developing health management information systems who library cataloguing in publication data...
TRANSCRIPT

WORLD HEALTH ORGANIZATIONREGIONAL OFFICE FOR THE WESTERN PACIFIC
DevelopingHealth ManagementInformation Systems
A PRACTICAL GUIDE FORDEVELOPING COUNTRIES

ii
WHO Library Cataloguing in Publication Data
Developing health management information systems: a practical guide fordeveloping countries
1. Management information systems 2. Guidelines 3. Developing countries
ISBN 92 9061 1650 (NLM Classification: WA 26.5)
© World Health Organization 2004All rights reserved.
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the World Health Organization concerning the legalstatus of any country, territory, city or area or of its authorities, or concerning the delimitation of itsfrontiers or boundaries. Dotted lines on maps represent approximate border lines for which there maynot yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they areendorsed or recommended by the World Health Organization in preference to others of a similar naturethat are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguishedby initial capital letters.
The World Health Organization does not warrant that the information contained in this publication iscomplete and correct and shall not be liable for any damages incurred as a result of its use.
Publications of the World Health Organization can be obtained from Marketing and Dissemination,World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax:+41 22 791 4857; email: [email protected]). Requests for permission to reproduce WHO publications,in part or in whole, or to translate them – whether for sale or for noncommercial distribution – should beaddressed to Publications, at the above address (fax: +41 22 791 4806; email: [email protected]).For WHO Western Pacific Regional Publications, request for permission to reproduce should be addressedto Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932,1000, Manila, Philippines, Fax. No. (632 521-1036, email: [email protected]).
The named author/s alone is/are responsible for the views expressed in this publication.
Acknowledgements
The WHO Regional Office for the Western Pacific acknowledges the contributions made
by Dr Ophelia Mendoza, WHO Consultant, and Dr Y.C. Chong, Regional Adviser in
Health Information.
iii
Acknowledgements . . . . . . . . . . . ii
Abbreviations . . . . . . . . . . . . v
1 Introduction . . . . . . . . . . . . 1
2 The basic concepts . . . . . . . . . . 3
3 Reviewing the existing system . . . . . . . . 5
4 Defining data needs . . . . . . . . . . 9
5 Determining the data flow . . . . . . . . . 13
6 Designing the data collection and reporting tools . . . . 17
7 Developing procedures for data processing . . . . . 21
8 Developing the training programme . . . . . . . 25
9 Pre-testing the system . . . . . . . . . . 29
10 Monitoring and evaluating the system . . . . . . 33
11 Developing data dissemination and feedback mechanisms . . 37
12 Enhancing the HMIS . . . . . . . . . . 41
Examples . . . . . . . . . . . . . 45
References . . . . . . . . . . . . . 53
Contents

iv

v
Abbreviations
ARICP Acute Respiratory Infection Control Programme
BCG Bacille-Calmette Guérin
CDSS Communicable Disease Surveillance System
CHC Commune Health Centre
DHC District Health Centre
DHS Department of Hospital Services
DOF Department of Finance
DMCH Department of Maternal and Child Health
DP Department of Planning
DPT Diphteria-Pertussis-Tetanus
DSS Disease Surveillance System
EH Environmental Health
EPI Expanded Programme of Immunization
FPSF Family Planning Service Facilities
H Hospital
HACP HIV/AIDS Control Programme
HMIS Health Management Information Systems
MCH Maternal and Child Health
MOE Ministry of Education
MOH Ministry of Health
NIN National Institute of Nutrition
NMCP National Malaria Control Programme
NSO National Statistics Office
NTCP National Tuberculosis Control Programme
OPV Oral Polio Vaccine
ORS Oral Rehydration Salts
PHC Primary Health Centre
PHO Provincial Health Office
PMC Preventive Medical Centre
TT Tetanus Toxoid

vi

1
Purpose of the Manual
This Manual is designed to be a quick-and-easy, user-friendly reference for the
development of health management information systems (HMIS), with the focus
on applications. It serves as a primer on HMIS development and provides a general
overview of the basic principles, as well as the fundamental steps and issues
involved in the different activities to be undertaken. The information is presented
in a concise, direct-to-the point, easy-reading, and outline format. It aims simply
to provide the basic elements on HMIS development for people who do not
have the time or the need to read deeply on the subject. For those who wish to
develop a more in-depth knowledge, the Manual can also serve as the springboard
for further reading and research.
Prospective Users of the Manual
This Manual was designed with the following persons in mind:
➤ Heads and staff of Statistics Units at the national, provincial, or even the
district health service level who are actively involved in the development of
their HMIS
➤ People who do not have the in-depth background on HMIS but need to have
a general overview of its components because they are members of Multi-
disciplinary Committees tasked with overseeing the development of the HMIS
in their country
➤ Managers and staff of vertical programmes whose responsibilities include
any component of the information system of their respective programmes
Scope and Style of the Manual
Each chapter in this Manual has four parts:
(a) Principles
(b) Steps
(c) Issues
(d) Worksheets
1 Introduction

2
The worksheets give the reader an idea of how to go through the different steps,
or how to process the different issues in an organized and systematic manner.
Sample entries for the worksheets are provided to demonstrate how they are
filled out.
The last part of the Manual gives an example of a list of basic indicators that
might be used in Ministry of Health programmes, together with the corresponding
data sources, modes and frequency of data collection, as well as the lowest
administrative level where the indicator is computed. While the reader can adopt
some of these indicators for their use, the main objective of the example is to
show how the set of indicators used by a country can be presented so that it will
be easy for the staff of the Statistics Unit to monitor their status. Also provided
at the end of the Manual is an example of a flow chart of the HMIS of hypothetical
country X. As in the first example, the aim is to show not “what”, but “how”;
not to prescribe a model flowchart for the HMIS as such, but rather to demonstrate
how the HMIS can be presented by means of a flow chart.

3
Some Definitions
System A collection of components that work together to achieve a common
objective1
Information System A system that provides information support to the
decision-making process at each level of an organization2
Health Information System A system that integrates data collection,
processing, reporting, and use of the information necessary for improving health
service effectiveness and efficiency through better management at all levels of
health services3
Health Management Information System An information system
specially designed to assist in the management and planning of health
programmes, as opposed to delivery of care4
Steps in Developing a Health Management Information System
(1) Review the existing system
(2) Define the data needs of relevant units within the health system
(3) Determine the most appropriate and effective data flow
(4) Design the data collection and reporting tools
(5) Develop the procedures and mechanisms for data processing
(6) Develop and implement a training programme for data providers and data
users
(7) Pre-test, and if necessary, redesign the system for data collection, data flow,
data processing and data utilization
(8) Monitor and evaluate the system
(9) Develop effective data dissemination and feedback mechanisms
(10) Enhance the HMIS
1 World Health Organization (2000)2 Hurtubise (1984)3 World Health Organization (2000)4 World Health Organization (1993)
2 The basic concepts

4

5
S T E P S
P R I N C I P L E
(1) Make an inventory of the forms, log books and other tools used to record and
summarize data at different levels.
(2) Assess the quality of the data being collected using the existing forms at different
levels. Among the aspects to be included in the assessment are:
➤ Accuracy
➤ Completeness
➤ Adequacy
➤ Timeliness
(3) Determine the problems encountered with the current system of data collection at
different levels, including the timing and flow of information.
(4) Determine the current status of the other components of the HMIS like:
➤ Data processing
➤ Data analysis
➤ Data dissemination
➤ Supply and logistics
➤ Staff development
➤ Coordination, cooperation and communication within and between different
units in the Ministry of Health, as well as with related agencies outside of the
ministry
Do not destroy existing systems; build on the strengths and learnfrom the weaknesses of what already exists.
3 Reviewing theexisting system

6
I S S U E S
(1) Who has the authority to make the assessment?
(2) Availability of technical expertise and resources to do the assessment.
(3) Cooperation among the different units in the assessment process; involvement of
end-users at all levels.
(4) Formation of a body (ideally an inter-departmental committee) tasked with planning,
monitoring and managing all phases of the development of the HMIS, from the
baseline assessment to the evaluation phase.
(5) Identify the aspects of the system that need to be:
➤ Retained
➤ Modified
➤ Abolished
(6) Summarize the results of the assessment in a formal report.
(7) Discuss results of the assessment with proper authorities.

7
WO
RK
SH
EE
TS
Wo
rksh
eet
3.1:
Ch
eck
list
of
Pro
ble
ms
En
cou
nte
red
Wit
h t
he E
xis
tin
g H
MIS
, at
Dif
fere
nt
Ad
min
istr
ati
ve L
evels
Typ
e o
f Pr
ob
lem
s En
cou
nte
red
Vill
age
Dis
tric
tPr
ovi
nce
Nat
ion
al
Dup
licat
ion
of f
orm
s✓
Too
man
y re
cord
boo
ks/f
orm
s be
ing
fille
d ou
t at
thi
s le
vel
✓
Lack
of
cons
tant
sup
ply
of f
orm
s
Repo
rts
not
subm
itted
on
time
Inad
equa
te t
rain
ing
of h
ealth
wor
kers
on
how
to
fill o
ut f
orm
s✓
✓
Hig
h de
gree
of
inac
cura
cies
in d
ata
colle
cted
✓✓
Lack
of
tech
nica
l exp
ertis
e of
sta
ff t
o pr
oper
ly a
naly
ze t
he d
ata
colle
cted
✓✓
✓✓
Lack
of
utili
zatio
n of
dat
a be
ing
colle
cted
✓✓
✓✓
Low
leve
l/no
diss
emin
atio
n of
and
fee
dbac
k ab
out
data
col
lect
ed

8
Wo
rksh
eet
3.2:
Ch
eck
list
of
Pro
ble
ms
En
cou
nte
red
Wit
h t
he E
xis
tin
g F
orm
s
Typ
e o
f Pr
ob
lem
s En
cou
nte
red
MC
H F
orm
Form
2--
----
----
-Fo
rm (
n)
Entr
ies
in t
his
form
dup
licat
e th
ose
of o
ther
for
ms
✓
Too
man
y da
ta e
lem
ents
req
uire
d to
com
plet
e th
is f
orm
✓
Stru
ctur
e of
the
for
m is
too
com
plic
ated
, mak
ing
it di
ffic
ult
to f
ill o
ut
Diff
icul
t to
col
lect
the
dat
a re
quire
d to
fill
out
the
for
m
Writ
ten
inst
ruct
ions
on
how
to
fill o
ut t
he f
orm
are
not
ava
ilabl
e✓
Lack
of
cons
tant
sup
ply
of t
his
form
Com
plet
ed f
orm
not
sub
mitt
ed o
n tim
e
Inad
equa
te t
rain
ing
of h
ealth
wor
kers
on
how
to
fill o
ut t
he f
orm
✓
Hig
h de
gree
of
inac
cura
cies
in d
ata
colle
cted
✓
Not
all
item
s in
the
for
m a
re f
illed
out
or
com
plet
ed✓
Ther
e ar
e di
ffic
ultie
s in
col
lect
ing
dat
a fo
r th
is f
orm
fro
m a
ll ge
ogra
phic
or
serv
ice
area
s co
vere
d
Lack
of
tech
nica
l exp
ertis
e of
sta
ff t
o pr
oper
ly a
naly
ze t
he d
ata
colle
cted
fro
m t
his
form
✓
Lack
of
utili
zatio
n of
dat
a be
ing
colle
cted
fro
m t
his
form
✓
Low
leve
l/no
diss
emin
atio
n of
dat
a co
llect
ed f
rom
thi
s fo
rm

