exos certification plyomedball - final (3)© 2014 athletes’ performance, inc. 3 transfer to...
TRANSCRIPT

© 2014 Athletes’ Performance, Inc. 1
MEDICINE BALL
THEORY AND APPLICATION
2© 2014 Athletes’ Performance, Inc.
Define medicine ball training and list the four primary components
Identify and describe each sub-component within the four primary components of
medicine ball training
Describe the performance and injury prevention benefits associated with
medicine ball training
Identify and design effective medicine ball programming relative to individual
differences and session demand
LEARNING OBJECTIVES

© 2014 Athletes’ Performance, Inc. 2
3© 2014 Athletes’ Performance, Inc.
What do we think about when we hear rotational power and kinetic linking?
Transfer to light objects…
© 2014 Athletes’ Performance, Inc. 3
Transfer to heavier objects…
Transfer through an implement…

© 2014 Athletes’ Performance, Inc. 4
Transfer into an opponent…
MEDICINE BALL: DEFINED

© 2014 Athletes’ Performance, Inc. 5
9© 2014 Athletes’ Performance, Inc.
Drills involving implement propulsion, aimed at linking optimal strength and speed during fundamental movement patterns
DEFINING MEDICINE BALL TRAINING
Characterized by the projection of an implement in a ballistic manner
10© 2014 Athletes’ Performance, Inc.
Ballistic movements involve the transfer of force into an object, implement, or opponent

© 2014 Athletes’ Performance, Inc. 6
11© 2014 Athletes’ Performance, Inc.
Ballistic movements are dependent on the generation and transfer of force from proximal segments to distal segments
12© 2014 Athletes’ Performance, Inc.
MEDICINE BALL COMPONENTS
STANCE
Dictates the complexity of the
motor task and magnitude of force
that can be generated
DIRECTION
Dictates the dominant force
vectors and sequence of force
transfer through the body
INITIATION
Dictates contraction type and the
resulting speed-strength quality
adaptation
BALL
Load/type of ball is associated with
the initiation and speed-strength
quality adaptation

© 2014 Athletes’ Performance, Inc. 7
13© 2014 Athletes’ Performance, Inc.
MEDICINE BALL: STANCE
TALL KNEELING
HALFKNEELING
BASE POSITION
SPLIT POSITION
SINGLE LEG
Action takes place from a kneeling position
where both knees are on the ground
Action takes place from a position where the back knee is on the ground and the front foot is on the ground in a linear orientation
Action takes place from a position where
feet are parallel and shoulder width apart
Action takes place from a split squat position
where the feet are split forward and back
Action takes place with one leg on the
ground an the free leg in a flexed position
14© 2014 Athletes’ Performance, Inc.
Tall Kneeling Horizontal Chest Pass Base Position Horizontal Chest Pass
STANCE01

