theeffects of IOP.32
Eyes with thick corneas also exhibitunusual properties with respect toglaucoma, as they appear to be
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 33

CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔Sponsored by:
14/1
1/08
CE
T
34
somewhat protected against the effect ofhigh IOP.33 Researchers have also notedthat eyes with thick corneas are less responsive to IOP-loweringmedications, again in a way that cannotbe accounted for by corneal thickness-related errors in IOP measurement.34
Measurement of CCTOptometrists may benefit from CCTmeasurement. Due to the risk of CCT-induced measurement errors intonometry, the increased risk ofglaucoma associated with thin corneas,and the effect of CCT on theeffectiveness of IOP loweringmedications, several prominentOphthalmological associations(including the Royal College ofOphthalmologists in the UK and theAmerican Association ofOphthalmologists in the USA) are nowrecommending that CCT is routinelymeasured in eyes with a raised IOP, inglaucoma suspects and in allglaucomatous patients at diagnosis.Given that pachymetry is quick, simpleand can be conducted at minimal risk tothe patient, Optometrists may alsobenefit from the additional informationthat can be gained by measuring CCT.
How is CCT measured?CCT is measured using ultrasonicpachymetry by applying a small probedirectly to the corneal surface followingthe instillation of a topical anaesthetic.The most reliable measurements can beobtained by adhering to the followingguidelines:1. The cornea thickens away from thecentre so take care to apply the probeover the centre of the pupil. It must beheld at a 90º angle to the corneal apex. 2. Record the average of three readingsand the time of day.3. Do not take measurements within 2hours of awakening as overnightcorneal oedema may still be present andwill interfere with the readings.4. Be aware of factors that may affectCCT such as recent contact lens wear,corneal refractive surgery or cornealabnormalities such as keratoconus orFuchs’ endothelial dystrophy.
thin corneas and overestimated ineyes with thick corneas, they have notbeen able to confirm a specificnumerical relationship between thetwo, and thus there is no universallyaccepted correction factor.2. Other corneal factors are almostcertainly as important as CCT to theaccuracy of IOP measurement, andthus a correction factor based solelyon CCT cannot be accurate.
However, this does not mean thatwe should stop measuring CCT. Whilethere is no clear point dividingnormal CCT from abnormal CCT, andthere is no correction factor known tobe suitable for all patients, largedifferences from the average CCTvalues are clinically importantbecause it may affect the managementof our patients via the link to the riskof glaucoma.
Why CCT measurementisn’t enoughAs discussed above, the accuracy ofIOP measurement depends on theproperties of the cornea throughwhich it is measured; CCT is a well-
< Figure 3 The Ocular Response Analyser (ORA) and computer
Should IOP measurementsbe corrected for CCT?Correction of IOP based on CCT aloneis inaccurate. The discovery of therelationship between CCT and theaccuracy of IOP measurement has leadto the development of cornealcorrection factors. Though there areseveral different correction factorsavailable, the premise for using themis the same – CCT is measured for eachpatient, a correction factor (in mmHg)is deduced from the CCT, and thisvalue is then added or subtracted fromthe IOP reading in order to produce anadjusted IOP measurement that shouldtheoretically be closer to the true IOP. These correction factors are becomingincreasingly available to Optometristsvia a variety of sources; they may beelectronically incorporated intosoftware, or appear as a summary tableon a card that can quickly convert aCCT measurement into an IOPreading. However, it is generally notappropriate to correct an IOP based onCCT because:1. While most researchers agree thatIOP is underestimated in eyes with
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 34
Sponsored by:
CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔
14/1
1/08
CE
T
35
established influence but is not theonly one, and many other cornealfactors that have been shown toinfluence the accuracy of IOPmeasurement.
Corneal biomechanicalbehaviourAn recent article in Optometry Today(The biomechanics of keratorefractivesurgery September 5 2008) describedthe concept of corneal biomechanics insome detail, so the present article willrefrain from further discussion exceptto say that corneas can vary from verypliable to very inflexible, meaning thatcorneas with identical thickness canbehave entirely differently duringtonometry depending on whether theyhave a soft or rigid biomechanicalnature. In the average healthypopulation, the natural variation incorneal biomechanical behaviour issufficient to cause an error in IOPmeasurement that is almost the samesize as the CCT-related errors.35 Thiscould create serious complications ifCCT-based correction factors are usedin eyes that have soft thick corneasbecause the “corrected” IOP may beeven further away from the true IOP
than the raw Goldmann reading.Unfortunately, biomechanicalbehaviour does not change theclinical appearance of a cornea and itcannot be measured usingconventional optometric equipment.