9
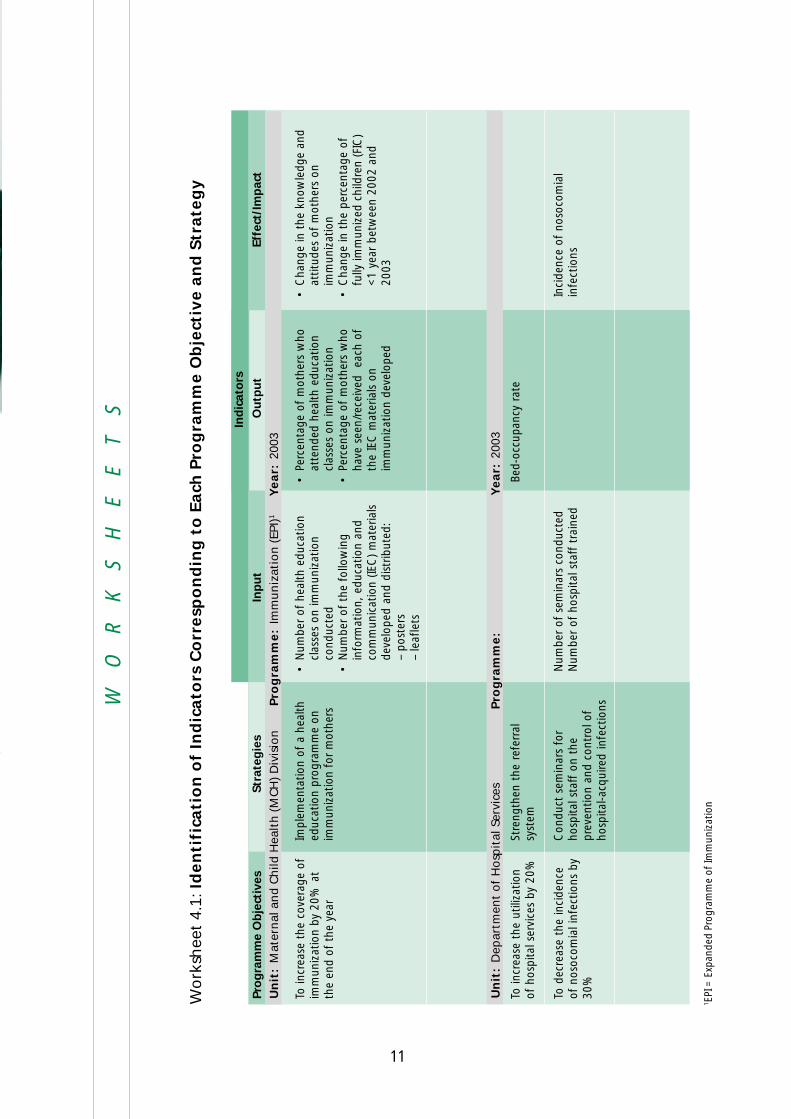
(1) Define the different roles/functions of each level, for each of the major programmes.
A common set-up is as follows:
Different administrative levels in the health system have
different roles, and therefore have different data needs.
Not all data needs should be generated through the
routine system of data collection. Data that are not
frequently needed or are required only for certain subsets
of the population can be generated through special studies
and sample surveys.
(2) Identify the indicators needed by each level to perform its functions. Note that
some levels, especially at higher administrative levels, need data coming from other
ministries or departments related to the health sector.
(3) Determine the formula and identify the variables or data elements needed in order
to compute the indicators.
P R I N C I P L E S
S T E P S
4 Defining data needs
Administrative Level Function
Village Case finding; service delivery
District Monitoring and supervision
Province Programme planning; evaluation
National Policy formulation

10
(1) Roles and functions of different units with respect to data generation and utilization
are not well defined.
(2) Defining minimum basic data needs.
(3) Differentiating data that should be included in the routine data collection system,
from data that are best generated through the conduct of special studies and
sample surveys.
(4) Inability of staff at different levels to identify their data needs; understanding of
indicators often lacking.
(4) Determine the source of the different data elements needed for both the numerator
and denominator of each indicator. The major sources can be:
➤ Routine data generated from the health management information system of
the Ministry of Health
➤ Special studies and surveys conducted by the Ministry of Health, as the need
arises
➤ Other health-related information systems under the responsibility of other
agencies or institutions (Examples of these are the vital registration system –
usually under the Department of Justice or the National Statistics Office – and
the nutrition data collected by the Ministry or Department of Agriculture)
I S S U E S
Group discussion on selecting relevant health indicators.
11
WO
RK
SH
EE
TS
Wo
rksh
eet
4.1:
Id
en
tifi
cati
on
of
Ind
icato
rs C
orr
esp
on
din
g t
o E
ach
Pro
gra
mm
e O
bje
ctiv
e a
nd
Str
ate
gy
Pro
gra
mm
e O
bje
ctiv
es
To in
crea
se t
he c
over
age
ofim
mun
izat
ion
by 2
0% a
tth
e en
d of
the
yea
r
To in
crea
se t
he u
tiliz
atio
nof
hos
pita
l ser
vice
s by
20%
To d
ecre
ase
the
inci
denc
eof
nos
ocom
ial i
nfec
tions
by
30%
Inp
ut
•N
umbe
r of
hea
lth e
duca
tion
clas
ses
on im
mun
izat
ion
cond
ucte
d•
Num
ber
of t
he f
ollo
win
gin
form
atio
n, e
duca
tion
and
com
mun
icat
ion
(IEC
) m
ater
ials
deve
lope
d an
d di
strib
uted
:–
post
ers
–le
afle
ts
Num
ber
of s
emin
ars
cond
ucte
dN
umbe
r of
hos
pita
l sta
ff t
rain
ed
Ind
icat
ors
Effe
ct/I
mp
act
•C
hang
e in
the
kno
wle
dge
and
attit
udes
of
mot
hers
on
imm
uniz
atio
n•
Cha
nge
in t
he p
erce
ntag
e of
fully
imm
uniz
ed c
hild
ren
(FIC
)<
1 ye
ar b
etw
een
2002
and
2003
Inci
denc
e of
nos
ocom
ial
infe
ctio
ns
Stra
teg
ies
Impl
emen
tatio
n of
a h
ealth
educ
atio
n pr
ogra
mm
e on
imm
uniz
atio
n fo
r m
othe
rs
Stre
ngth
en t
he r
efer
ral
syst
em
Con
duct
sem
inar
s fo
rho
spita
l sta
ff o
n th
epr
even
tion
and
cont
rol o
fho
spita
l-acq
uire
d in
fect
ions
Ou
tpu
t
•Pe
rcen
tage
of
mot
hers
who
atte
nded
hea
lth e
duca
tion
clas
ses
on im
mun
izat
ion
•Pe
rcen
tage
of
mot
hers
who
have
see
n/re
ceiv
ed
each
of
the
IEC
mat
eria
ls o
nim
mun
izat
ion
deve
lope
d
Bed-
occu
panc
y ra
te
Un
it:
Mat
ern
al a
nd
Ch
ild H
ealt
h (
MC
H)
Div
isio
nPro
gra
mm
e:
Imm
un
izat
ion
(EP
I)1
Year:
2003
Un
it:
Dep
artm
ent
of
Ho
spit
al S
ervi
ces
Pro
gra
mm
e:
Year:
2003
1 EPI
= E
xpan
ded
Prog
ram
me
of Im
mun
izat
ion

12
Wo
rksh
eet
4.2:
Id
en
tifi
cati
on
of
Data
Need
s at
Dif
fere
nt
Levels
Ind
icat
or
Num
ber
of h
ealth
educ
atio
n cl
asse
son
imm
uniz
atio
nco
nduc
ted
Perc
enta
ge o
fch
ildre
n <
1 w
hoar
e fu
llyim
mun
ized
(FIC
)
Bed
Occ
upan
cyRa
te
Nos
ocom
ial
Infe
ctio
n Ra
te
Un
it R
equ
irin
g In
dic
ato
r
Uti
lizat
ion
Vill
age
Vill
age
Dis
tric
t
Dis
tric
t
Pro
v.H
lth
Serv
.
Nat
l.M
CHPr
og
.
Nat
l.Pl
an/S
tat.
Ofc
.O
ther
s
Dis
t.H
lth
Serv
.C
olle
ctio
n
Vill
age
Vill
age
Dis
tric
t
Dis
tric
tLow
est
Leve
l of
Freq
uen
cy o
fC
olle
ctio
n
Qua
rter
ly
Bian
nual
Mon
thly
Ann
ually
Dat
a So
urc
e fo
r
Nu
mer
ato
r
MC
H F
orm
1
EPI F
orm
1
Dai
lyH
ospi
tal
Cen
sus
Form
Patie
ntM
edic
alRe
cord
s
Den
om
inat
or
Not
App
licab
le
Targ
et C
lient
List
for
EPI
Med
ical
Reco
rds
Dep
t.
Med
ical
Reco
rds
Dep
t.
Form
ula
Non
e
(No.
of
FIC
am
ong
1yr
old
chi
ldre
n / T
otal
no. o
f ch
ildre
n <
1) x
100
(No.
of
occu
pied
bed
-da
ys/t
otal
ava
ilabl
ebe
d-da
ys)
x 10
0
(No.
of
in-p
atie
nts
who
dev
elop
hosp
ital-a
cqui
red
infe
ctio
ns w
ithin
the
year
/tot
al n
umbe
r of
hosp
ital i
n-pa
tient
-da
ys w
ithin
the
yea
r)x
100
Dep
art
men
t o
f M
ate
rnal
an
d C
hil
d H
ealt
h
Dep
art
men
t o
f H
osp
ital Serv
ices

13
(1) Determine what data will be submitted to whom. This involves the:
➤ Identification of variables/indicators that need to be submitted to higher levels
➤ Identification of most appropriate unit and position of person to whom
summaries will be submitted
A major determining factor for this step is the function of the office and/or the
person to whom the data is submitted in relation to the generation and utilization
of information.
(2) Determine how frequently data should be submitted to each level, considering the
following factors:
➤ Needs of each level
➤ How common phenomenon is observed
Reports on infrequent events, or ones that are not often needed (e.g., the number
of immunization campaigns conducted in a village) can be submitted on a quarterly
or on a semi-annual basis, instead of monthly.
(3) Determine in what form data will be submitted to each level.
➤ Raw data versus summaries
➤ Hard copies versus electronic files
Not all the data collected at a certain level need to be submittedto higher levels. The most detailed data should be kept at the
source, and reporting requirements to higher levels should be keptat a minimum.
5 Determiningthe data flow
P R I N C I P L E
S T E P S

14
(1) Lack of understanding of use for which data is collected.
(2) Inability to distinguish which data are needed for service delivery and which data
are needed for programme management and monitoring.
(3) Inability of lower administrative levels to generate summaries of raw data collected
due to:
➤ Lack of technical expertise of staff
➤ Lack of data processing facilities (calculators, computers, etc.)
➤ Lack of computer skills of staff
(4) Lack of storage facilities for raw data at lower administrative levels.
(5) Data retrieval issues; inability to generate any information because of computer
breakdown.
(4) Make a flow chart that shows the flow of information from the peripheral to the
highest level. An example of this flow chart is shown in Figure 5.1. Another example
is shown in the Appendix.
I S S U E S
Discussion on how to streamline morbidity/mortality reporting.

