evolving treatment paradigm for patients with...
TRANSCRIPT
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
Go online to complete the post-test and earn your CME credit!
www.peercme.com/ACC900
Matthew Smith, MD, PhDHarvard Medical SchoolMassachusetts General HospitalBoston, Massachusetts, USA
An Evidentiary Review of Emerging Androgen Receptor Pathway Inhibitors
Karim Fizazi, MD, PhDGustave Roussy Cancer Institute Villejuif, France
The Treatment Plan for Patients With Advanced Prostate Cancer: Where Do Androgen Receptor Pathway Inhibitors Belong?

2
Funding DisclosureThis activity is supported by an educational grant from Bayer HealthCare Pharmaceuticals.
Activity Description and Educational ObjectivesIn this activity, experts in the management of prostate cancer discuss sequencing strategies with current and emerging androgen receptor pathway inhibitors (ARPIs) in order to maximise patients’ survival and quality of life.
Upon completion of this activity, participants should be better able to:• Identify patient- and disease-related factors that may affect treatment decisions
and response to therapy with androgen receptor pathway inhibitors (ARPIs)• Describe how current treatment plans may change for patients with advanced
prostate cancer, given the recent and emerging clinical trial data• Explain the similarities and differences between current and emerging ARPIs
Target AudienceThis activity has been designed to meet the educational needs of medical oncologists, urologists, and other clinicians involved in prostate cancer management.
Faculty Disclosure Statement / Conflict of Interest PolicyOakstone Publishing, LLC has assessed conflict of interest with its faculty, authors, editors, and any individuals who were in a position to control the content of this CME activity. Any identified relevant conflicts of interest were resolved for fair balance and scientific objectivity of studies utilized in this activity. Oakstone Publishing’s planners, medical reviewers, and editorial staff disclose no relevant financial relationships with commercial interests.
Course DirectorKarim Fizazi, MD, PhDHead of Department, Department of Cancer Medicine Gustave Roussy Cancer Institute Villejuif, France
Karim Fizazi, MD, PhD, has a financial interest/relationship or affiliation in the form of:Honoraria from Astellas Pharma EMEA; Janssen-Cilag Pharmaceuticals SA; and Sanofi. Advisory Board for Astellas Pharma EMEA; Bayer AG; Clovis Oncology, Inc.; ESSA Pharma, Inc.; Genentech, Inc; Janssen-Cilag Pharmaceuticals SA; Orion Corporation; and Sanofi.
FacultyMatthew Smith, MD, PhDProfessor of Medicine Harvard Medical School Director, Genitourinary Malignancies Program Massachusetts General Hospital Boston, Massachusetts, USA
Matthew Smith, MD, PhD, has a financial interest/relationship or affiliation in the form of:Consultant for Amgen Inc; Bayer AG; ESSA Pharma Inc.; Janssen-Cilag Pharmaceuticals SA; and Pfizer Inc. Advisory Board for Amgen Inc; Bayer AG; ESSA Pharma Inc.; Janssen-Cilag Pharmaceuticals SA; and Pfizer Inc.
PeerVoice Medical DirectorSerena Welch has no financial interests/relationships or affiliations in relation to this activity.
Disclosure of Unlabelled UseThe faculty of this educational activity may include discussions of products or devices that are not currently labelled for use in certain jurisdictions. Faculty members have been advised to disclose to the audience any reference to an unlabelled or investigational use.
No endorsement of unapproved products or uses is made or implied by coverage of these products or uses in our materials. No responsibility is taken for errors or omissions in our materials.
Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
AccreditationThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Oakstone Publishing, LLC and PeerVoice. Oakstone Publishing, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Oakstone Publishing, LLC designates this enduring material for a maximum of 0.5 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
The European Union of Medical Specialists (UEMS)-European Accreditation Council for Continuing Medical Education (EACCME) has an agreement of mutual recognition of continuing medical education (CME) credit with the American Medical Association (AMA). European physicians interested in converting AMA PRA Category 1 CreditTM into European CME credit (ECMEC) should contact the UEMS (www.uems.eu).
This CME activity is jointly provided by Oakstone Publishing, LLC and PeerVoice.
Requirements for Successful CompletionTo receive credit, participants must complete the activity, the post-test, and the evaluation form prior to the expiration date noted below. There are no pre-requisites and there is no fee to participate in this activity or to receive credit. Statements of Credit are awarded upon successful completion of the post-test and evaluation form. Consult your professional licensing board for information about your eligibility to claim credit for participation in this educational activity. A minimum performance level of 70% is needed.
Media: Enduring MaterialRelease and Expiration Dates: May 8, 2017 - May 7, 2018Time to Complete: 30 minutes
DisclaimerThe participants of this educational activity have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patients' conditions and possible contraindications on dangers in use, review of any applicable manufacturer's product information, and comparison with recommendations of other authorities.
The materials presented here are used with the permission of the authors and/or other sources. These materials do not necessarily reflect the views of PeerVoice or any of its supporters.
CME Details
www.peercme.com/ACC900

3
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
Karim Fizazi, MD, PhDGustave Roussy Cancer Institute Villejuif, France
The Treatment Plan for Patients With Advanced Prostate Cancer: Where Do Androgen Receptor Pathway Inhibitors Belong?
