designing home health technologies for older adults: the...
TRANSCRIPT

361Biomedical Instrumentation & Technology September/October 2014
Features
Designing Home Health Technologies For Older Adults: The Human Systems Integration Approach
Cara Fausset and Linda Harley
From intensive care units with dozens of highly trained healthcare professionals to home healthcare in which patients manage their own health, the modern healthcare system spans many users, tasks, and environ-ments. The home healthcare system is vast and variable, depending on the level of care that each person requires. Our goal is to discuss the human systems integration approach for designing home health technolo-gies for older adults. By understanding user abilities and task demands, and how those factors interact within the home environment, designers can develop technologies that positively impact older adults’ quality of life. For the purposes of demonstrating how the human systems integration approach may be applied to medical device development, the scope of this article has been limited to older adult patients living alone in their homes who need to use a blood pressure monitor.
There is an ever increasing need for health technology to migrate into the home environ-ment. According to the Association of American Medical Colleges, the U.S. is facing a tremendous shortage of doctors and nurses.1 The expansion of healthcare services through the Affordable Care Act, coupled with the growing population of older adults and the large number of primary-care physicians set to retire are cited as contributors to a need for more than 52,000 primary-care doctors by 2025.2 In addition, nursing home costs have risen from an average of $8,280 per patient
per year to an average of $57,600 per patient per year in 2002 according to the Centers for Disease Control and Prevention (CDC).3 With costs rising rapidly, an affordable option is for older adults to manage their own health at home.4,5 Properly designed home health technology can be used to deliver medical care (e.g., oxygen, infusion, dialysis) and monitor health status in real time (e.g., blood pressure, glucose, fall detection), potentially saving both time and money that would otherwise be spent in a doctor’s office or nursing home.
The potential benefits of home health technology are numerous. Home health monitoring can alert healthcare professionals to provide proactive care and reduce the likelihood of a hospital visit. Proper health management at home can also reduce the number of days a person stays in the hospi-tal, thereby lowering costs and the probability of contracting a hospital-borne disease.6 Well-designed home health technology can also support the goal of older adults’ to maintain their independence.7,8
About the Authors
Cara Fausset is a research scientist at the Georgia Tech Research Institute in Atlanta, GA. E-mail: [email protected]
Linda Harley is a research scientist at the Georgia Tech Research Institute in Atlanta, GA. E-mail: [email protected]
By understanding user abilities and task demands, and how those factors interact within the home environment, designers can develop technologies that positively impact older adults’ quality of life.
© Copyright AAMI 2014. Single user license only. Copying, networking, and distribution prohibited.
362 Biomedical Instrumentation & Technology September/October 2014