15
WO
RK
SH
EE
T
Wo
rksh
eet
5.1:
Su
mm
ary
of
Data
Flo
w o
f EPI
Rep
ort
at
Each
Ad
min
istr
ati
ve L
evel
Ad
min
istr
ativ
eLe
vel
Vill
age
Dis
tric
t
Prov
ince
Nat
iona
l
Posi
tio
n o
f Pe
rso
n in
Ch
arg
eo
f A
cco
mp
lish
ing
Fo
rm/R
epo
rt
Publ
ic H
ealth
Nur
se in
cha
rge
ofEP
I pro
gram
me
EPI D
istr
ict
Nur
se S
uper
viso
r
EPI P
rovi
ncia
l Nur
se S
uper
viso
r
MC
H P
rogr
amm
e In
form
atio
nO
ffic
er
Form
s/R
epo
rts
Acc
om
plis
hed
at
this
Lev
el
EPI V
illag
e H
ealth
Cen
tre
Form
1
EPI D
istr
ict
Sum
mar
y Fo
rm 1
EPI P
rovi
nce
Sum
mar
y Fo
rm 1
EPI N
atio
nal S
umm
ary
Form
1
Posi
tio
n o
f Pe
rso
n in
Ch
arg
e
EPI D
istr
ict
Nur
se S
uper
viso
r
EPI P
rovi
ncia
l Nur
se S
uper
viso
r
MC
H P
rogr
amm
e M
anag
er
Info
rmat
ion
Off
icer
Un
it/O
ffic
e
Stat
istic
s U
nit,
Dis
tric
t H
ealth
Ser
vice
Stat
istic
s U
nit,
Pro
vinc
ial H
ealth
Ser
vice
MC
H D
ivis
ion,
Nat
iona
l Off
ice
MO
H P
lann
ing
and
Stat
istic
s O
ffic
e
Freq
uen
cy o
fSu
bm
issi
on
Qua
rter
ly
Qua
rter
ly
Qua
rter
ly
Qua
rter
ly
To W
ho
m C
om
ple
ted
Fo
rm/R
epo
rt is
Su
bm
itte
d

16
Fig
ure
5.1
Flo
w C
hart
of
EPI
Data
Fro
m t
he V
illa
ge t
o t
he N
ati
on
al
Level
���
���
���
���
��
��
�
����������� ���������� �������� ��������������
��
��
����
��
���
��
���
��
���
����
��
� �
���
�����������������������������
��
��
����
��
���
��
���
����
�����
����
��
� �
���
�������������������������������
��
���
����
���
����
���
����
���
���
���
��������������������
���
��
���
���
���
��
���
���
����
���
��
���
����
���
���
���
��������������������
��������
����������
��������
�����
������� ����������

17
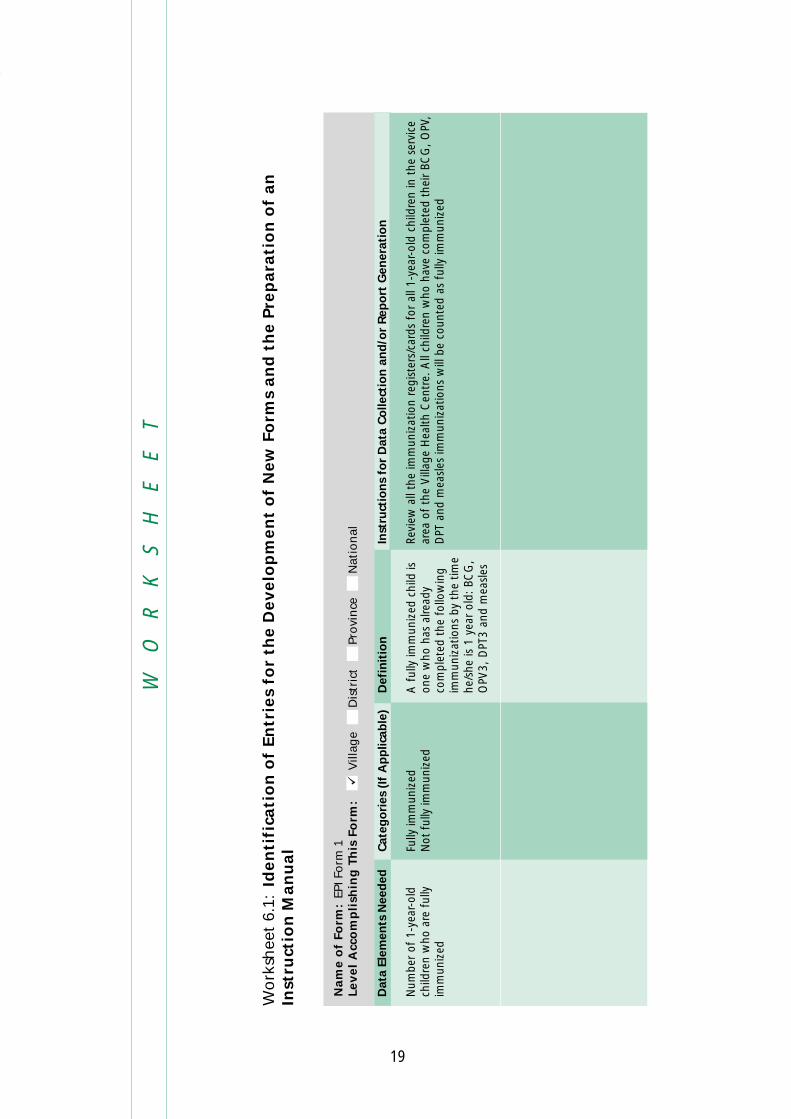
(1) Develop the first draft of each form that is needed, using as a guide the list of
indicators to be used for the programme. This step entails either the modification
of existing forms, or the development of new ones.
(2) Compare the first draft of the form that has been developed with the list of indicators
to ensure that all the data needs can be generated from the form.
(3) Present the first draft of the form to relevant staff members and discuss with them
the following aspects of the new form:
➤ How does it compare with the old forms?
➤ What are the advantages and disadvantages of the new form?
➤ What modifications need to be done to the new form to enhance its advantages
and minimize the disadvantages?
➤ For countries that have a number of dialects, is it necessary to translate the
forms into the major dialects used in the different regions of the country?
(4) Prepare a draft of the Instructions Manual on how to fill out the new forms.
(5) Pre-test the use of the new forms as well as the Instructions Manual.
(6) Assess the results of the pre-test.
(7) Modify the forms and the Instructions Manual based on the results of the pre-test.
6 Designing thedata collection andreporting tools
P R I N C I P L E S
S T E P S
The capability of the staff who will be tasked with filling out theforms must be taken into consideration in designing them.
The most effective data collection and reporting tools are simpleand short.

18
(1) Technical expertise/capability of data providers at data source is not consistent with
the level of complexity needed for data collection tools to meet the data needs of
users.
(2) Designing the pre-testing activity, ensuring the comparability of conditions with
actual implementation.
➤ Where?
➤ Who will be involved?
➤ How long?
I S S U E S
19
WO
RK
SH
EE
T
Wo
rksh
eet
6.1:
Iden
tifi
cati
on
of
En
trie
s fo
r th
e D
evelo
pm
en
t o
f N
ew
Fo
rms
an
d t
he P
rep
ara
tio
n o
f an
Inst
ruct
ion
Man
ual
Dat
a El
emen
ts N
eed
ed
Num
ber
of 1
-yea
r-ol
dch
ildre
n w
ho a
re f
ully
imm
uniz
ed
Def
init
ion
A f
ully
imm
uniz
ed c
hild
ison
e w
ho h
as a
lread
yco
mpl
eted
the
fol
low
ing
imm
uniz
atio
ns b
y th
e tim
ehe
/she
is 1
yea
r ol
d: B
CG
,O
PV3,
DPT
3 an
d m
easl
es
Nam
e o
f Fo
rm:
EPI F
orm
1Le
vel
Acc
om
pli
shin
g T
his
Fo
rm:
V
illag
eD
istr
ict
Pro
vin
ceN
atio
nal
Cat
ego
ries
(If
Ap
plic
able
)
Fully
imm
uniz
edN
ot f
ully
imm
uniz
ed
Inst
ruct
ion
s fo
r D
ata
Co
llect
ion
an
d/o
r R
epo
rt G
ener
atio
n
Revi
ew a
ll th
e im
mun
izat
ion
regi
ster
s/ca
rds
for
all 1
-yea
r-ol
d ch
ildre
n in
the
ser
vice
area
of
the
Vill
age
Hea
lth C
entr
e. A
ll ch
ildre
n w
ho h
ave
com
plet
ed t
heir
BCG
, OPV
,D
PT a
nd m
easl
es im
mun
izat
ions
will
be
coun
ted
as f
ully
imm
uniz
ed

20

21
(1) Assess the advantages and disadvantages of manually processing the data compared
to using computers, considering the following factors:
➤ Cost
➤ Availability of personnel with the proper background/level of technical expertise
to run a computerized system; in particular the software skills of the staff at the
lowest level where computers can be provided should be looked into
➤ Availability of technical support in case of hardware breakdown
(2) If a computerized system is to be implemented, decide the lowest level where
computers will be used to process data. Among the important considerations in
choosing this level is the presence of staff trained in system maintenance.
(3) Define the specifications for software development, in consultation with different
levels of data users. Among the important aspects to be decided are:
➤ Summary Reports to be routinely generated
➤ Data quality control mechanisms/checks to be incorporated within the software
➤ Data analysis requirements of the data users
7 Developingprocedures fordata processing
P R I N C I P L E
S T E P S
The way the HMIS data is processed should be consistent withthe objectives for data collection and the plans for data analysis
and utilization.

22
(4) Develop the software needed to process the data at each level where computers
will be used, based on the required specifications. It may also be possible that the
softwares designed to generate outputs similar to those of the HMIS have already
been developed, requiring only minor modifications to customize it. In this situation,
the resources needed to acquire and customize the software should be determined.
A decision then needs to be made on whether to develop new software or acquire
and modify an existing program.
(5) Pre-test the software, paying attention to:
➤ Identification of bugs
➤ Ability of software to generate the expected data
➤ Ability of staff to use it
(6) Develop and pre-test the User’s Manual for the software.
(7) Design a training programme to train relevant staff on the use of the software.
I S S U E S
(1) Capability of existing hardware, especially at the lower levels, to accommodate the
software, as well as its ability to store all the data.
(2) Compatibility of the developed software with other existing software (both within
and outside the Ministry of Health) that it might need to interface with in the
future.
(3) Basic system maintenance procedures.
(4) Security system.

