exercise in medicine
TRANSCRIPT
Exercise in Medicine
นพ. ฉกาจ ผ่องอักษร
ภาควชิาเวชศาสตร์ฟ้ืนฟู คณะแพทยศาสตร์ศิริราชพยาบาล

Aerobic Exercise Exercises use large muscle groups, continuous and
rhythmic in nature duration 20-60 min or more
Intensity range of training
60-90 % HRmax
50-85 % VO2max
or %HRR

Aerobic Ex Training Effects
Aerobic Benefit
• Improve lipid oxidation (fat metabolism)
• Improve mood by endorphin
• Improve blood circulation
• Anti-atherosclerotic effect

Monitoring Exercise Intensity
% VO2 max
%HRmax or %HR reserve
%HRmax = (HRmax x % number)/100
%HR reserve = (HRmax–HR resting) x % number/100
Rate of Perceived Exertion by Borg’s Scale (RPE),
6 = very, very light - 20 very very hard
Talk test, METs

Heart Rate Methods Heart Rate Monitoring
VO2 = CO (HR x SV) x a-v O2
difference
Linearly related to VO2 during
exercise
%HRmax (HRmax X %/100)
%HR reserve (HRmax – HR
resting)
Factors affecting HR, e.g. caffeine,
sleep, emotion, overtraining

Calculation of Heart Rate Reserve
Compute age predicted HR (220-20 = 200)
Compute HRR (220-60) = 140
Select training intensity (80%)
Calculate % of reserve (140 x 0.80 = 112)
Add resting HR (112+60 = 172)
Target HR (= 172) + 5 bpm

ค่าคะแนนความเหน่ือย Rate of Perceived
Exertion

Method Comparison of Exercise Intensity
Comparison of Aerobic Exercise Intensity %HRmax
%HRR/VO2max
RPE
Intensity
<35
<20
<10
Very light 35-54
20-39
10-11
Light
55-69
40-59
12-13
Moderate 70-89
60-84
14-16
Hard
> 90
>85
17-19
Very hard 100
100
20
Maximal
METs
1-3
3-6
> 6
Resistance/Strengthening Ex
Definition
Form of active Ex in which a dynamic or static muscular contraction is resisted by an outside force.
Manual or Mechanical Resistance Ex
Goals & Indications
Inc. strength
Inc. muscular endurance
Inc. muscle power
Principles
Overload
Specificity
Reversibility

10
Resistant/Strength Training Exercise

11
Conditioning Exercise

Changes in NMS to Muscle Strength
Recruitment
1st few weeks
Greater number of motor unit firing
Hypertrophy vs Hyperplasia
Inc. amount of protein in muscle fiber
Inc. density of capillary bed
Biomechanical changes

Types of Resistance Exercise Isometric/Static Resistance Exercise
At least 6 sec., 60-80% Max muscle force to gain strength Muscle setting exercise (retard atrophy), Agonist-Antagonist Co-contraction
Isotonic Resistance Exercise Concentric contraction exercise Eccentric contraction exercise Open/Close chain kinetic exercise
Isokinetic Resistance Exercise (Speed constant) or Accommodating Resistance Exercise

Variables in Mechanical REx
Load and Number of repetitions Repetition Maximum (RM)
Resting time
Bouts and frequency
Duration
Speed-specific vs Velocity spectrum Isokinetic training
Type of muscle contraction
Patient position and Range of movement

Repetition Maximum (RM)
จ านวนครัง้ที่ยก
Repetition Factor 1
1.00
2
1.07 3
1.10
4
1.13 5
1.16
6
1.20 7
1.23
8
1.27 9
1.32
10
1.36 11
1.40
12
1.43

Isotonic Regimens
DeLorme technique
Progressive resistive exercise (PRE)
Oxford technique
Daily Adjustable Progressive Resistance Exercise – DAPRE technique
Circuit weight training

Resistance Exercise Precaution
Cardiovascular complication Valsalva’s maneuver
Reminding, exhale, count or talk
Fatigue Recovery period
Multiple sclerosis, PVD, Pulm. Disease
Overwork / Overtraining
Substitute motions
Osteoporosis
Delayed Onset of Muscle Soreness (DOMS 24-48 hr.)

