In this Issue
HTAHealth Technology Update
Supporting informed decisions . . .
Scanning the HorizonInforming Decision Makers About Emerging Medical Technologies
Issue 5 January 2007
A newsletter on new and emerging health care technologies in Canada
Medical device regulation inCanada: a primer on how HealthCanada regulates medical devices.
CyberKnife®: a radiosurgery systemthat uses focused beams ofradiation, rather than a surgical“knife”, to destroy tumours andother lesions.
Ultrasound-enhanced stroketreatment: ultrasound technologiesmay improve acute stroketreatment by enhancing thedelivery of clot-busting drugs.
Testing newborns for alcoholexposure: a biomarker in anewborn’s first bowel movementmay be used to identify babies atrisk for fetal alcohol spectrumdisorder.
Interactive voice-response system:an automated telephone follow-upprogram allows clinicians to
monitor patients’ recovery afterdischarge from hospital.
New and emerging health technologyreports: a listing of recent publicationsfrom CADTH and other healthtechnology assessment agencies.
As we launch into 2007, our fifth issue ofHealth Technology Update brings youinformation on several new healthtechnologies for the diagnosis andtreatment of disease. The Update alsointroduces an innovative system thatfollows up with patients after they gohome from hospital.
For this issue, we’ve enlisted help fromDr. William Freeland, a British-trainedfamily physician who served as HealthCanada’s Chief of the Device EvaluationDivision in the Bureau of Medical Devicesfrom 1992 until his recent retirement. Dr.Freeland has prepared a primer article forus on how medical devices are regulatedin Canada. We are very fortunate to beable to benefit from Dr. Freeland’sexpertise in this area.
We hope that you find this issue of theHealth Technology Update informativeand useful. And from all of us at CADTH,we wish you a happy, healthy andfulfilling New Year!
A wintry Niagara Falls, Ontario.
Phot
o co
mpo
sitio
n by
Pau
l Tin
g (C
ADTH
) and
Ont
ario
Tour
ism
.
2
5
6
8
4
Sign up for complimentary future issues at https://secure.cadth.ca/index.php/en/subscribe
Your feedback on the newsletter is alwayswelcome, as are suggestions for new
technologies to review in future issues. Pleasesend comments to: Catherine Allison, Editor.
E-mail: <<[email protected]>>
7
2 Issue 5 January 2007
HEALTH TECHNOLOGY UPDATE
In vitro Diagnostic Devices
In vitro diagnostic devices (IVDDs) includereagents, assays and equipment used forexamining specimens taken from thebody. IVDDs are regulated with a separateclassification system, but are alsodesignated as Class I, II, III and IV, based onthe degree of risk associated with theiruse. For example, a blood test that detectsbacterial meningitis is categorized as aClass III IVDD because of the risk that afalse-negative test result may cause deathor long-term disability due to delayeddiagnosis. Class IV IVDDs include donorscreening tests for transmissible virusessuch as HIV and hepatitis, which present ahigh public health risk.
Quality Requirements
The Medical Devices Regulations requireClass II medical devices to bemanufactured under a quality standard(ISO standard 13488:2003) developed bythe International Organization forStandardization. Class III and IV devicesmust meet ISO standard 13485:2003,which deals with both design andmanufacturing standards.
Sign up for complimentary future issues at https://secure.cadth.ca/index.php/en/subscribe
Medical devices are used in the diagnosis,treatment, mitigation orprevention of a medicalcondition. They include avast range of equipment,from a simplethermometer or tonguedepressor to highlysophisticated magneticresonance imaging (MRI)machines or roboticallyassisted surgicalequipment.
In Canada, medical devices are regulatedby Health Canada’s Therapeutic ProductsDirectorate and are subject to theMedical Devices Regulations under theFood and Drugs Act.
Medical Device Regulation in Canada: A PrimerThe goal of the Medical DevicesRegulations is to ensure, to the extentpossible, that devices offered for sale inCanada are safe, effective, and meetquality standards.
Device Licensing
Most medical devices must have a licencebefore they can be sold in Canada. HealthCanada categorizes devices as Class I, II,III, or IV, based on the risks associatedwith their use, including the degree ofinvasiveness, duration of contact with thepatient, energy transmission hazard, andconsequences of device malfunction orfailure.
Class I devices present the lowestpotential risk and do not require a licence.Class II devices require the manufacturer’sdeclaration of device safety andeffectiveness, whereas Class III and IVdevices present a greater potential for riskand are subject to in-depth regulatoryscrutiny before licensing and sale. Thecost-effectiveness of medical devices isnot considered. Surgical procedures do notrequire Health Canada licensing.