23
WO
RK
SH
EE
T
Wo
rksh
eet
7.1:
Co
mp
ara
tive A
ssess
men
t o
f So
ftw
are
to
be U
sed
in
th
e H
MIS
Cri
teri
a f
or
Sele
ctio
nSo
ftw
are
1So
ftw
are
2So
ftw
are
3
Cos
t of
acq
uirin
g/de
velo
ping
the
sof
twar
e2
1 –
Very
exp
ensi
ve2
– M
oder
atel
y ex
pens
ive
3 –
Nil/
free
Exis
tenc
e of
sta
ff w
ithin
MO
H w
ho k
now
how
to
use
the
soft
war
e2
1 –
Non
e2
– So
me
3 –
Seve
ral
Ava
ilabi
lity
of lo
cal t
echn
ical
sup
port
in c
ase
of p
robl
ems
31
– N
one
2 –
Lim
ited
avai
labi
lity
3 –
Hig
hly
avai
labl
e
Com
patib
ility
with
the
ope
ratin
g sy
stem
s of
the
com
pute
rs u
sed
by o
ther
uni
ts w
ithin
the
2M
OH
with
who
m t
he H
MIS
nee
ds t
o in
terf
ace
1 –
Not
com
patib
le2
- C
ompa
tible
Com
patib
ility
with
oth
er s
oftw
are
used
in t
he M
OH
tha
t H
MIS
nee
ds t
o in
terf
ace
with
31
– N
ot c
ompa
tible
at
all
2 –
Soft
war
e in
terf
ace
poss
ible
aft
er a
dditi
onal
pro
cess
es3
– N
o co
mpa
tibili
ty p
robl
ems
3
Ava
ilabi
lity
of U
ser’s
Man
ual f
or t
he s
oftw
are
1 –
Not
ava
ilabl
e at
all
2 –
Ava
ilabl
e, b
ut c
anno
t be
acq
uire
d lo
cally
3 –
Ava
ilabl
e lo
cally
Leve
l of
com
pute
r sk
ills
need
ed t
o us
e th
e so
ftw
are
21
– H
igh/
adva
nced
2 –
Mod
erat
e3
– Lo
w (
very
use
r-fr
iend
ly)
Tota
l17
Sco
re

24

25
(1) Conduct a training needs assessment for data providers and data users. Four types
of training are usually conducted. These are:
➤ Training of trainers
➤ Training of data providers at the peripheral levels on how to fill out forms
➤ Training of computer operators on the use of the software and hardware
➤ Training of staff at different levels on data utilization
A separate training-needs assessment should be conducted for each type of training.
Among the variables to be collected for the training-needs assessment are as follows:
➤ Basic functions of each staff related to HMIS
➤ Extent of previous training received on the performance of such functions
➤ When training was received
➤ Adequacy of previous training to enable staff to perform expected functions
➤ Desired training areas
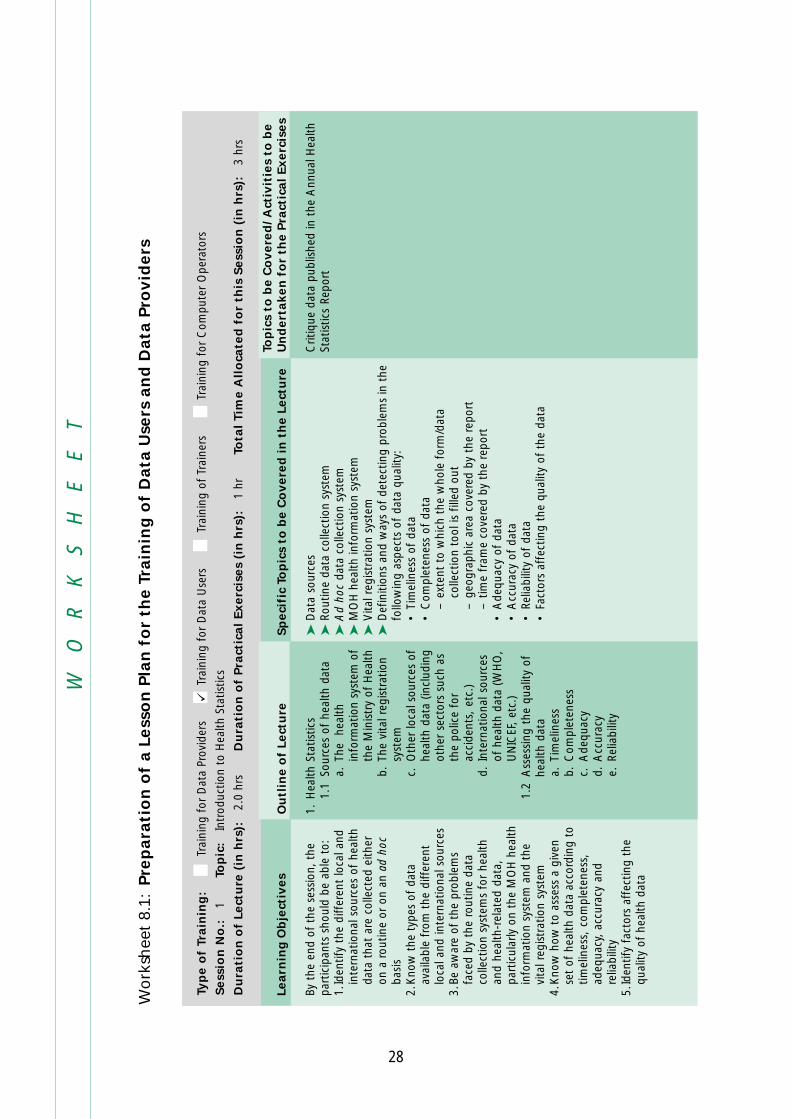
(2) Develop the curriculum for each type of training, based on the results of the training
needs assessment. The following aspects should be covered:
➤ Target group (For Whom?)
➤ Content (What?)
➤ Strategies (How?)
➤ Duration (How long?) – This refers to the total duration of the training
programme, as well as the time allocated for each topic included in the training
8 Developing thetraining programme
P R I N C I P L E
S T E P S
Training programmes should be designed according to the needsand level of the target groups.

26
The output of this step is a course syllabus for each training programme to be
conducted.
(3) Develop the training materials. The following training materials are suggested:
The participants of the Training of Trainers should be provided with a copy of the
Data Dictionary, the Manual for Data Providers and the Manual for Data Users.
(4) Reproduce the training materials. Since there is a chance that some modifications
in the format, structure and content of the training materials will be made based
on the evaluation results, the number of copies to be reproduced at this point
should be limited.
(5) Formulate the evaluation design for the training programme. It is important to
determine this prior to the conduct of the training activities, since most evaluation
designs require the collection of a baseline or a pre-training level of knowledge
among the participants.
(6) Identify the most appropriate participants for each type of training, based on their
duties and responsibilities related to data generation, management and utilization.
An efficient strategy to use is to identify and train a core set of staff who can act as
trainers for the neighbouring areas. If this strategy is adopted, it is important to
consider the geographic distribution of participants for the Training of Trainers.
(7) Conduct the training of data providers.
(8) Conduct the training of data users. This is usually conducted after sufficient data
from the HMIS has been collected for use as examples during the training.
(9) Evaluate the training programme, including the training materials used.
Type of Training
Training for DataProviders
Training for Data Users
Training for ComputerOperators
Training of Trainers
Training Material
Data Dictionary
Manual for DataProviders(separate Manual foreach level)
Manual for Data Users(separate Manual foreach level)
Computer SoftwareUser’s Manual
Trainer’s Manual
Contents
List of indicators, formulas, definitions,data sources
Instructions on how to fill out forms
Data analysis, interpretation and utilization
Detailed instructions (with examples) onhow to use the software; troubleshooting
Instructions on how to implement thetraining programme for data providers anddata users; teaching strategies; guidelineson the use of the Manual for Data Usersand Manual for Data Providers

27
(10) Modify the training materials and the training programme itself based on the results
of the evaluation. This should be done prior to the conduct of another series of
training activities.
(1) Selection of the appropriate participants for the different training programmes to
be conducted.
(2) Backgrounds of staff identified to enter data and generate reports using the software
developed for the HMIS. Are they very different?
(3) Language/dialects to be used for the training materials.
(4) Extent of dissemination of training materials and manuals.
(5) Preparation of adequate facilities to conduct training.
I S S U E S
Training seminar on data use.
28
WO
RK
SH
EE
T
Wo
rksh
eet
8.1:
Pre
para
tio
n o
f a L
ess
on
Pla
n f
or
the T
rain
ing
of
Data
Use
rs a
nd
Data
Pro
vid
ers
Learn
ing
Ob
ject
ives
By t
he e
nd o
f th
e se
ssio
n, t
hepa
rtic
ipan
ts s
houl
d be
abl
e to
:1.
Iden
tify
the
diff
eren
t lo
cal a
ndin
tern
atio
nal s
ourc
es o
f he
alth
data
tha
t ar
e co
llect
ed e
ither
on a
rou
tine
or o
n an
ad
hoc
basi
s2.
Kno
w t
he t
ypes
of
data
avai
labl
e fr
om t
he d
iffer
ent
loca
l and
inte
rnat
iona
l sou
rces
3.Be
aw
are
of t
he p
robl
ems
face
d by
the
rou
tine
data
colle
ctio
n sy
stem
s fo
r he
alth
and
heal
th-r
elat
ed d
ata,
part
icul
arly
on
the
MO
H h
ealth
info
rmat
ion
syst
em a
nd t
hevi
tal r
egis
trat
ion
syst
em4.
Kno
w h
ow t
o as
sess
a g
iven
set
of h
ealth
dat
a ac
cord
ing
totim
elin
ess,
com
plet
enes
s,ad
equa
cy,
accu
racy
and
relia
bilit
y5.
Iden
tify
fact
ors
affe
ctin
g th
equ
ality
of
heal
th d
ata
Ou
tlin
e o
f Le
ctu
re
1.H
ealth
Sta
tistic
s1.
1So
urce
s of
hea
lth d
ata
a.Th
e h
ealth
info
rmat
ion
syst
em o
fth
e M
inis
try
of H
ealth
b.Th
e vi
tal r
egis
trat
ion
syst
emc.
Oth
er lo
cal s
ourc
es o
fhe
alth
dat
a (in
clud
ing
othe
r se
ctor
s su
ch a
sth
e po
lice
for
acci
dent
s, e
tc.)
d.In
tern
atio
nal s
ourc
esof
hea
lth d
ata
(WH
O,
UN
ICEF
, et
c.)
1.2
Ass
essi
ng t
he q
ualit
y of
heal
th d
ata
a.Ti
mel
ines
sb.
Com
plet
enes
sc.
Ade
quac
yd.
Acc
urac
ye.
Relia
bilit
y
Sp
eci
fic
Top
ics
to b
e C
overe
d i
n t
he L
ect
ure
➤D
ata
sour
ces
➤Ro
utin
e da
ta c
olle
ctio
n sy
stem
➤A
d ho
c da
ta c
olle
ctio
n sy
stem
➤M
OH
hea
lth in
form
atio
n sy
stem
➤V
ital r
egis
trat
ion
syst
em➤
Def
initi
ons
and
way
s of
det
ectin
g pr
oble
ms
in t
hefo
llow
ing
aspe
cts
of d
ata
qual
ity:
•Ti
mel
ines
s of
dat
a•
Com
plet
enes
s of
dat
a–
exte
nt t
o w
hich
the
who
le f
orm
/dat
aco
llect
ion
tool
is f
illed
out
–ge
ogra
phic
are
a co
vere
d by
the
rep
ort
–tim
e fr
ame
cove
red
by t
he r
epor
t•
Ade
quac
y of
dat
a•
Acc
urac
y of
dat
a•
Relia
bilit
y of
dat
a•
Fact
ors
affe
ctin
g th
e qu
ality
of
the
data
Top
ics
to b
e C
overe
d/ A
ctiv
itie
s to
be
Un
dert
aken
fo
r th
e P
ract
ical
Exerc
ises
Crit
ique
dat
a pu
blis
hed
in t
he A
nnua
l Hea
lthSt
atis
tics
Repo
rt
Typ
e o
f Tr
ain
ing
:Tr
aini
ng f
or D
ata
Prov
ider
sTr
aini
ng f
or D
ata
Use
rsTr
aini
ng o
f Tr
aine
rsTr
aini
ng f
or C
ompu
ter
Ope
rato
rs
Sess
ion
No
.:1
Top
ic:
Intr
oduc
tion
to H
ealth
Sta
tistic
s
Du
rati
on
of
Lect
ure
(in
hrs
):2.
0 hr
sD
ura
tio
n o
f Pra
ctic
al
Exerc
ises
(in
hrs
):1
hrTo
tal
Tim
e A
llo
cate
d f
or
this
Sess
ion
(in
hrs
):3
hrs
29
(1) Prepare the guidelines for pre-testing the system. This involves addressing the
following questions:
(1.1) Where? Selection of the place(s) where the pre-testing will be conducted.
There is a need to develop criteria for selecting the pre-testing sites. These
can include technical factors like the level of expertise or qualifications of the
staff in the area, or practical considerations like the proximity of the area, the
provision/availability of infrastructure support, or how cooperative the staff
are.
(1.2) Who? Who will participate in the pre-testing? It is important for the different
types of data providers and data users to participate in the pre-testing.
(1.3) What? What are the specific objectives of the pre-testing? Specifically, what
aspects of the HMIS will be pre-tested? What are the different activities to be
undertaken to achieve these objectives?
(1.4) How? What modes and tools for data collection will be utilized to
systematically collect the data required for an efficient pre-testing of the
forms?
(1.5) How long? For how long will the pre-testing be conducted?
(2) Orient the staff involved in the pre-testing.
(2.1) Inform them on the objectives of and procedures for the pre-testing.
(2.2) Train the data users and data providers in the pre-test areas on the new
system.
The system should be pre-tested in conditions that reflect as muchas possible the actual conditions prevailing during its
implementation.
9 Pre-testingthe system
P R I N C I P L E
S T E P S

