ecare clinical protocols - overview dorset v1 · twinfield spark r full (md -1.2, psd 0.4, ght wnl)...
TRANSCRIPT
eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
1 | P a g e 1 | P a g e
Business Unit Head Office Location The Dairy, Stonor Park, Stonor, Henley-on-Thames, Oxon, RG9 6HF Completed By Christian Dutton
Business Unit Head Sign Off Peter Price-Taylor Date 28/03/2018 Review Date 19/05/2018 Version 1.2
eCare Clinical Protocols - Overview March 2018
eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
2 | P a g e 2 | P a g e
Overview We have included a selection of clinical protocols for the benefit of prospective service providers. These protocols have been extracted from the eCare Affiliate handbook and DO NOT FORM A STANDALONE DOCUMENT; they are indicative of the clinical investigations to be undertaken. Affiliates must use these protocols in conjunction with the Affiliate handbook in its entirety. There are 2 main pathway tiers:
1. Optometry led pathways (ESO-IOP/fields, Anterior ESO, Posterior ESO) 2. Ophthalmology-led pathways, delivered either by an ophthalmologist or optometrist (Telemedicine Primary
Assessment Service, glaucoma sub-protocol, AMD sub-protocol) Following feedback from our engagement events, the service commissioned in Dorset will be separated into ESO and telemedicine pathways from 1st April. As discussed, we take a pragmatic approach to the evolution of the service and our experience in other CCGs has shown the benefits of having optometry pathways in addition to the telemedicine pathway. Dorset clinicians will therefore have the autonomy to manage a broader range of suitable patients without telemedicine oversight. Telemedicine will be mandated for the glaucoma pathway and available in cases of uncertainty. Nevertheless, all outcome decisions are still audited by our senior clinical team/ophthalmologist panel to ensure appropriate clinical decisions are being made by our provider network. The eCare Affiliate handbook is a cross-CCG document. Please note that within Dorset the service can only accept those conditions specified in the inclusion criteria (attached) and the CCG-specific time to care requirements will supersede the content of this generic handbook.
eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
3 | P a g e 3 | P a g e
IOP/Field Repeat Enhanced Service Optometry (ESO) Pathway Clinical Appointment Test Protocol The level of examination should be appropriate to the reason for referral and all procedures are at the discretion of the clinician, however this pathway examination protocol is the recommended safe minimum level. Follow-up appointments should include investigations which are appropriate to the condition under review. History and symptoms
• Specific questions relevant to the presenting condition • Personal medical history (including medications) • Personal ocular history • Family ocular history
Anterior segment
• Slit-lamp examination o Cornea, iris, lens
• Anterior chamber angle examination • Intra-ocular pressure (IOP)
o Contact applanation tonometry and time (Goldmann Applanation Tonometry is the gold standard)
Visual fields
• Full threshold test (SITA, ZATA and other algorithms acceptable) Visit Outcomes Allowable outcomes resulting from the consultation are:
• Discharge and self-monitoring • Follow-up and monitor • Onward referral to another pathway
In ALL cases, patient information should be provided to aid and support early detection and prevention planning through:
• Written guidance as appropriate (e.g. College of Optometrists leaflet) o Education about disease prognosis o Discussion of lifestyle changes o Information detailing available support/rehabilitation services o Advice to return/seek advice (with appropriate urgency) if new symptoms develop
• Home monitoring Consideration should be given to the Joint College’s advice and NICE Guidelines.

eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
4 | P a g e 4 | P a g e
Anterior Enhanced Service Optometry (ESO) Pathway Clinical Appointment Test Protocol The level of examination should be appropriate to the reason for referral and all procedures are at the discretion of the clinician, however this pathway examination protocol is the recommended safe minimum level. Follow-up appointments should include investigations which are appropriate to the condition under review. History and symptoms
• Specific questions relevant to the presenting condition • Personal medical history (including medications) • Family medical history • Personal ocular history • Family ocular history
Examination
• Visual acuity (distance and near) with refraction where indicated • Ocular motility • Pupil reactions • Intra-ocular pressure (IOP)
o Contact applanation tonometry and time (Goldmann Applanation tonometry is the gold standard) • Slit-lamp examination -
o Lids, lashes, conjunctiva (bulbar and palpebral), sclera, cornea, limbus, anterior chamber, iris, lens o Discharge, tear film, fluorescein staining
• Anterior chamber angle examination Where indicated, a dilated slit-lamp bio-microscopic examination should be undertaken.
eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
5 | P a g e 5 | P a g e
Posterior Enhanced Service Optometry (ESO) Pathway Clinical Appointment Test Protocol The level of examination should be appropriate to the reason for referral and all procedures are at the discretion of the clinician, however this pathway examination protocol is the recommended safe minimum level. Follow-up appointments should include investigations which are appropriate to the condition under review. History and symptoms
• Specific questions relevant to the presenting condition • Personal medical history (including medications) • Family medical history • Personal ocular history • Family ocular history
Pre-dilation
• Visual acuity (distance and near) with refraction where indicated • Visual fields • Monocular colour vision where indicated • Amsler where indicated • Pupil reactions • Intra-ocular pressure (IOP)