Corneal hydrationThe hydration of all human corneasvaries over a 24-hour period; thismanifests as a characteristic morecommonly known as the diurnalvariation of corneal thickness, whichaverages about 3.5%.36
Figure 2 shows how cornealthickness and IOP behave duringwaking hours. For the first two hours,the IOP measurement follows thesame pattern as the CCTmeasurement, which indicates thatthe small corneal oedema present onawakening causes an overestimationerror in IOP.37 This overestimationwas also confirmed in eyes withartificially induced corneal oedemathrough contact lens wear, and thusappears not to be a coincidentalfinding that might be related toposture or other sleep-relatedphenomena.38,39
The overestimation of IOP by
tonometry due to corneal oedema is arelatively new finding, and manytextbooks still indicate that cornealoedema will result in anunderestimation in IOP.40 The latterremains true but occurs only in highlyswollen corneas, mostly because it isquite easy for a tonometer to “squash”the soft swollen epithelium into anapplanated shape; in thesecircumstances, the tonometer readingwill be unrelated to the IOP.
The clinical advice is that IOPmeasurement should not beperformed until overnight oedemahas had sufficient time to clear – thisis currently two hours in younghealthy subjects but it is possible thatthis may need to be longer in olderindividuals due to the decrease incorneal endothelial function thatoccurs with aging. Tonometrygenerally should not be attemptedwhen the cornea is highly swollen.
Corneal curvatureTheoretically, corneal curvature iscapable of affecting the accuracy ofGAT, but research results have beeninconclusive.27,41-43 The generalconsensus appears to be that the IOP
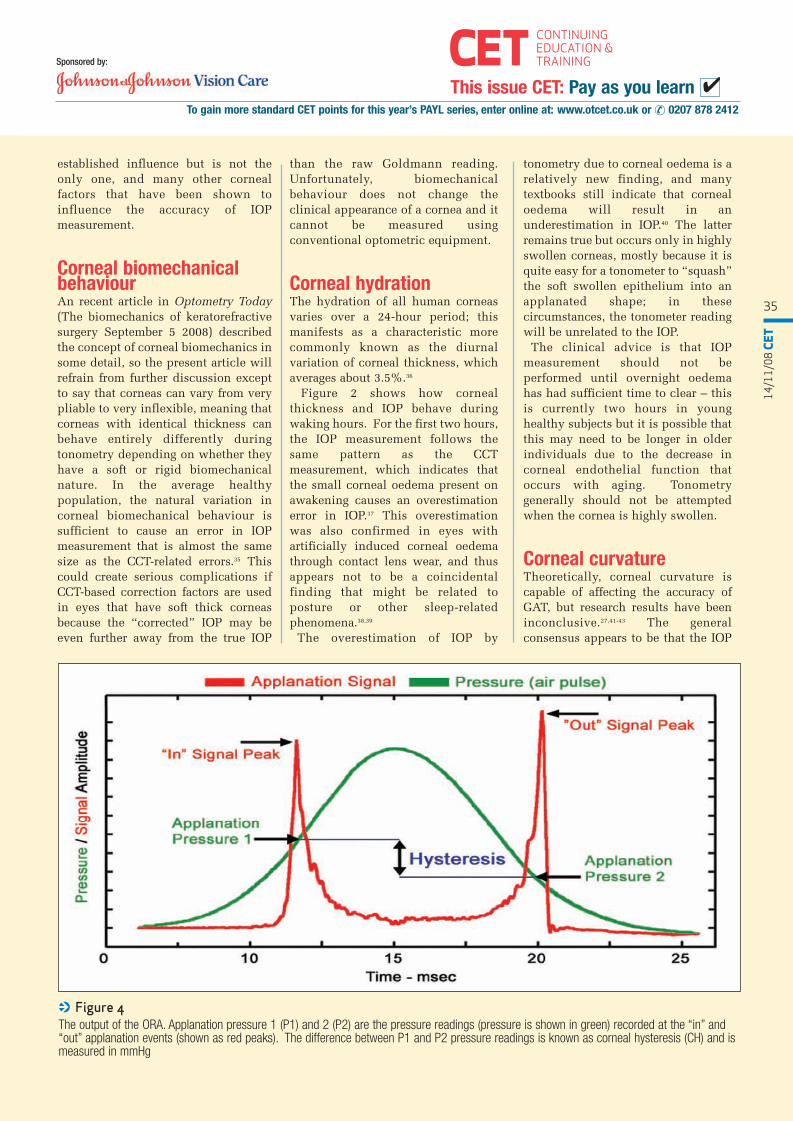
< Figure 4 The output of the ORA. Applanation pressure 1 (P1) and 2 (P2) are the pressure readings (pressure is shown in green) recorded at the “in” and“out” applanation events (shown as red peaks). The difference between P1 and P2 pressure readings is known as corneal hysteresis (CH) and ismeasured in mmHg
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 35

CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔Sponsored by:
14/1
1/08
CE
T
36
will be underestimated slightly in flatcorneas and overestimated slightly insteep corneas, but the effect isprobably confined to the extremelimits of “normal” corneal curvatureand thus is generally not a significantfactor in the average clinical setting.