Castration-Naïve PC CRPC
M0
M1
M0
M1 1st Line
M1 2nd Line
M1 3rd Line
ADT
ADT
Management of patients with non-metastatic (M0) CRPC
Conceptual Framework for the Management of AdvancedProstate Cancer (St Gallen APCCC)
Abbreviation(s): ADT: androgen-deprivation therapy; APCCC: Advanced Prostate Cancer Consensus Conference; CRPC: castration-resistant prostate cancer (PC); M0: no evidence of metastases on imaging; M1: metastases documented on imaging.Reference(s): Gillessen S et al. Ann Oncol. 2015;26:1589-1604.
Karim Fizazi, MD, PhD: Hello, this is Karim Fizazi from Institut Gustave Roussy in Villejuif, France. Welcome to this educational activity on treatment of advanced prostate cancer. We're going to review what is the current role of androgen receptor pathway inhibitors in the treatment sequence; and also, we'll look at how this role may evolve in the near future.
So, this slide is derived from the St Gallen Consensus Meeting in 2015, and it's really showing you the framework for advanced prostate cancer. So some patients have non-metastatic disease, but we already know that they have advanced disease because the disease has become resistant to castration, which is M0 CRPC; while some other patients are entering the disease upfront with evidence of metastasis—what we call M1 castration-naïve prostate cancer.
Whatever the pathway, the disease evolves to metastatic castration-resistant disease (mCRPC), and we are talking about first-line, second-line, third-line, etc, CRPC treatments.
a COU-AA-301 study design: Phase 3 double-blind trial wherein patients (N = 1,195) were randomised to receive either abiraterone acetate+ prednisone (n = 797) or placebo + prednisone (n = 398).1
b AFFIRM study design: Phase 3 double-blind trial wherein patients (N = 1,199) were randomised to receive either enzalutamide (n = 800)or placebo (n = 399).2
Data are from multiple trials and cannot be directly compared.
COU-AA-301: Abiraterone/Preda,1 AFFIRM: Enzalutamideb,2
OS
, %
Time, mo
HR, 0.74 (95% CI, 0.64-0.86)P < .0001
PBO + Pred
ABI + Pred
100
80
60
40
20
00 6 12 18 3024
Time, mo
OS
, %
HR, 0.63 (95% CI, 0.53-0.75)P < .001
PBO
ENZA
100
80
60
40
20
00 6 12 18 24
Ef�cacy Associated With Approved ARPIs Abiraterone andEnzalutamide for mCRPC (Post-Docetaxel)
Abbreviation(s): ABI: abiraterone acetate; ARPI: androgen receptor pathway inhibitor; ENZA: enzalutamide; mCRPC: metastatic CRPC; OS: overall survival; PBO: placebo; Pred: prednisone.Reference(s): 1. Fizazi K et al; COU-AA-301 Investigators. Lancet Oncol. 2012;13:983-992.2. Scher HI et al; AFFIRM Investigators. N Engl J Med. 2012;367:1187-1197.
Abiraterone and enzalutamide are the two approved androgen receptor pathway inhibitors that showed efficacy in large phase 3 trials. This is, for example, the COU-301 and AFFIRM randomised phase 3 trials, respectively, showing that approximately a 30% reduction in the risk of death can be achieved when using these agents in the post-docetaxel setting.

4
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
a Seizure occurred in 0.5% of patients treated with enzalutamide; 0.1% of patients treated with placebo; and 0.3% of patients treatedwith bicalutamide.
Summary of Safety Profile forAbiraterone1
Most Common AEs• Peripheral oedema• Hypokalaemia• Hypertension• Urinary tract infection
Other Important AEs• Cardiac disorders• Hepatotoxicity• Fractures• Allergic alveolitis
Summary of Safety Profile forEnzalutamide2
Most Common AEs• Fatigue• Hot �ush• Headache• Hypertension
Other Important AEs• Falls• Fractures• Cognitive disorders• Neutropenia• Seizurea
Safety Associated With Approved ARPIs Abiraterone andEnzalutamide for mCRPC
Abbreviation(s): AE: adverse event.Reference(s): 1. Abiraterone acetate Summary of Product Characteristics (SmPC). http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002321/WC500112858.pdf. Accesed April 6, 2017.2. Enzalutade SmPC. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002639/WC500144996.pdf. Accessed April 6, 2017.
Let's briefly review what is the safety pattern of these agents. Hypertension and a slight excess of cardiac disorders were seen in patients treated with abiraterone.
Now, fatigue and cognitive impairment emerge as side effects that are linked to enzalutamide use. This might be related to the fact that enzalutamide penetrates the blood-brain barrier. This agent is associated with a risk of seizure, and this is, of course, something, again, to pay attention to. We need to question the patient about seizures. Finally, again, we need to pay attention to hypertension and generally speaking, cardiac events. When considering treating your patients with these agents, you really need to ask the patient whether he has a previous history of cardiac disorders and perhaps you need to refer him to the cardiologist before starting treatment.
Also, because these treatments are generally well tolerated, they are now used [as approved] more and more in patients who are chemotherapy-naïve.
Schrader et al 2013 35 4.9 mo 29% -
Badrising et al 2014 61 3.0 mo 21% -
Bianchini et al 2014 39 2.9 mo 23% -
Schmid et al 2014 35 2.8 mo 10% -
Brasso et al 2014 137 3.2 mo 18% -
Enzalutamide Abiraterone
Enzalutamide Abiraterone
Author N Duration of Second Therapy â PSA ≥50% Median PFS
Author N Duration of Second Therapy â PSA ≥50% Median PFS
Loriot et al 2013 38 3.0 mo 3% 2.7 mo
Noonan et al 2013 30 13.0 wk 3% 3.8 mo
Cross-Resistance Between Approved ARPIs Abiraterone and Enzalutamide
Abbreviation(s): PFS: progression-free survival; PSA: prostate-specific antigen.Reference(s): Zhang T et al. Expert Opin Pharmacother. 2015;16:473-485.