Features
Bringing health technology into older adults’ homes presents challenges. Older adults may have limited experience or familiarity with technology in general, possibly putting them at a disadvantage when interacting with health technologies likely designed based on existing technology (e.g., touchscreens). Age-related changes in cognition, perception, and physical capabili-ties exacerbated by illness may also interfere with optimal health technology adoption and acceptance.9,10,11 Moreover, the home environ-ment may not be suitable for interacting with health technology due to factors such as unreliable power sources, inadequate lighting, loud ambient noise (e.g., TV is always on), limited space for operation and storage, and intermittent or no Internet
connectivity.7 Given these challenges, home health technology that is designed without consideration of users’ abilities, task demands, and home environment factors could compromise users’ safety and technol-ogy effectiveness.11
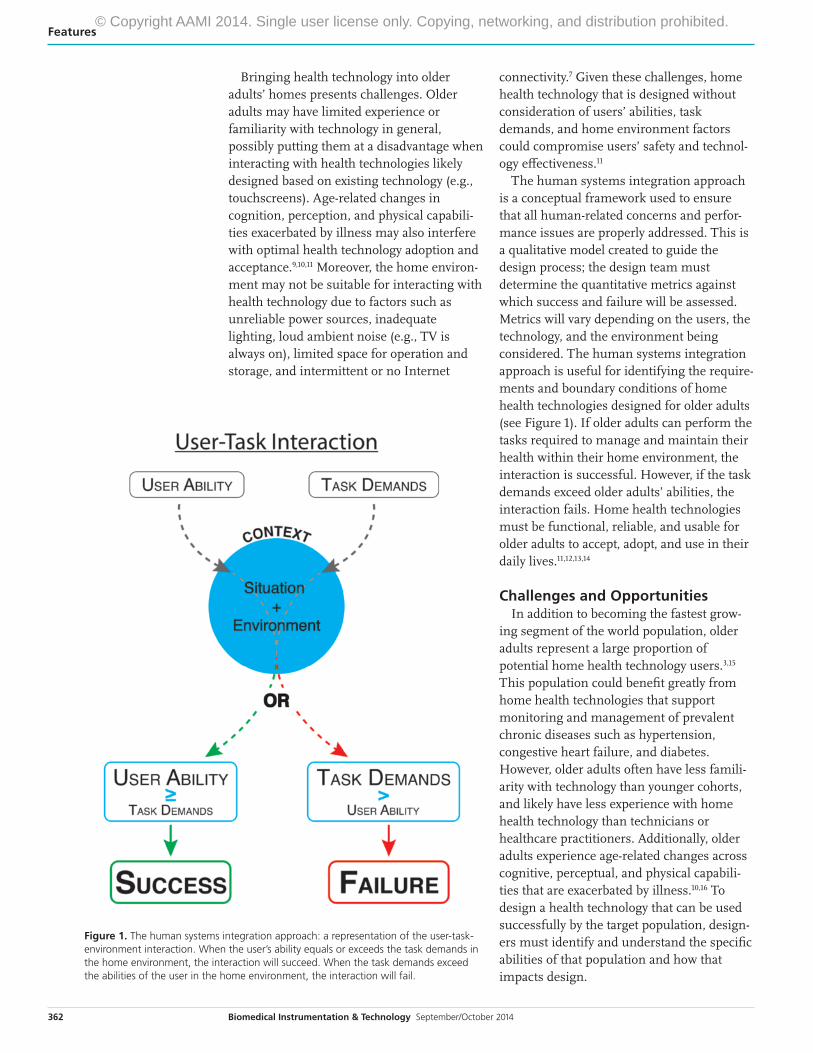
The human systems integration approach is a conceptual framework used to ensure that all human-related concerns and perfor-mance issues are properly addressed. This is a qualitative model created to guide the design process; the design team must determine the quantitative metrics against which success and failure will be assessed. Metrics will vary depending on the users, the technology, and the environment being considered. The human systems integration approach is useful for identifying the require-ments and boundary conditions of home health technologies designed for older adults (see Figure 1). If older adults can perform the tasks required to manage and maintain their health within their home environment, the interaction is successful. However, if the task demands exceed older adults’ abilities, the interaction fails. Home health technologies must be functional, reliable, and usable for older adults to accept, adopt, and use in their daily lives.11,12,13,14
Challenges and OpportunitiesIn addition to becoming the fastest grow-
ing segment of the world population, older adults represent a large proportion of potential home health technology users.3,15 This population could benefit greatly from home health technologies that support monitoring and management of prevalent chronic diseases such as hypertension, congestive heart failure, and diabetes. However, older adults often have less famili-arity with technology than younger cohorts, and likely have less experience with home health technology than technicians or healthcare practitioners. Additionally, older adults experience age-related changes across cognitive, perceptual, and physical capabili-ties that are exacerbated by illness.10,16 To design a health technology that can be used successfully by the target population, design-ers must identify and understand the specific abilities of that population and how that impacts design.
Figure 1. The human systems integration approach: a representation of the user-task-environment interaction. When the user’s ability equals or exceeds the task demands in the home environment, the interaction will succeed. When the task demands exceed the abilities of the user in the home environment, the interaction will fail.
© Copyright AAMI 2014. Single user license only. Copying, networking, and distribution prohibited.