30
(3) Implement the pre-testing activities.
(4) Write a report on the results of the pre-testing.
(5) Formulate recommendations, based on the results of the pre-testing.
I S S U E S
(1) Implementation of a systematic and proactive monitoring mechanism during the
pre-testing phase.
(2) Systematic updating of the software in all units where it has been installed.
(3) Ensuring that all elements and staff are ready for the pre-testing phase.

31
WO
RK
SH
EE
T
Wo
rksh
eet
9.1:
Log
bo
ok o
f Pro
ble
ms
Iden
tifi
ed
Du
rin
g t
he P
re-t
est
ing
Ph
ase
Act
ion
Tak
en
Add
ition
al s
uppl
y of
new
form
s se
nt t
he f
ollo
win
g da
y
Prob
lem
ref
erre
d to
sof
twar
ede
velo
per
Prob
lem
ref
erre
d to
EPI
Uni
t
Res
ult
/Sta
tus
of
Pro
ble
m
Prob
lem
sol
ved
Bug
in t
he s
oftw
are
iden
tifie
d;co
rrec
tion
of s
oftw
are
inst
alle
d in
all
dist
ricts
sch
edul
ed f
or n
ext
wee
k
Age
cut
-off
ver
ified
to
be <
1;w
ritte
n cl
arifi
catio
n of
def
initi
on o
fFI
C d
istr
ibut
ed t
o al
l hea
lth c
entr
es
Oth
ers
Co
mp
ute
r1Fo
rms
Des
crip
tio
n o
f Pr
ob
lem
Ran
out
of s
uppl
y of
new
form
s
Com
pute
r do
uble
s th
een
trie
s fo
r so
me
form
s
Con
fusi
on in
def
initi
on o
fFI
C –
whe
ther
cut
-off
age
is <
1 or
<2
Oth
ers
(Sp
ecif
y)Fi
eld
Vis
itPh
on
eC
all
Dat
e
3/1/
03
3/3/
03
3/10
/03
1 Incl
udes
bot
h so
ftw
are
and
hard
war
e-re
late
d pr
oble
ms
Pro
vin
ce:
____
____
____
____
__D
istr
ict:
____
____
____
____
__V
illa
ge
He
alt
h C
en
tre
:__
____
____
____
____
Mo
nth
/Ye
ar:
____
____
____
____
__M
arch
200
3
Ho
w P
rob
lem
Was
Iden
tifi
edPr
ob
lem
Are
a

32

33
(1) Develop a plan for the systematic monitoring and evaluation of the system.
➤ What will be monitored and evaluated?
➤ How will it be done?
➤ Who will do it?
➤ How frequently will it be conducted?
➤ How will the results be systematically disseminated?
➤ How will action resulting from the evaluation results be generated?
(2) Identify the resources needed to implement the monitoring and evaluation plan.
(3) Prioritize the activities, based on availability of resources and need.
(4) Implement the monitoring and evaluation plan.
(5) Document and disseminate the results of monitoring and evaluation activities.
(6) Make recommendations based on the results of monitoring and evaluation activities.
10 Monitoringand evaluatingthe system
P R I N C I P L E
S T E P S
The goal of monitoring and evaluation is not to focus on what iswrong and condemn it; rather, it is to highlight the positive
aspects of the system that make it work, as well as to identify whatwent wrong as a basis for improving the system.

34
I S S U E S
(1) Institutionalization of monitoring and evaluation to ensure that it becomes a regular
activity and will be allocated the corresponding resources.
(2) Availability of technical expertise and other resources for monitoring and evaluation.
Checking data entry work at a health centre.

35
WO
RK
SH
EE
T
Wo
rksh
eet
10.1
:D
ata
Co
llect
ion
Act
ivit
ies
for
the E
valu
ati
on
of
the H
MIS
Are
a
Dat
age
nera
tion
and
repo
rtco
mpi
latio
n
Dat
aut
iliza
tion
Com
pute
rso
ftw
are
and
hard
war
e
Trai
ning
Mon
itorin
g
Gen
eral
Maj
or
Var
iab
les
to b
e C
ove
red
➤D
ata
qual
ity in
clud
ing
timel
ines
s, c
ompl
eten
ess,
acc
urac
y an
d re
liabi
lity
➤C
orre
ct c
ompu
ting
of in
dica
tors
➤A
ppro
pria
tene
ss o
f da
ta s
ourc
es➤
Exte
nt a
nd n
atur
e of
pro
blem
s m
et b
y vi
llage
hea
lth c
entr
e st
aff
on d
ata
entr
y an
d re
port
gen
erat
ion
➤A
dequ
acy
of f
orm
s to
mee
t th
e ne
eds
of t
he n
atio
nal,
prov
inci
al,
dist
rict
and
villa
ge le
vels
➤Ex
tent
and
nat
ure
of in
tera
ctio
n am
ong
staf
f at
diff
eren
t le
vels
on
the
HM
IS f
orm
s an
d re
port
s➤
By w
hom
and
how
dat
a ge
nera
ted
from
the
HM
IS a
re u
tiliz
ed a
t th
e na
tiona
l, pr
ovin
cial
, dis
tric
t, a
ndvi
llage
leve
ls
➤Ex
tent
and
nat
ure
of p
robl
ems
in d
ata
entr
y an
d re
port
gen
erat
ion
at t
he n
atio
nal,
prov
inci
al,
dist
rict
and
villa
ge le
vels
➤A
dequ
acy
of t
he s
oftw
are
to m
eet
the
need
s of
the
pro
vinc
es a
nd d
istr
icts
, as
wel
l as
the
natio
nal l
evel
➤Pr
oble
ms
met
with
the
sof
twar
e
➤A
sses
smen
t of
the
tra
inin
g fo
r da
ta u
sers
and
dat
a pr
ovid
ers
➤A
sses
smen
t of
the
tra
inin
g of
tra
iner
s➤
Ass
essm
ent
of t
he t
rain
ing
on t
he u
se o
f th
e so
ftw
are
➤A
sses
smen
t of
the
Use
r’s M
anua
l for
the
sof
twar
e
➤M
onito
ring
activ
ities
and
str
ateg
ies
used
at
the
natio
nal,
prov
inci
al,
and
dist
rict
leve
ls.
Of
part
icul
arim
port
ance
are
mon
itorin
g ac
tiviti
es f
or t
he f
ollo
win
g ar
eas:
•da
ta q
ualit
y•
data
ext
ract
ion
from
var
ious
sou
rces
•ut
iliza
tion
of H
MIS
pro
duct
s➤
Mon
itorin
g ac
tiviti
es a
t th
e na
tiona
l and
pro
vinc
ial l
evel
on
the
use
of t
he s
oftw
are
➤Su
pply
of
form
s, c
ompu
ter
supp
lies,
and
oth
er m
ater
ials
nee
ded
for
the
vario
us c
ompo
nent
s of
the
HM
IS➤
Form
s an
d so
urce
s of
add
ition
al s
uppo
rt n
eede
d at
the
nat
iona
l, pr
ovin
cial
, di
stric
t, a
nd v
illag
e le
vels
Mo
de
of
Dat
a C
olle
ctio
n
Key
info
rman
t in
terv
iew
sFo
cus
grou
p di
scus
sion
s
Key
info
rman
t in
terv
iew
sFo
cus
grou
p di
scus
sion
s
Revi
ew o
f lo
gboo
k of
com
pute
r pr
oble
ms
Key
info
rman
t in
terv
iew
sFo
cus
grou
p di
scus
sion
s
Key
info
rman
t in
terv
iew
sFo
cus
grou
p di
scus
sion
sRe
view
of
reco
rds
and
logb
ooks
Key
info
rman
t in
terv
iew
sFo
cus
grou
p di
scus
sion
s
Dat
a C
olle
cto
r
HM
IS e
valu
atio
nC
onsu
ltant
HM
IS e
valu
atio
nC
onsu
ltant
IT s
peci
alis
t,N
atio
nal O
ffic
e
HM
IS e
valu
atio
nC
onsu
ltant
HM
IS e
valu
atio
nC
onsu
ltant
HM
IS e
valu
atio
nC
onsu
ltant

36

37
P R I N C I P L E
S T E P S
(1) Determine the most effective and efficient way of disseminating the data generated
from the HMIS by considering the following factors:
(1.1) To whom should the data be disseminated? The needs of target groups
have to be considered.
(1.2) What should be disseminated? This should include not only the outputs of
the HMIS, but also feedback on who is using the information and what/how
they are using it.
(1.3) How often should data be disseminated to the different target groups?
(1.4) In what form should the data be disseminated to each of the different target
groups? The whole range of forms and venues for data dissemination should
be considered.
(2) Identify the human, financial and other resources needed to implement the data
dissemination plan.
(3) Prioritize the different modes of data dissemination to be adopted, based on need
and availability of resources.
(4) Implement the data dissemination activities.
11 Developingdata disseminationand feedbackmechanisms
An effective way of motivating data producers is to constantlyprovide them with both positive and negative feedback on the
status of the data they produce.