© 2014 Athletes’ Performance, Inc. 8
15© 2014 Athletes’ Performance, Inc.
Split Position Horizontal Chest Pass Single Leg Horizontal Chest Pass
STANCE01
16© 2014 Athletes’ Performance, Inc.
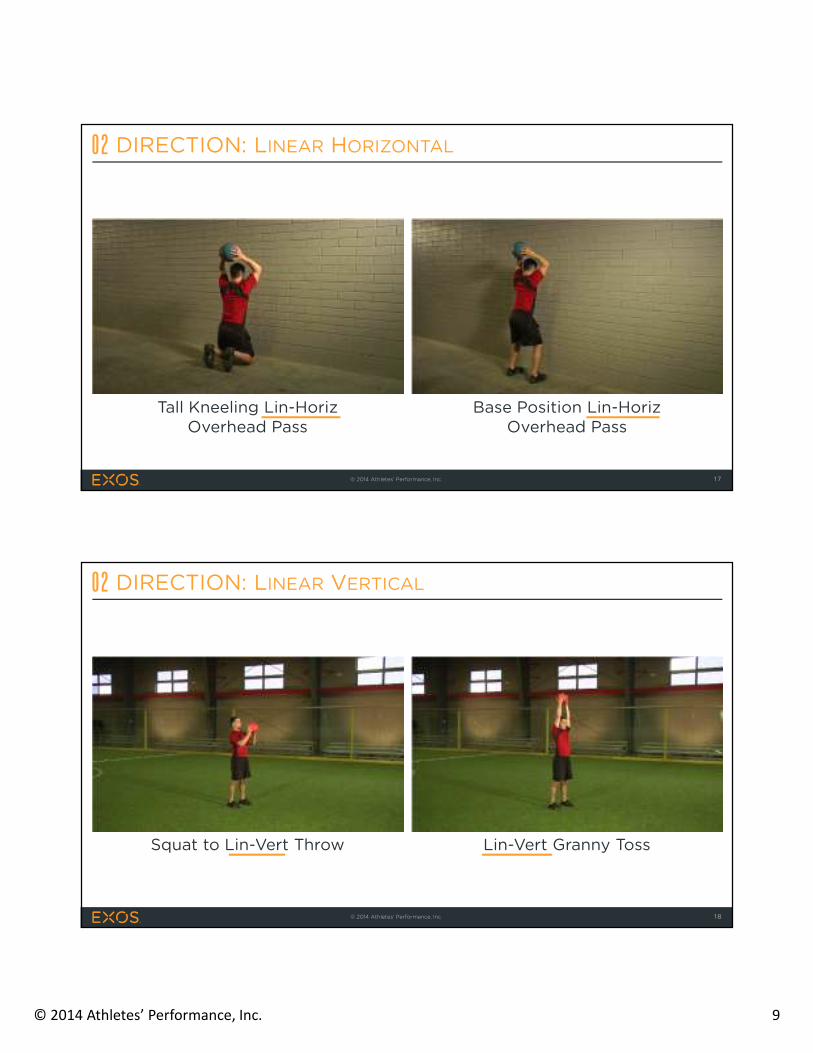
MEDICINE BALL: DIRECTION
Action takes place within
sagittal plane with an
emphasis on vertical or
horizontal motion
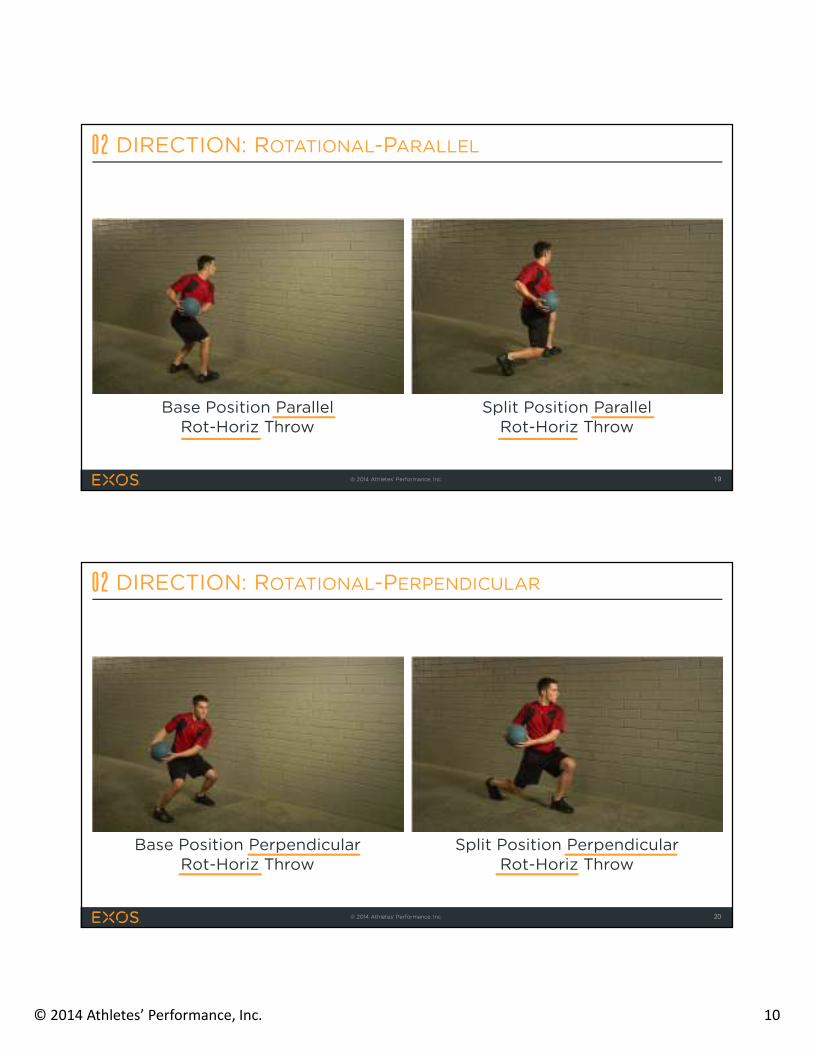
Action takes place within
transverse plane with a
parallel orientation to a wall
and horizontal emphasis
Action takes place within
transverse plane with a
perpendicular orientation to a
wall and horizontal emphasis
LINEAR
ROTATIONALParallel
ROTATIONALPerpendicular
© 2014 Athletes’ Performance, Inc. 9
17© 2014 Athletes’ Performance, Inc.
Tall Kneeling Lin-HorizOverhead Pass
Base Position Lin-HorizOverhead Pass
DIRECTION: LINEAR HORIZONTAL02
18© 2014 Athletes’ Performance, Inc.
Squat to Lin-Vert Throw Lin-Vert Granny Toss
DIRECTION: LINEAR VERTICAL02
© 2014 Athletes’ Performance, Inc. 10
19© 2014 Athletes’ Performance, Inc.
Base Position Parallel Rot-Horiz Throw
Split Position Parallel Rot-Horiz Throw
DIRECTION: ROTATIONAL-PARALLEL02
20© 2014 Athletes’ Performance, Inc.