Passive Stretching Manual passive stretching
Applied force and controls the direction, speed, intensity and duration of the stretch beyond their resting length
For at least 15-30 sec, 5-10 repetitions
Static vs. Ballistic stretch
Gains achieve in ROM are transient and from temporary sarcomere give
Prolong mechanical PS Low wt. (5-15 lb) over a
prolong period using traction and pulley systems or with dynamic splints or serial casts
More effective and cause permanent lengthening (plastic changes) contractile & noncontractile tissues.
Cyclic mechanical stretching


Reference
American College of Sports Medicine, Appropriate intervention strategies for weight loss and prevention of weight regain for adults,2009
North American Association for the Study of Obesity and the National Heart, Lung and Blood Institute, Practical guide to the identification, evaluation and treatment of overweight and obesity in Adults, 2000
Vivian H. Heyward, Advance fitness assessment and exercise prescription, second edition, USA
20

Obesity in Thailand
Age-standardized prevalence of
• overweight (23 ≤ BMI ˂ 25)
• Class I obesity (25 ≤ BMI ˂ 30)
• Class II obesity (BMI ≥ 30)
• Abdominal obesity (WC 90 cm
in men, 80 cm in women)
In adults 18 to 59 years of age
by sex, Thailand 1997 and
2004.
21 Wichai Aekplakorn et al. Trends in Obesity and Associations with Education and Urban or Rural Residence in Thailand OBESITY
.2007;15:3113-3121.

Health risk associated with obesity
23 The Western Pacific Region, World Health Organization, International Associates for the Study of Obesity, International Obesity Task
Force. The Asia-Pacific Perspective: redefining obesity and its treatment. Melbourne: Health Communications Australia, 2000.

Development of Obesity The total number of fat cell: determined during the growing years
First year
Puberty
Hyperplastic
Hypertrophic
An abnormal number of fat cell
An increase in size of fat cell
24

Causes of obesity
• Positive energy balance
• Input> expenditure • 3500 kcal:1 pound of fat is
stored in the body
• Negative energy balance
• Expenditure> input
25

Causes of Obesity
Genetic component:
• Metabolic response to food
intake and physical activity
Behavioral component:
• Eating and exercise
behaviors
26 Stanly P. Brown, Wayne C. Miller, Jane M. Eason: Exercise physiology basis of human movement in health and disease. Lippincott
William & Wilkins 2006.

Metabolic Rate and Overweight/Obesity
Basal metabolic rate
Varies to age, gender, body size, body composition and regulated by hormone
Rest, controlled environment
Not practical
Resting metabolic rate
Energy required to maintain essential physiological process in relaxed, awake and reclined state
27

