foot arch deformities 2
TRANSCRIPT
PRESENTATION BY,
MOHAMMAD AZHARUDDIN,
B.P.T
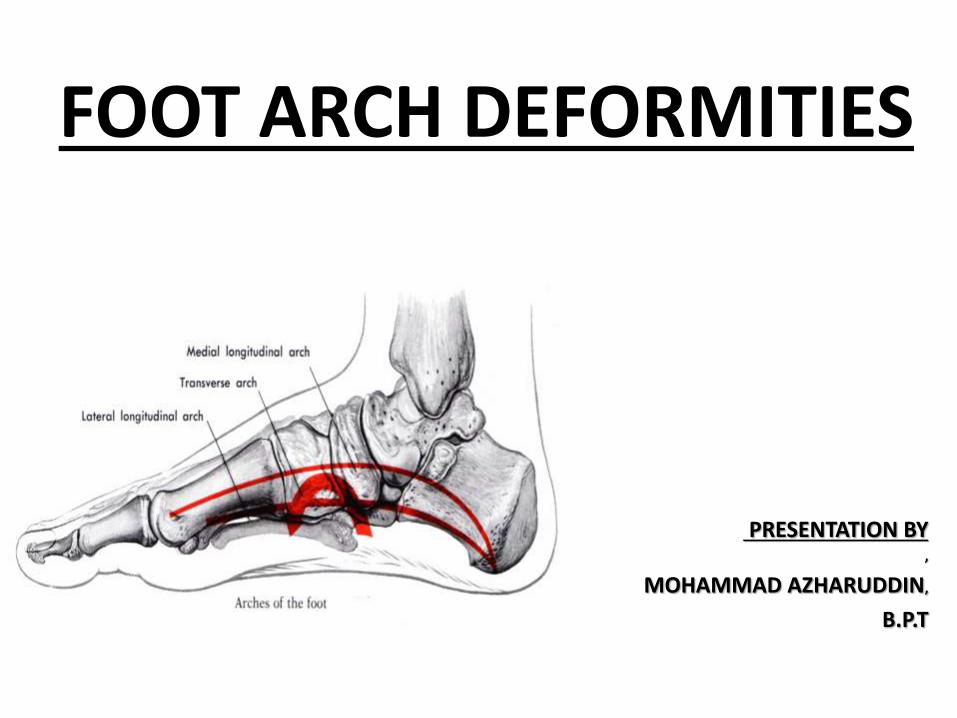
FOOT ARCH DEFORMITIES
WHAT ARE ARCHES AND WHY THEY ARE IMPORTANT
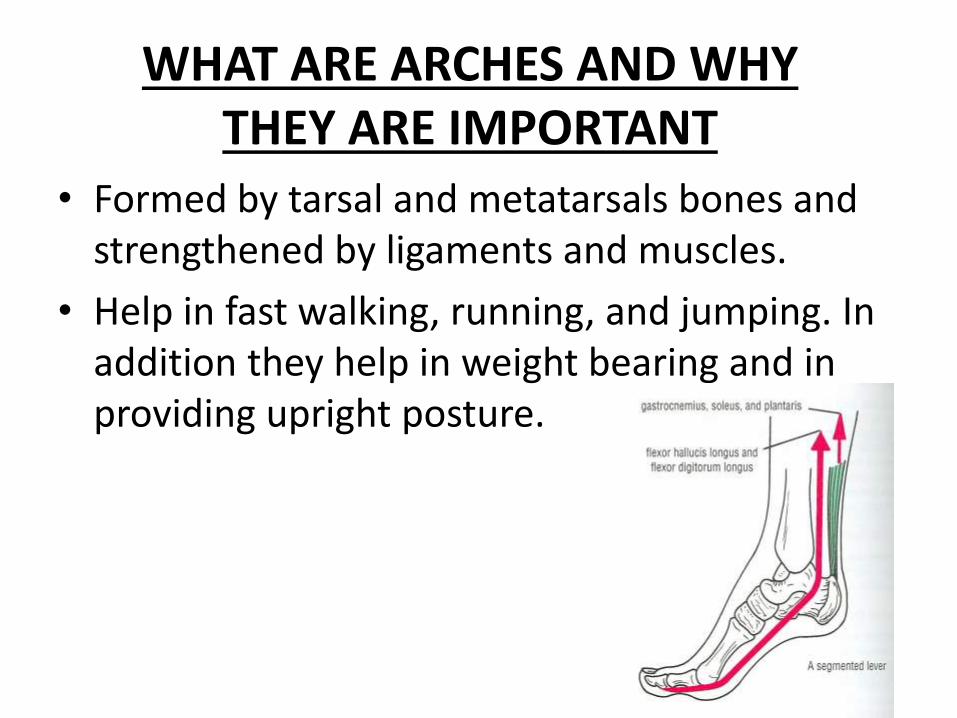
• Formed by tarsal and metatarsals bones and strengthened by ligaments and muscles.