Unfortunately, cross-resistance between the two agents is quite high. If you're using enzalutamide after abiraterone, perhaps a slightly higher proportion of patients will benefit, but generally speaking, this is probably not the best sequence to consider, at least for most patients.
a COU-AA-301 post-hoc analysis: Assessment of clinical responses to DOC as �rst subsequent therapy among patients (N = 100) whoprogressed following protocol-speci�ed treatment with abiraterone. Median duration of DOC was 4.2 months.1
b Study design: Antitumour activity of cabazitaxel assessed in patients with mCRPC and progressive disease after treatment with DOCand abiraterone (N = 79). Median duration of cabazitaxel was 6 cycles.2
Docetaxela,1Abiraterone
Median TTPa of 7.6 mo
40% of patients with â PSA ≥50%a
Abiraterone Docetaxel Cabazitaxelb,2
Median TTPb of 4.4 mo
35% of patients with â PSA ≥50%b
Ef�cacy Associated With Chemotherapy Post-Abiraterone for mCRPC
Abbreviation(s): DOC: docetaxel; TTP: time to progression.Reference(s): 1. de Bono JS et al. Eur Urol. 2017;71:656-664.2. Al Nakouzi N et al. Eur Urol. 2015;68:228-235.
On the other hand, most patients receiving docetaxel when they have failed abiraterone seem to benefit. So, even if there is perhaps some cross-resistance between the two drugs, it's probably not as high as the cross-resistance between abiraterone and enzalutamide.
This is also true when treating patients with cabazitaxel when they have failed abiraterone—and actually in this experience, they had also failed docetaxel. So obviously, if the patient is fit enough to get chemotherapy, most patients will actually derive some benefit.

5
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
Evolving role of ARPIs for advanced prostate cancer
Metastatic CSPC• LATITUDE• STAMPEDE• ARASENS
M0 CRPC• ARAMIS• SPARTAN• PROSPER
Combination with alternativemCRPC treatments• NCT01949337• NCT02257736
The Evolving Role of ARPI Therapy for Advanced Prostate Cancer
Abbreviation(s): CSPC: castration-sensitive prostate cancer.
Now let's talk about where the use of these ARPI agents is heading. One obviously is to use them upfront, so earlier in the course of the disease. For example, in patients with castration-sensitive or castration-naïve metastatic disease—so patients who are just entering this disease with evidence of metastasis.
A second potential indication in the near future might be non-metastatic CRPC [M0 CRPC]—so patients with nondetectable lesions that are progressing while on castration therapy.
Finally, the third strategy might be to combine these drugs, either together, or with other agents.
ExperimentalArm
ControlArm
Clinical TrialIdentifier (Study Name)
Clinical State PriorChemotherapy
ABI + ADT +Pred
ADT NCT01715285(LATITUDE)1 • Visceral mets
• ≥3 Bone mets• Gleason score ≥8
mCSPC with 2 ofthe following:
No
ABI + ADT ADT NCT00268476(STAMPEDE)2 mCSPC No
Metastatic CSPC: Phase 3 Studies With Abiraterone
Abbreviation(s): mets: metastases; mCSPC: metastatic CSPC.Reference(s): 1. ClinicalTrials.gov Identifier: NCT01715285. https://clinicaltrials.gov/ct2/show/NCT01715285. Accessed March 30, 2017.2. ClinicalTrials.gov Identifier: NCT00268476. https://clinicaltrials.gov/ct2/show/NCT00268476. Accessed March 30, 2017.
For patients with newly diagnosed metastatic prostate cancer, who are just about to start castration therapy, we are waiting for data from two trials testing the role of abiraterone on top of castration therapy.
LATITUDE is a large phase 3 trial looking at really nasty metastatic prostate cancer, and nasty because they have to have at least two poor-risk factors, out of visceral metastasis, at least 3 bone metastases, and a Gleason score of 8 or greater.
A second trial is also looking at this question for more all-comers—patients with prostate cancer about to start ADT—and we see in an academic trial called STAMPEDE. So the two trials are really expected very, very soon.
Study design: Meta-analysis of three studies (CHAARTED, GETUG-15, STAMPEDE; N = 2,992). For each trial, HRs of the effects of DOC or bisphosphonates on survival (time from randomisation until death from any cause) and failure-free survival (time from randomisation to biochemical or clinical failure or death from any cause) were extracted. Figure shown was for M1 disease.
Survival Effect of Docetaxel in Patients With Early Metastatic Disease
Favours SOC + DOC Favours SOC
0.5 1 2
Treatment
101/397
NA/192
144/362
158/365
HR (95% CI)
0.61 (0.47-0.80)
0.90 (0.69-1.81)
0.76 (0.62-0.93)
0.85 (0.65-1.10)
0.77 (0.68-0.87)
Control
136/393
NA/193
350/724
170/366
CHAARTED
GETUG-15
STAMPEDE (SOC ± DOC)
STAMPEDE (SOC + ZA ± DOC)
Overall
Heterogeneity χ2 = 4.80; df = 3; P = .187; I2 = 37.5%
Metastatic CSPC: Clinical Studies Assessing Docetaxel Treatment
Abbreviation(s): NA: not available; SOC: standard of care; ZA: zoledronic acid.Reference(s): Vale CL et al; STOpCaP Steering Group. Lancet Oncol. 2016;17:243-256.