38
(5) Develop and implement a system for monitoring and evaluating the data disse-
mination and feedback activities conducted. Among the factors to be considered
are:
➤ Coverage — to what extent is the material reaching the target audience?
➤ Effect of the feedback system on the staff
➤ Degree of utilization by the target audience — are they actually using the data
presented in the different materials prepared?
I S S U E S
(1) Preparation of a Management Report.
(2) Limited financial resources for dissemination.
(3) Ensuring that dissemination activities reach the ‘correct’ audience.
(4) Consistency between the data disseminated by the HMIS, and similar data published
and disseminated by other units within the ministry, especially those of the vertical
programmes.

39
WO
RK
SH
EE
T
Wo
rksh
eet
11.1
:Su
mm
ary
of
Data
Dis
sem
inati
on
an
d F
eed
back
Act
ivit
ies
Typ
e o
f R
ep
ort
/Act
ivit
y
Ann
ual H
ealth
Sta
tistic
s Re
port
Wee
kly
Mor
bidi
ty R
epor
tfo
r N
otifi
able
Dis
ease
s
Dis
tric
t M
onth
ly H
MIS
Mon
itorin
g M
eetin
gs
To W
ho
m I
t N
eed
s to
be D
isse
min
ate
d
➤G
over
nmen
t St
atis
tics
Off
ice
➤Se
cret
ary
of H
ealth
➤N
atio
nal H
ealth
Pla
nner
➤A
ll Pr
ogra
mm
e M
anag
ers
at t
he n
atio
nal l
evel
➤A
ll Pr
ovin
cial
Hea
lth O
ffic
es
➤D
istr
ict
Hea
lth O
ffic
es➤
Prov
inci
al H
ealth
Off
ices
➤Pr
ogra
mm
e D
irect
ors
➤N
atio
nal D
isea
se C
ontr
ol U
nit
➤Pr
ogra
mm
e M
anag
ers
at t
he d
istr
ict
leve
l➤
Vill
age
Hea
lth C
entr
e st
aff
Mo
de o
f D
isse
min
ati
on
Publ
icat
ion
➤Ra
dio
➤Te
leph
one
➤Fa
x➤
Emai
l
Mee
ting
Freq
uen
cy o
f D
isse
min
ati
on
/Co
nd
uct
Ann
ual
Wee
kly
Mon
thly

40

41
(1) Review the results of monitoring and evaluation activities conducted on the HMIS
in recent years.
(2) Identify aspects of the HMIS that need to be developed further to facilitate the
functioning of the core system. The basic question to be answered is, “Where do
we go next?”. Among the possible aspects that need looking into:
➤ Enhancement and institutionalization of procedures to assure data quality control
➤ Developing capacity to conduct special studies and sample surveys
➤ Defining coordinating mechanisms for the horizontal use of data generated
from vertical programmes
➤ Developing strategies to create and/or sustain the interest of staff at different
levels to use the data for programme planning, management and evaluation
➤ Establishing inter- and intra-sectoral linkages among units involved in different
aspects of the HMIS
➤ Unifying and coordinating initiatives of sectors and funding agencies involved
in activities related to the HMIS
(3) Identify resources needed to implement the different options for the enhancement
of the HMIS. This should include specific types of resources for each planned
expansion activity; the budgetary requirements (if any); and the desired source of
support for each type of resource needed.
The development of the HMIS is always a work in progress. It is adynamic endeavour where managers and workers strive for
constant improvement.
12 Enhancing the HMIS
P R I N C I P L E
S T E P S

42
(4) Prioritize the different options according to degree and urgency of need, and
availability of resources for its proper implementation.
(5) Prepare a timetable for the implementation of the different activities for the
expansion of the HMIS.
(6) Conduct the different activities needed to implement the desired enhancement of
the HMIS.
(7) Monitor and evaluate the effect of newly implemented aspect of the HMIS.
I S S U E S
(1) Sustaining interest among different stakeholders for the continuous development
of the HMIS.
(2) Generation of resources to support the different activities for system enhancement.
(3) Coordinating the activities of the different donor agencies so as to minimize the
proliferation of data collection forms and the duplication of efforts in areas related
to HMIS development.
(4) Ensuring the continued existence of a body/committee to oversee the HMIS after
the pilot-testing phase.
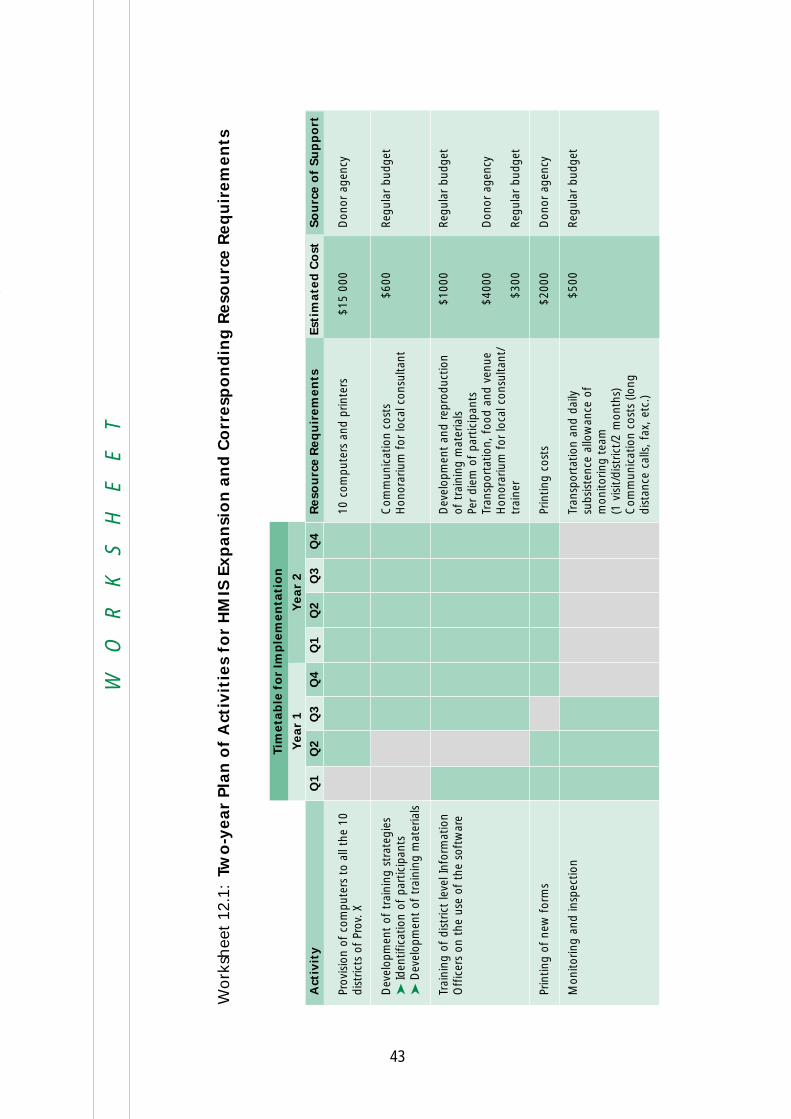
43
WO
RK
SH
EE
T
Wo
rksh
eet
12.1
:Tw
o-y
ear
Pla
n o
f A
ctiv
itie
s fo
r H
MIS
Exp
an
sio
n a
nd
Co
rresp
on
din
g R
eso
urc
e R
eq
uir
em
en
ts
Act
ivit
y
Prov
isio
n of
com
pute
rs t
o al
l the
10
dist
ricts
of
Prov
. X
Dev
elop
men
t of
tra
inin
g st
rate
gies
➤Id
entif
icat
ion
of p
artic
ipan
ts➤
Dev
elop
men
t of
tra
inin
g m
ater
ials
Trai
ning
of
dist
rict
leve
l Inf
orm
atio
nO
ffic
ers
on t
he u
se o
f th
e so
ftw
are
Prin
ting
of n
ew f
orm
s
Mon
itorin
g an
d in
spec
tion
Reso
urc
e R
eq
uir
em
en
ts
10 c
ompu
ters
and
prin
ters
Com
mun
icat
ion
cost
sH
onor
ariu
m f
or lo
cal c
onsu
ltant
Dev
elop
men
t an
d re
prod
uctio
nof
tra
inin
g m
ater
ials
Per
diem
of
part
icip
ants
Tran
spor
tatio
n, f
ood
and
venu
eH
onor
ariu
m f
or lo
cal c
onsu
ltant
/tr
aine
r
Prin
ting
cost
s
Tran
spor
tatio
n an
d da
ilysu
bsis
tenc
e al
low
ance
of
mon
itorin
g te
am(1
vis
it/di
stric
t/2
mon
ths)
Com
mun
icat
ion
cost
s (lo
ngdi
stan
ce c
alls
, fa
x, e
tc.)
Est
imate
d C
ost
$15
000
$600
$100
0
$400
0
$300
$200
0
$500
So
urc
e o
f Su
pp
ort
Don
or a
genc
y
Regu
lar
budg
et
Regu
lar
budg
et
Don
or a
genc
y
Regu
lar
budg
et
Don
or a
genc
y
Regu
lar
budg
et
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
Year
1Y
ear
2
Tim
eta
ble
fo
r Im
ple
men
tati
on

44
45
Examples
Example 1 is a list of basic indicators that might be used in Ministry of Health programmes,
together with the corresponding data sources, modes and frequency of data collection,
as well as the lowest administrative level where the indicator is computed. While the
reader can adopt some of these indicators for their use, the main objective of the
example is to show how the set of indicators used by a country can be presented so
that it will be easy for the staff of the Statistics Unit to monitor their status.
Example 2 is a flow chart of the HMIS of hypothetical country X. As in the first example,
the aim is to show not “what”, but “how”; not to prescribe a model flowchart for the
HMIS as such, but rather to demonstrate how the HMIS can be presented by means of
a flow chart.