• Help in fast walking, running, and jumping. In addition they help in weight bearing and in providing upright posture.

NATURAL HISTORY OF ARCHES
Initially, we see significantly bowed legs, noticeable out-toeing, and noevidence of a medial arch.
The arches slowly become more obvious and increase in height as our gaitimproves. The foot grows faster than the rest of the body; it achieves threequarters of its mature length by the time the child is seven years old.
By six or seven years of age, most children have also developed their adultmedial arch, although some take until age ten or eleven to completedevelopment
FACTORS RESPONSIBLE FOR MAINTENANCE OF ARCHES
• Shape of the bones.
• Intersegment ties or ligaments and muscles hold different segments of arch together.
• The beams that connect the two ends of the arch.
• Slings keep the summit of arch pulled up.
FUNCTIONS OF ARCHES
• Body weight distribution.
• Act as a spring which help in walking and running.
• Act as shock absorber in stepping and particularly in jumping.
• Concavity of arches protects the soft tissues of the sole against pressure.
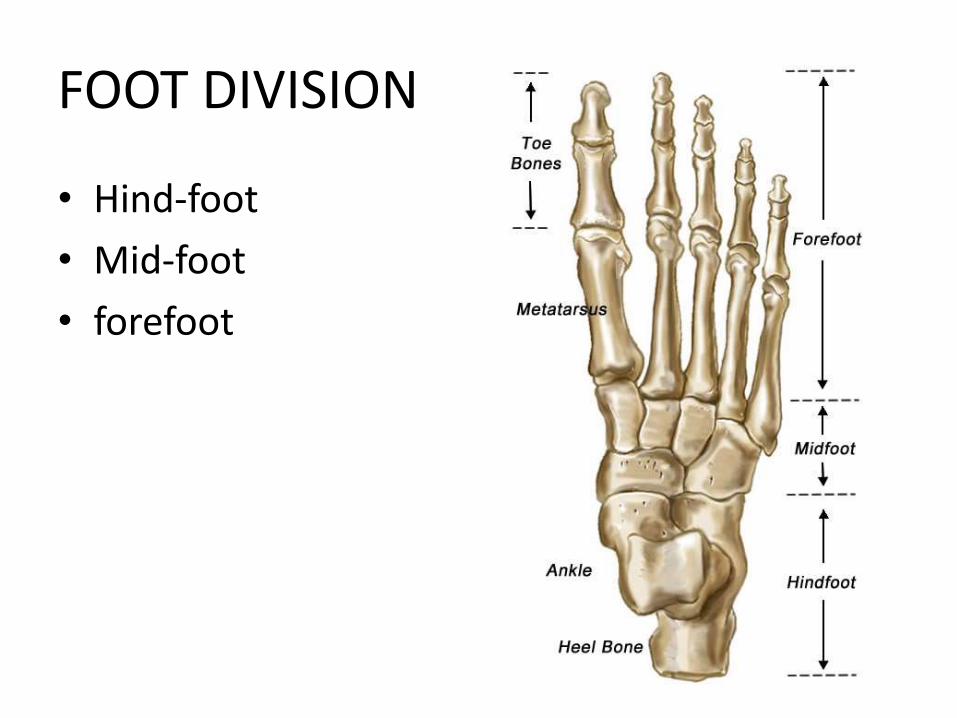
FOOT DIVISION
• Hind-foot
• Mid-foot
• forefoot
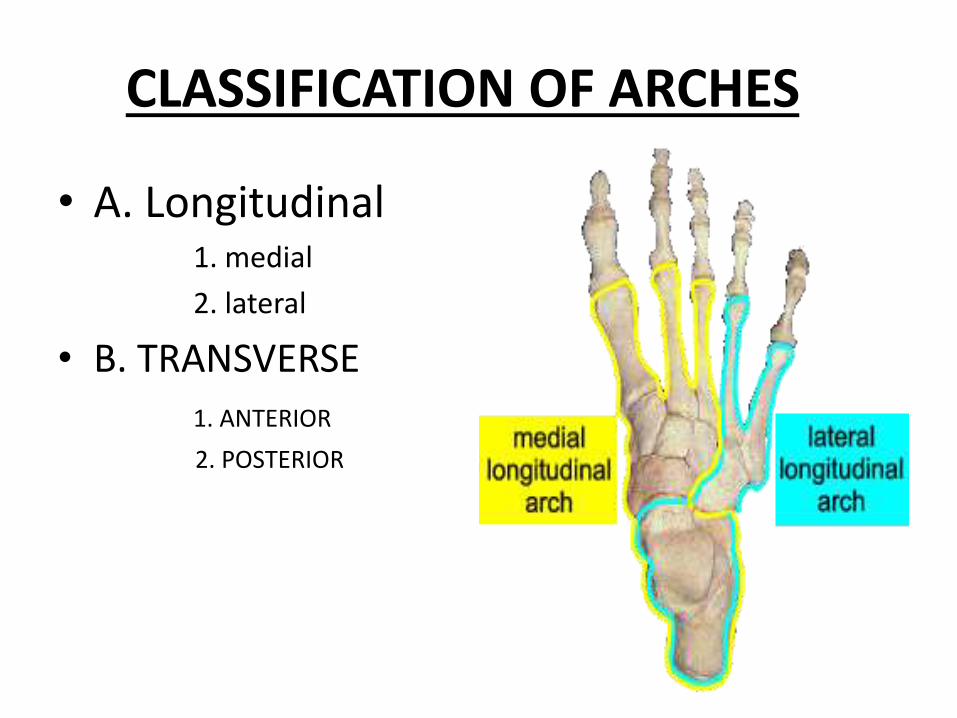
CLASSIFICATION OF ARCHES
• A. Longitudinal 1. medial
2. lateral
• B. TRANSVERSE
1. ANTERIOR
2. POSTERIOR
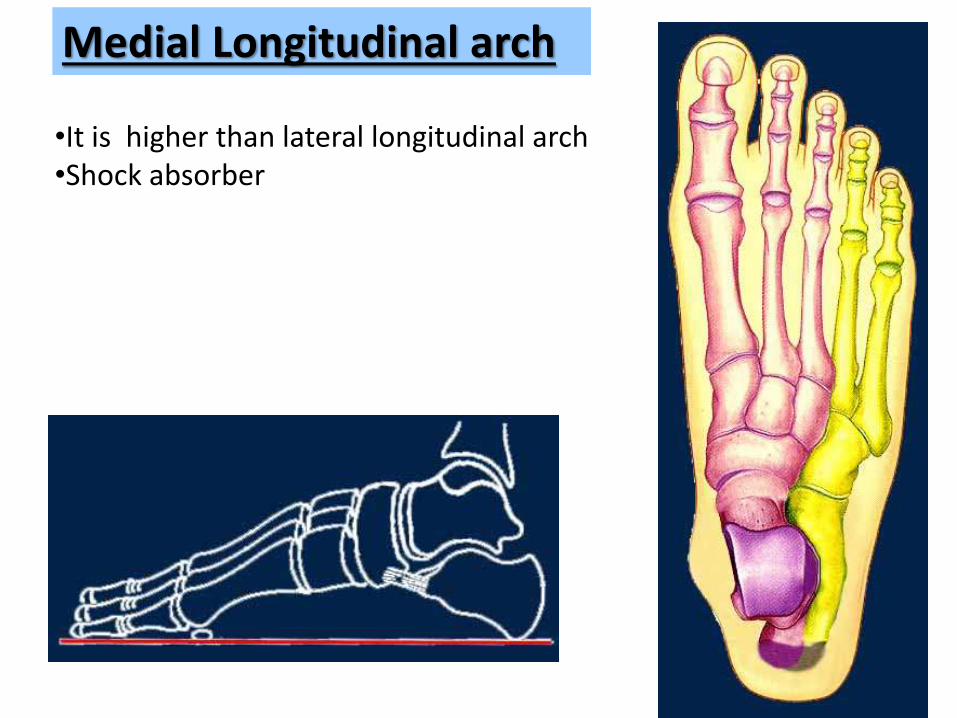
