diabetes mellitus pediatric critical care medicine emory university children’s healthcare of...
TRANSCRIPT
Diabetes Mellitus
Pediatric Critical Care MedicineEmory University
Children’s Healthcare of Atlanta
2
Goals & Objectives• Understand the action of insulin on the
metabolism of carbohydrates, protein & fat• Understand the pathophysiology of IDDM & DKA• Understand the management approach to the
patient with DKA• Appreciate the complications that occur during
treatment
3
Classification• Type I (insulin-dependent diabetes mellitus, IDDM)
– Severe lacking of insulin, dependent on exogenous insulin– DKA– Onset in childhood– ?genetic disposition & is likely auto-immune-mediated
• Type II (non-insulin-dependent diabetes mellitus, NIDDM)– Not insulin dependent, no ketosis– Older patient (>40), high incidence of obesity– Insulin resistant– No genetic disposition– Increase incidence due to prevalence of childhood obesity
4
IDDM: Epidemiology• 1.9/1000 among school-age children in the US;
12-15 new cases/100,00• Equal male to female • African-Americans: occurrence is 20-30%
compared to Caucasian-Americans• Peaks age 5-7 yrs and adolescence• Newly recognized cases: more in autumn &
winter• Increase incidence in children with congenital
rubella syndrome

5
Type I DM• 15-70% of children with Type I DM present in DKA
at disease onset• 1/350 of type I DM will experience DKA by age 18
yo• Risk of DKA increased by:
– Very young children– Lower socioeconomic background– No family history of Type I DM
• DKA:– Most frequent cause of death in Type I DM– One of the most common reasons for admission to PICU
6
IDDM: Etiology & Pathophysiology
• Diminished insulin secretion by destruction of pancreatic islets cells via autoimmune process
• 80-90% of newly diagnosed cases have anti-islet cell antibodies
• More prevalent in persons with Addison’s disease, Hashimoto’s thyroiditis, pernicious anemia

