fat studies in mental health training aamft 2012 drs. sheila addison & michael loewy alliant...
TRANSCRIPT

Fat Studies in Mental Health Training
AAMFT 2012
Drs. Sheila Addison & Michael LoewyAlliant International University
With slides borrowed from Drs. Linda Bacon, Barbara Altman Bruno, Deb Burgard, Glenn
Gaesser, Joanne Ikeda & Esther Rothblum

Activity 1
• Write 4 words or phrases that you associate with “fat people.”
• Don’t censor yourself - write whatever comes to mind.

Activity 2
• Write 4 words or phrases that you associate with your own body.
• Don’t censor yourself - write whatever comes to mind.

What exactly does “fat” look like?
Take a moment to picture what a person looks like who is underweight, normal
weight, overweight, obese, morbidly obese (BMI categories).
BMI slideshow project © Kate Harding, 2007
http://www.shakesville.com/2007/09/why-bmi-is-crock-in-pictures.html

What’s my BMI? 1 & 2

What’s my BMI? 3 & 4

What’s my BMI? 5 & 6

What’s my BMI? 7 & 8

What’s my BMI? 9 & 10

What’s my BMI? 11, 12, 13
What’s my BMI? 14 & 15

What’s my BMI? 1 & 2
5’0, 130 lbs, BMI 25.4, overweight
5’7, 170 lbs, BMI 26.6, overweight

What’s my BMI? 3 & 4
5’6 1/2, 227 lbs, BMI 36.1, obese5’4, 250 lbs, BMI 42.9, morbidly obese

What’s my BMI? 5 & 6
5’7, 129 lbs, BMI 20.2, normal
6’0, 216 lbs, BMI 29.3 – overweight, 5 lbs below obese
5’4, 150 lbs, BMI 25.7, overweight
5’11, 190 lbs, BMI 26.5, overweight

What’s my BMI? 7 & 8
6’0, 135 lbs, BMI 18.3, underweight, 1 lb below normal
4’11, 120-125 lbs, BMI 24.2-25.2, fluctuates between normal and overweight
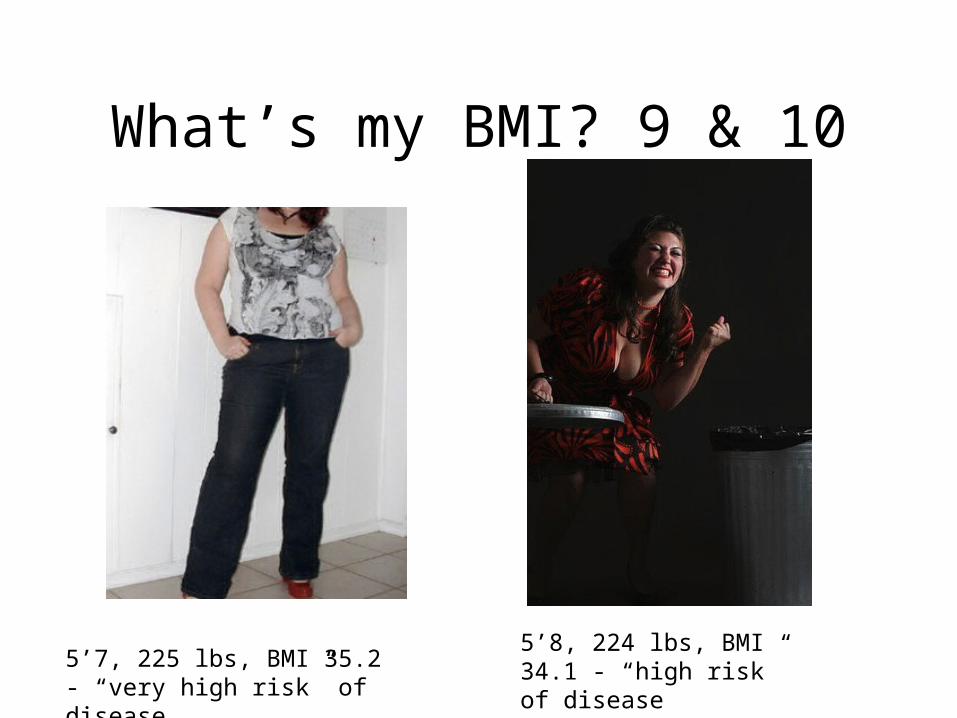
What’s my BMI? 9 & 10
5’7, 225 lbs, BMI 35.2 - “very high risk” of disease
5’8, 224 lbs, BMI 34.1 - “high risk” of disease