o Contact applanation tonometry and time Anterior segment
• Slit-lamp examination o Lids, lashes, conjunctiva (bulbar and palpebral), sclera, cornea, limbus, iris, lens
• Anterior chamber angle examination
Posterior segment • Dilated slit lamp binocular indirect ophthalmoscopy (SL-BIO)
o Vitreous, retina, macula, disc (C:D, size and features), choroid • Fundus imaging • Post-dilation IOP review as appropriate
eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
6 | P a g e 6 | P a g e
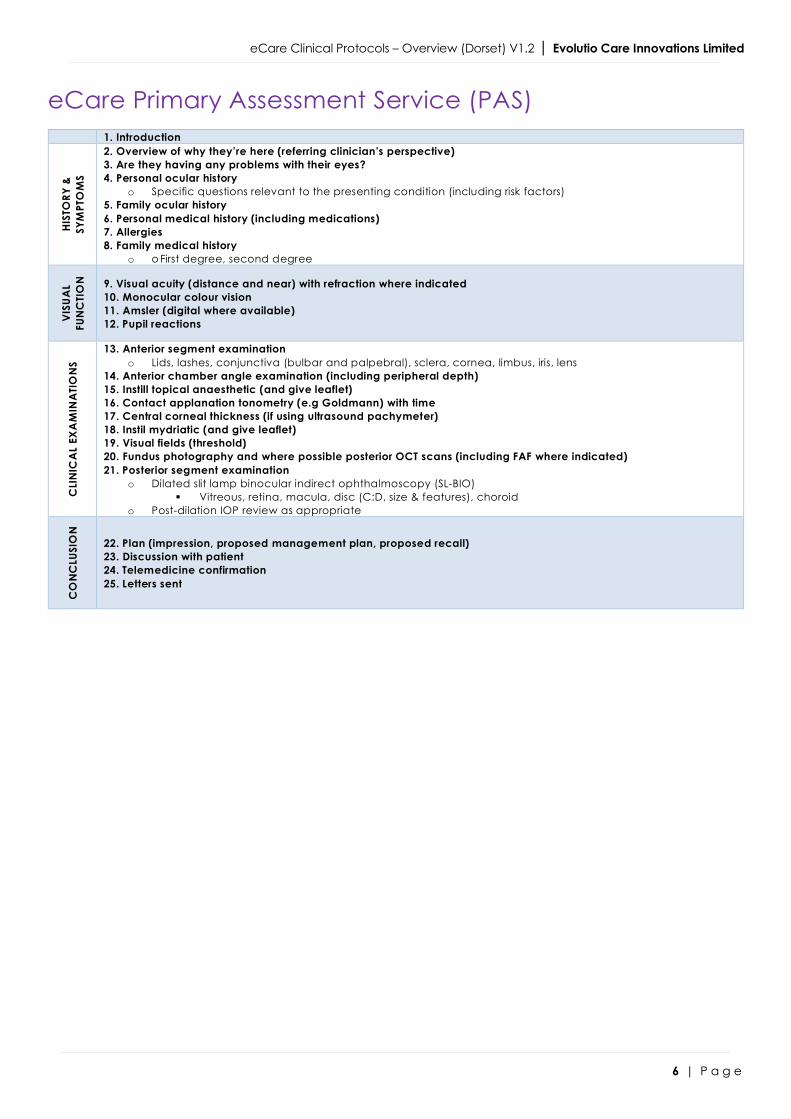
eCare Primary Assessment Service (PAS)
1. Introduction
HIST
ORY
&
SYM
PTO
MS
2. Overview of why they’re here (referring clinician’s perspective) 3. Are they having any problems with their eyes? 4. Personal ocular history
o Specific questions relevant to the presenting condition (including risk factors) 5. Family ocular history 6. Personal medical history (including medications) 7. Allergies 8. Family medical history
o o First degree, second degree
VIS
UAL
FUN
CTI
ON
9. Visual acuity (distance and near) with refraction where indicated 10. Monocular colour vision 11. Amsler (digital where available) 12. Pupil reactions
CLI
NIC
AL
EXA
MIN
ATI
ON
S
13. Anterior segment examination o Lids, lashes, conjunctiva (bulbar and palpebral), sclera, cornea, limbus, iris, lens
14. Anterior chamber angle examination (including peripheral depth) 15. Instill topical anaesthetic (and give leaflet) 16. Contact applanation tonometry (e.g Goldmann) with time 17. Central corneal thickness (if using ultrasound pachymeter) 18. Instil mydriatic (and give leaflet) 19. Visual fields (threshold) 20. Fundus photography and where possible posterior OCT scans (including FAF where indicated) 21. Posterior segment examination
o Dilated slit lamp binocular indirect ophthalmoscopy (SL-BIO) § Vitreous, retina, macula, disc (C:D, size & features), choroid
o Post-dilation IOP review as appropriate
CO
NC
LUSI
ON
22. Plan (impression, proposed management plan, proposed recall) 23. Discussion with patient 24. Telemedicine confirmation 25. Letters sent
eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