In the meantime, after these trials were designed and conducted, docetaxel emerged as a standard of care for fit patients [good performance status] with castration-sensitive disease—at least those patients with multiple bony metastasis or visceral disease.
This is, for example, the meta-analysis of large phase 3 trials. The overall analysis resulted in a 23% reduction in the risk of death when docetaxel is, indeed, used upfront in these gentlemen. So this is for most of us, I guess, now a current standard.

6
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
For example, many experts seea role for early use of docetaxelin patients with:
• Multiple bony metastases
• Visceral metastases
Q: Do you recommend ADT + docetaxel in patientswith castration-naïve “high-volume” disease?
Findings from the second St Gallen APCCC Expert Panel will be published soon
Majority,50%
No,11%
Minority,39%
Metastatic CSPC: St Gallen APCCC Expert Use of Docetaxel
Reference(s): Gillessen S et al. Ann Oncol. 2015;26:1589-1604.
There is debate as whether this is true for all-comers, or whether we should restrict docetaxel use for patients with very advanced disease—namely those with multiple bony metastases or those with visceral metastases. The experts just had the second St Gallen consensus meeting; most of us are now using docetaxel early in advanced prostate cancer.
Metastatic CSPC: Phase 3 ARASENS Study AssessingDarolutamide (ODM-201)
1
1PBO
+ ADT + DOC
Phase 3 randomised,double-blind,multinational study
Patients (N ~1,300) with:
• Histologically or cytologically con�rmed disease
• Metastatic, hormone-sensitive disease
• Candidates for ADT/DOC
• ECOG PS 0/1
• Adequate bone marrow,
liver, and renal function
Darolutamide+ ADT + DOC
Primary endpoint
• OS
Key secondary endpoints
• Time to CRPC
• Time to subsequent therapy
• SSE-FS
• Time to:
– First SSE
– Opioid use
– Pain progression
– Worsening physical symptoms
R
Planned completion date:August 2022
Abbreviation(s): ECOG PS: Eastern Cooperative Oncology Group performance status; OS: overall survival; SSE: symptomatic skeletal events; SSE-FS: SSE-free survival.Reference(s): ClinicalTrials.gov Identifier: NCT02799602. https://clinicaltrials.gov/ct2/show/NCT02799602. Accessed March 30, 2017.
The next question will be, should we use androgen receptor pathway inhibitors on top not only of castration therapy, but also on top of docetaxel?
We do have trials looking at whether next-generation AR-targeted drugs may make a difference. The ARASENS phase 3 trial is really looking at whether ODM-201 (darolutamide) will further improve overall survival in a context of the patients who's treated with ADT plus docetaxel. So this will be a really complementary to the previous trials I just mentioned. ODM-201 (darolutamide) is chemically different [from other ARPIs]; it doesn't penetrate the brain-blood barrier, which might be important because, part of the toxicity of enzalutamide, at least in some patients, might be related to the fact that it penetrates the brain and binds to the GABA receptor.
a High risk de�ned as PSA doubling time ≤10 months.b Agent currently unapproved for CRPC.
Approved ARPI
Experimental Arm Control Arm Clinical Trial Identifier (Study Name)
Clinical State Prior Chemotherapy
Enzalutamide PBO NCT02003924(PROSPER)1
High-riska
M0 CRPC
No
Emerging ARPIb
Experimental Arm Control Arm Clinical Trial Identifier (Study Name)
Clinical State Prior Chemotherapy
Apalutamide(ARN-509)
PBO NCT01946204(SPARTAN)2
High-riska
M0 CRPCNo
Darolutamide(ODM-201)
PBO NCT02200614(ARAMIS)3
High-riska
M0 CRPCNo
M0 CRPC: Phase 3 Studies of Approved and Emerging ARPIs
Reference(s): 1. ClinicalTrials.gov Identifier: NCT02003924. https://clinicaltrials.gov/ct2/show/ NCT02003924. Accessed April 4, 2017.2. ClinicalTrials.gov Identifier: NCT01946204. https://clinicaltrials.gov/ct2/show/NCT01946204. Accessed April 4, 2017.3. ClinicalTrials.gov Identifier: NCT02200614. https://clinicaltrials.gov/ct2/show/ NCT02200614. Accessed April 4, 2017.
Now, a very different clinical situation, again, is that of patients with non-mCRPC [M0 CRPC]. So again, we do have the ARAMIS phase 3 trial testing ODM-201 (darolutamide), also the SPARTAN phase 3 trial looking at ARN-509 (apalutamide), and the PROSPER phase 3 trial looking at enzalutamide. With ARN-509 (apalutamide), honestly, we don't necessarily see much different as compared with enzalutamide. In the phase 1/2 development, you also don't see much difference.
7
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
a Emerging agent, currently unapproved for CRPC.