Medial Longitudinal arch
•It is higher than lateral longitudinal arch•Shock absorber
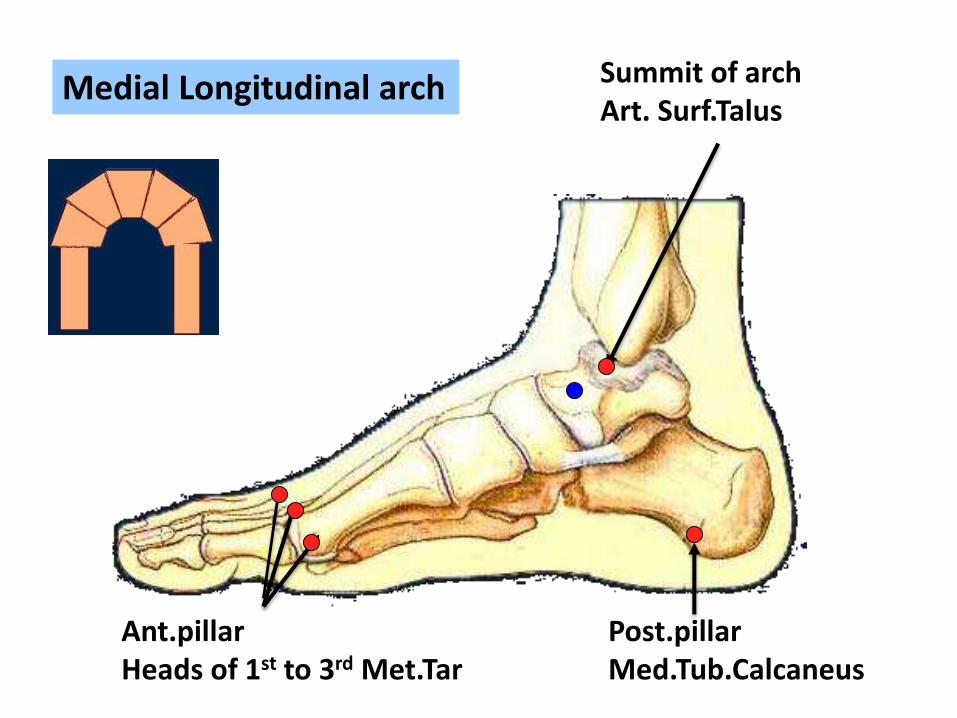
Medial Longitudinal arch Summit of archArt. Surf.Talus
Post.pillarMed.Tub.Calcaneus
Ant.pillarHeads of 1st to 3rd Met.Tar

Lateral Longitudinal arch
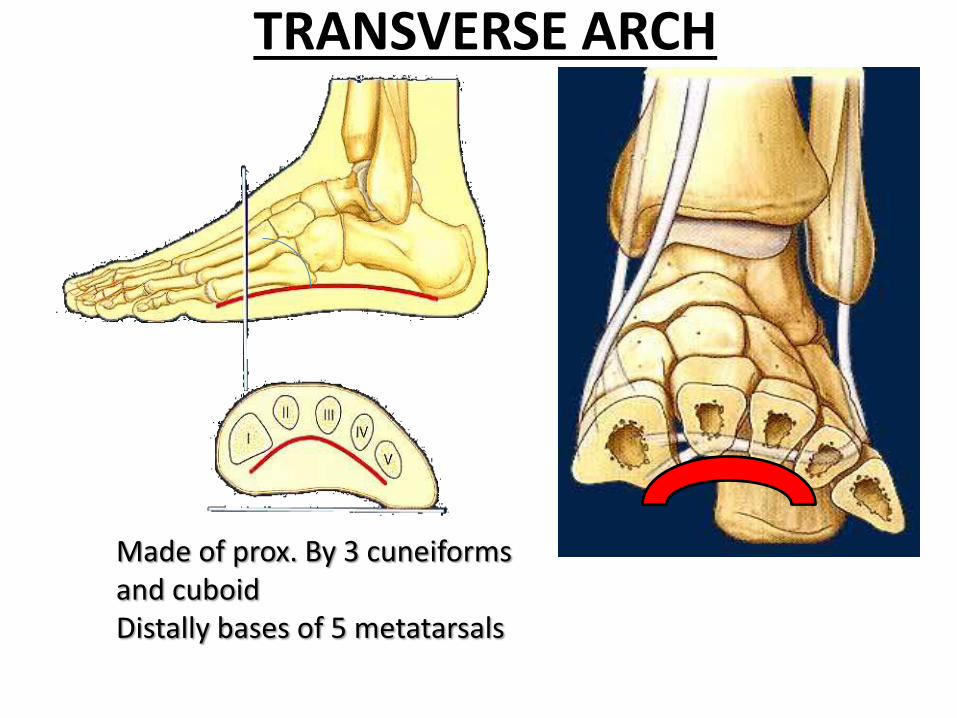
TRANSVERSE ARCH
Made of prox. By 3 cuneiformsand cuboidDistally bases of 5 metatarsals
PES PLANUSCondition in which medial longitudinal arch of foot is diminished or absent and foot is come in contact with the ground
People with hypertrophied planter foot muscles (lifelong barefoot walkers) might appear to have flat feet, when their bony arches are normal.
