delirium prevention, assessment and management susan schumacher, ms, g-cns
TRANSCRIPT

Delirium Prevention, Assessment and Management
Susan Schumacher, MS, G-CNS
Objectives
• Identify 3 differences in clinical presentation of delirium versus underlying dementia.
• Explain how to perform the Confusion Assessment Method (CAM).
• Identify at least 3 factors contributing to the development of delirium.
• Identify appropriate interventions to prevent or shorten the course of delirium.
• Describe pharmacological treatment of delirium.

What is Delirium?
A transient state of cognitive impairment manifested by simultaneous disturbance of behaviors that develop abruptly and fluctuate diurnally (daily)

Changes Observed in Delirium
• Level of consciousness• Attention• Perception• Memory• Thinking• Orientation• Psychomotor behavior
Perceptions from Patients
• “I thought there were some photographers and things around taking advantage of people.”
• Felt like “someone had pulled a curtain.”• Felt like “hospital staff were plotting
against me.”
– McCurren, Cronen (2003)
How Common is Delirium?
• Incidence within hospital 4-53.3%• Complicates hospital stay for more than 2.3
million older persons annually• Occurs in 5-61% of orthopedic patients,
especially those with hip fractures• Between 22-89% of patients with delirium have
underlying dementia.• Prevalence in patients receiving mechanical
ventilation is as high as 83%.
Differentiating Delirium and Dementia
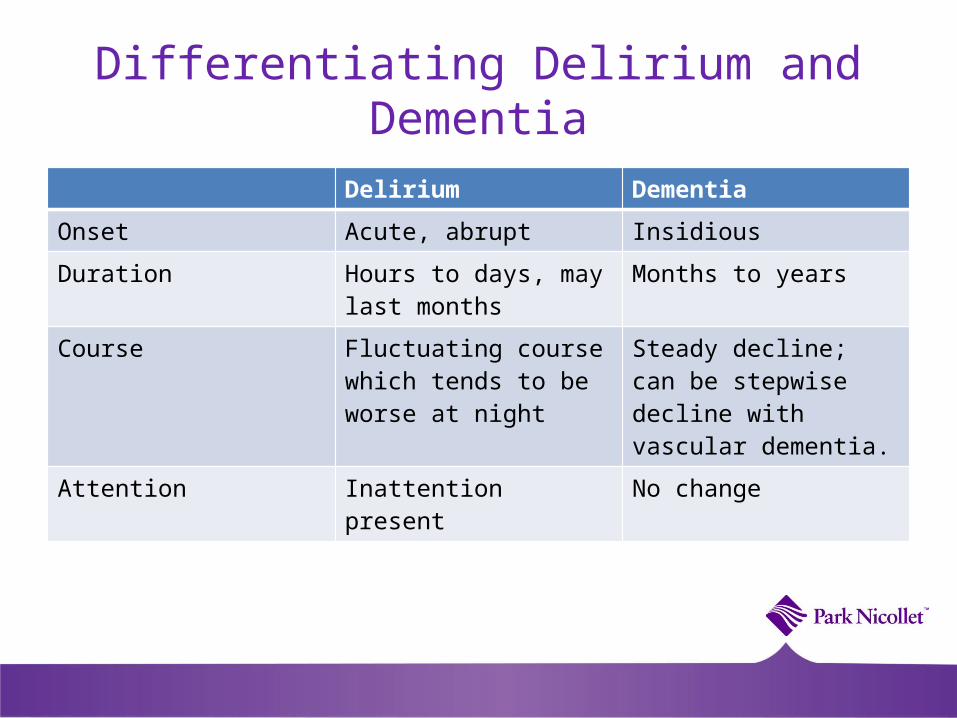
Delirium Dementia
Onset Acute, abrupt Insidious
Duration Hours to days, may last months
Months to years
Course Fluctuating course which tends to be worse at night
Steady decline; can be stepwise decline with vascular dementia.
Attention Inattention present No change
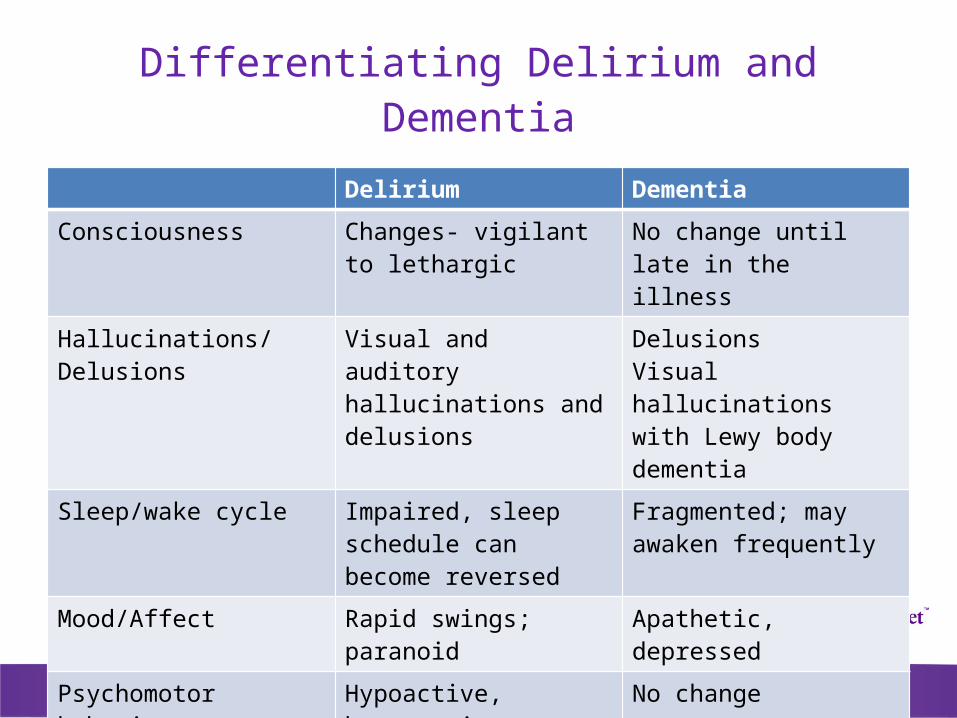
Differentiating Delirium and Dementia
Delirium Dementia
Consciousness Changes- vigilant to lethargic
No change until late in the illness
Hallucinations/Delusions Visual and auditory hallucinations and delusions
DelusionsVisual hallucinations with Lewy body dementia
Sleep/wake cycle Impaired, sleep schedule can become reversed
Fragmented; may awaken frequently
Mood/Affect Rapid swings; paranoid Apathetic, depressed
Psychomotor behavior Hypoactive, hyperactive or mixed
No change