46
Exam
ple
1:
List
of
Ind
icato
rs U
sed
by t
he M
inis
try o
f H
ealt
h o
f C
ou
ntr
y X
Wit
h C
orr
esp
on
din
g D
ata
So
urc
es
an
d M
od
e o
f D
ata
Co
llect
ion
Col
ly, is
it p
ossi
ble
to p
rovi
de a
shor
t exp
lana
tion
of w
hat t
he fo
llow
ing
exam
ples
are
all
abou
t? E
ven
one
sent
ence
will
do,
so
as n
ot to
leav
eth
is p
age
blan
k (t
o re
plac
e th
is p
arag
raph
). A
noth
er o
ptio
n w
ould
be a
quo
tatio
n.
Ind
icato
rFo
rm/R
eg
iste
rFr
eq
uen
cy o
fD
ata
Co
llect
ion
Sp
eci
al
Surv
eyR
ou
tin
eSyst
em
Oth
er
Ag
en
cies
(Ple
ase
Sp
eci
fy)
Un
it/D
ivis
ion
Low
est
Level W
here
Ind
icato
r is
Co
mp
ute
dA
.Po
pu
lati
on
, So
cio
-eco
no
mic
an
d E
nvir
on
men
tal In
dic
ato
rs
1.Po
pula
tion
grow
th r
ate
NSO
Ann
ually
Vill
age
2.N
atur
al p
opul
atio
n gr
owth
rat
eN
SOA
nnua
llyV
illag
e
3.C
rude
birt
h ra
teN
SOA
nnua
llyV
illag
e
4.C
rude
dea
th r
ate
NSO
Ann
ually
Vill
age
5.To
tal f
ertil
ity r
ate
NSO
Ann
ually
Vill
age
6.Pe
rcen
tage
of
the
popu
latio
n by
age
and
sex
NSO
Ever
y 5
yrs
Dis
tric
t
7.G
ross
dom
estic
pro
duct
per
cap
itaN
SOA
nnua
llyN
atio
nal
8.Li
tera
cy r
ate
a.O
vera
llb.
Mal
esc.
Fem
ales
NSO
; MO
EEv
ery
5 yr
sPr
ovin
ce
9.Pe
rcen
tage
of
the
popu
latio
n us
ing
safe
wat
era.
Ove
rall
b.U
rban
c.Ru
ral
EHN
SOEv
ery
5 yr
sPr
ovin
ce
10.P
erce
ntag
e of
the
pop
ulat
ion
usin
ghy
gien
ic t
oile
ta.
Ove
rall
b.U
rban
c.Ru
ral
EHN
SOEv
ery
5 yr
sPr
ovin
ce
B.
Res
ou
rce
Ind
icat
ors
11.P
erce
ntag
e of
gov
ernm
ent
heal
thbu
dget
in G
DP
PHO
DO
FM
OH
DO
FN
SOA
nnua
llyN
atio
nal
MO
HSo
urc
eM
od
e o
fD
ata
Co
llect
ion
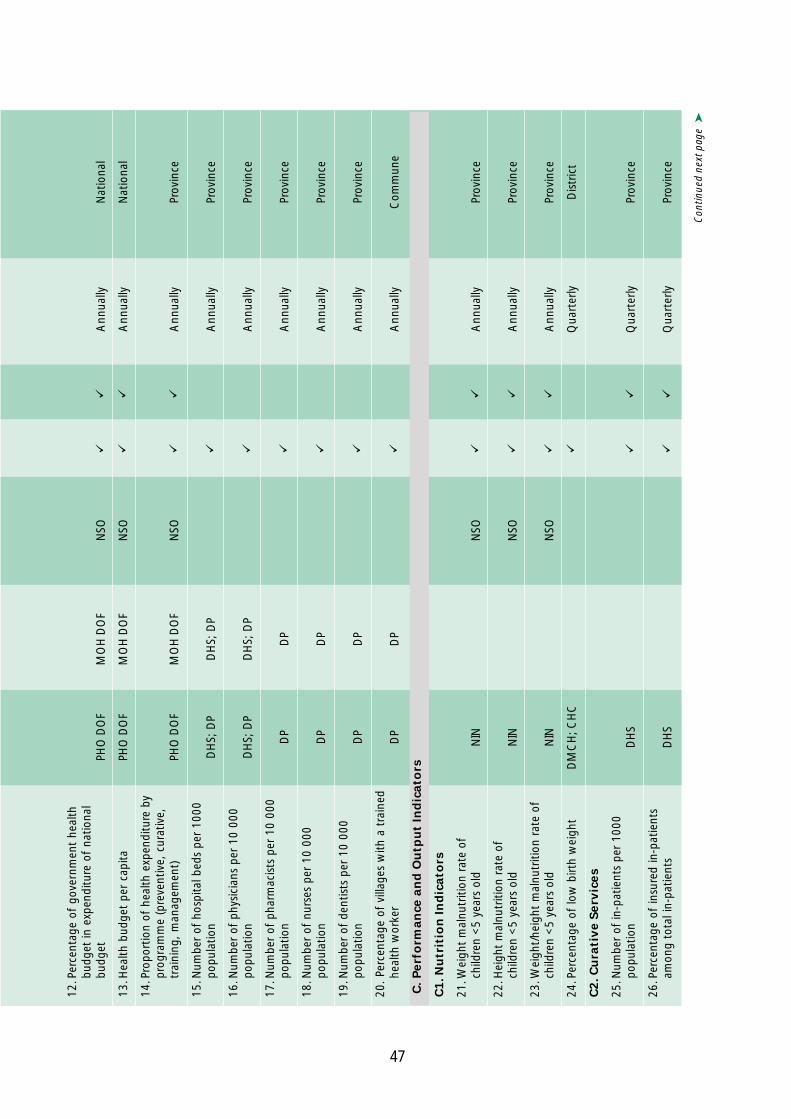
47
Con
tinue
d ne
xt p
age
➤
12.P
erce
ntag
e of
gov
ernm
ent
heal
thbu
dget
in e
xpen
ditu
re o
f na
tiona
lbu
dget
PHO
DO
FM
OH
DO
FN
SOA
nnua
llyN
atio
nal
13.H
ealth
bud
get
per
capi
taPH
O D
OF
MO
H D
OF
NSO
Ann
ually
Nat
iona
l
14.P
ropo
rtio
n of
hea
lth e
xpen
ditu
re b
ypr
ogra
mm
e (p
reve
ntiv
e, c
urat
ive,
trai
ning
, m
anag
emen
t)PH
O D
OF
MO
H D
OF
NSO
Ann
ually
Prov
ince
15.N
umbe
r of
hos
pita
l bed
s pe
r 10
00po
pula
tion
DH
S; D
PD
HS;
DP
Ann
ually
Prov
ince
16.N
umbe
r of
phy
sici
ans
per
10 0
00po
pula
tion
DH
S; D
PD
HS;
DP
Ann
ually
Prov
ince
17.N
umbe
r of
pha
rmac
ists
per
10
000
popu
latio
nD
PD
PA
nnua
llyPr
ovin
ce
18.N
umbe
r of
nur
ses
per
10 0
00po
pula
tion
DP
DP
Ann
ually
Prov
ince
19.N
umbe
r of
den
tists
per
10
000
popu
latio
nD
PD
PA
nnua
llyPr
ovin
ce
20.
Perc
enta
ge o
f vi
llage
s w
ith a
tra
ined
heal
th w
orke
rD
PD
PA
nnua
llyC
omm
une
C.
Perf
orm
an
ce a
nd
Ou
tpu
t In
dic
ato
rs
C1.N
utr
itio
n I
nd
icato
rs
21.W
eigh
t m
alnu
triti
on r
ate
ofch
ildre
n <
5 ye
ars
old
NIN
NSO
Ann
ually
Prov
ince
22.H
eigh
t m
alnu
triti
on r
ate
ofch
ildre
n <
5 ye
ars
old
NIN
NSO
Ann
ually
Prov
ince
23.W
eigh
t/he
ight
mal
nutr
ition
rat
e of
child
ren
<5
year
s ol
dN
INN
SOA
nnua
llyPr
ovin
ce
24.P
erce
ntag
e of
low
birt
h w
eigh
tD
MC
H; C
HC
Qua
rter
lyD
istr
ict
C2
.Cu
rati
ve S
erv
ices
25.N
umbe
r of
in-p
atie
nts
per
1000
popu
latio
nD
HS
Qua
rter
lyPr
ovin
ce
26.P
erce
ntag
e of
insu
red
in-p
atie
nts
amon
g to
tal i
n-pa
tient
sD
HS
Qua
rter
lyPr
ovin
ce