7
Type I DM: Pathophysiology• Progressive destruction of -cells progressive
deficiency of insulin permanent low-insulin catabolic state
• Phases:– Early: defect in peripheral glucose predominates– Late: insulin deficiency becomes more severe
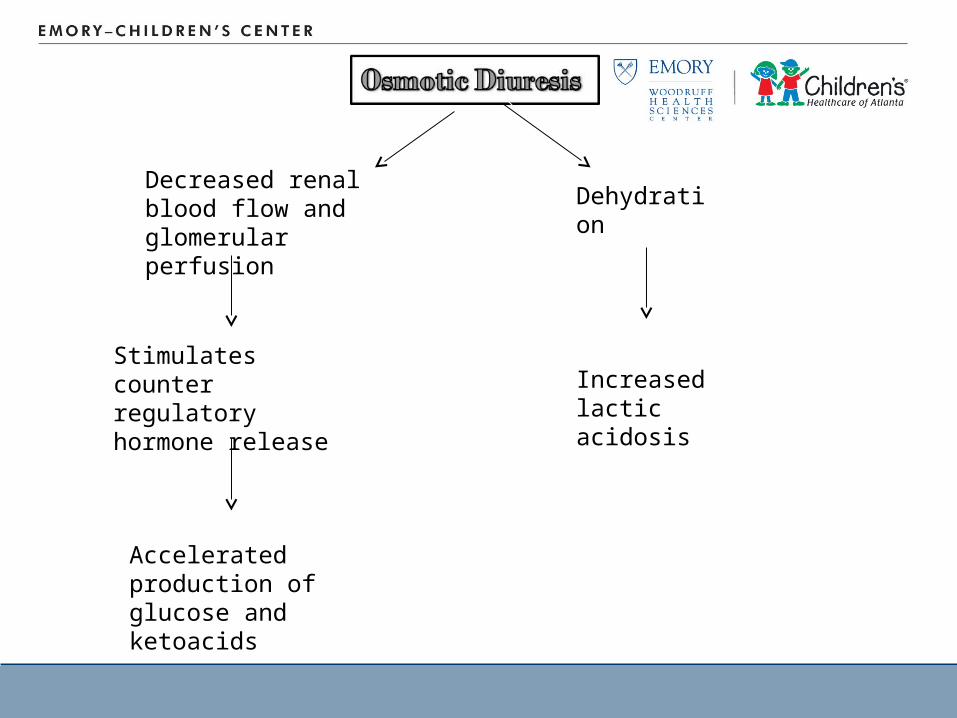
Decreased renal blood flow and glomerular perfusion
Stimulates counter regulatory hormone release
Dehydration
Increased lactic acidosis
Accelerated production of glucose and ketoacids
10
Type I DM: Pathophysiology• Hyperglycemia glucosuria (renal threshold 180
g/dL) osmotic diruresis: polyuria, urinary losses of electrolytes, dehydration, & compensatory polydipsia
• Hyperglycemia hyperosmolality: cerebral obtundation– {Serum Na+ + K+} x 2 + glucose/18 + BUN/3
• Counter-regulatory hormones (glucagon, catecholamines, cortisol) are released– Increased hepatic glucose production impairing
peripheral uptake of glucose
11
Type I DM: DKA• Lipid metabolism: increase lipolysis
– Increased concentration of total lipids, cholesterone, TG, free FA
– Free FA shunted into ketone body formation; rate of production>peripheral utilization & renal excretion ketoacids
– Ketoacidosis -hydroxybutyrate & acetoacetate metabolic acidosis
– Acetone (not contribute to the acidosis)
12
Type I DM: DKA• Electrolytes loss
– Potassium: 3-5 mEq/kg– Phosphate: 0.5-1.5 mmol/kg
» 2,3-diphosphoglycerate: facilitates O2 release from HgB
» Deficient in DKA, may contribute to formation of lactic acidosis
– Sodium: 5-10 mEq/kg
DKA: Presenting Features• Polyuria• Polydipsia• Polyphagia• Nocturia• Enuresis
• Abdominal pain• Vomiting• Profound weight loss• Altered mental status• weakness
13
14
Type I DM: Clinical Manifestations• Ketoacidosis is responsible for the initial
presentation in up to 25% of children– Early manifestations: vomiting, polyuria, dehydration– More severe: Kussmaul respirations, acetone odor on the
breath– Abdominal pain or rigidity may be present & mimic
acute abdomen– Cerebral obtundation & coma ultimately ensue
• DKA exists when there is hyperglycemia (>300 mg/dL & usually <1,000 mg/dL); ketonemia, acidosis, glucosuria & ketonuria
15
DKA: Physical Exam• Tachycardia• Dry mucous membrane• Delayed capillary refill• Poor skin turgor• Hypotension• Kussmaul breathing

16
DKA: Physical Exam• Dehydration
– Hyperosmolar: translocation of intracellular water to extracellualr comparment
– A rough estimation of how dehydrated the patient is to facilitate proper rehydration
– Studies have shown that clinical approximations often are poor
17
DKA: Laboratory• Blood glucose• Urinary/plasma ketones• Serum electrolytes• BUN/Cr• Osmolarity• CBC, blood cx (if infection is suspected)• Blood gas

18
DKA: Laboratory Findings• Elevated blood glucose (usually <1,000)• Low bicarbonate level• Anion gap metabolic acidosis
– Unmeasured ketoacids– Urine dipsticks measure acetoacetate: in DKA B-
hydroxybutyrate to acetoacetate is 10:1– Helpful in determining if there is ketoacids in urine but
not sererity of DKA or response to treatment
19
DKA: Laboratory Findings• Sodium: low
– Osmotic flux of water into extracellular space reduces serum sodium concentration
– Actual sodium: 1.6mEq/L per 100mg/dL rise in glucose over 100
– Hypertriglyceridemia low sodium pseudohyponatremia
• Potassium: – Level varies depending on urinary loss and severity of
acidosis– Potassium moves extracellularly in exchange for
hydrogen ions typical hyperkalemia on presentaion– Total body stores are depleted due to urinary loss
20
DKA: Laboratory Findings• Phosphate
– Depleted in the setting of DKA– Serum level may not accurately represent total body
stores
21
DKA: Management• Goals: correction of
– Dehydration– Acidosis– Electrolytes deficits– Hyperglycemia