Base Position Perpendicular Rot-Horiz Throw
Split Position Perpendicular Rot-Horiz Throw
DIRECTION: ROTATIONAL-PERPENDICULAR02
© 2014 Athletes’ Performance, Inc. 11
21© 2014 Athletes’ Performance, Inc.
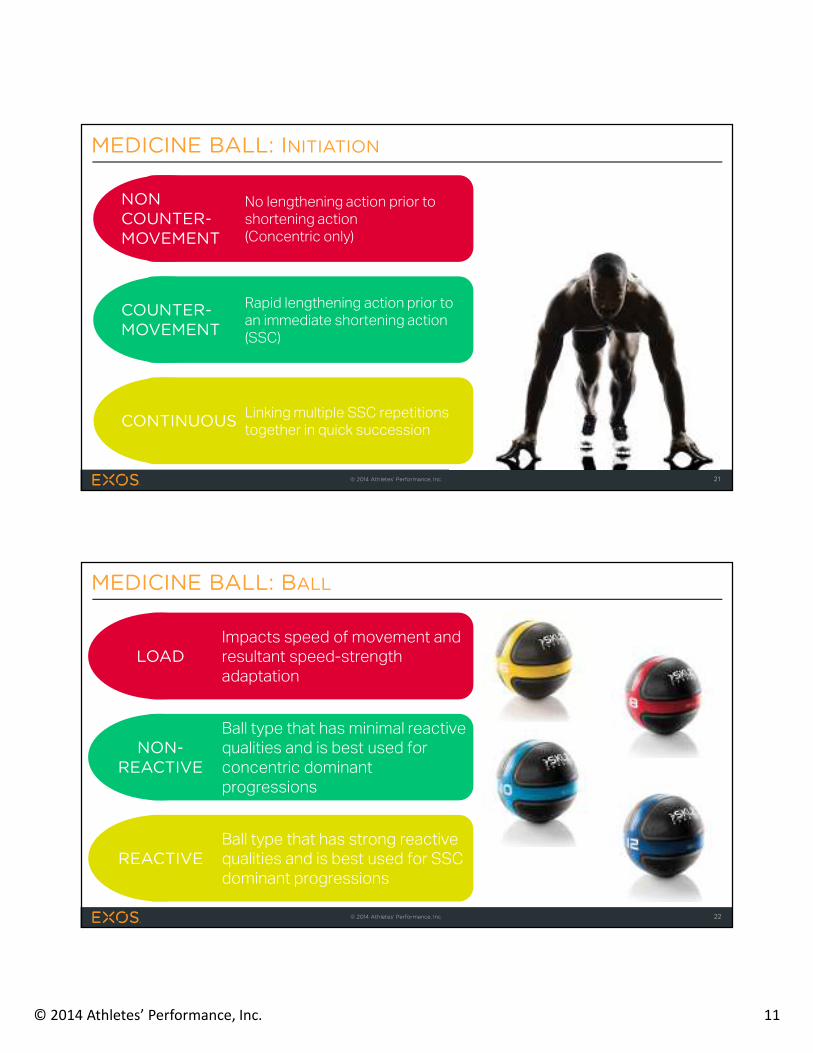
MEDICINE BALL: INITIATION
No lengthening action prior to
shortening action
(Concentric only)
Rapid lengthening action prior to
an immediate shortening action
(SSC)
Linking multiple SSC repetitions
together in quick succession
COUNTER-MOVEMENT
CONTINUOUS
NON COUNTER-MOVEMENT
22© 2014 Athletes’ Performance, Inc.
MEDICINE BALL: BALL
LOAD
NON-REACTIVE
REACTIVE
Impacts speed of movement and
resultant speed-strength
adaptation
Ball type that has minimal reactive
qualities and is best used for
concentric dominant
progressions
Ball type that has strong reactive
qualities and is best used for SSC
dominant progressions
© 2014 Athletes’ Performance, Inc. 12
23© 2014 Athletes’ Performance, Inc.
List the 4 primary components of medicine
ball training and the associated 3-5 sub-
components
Write down 3-5 different medicine ball
training movements using the appropriate
labeling
CHECK FOR LEARNING 01
OPTIMIZING TRANSFER