363Biomedical Instrumentation & Technology September/October 2014
Features
From Telegram to SmartphoneThe range and variability in home health technologies present different challenges for users; therefore it is essential that a task analysis be conducted to fully understand the task demands each health technology places on its users. There are many different types of task analyses that can be conducted, but all analyses provide a systematic way to describe the human interaction with a system.17 The goal of conducting task analyses is to understand how to match users’ capabilities to the system demands. Important types of information assessed in a task analysis include the following: hierarchical relationships; information flow; task sequence; location; and environmental conditions.3 A complete system task analysis should include not only the user interface, but should also investigate the ease of storage, portability, professional support infrastructure, and maintenance of the technology, as well as that of educational materials on how to use the technology.14,17
The following high-level task analysis example explores the tasks necessary to use a blood pressure monitor that connects to a smartphone:1. Connect blood pressure monitor to smart-
phone2. Launch smartphone application3. Place blood pressure cuff around arm4. Start measurement5. Wait until measurement completes6. Read measurement7. Remove blood pressure cuff8. Send reading to electronic health records9. Close the smartphone application10. Disconnect blood pressure monitor from
smartphone11. Use results to inform future health
decisions such as food choices, salt intake, etc.
No Two Homes are AlikeThe home environment presents unique challenges because of the unpredictability and the variability of the home environment. A range of characteristics must be consid-ered, from a state-of-the-art senior housing development designed to support aging in place to a 1920s two-story home with narrow doorways, steep stairwells, poor insulation,
and dim lighting. Some examples of these characteristics may include:• Availability of proper infrastructure (e.g.,
power, Internet connectivity, refrigeration) • Environmental factors (e.g., narrow
doorways, noise, temperature, lighting, humidity, storage space)
• Access to services (e.g., cleaning, mainte-nance, technical assistance, waste disposal)
• Controlling access to the health technology (e.g., kids, animals, nurses, pharmacists)
Currently, many medical technologies designed for the hospital environment are directly translated into the home environ-ment. However, there are some fundamental differences in the environment between the hospital and home that should be considered, such as availability of trained medical staff to operate the technology, ease of maintaining and replacing faulty technology, and infra-structure. For example, in most hospitals, oxygen lines are built into the infrastructure so as to provide a hookup valve next to the patient’s bed. However, in the home, portable oxygen systems are employed so as to allow the person to move around their home freely. Different environments often result in different design criteria.
The Human Systems Integration ApproachTo illustrate using the human systems integration approach, let’s consider Harold. He is 72 and has hypertension and diabetes. Hypertension can cause severe headaches, fatigue, confusion, vision problems, chest pain, difficulty breathing, and irregular heartbeat. Diabetes can cause fatigue, nausea, blurred vision, and neuropathy. His severe diabetic highs and lows cause decrements in his cognitive processing and
Currently, many medical technologies designed for the hospital environment are directly translated into the home environment. However, there are some fundamental differences in the environment between the hospital and home that should be considered, such as availability of trained medical staff to operate the technology, ease of maintaining and replacing faulty technology, and infrastructure.
© Copyright AAMI 2014. Single user license only. Copying, networking, and distribution prohibited.

364 Biomedical Instrumentation & Technology September/October 2014
Features
fine movement control, and can impact his use of devices. Harold must monitor his blood pressure and glucose daily. Harold lives by himself in an old house with poor lighting, clutter, and the television is always on. Recently, Harold’s doctor recommended that he use a blood pressure monitor that connects to a smartphone.