22
DKA: Management• Fluids:
– Avoid impending shock» Fluid replacement >4L/m2/24 hrs has been associate with
cerebral edema
– Usually necessary to help expand vascular compartment» Fluid deficit should gradually be corrected over 36-48 hrs
– Rehydration fluids should contain at least 115-135 mEq/L of NaCl
» Start with NS and switch to ½ NS if neccessary
23
DKA: Management• Postassium:
– Total body depletion will become more prominent with correction of acidosis
– Continuous EKG monitoring is standard of care– 30-40 mEq/L: in either KCl or KPhos
24
DKA: Management• Phosphate:
– Total body depletion will become more prominent with correction of acidosis
– Hypophosphatemia may cause rhabdomyolysis, hemolysis, impaired oxygen delivery
– Calcium should be monitored during replacement
25
DKA: Management• Insulin should be initiated immediately
– Insulin drips 0.1 U/kg/hr (NO BOLUS)– Gradual correction reducing serum glucose by 50-100
mg/dL/hr– Serum glucose often falls after fluid bolus: increase in
glomerular filtration with increased renal perfusion
26
DKA: Management• Dextrose should be added to IVF when serum
glucose <300– Blood glucose levels often correct prior to ketoacidosis– Should not lower insulin infusion unless: rapid correction
of serum glucose or profound hypoglycemia
27
DKA: Management• Bicarbonate is almost never administered
– Bicarb administration leads to increased cerebral acidosis:
– HCO3- + H+ dissociated to CO2 and H2O
– Bicarbonate passes the BBB slowly
– CO2 diffuses freely exacerbating cerebral acidosis & depression
• Indications for bicarbonate use: only in severe acidosis leading to cardiorespiratory compromise
28
DKA: Complication, Cerebral Edema• Cerebral edema: 0.5-1% of pediatric DKA
– Mortality rate of 20%– Responsible for 50-60% of diabetes deaths in children– Permanent neurologic disability rate of 25%
• Typically develops within the first 24 hrs of treatment
• Etiology is still unclear• Signs & symptoms:
– Headache – Confusion– Slurred speech– Bradycardia– Hypertension

29
DKA: Complication, Cerebral Edema• Theories of cerebral edema
– Rapid decline in serum osmolality» This leads to the recommendation of limiting the rate of
fluid administration
– Edema due to cerebral hypoperfusion or hypoxia– Activation of ion transporters in the brain– Direct effects of ketoacidosis and/or cytokines on
endothelial function

DKA: Cerebral Edema, risk factors
• Younger age• New onset• Longer duration of
symptoms
• Lower PCO2
• Severe acidosis
• Increase in BUN• Use of bicarbonate• Large volumes of
rehydration fluids• Failure of correction of
Na with treatment
30
31
DKA: Cerebral Edema, treatment• Lower intracranial pressure
– Mannitol or 3% saline
• Imaging to rule out other pathologies• Hyperventilation & surgical decompression are
less successful at preventing neurologic morbidity & mortality
DKA: Complications• Thrombosis (esp with
CVL)• Cardiac arrhythmias• Pulmonary edema• Renal failure• Pancreatitis
• Rhabdomyolysis• Infection
– Aspiration pneumonia– Sepsis– Mucormycosis
32
Hyperglycemia Hyperosmolar Syndrome
33
34
Pathophysiology• Insulin levels are sufficient to suppress lipolysis
and ketogenesis• Insulin levels are inadequate to promote normal
anabolic function & inhibit gluconeogeneis & glycogenolysis
• Cell deprivation triggers counter-regulatory surge, increasing glucose via enhanced hepatic glucose generation & insulin resistance
35
Pathophysiology• Hyperglycemia heightened inflammatory state
exacerbating glucose dysregulation
• Osmotic diuresis dehydration decreased GFR further glucose elevation