TYPES1. developmental or acquired
2. Flexible or fixed
IN CHILDREN1. pes planus can be a part of normal development2. Abnormal development of foot
IN ADULTS1. Physiological pes planus2. Adult acquired pes planus
CONTINUE…..CONTRIBUTING FACTORS
• Footwear: shoes which limit toe movement; high heels.Barefoot walking may be protective.
• A tight Achilles tendon or calf muscles (heel cordcontracture). This may help to cause PP, or may contributeto symptoms such as foot pain when there is existing PP.
• Obesity• Other bony abnormalities, e.g. rotational deformities, tibial
abnormalities, coalition (fusion) of tarsal bones, equinusdeformity.
• Ligamentous laxity, e.g. familial, Down's syndrome.• Other factors causing foot pronation, e.g. hip abductor
weakness and genu valgum.
CONTINUE…PRESENTATION AND ASSESSMENT
CHILDREN• History of the PP and any changes.
• Symptoms: walking/running ability and any foot pain.
• Past medical history: other diseases, developmental delay.
ADULTS• Is the PP new? Is it symmetrical?
• Is there foot pain or interference with walking?
• Are there any other lower limb symptoms, e.g. knee pain?
• Past medical history: injuries, other related disease (neurological, rheumatological, musculoskeletal).
• Occupation and hobbies.
• If PP is new, asymmetrical or painful, ask about symptoms of tibialis posterior dysfunction, which are:– Pain or swelling behind the medial malleolus and along the instep.
– Change in foot shape.
– Decreasing walking ability and balance.