The human systems integration approach allows designers to identify problem areas and discuss possible mitigations. Table 1 outlines Harold’s ability profile, considering two different user interface options of connecting the blood pressure monitor to the smartphone, and the problems that arise when given the interaction of the user-task
environment. As shown in this task analysis, the wired connection requires a high degree of physical dexterity to connect the device to the smartphone, but once it is connected, the application could launch without further interaction. In contrast, the
Bluetooth connection requires a high degree of knowledge to pair the device with the smartphone, but the physical requirements are reduced. If designers are concerned about the physical constraints of the user, they may decide to forego a physical connection between the blood pressure monitor and the smartphone and instead rely on Bluetooth connection. However, this may present a new set of issues, such as how to provide instruc-tions on how to pair the blood pressure
monitor with the smartphone (electronic manual versus paper manual, font size, etc.), as well as concerns surrounding transmitting patient data securely between devices. If designers want to reduce the cognitive requirements of the device, they may decide to implement the wired connection over the Bluetooth connection. Designers must recognize that mitigations may introduce new problems, and therefore should consider the tradeoffs between different designs.
ConclusionA few of the benefits and challenges intro-duced by bringing health technologies into the homes of older adults have been pre-sented. The grand challenge facing home health technology designers is providing technologies that are both safe and easy to use by older adults in the home environment. The human systems integration approach is a conceptual framework that is intended to guide the design process in identifying the requirements, trade-offs, and boundary conditions of home health technologies designed for older adults.
Designers are tasked with ensuring that the tasks required to operate home health technologies do not exceed the abilities of the user. This requires an in-depth assessment of both the capabilities and limitations of the target user, as well as an assessment of the skills and abilities necessary to use the device. If the task demands exceed the abilities of the older adults, the technology is unlikely to be useful. Home health technolo-
The grand challenge facing home health technology designers is providing technologies that are both safe and easy to use by older adults in the home environment.
Factors Demands User Ability
Wired Connection
Physical High: Fine motor dexterity and strength required to insert connector into smartphone and monitor.
Neuropathy leads to loss of dexterity and inability to complete this task.
Cognitive Low: Knowledge required to know which end of the connector goes into which device.
Hypertension and diabetes can lead to confusion and therefore inability to know what to do for this task.
Perceptual High: Visual acuity required to see the connection points in the devices.
The inputs on the phone and monitor may be too small to read for people with vision impairment.
Bluetooth Connection
Physical Low: Gross movement control to tap the screen of the smartphone.
Neuropathy leads to loss of sensation in fingertips and the ability to sense touch.
Cognitive High: Knowledge required to pair the device to the smartphone.
Inability to know what to do for this task. More demanding than the wired.
Perceptual High: Visual acuity required to see the on-screen smartphone information.
The font size may be too small, or the contrast may be too low, for people to read text.
Table 1. A human systems integration example of connection blood pressure monitor to a smartphone.
© Copyright AAMI 2014. Single user license only. Copying, networking, and distribution prohibited.
365Biomedical Instrumentation & Technology September/October 2014
Features
gies must be functional, reliable, and usable for older adults to accept, adopt, and use in their daily lives. The degree to which design-ers account for these challenges and adopt the human systems integration approach will support the success of future home health technology design. n
References1. Dill MJ, Salsberg ES. The Complexities of Physician
Supply and Demand: Projections Through 2025.
Association of American Medical Colleges.
2008. Available at: https://members.aamc.org/
eweb/upload/The%20Complexities%20of%20
Physician%20Supply.pdf. Accessed Sept. 4, 2014.
2. Petterson SM, Liaw WR, Phillips RL, Rabin
DL, Meyers DS, Bazemore AW. Projecting U.S.
Primary Care Physician Workforce Needs: 2010-
2025. Ann Fam Med. 2012;10(6):503-509.
3. National Center for Health Statistics. Health,
United States, 2012: With Special Feature on
Emergency Care: 2013. Hyattsville, MD. Available
at: www.cdc.gov/nchs/data/hus/hus12.pdf.
Accessed Sept. 4, 2014.
4. Chappell NL, Havens B, Honorary D, Hollander
MJ, Miller JA, McWilliam C. Comparative
Costs of Home Care and Residential Care. The
Gerontologist. 2004;44:389-400.
5. Grabowski DC. The Cost Effectiveness of Non-
Institutional Long-Term Care Services: Review
and Synthesis of the Most Recent Evidence. Med
Care Res Rev. 2006;63:3-28.