36
Pathophysiology• Morbidity & mortality associated with acute
hyperglycemia– Vascular injury– Thrombus formation– Disrupts the phagocytotic & oxidative burst functions of
the immune systemt– Disrupts BBB– Disrupts metabolism of the CNS worsens the effects of
ischemia on brain tissue
37
Pathophysiology• Dehydration is a major component• 15-20% volume depleted
– 5-10% in DKA
• Greater electrolyte loss due to massive osmotic diuresis
38
Clinical Presentation• Similar to DKA
– Polyuria– Polydipsia– Weight loss– Neurologic impairment
• Different from DKA– Kussmaul breathing– Acetone breath– Abdominal discomfort, nausea & vomiting are less
severe
39
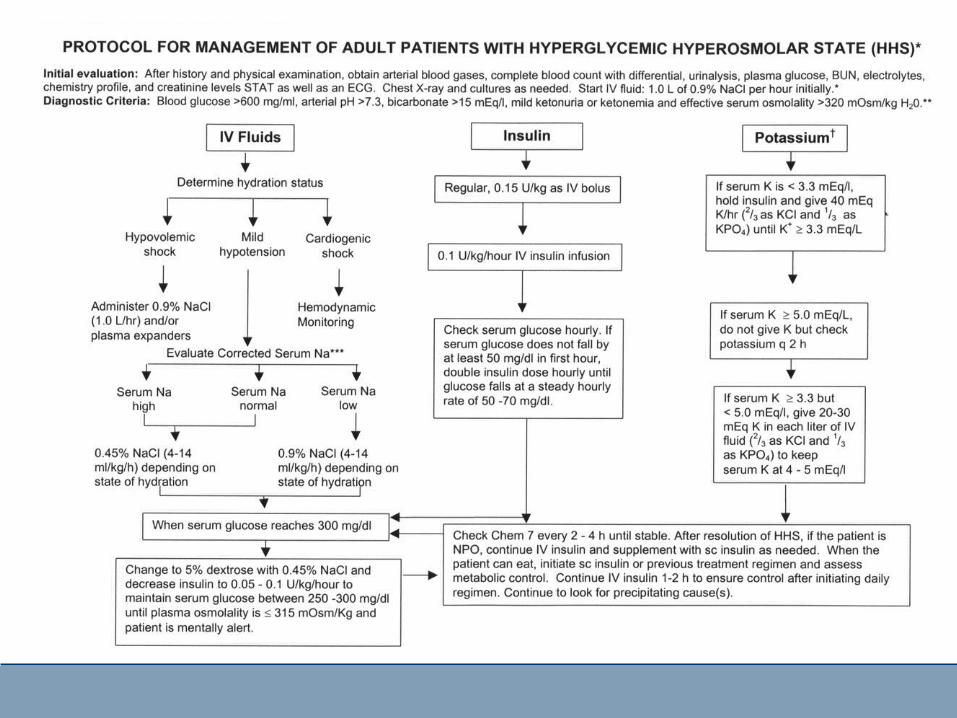
Laboratory Findings• Glucose: >600 mg/dL• HCO3>15• Serum osmolarity >320 mOsml/L• pH>7.3 without evidence of significant ketosis
– Level of acidemia is influenced by severity of shock & starvation
• Lab values consistent with acute renal failure, rhabodmyolysis & pancreatitis
40
Treatment• Insulin plays a secondary role
– Hyperglycemia can often be corrected via volume resuscitation
– Renal perfusion is improved, GF is enhanced– Insulin gtt 0.1 U/kg/hr
Complications• Cardiac arrest• Refractory
arrhythmias• Pulmonary
thromboemboli• Circulatory collapse• Refractory shock
• Acute renal failure• Rhabdomyolysis• Neurologic deficits• Electrolyte
disturbances• Multisystem organ
failure
41

