5/23/17
1
UpdateinWomen’sHealth
JudithWalshMD,MPHDivisionofGeneralInternalMedicineWomen’sHealthCenterofExcellence
Planfortoday…• Reviewsomeofthemostsignificantpublishedadvancesin
theWomen’sHealthmedicalliteratureoverthepastyear– Toparticles– Keyarticles– Guidelines
• Assessthestrengthandscopeoftheevidencepresentedintheselectedliterature
• Applythisnewinformationtoourclinicalpractice– Take-homepoints
• SGIMAnnualMeeting,April2017– ErinContratto MD,Bimla Schwarz,MDandLydiaPaceMD
Process
16JournalsMarch12016-Feb20174Independentreviewers:ranked1-4stars
Criteria
• Hownew/innovativeisthisinformation?• Strengthoftheevidence?• Howwillitchangemypractice?
5/23/17
2
• OCPsandCancer• BingeEating• CranberryandUTIs• Tomosynthesis
• Lymphedema&blooddraws
• HormonetherapyandCVD
• DXAmonitoringontherapy
• Atypicalfractures
ISSUESAFFECTINGREPRODUCTIVEAGEWOMEN
Case
• 39yearoldwomanwhohasbeenonOCPssinceshewas19,whenshestartedthemforirregularandpainfulmenses.Shedoesnotdesirechildrenandishappywithherlightandrelativelypainlessmenses.Shewouldliketocontinuebutisworriedthattheymaynotbesafeforwomenafter40.Whatdoyoutellher?
TheNews
• Lifetimecancerriskandcombinedoralcontraceptives:theRoyalCollegeofGeneralPractitioners'Oral Contraception Study– Iversen etal.AJOG2017
5/23/17
3
UKRoyalCollegeofGeneralPractitioners'Oral Contraception Study
• 46,022womenrecruited1968-1969• Followedforupto44years
– 4661everCOCuserswithatleastonecancerduring884,895woman-yearsofobservation
– 2341neverCOCuserswithatleastonecancerduring388,505woman-yearsofobservation.
Iversen etal.AJOG2017
Results
• Previousconcernsofanyincreasedriskofbreast andcervical cancerlostwithinfiveyearsofstoppingCOC– noevidenceofincreasedriskofeithercancerrecurringwithtime.
– Suggestsearlierdiagnosisratherthantrueharm• Increasedriskoflung cancerwasseenonly
amongeveruserswhosmoked
ImportantcancerreductionspersistmanyyearsafterstoppingCOCuse
• Poissonregressiontoestimateincidencerateratios(IRR)betweeneverandneverCOCusers– adjustedforage,parity,smoking,andsocialclass
EveruseofCOCassociatedwithreducedcancer:• Endometrial (IRR0·66,99%CI0·48-0·89)• Ovarian (IRR0·67,99%CI0·50-0·89)• Colorectal (IRR0·81,99%CI0·66-0·99)• Lymphatic/ (IRR0·74,99%CI0·58-0·94)Hematopoietic
Iversen etal.AJOG2017
Implicationsforpractice
• Hormonal“contraception”maybeimportantforcancerprevention– EspeciallyifBMI>30– Evenifshewerenotseekingcontraception– Evenifshewere50yearsofage
• Levonorgestrel IntrauterineDeviceasanEndometrialCancerPreventionStrategyinObeseWomen:ACost-EffectivenessAnalysis
– Dottino JA,etal.ObGyn 2016
5/23/17
4
Irregularbleedinginpremenopausalwomen?
• Bodymassindextrumpsageindecisionforendometrialbiopsy:cohortstudyofsymptomaticpremenopausalwomen– Wiseetal.AJOG2016
• AIM:Toassesstheeffectofbodymassindexonriskofendometrialhyperplasiaorcancerinyoungsymptomaticpremenopuasal women
Methods
• Retrospectivecohortof916premenopausal womenreferredforendometrialbiopsyforabnormaluterinebleeding– Noknownhistoryofendometrialcancer
• SinglesiteinNewZealand,2008-2014• Meanage=42yo• 50%obese(BMI>30)
Wiseetal.AJOG2017
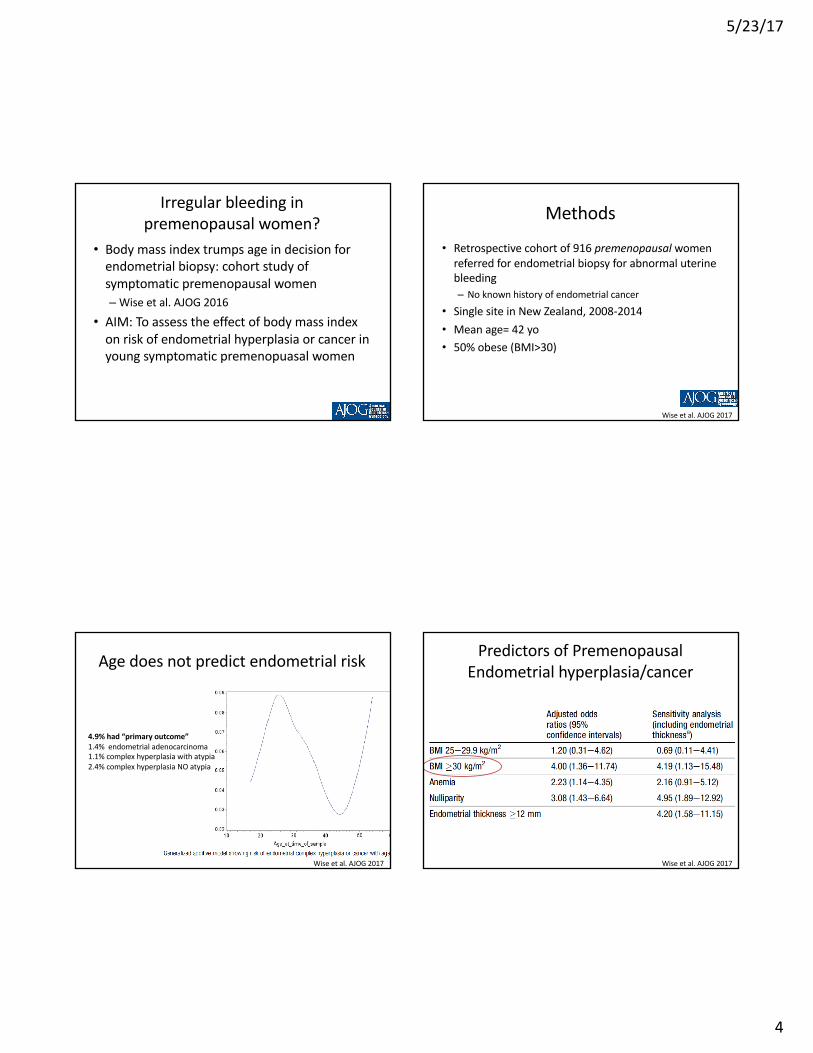
4.9%had“primaryoutcome”1.4%endometrialadenocarcinoma1.1%complexhyperplasiawithatypia2.4%complexhyperplasiaNOatypia
Agedoesnotpredictendometrialrisk
Wiseetal.AJOG2017
PredictorsofPremenopausalEndometrialhyperplasia/cancer
Wiseetal.AJOG2017
5/23/17
5
Implicationsforpractice
• Thinkaboutpreventingendometrialcancerwhencaringforobesewomen
• Considerultrasoundtoassessendometriallining+/- Biopsy– Especiallyifmenorrhagiaresultsinanemia
Case:HPV• 25yearoldwomanreceived2dosesofHPVvaccineseveralyearsagoandwantstoknowifsheshouldrestarttheHPVseries?Youtellher…