7 | P a g e 7 | P a g e
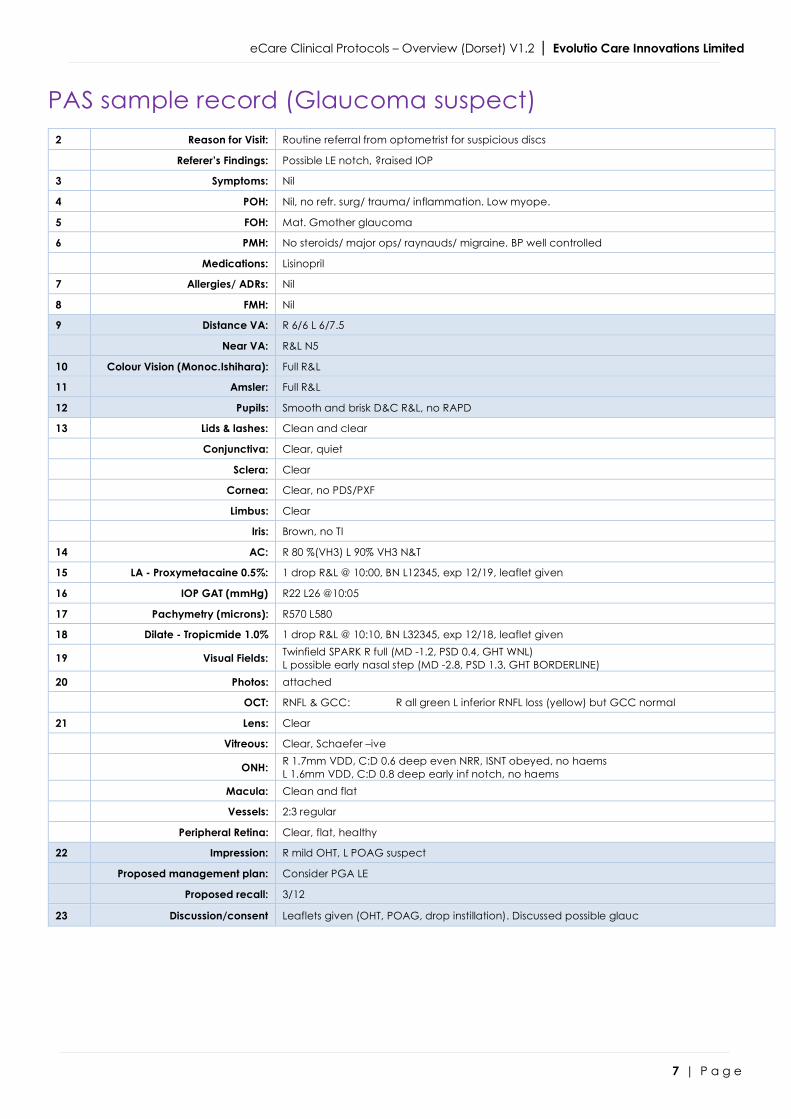
PAS sample record (Glaucoma suspect)
2 Reason for Visit: Routine referral from optometrist for suspicious discs
Referer’s Findings: Possible LE notch, ?raised IOP
3 Symptoms: Nil
4 POH: Nil, no refr. surg/ trauma/ inflammation. Low myope.
5 FOH: Mat. Gmother glaucoma
6 PMH: No steroids/ major ops/ raynauds/ migraine. BP well controlled
Medications: Lisinopril
7 Allergies/ ADRs: Nil
8 FMH: Nil
9 Distance VA: R 6/6 L 6/7.5
Near VA: R&L N5
10 Colour Vision (Monoc.Ishihara): Full R&L
11 Amsler: Full R&L
12 Pupils: Smooth and brisk D&C R&L, no RAPD
13 Lids & lashes: Clean and clear
Conjunctiva: Clear, quiet
Sclera: Clear
Cornea: Clear, no PDS/PXF
Limbus: Clear
Iris: Brown, no TI
14 AC: R 80 %(VH3) L 90% VH3 N&T
15 LA - Proxymetacaine 0.5%: 1 drop R&L @ 10:00, BN L12345, exp 12/19, leaflet given
16 IOP GAT (mmHg) R22 L26 @10:05
17 Pachymetry (microns): R570 L580
18 Dilate - Tropicmide 1.0% 1 drop R&L @ 10:10, BN L32345, exp 12/18, leaflet given
19 Visual Fields: Twinfield SPARK R full (MD -1.2, PSD 0.4, GHT WNL) L possible early nasal step (MD -2.8, PSD 1.3, GHT BORDERLINE)
20 Photos: attached
OCT: RNFL & GCC: R all green L inferior RNFL loss (yellow) but GCC normal
21 Lens: Clear
Vitreous: Clear, Schaefer –ive
ONH: R 1.7mm VDD, C:D 0.6 deep even NRR, ISNT obeyed, no haems L 1.6mm VDD, C:D 0.8 deep early inf notch, no haems
Macula: Clean and flat
Vessels: 2:3 regular
Peripheral Retina: Clear, flat, healthy
22 Impression: R mild OHT, L POAG suspect
Proposed management plan: Consider PGA LE
Proposed recall: 3/12
23 Discussion/consent Leaflets given (OHT, POAG, drop instillation). Discussed possible glauc
eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
8 | P a g e 8 | P a g e
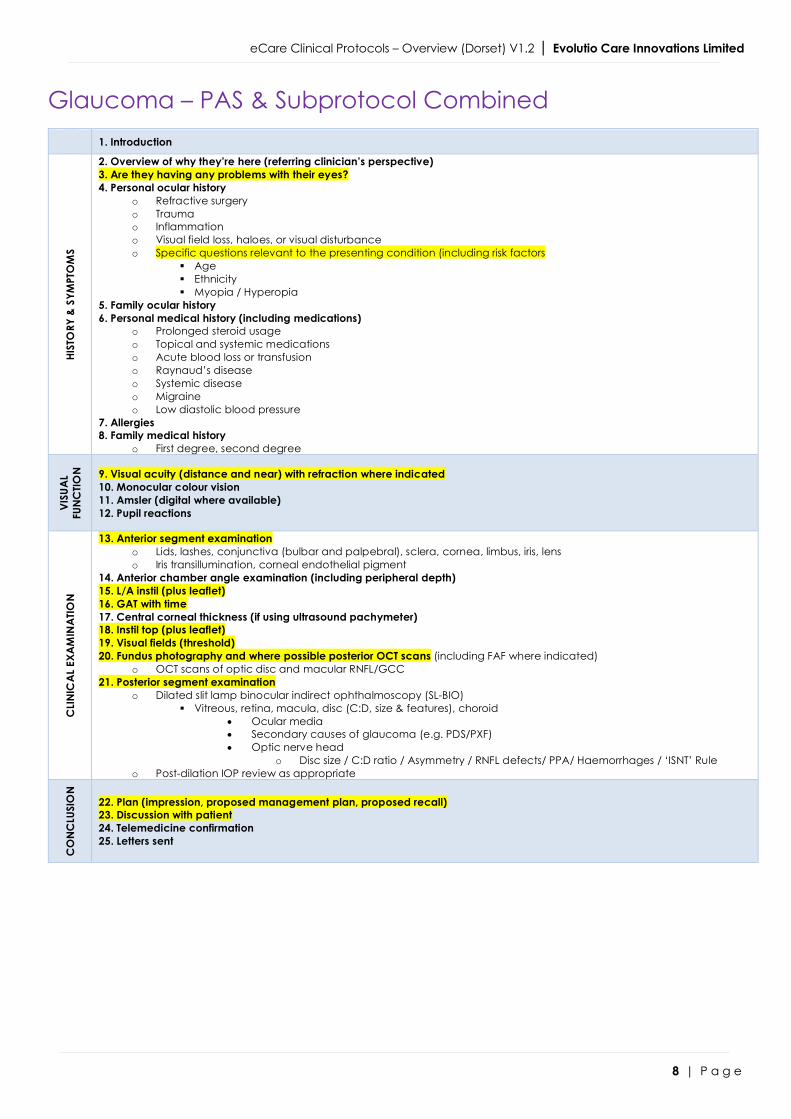
Glaucoma – PAS & Subprotocol Combined
1. Introduction
HIST
ORY
& S
YMPT
OM
S
2. Overview of why they’re here (referring clinician’s perspective) 3. Are they having any problems with their eyes? 4. Personal ocular history