What’s my BMI? 11, 12, 13
5’7, 134 lbs, BMI 21, normal
6’1, 200 lbs, BMI 26.4, overweight
5’1 1/2, 200 lbs, BMI 37.2, obese

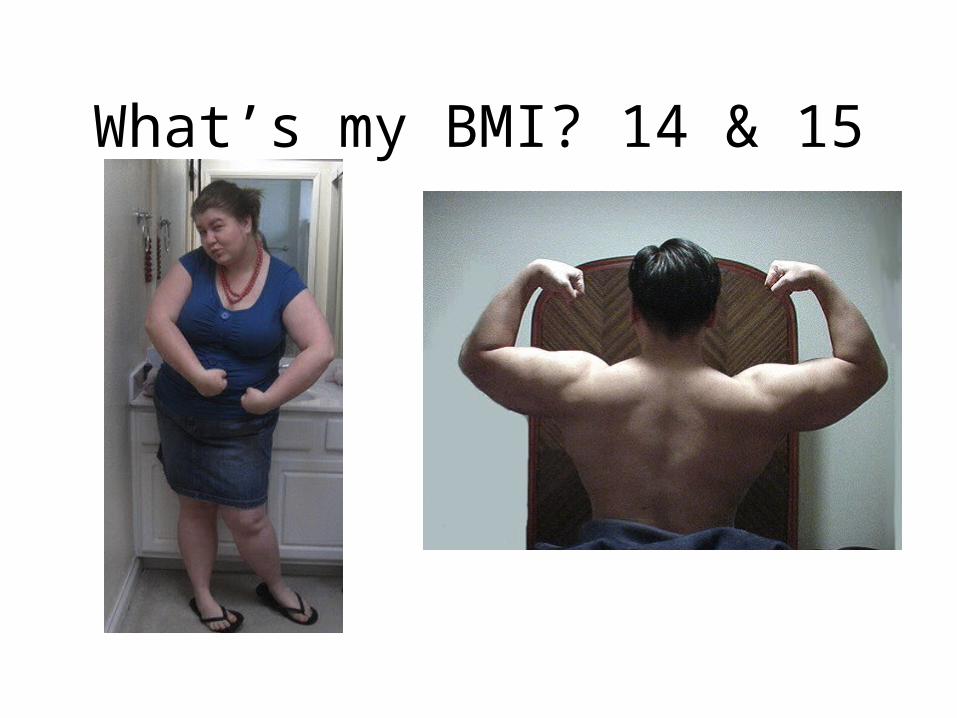
What’s my BMI? 14 & 15
5’7, 280 lbs, BMI 43.8, morbidly obese
5’4, 185 lbs, BMI 31.8, obese

How did you do?
• BMI (body mass index) is weight (in kg) divided by height (in meters) squared
• BMI for “overweight” changed from 27 to 25 in 1998
• 30,500,000 people became “overweight” overnight

How did you do?• BMI is not magic or even
scientific• IT’S JUST ANOTHER
WEIGHT/HEIGHT RATIO• 1998 change was not informed
by empirical research - the change was effectively arbitrary
• 2010 study - BMI poorly predicts health
Schneider, H. J. et. al. (2010) "The Predictive Value of Different Measures of Obesity for Incident Cardiovascular Events and Mortality". Journal of Clinical Endocrinology & Metabolism 95 (4): 1777–85.