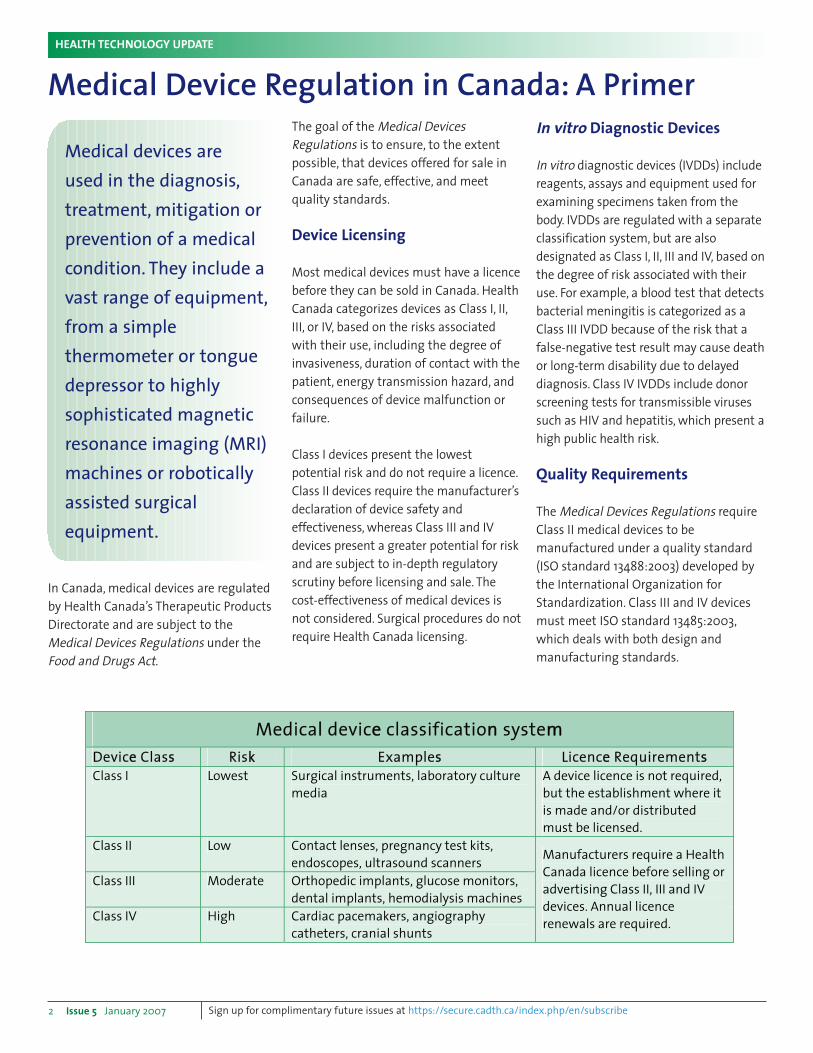
Medicall devicee classificationn systemm Devicee Classs Riskk Exampless Licencee Requirementss Class I Lowest Surgical instruments, laboratory culture
media A device licence is not required, but the establishment where it is made and/or distributed must be licensed.
Class II Low Contact lenses, pregnancy test kits, endoscopes, ultrasound scanners
Class III Moderate Orthopedic implants, glucose monitors, dental implants, hemodialysis machines
Class IV High Cardiac pacemakers, angiography catheters, cranial shunts
Manufacturers require a Health Canada licence before selling or advertising Class II, III and IVdevices. Annual licence renewals are required.
Issue 5 January 2007 3
HEALTH TECHNOLOGY UPDATE
• it is not contrary to the best interests of the patients recruited to the trial
• the objective of the testing will be achieved.
Formal authorization is not required touse a Class I device in a clinical trial,although full trial records must beretained. Devices must be labelled “forinvestigational use only” and any seriousadverse events must be reported toHealth Canada within 72 hours.
Trial sponsors must identify allinvestigators and clinical trial sites andmust comply with Research Ethics Boardrequirements, including protocol approvaland informed patient consent. In makingtheir final decision on the application,Health Canada reviewers evaluate thestudy protocol and design, the hypotheses,the validity of the endpoints and statisticalmethods, as well as the documentationand management of the trial.
The Special Access Program
This program allows health careprofessionals to apply for authorizationto use medical devices that are not yetlicensed in Canada for emergency use, orif conventional therapies have failed, areunavailable or unsuitable. Therapeutic
Sign up for complimentary future issues at https://secure.cadth.ca/index.php/en/subscribe
Cour
tesy
of H
ealth
Can
ada.
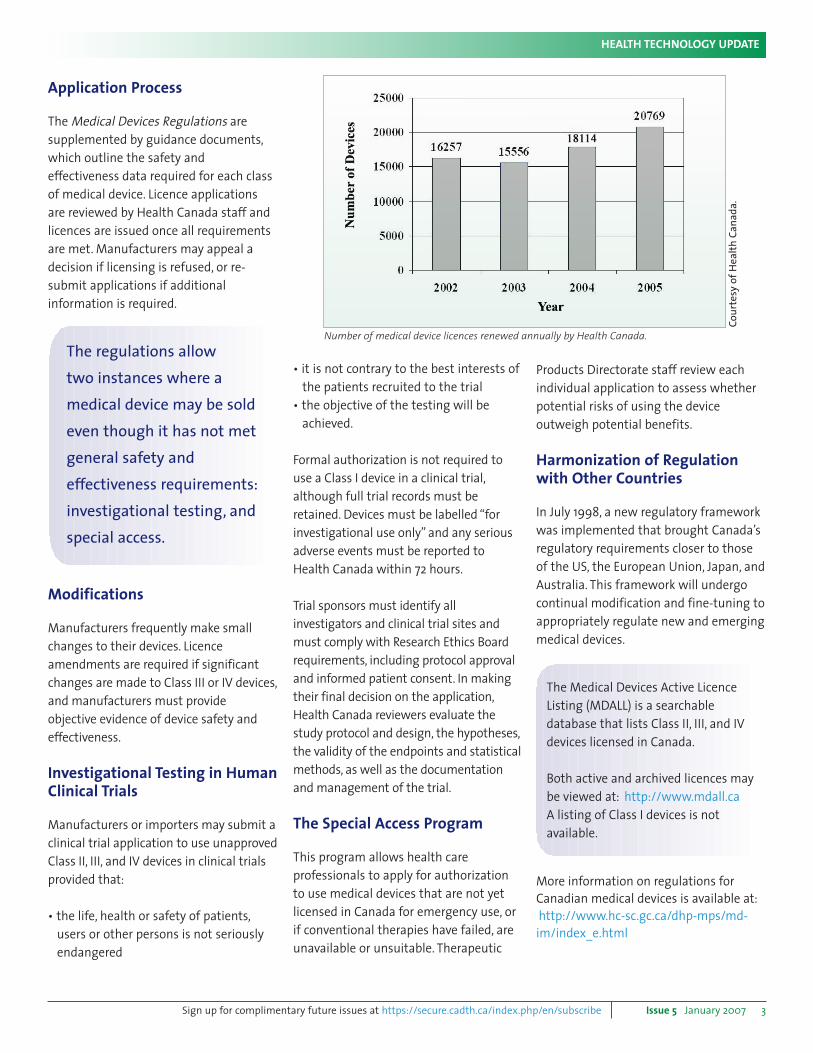
Number of medical device licences renewed annually by Health Canada.