A. Sincelastdose>12monthsago,sheshouldrestartthefull3doseseries.
B. Ifshereceived2dosesbeforeage15,nofurtherdosesareneeded.
C.HPVvaccineisonly2dosesnow,regardlessofage.
Background:HPVvaccination
v9vHPVvaccine– Gardasil9(Merck®)– FDAapprovedDec2014– 2016:onlyvaccinedistributedinUS– 6,11 (genitalwarts)– 16,18+31,33,45,52,58(oncogenic)
MMWRDec16,2016
TheNewsv TwovsThreeDosesofHumanPapillomavirusVaccineNewPolicyforthe
SecondDecadeoftheVaccinationProgram- Markowitzetal.JAMA.2016
v Immunogenicityof9-valentHPVvaccineUsing2-DoseRegimeninGirlsandBoysvsa3-DoseRegimeninWomen– Iversen etal.JAMA2016§ 1377boys&girlsages9-14§ 97.9%seroconversion4weeksafter2nd dose
vACIPDec2016(AdvisoryCommitteeonImmunizationPractices)• Routinevaccine11-12yo• 2doseseriesages9-14(0,6-12mo)• 15-26:3doseseries(0,1-2,6mo)
MMWRDec16,2016
5/23/17
6
Conclusion
vHowmanydosesofHPVvaccineshouldpatientsreceive?
• If2dosesinitiatedbeforeage15years,nofurtherdoses.
• Ifseriesstartedafterage15,3dosesgiven.• Ifvaccinationscheduleisinterrupted,donotrestartseries.
MMWRDec16,2016
Case:BingeEatingDisorder38yo womanpresentstodiscussweightlossoptions.Shehasdifficultywithportioncontrolanddescribesweeklyepisodesofeatinglargequantitiesoffoodinashortperiodoftime.Shefeelsthatshecannotcontrolherselfduringthesebinges.RecentlysheconsumedanentirebagofOreosin30minutes.Shedoesnotinducevomitingorexerciseexcessivelyafterbinges.BMIis29.Whattherapywillpreventbingeeating&reduceweight?
A.sibutramineB.self-directed- cognitivebehaviortherapyC.lisdexamfetamineD.sertraline
BingeEatingDisorder• MostcommoneatingdisorderintheUS
• Lifetimeprevalence– women 3.5%(vsmen2%)– obese 5-30%
• DSMVCriteria– recurrent(>1x/wk)over3mo– brief(<2hrs)– psychologicallydistressedbinge-eating:consumelargeramountsoffoodthanmostpeoplewouldundersimilarcircumstances&lackcontrolovereating
• Currenttreatmentguidelinesareconflicting(AmericanPsychiatricAssociation,NationalInstituteforHealth&CareExcellence)
News:LisdexamfetamineforBingeEatingdisorders
vBinge-EatingDisordersinAdults:AsystematicReviewandMeta-analysis
- Brownley etal.AnnalsofInternalMedicine2016.
Objective:summarizeevidenceaboutbenefits&harmsofpsychological&pharmacologictherapiesforadultswithbinge-eatingdisorder.Methods:systematicreviewFunding:AHRQ
5/23/17
7
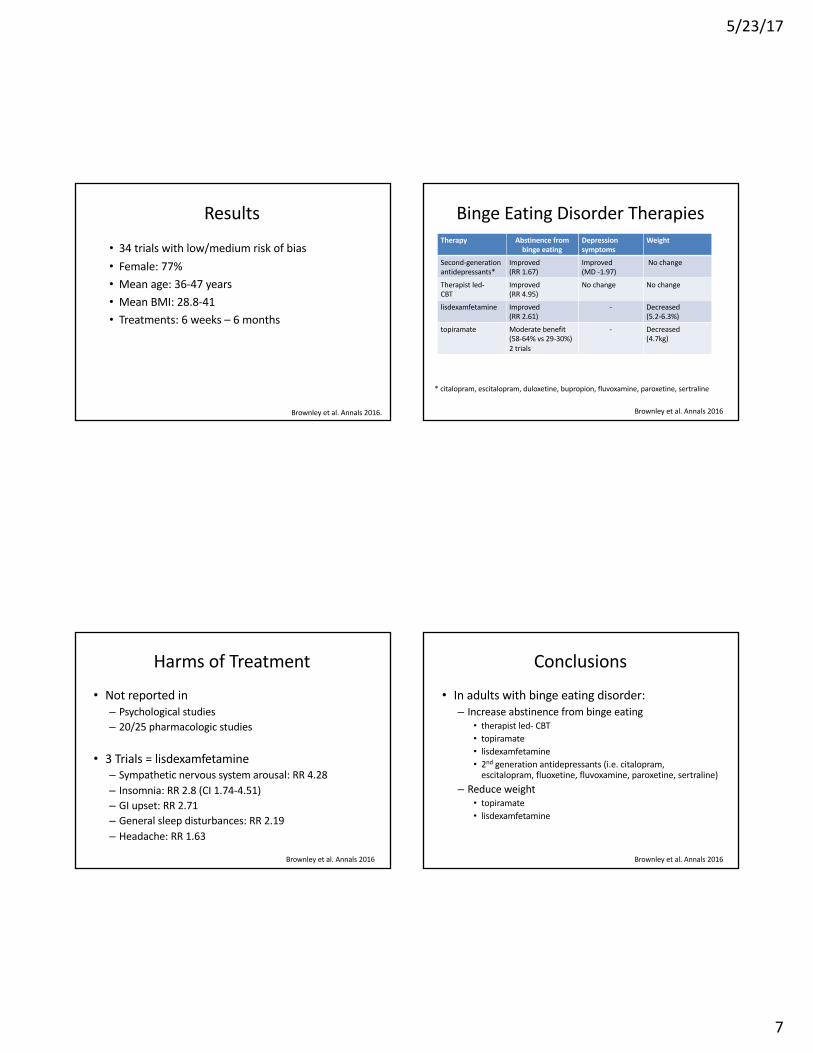
Results
• 34trialswithlow/mediumriskofbias• Female:77%• Meanage:36-47years• MeanBMI:28.8-41• Treatments:6weeks– 6months
Brownley etal.Annals2016.