Outcomes Related to Delirium
• Length of stay• Higher level of care at discharge• Increased mortality after discharge • Increased risk of adverse events
Investigating the factors leading to Delirium (Multi-factorial)
• Underlying risk factors: Factors that cannot be changed which impact delirium.
• Precipitating factors: Factors that contribute to development of delirium which can be changed.

Underlying Risk Factors
• Dementia• Substance abuse• Parkinson’s disease• Sensory deficits• Age• Traumatic brain injury• Chronic kidney disease
Precipitating Factors
• Hypoxia• Infections• Electrolyte imbalances• Anemia• Medications• Uncontrolled pain• Constipation• Tethers (catheters)

What is Confusion Assessment Method(CAM)?
• Diagnostic assessment tool for delirium developed by Sharon Inouye (Yale)
• Assesses 4 features of delirium:– Acute onset and fluctuating course– Inattention– Disorganized thinking– Altered level of consciousness
Completion of CAM
• On admission for all patients greater than 70 years
• Every 8 hours for patients greater than 70 years• Supportive information:
– Hours of sleep– Agitation score– Behaviors– Nursing interventions
CAM Assessment on Admission
• Completed and documented within 4 hours of admission– Baseline Cognitive Status Impairment
(dementia, traumatic brain injury, other neurologic diseases impacting cognition)
– Admission Cognitive Status– CAM completed by Surgery Center RN for
surgical patients (documented in PICIS)
Criteria for Patients Unable to Complete the CAM
• Language Barrier (unable to speak english)
• Receptive/Expressive Aphasia• Unconscious or sedated (Use CAM-ICU)• Severe stage of dementia or brain injury
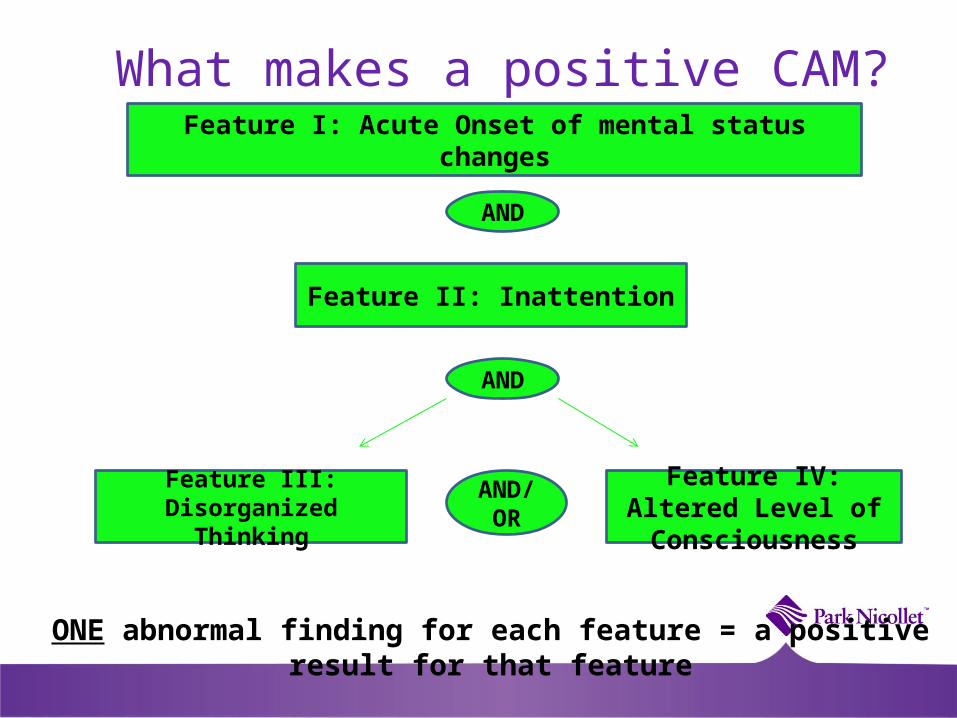
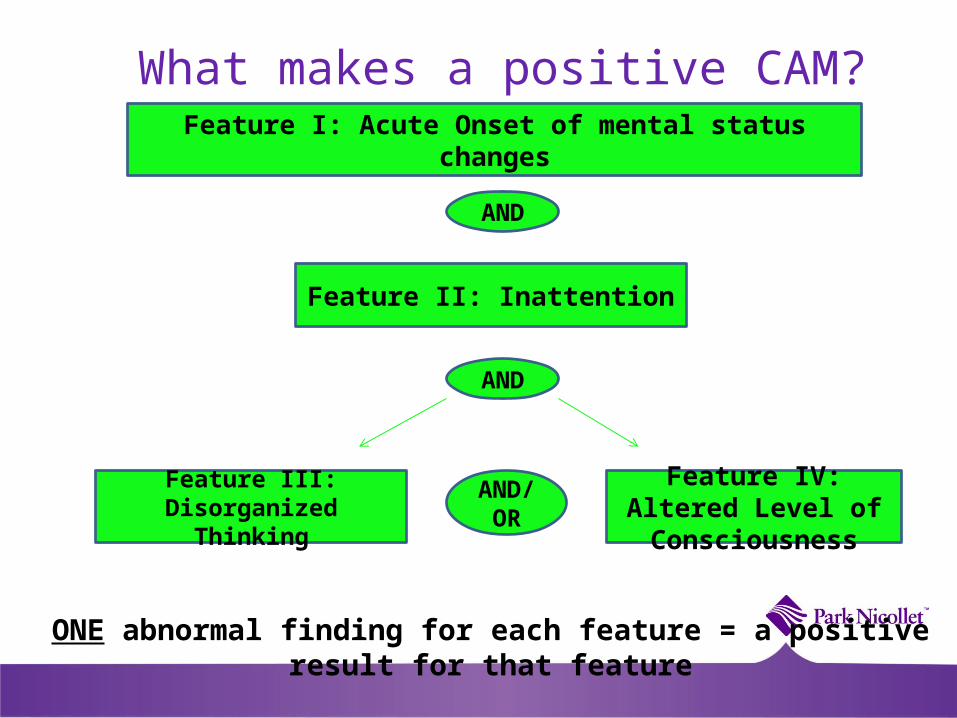
What makes a positive CAM?Feature I: Acute Onset of mental status changes
AND
Feature II: Inattention
Feature III: Disorganized Thinking
Feature IV: Altered Level of
Consciousness
ONE abnormal finding for each feature = a positive result for that feature
AND
AND/ OR
Confusion Assessment Method(CAM)
• Criteria 1 (Acute onset and Fluctuating Course)- Has patient changed from their baseline cognitive status? Does the behavior fluctuate during the day, such as worse in the evening or night?