The regulations allow
two instances where a
medical device may be sold
even though it has not met
general safety and
effectiveness requirements:
investigational testing, and
special access.
Application Process
The Medical Devices Regulations aresupplemented by guidance documents,which outline the safety andeffectiveness data required for each classof medical device. Licence applicationsare reviewed by Health Canada staff andlicences are issued once all requirementsare met. Manufacturers may appeal adecision if licensing is refused, or re-submit applications if additionalinformation is required.
Modifications
Manufacturers frequently make smallchanges to their devices. Licenceamendments are required if significantchanges are made to Class III or IV devices,and manufacturers must provideobjective evidence of device safety andeffectiveness.
Investigational Testing in HumanClinical Trials
Manufacturers or importers may submit aclinical trial application to use unapprovedClass II, III, and IV devices in clinical trialsprovided that:
• the life, health or safety of patients,users or other persons is not seriously endangered
The Medical Devices Active LicenceListing (MDALL) is a searchabledatabase that lists Class II, III, and IVdevices licensed in Canada.
Both active and archived licences maybe viewed at: <<http://www.mdall.ca>>
A listing of Class I devices is notavailable.
Products Directorate staff review eachindividual application to assess whetherpotential risks of using the deviceoutweigh potential benefits.
Harmonization of Regulationwith Other Countries
In July 1998, a new regulatory frameworkwas implemented that brought Canada’sregulatory requirements closer to those of the US, the European Union, Japan, andAustralia. This framework will undergocontinual modification and fine-tuning toappropriately regulate new and emergingmedical devices.
More information on regulations forCanadian medical devices is available at:<<http://www.hc-sc.gc.ca/dhp-mps/md-im/index_e.html>>
4 Issue 5 January 2007
HEALTH TECHNOLOGY UPDATE
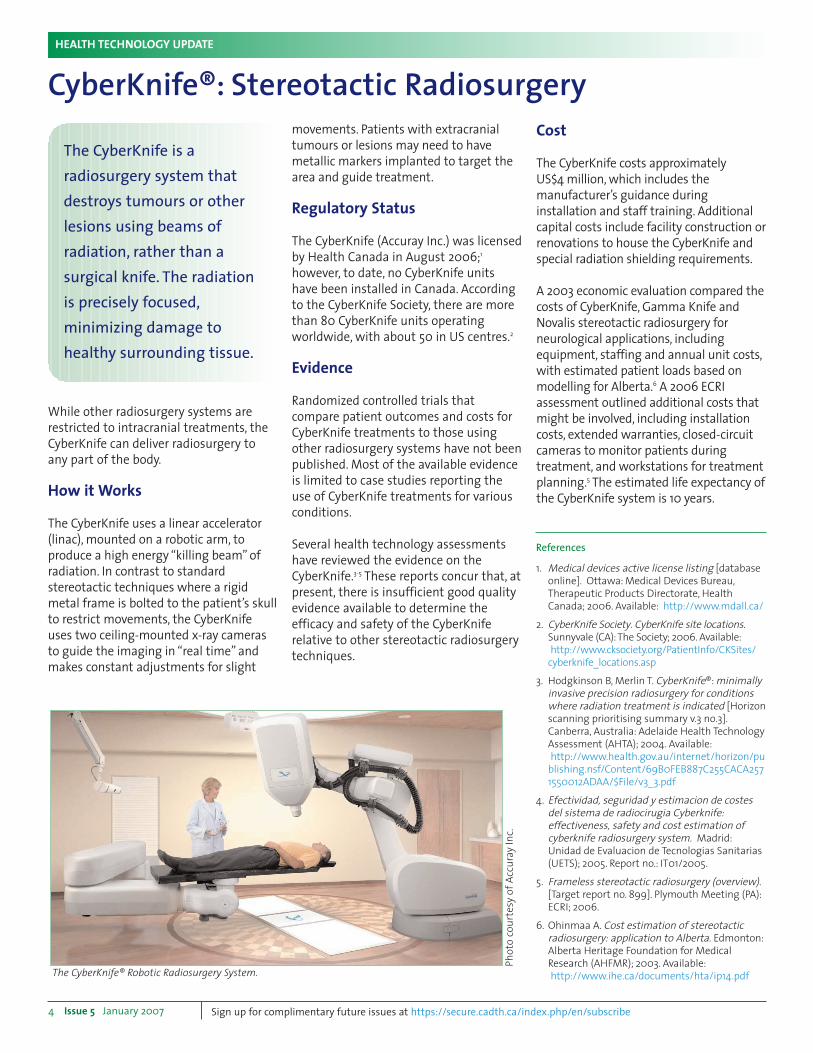
movements. Patients with extracranialtumours or lesions may need to havemetallic markers implanted to target thearea and guide treatment.
Regulatory Status
The CyberKnife (Accuray Inc.) was licensedby Health Canada in August 2006;1
however, to date, no CyberKnife unitshave been installed in Canada. Accordingto the CyberKnife Society, there are morethan 80 CyberKnife units operatingworldwide, with about 50 in US centres.2
Evidence
Randomized controlled trials thatcompare patient outcomes and costs forCyberKnife treatments to those usingother radiosurgery systems have not beenpublished. Most of the available evidenceis limited to case studies reporting theuse of CyberKnife treatments for variousconditions.
Several health technology assessmentshave reviewed the evidence on theCyberKnife.3-5 These reports concur that, atpresent, there is insufficient good qualityevidence available to determine theefficacy and safety of the CyberKniferelative to other stereotactic radiosurgerytechniques.