48
Exam
ple
1 (
Co
nt’
d)
Ind
icato
rFo
rm/R
eg
iste
rFr
eq
uen
cy o
fD
ata
Co
llect
ion
Sp
eci
al
Surv
eyR
ou
tin
eSyst
em
Oth
er
Ag
en
cies
(Ple
ase
Sp
eci
fy)
Un
it/D
ivis
ion
Low
est
Level W
here
Ind
icato
r is
Co
mp
ute
d
C2.C
ura
tive S
erv
ices
(Co
nt’
d)
27.N
umbe
r of
out
-pat
ient
s pe
r 10
00po
pula
tion
DH
SQ
uart
erly
Prov
ince
28.A
vera
ge le
ngth
of
stay
in t
heho
spita
lD
HS
Qua
rter
lyD
istr
ict
29.B
ed o
ccup
ancy
rat
eD
HS
Qua
rter
lyD
istr
ict
30.B
ed t
urn-
over
rat
eD
HS
Qua
rter
lyD
istr
ict
C3.R
ep
rod
uct
ive H
ealt
h a
nd
Fam
ily P
lan
nin
g
31.P
erce
ntag
e of
pre
gnan
t w
omen
vacc
inat
ed w
ith T
etan
us T
oxoi
d ≥2
EPI;
CH
C; D
MC
HQ
uart
erly
Dis
tric
t
32.P
erce
ntag
e of
wom
en w
ith ≥
3an
tena
tal v
isits
dur
ing
preg
nanc
yC
HC
; D
MC
HQ
uart
erly
Com
mun
e
33.P
erce
ntag
e of
del
iver
ies
in h
ealth
faci
litie
sC
HC
; DM
CH
Qua
rter
lyC
omm
une
34.P
erce
ntag
e of
del
iver
ies
atte
nded
by a
hea
lth w
orke
rC
HC
; D
MC
HQ
uart
erly
Com
mun
e
35.P
erce
ntag
e of
mot
hers
who
rece
ived
pos
tnat
al c
are
CH
C;
DM
CH
Qua
rter
lyC
omm
une
36.P
erce
ntag
e of
pre
gnan
t w
omen
amon
g <
19 y
ears
old
CH
C; D
MC
HN
SOEv
ery
2 yr
sD
istr
ict
37.C
ontr
acep
tive
prev
alen
ce
rate
FPSF
NSO
Qua
rter
lyD
istr
ict
38.M
etho
d-sp
ecifi
c co
ntra
cept
ive
rate
(IUD
, Pi
ll, e
tc.)
FPSF
NSO
Qua
rter
lyD
istr
ict
39.S
pont
aneo
us a
bort
ion
ratio
HQ
uart
erly
Dis
tric
t
40.M
orbi
dity
and
mor
talit
y ra
tio o
fob
stet
ric c
ompl
icat
ions
HQ
uart
erly
Prov
ince
MO
HSo
urc
eM
od
e o
fD
ata
Co
llect
ion
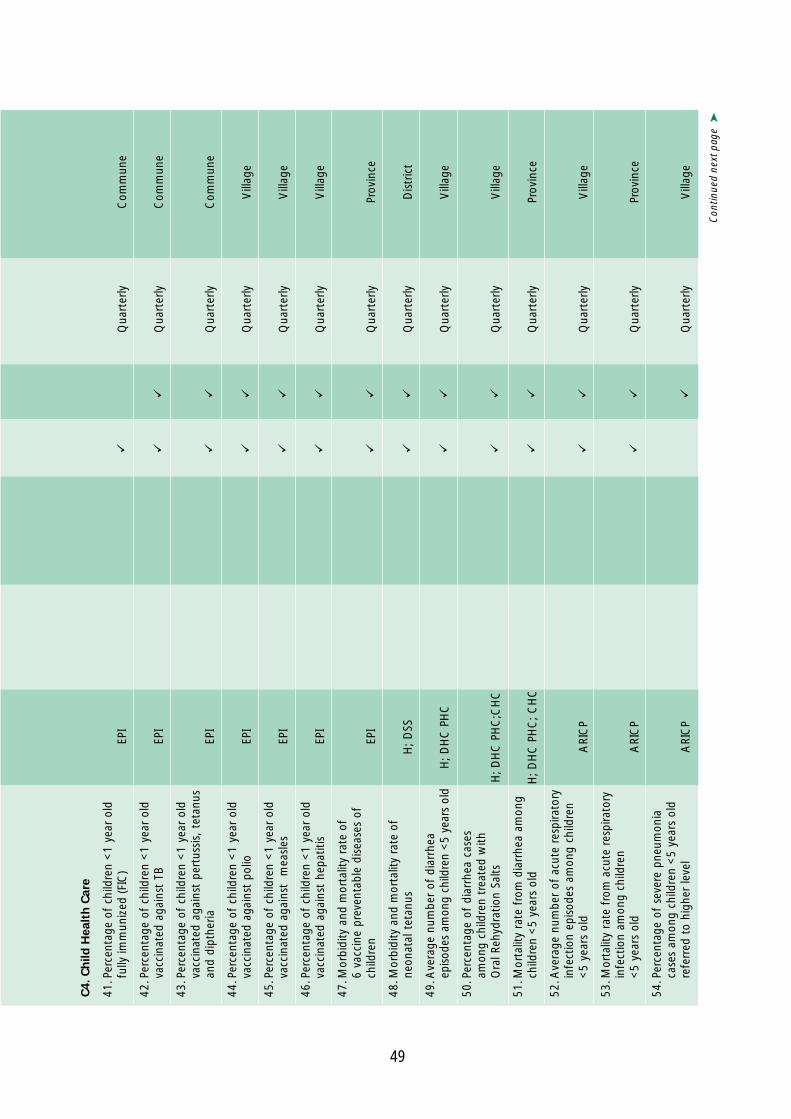
49
Con
tinue
d ne
xt p
age
➤
C4.
Ch
ild H
ealt
h C
are
41.P
erce
ntag
e of
chi
ldre
n <
1 ye
ar o
ldfu
lly im
mun
ized
(FIC
)EP
IQ
uart
erly
Com
mun
e
42.P
erce
ntag
e of
chi
ldre
n <
1 ye
ar o
ldva
ccin
ated
aga
inst
TB
EPI
Qua
rter
lyC
omm
une
43.P
erce
ntag
e of
chi
ldre
n <
1 ye
ar o
ldva
ccin
ated
aga
inst
per
tuss
is,
teta
nus
and
dipt
heria
EPI
Qua
rter
lyC
omm
une
44.P
erce
ntag
e of
chi
ldre
n <
1 ye
ar o
ldva
ccin
ated
aga
inst
pol
ioEP
IQ
uart
erly
Vill
age
45.P
erce
ntag
e of
chi
ldre
n <
1 ye
ar o
ldva
ccin
ated
aga
inst
m
easl
esEP
IQ
uart
erly
Vill
age
46.P
erce
ntag
e of
chi
ldre
n <
1 ye
ar o
ldva
ccin
ated
aga
inst
hep
atiti
sEP
IQ
uart
erly
Vill
age
47.M
orbi
dity
and
mor
talit
y ra
te o
f6
vacc
ine
prev
enta
ble
dise
ases
of
child
ren
EPI
Qua
rter
lyPr
ovin
ce
48.M
orbi
dity
and
mor
talit
y ra
te o
fne
onat
al t
etan
usH
; D
SSQ
uart
erly
Dis
tric
t
49.A
vera
ge n
umbe
r of
dia
rrhe
aep
isod
es a
mon
g ch
ildre
n <
5 ye
ars
old
H; D
HC
PH
CQ
uart
erly
Vill
age
50.P
erce
ntag
e of
dia
rrhe
a ca
ses
amon
g ch
ildre
n tr
eate
d w
ithO
ral R
ehyd
ratio
n Sa
ltsH
; DH
C P
HC
;CH
CQ
uart
erly
Vill
age
51.M
orta
lity
rate
fro
m d
iarr
hea
amon
gch
ildre
n <
5 ye
ars
old
H; D
HC
PH
C; C
HC
Qua
rter
lyPr
ovin
ce
52.A
vera
ge n
umbe
r of
acu
te r
espi
rato
ryin
fect
ion
epis
odes
am
ong
child
ren
<5
year
s ol
dA
RIC
PQ
uart
erly
Vill
age
53.M
orta
lity
rate
fro
m a
cute
res
pira
tory
infe
ctio
n am
ong
child
ren
<5
year
s ol
dA
RIC
PQ
uart
erly
Prov
ince
54.P
erce
ntag
e of
sev
ere
pneu
mon
iaca
ses
amon
g ch
ildre
n <
5 ye
ars
old
refe
rred
to
high
er le
vel
ARI
CP
Qua
rter
lyV
illag
e

50
Exam
ple
1 (
Co
nt’
d)
Ind
icato
rFo
rm/R
eg
iste
rFr
eq
uen
cy o
fD
ata
Co
llect
ion
Sp
eci
al
Surv
eyR
ou
tin
eSyst
em
Oth
er
Ag
en
cies
(Ple
ase
Sp
eci
fy)
Un
it/D
ivis
ion
Low
est
Level W
here
Ind
icato
r is
Co
mp
ute
d
C5.S
ele
cted
Dis
ease
s
55.P
reva
lenc
e of
lepr
osy
DH
C P
MC
Qua
rter
lyPr
ovin
ce
56.P
erce
ntag
e of
new
lepr
osy
case
sw
ith d
isab
ility
deg
ree
2 an
d ov
erD
HC
PM
CQ
uart
erly
Prov
ince
57.M
orbi
dity
and
mor
talit
y ra
te o
ftu
berc
ulos
isN
TCP
Qua
rter
lyPr
ovin
ce
58.N
otifi
catio
n ra
te (
inci
denc
e) o
ftu
berc
ulos
isN
TCP
Qua
rter
lyPr
ovin
ce
59.P
erce
ntag
e of
tub
ercu
losi
s pa
tient
str
eate
d w
ith D
OTS
NTC
PQ
uart
erly
Prov
ince
60.C
ase
fata
lity
rate
for
tub
ercu
losi
s(a
mon
g tr
eate
d ca
ses)
NTC
PQ
uart
erly
Prov
ince
61.M
orbi
dity
and
mor
talit
y ra
te f
orm
alar
iaN
MC
P;C
DSS
Qua
rter
lyD
istr
ict
62.P
erce
ntag
e of
blo
od s
mea
rs p
ositi
vew
ith p
aras
iteN
MC
PQ
uart
erly
Dis
tric
t
63.N
umbe
r of
mal
aria
out
brea
ksN
MC
P;C
DSS
Qua
rter
lyD
istr
ict
64.P
erce
ntag
e of
hou
seho
lds
usin
gio
dize
d sa
ltN
INEv
ery
5 yr
sPr
ovin
ce
65.P
reva
lenc
e of
goi
ter
amon
gsc
hool
-age
chi
ldre
nN
INEv
ery
5 yr
sPr
ovin
ce
66.N
umbe
r of
new
HIV
-AID
S ca
ses
HA
CP
Mon
thly
Prov
ince
67.C
umul
ativ
e nu
mbe
r of
HIV
-AID
Sca
ses
HA
CP
Mon
thly
Prov
ince
68.N
umbe
r of
dea
ths
due
to A
IDS
HA
CP
Mon
thly
Prov
ince
69.N
umbe
r of
foo
d po
ison
ing
outb
reak
sA
nnua
llyC
omm
une
MO
HSo
urc
eM
od
e o
fD
ata
Co
llect
ion

51
D.I
mp
act
In
dic
ato
rsA
nnua
lly
70.M
orbi
dity
and
mor
talit
y ra
te f
orse
lect
ed c
omm
unic
able
dis
ease
sC
DSS
Ann
ually
Vill
age
71.T
en le
adin
g ca
uses
of
mor
bidi
tyan
d m
orta
lity
in h
ospi
tals
HA
nnua
llyD
istr
ict
72.P
erce
ntag
e of
hos
pita
l adm
issi
ons
acco
rdin
g to
diff
eren
t gr
oups
of
dise
ases
(ba
sed
on IC
D-1
0ca
tego
ries)
HA
nnua
llyD
istr
ict
73.U
nder
-fiv
e m
orta
lity
rate
MO
HN
SOA
nnua
llyPr
ovin
ce
74.I
nfan
t m
orta
lity
rate
MO
HN
SOA
nnua
llyPr
ovin
ce
75.P
erin
atal
mor
talit
y ra
teM
OH
NSO
Ann
ually
Prov
ince
76.M
ater
nal m
orta
lity
ratio
MO
HA
nnua
llyPr
ovin
ce
77.L
ife e
xpec
tanc
y at
birt
ha.
Mal
esb.
Fem
ales
NSO
Ever
y 5
yrs
Prov
ince
78.H
uman
dev
elop
men
t in
dex
NSO
Ever
y 5
yrs
Nat
iona
l

52
Exam
ple
2: D
ata
Flo
w f
or
the H
MIS
of
Co
un
try X
��
�� !����"��������������
�������������� ������
!����"��������������
������������ ������
���������"�����
���������
���������������
�������������� ������
������������!���
������������ ������
������������!���
����������
������������!���
����������" �����
��� ������
��������������
��
�
�
�
� �
��� ��������#���$
��#�
������������������$
�����%����#�������$
�� ��������
&����� ��� ���#�������$
#������ ���#���$������#��'
��#���������'�#���$�#���
���������������������'�
� �
(����
)#���*
���
��
�

53
References
Hurtubise, R. Managing information systems: concepts and tools. West Hartford, CT,
Kumarian Press, 1984.
Lippeveld, T., et al, eds. Design and implementation of health information systems.
Geneva. World Health Organization, 2000.
World Health Organization Regional Office for the Western Pacific. Workshops on the
assessment and development of national Health Information Systems (HMIS) and
epidemiological surveillance. Manila, Philippines. World Health Organization, 1986
(Unpublished document, (WP)HIN/ICP/HST/005-E).
World Health Organization Regional Office for the Western Pacific. A selection of
important health indicators. Manila, Philippines. World Health Organization, 2000.
World Health Organization Regional Office for the Western Pacific. Guidelines for the
development of Health Management Information Systems. Manila, Philippines.
World Health Organization, 1993.

54