does infusion of colloid influence the occurrence of postoperative nausea and vomiting after...
TRANSCRIPT

Does Infusion of Colloid Influence the Occurrence of Postoperative Nausea
and Vomiting After Elective Surgery in
Women? (Anesth Analg 2009;108:1788 –93)
BACKGROUND
The prevention of postoperative nausea and vomiting (PONV) has been the subject of several studies
In addition to the effects of various drugs, it has been shown that the administration of high volumes of intraoperative fluid replacement, commonly crystalloids, can decrease the incidence of PONV
BACKGROUND
The impact of the type of fluid on postoperative nausea and vomiting (PONV) is not well defined.
In this study we investigated the effects of colloids or crystalloids on PONV when given in addition to a background minimal crystalloid infusion in a female population of surgical patients.

METHODS
115 female patients with ASA I or II elective gynecological or breast surgery randomly allocated to receive HES 130/0.4 or
0.9% NaCl Exclusion criteria: <18 yr coagulopathy (凝血) significant hepatic or renal dysfunction (肝肾功能) congestive heart failure (充血性心衰) hypersensitivity to HES (过敏)
METHODS
background solution starting at the induction of anesthesia 5% dextrose in 0.45% NaCl 0.5 mL /kg/h for 24 h
study solution before the induction of anesthesia 500 mL HES 130/0.4 or 0.9% NaCl 1 mL /kg/ h for 24 h

METHODS
No antiemetic prophylaxis ECG, NBP, SPO2, and CO2 induced : 1–2.5 mg/kg propofol 10–20 ug sufentanil
neuromuscular blocking drug maintained : sevoflurane (1–2 MAC) sufentanil and/or neuromuscular blocking drugs
Patients received IV analgesia for postoperative pain relief consisting of 1 g paracetamol 4 times per day , and 1 mg/kg diclofenac twice per day to a maximum of 75 mg twice per day
Primary End Points
The occurrence of any postoperative nausea or vomiting during the 24 h after surgery
Nausea (恶心) the urge to vomit without expulsion of gastric contents and withou
t effort to empty the stomach Vomiting (呕吐) the forceful expulsion of liquid gastric contents Retching (干呕) vomiting efforts, but without gastric emptying, and was considere
d the same as vomiting for the purpose of this study
The severity of nausea was rated on an 11-point number rating scale (NRS): any score on the 11-point NRS more than zero was considered to be a positive event
PONV was evaluated every hour for the first 4 h, and then every 3 h for 24 h.
Secondary End Points The frequency of antiemetic rescue therapy use Treatment : 5 mg dexamethasone 1.25 mg droperidol 100 mg alizapride 4 mg IV ondansetron if each of the previous treatments failed
The need for antiemetic therapy and the number of times antiemetic therapy was required were noted (mono, bi, tri, or quadritherapy )
The incidence of hypotensive events (Hypotension defined as a 20% decrease in systolic blood pressure compared with the baseline)
Hypotension and nausea occurring at the time of the patient’s first mobilization after surgery
The severity of pain In addition, pain severity was rated on an 11-point N
RS and evaluated at the same intervals as PONV

RESULTS

RESULTS
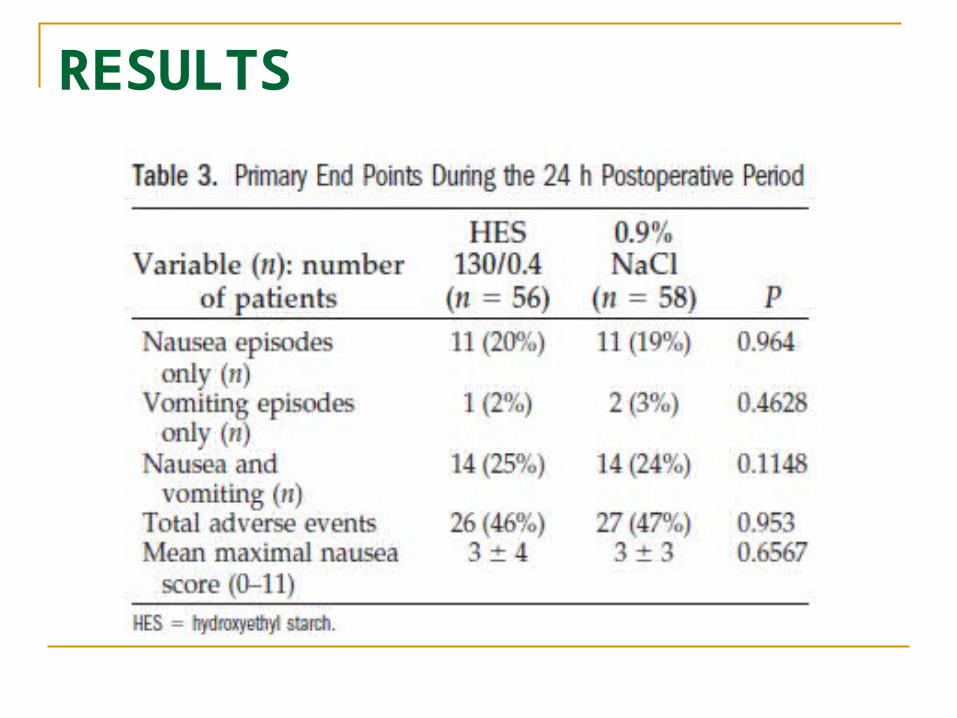
RESULTS

RESULTS

DISCUSSION Previous studies investigating the effect of colloid
versus crystalloid for surgeries in which large fluid shifts or blood loss was expected showed a 50% reduction in the incidence of PONV
The present study using female patients having surgery with limited fluid shifts or blood loss was unable to demonstrate that the infusion of HES 130/0.4, in addition to a fixed background infusion of 5% dextrose in 0.45% NaCl, could produce such a profound effect on the incidence of PONV or the need for antiemetic treatment compared with 0.9% normal saline
DISCUSSION
limitations First, there was no placebo arm, but this woul
d have been difficult, as some fluids are required by all patients .We could perhaps have added a group with intraoperative lactated Ringer’s solution followed by 5% dextrose in 0.45% NaCl, which is our standard practice.

Second, our choice of antiemetic drugs may not have been optimal; by choosing dexamethasone as the primary rescue antiemetic, this may have delayed the treatment of PONV and hence increased the incidence of PONV; nevertheless, this effect would have been the same for the two groups

CONCLUSION
In conclusion, in women undergoing gynecological or breast surgery with no major blood loss, HES 130/0.4 and 0.9% NaCl, at the volumes used in this study, had similar effects on PONV when administered along with a low-volume baseline infusion of 5% dextrose in 0.45% NaCl
This is in contrast to when large fluid shifts or blood loss occur where colloid solutions seem to have a more profound effect on PONV
THANK YOU!
THANK YOU!