BingeEatingDisorderTherapiesTherapy Abstinencefrom
bingeeatingDepressionsymptoms
Weight
Second-generationantidepressants*
Improved(RR1.67)
Improved(MD-1.97)
Nochange
Therapist led-CBT
Improved(RR4.95)
Nochange Nochange
lisdexamfetamine Improved(RR2.61)
- Decreased(5.2-6.3%)
topiramate Moderate benefit(58-64%vs29-30%)2 trials
- Decreased(4.7kg)
*citalopram, escitalopram, duloxetine, bupropion,fluvoxamine,paroxetine,sertraline
Brownley etal.Annals2016
HarmsofTreatment
• Notreportedin– Psychologicalstudies– 20/25pharmacologicstudies
• 3Trials=lisdexamfetamine– Sympatheticnervoussystemarousal:RR4.28– Insomnia:RR2.8(CI1.74-4.51)– GIupset:RR2.71– Generalsleepdisturbances:RR2.19– Headache:RR1.63
Brownley etal.Annals2016
Conclusions
• Inadultswithbingeeatingdisorder:– Increaseabstinencefrombingeeating
• therapistled- CBT• topiramate• lisdexamfetamine• 2nd generationantidepressants(i.e.citalopram,escitalopram,fluoxetine,fluvoxamine,paroxetine,sertraline)
– Reduceweight• topiramate• lisdexamfetamine
Brownley etal.Annals2016
5/23/17
8
Case:Cranberryjuice• 36yo womanrecoveringfromrecentE.coliUTIstates,“mymothertoldmecranberryjuicetreatsUTI’s,isthistrue?”Youtellher…
A) ThereisnoevidenceoncranberryjuiceandUTIsB) Cranberryjuice/capsuleshavenotbeenproved
effectiveatpreventingUTIC) Cranberryjuice/capsulespreventUTIsfornursing
homepatientsD) Wrongjuice- tryorangejuice
Background• Cranberryproanthocyanidins
– inhibitadherenceofE.colitouroepithelial cells
• PriorstudiesUTIprophylaxis– women78.5yrs– 300mL(~10oz)=36mg– dailyx6months– decreasedbacteria&pyuria
Howelletal.NEngl JMed.1998Lavigne etal. Clin Microbiol Infect.2008Avorn etal. JAMA.1994
TheNews
• Effectof Cranberry Capsules onBacteriuriaPlus Pyuria Among Older Women in NursingHomes.– Juthani-Mehtaetal.JAMA. 2016
• Objectives– effectof2cranberry capsules/day
(72mgproanthocyanidin)• bacteriuria+ pyuria• womennursinghomeresidents
MethodsStudyDesign
– Double-blindplacebo-controlled,efficacyRCT– 21NursingHomes:Aug2012-Oct2014
Outcomes– Bacteriuria(>100KCFU)+pyuria(WBC)
• assessedq2months,followed12months