Experimental Arm Control Arm Clinical TrialIdentifier
Clinical State PriorChemotherapy
Apalutamidea
+ ABI/Pred
Abiraterone + PBO NCT022577361 mCRPC No
Enzalutamide + ABI/Pred
Enzalutamide NCT019493372 mCRPC No
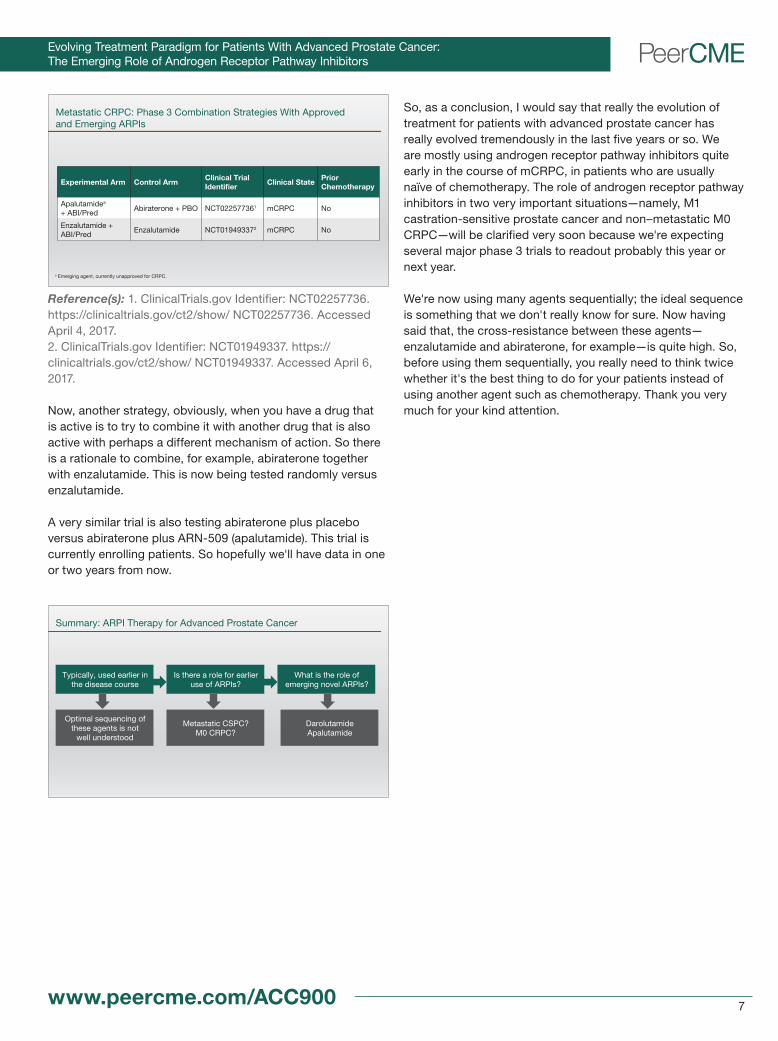
Metastatic CRPC: Phase 3 Combination Strategies With Approvedand Emerging ARPIs
Reference(s): 1. ClinicalTrials.gov Identifier: NCT02257736. https://clinicaltrials.gov/ct2/show/ NCT02257736. Accessed April 4, 2017.2. ClinicalTrials.gov Identifier: NCT01949337. https://clinicaltrials.gov/ct2/show/ NCT01949337. Accessed April 6, 2017.
Now, another strategy, obviously, when you have a drug that is active is to try to combine it with another drug that is also active with perhaps a different mechanism of action. So there is a rationale to combine, for example, abiraterone together with enzalutamide. This is now being tested randomly versus enzalutamide.
A very similar trial is also testing abiraterone plus placebo versus abiraterone plus ARN-509 (apalutamide). This trial is currently enrolling patients. So hopefully we'll have data in one or two years from now.
Typically, used earlier in the disease course
Is there a role for earlier use of ARPIs?
Optimal sequencing of these agents is not
well understood
Metastatic CSPC? M0 CRPC?
What is the role of emerging novel ARPIs?
Darolutamide Apalutamide
Summary: ARPI Therapy for Advanced Prostate Cancer
So, as a conclusion, I would say that really the evolution of treatment for patients with advanced prostate cancer has really evolved tremendously in the last five years or so. We are mostly using androgen receptor pathway inhibitors quite early in the course of mCRPC, in patients who are usually naïve of chemotherapy. The role of androgen receptor pathway inhibitors in two very important situations—namely, M1 castration-sensitive prostate cancer and non–metastatic M0 CRPC—will be clarified very soon because we're expecting several major phase 3 trials to readout probably this year or next year.
We're now using many agents sequentially; the ideal sequence is something that we don't really know for sure. Now having said that, the cross-resistance between these agents—enzalutamide and abiraterone, for example—is quite high. So, before using them sequentially, you really need to think twice whether it's the best thing to do for your patients instead of using another agent such as chemotherapy. Thank you very much for your kind attention.

8
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
FDA Approval Timeline 1993 2010 2013
Emergingagents
Stront
ium-8
9 (R
P)
Mito
xant
rone
(CT)
Samar
ium-1
53 (R
P)
Zoledro
nic A
cid (B
P)
Docet
axel
(CT)
Denos
umab
(BP)
Sipuleuc
el-T
(IO)
Abirate
rone
(ARPI)
Cabaz
itaxe
l (CT)
Enzalu
tam
ide (ARPI)
Radium
-223
(RP)
Survival
Palliation
Currently Approved Therapies for mCRPC: Moving From Palliationto Survival Bene�t
Abbreviation(s): ARPI: androgen receptor (AR) pathway inhibitor; BP: bisphosphonate; CT: chemotherapy; IO: immunotherapy; mCRPC: metastatic castration-resistant prostate cancer; RP: radiopharmaceutical.Reference(s): Adapted by: Matthew Smith, MD, PhD; March 2017.