Estimation of Basal (Resting) Metabolic Rate (Harris-Benedict Equation)
28
Males:
RMR (kcal/day)= 88.362 + (4.799*Height) +
(13.397*Weight) – (5.677*Age)
Females:
RMR (kcal/day) = 447.593 + (3.098*Height) +
(9.247*Weight) – (4.330*Age)
Where; Height = Height in centimeters
Weight = Weight in kilograms
Age = Age in years
Sharon A. Plowman, Denise L. Smith, Exercise physiology for health, fitness and performance.2008
The Harris Benedict equation reevaluated. A.M. Roza and H.M. Shizgal.
American Journal of Clinical Nutrition. Vol. 40, No. 1 (July 1984): 168-182.
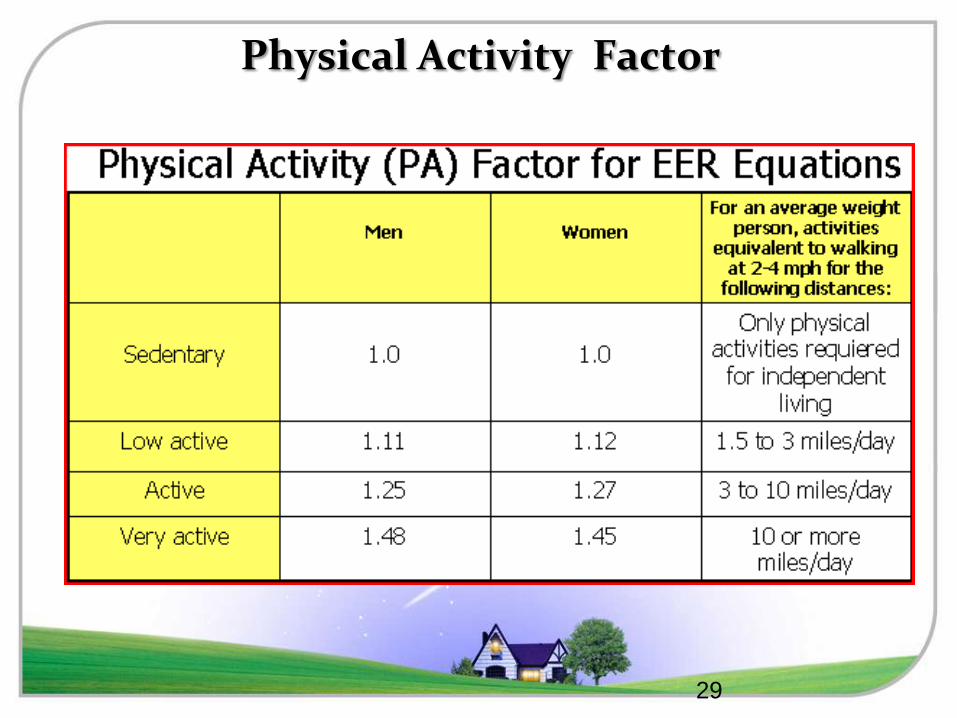
Physical Activity Factor
29
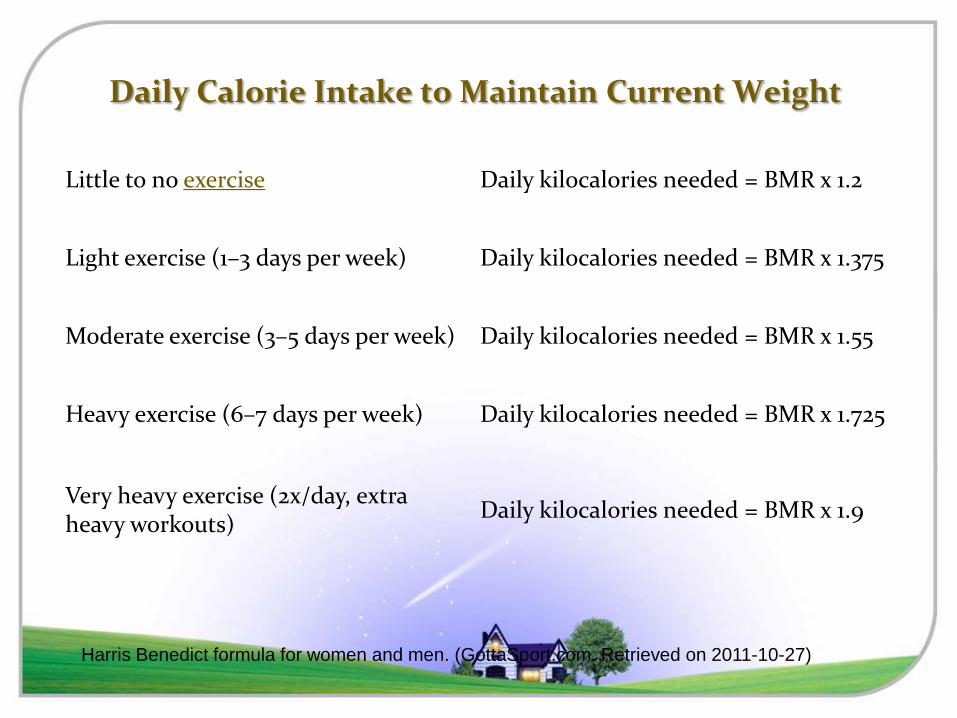
Daily Calorie Intake to Maintain Current Weight
Little to no exercise Daily kilocalories needed = BMR x 1.2
Light exercise (1–3 days per week) Daily kilocalories needed = BMR x 1.375
Moderate exercise (3–5 days per week) Daily kilocalories needed = BMR x 1.55
Heavy exercise (6–7 days per week) Daily kilocalories needed = BMR x 1.725
Very heavy exercise (2x/day, extra heavy workouts)
Daily kilocalories needed = BMR x 1.9
Harris Benedict formula for women and men. (GottaSport.com. Retrieved on 2011-10-27)
Causes of Overweight and Obesity
TEXT TEXT TEXT •Positive
energy balance
•Input> Expenditure •3500 kcal
•1 pound
of fat is
stored in the body
•Energy balance
•Input = Output
RMR+
Activity level
•Negative energy
balance
Expenditure>Input
Food Intake
PA
31

Causes of Overweight and Obesity
Improper diet
Overeating
Hormonal disturbance
Physical inactivity
?? Genetics and environment
Psychological factors: Overeating and compulsive eating may be defense mechanism in anxiety, depression, stress
+ energy balance
32

Goal Management of Obesity
Reducing size of fat cell
Key to prevent obesity
Monitor dietary intake and energy expenditure esp. during adolescent growth
spurt and puberty Retard the development of new fat cell and control the size
Diet and exercise
33

Effects of Weight Loss on Risk Status
weight loss
Add Your Text
Lower elevated BP in HT
Lower elevated blood glucose levels in DM
•Lower elevated levels of TC, LDLTG •Raise low levels of HDL in dyslipidemia.
34

Treatment Guidelines
Tailor treatment to the needs of the patient
Aim of this guide
weight reduction maintain a lower body weight
2 step process
Assessment Management
35

Assessment Body mass index (BMI
Practical approach for assessing body fat in the clinical setting
More accurate measure compared with the assessment of body weight alone Limitations
Overestimate- persons who are very muscular
Underestimat- persons who have lost muscle mass (e.g., many elderly)
Body mass index (BMI)
36

Overweight and Obesity Overweight
BMI 25-29.9 kg/m Obesity
BMI ≥ 30 kg/m Characterized by the accumulation of excessive levels of body fat
37

BMI for Asian
38 The Western Pacific Region, World Health Organization, International Associates for the Study of Obesity, International Obesity Task
Force. The Asia-Pacific Perspective: redefining obesity and its treatment. Melbourne: Health Communications Australia, 2000.