Exclusioncriteria– chronicsuppressiveantibiotics– ESRD– Unabletoprovidebaselinecleancatchurinespecimen– warfarin– hx ofnephrolithiasis– indwellingbladdercatheter– nursinghomeresidence<4weeks
Juthani-Mehtaetal.JAMA. 2016
5/23/17
9
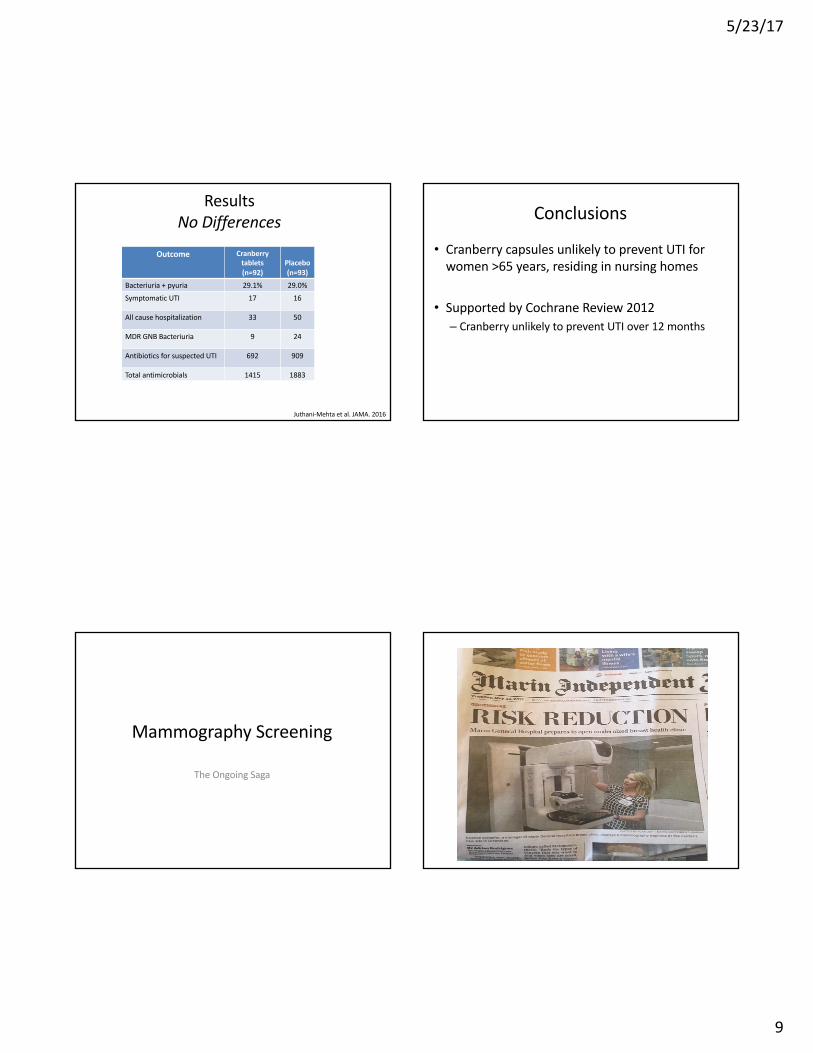
ResultsNoDifferences
Outcome Cranberrytablets(n=92)
Placebo(n=93)
Bacteriuria +pyuria 29.1% 29.0%SymptomaticUTI 17 16
Allcausehospitalization 33 50
MDRGNBBacteriuria 9 24
AntibioticsforsuspectedUTI 692 909
Totalantimicrobials 1415 1883
Juthani-Mehtaetal.JAMA. 2016
Conclusions
• CranberrycapsulesunlikelytopreventUTIforwomen>65years,residinginnursinghomes
• SupportedbyCochraneReview2012– CranberryunlikelytopreventUTIover12months
MammographyScreening
TheOngoingSaga
5/23/17
10
Case
Ms.Smithisa50yearoldwomanwhojusthadherfirstscreeningmammogramwhichshowsheterogeneouslydensebreastsbutnootherabnormalities.• Menarcheat12,firstchildat32• Nohistoryofabreastbiopsy• Nofhx ofbreastcancer
Sheasksifsheshouldhave“oneofthose3Dmammograms”?
Yousay:
• No,Digital(2D)mammograms,every2yearsarefineforyou
• Yes,Digital3Dmammograms(tomosynthesis),every3years
• 2Dor3Dmammogramsevery1yeararefine• Let’sreviewyourriskfordevelopingbreastcancerandyourpreferences
Background
Wangetal,MayoClin Proc2014
• 50%ofbreastsaredense• Tomosynthesis (3Dmammography)
• Nowavailable~22%ofU.S.facilities• Variablycoveredbyinsurance
TheNews• Raffertyetal,BreastCancerScreeningUsingTomosynthesis
andDigitalMammographyinDenseandNondense Breasts,JAMAApril2016
• Objective:– screeningperformanceaccordingtobreastdensitylevel– digitalmammogram+tomosynthesis vsdigitalmammogramalone
• Funding– Hologic
5/23/17
11
Methods
– Retrospectivepre/postanalysisofscreeningperformancemetricsfrom13centers
– 452,320screeningmammograms• 278, 906digitalmammos (2D)• 173,414digitalmammos +tomosynthesis (3D)
– Compareddifferencesin(a)recalland(b)cancerdetectionrates,amongwomenwithdensevs.nondensebreasts
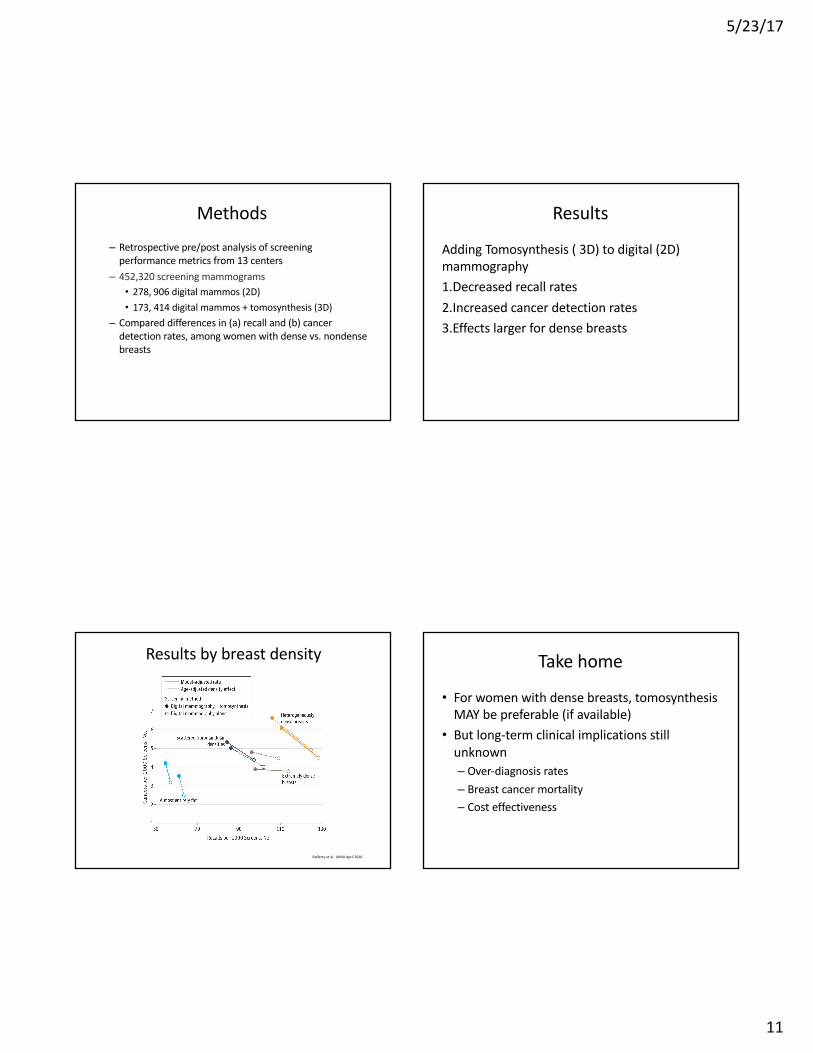
Results
AddingTomosynthesis (3D)todigital(2D)mammography1.Decreasedrecallrates2.Increasedcancerdetectionrates3.Effectslargerfordensebreasts
Resultsbybreastdensity
Raffertyetal.JAMAApril2016.