Case Study- Criteria 1
• An 88 yr old woman who is admitted with an intracranial bleed and has underlying mild cognitive impairment. She has been alert and oriented to person, place and time. She is cooperative with cares, but has a difficult time remembering to use the call light. At 3am she wakes up and cries out for help, pulls out her IV line, tries to push nursing staff away and is paranoid about what the staff are trying to do with her.
Case Study- Criteria 1
• A 79 yr old man admitted for total hip is POD #3. He has underlying dementia (mild), CAD, Type II diabetes, and osteoarthritis. Patient’s bed alarm is going off 2-3 times/ shift, as he tries to get out of bed to use bathroom and he forgets to use the call light. He is alert and oriented to person and place, slept well during the night and cooperates with nursing cares. He asks the staff about calling his wife several times every shift.

Confusion Assessment Method (CAM)
Criteria 2-Inattention
• Does the patient have difficulty focusing attention, for example, being easily distractible, or having difficulty keeping track of what was being said?
Case Study- Criteria 2
• Talking with a patient about his hospital stay, patient gives eye contact to the nurse initially, but when an x-ray machine moves past his door, his focus shifts to the hallway. Also, patient unable to follow the directions that nurse has provided about using call light when needing assistance.

Confusion Assessment Method(CAM)
• Criteria 3(Disorganized Thinking) Is the patient’s speech disorganized or incoherent, such as rambling or irrelevant conversation, unclear or illogical flow of ideas, or unpredictable switching from subject to subject?

Confusion Assessment Method(CAM)
Criteria 4
• Overall, how would you rate this patient’s level of consciousness?
Levels of Consciousness
• Alert (normal)• Vigilant (hyperalert)• Lethargic (drowsy, easily
aroused)• Stupor (difficult to arouse)• Coma (unarousable)

Score
Term Description
+4 Combative Overtly combative, violent, immediate danger to staff
+3 Very agitated Pulls or removes tubes or catheters, aggressive
+2 Agitated Frequent non-purposeful movement, fight ventilator
+1 Restless Anxious but movements not aggressive, vigorous
0 Alert and calm
-1 Drowsy Not fully alert, but has sustained awakening (eye opening/eye contact) to voice (> 10 seconds)
-2 Light Sedation Briefly awakens with eye contact to voice (< 10 seconds)
-3 Moderate Sedation
Movement or eye opening to voice (but no eye contact)
-4 Deep Sedation No response to voice, but movement or eye opening to physical stimulation
-5 Unarousable No response to voice or physical stimulation
Richmond Agitation Sedation Scale (RASS)
What makes a positive CAM?Feature I: Acute Onset of mental status changes
AND
Feature II: Inattention
Feature III: Disorganized Thinking
Feature IV: Altered Level of
Consciousness
ONE abnormal finding for each feature = a positive result for that feature
AND
AND/ OR

Let’s Practice!
E-paging a new Positive CAMDelirium is an urgent medical condition. A positive CAM test should be
reported immediately so the patient can be evaluated for delirium quickly.
Have this information ready when you page:• BGM• Last void/is patient retaining urine• Oxygen saturation• Last BM• Pain status• Temperature & Blood Pressure• I & O balance• Latest labs if available (serum K, Na, Mg, Cr, etc)• Agitation Score
Confirm your CAM POSITIVE result with the Charge Nurse before paging.
If no response within 10 mins,
call an RET
Interventions to Prevent and Manage Delirium
• Delirium Prevention Trial (Inouye)– Patients in the highest adherence group
demonstrated an 89% reduction in delirium risk compared with patients in the lowest group.
– Protocols for orientation, therapeutic activities and mobility make a significant difference when implemented consistently!