6. Korhonen I, Parkka J, Van Gils M. Health
Monitoring in the Home of the Future.
Engineering in Medicine and Biology
Magazine. 2003;22(3):66-73. Available at:
http://ieeexplore.ieee.org/stamp/stamp.
jsp?tp=&arnumber=1213628&isnumber=27287.
Accessed Sept. 4, 2014.
7. Barrett LL. Healthy @ Home 2.0: Full Report.
Washington, DC: AARP; 2011.
8. Bronstein L, Gellis Z D, Kenaley BL. A
Neighborhood Naturally Occurring Retirement
Community: Views from Providers and Residents.
J Appl Genontol. 2011; 30:104-112.
9. Birren JE, Schaie KW. Handbook of the Psychology
of Aging. 6th ed. Amsterdam: Elsevier Academic
Press, 2011.
10. Eggermont LH, de Boer K, Muller M, Jaschke
AC, Kamp O, Scherder EJ. Cardiac Disease and
Cognitive Impairment: A Systematic Review.
Heart. 2012;98(18):1334-1340.
11. Fisk AD, Rogers WA, Charness N, Czaja SJ,
Sharit J. Designing for Older Adults: Principles and
Creative Human Factors Approaches. 2nd ed. Boca
Raton: CRC Press.
12. Salvendy G. Handbook of Human Factors and
Ergonomics. 3rd ed. Hoboken: John Wiley, 2006.
13. US Food and Drug Administration. Design
Considerations for Devices Intended for Home Use.
DRAFT: 2012. Available at: www.fda.gov/downloads/
MedicalDevices/DeviceRegulationandGuidance/
GuidanceDocuments/UCM331681.pdf. Accessed
Sept. 4, 2014.
14. Wickens CD, Lee JD, Liu Y, Becker SEG. An
Introduction to Human Factors Engineering. 2nd
ed. Upper Saddle River: Pearson, 2004.
15. United Nations Department of Economic and
Social Affairs. World Population Aging 2013.
New York, NY: UN Department of Economic and
Social Affairs; 2013. Available at: www.un.org/en/
development/desa/population/theme/ageing/
index.shtml. Accessed Sept. 4, 2014.
16. Hung WW, Wisnivesky JP, Siu AL, Ross JS.
Cognitive Decline Among Patients with Chronic
Obstructive Pulmonary Disease. Am J Resp Crit
Care. 2009;180(2):134-137.
17. Kirwan B, Ainsworth LK. A Guidebook to Task
Analysis. 1st Ed. Bristol: Taylor & Francis Inc., 1992.
© Copyright AAMI 2014. Single user license only. Copying, networking, and distribution prohibited.

Order Your Copy Today! Call +1-877-249-8226 Visit http://my.aami.org/store
Benchmark It!Select the web-based benchmarking resource to fit your needs...
Designed for healthcare technology management departments, this features over 70 measurements:
• Staffing levels
• Cost of maintenance contracts
• Personnel qualifications and responsibilities
• Number of devices maintained
Designed for sterile processing departments, this features more than 175 benchmarking metrics:
• Budgeting and financial issues
• Sterilization practices
• Volume and types of work performed
• Staffing, qualifications, and much more.
Helps device companies compare elements of their quality management systems with those of their peers. It features more than 100 measurements covering:
• RISK MANAGEMENT: Adherence to standards, management involvement, and documentation
• CORRECTIVE & PREVENTIVE ACTION (CAPA): Issue escalation, CAPA management, and preventive action statistics
Order code: ABS
List $850
AAMI member $750
Order code: SPB
List $850
AAMI member $750
Order code: QMS
List $1,450
AAMI member $1,100
Benchmarking SolutionsSterile Processing
Benchmarking SolutionsHTM
Benchmarking SolutionsQuality Management System for Medical Devices
Benchmarking data can be submitted at the corporate, division, or site level. Developed with input from FDA, AdvaMed, and leading Risk Management and CAPA experts.
© Copyright AAMI 2014. Single user license only. Copying, networking, and distribution prohibited.