Takehome
• Forwomenwithdensebreasts,tomosynthesisMAYbepreferable(ifavailable)
• Butlong-termclinicalimplicationsstillunknown– Over-diagnosisrates– Breastcancermortality– Costeffectiveness
5/23/17
12
USPSTFGuidelinesMammography• Age 50-74: screening mammography every 2 years• Age 40-49: individualize decision to begin biennial
screening according to patient’s context and values• Age ≥75: no recommendation (insufficient evidence)
BreastExam• Clinicalbreastexaminationalone– insufficientevidence• Recommendagainstteachingwomentoperformroutine
breastself-examination– Nomortalitybenefit– Higherratesofbenignbreastbiopsies
» USPSTF2016
USPSTFGuidelines
• Evidenceisinsufficienttoassessthebalanceofbenefitsandharmsfordigitalbreasttomosynthesis(DBT)
• Theevidenceisinsufficienttoassesstherisksandbenefitsofadjunctivescreening(ultrasound,MRIorDBT)forwomenwithdensebreastsandanotherwisenegativescreeningmammogram
– January,2016
TheNews
• TailoringBreastCancerScreeningIntervalsbyBreastDensityandRiskforWomenAged50YearsorOlder:CollaborativeModelingofScreeningOutcomes– Trentham-Dietzetal,AnnInt Med2016
• Modelingstudyofwomenaged50-74at4differentrisklevelsand4breastdensitylevels
• Examinedoutcomesfromannual,biennialandtriennialscreening
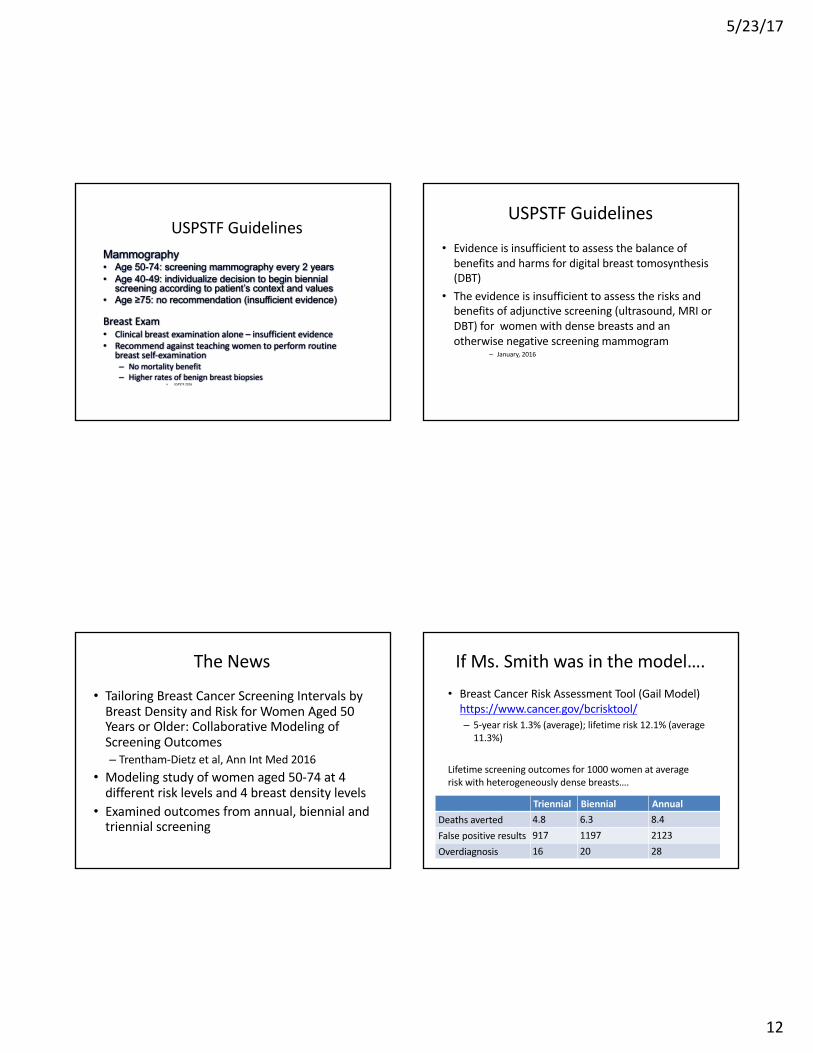
IfMs.Smithwasinthemodel….• BreastCancerRiskAssessmentTool(GailModel)https://www.cancer.gov/bcrisktool/– 5-yearrisk1.3%(average);lifetimerisk12.1%(average11.3%)
Lifetimescreeningoutcomesfor1000womenataverageriskwithheterogeneouslydensebreasts….
Triennial Biennial AnnualDeathsaverted 4.8 6.3 8.4Falsepositiveresults 917 1197 2123Overdiagnosis 16 20 28
5/23/17
13
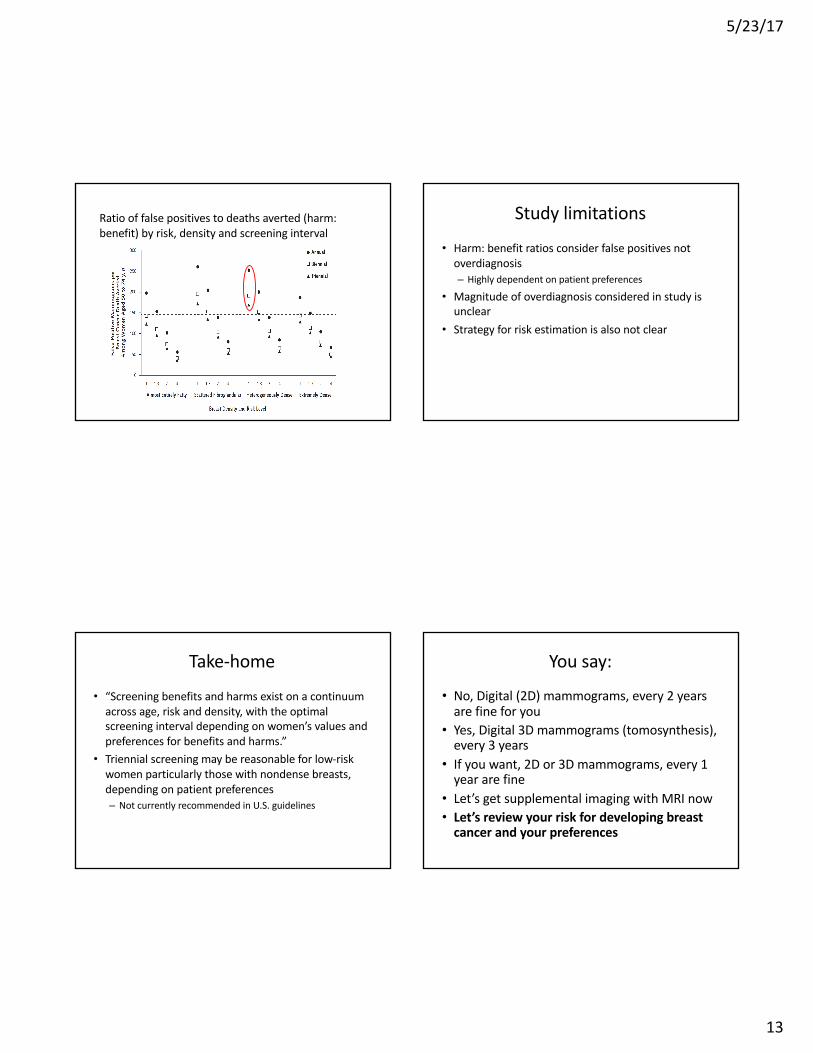
Ratiooffalsepositivestodeathsaverted(harm:benefit)byrisk,densityandscreeninginterval
Studylimitations
• Harm:benefitratiosconsiderfalsepositivesnotoverdiagnosis– Highlydependentonpatientpreferences
• Magnitudeofoverdiagnosis consideredinstudyisunclear
• Strategyforriskestimationisalsonotclear
Take-home
• “Screeningbenefitsandharmsexistonacontinuumacrossage,riskanddensity,withtheoptimalscreeningintervaldependingonwomen’svaluesandpreferencesforbenefitsandharms.”