Intervention Protocols
Protocols:
• Orientation
• Therapeutic activities
• Mobility

Interventions for Delirium
• Medication management– Review for culprit
medications– Pharmacy consult– Administer
medications for delirium per order set
– Pain Management
Interventions for Preventing and Resolving Delirium
• A2 Evidence – Promotion of nutrition– Removal of urinary catheter and
other tethers– Early mobilization– Glasses and hearing aides– Pain management– Bowel and bladder needs– Fluids and electrolyte balance– Adequate 02

Patient and Family Education
• Brochure/Booklet– What is Delirium?– Why is it occurring ? – What can be done to
treat and resolve it?– What can family
members do to help?
Comfort Measures and patients with Dementia
• Temperature (hot or cold?)
• Hungry or thirsty• Over or under- stimulated• Bowel or bladder needs• Provide reassurance• Personal items such as
family pictures
Hospital Elder Life Program (HELP)
• A comprehensive program of care for hospitalized older patients, designed to PREVENT delirium and functional decline.
• Target patient =>70 years old with a LOS > 2 days.
HELP® Goals• Maintain physical and cognitive functioning throughout hospitalization
(through daily interventions) • Maximize independence at discharge • Assist with the appropriate transition from hospital to home or step-down
setting • Improve geriatric skills of staff throughout the general medicine units.
Hospital Elder Life Program (HELP)
Trained program volunteers: 100
Patient visits per
month: 400!!

Hospital Elder Life Program (HELP)
Key interventions of the program• Daily visitor program with structured cognitive orientation • Therapeutic activities program • Early mobilization • Non-pharmacologic sleep protocol • Hearing and vision protocol • Feeding and fluid assistance • Geriatric patient care education for unit nursing staff
How to order a HELP consult

Delirium Order set- Medications
• IV Haloperidol (Haldol) (Severe, Moderate Hyperactive Delirium and Hypoactive Delirium)– Scheduled doses of Haldol based on RASS score – PRN doses to reduce agitation to 0 on RASS scale or until 8mg
given (moderate) 12mg (severe)– Contact provider if Haldol every 30 minutes for 2hours is not
decreasing agitation.– Weaning off Haldol (once pt goes 24 hours without prn dose)– Try to avoid in patients with Parkinson’s disease– Risk of prolongation of the QT/QTc interval (baseline and daily
EKG)

Why the daily EKG?
Prolongation of QT/QTc interval may occur with any antipsychotic medication (Haldol) and increases risk for Torsades de Pointes.

Delirium Order set- Medications
• QUEtiapine (Seroquel)– Used for patients with
Parkinson’s disease– May give Haldol and Ativan
additionally for RASS score of +3. (Combative patient)
– Watch of orthostatic hypotension
• LORazepam (Ativan)– Given with IV Haldol for
very agitated patients ONLY

Prevention of Delirium is Key!
References• Inouye,S., Baker, D., Fugal, P. & Bradley, E. (2006). Dissemination of the hospital
elder life program: Implementation, adaptation, and successes. Journal of Gerontological Society, 54:1492-1499.
• Inouye,S., Bogardus,S., Williams,C. & Leo-Summers,L. (2003). The role of adherence on the effectiveness of nonpharmacologic interventions. Archives of Internal Medicine, 163: 958-964.
• Robinson,S., Rich, C., Weitzel,T., Vollmer, C. & Eden,B. (2008). Delirium prevention for cognitive, sensory, and mobility impairments. Research and Theory for Nursing practice: An International Journal, 22(2): 103-113.
• Sendelbach, S.& Finch Guthrie,P. (2009). Acute Confusion/Delirium. In M.G. Titler (Series Ed.), Series on Evidence-Based Practice for Older Adults, Iowa
City, IA: The University of Iowa College of Nursing Interventions Research Center, Research Translation and Dissemination Core.