o Refractive surgery o Trauma o Inflammation o Visual field loss, haloes, or visual disturbance o Specific questions relevant to the presenting condition (including risk factors
§ Age § Ethnicity § Myopia / Hyperopia
5. Family ocular history 6. Personal medical history (including medications)
o Prolonged steroid usage o Topical and systemic medications o Acute blood loss or transfusion o Raynaud’s disease o Systemic disease o Migraine o Low diastolic blood pressure
7. Allergies 8. Family medical history
o First degree, second degree
VISU
AL
FUN
CTIO
N
9. Visual acuity (distance and near) with refraction where indicated 10. Monocular colour vision 11. Amsler (digital where available) 12. Pupil reactions
CLI
NIC
AL
EXA
MIN
ATIO
N
13. Anterior segment examination o Lids, lashes, conjunctiva (bulbar and palpebral), sclera, cornea, limbus, iris, lens o Iris transillumination, corneal endothelial pigment
14. Anterior chamber angle examination (including peripheral depth) 15. L/A instil (plus leaflet) 16. GAT with time 17. Central corneal thickness (if using ultrasound pachymeter) 18. Instil top (plus leaflet) 19. Visual fields (threshold) 20. Fundus photography and where possible posterior OCT scans (including FAF where indicated)
o OCT scans of optic disc and macular RNFL/GCC 21. Posterior segment examination
o Dilated slit lamp binocular indirect ophthalmoscopy (SL-BIO) § Vitreous, retina, macula, disc (C:D, size & features), choroid
• Ocular media • Secondary causes of glaucoma (e.g. PDS/PXF) • Optic nerve head
o Disc size / C:D ratio / Asymmetry / RNFL defects/ PPA/ Haemorrhages / ‘ISNT’ Rule o Post-dilation IOP review as appropriate
CO
NC
LUSI
ON
22. Plan (impression, proposed management plan, proposed recall) 23. Discussion with patient 24. Telemedicine confirmation 25. Letters sent

eCare Clinical Protocols – Overview (Dorset) V1.2 | Evolutio Care Innovations Limited
9 | P a g e 9 | P a g e
Maculopathy – PAS & Subprotocol Combined
1. Introduction
HIST
ORY
& S
YMPT
OM
S
2. Overview of why they’re here (referring clinician’s perspective) 3. Are they having any problems with their eyes? 4. Personal ocular history