Assessment Clinical judgment must be used in interpreting BMI
Situations that may affect its accuracy Edema, high muscularity, muscle wasting
The relationship between BMI and body fat content varies
Age, gender, ethnicity
Differences in the composition of lean tissue, sitting height and hydration state
39

Assessment Waist circumference
•The most practical tool a clinician can use to evaluate a patient’s abdominal fat •Before and during weight loss treatment •Computed tomography and magnetic resonance imaging
•More accurate •Impractical for routine clinical use
40

Assessment Waist circumference
Fat located in the abdominal region is associated with a greater health risk than peripheral fat
High-Risk Waist Circumference Men: > 40 in (> 102 cm) Women: > 35 in (> 88 cm)
41

Assessment
Waist circumference Provides an independent prediction of risk over that of BMI Useful: normal or overweight in BMI
Provide an estimate in abdominal fat, in the absence of changes in BMI Obese patients with metabolic complications
Changes in waist circumference are useful predictors of changes in CVD risk factors
42

Waist Circumference Assessment
• Locate the upper hip bone and the top of the right iliac crest
• Horizontal plane around the
abdomen at the level of the iliac crest
• Not compress the skin • At the end of a normal
expiration
43

Assessment
44

Body Fat Percentage Categories
45
Classification Women Men
Essential Fat 10-12% 2-4%
Athlete 14-20% 6-13%
Fitness 21-24% 14-17%
Acceptable 25-31% 18-25%
Obese 32%+ 25%+

Assessment of Risk Status Required to determine the intensity of a clinical intervention
1. Determine the relative risk status based on overweight and obesity parameters
2. Identify patients at very high absolute risk Coronary heart disease Other atherosclerotic diseases Type 2 DM (FPG ≥ 126 mg/dL or 2-hPPG
≥ 200 mg/dL) Sleep apnea
46

Assessment of Risk Status 3. Identify other obesity-associated diseases
Gynecological abnormalities e.g., menorrhagia, amenorrhea
Osteoarthritis Gallstones Stress incontinence
47

Assessment of Risk Status 4. Identify cardiovascular risk factors that impart a
high absolute risk Cigarette smoking Hypertension
SBP ≥140 mm Hg or DBP≥ 90 mm Hg Use of antihypertensive agents
LDL ≥ 160 mg/dL
A borderline high-risk LDL 130 to 159 mg/dL) plus 2 or more other risk factors
48

Assessment of Risk Status HDL < 35 mg/dL IFG fasting plasma glucose 110-125mg/dL Family history of premature CHD
MI or sudden death experienced by the father or other male first-degree relative at or before 55 years
by the mother or other female first-degree relative at or before 65 years
Age ≥ 45years for men or age ≥ 55 years for women (or postmenopausal)
49

Assessment of Risk Status
Other risk factors
Physical inactivity Exacerbates the severity of other risk factors An independent risk factor for all-cause
mortality or CVD mortality
Increased physical activity
•Promotes weight reduction
•Weight maintenance •Modifies obesity associated risk factors
50
Exclusion From Weight Loss Therapy
Most pregnant or lactating women Serious uncontrolled psychiatric illness
Major depression Serious illnesses
Caloric restriction might exacerbate the illness
Active substance abuse and History of anorexia nervosa or bulimia nervosa
51

Weight Management Techniques
Surgery
physical
activity
Behavior
therapy
Pharmacotherapy
Diet
52

Weight Management Methods
53

Rate of Weight Loss
10 percent reduction in body weight in 6 months of therapy
Energy deficit Significant loss of weight
1 to 2 pounds per week
Based on a caloric deficit between
500 - 1,000 kcal/day
54

Dietary Therapy
1,000-1,200 kcal/d
for most women
Low calorie diet
(LCD)
1,200 to 1,600 kcal/d for men
and women who weigh 165 lbs
or more
very low calorie diet (VLCD)
Hungry increase the calories by 100 -200 /day.
55

Rate of weight loss
After control for 6 months
Theoretically: 26-52 pounds Actually: 20-25 pounds
Changes in resting metabolic rates
Difficult for most patients to continue to lose weight after 6 months
Diet and physical activity goals need to be revised for energy deficit
56