Refractive surgeryIOP measurements are usuallysignificantly reduced by severalmmHg in eyes that have had LASIK,LASEK or PRK, but by an amount thatcannot be fully explained orpredicted by the decrease in cornealthickness, the amount of refractiveerror corrected or the change incorneal curvature.32 Therefore, caremust be taken when interpreting anIOP measurement performed by GATin an eye that has had cornealrefractive surgery. It would be wise tolook more closely for other signs ofglaucomatous damage rather thanrely on traditional IOP measurementsin these patients, or consider using analternative tonometer (see below formore details).
Peripheral cornealthicknessUntil recently, almost all of theresearch that has looked at the effectof corneal thickness on IOPmeasurement has considered thethickness in the centre of the corneaonly (CCT). However, both GAT andNCT applanate an area that is over3mm in diameter, and it has beenknown for many years that the corneaincreases in thickness towards theperiphery.44 It has recently beenshown that the increase in cornealthickness towards the periphery,specifically 2.5mm to the temporalside of the corneal centre, caninterfere with NCT readings.45 In thisstudy, the increase in temporalcorneal thickness was associated withan overestimation error in IOP, inaddition to any error already inducedby the CCT, and importantly, thisinterference from the peripheralcorneal thickness was almost thesame size as the effect of CCT.45 Tocomplicate matters further, theincrease in thickness that occurs in
the periphery cannot be estimated bythe measurement of CCT and thusmust be measured independently.45
However, preliminary data conductedby the same researchers suggests thatconventional ultrasound pachymetrymay not be adequate to performthickness measurements of the mid-peripheral cornea reliably, and that awide-field pachymetry device such asthe Orbscan IIz or Pentacam would bemore appropriate. Research is currently underway todetermine whether peripheral cornealthickness has a similar effect onGoldmann tonometry, so in themeantime, the clinical advice is tokeep this factor in mind but awaitfurther information before attemptingto incorporate it into routine cornealthickness measurement.
New tonometry methodsGiven that the cornea has such a strongability to influence IOP measurementsusing traditional tonometers, severalnew tonometers have been introducedinto the marketplace, which haveattempted to address the interferenceof corneal behaviour in two distinctlydifferent ways:1. To measure corneal behaviourdirectly and then compensate for it(e.g. the Ocular Response Analyzer -ORA).2. To obtain a measurement of IOP
without causing significant cornealapplanation, thus avoiding most ofthe corneal influence (eg the Pascaldynamic contour tonometer - PDCT).
Ocular Response Analyzer(ORA)The ORA (Figure 3) is a modifiedNCT that uses specialised computersoftware to obtain additionalinformation describing theapplanation process. Themeasurements are performed as forNCT (average of three readings pereye) and similarly, applanation isdetected via an infrared (IR) emitterand detector such that in a non-applanated cornea, very little IR lightis able to reach the detector becausethe rounded cornea disperses it andthe resulting light signal intensity islow. When the increasing force of theair pulse is sufficient to causeapplanation however, the cornealsurface temporarily becomes a flatreflecting surface that directs themaximum amount of IR light into thedetector, which causes a peak in thelight intensity. In a conventional NCT,the air-puff is terminated and apressure reading is recorded onceapplanation has been detected.However, the ORA continues torecord the pressure over a longerperiod of time. There is a slight delayin switching off the air pulse, which
Parameter Definition
IOPG Goldmann correlated IOPThis measurement is directly comparable with any conventional contact or non-contacttonometer
IOPCCCorneal compensated IOPAn IOP measurement that is less influenced by corneal properties such as elasticity and thickness
CH Corneal hysteresisThis is calculated as the difference between Applanation pressures 1 and 2, as shown inFigure 4.It is an indicator of a particular aspect of corneal behaviour called viscous damping, andthis number is used in further analysis
CRF Corneal resistance factorA measurement of the total viscoelastic response of the cornea, which includes elasticityand thickness
< Table 3 Measurements produced by the Ocular Response Analyzer (ORA)
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 36

Sponsored by:
CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔
14/1
1/08
CE
T
37
means that the force of the air pulsetemporarily increases beyond thelevel required for applanation, and sothe cornea indents momentarilywhich is seen as a reduction in thelight signal reaching the detector Asthe force of the air pulse decreases,the cornea passes through a secondapplanation point before returning toits normal shape. The differencebetween the two-applanation pointsproduces a unique value calledcorneal hysteresis (CH), which isrepresentative of the cornealbiomechanical properties (Figure 4).
In addition to the waveform shownin Figure 4, the current version of theORA also produces four differentnumbers: two different types of IOPmeasurements and two measurementsrepresenting corneal biomechanicalbehaviour. A summary of these can befound in Table 3.
The two IOP measurements IOPG
and IOPCC are of most interest toclinicians. IOPG is important becauseit allows a direct comparison withconventional tonometry (particularlyuseful when comparing new readingsto those taken with a previoustonometer), while IOPCC is importantbecause it is believed to provide anIOP measurement has been correctedfor the interference of cornealproperties, including thickness.
Via its analysis of cornealproperties, the ORA may also providea way of distinguishing between trueocular hypertension and eyes withartificially elevated IOP due tomeasurement errors. Additionally,early findings indicate that CH andCRF may be able to detect structuralchanges due to glaucoma.46
Pascal Dynamic ContourTonometerThe Pascal Dynamic ContourTonometer (PDCT) (Figure 5) is a slit-lamp mounted device designed tomeasure IOP without interferencefrom corneal properties. Though itmay look like a Goldmann tonometerin some ways, it is significantlydifferent because:1. The tip of the probe is concaverather than flat (Figure 6). This designfeature is intended to follow the
corneal contour and neutralise thecorneal forces rather than forcingapplanation, which thenreduces/eliminates the influence ofcorneal properties on IOPmeasurement.2. The IOP is measured by anelectronic pressure sensor embeddedin the probe tip.3. Readings are displayed digitally soit is more objective than GAT.4. The IOP is monitored continuouslyover a period of several seconds,providing a measurement of theocular pulse amplitude (OPA).
The PDCT provides a measurementof IOP but also two additionalparameters called the Q-value and theocular pulse amplitude (OPA). Theseare summarised in Table 4.The OPA is thought to be related tothe overall biomechanicalcharacteristics of the eye and throughthis it may also be related to the riskof glaucoma. The process of IOPmeasurement is similar to Goldmanntonometry except that no fluoresceinis required to perform themeasurements. The pressure sensor isvisually aligned with the centre of thepupil and the probe tip is rested on
the cornea for several seconds to recordan IOP measurement. As withconventional tonometry, record theaverage of three IOP readings andrecord the time of day. Due to the factthat GAT is sensitive to cornealproperties but the PDCT is not, the IOPreadings from the two instruments arenot directly comparable. Many studies have assessed theaccuracy of the PDCT since its releasein 2005 including several that havecompared direct measurement of IOPvia intracameral tonometry to thePDCT measurements. It has been foundto measure IOP accurately in eyes aftercorneal refractive surgery, with highlyswollen corneas and in eyes withcorneal disease such as keratoconus.47,48
However, there are early indicationsthat the PDCT measurements of IOPwould be better described as “less”influenced by corneal properties thanGAT, rather than completely free of thecorneal-related factors, as studies haveshown that corneal hydration and CCTmay have a small effect.49,50
Assuming that future assessment ofthis instrument follows current trends,the Pascal DCT is on track to becomethe new gold standard device for themeasurement of IOP. However, IOPmeasurements should still beconfirmed with Goldmann tonometry
< Figure 5 The Pascal Dynamic Contour Tonometermounted on a conventional slit lamp
< Figure 6The measurement probe of the PascalDynamic Contour Tonometer. Note that theprobe tip is concave
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 37

14/1
1/08
CE
T
38
CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔Sponsored by:
prior to referral until furtherinformation becomes available.
Maximising traditionaltonometryThough future developments intonometry are promising, newtechnology is typically more expensivethan conventional instruments andthus many Optometrists will be likelyto continue to use traditional contactand non-contact tonometry for manyyears to come. Therefore, it is prudentto conduct IOP measurements in lightof the issues discussed in this article inorder to reach the best clinical decisionpossible with the available evidence –a summary of the key “take home”messages appears below.
Understand IOP•There is no such thing as a “normalIOP”. •Be aware of the short and long-termfactors that can cause IOP to change,including the diurnal variation of IOP.Always record the time of day thatmeasurements are taken.•Do not measure IOP during the firsttwo hours of awakening as your resultcould be influenced by residualovernight corneal oedema.
Make sure the IOP is what you think it is•Confirm on a second day, at adifferent time, and with a Goldmanntonometer UNLESS signs of cornealoedema are present (indicating that anextreme IOP is/has been recentlypresent).•Remain aware that accuracy of IOP islimited by tonometer design. Considerthe effect of the cornea on IOPmeasurements; measure CCT but
interpret results in view of recentresearch findings.•Tonometer calibration must bechecked regularly.•Use standardised consistent methodsfor contact and non-contact tonometry,including recording the average ofthree readings per eye.
Consider the big picture•Remember that IOP is not the onlyrisk factor for glaucoma, but considerthe overall picture when makingclinical decisions about IOP.
Should I refer based on IOP alone?Referral guidelines for suspectedglaucoma vary depending on a numberof factors including your local healthauthority guidelines, the preferences ofyour local Ophthalmologists andwhether you are involved with co-management of glaucoma. Newreferrals can be accepted based on araised IOP in the absence of otherglaucomatous signs, but generallyrequire that the Optometrist hasobtained an elevated reading on 2separate days with a Goldmanntonometer.
It is necessary to refer patients withhighly elevated IOP readings(30+mmHg), but it can also bedesirable to refer a patient with an IOPin the mid-20’s if they have othersignificant risk factors for glaucoma.Whether or not treatment will beinstituted based solely on IOP is at thediscretion of the Ophthalmologist, butthey may consider the followingfactors.16
1. Risk of glaucoma is generally low inthe population
2. Burden of long term treatmentincluding possible adverse effects, costand inconvenience3. The individual’s specific risk ofdeveloping OAG and/or current state ofprogression4. The individual’s specific likelihoodof benefiting from treatment5. Health status, co-existing visionproblems and life expectancy
In an attempt to clarify the roles ofindividuals involved with glaucomadiagnosis and management, includingOptometrists, GP’s andOphthalmologist, the National Institutefor Health and Clinical Excellence(NICE) is due to release guidelines inApril 2009 and these will be madeavailable on their websitehttp://www.nice.org.uk/.
ConclusionIOP is a very strong risk factor forglaucoma and thus IOP measurementremains a key component of routine eyeexaminations conducted byOptometrists. Appropriatemeasurement and interpretation of theresults requires a good understandingof the ever-changing nature of IOP, theinfluence of the cornea on IOPmeasurement and the limitations of theinstruments themselves. Research isvery active in this field it is importantto be on the lookout for new technologyand information as it becomesavailable.
About the Author Dr Kirsten Hamilton is a lecturer at theSchool of Optometry and VisionSciences at Cardiff University. Herresearch interests are concentrated onthe relationships between the physicalcharacteristics of ocular tissues, IOPmeasurement and glaucoma.
AcknowledgementsThe author would like to thank DaveTaylor from Reichert, and YolandaSchneeberger and Jürg Blaser fromZiemer Ophthalmic Systems forallowing use of the images of the OcularResponse Analyzer and Pascal DynamicContour Tonometer respectively.
References See www.optometry.co.uk/references
Parameter Definition
IOP Intraocular pressure An IOP measurement that is said to be free of corneal influence. This reading is notdirectly comparable with GAT.
Q-value Quality valueThis is a measure of the quality of the measurement. A Q value of 1, 2 and 3 areacceptable, but 4 or 5 requires the measurement to be repeated.