• Triennialscreeningmaybereasonableforlow-riskwomenparticularlythosewithnondense breasts,dependingonpatientpreferences– NotcurrentlyrecommendedinU.S.guidelines
Yousay:
• No,Digital(2D)mammograms,every2yearsarefineforyou
• Yes,Digital3Dmammograms(tomosynthesis),every3years
• Ifyouwant,2Dor3Dmammograms,every1yeararefine
• Let’sgetsupplementalimagingwithMRInow• Let’sreviewyourriskfordevelopingbreastcancerandyourpreferences
5/23/17
14
Case• Ms Jonesisa75FwithahistoryofHTNandLbreastcancer12yearsago,s/pmastectomy,chemo,tamoxifen
• Today,BPis175/80ontheR.Yousuggestcheckingbotharms,butshestopsyou,sayingaboutherLarm,“that’smymastectomyarm!”
Yousay:a) Oh,you’reright,thankyousomuchforremindingmeb) Thatisaloadofbaloney,anybreastcancersurvivor
canhaveBPchecksonbotharms.c) Whatkindofmastectomydidyouhave?
TheNews• ImpactofIpsilateralBloodDraws,Injections,BloodPressure
Measurements,andAirTravelontheRiskofLymphedemaforPatientsTreatedforBreastCancer.– Fergusonetal,JournalofClinicalOncology 2016
• Objective:– Evaluateassociationbetweentrauma&armswellinginpatientstreatedforbreastcancer
Breastcancer–relatedlymphedema
• Armswelling,discomfort,andultimatelyimpairedfunctionduetocompromisedlymphaticdamage– Removedlymphnodes(sentinelbx orALND)/axillaryXRT
– Lifetimerisk;14.4mo.averagetimetoonset• Knownriskfactors:ALND,obesity,increasedageatDx
Commonrecommendationsforpreventinglymphedema
• Avoidtraumatoipsilateralarm– blooddraws,injections,BPchecks
• Onplaneflights(pressurechange),wearcompressionsleeves
• Theseguidelinesarebasedonanecdotalevidence,notrigorousstudies
• Placeburden/stressonpatients&providersACS: Lymphedema; NationalLymphedemaNetwork; www.hopkinsmedicine.org;http://ww5.komen.org/BreastCancer/Lymphedema.html
5/23/17
15
MethodsStudyDesign:singlesite,prospectivecohortstudyofwomenscreenedforlymphedemainbreastsurgicalclinicParticipants:632womennewlydiagnosedbreastcancer• allhadmastectomyorlumpectomy• 65%hadsomeradiationMethods:
• Prospectivescreeningforlymphedemawperometer(infraredvolumeassessment)pre-op,post-op,thenq3-7months
• Patientsurveyateachvisit» #intervalblooddraws/injections/BPreadings/traumaatriskarm» #flights
Fergusonetal.JournalofClinicalOncology2016
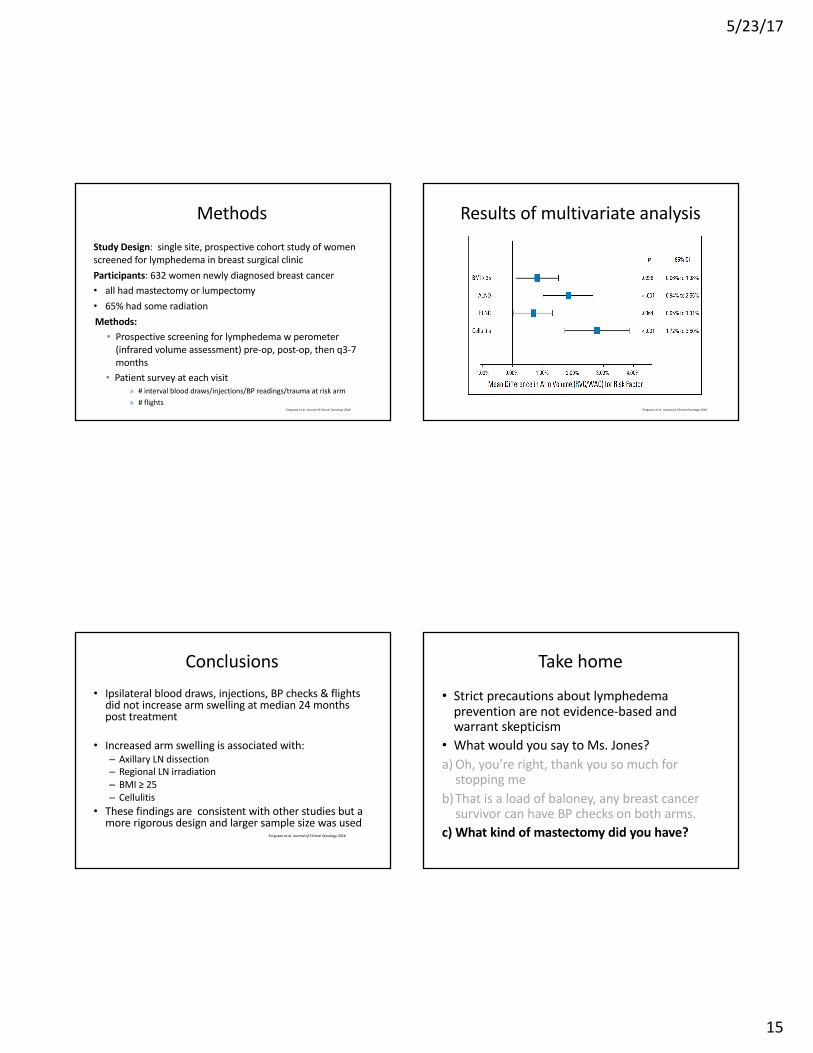
Resultsofmultivariateanalysis
Fergusonetal.JournalofClinicalOncology2016
Conclusions• Ipsilateralblooddraws,injections,BPchecks&flightsdidnotincreasearmswellingatmedian24monthsposttreatment
• Increasedarmswellingisassociatedwith:– AxillaryLNdissection– RegionalLNirradiation– BMI≥25– Cellulitis
• Thesefindingsareconsistentwithotherstudiesbutamorerigorousdesignandlargersamplesizewasused
Fergusonetal.JournalofClinicalOncology2016
Takehome
• Strictprecautionsaboutlymphedemapreventionarenotevidence-basedandwarrantskepticism
• WhatwouldyousaytoMs.Jones?a) Oh,you’reright,thankyousomuchforstoppingme
b)Thatisaloadofbaloney,anybreastcancersurvivorcanhaveBPchecksonbotharms.