Matthew Smith, MD, PhD: Hello, I’m Dr. Matthew Smith, Professor of Medicine at Harvard Medical School, and Director of the Genitourinary Malignancies Program at Massachusetts General Hospital Cancer Center. Currently, there are six FDA-approved therapies for metastatic castration-resistant prostate cancer (mCRPC).
These approved agents include two androgen receptor pathway inhibitors, abiraterone acetate and enzalutamide. Abiraterone acetate and enzalutamide are important parts of our toolbox for the management of advanced disease. Both drugs are approved for the treatment of mCRPC before and after docetaxel chemotherapy, based on Level 1 evidence for improved progression-free (PFS) and overall survival (OS).
Current ARPIs: Abiraterone and Enzalutamide
Proven ef�cacy formCRPC management
Acceptable safety/tolerability pro�le
Can agents targeting the ARpathway be effectiveEARLIER in the aPCtreatment paradigm?
Can known safety andtolerability issues
be minimised?
New ARPI options needed
Evolving the Standard of Care for Advanced Prostate Cancer:Optimising ARPI Therapy
Abbreviation(s): aPC: advanced prostate cancer.
While abiraterone acetate and enzalutamide are well tolerated, there are some patients who, in fact, have unacceptable side effects with one or both of those agents, so there is an unmet need for drugs that are better tolerated. There’s also a need to look at this class of agents in other clinical settings, including some settings where tolerability will be particularly important. For example, in the setting of non–metastatic CRPC, there would be an expected long period of treatment, and in order for that to be acceptable, we would prefer to have agents that have an extremely favourable safety profile.
Non-metastatic Metastatic and asymptomatic Metastatic and symptomatic
No detectabledisease;
asymptomatic
Low-volume bone disease; asymptomatic
High-volume bonedisease; pain,
fatigue, anaemia
Visceral disease
TIME
PS
A C
ON
CE
NT
RA
TIO
N
Use of current ARPIs abiraterone and enzalutamide Opportunity for ARPIs
earlier in aPC paradigm?
Evolving the Standard of Care for Advanced Prostate Cancer:Can ARPIs Be Used Earlier in Disease Management?
Abbreviation(s): PSA: prostate-specific antigen.Reference(s): Lorente D et al. Lancet Oncol. 2015;16:e279-e292.
Matthew Smith, MD, PhDHarvard Medical SchoolMassachusetts General HospitalBoston, Massachusetts, USA
An Evidentiary Review of Emerging Androgen Receptor Pathway Inhibitors

9
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
This activity will review the role of novel androgen receptor pathway inhibitors in phase 3 clinical development, and how the ongoing clinical trials may shape the future use of this class of drugs in other important settings in prostate cancer, including non–metastatic CRPC (non–mCRPC) and hormone-sensitive (or castration-sensitive) prostate cancer.
Novel ARPIs in Phase 3 Clinical Development: Apalutamide
Approved ARPIs Emerging ARPIs • Abiraterone
• Enzalutamide
• Apalutamide
• Darolutamide
Apalutamide (ARN-509)
• Anti-androgen• Structurally similar to enzalutamide• High af�nity for AR• Crosses the BBB Apalutamide Enzalutamide
NC N
NN O
O
HNF
F3C
SNC
NN O
O
HNF
F3C
S
Abbreviation(s): BBB: blood-brain barrier.Reference(s): Toren PJ, Gleave ME. Transl Androl Urol. 2013;2:265-277.Bambury RM, Rathkopf DE. Urol Oncol. 2016;34:348-355.
There are two novel androgen pathway inhibitors in phase 3 clinical development, apalutamide and darolutamide.
Apalutamide, formerly known as ARN-509, is an anti-androgen that is structurally very similar to enzalutamide. Like enzalutamide, it also has a high affinity for the androgen receptor and crosses the blood-brain barrier.
Study design: To evaluate the ef�cacy of apalutamide before or after treatment with abiraterone + prednisone in progressive mCRPC,abiraterone/prednisone-naïve (n = 25) and post-abiraterone/prednisone (n = 21) patients who had received ≥6 months of abiraterone/prednisone with progressive mCRPC without prior CT received apalutamide 240 mg/day.
Metastatic CRPC: Phase 2 Study With Apalutamide
Abiraterone/Pred-Naïve (n = 25)
PSA Response Rate, 22%
Post-Abiraterone/Pred-Naïve (n = 21) 180160
120
80
40
140
100
60
200
12-W
k P
SA
Cha
nge
Fro
m B
asel
ine
in P
ost
-Ab
irat
ero
ne/P
red
Pat
ient
s, %
-20-40-60-80
-100
PSA Response Rate, 88%
100
80
60
40
20
0
12-W
k P
SA
Cha
nge
Fro
m B
asel
ine
in A
bir
ater
one
/Pre
d-N
aïve
Pat
ient
s, %
-20
-40
-60
-80
-100
Abbreviation(s): Pred: prednisone.Reference(s): Rathkopf DE et al; Clin Cancer Res. 2017 Feb 17. pii: clincanres.2509.2016 [Epub ahead of print]. doi:10.1158/1078-0432.CCR-16-2509.
In a phase 2 clinical trial, apalutamide demonstrated activity in mCRPC. Among 25 patients who were abiraterone acetate–naïve, PSA response rate at 12 weeks was 88%. Among patients who had progression despite prior abiraterone acetate, response rates dropped to 22%, consistent with overlapping cross-resistance between the androgen pathway inhibitors.