© 2014 Athletes’ Performance, Inc. 13
PERFORMANCE ENHANCEMENT
26© 2014 Athletes’ Performance, Inc.
Develop three dimensional power using integrated upper body
and total body movements that emphasize the ability to
generate and resist rotational forces
MEDICINE BALL: PRIMARY GOAL
© 2014 Athletes’ Performance, Inc. 14
27© 2014 Athletes’ Performance, Inc.
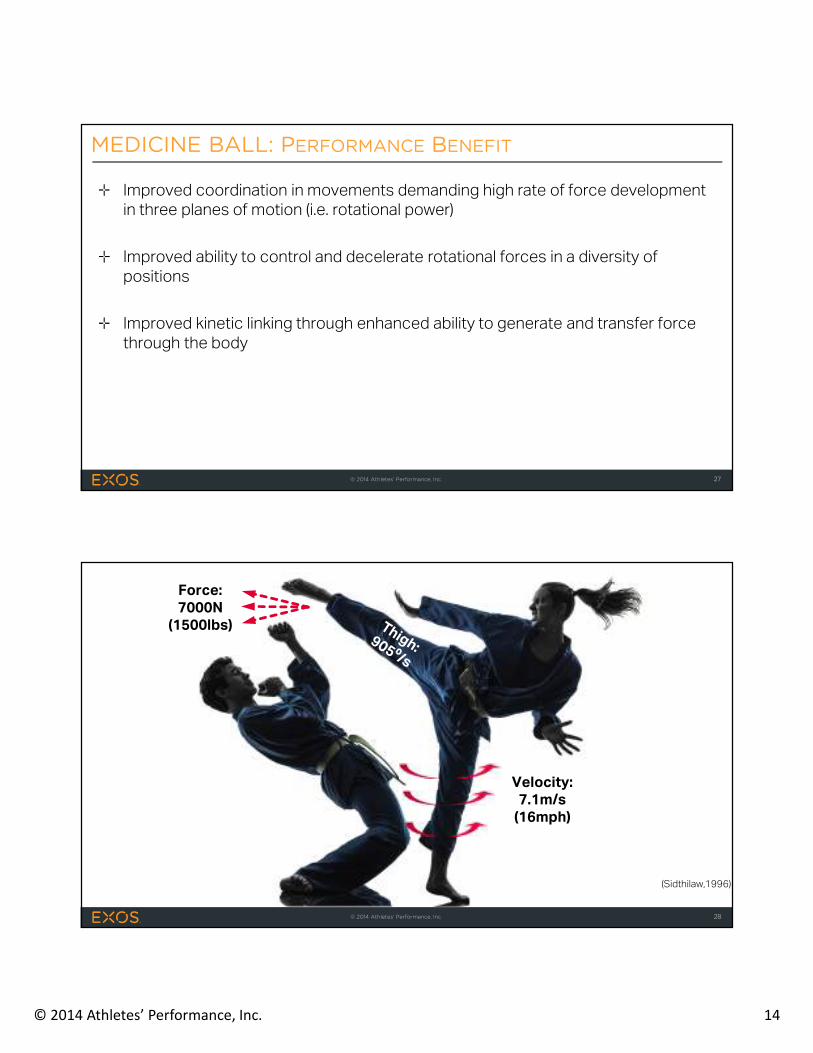
Improved coordination in movements demanding high rate of force development
in three planes of motion (i.e. rotational power)
Improved ability to control and decelerate rotational forces in a diversity of
positions
Improved kinetic linking through enhanced ability to generate and transfer force
through the body
MEDICINE BALL: PERFORMANCE BENEFIT
28© 2014 Athletes’ Performance, Inc.
Force:7000N
(1500lbs)
Velocity:7.1m/s
(16mph)
(Sidthilaw,1996)