How fat is “fat”?
GUESS MARIANNE’S
HEIGHT/ WEIGHT!
Marianne Kirby, co-author of “Lessons from the Fat-o-sphere: Quit Dieting
and Declare a Truce with Your Body”
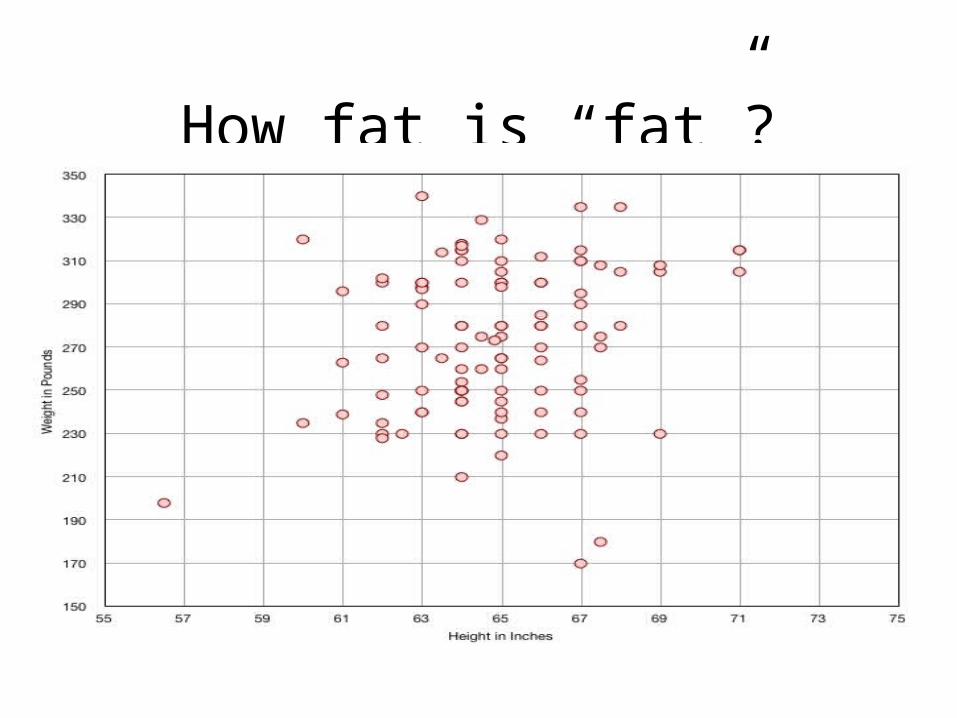
How fat is “fat”?

How fat is “fat”?

How fat is “fat”?Marianne says: So why is this? Is it just that… people have no idea what certain weights look like?
I think that is a really big part of this. The guesses that most boggled my mind were from men who said I looked like their wives and their wives weighed x number of pounds. Those guesses were all under 200 pounds.
There were a lot of guesses that started out, “well, you look just like me so….” and were totally off. But even those guesses, for the most part… were closer to the mark than the guys using their wives’ weights.
So. Either these guys are DESPERATELY bad at a game very, VERY few people are good at, or their wives are lying about their weight.
WHY MIGHT THAT BE?• Shame - about what it means to be X weight
• Stigma - about what X weight looks like/means• Distorted perceptions of self & others

What does this mean for mental health?
• Fat shame and stigma is pervasive - research suggests they have more health effects than actual weight
• Distorted ideas about weight and health are pervasive - culture equates “thin” with “healthy” despite evidence to the contrary
• The weight “loss” and bariatric industries sell us (and our clients) more of these ideas every day at tremendous financial and personal costs
• Yet most weight loss efforts do not succeed• As clinicians, teachers, & supervisors, we are not immune• Self-of-the-therapist: We have bodies, and weight
histories, and feelings about them, which must be addressed.
What does this mean for mental health?
• Our field is currently trying to get on board the “obesity crisis” train because there is $$ to be made– APA Task Force on Obesity– AAMFT - Clinical Updates on bariatric surgery & Childhood
Obesity– ACA - recommends “intensive counseling” for all obese adults and
requires insurers to pay• Body size is a dimension of diversity; sizeism is a social
justice issue• Our students, teachers, superviors, & clinicians badly need
training in a weight-neutral approach • Little or nothing is offered in most mental health programs

Fat Studies comes to mental health
• In 2009, Alliant International University began offering a 1-unit elective, “Fat Acceptance and Health at Every Size,” to its PhD and PsyD Psychology students
• Offered at the San Francisco campus as a 2-day weekend intensive
• Students were asked to do all assigned reading prior to class
• Based on ideas from “Fat Studies” classes taught in other disciplines elsewhere