All-
Gra
de
TE
AE
in >
15%
of
Pat
ient
s, %
60 56
48 44
28 28 24 24 24
20 20 16 16 16
52
33
10
38
14
0
29
19
10 14
0
24
10 5
0
10
20
30
40
50
60
70
Fatig
ue
Nause
a
Abdomina
l Pain
Diarrh
oea
Dyspno
ea
Rash
Arthra
lgia
Back P
ain
Cough
Anaem
ia
Hot F
lush
Decre
ased
Appet
ite
Dizzine
ss
Insom
nia
Abiraterone/Pred-Naïve (n = 25)
Post-Abiraterone/Pred (n = 21)
Metastatic CRPC: Phase 2 Safety Outcomes With Apalutamide
Abbreviation(s): TEAE: treatment-emergent adverse event (AE).Reference(s): Rathkopf DE et al; Clin Cancer Res. 2017 Feb 17. pii: clincanres.2509.2016 [Epub ahead of print]. doi:10.1158/1078-0432.CCR-16-2509.
The most common adverse events associated with apalutamide were fatigue, nausea, abdominal pain, and diarrhoea. Notably, most of the adverse events were grade 1 or 2.
High-risk localised/LA aPC
High-risk M0 CRPC
Low-volumemCSPC
mCRPC
NCT02531516(ATLAS)
Apalutamide +GnRH + RT
vs
GnRH + RT + PBO
NCT01946204(SPARTAN)
Apalutamide
vs
PBO
NCT02489318(TITAN)
Apalutamide + ADT
vs
ADT + PBO
NCT02257736
ABI/Pred + apalutamide
vs
PBO/Pred
Disease Course
Phase 3 Studies of Apalutamide
Abbreviation(s): ABI: abiraterone; ADT: androgen deprivation therapy; GnRH: gonadotropin-releasing hormone; LA: locally advanced; mCSPC: metastatic castration-resistant prostate cancer; PBO: placebo; RT: radiation therapy.Reference(s): Anantharaman A, Friedlander TW. Urol Oncol. 2016;34:356-367.

10
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
There are currently four phase 3 clinical trials of apalutamide. The ATLAS study will evaluate the addition of apalutamide to androgen deprivation therapy (ADT) and radiation therapy for men with high-risk localised prostate cancer. The SPARTAN study will evaluate apalutamide in men with high-risk non–mCRPC. The TITAN study will evaluate apalutamide in men with low-volume metastatic hormone-sensitive prostate cancer. Another study will evaluate the addition of apalutamide to abiraterone in men with mCRPC.
Novel ARPIs in Phase 3 Clinical Development: Darolutamide
Approved ARPIs Emerging ARPIs • Abiraterone
• Enzalutamide
• Apalutamide
• Darolutamide
Darolutamide (ODM-201)
• Anti-androgen• Structurally distinct from any known anti-androgens• Great af�nity for AR Darolutamide
N
NC
CINN
NH NH
OHO
(S)
Reference(s): Wong YN et al. Nat Rev Clin Oncol. 2014;11:365-376.Moilanen A-M et al. Sci Rep. 2015;5:12007.Bambury RM, Rathkopf DE. Urol Oncol. 2016;34:348-355.
Darolutamide, formerly known as ODM-201, is also a potent anti-androgen; it is structurally distinct from other known anti-androgens. It also has a greater affinity for the androgen receptor.
a The very low access of darolutamide into the brain was con�rmed with a quantitative whole-body autoradiography (QWBA).
Darolutamide3%
Comparative Penetration of the Blood-Brain Barrier by ARPIs
Apalutamide29%
Enzalutamide 19%
BBB Penetration1
62
27
0 10 20 30 40 50 60 70
Enzalutamide
Apalutamide
Darolutamide
Brain/Plasma Ratio in Mouse, %a,2
1.9-3.9
Abbreviation(s): QWBA: quantitative whole-body autoradiography.Reference(s): 1. Moilanen AM et al. European Cancer Congress 2013 (ECC 2013). Poster. http://www.orion.fi/globalassets/documents/rd/congress-posters/esmo-2013-nonclinical-poster.pdf. Accessed April 13, 2017.2. Moilanen AM et al. Sci Rep. 2015;5:12007.
Limited penetration of the blood-brain barrier also distinguishes darolutamide from other anti-androgens. In this non-clinical model, for example, the blood-brain-barrier penetration for darolutamide was only 3% compared with 19% and 29% for enzalutamide and apalutamide, respectively. The predicted lower blood-brain penetration and lower brain exposure with darolutamide may confer a safety advantage for darolutamide relative to other anti-androgens. This will be assessed in multiple ongoing large clinical trials.
Study design: To evaluate the safety, pharmacokinetics, and activity of darolutamide, the phase 1 portion of the open-label dose-�nding study. In phase 2, patients were randomly assigned centrally, and strati�ed by previous CT and treatment with CPY17 inhibitors, to receive one of three daily doses of darolutamide (200 mg, 400 mg, and 1,400 mg). The primary endpoint in phase 2 was the proportion of patients with a PSA response (≥50% decrease in serum PSA) at week 12.
-100
-50
0
50
100
PS
A C
hang
e Fr
om
Bas
elin
e to
Wk
12, %
-100
-50
0
50
100
PS
A C
hang
e Fr
om
Bas
elin
e to
Wk
12, %
Chemotherapy- andCPY17i-Naïve Patient Group
Post-CPY17i Patient Group
200 mg
PSA ≥50%: 50% (200 mg) 69% (400 mg) 86% (1,400 mg)
PSA ≥50%: 0 (200 mg) 18% (400 mg) 7% (1,400 mg)
400 mg 1,400 mg
Metastatic CRPC: Phase 2 Study With Darolutamide (ARADES)
Abbreviation(s): CPY17i: CPY17 inhibitor.Reference(s): Fizazi K et al. Lancet Oncol. 2014;15:975-985.