– Ache on walking long distances.
CONTINUE…EXAMINATION
INVESTIGATIONIn some cases, standing foot X-rays may be used to show the degree of deformity:o Standing lateral view shows the longitudinal arch and talonavicular joint.o Standing AP view shows the degree of heel valgus(talocalcaneal angle).
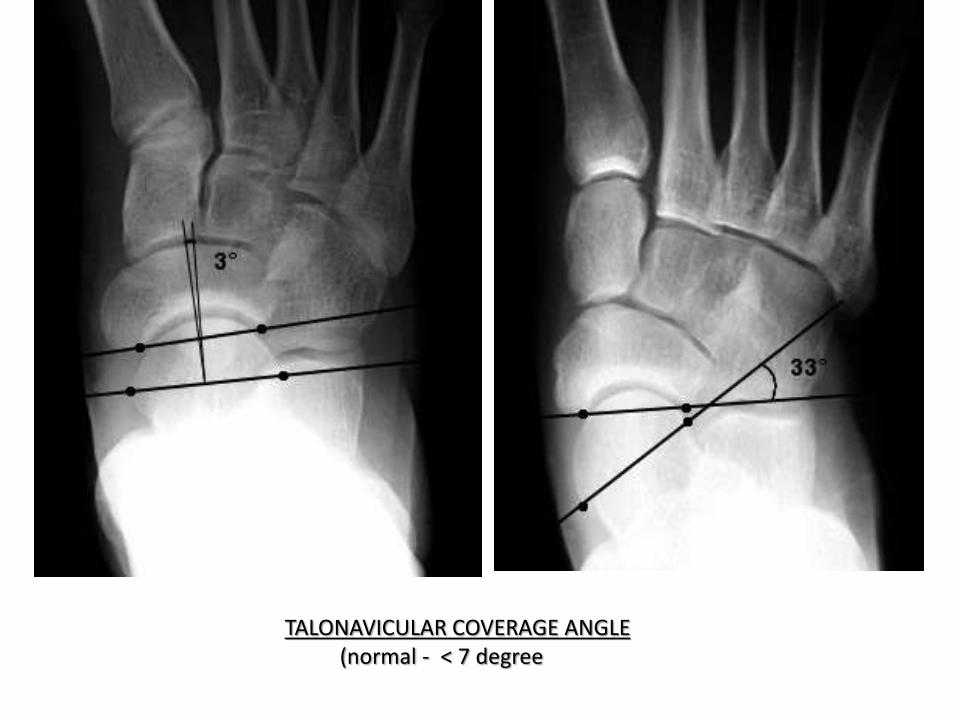
TALONAVICULAR COVERAGE ANGLE(normal - < 7 degree
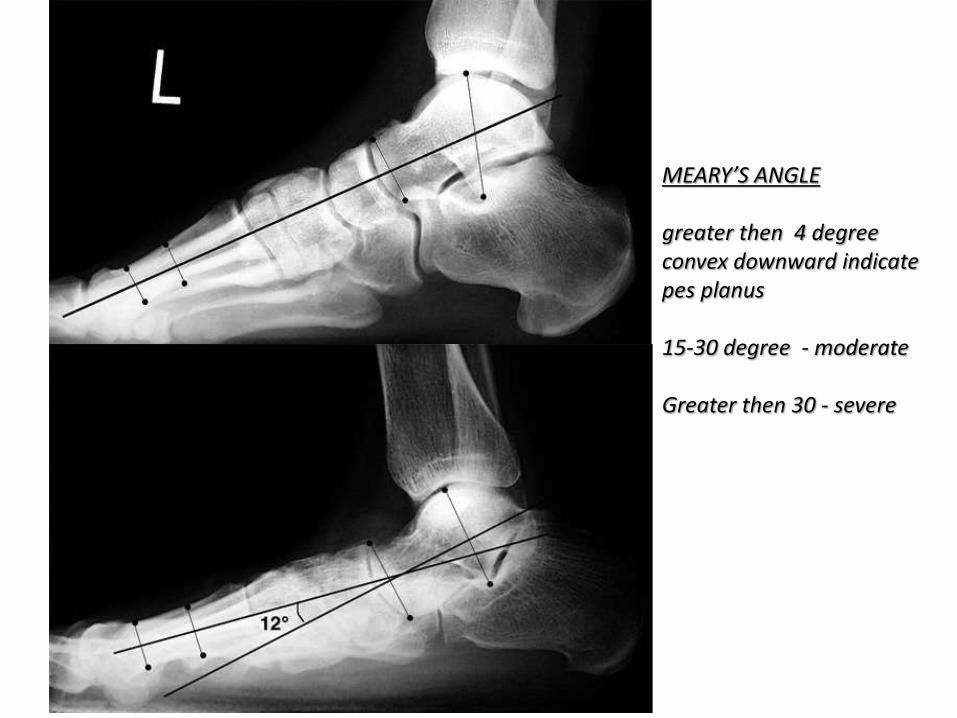
MEARY’S ANGLE
greater then 4 degree convex downward indicate pes planus
15-30 degree - moderate
Greater then 30 - severe
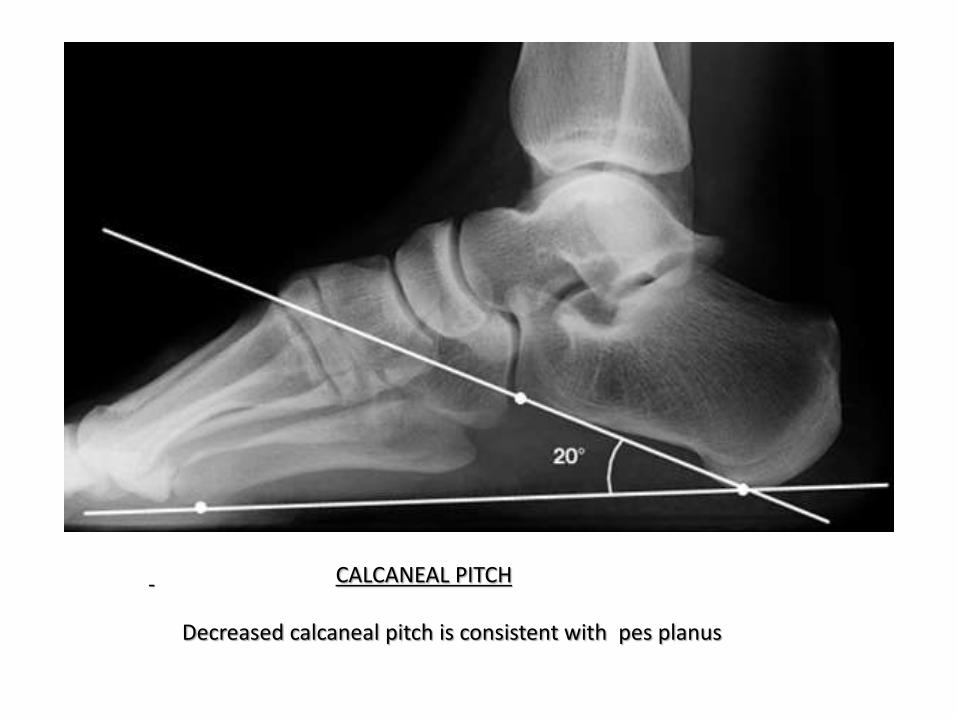
CALCANEAL PITCH
Decreased calcaneal pitch is consistent with pes planus
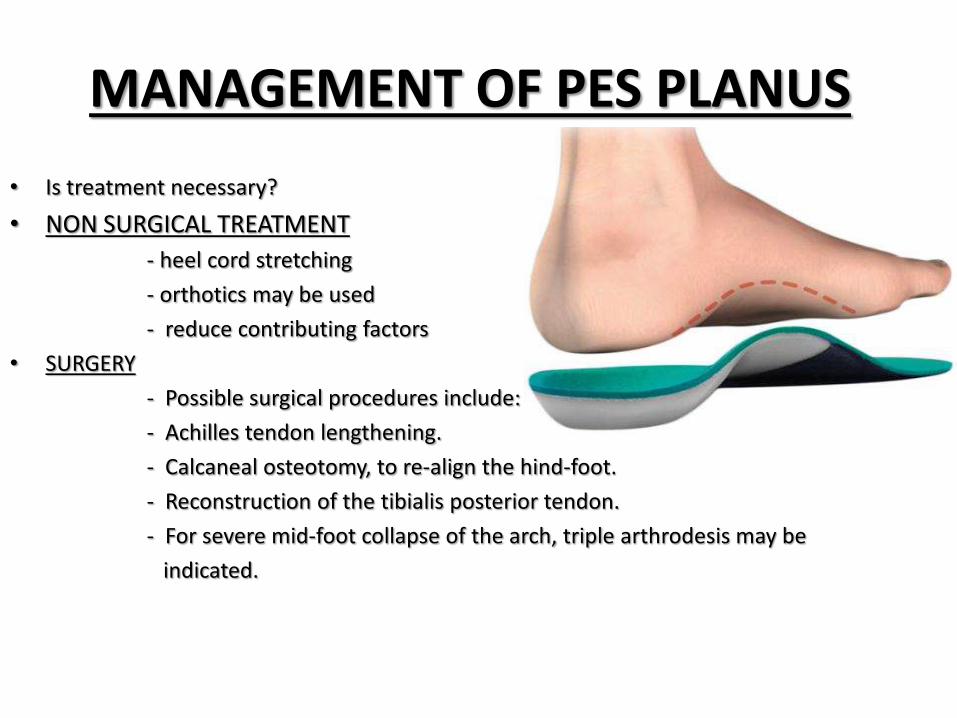
MANAGEMENT OF PES PLANUS
• Is treatment necessary?