c) Whatkindofmastectomydidyouhave?
5/23/17
16
Menopause
VasomotorSymptoms
• MinniePauseisa53yearoldwomanwhohadherlastmenstrualperiod18monthsago.Sheisstillhavinghotflashesandawakensatleasttwiceanightwiththem.Shefeelsexhaustedatworkeverydayandwantssomethingthatwill“reallywork.”Heronlymedicalhistoryishypertensionwellcontrolledonlisinopril.Sheisconsideringtakingestrogenbutwantstoknowifitissafe.Whatdoyoutellher?
Whatdoyoutellher?
• Whydon’tyoutryblackcohash- thatwillworkjustaswell
• Venlafaxineisaseffectiveashormonesanditisalotsafer
• Hormonetherapyisprobablyok,ifyoudon’ttakeitfortoolong
• Absolutelynot- noonetakeshormonesanymore
5/23/17
17
Whatdoyoutellher?
• Whydon’tyoutryblackcohash- thatwillworkjustaswell
• Venlafaxineisaseffectiveashormonesanditisalotsafer
• Hormonetherapyisprobablyok,ifyoudon’ttakeitfortoolong
• Absolutelynot- noonetakeshormonesanymore
ShouldIusehormones?
• Ok,sotheymayhelpmysymptoms……butaretheysafe?
Background
• ManyobservationalstudiesshowedaninverseassociationbetweenhormonetherapyandCHD
• Clinicaltrialshavesuggestedeithernooradverseeffects
• WomenintheobservationalstudiesweretypicallyyoungerwithHTinitiatedclosertomenopause– “TimingHypothesis”
TheNews
• VascularEffectsofEarlyvsLatePostmenopausalTreatmentwithEstradiol(ELITE)– Hodis etal.NEJM2016
• Objective– Tocomparetheimpactofhormonetherapyonsubclinicalatherosclerosiswhentherapyisinitiatedsoonaftermenopausevs alongtimetimeaftermenopause
5/23/17
18
Methods:ELITE• 643healthypostmenopausalwomenwithoutdiabetesorclinicalCVD– Stratifiedbytimesincemenopause
• <6yearsvs.≥10years
• Randomizedto1mgestradiolpluscyclicprogesteronevaginalgel(45mg)vs.placebopillsandgel
• Primaryoutcome:changeincarotidarteryintimalthickness– Measuredevery6months– Secondaryoutcome:coronaryatherosclerosismeasuredbycardiacCT
Results:ELITE
• Amongwomen<6yearsfrommenopause– Inplacebogroup,CIMTincreasedby0.0078mm/year– Inestradiolgroup,CIMTonly0.00044mm/year
• P=0.008
• Amongwomen10+yearspostmenopause– CIMTincreased0.0088mm/yearvs0.0100mm/year
• P=0.29
• NodifferencesincardiacCTmeasuresofatherosclerosisineitherstratum
Conclusion
• Oralestradiolwasassociatedwithlessprogressionofsubclinicalatherosclerosiswheninitiatedwithin6yearsofmenopause,butnotwheninitiated10+yearsaftermenopause
TakeHome
• Estrogentherapygivenaroundthetimeofmenopausedoesnotappeartohavedeleteriouscardiovasculareffects
• Thiscanbetakenintoaccountfordecisionmakingaboutestrogentherapyformenopausalsymptoms
5/23/17
19
Osteoporosis
BoneDensityMonitoringEmergingTherapies
Case
• Bonnie Bony is a 68 year old woman who wants to know whether she should have another bone mineral density test. You started her on alendronate last year after a t-score of -2.9. What do you tell her?
Bonnie
1) Let’s schedule it now2) We should do it next year3) There is no need to do it4) I have no idea…what do you think?
Background
• PriorstudieshavenotshownthatrepeatedBMDmeasurementsaremorepredictiveoffracturethanbaselinemeasurement
• WhetherornottomeasureBMDduringpharmacotherapyiscontroversial
• Treatmentfailureisuncommon
5/23/17
20
TheNews
• ChangeinBoneMineralDensityisanIndicatorofTreatment-RelatedAntifracture EffectinRoutineClinicalPractice– LeslieWDetal.AnnInt Med2016
• Objective– ToevaluatewhetherrepeatBMDtestingisanindicatoroftreatment-relatedfractureriskreduction
Methods• PopulationbasedregistryinManitoba,Canada• CanadianGuidelines
– Baselinetestingatage65– 3yearfollowupformostpatients– 1yearfollowupforthoseonAIorsteroids– 5yearfollowupforthoseconsideredlowrisk
• DXAdatabase99%completeandaccurateandcanbelinkedwithotherpopulationbasedhealthdatabases
• Outcomes:Incidentnontraumatic hip,clinicalvertebral,forearmandhumerus fractures
Results
• 6629womeninitiatingosteoporosistreatmentwherechangeinBMDcouldbeassessedatoneormoreskeletalsites– 85%initiallyreceivedbisphosphonates
• DetectablechangeinBMD:– Detectableincreasein30.4%ofwomen– Detectabledecreasein18.8%ofwomen– Stablein50.8%
Results• 61,088personyearsoffollowup
– Median9.2years• WomenwithadetectabledecreaseintotalhipBMDhadincreasedriskoffracture– 2.9%(95%CI:1.5%to4.4%)at5yearfollowup– 5.5%(95%CI:2.8%to8.1%)at10yearfollowup
• WomenwithadetectableincreaseintotalhipBMDhadalowerriskoffracture– 1.3%(95%CI:0.4%to2.2%)at5yearfollowup– 2.6%(95%CI:0.7%to4.5%)at10yearfollowup
• ComparableresultsforfemoralneckBMDandlumbarspineBMD
5/23/17
21
Conclusions
• TreatmentrelatedincreasesinBMDareassociatedwithadecreasedfracturerisk
• TreatmentrelateddecreasesinBMDareassociatedwithanincreasedfracturerisk
• BMDmonitoringamongwomenonosteoporosistreatmentmay behelpfulinidentifyingthosewithsuboptimalresponses
Take-home
• MonitoringBMDamongwomenonosteoporosistherapymaybeusefulinidentifyingwomenwhohave“suboptimalresponses”totherapy
• Unansweredquestions– Whatis“suboptimalresponse?”– Whatis“treatmentfailure”– IfBMDgoesdown,whatwillyoudodifferently?
AtypicalFemoralFractures
• Althoughbisphosphonatesclearlyreduceriskofhipfracture,therehasbeenincreasingconcernaboutatypicalfemoralfractures
• Atypicalfemoralfractures:– Transversefracturesoriginatingatlateralfemoralcortex
– Subtrochanteric orfemoralshaft– Non-comminutedandassociatedwithcorticalthickening
TheNews
• Riskofhip,subtrochanteric andfemoralshaftfracturesamongmidandlongtermusersofalendronate:nationwidecohortandnestedcasecontrolstudy
• Objective– Todetermineoverallsafetyandefficacyoflongtermuseofalendronateinpatientswithosteoporosis
5/23/17
22
Methods
• NationwidepopulationbasedstudyinDenmark• 61,990menandwomenaged50-94atthestartoftreatmentwhohadnotpreviouslytakenalendronate
• Outcomes– Incidentfractureofhip,subtrochanteric femurorfemoralshaft
• Non-fracturecontrolsmatchedbysex,yearofbirthandyearofalendronateinitiation
Results• Incidenceofsubtrochanteric/femoralneckfracture
– 3.4/1000personyears(95%CI:3.2-3.6)• Incidenceofhipfracture
– 16.2/1000personyears(95%CI:15.8to16.6)• Risknohigherinlongtermusersthanincurrentorpastusers
• Highermedicationadherenceandlongerdurationofusewereassociatedwithareducedriskofhipfracture– 0.73(95%CI:0.68to0.78)forMPR>80%– 0.74(95%CI:0.56to0.97)foruse≥10years
Conclusion
• Thebenefit/riskratiosupportsabenefitofalendronateevenwithuseformorethan10years
TakeHome
• Theoverallbenefittoriskratioisfavorableforalendronate,evenwithlongtermuse.
• Longtermalendronateusewillavertmanymorehipfracturesthanwillitcauseatypicalfemoralfractures
5/23/17
23
CurrentTherapies
• Bisphosphonates• SelectiveEstrogenReceptorModulators• ParathyroidHormone• Calcitonin• Denosumab
NewTherapies
• Abaloparatide– PeptidethatselectivelybindstheRGconformationoftheparathyroidhormonetypeIreceptor
• Romosozumab– Monoclonalantibodythatbindssclerostin,increasesboneformationanddecreasedresorption
QuickTake:Abaloparatide
• Abaloparatide-ComparatorTrialinVertebralEndpoints(ACTIVE)Phase3doubleblindRCTwith2463women
• Over18months,abaloparatide reducedtheriskofnewvertebralandnonvertebral fractures
• Moreinformationaboutthebenefitsandrisksneeded
• Howdoesitcomparewithotherosteoporosistreatments?
– MillerPDetalJAMA2016
QuickTake:Romosozumab• FractureStudyinPostmenopausalWomenwithOsteoporosis(FRAME)doubleblindplacebocontrolstudyrandomized7180womentoreceiveromosozumab orplacebo
• Monthlysubcutaneousinjectionfor12monthsfollowedbydenosumab (every6months)for12months
• Lowerriskofvertebralfractureat12monthsandat24monthsaftertransitiontodenosumab
• OnecasesofONJandtwoatypicalfemoralfracturesinromosozumab group
• Howdoesitcomparetootherosteoporosistherapies?
5/23/17
24
TakeHome
• Twonewosteoporosismedicationsonthehorizonandornewlyapproved
• Wheretheyfitinwithothermoreestablishedmedicationsremainstobeseen
TakeHome
• OCPsappeartobesafeforlongtermuse• NewHPVVaccinerecommendationsarefortwodosesifseriesinitiatedbeforeage15
• Newevidencefortreatmentofbingeeatingdisorder.
• Roleoftomosynthesis needsadditionalstudy• CranberrydoesnotpreventUTIs• Newevidenceforlymphedemariskdependingonmastectomycharacteristics
Summary• Estrogengivenaroundthetimeofmenopausedoesnotappeartohaveanydeleteriouscardiovasculareffects
• MonitoringBMDinwomenontherapymayidentifythosehavingasuboptimalresponse
• Overallbenefittoharmratioforalendronatefavorsbenefitforlongtermtreatment
• Romosozumab andAbaloparatide bothpromisingnewtreatments– Needadditionalinformationabouthowtheycomparewithexistingtreatments
Questions?