Physical Activity
57

Physical Activity An important component of weight loss
Not lead to greater weight loss than diet alone over 6 months
Most weight loss occurs because of decreased caloric intake
Sustained physical activity
•Prevention of weight regain •Reducing risks
•Cardiovascular disease •Type 2 diabetes
58

Physical Activity ACSM recommends
Adults participate in at least 150 min/wkj of moderate-intensity PA
To prevent significant weight gain Reduce associated chronic disease risk factors
A dose effect of PA Weight loss, prevention of weight regained 250-300 min/wk (2000 kcal/wkj) of moderate intensity PA
59

Physical Activity Dose Response
Moderate-intensity PA for weight loss
Dose–response
PA < 150 min/wk promotes minimal
weight loss
PA >150 min/wk results in modest weight loss of 2-3 kg
PA 225-420 min/wk results in 5-7.5kg weight loss
60

Physical activity
PA to prevent weight gain.
Moderate-intensity PA of 150-250 min/wk with an energy equivalent of 1200-2000 kcal/wkj will prevent weight gain greater than 3% in most adults.
61
Weight Maintenance
After 6 months of weight loss, the rate at which the weight is lost usually declines, then plateaus •A regain of weight that is less than 6.6 lbs (3kg) in 2 years •Reduction in waist circumference of at least 1.6 inches (4 cm)
62

Weight Maintenance
Achieve targeted weight loss
Continue therapy
Long term monitoring
Long term success
In weight reduction
63

Physical Activity Intensity
Moderate-intensity PA for weight maintenance after weight loss
Some studies support: 200-300 min/wk
PA during weight maintenance to reduce weight regain after weight loss More is better
64

Physical activity
Initially
Long term goal
Moderate levels of PA for 30 to 45 mins, 3 to 5 days per week
To accumulate at least
30 minutes or more of moderate-intensity PA
on most and preferably all days of the week
65

66
Exercise Intensity and Fuel Usage
Stanly P. Brown, Wayne C. Miller, Jane M. Eason: Exercise physiology basis of human movement in health and disease. Lippincott
William & Wilkins 2006.
Exercise intensity and
fuel selection
• Recruitment of IIa and IIb
(high glycolytic) muscle fiber
• High level of epinephrine in
the blood (potent stimulator of
glycogenolysis and stimulate
lipolysis)
• Increase lactic acid that
reduce availability of fatty
acid to the muscle

Percent of Fat Burn on Ex Intensity

Fat Use & Exercise Intensity

The Basic Premise of Weight Loss

Calorie Complexities

Which Option is Better?

Physical Activity
72

Physical Activity Safety Avoid injury during physical activity
Extremely obese persons; need to start with simple exercises
Exercise testing for cardiopulmonary disease
Based on A patient’s age Symptoms Concomitant risk factors
73

Progression of Physical Activity Intensity increased gradually Initial activities: increasing small tasks of
daily living More strenuous activities
Fitness walking, cycling, aerobic dancing Depending on
Progress The amount of weight lost Functional capacity
Competitive sports -avoid injury, especially in older people
74

Physical Activity
Time of the day and duration
Try walking before going to work or evenings Accumulating minutes per day Can take an aerobics class instead Try to be more active There is no one right time of day to exercise.
75
Physical Activity
Reducing sedentary time
Patients should be encouraged to build physical activities into each day.
New forms of physical activity should be suggested.
Identifying a safe area to perform the activity
76

Physical Activity: Weight Training
Resistance training (RT) Not seem to be effective for weight reduction in the order of 3% of initial
Not add to weight loss when combined with diet restriction No evidence currently exists
Prevention of weight regain after weight loss or for a dose effect for resistance training and weight loss
77

Physical Activity : Weight Training
78

Physical Activity: Weight Training
Resistance training
Increases fat-free mass
When used alone or in combination with weight loss from diet restriction
May increase loss of fat mass When combined with aerobic exercise compared to resistance training alone
79

Physical activity
Associated with improvements in CVD risk factors
In the absence of significant weight loss HDL-C, LDL-C, insulin, blood pressure
Resistance training
80

Physical Activity Barrier and Obstacles
Obstacles
I don’t have the time to exercise.
It’s hard to
remember
to exercise
I don’t have the energy to be more active
I don’t like
to exercise
81
Behavior Therapy A useful adjunct to planned adjustments in food intake and physical activity Specific behavioral strategies
Stress management Stimulus control Problem-solving Contingency management Cognitive restructuring Social support
82

Pharmacotherapy
Approved by the FDA for long-term used
An adjunct to diet and physical activity
BMI ≥ 30 and without concomitant obesity-related risk factors or diseases
BMI ≥ 27 who have concomitant obesity-related risk factors or disease
83