42
Treatment• Adult mortality: 15%• Pediatric prevalence of HHS is unknown
43
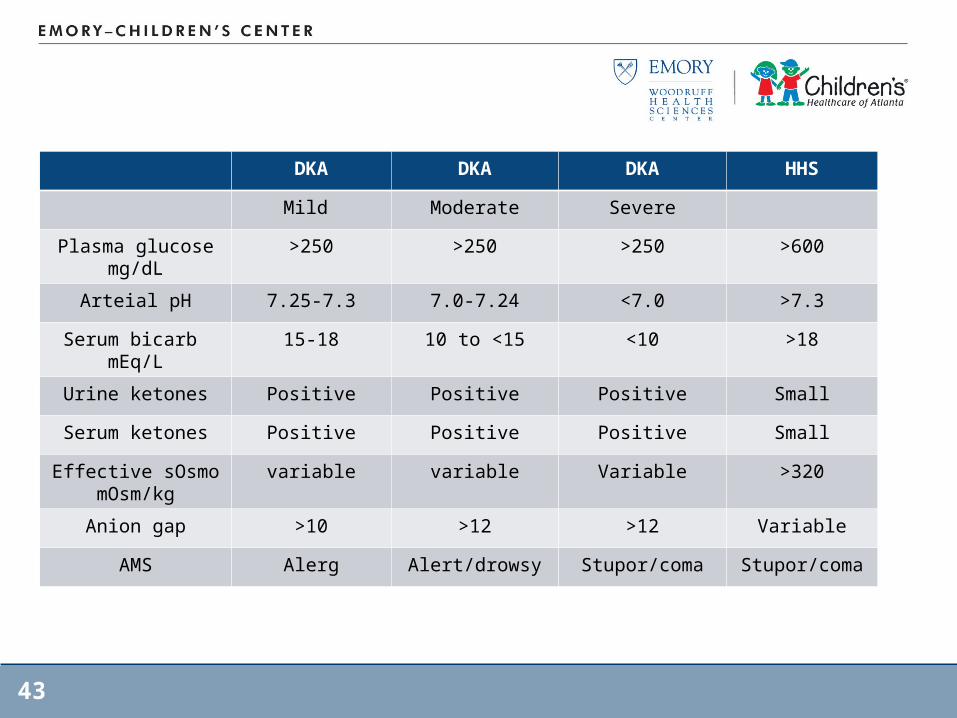
DKA DKA DKA HHS
Mild Moderate Severe
Plasma glucose mg/dL
>250 >250 >250 >600
Arteial pH 7.25-7.3 7.0-7.24 <7.0 >7.3
Serum bicarb mEq/L
15-18 10 to <15 <10 >18
Urine ketones Positive Positive Positive Small
Serum ketones Positive Positive Positive Small
Effective sOsmomOsm/kg
variable variable Variable >320
Anion gap >10 >12 >12 Variable
AMS Alerg Alert/drowsy Stupor/coma Stupor/coma
44
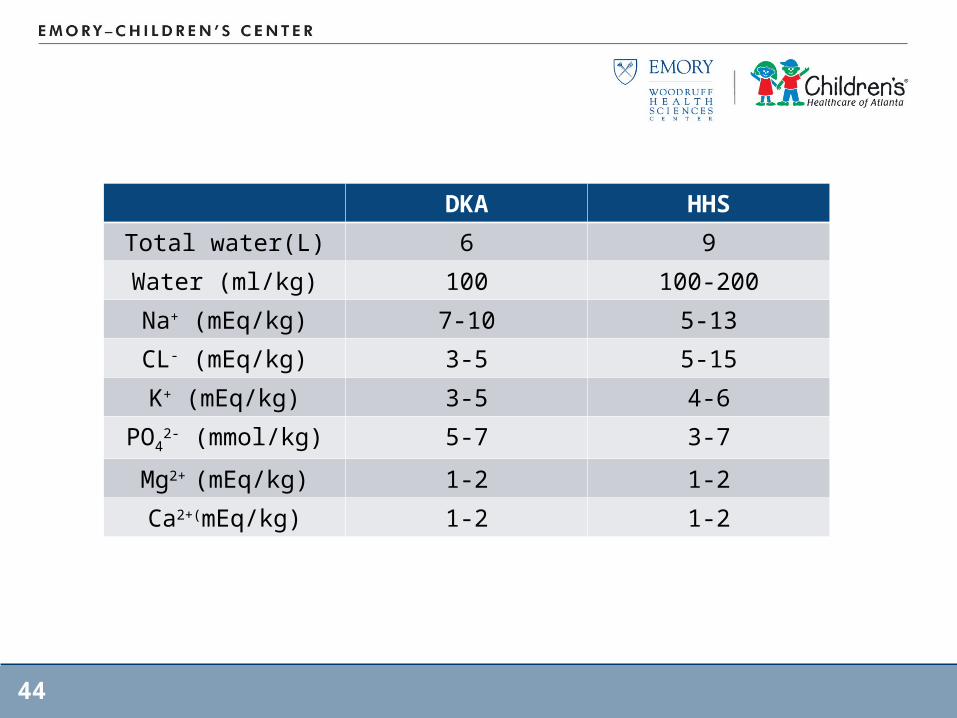
DKA HHS
Total water(L) 6 9
Water (ml/kg) 100 100-200
Na+ (mEq/kg) 7-10 5-13
CL- (mEq/kg) 3-5 5-15
K+ (mEq/kg) 3-5 4-6
PO42- (mmol/kg) 5-7 3-7
Mg2+ (mEq/kg) 1-2 1-2
Ca2+(mEq/kg) 1-2 1-2

45