© 2014 Athletes’ Performance, Inc. 15
29© 2014 Athletes’ Performance, Inc.180lbs = 81.81kgs = 800N
FT = 984N(221lbs)
Hip: 7140/s
Shoulder: 9370/s
Bat Speed:31m/s
(69mph)
(Welch et al., 1995)
(Szymanski et al., 2007)
Adding total body/rotational med-ball training to a periodized resistance program results in superior rotational strength and rotational med-ball throwing performance compared to the same program without

© 2014 Athletes’ Performance, Inc. 16
During conventional barbell training the last 24-52% of the movement can be spent decelerating the bar. This does not occur during medicine ball training due to the ballistic nature and the ability to release the ball.
(Newton & Kraemer, 1994; Newton et al., 1996)
INJURY PREVENTION
© 2014 Athletes’ Performance, Inc. 17
33© 2014 Athletes’ Performance, Inc.
Decrease risk of injury through increased tolerance to stretch
loads at various speeds, loads, and directions
MEDICINE BALL: SECONDARY GOAL
34© 2014 Athletes’ Performance, Inc.
Improved ability to transfer energy through the joints and minimize energy leaks
- Prevents movement compensations and optimizes sustainability
Improved ability to control rotation and decelerate during total-body rotational
movements
- Striking, Throwing, Kicking, Cutting, Running
(Boden et al., 2000 and Stodden et al., 2008)
MEDICINE BALL: INJURY PREVENTION BENEFIT