Weight Loss Surgery An option for weight reduction In patients with clinically severe obesity
BMI ≥ 40 or BMI ≥ 35 with comorbid conditions
Other methods of treatment have failed
Provides medically significant sustained weight loss for more than 5 years in most patients
84

Conclusion Obesity is an excess of body fat such that health risk increased.
Physical inactivity and overeating are common cause of obesity
A negative energy balance is created when the caloric expenditure exceeds the caloric intake, producing weight loss
Most effective way; diet and exercise
85

Conclusion Low calorie diet (LCD)
1,000 to 1,200 kcal/day for most women
1,200 to 1,600 kcal/day for
men
women who weigh 165 pounds or more
Physical activity
To accumulate at least 30 minutes or more of moderate-intensity PA on most
and preferably all days of the week
86

87

Ex and Hypertension (HTN) One of the most common medical disorders, is
associated with an increased incidence of all-cause
and cardiovascular disease (CVD) mortality.
Lifestyle modifications are advocated for the
prevention, treatment, and control of HTN, with exercise being an integral component.
Exercise programs that primarily involve endurance
activity prevent the development of HTN and lower
blood pressure (BP) in adults with normal BP and
those with HTN.

Changes in BP Classification JNC 7 felt that tx was the same for stages 2 and 3 so combine for simplification.
Hypertension 2003;289:2560-2572.

Reference Card

Blood Pressure Classification
BP Classification SBP mmHg* DBP mmHg Lifestyle
Modification
Drug
Therapy**
Normal <120 and <80 Encourage No
Prehypertension 120-139 or 80-89 Yes No
Stage 1
Hypertension 140-159 or 90-99 Yes
Single
Agent
Stage 2
Hypertension ≥ 160 or ≥ 100 Yes Combo
JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
*Treatment determined by highest BP category; **Consider treatment for compelling
indications regardless of BP

Lifestyle Modification
Modification Approximate SBP Reduction
(range)
Weight reduction 5-20 mmHg/ 10 kg weight loss
Adopt DASH eating plan 8-14 mmHg
Dietary sodium reduction 2-8 mmHg
Physical activity 4-9 mmHg
Moderation of alcohol
consumption 2-4 mmHg
JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314

Impact of a 5 mmHg Reduction
Overall Reduction
Stroke 14%
Coronary Heart Disease 9%
All Cause Mortality 7%
Hypertension 2003;289:2560-2572.

Ex and Hypertension (HTN)
The BP lowering effects of exercise are most
pronounced in people with HTN who engage in
endurance exercise with BP decreasing
approximately 5–7 mm Hg after an isolated exercise
session (acute) or following exercise training
(chronic).
Moreover, BP is reduced for up to 22 h after an
endurance exercise bout (e.g., postexercise
hypotension), with the greatest decreases among
those with the highest baseline BP.

Mechanism of BP Lowering
The proposed mechanisms for the BP lowering effects of exercise include neurohumoral, vascular, and structural adaptations.
Decreases in catecholamines and total peripheral resistance, improved insulin sensitivity, and alterations in vasodilators and vasoconstrictors are some of the postulated explanations for the anti-HTN effects of exercise.
Nonetheless, definitive conclusions regarding the mechanisms for the BP reductions following endurance exercise cannot be made at this time.

Effects of Ex Training in Hypertensive Patient
Decrease in plasma norepinephrine level.
Increase in circulation vasodilator substances.
Amelioration of hyperinsulinemia.
Alteration in renal function.

Exercise in Interim Individuals with controlled HTN and no CVD or
renal complications may participate in an exercise program or competitive athletics, should be evaluated, treated, and monitored closely.
Preliminary peak or symptom-limited exercise testing may be warranted, esp for men > 45 and women > 55 yr planning a vigorous exercise program.
It is reasonable for the majority of patients to begin moderate intensity Ex training (40-<60% VO2R) such as walking.

Ex Regimen for HTN The optimal training frequency, intensity, time, and type (FITT) need to be better defined to optimize the BP lowering capacities of exercise, particularly in children, women, older adults, and certain ethnic groups.
Based upon the current evidence, the following exercise prescription is recommended for those with high BP:
Frequency: on most, preferably all, days of the week
Intensity: moderate-intensity (40–60% of VO2R)
Time: 30 min of continuous or accumulated physical activity per day
Type: primarily endurance physical activity supplemented by resistance exercise
ACSM Position Stand: Exercise and Hypertension. MEDICINE & SCIENCE IN SPORTS & EXERCISE 2004

Blood Pressure Monitoring If BP >180/110, endurance training should be added to the treatment regimen only after initiating drug therapy.
Don’t Ex if resting SBP >200 mmHg or DBP > 115 mmHg.
Exercise training at somewhat lower intensities appears to lower BP as much as higher intensities.
Strength/resistive training is not recommended as the only form of Ex training for persons with HPN because, with the exception of circuit weight training, it has not consistently been shown to lower BP.
Resistive training using low resistances and high repetition should be prescribed.
Anti-HPN agents may predispose to post exercise hypotension, so longer cool-down exercise period is needed.