“A Fat Rant” - Joy Nash

CREATION OF FAT STUDIES
• Marilyn Wann, 1998

FAT STUDIES IN THE ACADEMY
• 2006 Fat and the Academy Conference, Smith College, co-organized by Sheana Director

THE NEW FAT STUDIES: PERFORMANCE
• Fat burlesque• Fat cheerleaders
• Fat synchronized swimming• …and many others

THE NEW FAT STUDIES
• “Weight discrimination will continue to thrive so long as efforts to end it focus on changing people’s bodies rather than changing people’s minds.”
• Marilyn Wann

Barbara Altman Bruno, Ph.D. 2008
A brief history of weight research
• Early research on weight loss-1944: Ancel Keys begins experiment
• 36 healthy young men
• 3 months 3,500 cal/day
• 6 months half rations (1750 cals), mostly whole grains and root vegetables, a little meat and dairy; adequate vitamins, minerals, and protein
A brief history of weight research• All lost ¼ of starting weight
• Depression, lethargy, irritability, loss of libido, indifference, obsession with food
• Two emotional breakdowns leading to leaving, another chopped off fingertip
• Last 3 months refeeding. Men miserable despite 4,000 cal/day Finally regained weight, less muscle and more fat
• Nine months after regain, finally regained lost muscle
Barbara Altman Bruno, Ph.D. 2008
Barbara Altman Bruno, Ph.D. 2008
E.A. Sims studies 4 college students, later groups of prisoners trying to gain 20-30 lbs. One needed 7,000 cal/day to maintain wt. gain. All doubled normal daily intake of food and needed 2,000 cal/day extra to maintain extra weight.
Lethargy, apathy.
“Essentially all of the subjects ... have lost weight ...with the same alacrity...as that with which most of our obese patients return to their usual and customary weight after weight loss.”
A brief history of weight research
- 1972: National Association to Advance Fat Acceptance
Vivian Mayer and Judy Freespirit. Mayer presented the following to women of LA radical therapy collective:
• Biology, not eating habits, is the main cause of fat.
• Health problems of fat people are not inherently due to fat, but the result of stress, self-hatred, and chronic dieting.
• Weight loss efforts damage health, almost never “succeed” except temporarily, and should not be used.
• Food binges are a natural response to chronic dieting.

1972: National Association to Advance Fat Acceptance
“The role of a radical [feminist] therapist is to help fat women feel good about themselves as fat women and stop trying to lose weight. To accomplish this, radical therapists should learn and teach accurate information about fat women's health and nutrition. They should provide emotional support for women on binges to continue eating and stop feeling guilty.”

WEIGHT AND INCOME - FAT IS A SOCIAL JUSTICE ISSUE
• Fatness is highly correlated with poverty. Fatness and poverty can often be used as synonyms
THIS IS WHAT PEOPLE ASSUME:POVERTY --------> FATNESS
First you are poor and this causes you to become fat
BUT THIS IS WHAT SOME RESEARCH SHOWS:FATNESS --------> POVERTY
First you are fat and this causes you to become poor
• “While there is evidence that poverty is fattening, a stronger case can be made for the converse: fatness is impoverishing” (Glen Gaesser, Fat Studies Reader)
Socioeconomic Status (SES)• Consider type 2 diabetes (the disease most highly associated
with weight)– Poverty and marginalization are much more strongly
associated with type 2 diabetes than weight.
McDermott, Soc. Sci. Med. 1998;47(9):1189Wamala, et al., Diabetes Care. 1999;22(12):1999

WEIGHT BIAS IN EMPLOYMENTStereotypes of fat (150 lb) and thin (120 lb) college women applying for jobs
when the job resumé was identical:
On one resumé (sales job), college woman was rated lower on supervisory potential, professional appearance, personal hygiene, and ability to do a physically strenuous job when she was listed as weighing 150 lbs than when the raters saw the IDENTICAL sales resumé but the woman was listed as weighing 120 lbs. For self-discipline, the fatter women was rated more positively. No effect for weight on the other resumé (service job).
Esther D. Rothblum, Carol T. Miller, & Barbara Garbutt (1988). Stereotypes of Obese Female Job Applicants. INTERNATIONAL JOURNAL OF EATING DISORDERS, 7, 277-283.