© 2014 Athletes’ Performance, Inc. 18
↓ Energy leaks = ↑ kinetic linking
(optimal transfer of force)
36© 2014 Athletes’ Performance, Inc.
Trunk control and the ability to re-stabilize after a lateral force has been removed is predictive of knee
injuries in collegiate athletes
(Zazulak et al., 2007)
© 2014 Athletes’ Performance, Inc. 19
37© 2014 Athletes’ Performance, Inc.
Write down 3-5 sentences describing the role of
medicine ball training in improving performance
in rotation dominant movements (ex. throwing)
Write down 3-5 sentences describing the role of
medicine ball training in preventing non-contact
injuries (ex. ACL injury)
CHECK FOR LEARNING 02
PROGRAMMING
© 2014 Athletes’ Performance, Inc. 20
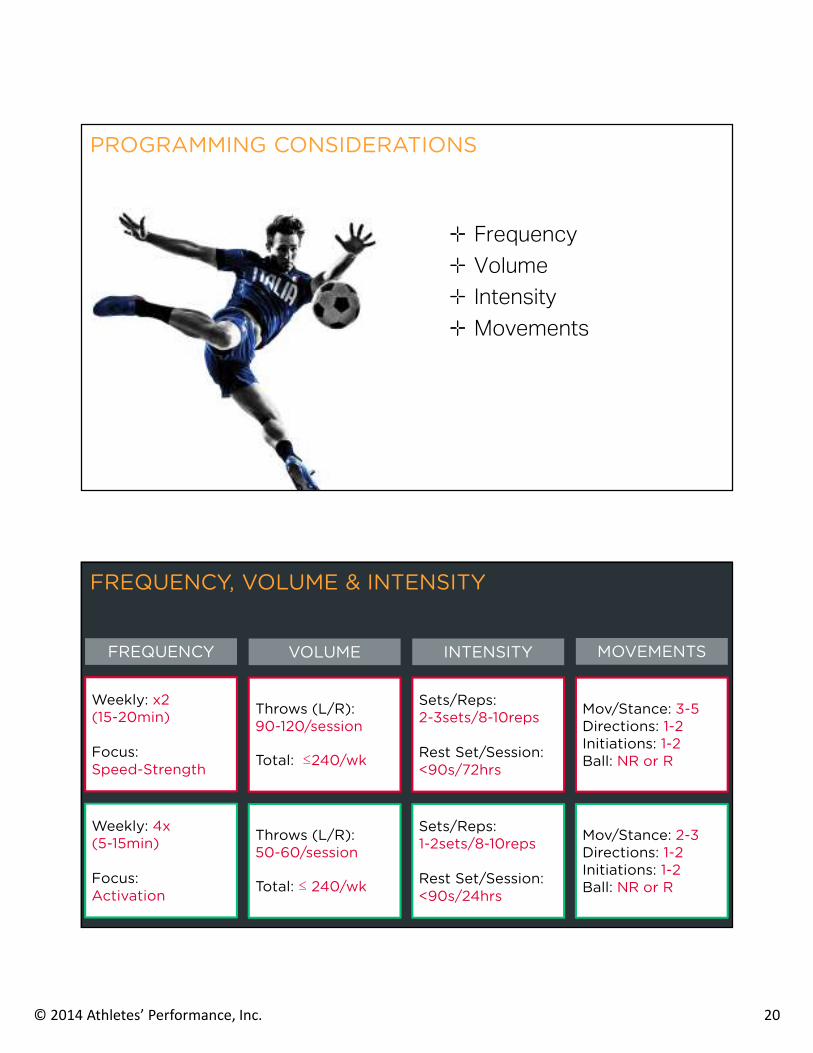
PROGRAMMING CONSIDERATIONS
Frequency
Volume
Intensity
Movements
Throws (L/R):90-120/session
Total: ≤240/wk
Throws (L/R):50-60/session
Total: ≤ 240/wk
VOLUME
Sets/Reps:2-3sets/8-10reps
Rest Set/Session:<90s/72hrs
Sets/Reps:1-2sets/8-10reps
Rest Set/Session:<90s/24hrs
Mov/Stance: 3-5Directions: 1-2Initiations: 1-2Ball: NR or R
Mov/Stance: 2-3Directions: 1-2Initiations: 1-2Ball: NR or R
INTENSITY MOVEMENTS
Weekly: x2 (15-20min)
Focus:Speed-Strength
Weekly: 4x(5-15min)
Focus:Activation
FREQUENCY
FREQUENCY, VOLUME & INTENSITY