Chakarg Pongurgsorn, MD., PhD. Dept. Rehabilitation Medicine, Faculty Medicine Siriraj Hospital.
Contents
Overview in DM
• Physiologic adaptation to exercise
• Benefit and risk of exercise
• Prevention & treatment of abnormal blood glucose before & after exercise
• Evaluation before exercise & exercise testing
• General exercise recommendation
• Exercise recommendation for specific complication
Exercise in DM

Overview in DM

Goal of Management
Glycemic control
Prevent or delay chronic complication

Glycemic control
Exercise • Improve insulin sensitivity • Improve other CVD risk
: HT, dyslipidemia, obesity
Medication
Diet

Benefit and Risk of Exercise in DM

Benefit from exercise Both type of DM
• Improved insulin sensitivity
• Improved blood lipids and lipoprotein levels
• ↓BP in hypertensive
• ↓Risk of CVD disease
• ↑Caloric expenditure • Reduction or maintenance body wt.
• Improved body composition
• Improved physical fitness and strength
• Improve psychological well-being • Enhance quality of life
• Improved self-esteem

Benefit from exercise
Type 2 DM
•↓Blood glucose & HbA1c
• Improve glucose tolerance
•↓Insulin requirement

Acute stimulation of muscle glucose transport
Acute enhancement of insulin action
Long term upregulation of the insulin signaling pathway resulting from regular exercise
Exercise Regulates BS thru 3 Distinct Mechanisms
Evaluation Before Exercise & Exercise Testing

Glycemic control
Physical limitation
Medication
Type & severity of complication
• Cardiovascular disease
• Diabetic neuropathy
• Diabetic nephropathy
• Diabetic retinopathy
Evaluation before starting exercise

ADA criteria for graded exercise testing with ECG monitoring before ↑ physical activity
Age > 40 yr
• Type 1 or type 2 DM of > 10 yr duration
• HT
• Smoking
• Dyslipidemia
• Proliferative or preproliferative retinopathy
• Nephropathy including microalbuminuria
Age > 30 yr and
• Known or suspected CAD, cerebeovascular disease, PVD)
• Autonomic neuropathy
• Advanced nephropathy with renal failure
Any of the following regardless of age
ADA statements, Exercise and Type 2 Diabetes. Diabetic Care 27. 2004

General exercise recommendation

Primary purpose
Endurance training
Type 1 DM
• Cardiovascular wellness
Type 2 DM
• Improve glucose disposal
• Weight loss/maintenance
Resistance training
Improve muscular
strength & endurance
Intensity
• Low-to-moderate intensity
(40-60% VO2 max)
Endurance training

Method Comparison of Exercise Intensity
Comparing Aerobic Exercise Intensity
%HRmax
%HRR/%VO2max
RPE
Intensity
<35
<20
<10
Very light 35-54
20-39
10-11
Light
55-69
40-59
12-13
Moderate 70-89
60-84
14-16
Hard
> 90
>85
17-19
Very hard 100
100
20
Maximal
METs
1-3
3-6
> 6

Intensity
• Low intensity
• Facilitate metabolic change
• May not meet minimum threshold for improvement cardio-respiratory fitness
• More comfortable and enhance adherence
• Lessening musculoskeletal injury & foot trauma
Endurance training

Duration
• 20-60 min/d continuous or accumulated in bolus of at least 10 min
• 150 min/wk of moderate intensity exercise
• Accumulate a minimum of 1,000 kcal/wk
Endurance training

Mode
• Easily maintained
• Require little skill
• Proper for exercise limitations
• Combined with personal interest & goal
Endurance training

Mode
• Walking is the most convenient low-impact mode
• Pt. with peripheral neuropathy or degenerative arthritis may require non-weight bearing activities (e.g. stationary cycling, aquatic activities)
Endurance training

Endurance training
Frequency
• 3-7 d/wk
• ≤ 2 consecutive days of physical inactivity should be allowed (72 hr effects of exercises)
• Daily exercise
• Diabetes pt. taking insulin • Reduce difficulty of balancing caloric needs &
insulin dosage
• Obese pt.