The efficacy of darolutamide in mCRPC has been demonstrated in a phase 2 clinical trial. Among patients with mCRPC and no prior exposure to abiraterone acetate or chemotherapy, PSA response rate was 86% at the highest dose studied. As expected, the PSA response rate was lower [7% among highest dose studied] among patients who had disease progression despite prior treatment with abiraterone acetate.
To
tal A
Es
in ≥
10%
of
Pat
ient
s, %
13 13 10 10 10 10 10
0
10
20
30
40
50
60
Nausea Fatigue Bone Pain AbdominalPain
Back Pain Diarrhoea Haematuria
Study design: Patients (N = 30) in this open-label phase 1 trial received a single 600-mg dose of darolutamide in capsules with food and one 600-mg dose of darolutamide tablet product (TabA or TabB) with food and in the fasted state in a random order. In the extension, patients received 600 mg twice daily darolutamide taken with food in capsules.
Metastatic CRPC: Phase 2 Safety Outcomes With Darolutamide (ARADES)
Reference(s): Massard C et al. Eur Urol. 2016;69:834-840.

11
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
www.peercme.com/ACC900
The most commonly reported adverse events associated with darolutamide were nausea, fatigue, bone pain, and abdominal pain. Notably though, the rate of these adverse events was very low, between 3% and 13%, and the majority of adverse events were grade 1.
While we always have to be careful about comparing between different phase 2 clinical trials—these were not head-to-head trials—the reported safety profile of darolutamide looked particularly favourable.
M0 CRPC mCSPC
NCT02200614(ARAMIS)
Darolutamide
vs
PBO
NCT02799602(ARASENS)
Darolutamide +ADT + DOC
vs
PBO + ADT+ DOC
Disease Course
Phase 3 Studies of Darolutamide
Abbreviation(s): DOC: docetaxel.Reference(s): Anantharaman A, Friedlander TW. Urol Oncol. 2016;34:356-367.
There are two ongoing phase 3 clinical trials of darolutamide in prostate cancer. The ARAMIS trial will evaluate darolutamide in men with high-risk non–mCRPC. The ARASENS trial evaluates ADT plus docetaxel, with or without darolutamide, in men with hormone-sensitive metastatic disease.
a In preclinical models.
Approved ARPIsAbiraterone
Enzalutamide
Emerging ARPIsApalutamideDarolutamide
Approved in both the pre- andpost-docetaxel settings
• Comparable efficacy, evaluated in both ARPI-naïve and ARPI-experienced patients• Darolutamide has lower BBB penetrationa
• Role of these agents is evolving in various aPC settings
Summary: Targeting the Androgen Receptor for Advanced Prostate Cancer
In summary, the androgen receptor is a validated target in prostate cancer. There are two novel anti-androgens in phase 3 clinical development. Apalutamide, or ARN-509, is structurally similar to enzalutamide, and is undergoing evaluation in four phase 3 clinical trials. Darolutamide is structurally distinct and is currently in phase 3 clinical development in two clinical trials.
There’s limited evidence to suggest there would be marked differences in efficacy between the different androgen receptor pathway inhibitors. From a distance, it would appear that darolutamide is particularly well tolerated and that might confer advantages, particularly in the settings where there is an anticipated long period of exposure. We will look to the results of the ongoing studies to determine whether in fact that’s the case.
The results of ongoing phase 3 clinical studies will not only assess the value of these novel anti-androgens, but also evaluate the role of this class of agents in an earlier disease state, so if successful and approved and used in that setting, the drugs might be moved in front of abiraterone or enzalutamide. So, the landscape has already been transformed in recent years and will be transformed again in coming years, as the results of these clinical trials mature and we better understand the optimal way to use these agents.
Narrator: Thank you for participating in this PeerCME educational activity. To obtain your CME certificate, complete the required post-test and evaluation form.
[Theme]
Evolving Treatment Paradigm for Patients With Advanced Prostate Cancer: The Emerging Role of Androgen Receptor Pathway Inhibitors
About This PeerCME Activity PeerVoice and Oakstone Publishing, LLC, are responsible for the selection of this activity's topics, the preparation of educational content, and the distribution of this activity. The preparation of PeerCME activities is supported by written agreements that clearly stipulate and enforce the independence of PeerVoice, Oakstone Publishing, LLC, and the faculty presenters.
The faculty may discuss unapproved products or uses of these products in certain jurisdictions. Faculty presenters have been advised to disclose any reference to an unlabelled or unapproved use. No endorsement of unapproved products or uses is made or implied by coverage of these products or uses in our activities. No responsibility is taken for errors or omissions.
For approved prescribing information, please consult the manufacturer's product monograph.
PeerVoice1140 Avenue of the Americas, 15th FloorNew York, NY 10036
© 2010-2017, PeerVoice
The materials presented here are used with the permission of the authors and/or other sources. These materials do not necessarily reflect the views of PeerVoice or any of its supporters.
This activity is supported by an educational grant from Bayer Healthcare Pharmaceuticals.
CRPCTreatmentPlan.peercme.comCheck out our curriculum website for more information and resources: