course description: objectives - c.ymcdn.comc.ymcdn.com/sites/€¦ · combining initiatives: safe...
TRANSCRIPT

Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 1
Combining Initiatives: Safe Patient Handling, Early Mobility, and
Fall Prevention, Oh My!
Margaret Arnold, PT, CEES, CSPHPInspire Outcomes, LLC
Jennifer McIlvaine, PT, MSPT, CSPHADuke University Health System
Combined Section Meeting 2016February 17-20th, 2016 – Anaheim, CA
Speakers and Disclosures:
• Margaret Arnold receives consulting fees, honorariums, and stipends through Inspire Outcomes, LLC.
• Jennifer McIlvaine has no relevant financial relationships.
Course Description:Physical Therapists in acute care hospitals face multiple, concurrent initiatives aimed at improving the care and safety of patients. Numerous, singularly-focused initiatives, however, can lead to staff indifference and poor compliance.
There is opportunity to integrate Safe Patient Handling, Early Mobility, and Fall Prevention initiatives into one comprehensive patient care program.
This lecture will review the benefits of all initiatives and how one, large university based health system has combined them into a comprehensive program for acute care patients across all disciplines.
Objectives:
1. Describe the role of Safe Patient Handling in both Early Mobility and Fall Prevention programs.
2. Discuss benefits of assessing and categorizing patient mobility levels for acute hospitalization.
3. Demonstrate uses of low and high technology patient handling equipment and devices to progress mobility for an ICU level patient.
4. Identify opportunities to combine like and overlapping hospital‐wide patient care initiatives.
Program Silos Resource Utilization
• Preparation for and attendance at meetings
• Prevention strategy
• Implementation strategy and planning
• Root cause analysis and brainstorming when there is a failure of process
• Training and Education
• Material resources
• Data collection and PDSA initiatives
Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 2
Goals of Initiative Integration
• Maximize efficiency of resources
• Achieve consistent terminology across initiatives and disciplines
• Maximize effectiveness of interventions
• Improve integration of patient care initiatives for care planning
• Improve quality of care for the patient
• Reduce likelihood of injury to either patient or caregiver
Falls in Hospitals• >700,000 patients a year are hospitalized because of a fall injury2
• Fall injuries are among the 20 most expensive medical conditions.3
• Over 140,000 patients fall per year IN hospital • Bouldin et al, 2013
• Average rate of 3.56 falls per 1000 patient days
• 26% resulted in a serious injury
• On average a fall will increase LOS 6-12 days per fall
• Increased cost of care ~ $13,000 per fall• Bouldin et al, 2013
• Some sources report up to $35,000 cost per fall (AHRQ)
Risk Factors for Falls
• Previous Falls
• Multiple Meds
• Confusion
• Disorientation
• Weakness
• Balance and gait impairments
• Incontinence or frequent urination
• Mobility devices
• Tethered devices such as IV poles
• Vision
• Orthostatism or other physiological causes
Assessment of Fall Risk
• Morse
• Hendrichs II
• Stratify
• Tinetti
• BERG
• Dynamic Gait Index
• Timed Up and Go
Components to Consider
• Specificity of fall risk measure
• Relatability to plan of care
• Nursing versus therapist fall risk assessment
• Competing patient care initiatives
• Ceiling effect
• Dilution of impact
• Ease of use versus usefulness to prevent falls
• Actions based on scores
Impact of Immobility
• Every system affected
• Weakness
• Delirium and disorganized thinking
• Balance and gait impairment
• Incontinence
• Depressed neurological function (reflexes, reaction time)
• Pain and anxiety
• Isolation and dis-engagement
Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 3
Assessment of Mobility
• There are over 20 different assessment tools
• Most common include• Functional Independence Measure (FIM) or subset of FIM• Physical Function ICU test (PFIT)• Functional Status Score for ICU (FSS)• Acute Care Index of Function • Perme ICU mobility Scale
Variability of measured components
• Specificity
• Weighting and capture of all contributing factors
• Ability to measure meaningful change over time (Sensitivity)
• Ease versus complexity to complete
• Multi-disciplinary use and interpretation
• Actions based on scores
Mobility Prevents FallsEM programs have shown:
• Decreased weakness• Decreased Delirium• Decreased pressure ulcers• Decreased time on a
ventilator• Improved time to functional
milestones• Increased function at
discharge• Increased chance of DC
home or Rehab
Connecting Mobility and Fall Prevention
EM programs have shown:• Decreased weakness• Decreased Delirium• Decreased pressure ulcers• Decreased time on a ventilator• Improved time to functional milestones• Increased function at discharge• Increased chance of DC home or Rehab
Point Prevalence Studies
• Variable reports of patient mobility Out of bed
• <25% of patients in 116 ICU were OOB
• Only 8% of patients with ETT tube were OOB
• Another study found that no mechanically ventilated patients were ambulated and only 25% of all ICU patients stood
The scope of the problem
Study of 45 patients’ activity levels during hospitalization
Spent <3% of the day standing or walking versus at least 20 of the 24 hours per day lying in bed.

Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 4
Therapist Barriers to Mobility
• Resources (Staff, time, equipment)
• Patient size, weight and dependency, sedation
• Productivity requirements
• Fear of adverse events
• Training
Patient Barriers to Mobility
• Fear of falling
• Anxiety and pain
• Lack of confidence in caregiver
• Do not want to fail in front of therapist
• Indignity of needing people to help (especially in bariatric patients)
Risks of Manual HandlingCumulative impact of lifting >35lbs
With Permission: Bill Marras, 2015
Impact of Therapist Injuries
• 90% lifetime prevalence of therapist injuries
• Impact:• Decreased Quality of Life outside of work• Altered work practice or setting• Altered treatment Interventions
Safe Mobility Prevents FallsAnd prevents therapist injury
The Role of Safe Patient Handling and Mobility
• Safe Patient handling programs reduce injuries by > 70% on average
• Opportunities for mobility across the continuum of care
• Interdisciplinary use
• Nursing use different from Therapy use
• Fall prevention interventions should include safe patient mobility activities
Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 5
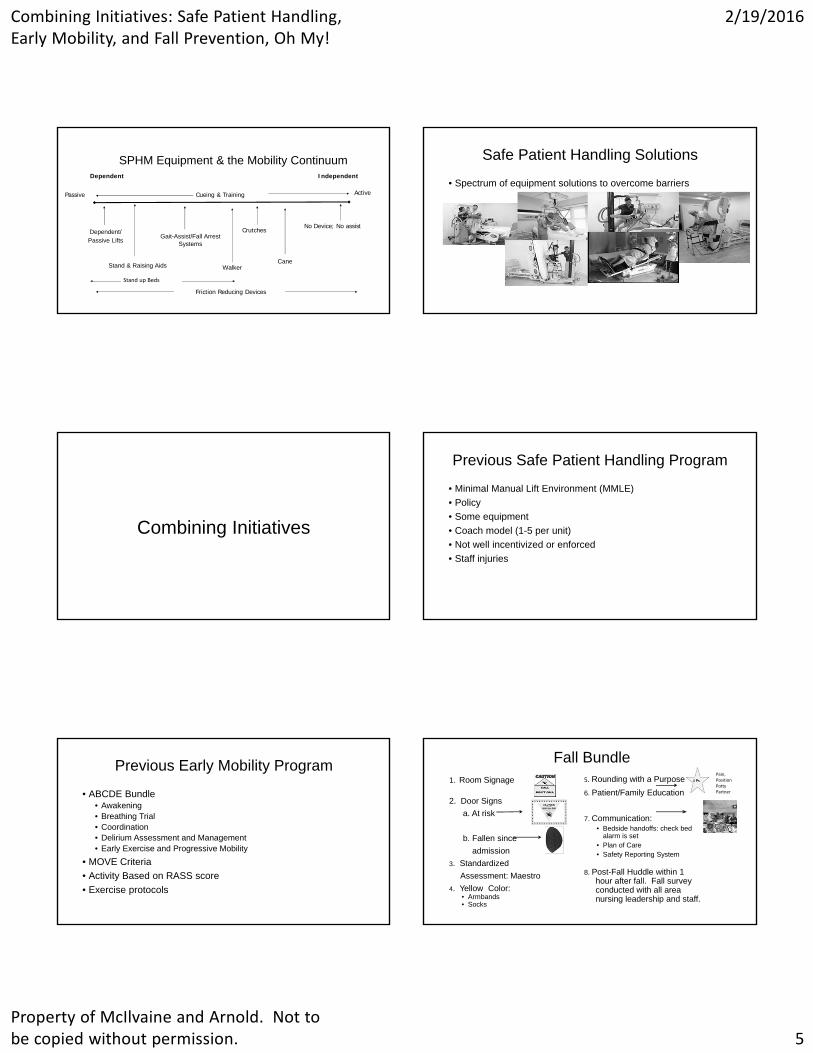
SPHM Equipment & the Mobility Continuum
CrutchesNo Device; No assist
Dependent/Passive Lifts
CaneWalkerStand & Raising Aids
Gait-Assist/Fall Arrest Systems
Passive Active
Dependent Independent
Cueing & Training
Friction Reducing Devices
Stand up Beds
Safe Patient Handling Solutions
• Spectrum of equipment solutions to overcome barriers
Combining Initiatives
Previous Safe Patient Handling Program
• Minimal Manual Lift Environment (MMLE)
• Policy
• Some equipment
• Coach model (1-5 per unit)
• Not well incentivized or enforced
• Staff injuries
Previous Early Mobility Program
• ABCDE Bundle• Awakening• Breathing Trial• Coordination• Delirium Assessment and Management• Early Exercise and Progressive Mobility
• MOVE Criteria
• Activity Based on RASS score
• Exercise protocols
Fall Bundle1. Room Signage
2. Door Signs
a. At risk
b. Fallen since
admission
3. Standardized
Assessment: Maestro
4. Yellow Color: • Armbands• Socks
5. Rounding with a Purpose
6. Patient/Family Education
7. Communication: • Bedside handoffs: check bed
alarm is set• Plan of Care• Safety Reporting System
8. Post-Fall Huddle within 1hour after fall. Fall surveyconducted with all areanursing leadership and staff.
4 Ps
Pain, PositionPottyPartner

Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 6
Patient Safety Initiatives
Safe Patient Handling & Movement
Fall Prevention
Early Mobility
SPHM ANA Interdisciplinary Standards
1. Culture of Safety
2. Sustainable SPHM Program
3. Ergonomic Design Principles
4. SPHM Technology
5. Education, Training, and Maintaining Competence
6. Patient-Centered Assessment
7. Reasonable Accommodation and Post-Injury Return
8. Comprehensive Evaluation System
Results of Benchmarking Survey
• Safe Patient Handling policy
• Metrics-injury data and worker’s compensation cost
• Champion/peer leader model
• Communication-EHR vs. board in patient room
• Annual budget-varies
• Program managed by FTE
Results of Benchmarking Survey
• Equipment needs based on unit risk assessments
• Equipment is purchased by units
• No rewards programs
• Re-validate skills annually
• Clinic staff do not assist & no equipment available
• Lift teams
Foundation
• Policy• Patient handling >35 lb• “All HCWs will avoid High Risk Patient Handling Tasks whenever
possible, with the exception of emergency situations.”• Training• Equipment maintenance and storage
• Role Descriptions• Facility Coordinator• Unit Champion• Unit Coach• Unit Manager
Duke MOVES Structure
Duke Moves Entity
Coordinator
ManagerClinical Team
Lead
Champion
Coach
10‐15 FL Staff
Coach
10‐15 FL Staff
Coach
10‐15 FL Staff
Coach
10‐15 FL Staff
DUHS Oversight
Committee

Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 7
Equipment Standard for Intensive/Critical Care Units Equipment Standard for Step-Down Units
Equipment for Medical/Surgical Units Additional Equipment:
Mobility Assessment
• ANA Standard 6: Assessing patients to plan care for their individual needs
• Differences between therapy and nursing
• Banner Mobility Assessment Tool
Mobility LevelDoes patient have activity order?Safety Screen Is it safe to move patient?
Strict Bedrest Bedfast
Mobility Level 1 Bedfast/DependentUnable to move or transfer self
Mobility Level 2 Moderately dependentCan come to sitting position but unable stand or transfer
Mobility Level 3 Minimal assistance required Can bear weight and may require assistive device(s)
Mobility Level 4 IndependentCan move and transfer self and requires no patient handling assistance

Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 8
Combining Initiatives Communication• All handoffs
• Bedside at change of shift: RN and NCA• Upon transfer from unit/department to unit/department
• Signage• Door• White Board recommended
• Plan of Care
• Collaborate closely with PT/OT to create a plan that includes therapy goals
Training
• Linking to Values—Safety, Excellence, Teamwork
• Patient safety = Staff safety
• Toolkit for Champions
• All resources on-line
• Videos
PT Role
• PTs have a strong influence on patient mobility in hospitals
• Leaders in patient safety initiatives
• Change therapy culture• adhere to 35 lb lift recommendation• patient and family education• manage expectations
• Collaborate with nursing staff
References:• Arnold M, Radawiec S, Campo M, & Wright L. Changes in functional independence measure ratings
associated with a safe patient handling and movement program. Rehab Nur. 2011;36(4):38-144.
• Arnold M, Wilson C, McIlvaine J, et al. Integrating mobility and safe patient handling: Practical considerations for interdisciplinary care. Am J SPHM. 2015;5(2):S1-S21.
• Boynton T, Kelly L, Perez A, et al. Banner Mobility Assessment Tool: Instrument Validation. Am J SPHM. 2014;4(3):86-94.
• Campo M, Shiyko M, Margulis H, & Darrag, A. Effect of a safe patient handling program on rehabilitation outcomes. Arch Phys Med Rehab. 2013;94(1):17-22.
• McIlvaine J, Anderson J, & Harwood K. Integrating patient handling equipment into physical therapy activities in a rehabilitation setting: A case series. Am J SPHM. 2011;1(3):16-22.
• Morris P, Goad A, Thompson C, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med. 2008;36(8):2238-2243.
• Nelson, A, Harwood K, Tracy C. et al. Myths and facts about safe patient handling in rehabilitation. Rehab Nursing. 2008;33(1):10-17.
• Waters T. When is it safe to manually lift a patient? Am J of Nur. 2007;107(8):53-58.
References:
• Oliver D. Falls risk-prediction tools for hospital inpatients. Time to put them to bed? Age Ageing2008;37(3):248-50. Available at: http://ageing.oxfordjournals.org/content/37/3/248.long.
• Bouldin ED, Andersen EM, Dunton NE, Simon M, Waters TM, et al. Falls among Adult Patients Hospitalized in the United States: Prevalence and Trends. J Patient Saf. 2013 Mar; 9(1): 13–17.doi: 10.1097/PTS.0b013e3182699b64
• Parry SM, Granger CL, Berney S, Jones J, Beach L, et al Assessment of impairment and activity limitations in the critically ill: a systematic review of measurement instruments and their clinimetricproperties. Intensive Care Med. 2015 May;41(5):744-62. doi: 10.1007/s00134-015-3672-x. Epub2015 Feb 5.
• Darragh, A. R., Campo, M. A., Frost, L., Miller, M., Pentico, M., & Margulis, H. (2013). Safe-patient-handling equipment in therapy practice: Implications for rehabilitation. American Journal of Occupational Therapy, 67, 45–53.
• Darragh AR, Campo M & Olson D. Therapy practice within a minimal lift environment: Perceptions of therapy staff. Work: A Journal of Prevention, Assessment, and Rehabilitation, 2009. 33(3); 241-253
• Covinsky KE, MD, MPH; Pierluissi E, MD; Johnston B, MD, MPH, (2011). Hospitalization-Associated Disability“She Was Probably Able to Ambulate, but I’m Not Sure” JAMA. 306(16):1782-1793. doi:10.1001/jama.2011.1556

Combining Initiatives: Safe Patient Handling, Early Mobility, and Fall Prevention, Oh My!
2/19/2016
Property of McIlvaine and Arnold. Not to be copied without permission. 9
References:
• Cromie JE, Robertson VJ & Best MO. Work-related musculoskeletal disorders in physical therapists: Prevalence, severity, risks and responses. Physical Therapy, 2000. 80(4); 336-351.
• Romano J. Rella A, Jost S, MK.Fitzpatrick. Promoting a Safe Patient Handling Culture in an Acute Care Hospital to Decrease Work-Related Injuries and Improve Quality Indicators, Poster, SPHM Conference 2009, , Hospital University of Pennsylvania
• Kimberley T, Samargia S, Shakya J, Lang C. Comparison of amounts and types of practice during rehabilitation for traumatic brain injury and stroke. Journal Of Rehabilitation Research & Development [serial online]. December 2010;47(9):851-861. Available from: CINAHL with Full Text, Ipswich, MA. Accessed March 29, 2012
• Morris PE, Griffin L, Berr M, Thompson C, Hite RD, Winkleman C, Hopkins RO, Ross A, Dixon L, Leach S & Haponik E, (2011). Receiving Early Mobility During an Intensive Care Unit Admission is a Predictor of Improved Outcomes in Acute Respiratory Failure. The American Journal of the Medical Sciences, 341(5), 373-377.
• Safe Patient Handling Programs : Effectiveness and Cost Savings. OSHApublication. Retrieved from<http://www.osha.gov/dsg/hospitals> on April 4, 2015.
References:
• Taylor, J; Sims, J; Haines, TP. The impact of manual handling on nursinghome resident mobility during transfers on and off furniture: a systematicreview Journal of Gerontological Nursing 2011:37(8): 48-56.
• Boyd CM, Landefeld, CS, Counsell SR, Palmer RM, Fortinski RH, Kresevic D, Covinsky KE. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008; 56: 2171-2179.
• Callen B, Mahoney J, Wells T, Enloe M, Hughes S. Admission and discharge mobility of frail hospitalized older adults. MedSurg Nursing. 2004; 13(3): 156-164.
• Vollman K. Progressive Mobility in the Critically Ill. Critical Care Nurse, 2010; 30(2): S3-S4.
• Casey CM. The study of activity in older ICU patients: an integrative review. J Gerontol Nurs. 2013; 39(8): 12-25. doi: 10.3928/00989134-20130603-02.
• Dai B, Ware W, & Guiliani C. A structural equation model relating physical function, pain, impaired mobility (IM) and falls in older adults. Archives of Gerentology and Geriatrics, 2012; 55: 645-652.
References:
• Daynard D, Yassi A, Cooper JE, Tate R, Norman R, Wells R. Biomechanical analysis of peak and cumulative spinal loads during simulated patient-handling activities: a substudy of a randomized controlled trial to prevent lift and transfer injury of health care workers. Applied Ergonomics. 2001; 32: 199-214.
• Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009; 373(9678): 1874–1882.
• Taylor ME, Delbaere K, Lord SR, Mikolaizak AS, Brodaty H, Close JCT. Neuropsychological, Physical, and Functional Mobility Measures Associated With Falls in Cognitively Impaired Older Adults. J Gerontol A Biol Sci Med Sci. 2014; 69(8): 987-995.