WEIGHT BIAS IN EMPLOYMENT
Surveyed members of NAAFA for experiences of actual fat people
Compared people who ranged in weight from very fat (50% or more above height and weight charts) to fat (20-49% above height and weight charts) to non-fat (19% or less above height and weight charts) about direct job discrimination and employment-related discrimination they had experienced.
There was a strong relationship between weight and number of reported incidences of employment discrimination, school victimization, concealment of weight (e.g., having a job that primarily involved talking on the telephone), and low self-confidence.
Esther D. Rothblum, Pamela A. Brand, Carol T. Miller, & Helen A. Oetjen (1990). The Relationship Between Obesity, Employment Discrimination, and Employment-Related Victimization. JOURNAL OF VOCATIONAL BEHAVIOR, 37, 251-266.

WEIGHT BIAS IN EMPLOYMENT
Review of weight bias literature in past decades. Fat people are:
• Less likely to be hired• Perceived as having undesirable traits• More harshly disciplined on the job• Given inferior assignments• Paid less• Viewed as liabilities for employee health benefits• Fired for not losing weight
Fikkan, J., & Rothblum, E.D. (2005). Weight bias in employment. In K.D. Brownell, R.M. Puhl, & M.B. Schwartz (Eds.). Bias, stigma, discrimination,
and obesity (pp. 13-28). Guilford Publications.

LEGAL STATUS OF WEIGHT BIAS
• In the U.S., the only places with weight anti-discrimination laws are Michigan, Washington D.C., San Francisco, Santa Cruz, and Madison, WI
• This means that in lawsuits, people have to use other legislation such as the Americans With Disabilities Act (ADA), sex discrimination law, etc.
THE STIGMA OF WEIGHT IN NON-EMPLOYMENT SETTINGS
A large body of research has shown that fat people, esriskspecially girls and women, are stigmatized (negatively evaluated) by:
-Children-Adolescents-Adults-Health Professionals (Nutritionists, Medical Students, Physicians)-LandlordsAnd the stigma of weight holds fat people responsible for their weight
Esther Rothblum (1992). The Stigma of Women's Weight: Social and Economic Realities. FEMINISM & PSYCHOLOGY, 2, 61-73.
WHAT DO WE KNOW ABOUT THE MENTAL HEALTH EFFECTS OF LIVING WITH STIGMA, BIAS, AND DISCRIMINATION?
STIGMA & DISCRIMINATION IS BAD FOR MENTAL HEALTH
• Discrimination based on weight is pervasive.
• Discrimination produces stress.• Stress is a risk factor for disease.• “Feeling fat” has stronger health effects
than being fat.
Puhl, et al., Int J of Obesity, 2008, 32:992. Muennig, et al., Am J Pub Hlth, 2008, 96(9): 1662-8.

WHY CAN'T THEY JUST LOSE WEIGHT?
POOR OUTCOMES OF WEIGHT-LOSS PROGRAMS• Meta-analysi of 50 published studies on weight loss
programs.• Nearly all of them excluded participants who had medical
problems• The typical participant was a white, middle-class woman
who was 48% over her average weight before treatment, who lost 12.8 lbs during a 13-week treatment program and then regained 4.3 lbs over the next 6.5 months
• Consider - would losing 8 pounds make anyone who is “obese” into someone of “normal” weight?
Cogan, J., & Rothblum, E.D. (1993). Outcomes of weight loss programs. Genetic, Social and General Psychology Monographs, 118, 385-415.

Confronting the failure of obesity “treatments”
“...the tremendous body of research employing a great variety of methodologies that has failed to yield any meaningful or replicable differences in the caloric intake or eating patterns of the obese compared to the nonobese.” David Garner and Susan Wooley, Clinical Psychology Review 11, 1991, p. 748
Barbara Altman Bruno, Ph.D. 2008

Confronting the failure of obesity “treatments”
New England Journal of Medicine “Losing weight: an ill-fated new year’s resolution” Editorial: Kassirer and Angell, 1/1/98
“Given the enormous social pressure to lose weight, one might suppose there is clear and overwhelming evidence of the risks of obesity and the benefits of weight loss. Unfortunately, the data linking overweight and death, as well as the data showing the beneficial effects of weight loss, are limited, fragmentary, and often ambiguous.”
META-ANALYSES SHOW - 95-98% OF WEIGHT LOSS EFFORTS FAIL Barbara Altman Bruno, Ph.D. 2008
DIETING HURTS MENTAL HEALTH?
• “Reinterpreting fat people as chronic dieters puts the psychology of obesity in a whole new light. If dieting is the crucial variable, then the fat do not eat because they hurt inside; rather, they hurt because they are trying not to eat, to make their bodies conform to social norms.” P. 34, The Dieter's Dilemma, Bennett & Gurin 1983

50
RISKS OF WEIGHT LOSS
• “Obesity has health risks. But the quest for weight loss is also a risky venture, and those risks include injury and death from dieting, weight loss, and attempted weight loss.”
Berg. Health Risks of Weight Loss, 3rd Ed. 1995.
51
Health Risks of Food Restriction and Weight Loss
• Inadequate nutrient intake
• Anemia• Headache• Fatigue/weakness• Cold intolerance• Muscle cramps• Amenorrhea
• Cardiac arrhythmias• Gallstones• High cholesterol• Decreased sex drive• Nausea• Diarrhea or
constipation• Death

52
Psychological Risks ofChronic Dieting
• Preoccupation with food, eating, & weight
• Increased response to external vs. internal eating cues
• Mood swings• Irritability
• Poor self-image• Disordered eating• Apathy/lethargy• Narcissism• Guilt• Depression

53
Consequences of RestrictingFood Intake
• Ignore/distrust hunger and satiety • Rely on external cues• Develop perfectionist tendencies
• On/off diet• Judge foods as good/bad
• Tendency to binge

Dieting/Weight Cycling• Dieting increases cortisol which triggers
inflammation.• Attempts to lose weight typically result in weight
cycling• Weight cycling results in increased inflammation• Inflammation is a risk factor for many diseases• Best predicting variable for obesity is a history of
dieting - iatrogenic effect?Tomiyama, et al., Psychosom Med, 2010; (72):1.Strohacker, et al., Front. Biosci. 2010;E2:98Lissner , et al., N. Engl. J. Med. 1991;324:1839Diaz, et al., J. Community Health. Jun 2005;30(3):153
“.…Until we have better data about the risks of being overweight and the benefits and risks of trying to lose weight, we should remember that the cure for obesity may be worse than the condition.”
Editors, New Engl. J. Med. 338, No. 1: 52-54, 1998
Basic Principles of Health At Every Size®
1. Accepting and respecting the diversity of body shapes and sizes.
2. Recognizing that health and well-being are multi-dimensional and that they include physical, social, spiritual, occupational, emotional, and intellectual aspects.
3. Promoting all aspects of health and well-being for people of all sizes.
4. Promoting eating in a manner which balances individual nutritional needs, hunger, satiety, appetite, and pleasure.
5. Promoting individually appropriate, enjoyable, life-enhancing physical activity, rather than exercise that is focused on a goal of weight loss.

WHY IS HAES IMPORTANT?• Diets do not work.• There is no intervention that has been shown to be safe
and effective for the majority of people to lose weight and maintain weight loss.
• All people deserve to enjoy the benefits of positive self-image; attention to self-care; enjoyable, appropriately challenging movement; mental and spiritual well-being; and a diverse diet that meets a variety of needs. Not just thin people, or those aspiring to become thin.
• (Many thin people are not practicing HAES either! We just equate health with thinness.)

The things that make people healthier are not dependent on
weight loss!• Good nutrition• Pleasurable physical activity• Social support• Restful sleep• Access to quality medical care• Meaningful work• Physical safety• A clean environment• Social justice• Freedom from stigma

HAES is an approach that evolved from
• The critical and careful reading of thousands of research studies;
• the clinical experience of thousands of healthcare professionals who have grown concerned about traditional weight-centered approaches that do not work;
• the lived experiences of thousands of people who have tried to follow decades of advice about losing weight as a path to health, who ended up less healthy, more discouraged, and more at war with the very bodies they must value enough to sustain the effort to be healthy.

61
Outcomes of Program Based on HAES/Non-Diet Principles
Improved health without harm, dependency, or
discrimination.

62
Evaluating aNon-Diet Intervention
• Comparison of non-diet wellness program to traditional diet program
• Randomized clinical trial with 6 month intervention
• Measures at baseline, 3 months, 6 months, and 1 year
Bacon et al. Int J Obes. 2002;26:854-865.

63
Non-Diet vs. Traditional Diet Intervention
Component Diet Non-Diet
Caloric restriction Yes No
Physical activity Yes Yes
Body/self acceptance No Yes
Internal cues (hunger/satiety) No Yes
Counselor facilitated Yes Yes

64
Selected Outcomes at One YearOutcome Diet Non-DietWeight Change -5.9 kg -0.1 kg
Cholesterol -33 mg/dl -32 mg/dl
LDL-cholesterol -12 mg/dl -9 mg/dl
Triglycerides -45 mg/dl -41 mg/dl
Systolic BP -8.2 mmHg -4.5 mmHg
Dropout Rate 41% 8%

65
Conclusions at One Year
• Traditional diet approach resulted in weight loss at 1 year; non-diet approach did not
• Non-diet and traditional diet approaches produced similar improvements in metabolic fitness, psychological measures, and eating behaviors
• Non-diet approach had significantly lower attrition rate
66
Follow-up at Two Years• Non-diet/HAES group:
– Maintained weight throughout– Sustained improvement in metabolic health
indicators, activity levels, eating behaviors, and psychological measures
• Traditional diet group:– Weight lost at one year was regained– Little sustained improvement
Bacon et al. J Am Diet Assoc. 2005;105:929-936.

67
Conclusions at Two Years
• Non-diet/HAES approach promotes long-term behavior change– Traditional diet approach does not
• Size acceptance, reduction in dieting behavior, and eating based on internal hunger/satiety cues results in improved health indicators

68
Review: HAES Paradigm for Obesity Treatment
• “Initial results of the HAES-based paradigm show some promise in offering a more realistic and long-term approach to weight and lifestyle.” (p. 43)
Miller and Jacob. Obes Rev. 2001;2:37-45.

HAES refocuses us on:
• helping people make sustainable self-care practices a lasting feature of their day-to-day lives
• teaching children to treasure their bodies and look to them for irreplaceable wisdom about making day-to-day decisions
• transforming a culture of weight obsession into a body positive, realistic celebration of our human diversity.

HAES refocuses us on
educating about the health impact of weight stigma, from
• the world of fashion and advertising, to • the doctor's office, to • the adoption agency, to • the airline ticket counter, to • the job interview, to • the online dating ads, to • the clothing store, to • the "I'm so fat" chatter of your best friends.

HAES refocuses us on
getting on with our lives and the hard, rewarding work in front of us.
72
Critical Need for HAES Now!
• Well-established failure of traditional weight loss approaches
• Physical and psychological damage from traditional approaches
• Health improvements NOT dependent on weight loss

73
“Do No Harm”
• Ethically, health care professionals seek treatments that:– Encourage autonomy– Help, not harm– Do not discriminate
• For successful treatment, must shift the traditional weight paradigm

“Do No Harm”
• “In sum, there is little support for the notion that diets lead to lasting weight loss or health benefits.”
– Mann, T. et al (2007) Medicare’s search for effective obesity treatments: Diets are not the answer. American Psychologist 62 (3) 220-233.
– http://mann.bol.ucla.edu/files/Diets_don%27t_work.pdf
• So when clients ask for our support in weight loss efforts, what are the ethical implications of agreeing when we know they will likely fail and have negative physical & mental health consequences ?

“Do No Harm”
• Muenning, 2008– “Our results raise the possibility that some of the
effects of the obesity epidemic are related to the way we see our bodies.”
• Neumark-Sztainer, 2006– “Adolescents using unhealthful weight-control behaviors at Time 1
increased their body mass index by about 1 unit more than adolescents not using any . . . and were at approximately three tiems greater risk for being overweight at time 2. . . (They) were also at increased risk for . . . extreme weight-control behaviors such as self-induced vomiting and use of diet pills, laxatives, and diuretics . . .”

“Do No Harm”
• Puhl and Brownell, 2006, 2007– “More frequent exposure to stigma was related to more
attempts to cope and higher BMI. Physicians and family members were the most frequent sources of weight bias reported. Frequency of stigmatization was not related to current psychological functioning . . .”
– “Participants who believed that weight-based stereotypes were true reported more frequent binge-eating and refusal to diet. . . These findings challenge the notion that stigma may motivate obese individuals to engage in efforts to lose weight.”
“Do No Harm”• Tylka , 2006
– Intuitive eating is associated with psychological well-being. “Women who accept their bodies are more likely to eat healthy.”
• Gailey, 2012– “Fat women who are involved in the size-acceptance
movement tend to have a better self-image and sexual relationships.”
• Arroyo, 2012– The more often someone engages in “fat talk,” the lower
that person's body satisfaction and the higher the level of depression after three weeks. "It is the act of engaging in fat talk, rather than passively being exposed to it, that has these negative effects.”
Research on Fat Studies in Mental Health Training
• Qualitative study of students who have completed the 1-unit elective course and agreed to participate in 2-hour interviews
• Interviews are guided by the question “how has the FA/HAES class impacted you?”
Research on Fat Studies in Mental Health Training
• N=6 thus far; goal is for N=8-12• Participants thus far
– Mixture of male and female– Mixture of body sizes– Range in age from 26 to 50– All participants so far ID as White– One IDs as Latino/Hispanic

Research on Fat Studies in Mental Health Training
• Participants have discussed– How they chose to take the class– Expectations/assumptions about the class and
classmates– Memorable parts of the class– Interactions with peers/colleagues in the class– Awareness of their own biases about body size– Awareness of stigma & micro-aggressions from others
Research on Fat Studies in Mental Health Training
• Participants have discussed– Impact of the class on their own body image– Impact on relationships with peers– Impact on relationships with partners/sig. others– Impact on relationships with parents, siblings, & other
family– Impact on relationships with friends, roommates,
partner’s friends, etc.– Impact on perception of their clients & training sites– Conflict over how much of an “activist” to become
Research on Fat Studies in Mental Health Training
• Participants have NOT noted an impact of the class on the general atmosphere at school– Conversations in the halls/break areas– Conversations about food, bodies, dieting when food is
brought to classes– Fat-stigmatizing comments from faculty in other
classes– Weight/body size generally not included in
“dimensions of diversity” conversations– Higher-weight students have not felt comfortable
challenging privilege of lower-weight students– Not sure how to initiate conversations with clients

Research on Fat Studies in Mental Health Training
• Students like the class content and process• Some wish the class were longer (more units)• Some wish the class had a clearer connection to clinical
practice• Some suggest that info on body size and weight stigma be
integrated into multicultural & group process classes• Some would like a practicum option to use this info in a
concrete, direct service way• Students feel a “gap” between research and practice, and
between the processes in the course and the overall climate of the program

Fat Studies in MFT Training?
• Opportunities– Another dimension of diversity/social justice,
particularly when looked at with an intersectional lens
– Deeply relevant to a field that is over 80% female and climbing
– Opportunities for research on FA/HAES with families, in couple processes, looking through intergenerational lenses

Fat Studies in MFT Training?• Challenges
– Pressures of time/content in courses already– Few academic resources that directly address mental
health - body size is not included in Family Life Cycle, other multicultural/diversity texts
– Funding for research on weight is nearly all controlled by weight “loss” & bariatric industries
– Resistance, from students & faculty - weight stigma is still seen as “useful” and “virtuous”

Fat Studies in MFT Training?
DISCUSS:• Look at your responses from the initial exercises.• What do our own self-of-therapist issues on this topic look
and feel like? – What is your personal history with dieting efforts and weight loss,
weight gain, weight cycling?– What stereotypes and stigma do you subscribe to regarding fat
people?– What beliefs or fears do you have about embracing Fat
Acceptance/Health at Every Size?– What is the culture of your workplace, school, or community
regarding fatness, dieting, eating, etc.?

Questions and comments?