Rate of progression
• Depend on
• Age
• Functional capacity
• Medical & clinical status
• Personal preference & goals
• Initially should focus on frequency & duration rather than intensity
Endurance training

Resistance Training
≥ 2 d/wk with at least 48 hr separating exercise session
2-3 set of 12-15 repetition at 60-80% 1-RM
8-10 multi-joint exercises of major muscle groups in same session or session split into selected muscle group

124
Conditioning Exercise

Resistance training
Prevent exacerbated BP response in cases of poor control
• ↓Intensity of lifting (low wt high reps)
• Not exercise to point of maximum exertion
• Minimizing or Avoiding
• Sustained gripping
• Isometric contraction
• Valsalva maneuver (counting trick)

126
Balance Exercises
Walk Heel to Toes

Stretching Exercise

Flexibility Exercises Less collagen property in Pre-diabetics
More stiff after inflammation
Heal slower in case of tendinitis
1 out of 3 shoulder tendinitis turn to frozen shoulder
Daily stretching is required
Poor flexibility cause more muscle strain and tendinitis

129
Static Stretching
Slow stretch muscle until full ROM, hold for 15-20 sec. (5-60s)
Decreased possibility of exceeding normal ROM
Less stimulation of stretch reflex
Lower energy requirements
Less muscle soreness

Acute glycemic response Hypoglycemia
M/C problem for pt. with DM who exercise
Occur mainly in pt. taking insulin or sulfonylurea
Hyperglycemia and ketosis
Risk of exercise

Prevention & Treatment of Abnormal Blood Glucose
Before & After Exercise
Abnormal blood glucose before & after exercise
Preexercise hypoglycemia
Preexercise hyperglycemia
Postexercise hypoglycemia
Postexercise hyperglycemia

Timing of exercise
• Not exercise during peak insulin action
• Short acting : 1 hr
• Intermediate and long acting : 2.5 hr
• Exercise before bed is not recommended
• Similar timing of daily exercise
Prevention & treatment of abnormal blood glucose

Prevention & treatment of abnormal blood glucose
Monitor blood glucose before & after exercise, especially when beginning or modifying exercise program
Adjust carbohydrate intake & medications based on blood glucose and exercise duration

Pre-exercise Hypoglycemia Prevention
Blood glucose Low intensity & short duration exercise
Moderate intensity & moderate duration exercise
Moderate intensity & long duration exercise
< 80 mg/dl 10-15 g carb 25-30 g carb 50 g carb
80-100 mg/dl 10-15 g carb 10-15 g carb 25-50 g car
> 100 mg/dl No extra carb No extra carb No extra carb

Avoid injecting insulin into exercising limbs, use abdominal wall
Exercise with partner or under supervision to ↓problem associated with hypoglycemic event
Prevention & treatment of abnormal blood glucose

Special consideration for specific complication

Special consideration for specific complication
Autonomic neuropathy
Peripheral neuropathy\
Nephropathy Retinopathy

Autonomic Neuropathy
Risk
• Choronotropic incompetence
• Blunt HR & BP response
• Silent ischemia
• Hypo-/ hypertension after vigorous activity
Recommendation
• Avoid high intensity exercise
• Use RPE to assess intensity
• Monitor ECG, BP

Autonomic neuropathy
Risk
• Prone to dehydration, Thermoregulatory dysfunction
Recommendation
• Maintain hydration • Avoid extreme
environment
Risk
• Hypoglycemic unawareness
Recommendation
• Careful blood glucose monitoring

Peripheral neuropathy
Risk
• Orthopedic injury
• Foot trauma/ulcer
Recommendation
• Non-wt. bearing exercise (swimming, cycling)
• Proper foot care and footwear

Nephropathy
Risk
• Sustained ↑BP is related to worsening nephropathy
• Exercise increased proteinuria
Recommendation
• Avoid activities that involved sustained↑ BP • High intensity
aerobic or resistance exercises
• Valsalva maneuver
Risk
• Effects of fluid balance change on BP
Recommendation
• Maintain hydration

Retinopathy
Risk
• Exercise increase systemic & retinal BP risk for retinal hemorrhage
Recommendation
• Avoid • High intensity
aerobic or resistance exercise
• Head-down activities
• Arm-overhead

Exercise is a major therapeutic modality for DM
Favorable changes in glucose tolerance and insulin sensitivity usually deteriorate within 72 hr of the last exercise session
Regular exercise is imperative to sustained glucose lowering effects and improve insulin sensitivity
Modification to exercise type and intensity may be necessary for pt. with diabetic complications
Conclusion

References ACSM’s Guidelines for Exercise Testing and Prescription, 2009
ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription, 2005
ADA statements, Exercise and Type 2 Diabetes, 2004
ACSM position stand, Exercise and Type 2 Diabetes, 2000
JK. Ehrman. Clinical exercise physiology, 2009
RA. Defronzo. International textbook of Diabetes Millitus, 2004
สมาคมผูใ้ห้ความรู้โรคเบาหวาน. การออกก าลงักายกบัโรคเบาหวาน, 2551

Thank you for Your Attention