o Retinal vascular disease o Ocular inflammatory disease o Trauma o Intraocular surgery o Refractive error, including change o Specific questions relevant to the presenting condition (including risk factors
§ Social history • Smoking • Alcohol consumption • Stress
§ Symptoms: • Metamorphopsia, micropsia, macropsia, diplopia, aniseikonia • Reduced visual acuity • Central scotoma • Charles Bonnet syndrome (CBS)
5. Family ocular history 6. Personal medical history (including medications)
o Hypertension o Diabetes mellitus o Ischaemic heart disease o Steroids o Anti-coagulant therapy o Nutritional supplements
7. Allergies 8. Family medical history
o First degree, second degree
VISU
AL
FUN
CTIO
N
9. Visual acuity (distance and near) with refraction where indicated 10. Monocular colour vision 11. Amsler (digital where available) 12. Pupil reactions
CLI
NIC
AL
EXA
MIN
ATIO
N
13. Anterior segment examination o Lids, lashes, conjunctiva (bulbar and palpebral), sclera, cornea, limbus, iris, lens
14. Anterior chamber angle examination (including peripheral depth) 15. L/A instil (plus leaflet) 16. GAT with time 17. Central corneal thickness (if using ultrasound pachymeter) 18. Instil top (plus leaflet) 19. Visual fields (threshold) 20. Fundus photography and where possible posterior OCT scans (including FAF where indicated)
o Macular OCT scans (including FAF), with attention to: § Sub-retinal/sub-RPE neovascularisation § Serous detachment of the neurosensory retina § RPE detachment § Haemorrhages and/or oedema:
• Sub-RPE • Sub-retinal • Intra-retinal • Pre-retinal • Breakthrough bleeding into the vitreous
§ Exudates (unrelated to other retinal disease) § Retinal angiomatous proliferations (RAP) and retinochoroidal anastomoses
o Vitreomacular traction and ERM 21. Posterior segment examination
o Dilated slit lamp binocular indirect ophthalmoscopy (SL-BIO) § Vitreous, retina, macula, disc (C:D, size & features), choroid, media
o Post-dilation IOP review as appropriate
CO
NC
LUSI
ON
22. Plan (impression, proposed management plan, proposed recall) 23. Discussion with patient 24. Telemedicine confirmation 25. Letters sent