Cost
The CyberKnife costs approximately US$4 million, which includes themanufacturer’s guidance duringinstallation and staff training. Additionalcapital costs include facility construction orrenovations to house the CyberKnife andspecial radiation shielding requirements.
A 2003 economic evaluation compared thecosts of CyberKnife, Gamma Knife andNovalis stereotactic radiosurgery forneurological applications, includingequipment, staffing and annual unit costs,with estimated patient loads based onmodelling for Alberta.6 A 2006 ECRIassessment outlined additional costs thatmight be involved, including installationcosts, extended warranties, closed-circuitcameras to monitor patients duringtreatment, and workstations for treatmentplanning.5 The estimated life expectancy ofthe CyberKnife system is 10 years.
CyberKnife®: Stereotactic Radiosurgery
References
1. Medical devices active license listing [databaseonline]. Ottawa: Medical Devices Bureau,Therapeutic Products Directorate, HealthCanada; 2006. Available: <<http://www.mdall.ca/>>
2. CyberKnife Society. CyberKnife site locations.Sunnyvale (CA):The Society; 2006. Available:<<http://www.cksociety.org/PatientInfo/CKSites/cyberknife_locations.asp>>
3. Hodgkinson B, Merlin T. CyberKnife®: minimallyinvasive precision radiosurgery for conditionswhere radiation treatment is indicated [Horizonscanning prioritising summary v.3 no.3].Canberra, Australia: Adelaide Health TechnologyAssessment (AHTA); 2004. Available:<<http://www.health.gov.au/internet/horizon/publishing.nsf/Content/69B0FEB887C255CACA2571550012ADAA/$File/v3_3.pdf>>
4. Efectividad, seguridad y estimacion de costesdel sistema de radiocirugia Cyberknife:effectiveness, safety and cost estimation ofcyberknife radiosurgery system. Madrid:Unidad de Evaluacion de Tecnologias Sanitarias(UETS); 2005. Report no.: IT01/2005.
5. Frameless stereotactic radiosurgery (overview).[Target report no. 899]. Plymouth Meeting (PA):ECRI; 2006.
6. Ohinmaa A. Cost estimation of stereotacticradiosurgery: application to Alberta. Edmonton:Alberta Heritage Foundation for MedicalResearch (AHFMR); 2003. Available:<<http://www.ihe.ca/documents/hta/ip14.pdf>>
The CyberKnife is aradiosurgery system thatdestroys tumours or otherlesions using beams ofradiation, rather than asurgical knife. The radiation is precisely focused,minimizing damage tohealthy surrounding tissue.
The CyberKnife® Robotic Radiosurgery System.
Ph
oto
co
urt
esy
of
Acc
ura
y In
c.
Sign up for complimentary future issues at https://secure.cadth.ca/index.php/en/subscribe
While other radiosurgery systems arerestricted to intracranial treatments, theCyberKnife can deliver radiosurgery toany part of the body.
How it Works
The CyberKnife uses a linear accelerator(linac), mounted on a robotic arm, toproduce a high energy “killing beam” ofradiation. In contrast to standardstereotactic techniques where a rigidmetal frame is bolted to the patient’s skullto restrict movements, the CyberKnifeuses two ceiling-mounted x-ray camerasto guide the imaging in “real time” andmakes constant adjustments for slight
benefit persons diagnosed with acuteischemic stroke. In 2004 to 2005, therewere 19,197 “new stroke episodes” inCanada, 88% of which involved ischemicstroke.5
Regulatory Approval
The SonoLysis system has not yet receivedapproval from any regulatory body. Thoughnot approved in Canada, the EKOS Micro-Infusion System has approval from the USFood and Drug Administration for regionalinfusion of contrast materials into selectedvessels in the neurovasculature.6
Evidence
A non-randomized trial comparedpatients treated with tPA, ultrasound andgalactose-based micro-bubbles topatients who received only tPA andultrasound, and those who received onlytPA.3 The complete recanalization rate(re-opening of blocked brain arteries) wassignificantly higher in patients treatedwith micro-bubbles than those in theother groups (54.5% versus 40.8% and23.9%, p=0.038).
SonoLysis therapy is being evaluated forthe treatment of acute ischemic stroke ina Phase I-II study.7
In a Phase II study, the EKOS Micro-Infusion Catheter was used in 34 of 52 patients who had a visible, treatableclot. The recanalization rate was higherthan that found in an earlier Phase I study,which did not use ultrasound catheters(69% versus 55.6%).8 A 40-centre Phase III
Issue 5 January 2007 5
HEALTH TECHNOLOGY UPDATE
Tissue plasminogen activator (tPA) is adrug used to treat acute ischemic stroke –stroke associated with a clot causingblockage of blood flow to the brain.Continuous transcranial ultrasoundmonitoring of an occluded (or blocked)artery induces changes in the structure ofthe clot, resulting in faster penetration oftPA and enhanced clot breakdown(thrombolysis).1
Other approaches to augment tPAtreatment include micro-bubbleadministration with transcranialultrasound,2,3 and a catheter with anultrasound transducer.4
How it Works
SonoLysis® therapy (ImaRx Therapeutics,Inc., Tucson, AZ) uses micro-bubbles –composed of a lipid shell and an inert,biocompatible gas – which are injectedintravenously, with or without athrombolytic drug. SonoLysis bubblespenetrate the clot, and transcranialultrasound causes them to expand andcontract. It is thought that this mechanicalenergy helps break up the clot.
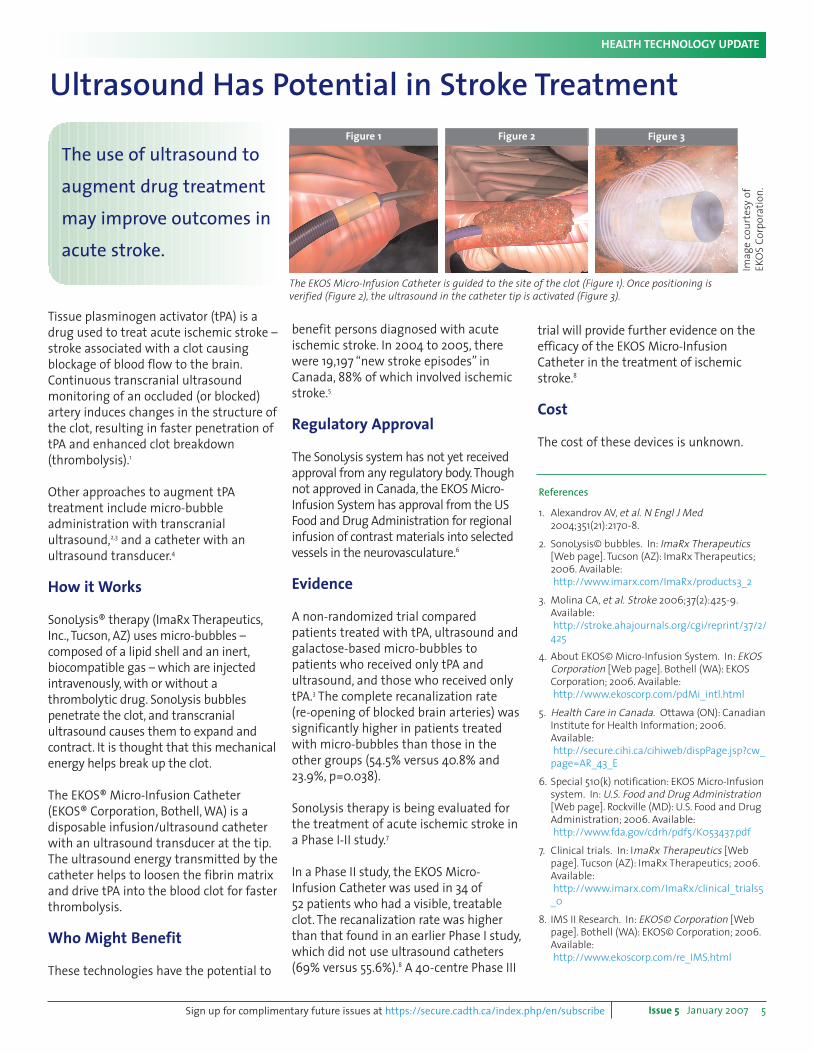
The EKOS® Micro-Infusion Catheter(EKOS® Corporation, Bothell, WA) is adisposable infusion/ultrasound catheterwith an ultrasound transducer at the tip.The ultrasound energy transmitted by thecatheter helps to loosen the fibrin matrixand drive tPA into the blood clot for fasterthrombolysis.
Who Might Benefit
These technologies have the potential to
trial will provide further evidence on theefficacy of the EKOS Micro-InfusionCatheter in the treatment of ischemicstroke.8
Cost
The cost of these devices is unknown.
Ultrasound Has Potential in Stroke Treatment
The use of ultrasound to
augment drug treatment
may improve outcomes in
acute stroke.
Ima
ge
co
urt
esy
of
EK
OS
Co
rpo
rati
on
.
The EKOS Micro-Infusion Catheter is guided to the site of the clot (Figure 1). Once positioning is
verified (Figure 2), the ultrasound in the catheter tip is activated (Figure 3).
References
1. Alexandrov AV, et al. N Engl J Med2004;351(21):2170-8.
2. SonoLysis© bubbles. In: ImaRx Therapeutics[Web page]. Tucson (AZ): ImaRx Therapeutics;2006. Available:<<http://www.imarx.com/ImaRx/products3_2>>
3. Molina CA, et al. Stroke 2006;37(2):425-9.Available:<<http://stroke.ahajournals.org/cgi/reprint/37/2/425>>
4. About EKOS© Micro-Infusion System. In: EKOSCorporation [Web page]. Bothell (WA): EKOSCorporation; 2006. Available:<<http://www.ekoscorp.com/pdMi_intl.html>>
5. Health Care in Canada. Ottawa (ON): CanadianInstitute for Health Information; 2006.Available:<<http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=AR_43_E>>
6. Special 510(k) notification: EKOS Micro-Infusionsystem. In: U.S. Food and Drug Administration[Web page]. Rockville (MD): U.S. Food and DrugAdministration; 2006. Available:<<http://www.fda.gov/cdrh/pdf5/K053437.pdf>>
7. Clinical trials. In: ImaRx Therapeutics [Webpage]. Tucson (AZ): ImaRx Therapeutics; 2006.Available:<<http://www.imarx.com/ImaRx/clinical_trials5_0>>
8. IMS II Research. In: EKOS© Corporation [Webpage]. Bothell (WA): EKOS© Corporation; 2006.Available:<<http://www.ekoscorp.com/re_IMS.html>>
Sign up for complimentary future issues at https://secure.cadth.ca/index.php/en/subscribe
Figure 1 Figure 2 Figure 3
6 Issue 5 January 2007
HEALTH TECHNOLOGY UPDATE
Canada, lifetime costs for additionaleducation, disability payments, and healthcare for one person with FASD have beenestimated at more than $800,000.2
Evidence
In published studies, the sensitivity of themeconium test (to correctly identify babiesthat have been exposed to alcohol) rangesfrom 26.9%4 to 100%.3 Its ability to trulyidentify those who have not been exposedto alcohol ranges from 96.8%4 to 98%.3
Variation could be due to maternalconsumption of small amounts of alcohol inmedications or foods, genetic variations inalcohol metabolism, or illness.1
Elevated levels of meconium FAEEs have notyet been correlated with adverse outcomes innewborn babies. Studies that monitor infantsfor several years are needed to determinewhether FAEEs in meconium can be used asbiomarkers of neurodevelopmental delay dueto fetal alcohol effect.4
In a recent Calgary study, no association wasfound between a mother’s self-reportedalcohol use during pregnancy and FAEElevels in the meconium of 238 infants.5
Publication of the study results is pending.
Availability and Cost
The Motherisk lab at Toronto’s Hospital forSick Children offers the only meconiumFAEE testing in Canada. The assay costsC$150. It is not covered by provincial healthinsurance plans.
mental, and behavioural effects due toprenatal alcohol exposure. Secondarydisabilities associated with FASD includemental health problems, disruptions inschooling, employment problems, criminalbehaviour, and alcohol or drug problems.3
FASD is difficult to diagnose because itrequires confirmation of heavy maternaldrinking, which is under-reported becausewomen are reluctant to admit to riskybehaviour during pregnancy. There arecurrently no specific laboratory markers fordiagnosing FASD.1
Benefits of Early Diagnosis
Early diagnosis of FASD is associated withbetter long-term outcomes.1,3 Targetedinterventions in childhood can reduce therisk for later secondary disabilities.3,4 Thediagnosis of FASD may also help preventalcohol use during subsequent pregnanciesby providing high-risk mothers withcounselling and education.2
Prevalence of Alcohol Use DuringPregnancy
An estimated 1% of infants show someprenatal alcohol-related damage.2,3 In
Testing Newborns for Exposure to Alcohol During Pregnancy
The presence of a biomarkerin a newborn baby’smeconium the first bowelmovement may determinewhether a mother drankalcohol during her pregnancy.
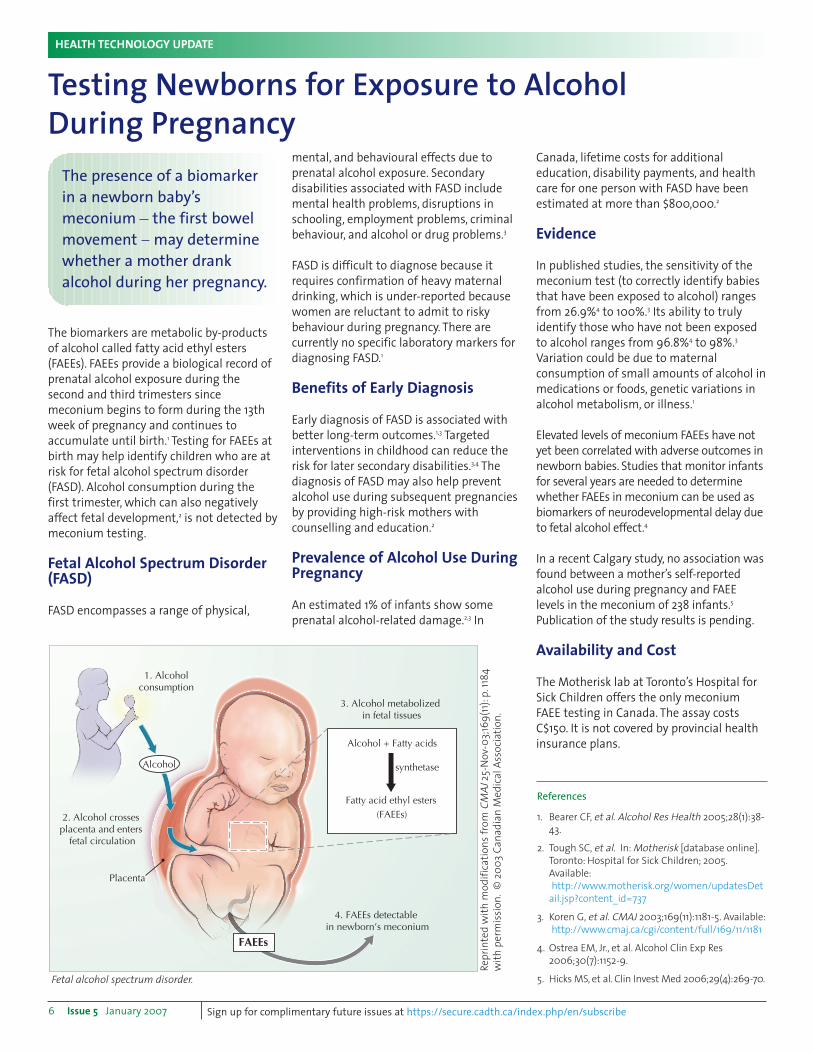
1. Alcoholconsumption
2. Alcohol crosses placenta and enters
fetal circulation
3. Alcohol metabolized in fetal tissues
4. FAEEs detectable in newborn’s meconium
Placenta
Alcohol
FAEEs
(FAEEs)
Alcohol + Fatty acids
Fatty acid ethyl esters
synthetase
Re
pri
nte
d w
ith
mo
dif
ica
tio
ns
fro
m C
MA
J2
5-N
ov-
03;
169
(11)
:p.1
184
wit
h p
erm
issi
on
.©
20
03
Ca
na
dia
n M
ed
ica
l A
sso
cia
tio
n.
Fetal alcohol spectrum disorder.
References
1. Bearer CF, et al. Alcohol Res Health 2005;28(1):38-
43.
2. Tough SC, et al. In: Motherisk [database online].
Toronto: Hospital for Sick Children; 2005.
Available:
<<http://www.motherisk.org/women/updatesDet
ail.jsp?content_id=737>>
3. Koren G, et al. CMAJ 2003;169(11):1181-5. Available:
<<http://www.cmaj.ca/cgi/content/full/169/11/1181>>
4. Ostrea EM, Jr., et al. Alcohol Clin Exp Res
2006;30(7):1152-9.
5. Hicks MS, et al. Clin Invest Med 2006;29(4):269-70.
Sign up for complimentary future issues at https://secure.cadth.ca/index.php/en/subscribe
The biomarkers are metabolic by-productsof alcohol called fatty acid ethyl esters(FAEEs). FAEEs provide a biological record ofprenatal alcohol exposure during thesecond and third trimesters sincemeconium begins to form during the 13thweek of pregnancy and continues toaccumulate until birth.1 Testing for FAEEs atbirth may help identify children who are atrisk for fetal alcohol spectrum disorder(FASD). Alcohol consumption during thefirst trimester, which can also negativelyaffect fetal development,2 is not detected bymeconium testing.
Fetal Alcohol Spectrum Disorder(FASD)
FASD encompasses a range of physical,
Potential Benefits IVR increases clinician efficiency bymonitoring the post-discharge progress ofall patients and separating out those whoneed to speak to a clinician in person.Prompt intervention during recovery athome can avoid re-admission to hospital.
Studies have shown that patients may bewilling to disclose more sensitiveinformation, such as compliance withmedication or alcohol use, during an IVRcall compared to speaking with a humaninterviewer.1
IVR in Canada Although telephone interviews with IVRsystems were developed several yearsago, their application in health care isrelatively new in Canada. Several IVRsystems have been developed by Ottawa-based TelASK Technologies Inc., incollaboration with the University ofOttawa Heart Institute.
Preliminary Evidence An unpublished, randomized controlledfeasibility study, conducted at the OttawaHeart Institute, reported the results ofIVR follow-up to support smokingcessation after patients were hospitalized
for coronary heart disease. Smokingabstinence in the control group was34.7% (17 of 49 patients) compared with46.0% (23 of 50) in the patients whoreceived IVR follow-up calls afterdischarge on days three, 14, and 30.
At the October 2006 CanadianCardiovascular Congress, an Ottawa HeartInstitute researcher reported that IVRfollow-up was effective in the earlyidentification of serious complicationsdeveloping among 1,116 patients recoveringat home following cardiac surgery.
CostAccording to TelASK, developing an IVRapplication costs from C$35,000 toC$50,000, depending on the complexityof the algorithm and the reportingrequired. Ongoing charges of up to C$20per patient cover the costs of placing thecalls, hosting the system in a secureInternet data centre, and providingtraining and support to hospital staff.
Issue 5 January 2007 7
HEALTH TECHNOLOGY UPDATE
Interactive Voice Response System Helps BridgeContinuity of Care Between Hospital and Home
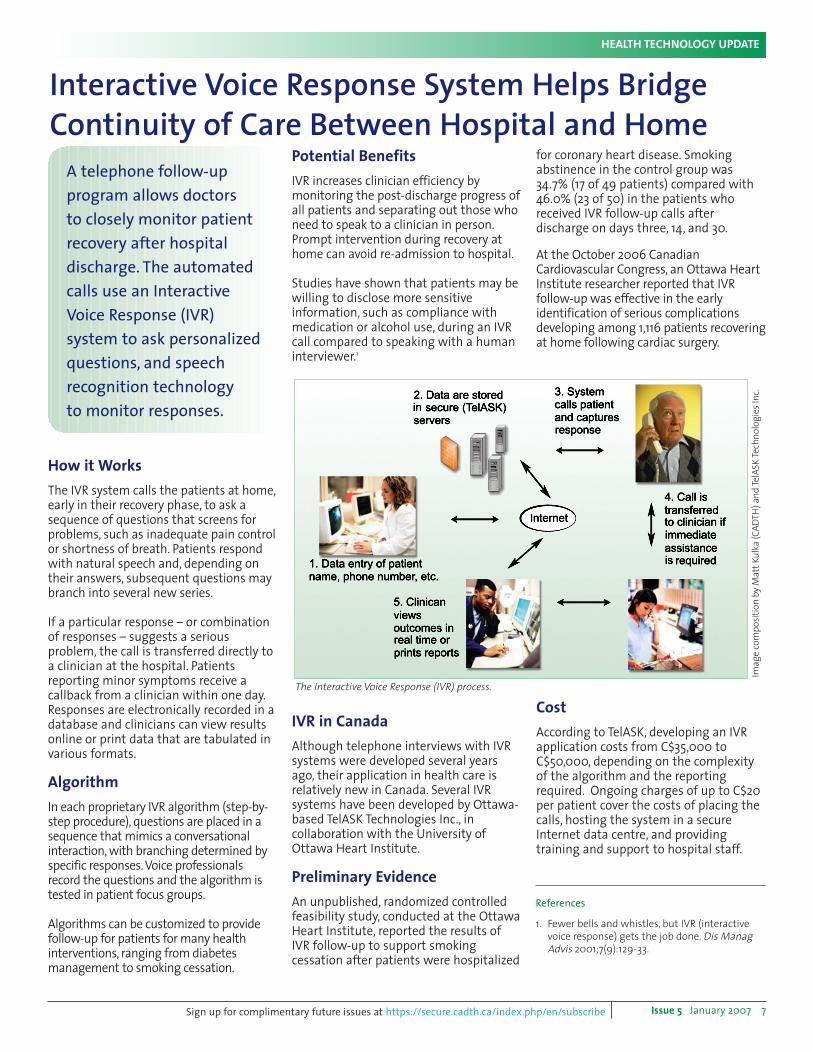
The Interactive Voice Response (IVR) process.
References
1. Fewer bells and whistles, but IVR (interactivevoice response) gets the job done. Dis ManagAdvis 2001;7(9):129-33.
A telephone follow-upprogram allows doctors to closely monitor patientrecovery after hospitaldischarge. The automatedcalls use an InteractiveVoice Response (IVR)system to ask personalizedquestions, and speechrecognition technologyto monitor responses.
Ima
ge
co
mp
osi
tio
n b
y M
att
Ku
lka
(C
AD
TH
) a
nd
Te
lAS
K T
ech
no
log
ies
Inc.
Sign up for complimentary future issues at https://secure.cadth.ca/index.php/en/subscribe
How it WorksThe IVR system calls the patients at home,early in their recovery phase, to ask asequence of questions that screens forproblems, such as inadequate pain controlor shortness of breath. Patients respondwith natural speech and, depending ontheir answers, subsequent questions maybranch into several new series.
If a particular response – or combinationof responses – suggests a seriousproblem, the call is transferred directly toa clinician at the hospital. Patientsreporting minor symptoms receive acallback from a clinician within one day.Responses are electronically recorded in adatabase and clinicians can view resultsonline or print data that are tabulated invarious formats.
Algorithm In each proprietary IVR algorithm (step-by-step procedure), questions are placed in asequence that mimics a conversationalinteraction, with branching determined byspecific responses. Voice professionalsrecord the questions and the algorithm istested in patient focus groups.
Algorithms can be customized to providefollow-up for patients for many healthinterventions, ranging from diabetesmanagement to smoking cessation.
HEALTH TECHNOLOGY UPDATE
Production Notes
Health Technology Update is published by:
Canadian Agency for Drugs and Technologies in Health (CADTH)600-865 Carling Ave.Ottawa, ON Canada K1S 5S8
Tel: (613) 226-2553Fax: (613) 226-5392Web site: www.cadth.ca
Editor/Writer: Catherine AllisonContributing Writers: William Freeland, DavidHailey, Leigh-Ann TopferInformation Specialists: Michelle Fiander, HayleyFitzsimmons, Shaila Mensinkai, Andra MorrisonCopy Editor: Kinneret GlobermanLayout and Design: Matt Kulka, Nathalie Charron Web Designers: Martha Hodgson-Oram, Paul Ting
This newsletter is available free of charge, in bothEnglish and French. Readers may subscribe toreceive e-mail notification of new issues usingthe subscription link on the CADTH web site orthe following URL:<<https://secure.cadth.ca/index.php/en/subscribe>>
Reproduction of this document for non-commercial purposes is permitted provided appropriate credit is given to CADTH.
Health Technology Update is an informationsource for those involved in planning andproviding health care in Canada. The informationincluded in this newsletter is based on a limitedliterature review and should not be construed asa recommendation for or against the use of aparticular health technology. Readers are alsocautioned that a lack of good quality evidence tosupport effectiveness does not necessarily meana lack of effectiveness, particularly in the case ofnew and emerging technologies.
Production of this newsletter is made possible bya financial contribution from Health Canada’sHealth Care Strategies and Policy, federal,provincial and territorial partnership grantprogram. CADTH takes sole responsibility for thefinal form and content of this newsletter. Thestatements, conclusions and views expressedherein do not necessarily represent the view ofHealth Canada or any provincial or territorialgovernment.
© 2007 Canadian Agency for Drugs andTechnologies in HealthISSN: 1715-5541 (print) • ISSN: 1715-555X (online)
Printed in English
New and Emerging HealthTechnology ReportsRecent Reports from CADTH and Other HTA Agencies
� Intra-articular hyaluronic acid(viscosupplementation) for kneeosteoarthritis
Available:<<http://www.cadth.ca/media/pdf/E0010_viscosupplementation_cetap_e.pdf>>
Ontario Medical Advisory Secretariat(MAS)� Energy delivery systems for treatmentof benign prostatic hyperplasia
Available:<<http://www.health.gov.on.ca/english/providers/program/mas/tech/reviews/pdf/rev_bph_081806.pdf>>
� Gastric electrical stimulation
Available:<<http://www.health.gov.on.ca/english/providers/program/mas/tech/reviews/pdf/rev_ges_081806.pdf>>
� Negative pressure wound therapy
Available:<<http://www.health.gov.on.ca/english/providers/program/mas/tech/reviews/pdf/rev_npwt_070106.pdf>>
US California Technology AssessmentForum (CTAF)� An interspinous process distractor(X Stop) for the treatment of spinal stenosisof the lumbar spine
Available:<<http://www.ctaf.org/content/assessments_pdf/82151206101_XSTOP0606.pdf;jsessionid=3C7B8118D138F067D1855CF9E44FEFC7>>
� Brachytherapy for accelerated partialbreast irradiation following conservingsurgery
Available:<<http://www.ctaf.org/content/assessments_pdf/82151206100_Brachytherapy0606.pdf;jsessionid=3C7B8118D138F067D1855CF9E44FEFC7>>
These reports are available without costat the web sites shown below:
Australia and New Zealand HorizonScanning Network (ANZHSN)� Primer and probe set for the diagnosisof avian influenza
Available:<<http://www.health.gov.au/internet/horizon/publishing.nsf/Content/8F86C8B4D8513895CA25715C0005D972/$File/Primer%20and%20probe%20set%20of%20avian%20influenza%20Vol%2014%20No%201%20Sept2006.pdf>>
� Nicotine metabolite ratio test as apredictor of smoking cessation
Available:<<http://www.health.gov.au/internet/horizon/publishing.nsf/Content/8F86C8B4D8513895CA25715C0005D972/$File/Nicotine%20metabolite%20Vol%2014%20No%204%20Sept2006.pdf>>
Canadian Agency for Drugs andTechnologies in Health (CADTH)� Transient elastography (FibroScan) fornon-invasive assessment of liver fibrosis
Available:<<http://www.cadth.ca/media/pdf/442_fibroscan_cetap_e.pdf>>
� Digital mammography: an update
Available:<<http://www.cadth.ca/media/pdf/444_digital_mammography_cetap_e.pdf>>
� Open magnetic resonance imaging(MRI) scanners
Available:<<http://www.cadth.ca/media/pdf/E0011_MRIScanners_cetap_e.pdf>>
� “Hot” techniques for tonsillectomy
Available:<<http://www.cadth.ca/media/pdf/E0003_tonsillectomy_cetap_e.pdf>>
Supporting informed decisions . . . www.cadth.ca