OPA Ocular pulse amplitudeThe IOP increase due to the change in choroidal volume during the cardiac cycle.
< Table 4 Numbers produced by the PDCT
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 38

Sponsored by:
CONTINUINGEDUCATION &TRAININGCET
To gain more standard CET points for this year’s PAYL series, enter online at: www.otcet.co.uk or � 0207 878 2412
This issue CET: Pay as you learn ✔
Module questions Course code: C-10134Please note, there is only one correct answer. Enter online or by the form provided
Please complete online by midnight on January 14 2009 - You will be unable to submit exams after this date – answers to the module will be published in our January 16 2009 issue
An answer return form is included in this issue. It should be completed and returned to CET initiatives (c-10134) OT, Ten Alps plc, 9 Savoy Street, London WC2E 7HR by December 2 2008
1) Which of the following is not an ocular risk factor for open angle glaucoma?
a) Raised IOPb) A cornea that is thinner than averagec) Decreasing aged) A large of asymmetric cup to disc (C/D) ratio
2. Which of the following is false about the relationship between IOP and open angle glaucoma?
a) A raised IOP is associated with an increased risk of glaucomab) About 10% of patients with glaucoma have an IOP of 21mmHg or lessc) 90% of eyes with ocular hypertension with an IOP of 24-32mmHg will not
develop glaucoma within a 5 year follow-up periodd) Patients with certain ocular or systemic risk factors are more sensitive to
the level of IOP
3. Which of the following is false about IOP?a) IOP is usually similar in both eyes of the same patientb) An IOP of 20mmHg in the morning and 11mmHg in the evening would be
considered an example of an average diurnal variation of IOPc) The 21mmHg “upper limit of normal IOP” is only a statistical markerd) There is no “normal” IOP that could be applied across all age ranges
4. Which of the following can cause IOP to change by several mmHg?a) Diurnal variation of IOPb) Repeating IOP measurements numerous timesc) Lid squeezingd) All of the above
5. How often should Goldmann tonometer calibration be checked?a) Every weekb) Every monthc) Every 6 monthsd) Once a year
6. It is useful to measure central corneal thickness (CCT) because:a) Eyes with thin corneas are at an increased risk of developing glaucomab) Tonometers generally overestimate the IOP in eyes with thick corneas and
underestimate the IOP in eyes with thin corneasc) CCT may affect the response to IOP-lowering medicationd) All of the above
7. Central corneal thickness (CCT) measurement is most accurate when:a) It is measured within 2 hours of awakeningb) Only one measurement is takenc) The measurement probe is positioned at a 90º angle to the corneal apexd) The measurement is taken at a position away from the pupil centre
8. Although central corneal thickness (CCT) can affect the accuracy of IOP measurement, IOPs should not be corrected for CCT because:
a) There is no “correction factor” that is accurate in all situationsb) It is impossible to measure CCT accuratelyc) Corneal characteristics such as biomechanical behaviour can influence
IOP readingsd) Both a and c
9. Which of the following is false about the Ocular Response Analyzer?a) It produces an IOP measurement called IOPG, which is similar to Goldmann
tonometry readingsb) It produces an IOP measurement called IOPCC, which is corrected for the
effects of corneal behaviourc) It produces a measurement called OPA, which is the ocular pulse amplituded) It produces a measurement called CH, which is calculated as the difference
in pressure between 2 applanations that occur during non-contact tonometry
10. Which of the following is true about the Pascal Dynamic Contour Tonometer?a) It is a modified non-contact tonometerb) The probe tip is concave to minimise the effect of corneal propertiesc) It does not require the use of an anaestheticd) It operates via the Imbert-Fick principle
11. Elevated IOP readings should not be confirmed by which of the following?a) Repeating IOP measurement with a Goldmann tonometerb) Repeating IOP measurement at a different timec) Taking the average of three readings with a non-contact tonometerd) Repeating IOP measurement on a different day
12. Which of the following statements about tonometry is false?a) Goldmann and non-contact tonometry both cause corneal applanation b) Non-contact tonometry may be more sensitive to corneal properties than
Goldmann tonometryc) Non-contact tonometry tends to underestimate the IOP if it is raisedd) Non-contact tonometry requires an average of three readings
14/1
1/08
CE
T
39
P30-36_OT_141108_CETPAYL.qxd:CET 11/11/08 10:01 Page 39