© 2014 Athletes’ Performance, Inc. 21
INTENSITY
INTENSITY
SINGLE LEG POSITION
SPLIT POSITION
BASE POSITION
LINEARVertical to Horizontal
ROTATIONALParallel
ROTATIONAL Perpendicular
Lin-Horiz Chest PassLin-Horiz Overhead Pass
Lin-Horiz Chest PassLin-Horiz Overhead Pass
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
Lin-Horiz Chest PassLin-Horiz Overhead Pass
Lin-Vert Squat to Throw
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
Lin-Horiz Chest PassLin-Horiz Overhead Pass
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
Rot-Horiz Throw-HipRot-Horiz Throw-Shld
TALL KNEELING HALF KNEELING
METHODS
MED-BALL: Linear Emphasis MED-BALL: Rotational Emphasis
Novice Athlete (4x per week)
Movement 1:-Lin-Vert Squat to Throw-CM/Non-Reactive Ball-2 x 10 repetitions
Movement 2:-Base Position Lin-Horiz Chest Pass-Single/Reactive Ball-2 x 10 repetitions
Movement 3:-Split Position Lin-Horiz Chest Throw-NCM/Non-Reactive Ball-2 x 5 repetitions each
Total Throws: 60
Advanced Athlete (2x per week)
Movement 1:-Base Position Parallel Rot-Horiz Throw-NCM/Non-Reactive Ball-2 x 10 repetitions each
Movement 2:-Split Position Parallel Rot-Horiz Throw-Continuous/Reactive Ball-2 x 5 repetitions each
Movement 3:-Base Position Perp. Rot-Horiz Throw-Continuous/Reactive Ball-2 x 10 repetitions each
Total Throws: 100
EXAMPLE PROGRAMMING: MEDICINE BALL
© 2014 Athletes’ Performance, Inc. 22
43© 2014 Athletes’ Performance, Inc.
Create a single 10 min medicine ball program
with a rotational emphasis based on 4x week
volume load considerations (Note: Only create the medicine ball portion and include as much detail on volume and intensity as possible)
CHECK FOR LEARNING 03
CLOSING
© 2014 Athletes’ Performance, Inc. 23
45© 2014 Athletes’ Performance, Inc.
Stance (Tall Kneeling – Base – Single Leg)
- More Stable to Less Stable
Direction (Linear – Parallel - Perpendicular)
- General to Specific (Vertical & Horizontal)
Initiation (NCM – CM – Continuous)
- Low Force to High Force (Progression & Continuum)
Ball (Non-Reactive Ball – Reactive Ball)
- Low Load (4-6lbs) to High Load (18-20lbs)
GUIDELINES
46© 2014 Athletes’ Performance, Inc.
Stance is selected based on the
level of athlete and the specific
movement characteristics in
need of development (movement
skills & sport)
STANCE

© 2014 Athletes’ Performance, Inc. 24
47© 2014 Athletes’ Performance, Inc.
Movement directions are selected based on the
level of athlete (linear to rotational) and the
specific directional force characteristics in need
of development (movement skills & sport)
DIRECTION
48© 2014 Athletes’ Performance, Inc.
Movement initiations (NCM to Continuous) and ball (Non-
Reactive to Reactive) are selected based on the level of
athlete and the specific speed-strength characteristics in
need of development (strength & movement skills)
INITIATION/BALL

© 2014 Athletes’ Performance, Inc. 25
50© 2014 Athletes’ Performance, Inc.
Boden, B. P., Dean, G. S., Feagin Jr, J. A., & Garrett Jr, W. E. (2000). Mechanisms of anterior cruciate ligament injury. Orthopedics, 23(6), 573-578.Newton, R. U., & Kraemer, W. J. (1994). Developing explosive muscular power: Implications for a mixed methods training strategy. Strength & Conditioning Journal, 16(5), 20-31.Newton, R. U., Kraemer, W. J., Häkkinen, K., Humphries, B. J., & Murphy, A. J. (1996). Kinematics, kinetics, and muscle activation during explosive upper body movements. Journal of Applied Biomechanics, 12, 31-43.Sidthilaw, S. (1996). Kinetic and kinematic analysis of Thai boxing roundhouse kicks. Oregon State University Dissertation.
Stodden, D. F., Campbell, B. M., & Moyer, T. M. (2008). Comparison of trunk kinematics in trunk training exercises and throwing. The Journal of Strength & Conditioning Research, 22(1), 112-118.Szymanski, D. J., Szymanski, J. M., Bradford, T. J., Schade, R. L., & Pascoe, D. D. (2007). Effect of twelve weeks of medicine ball training on high school baseball players. The Journal of Strength & Conditioning Research, 21(3), 894-901.Welch, C. M., Banks, S. A., Cook, F. F., & Draovitch, P. (1995). Hitting a baseball: A biomechanical description. Journal of Orthopaedic & Sports Physical Therapy, 22(5), 193-201.Zazulak, B. T., Hewett, T. E., Reeves, N. P., Goldberg, B., & Cholewicki, J. (2007). Deficits in neuromuscular control of the trunk predict knee injury risk a prospective biomechanical-epidemiologic study. The American journal of sports medicine, 35(7), 1123-1130.
APPENDIX