• NON SURGICAL TREATMENT
- heel cord stretching
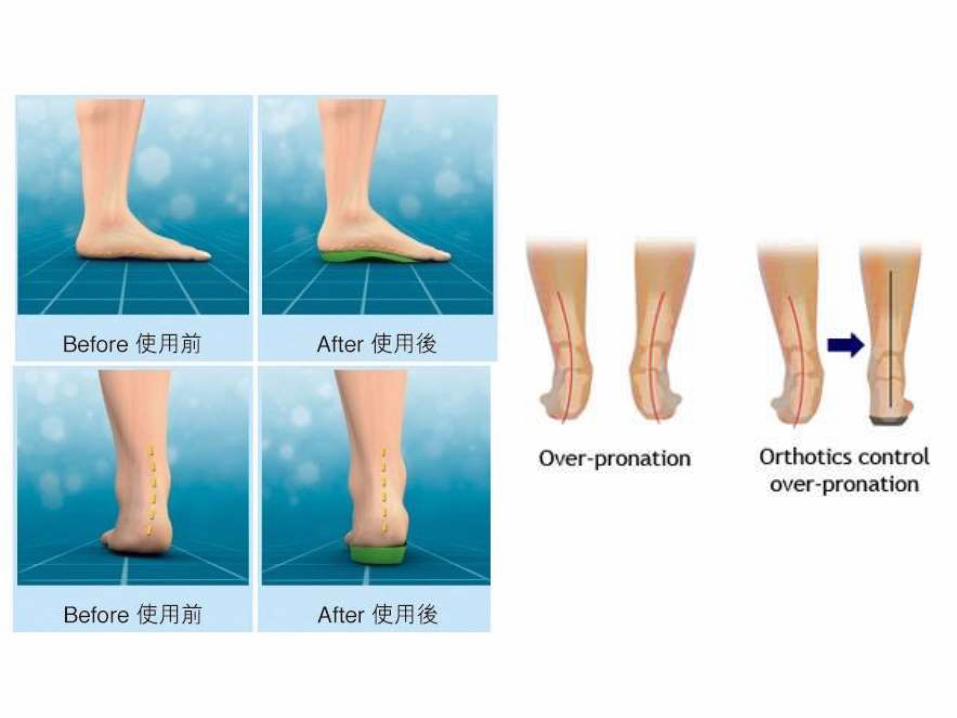
- orthotics may be used
- reduce contributing factors
• SURGERY
- Possible surgical procedures include:
- Achilles tendon lengthening.
- Calcaneal osteotomy, to re-align the hind-foot.
- Reconstruction of the tibialis posterior tendon.
- For severe mid-foot collapse of the arch, triple arthrodesis may be
indicated.
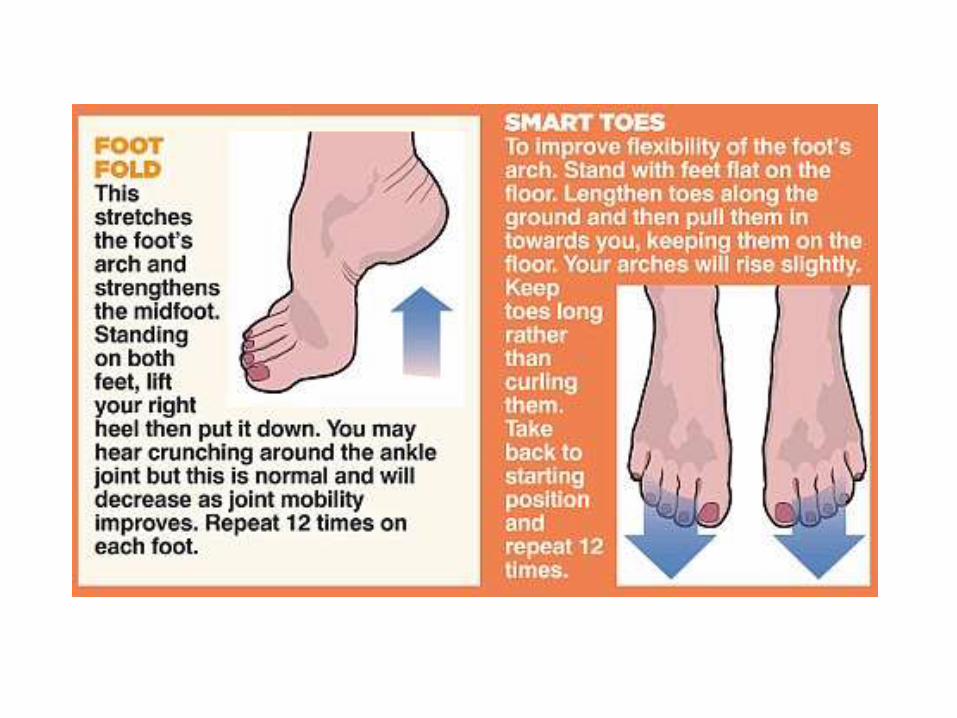
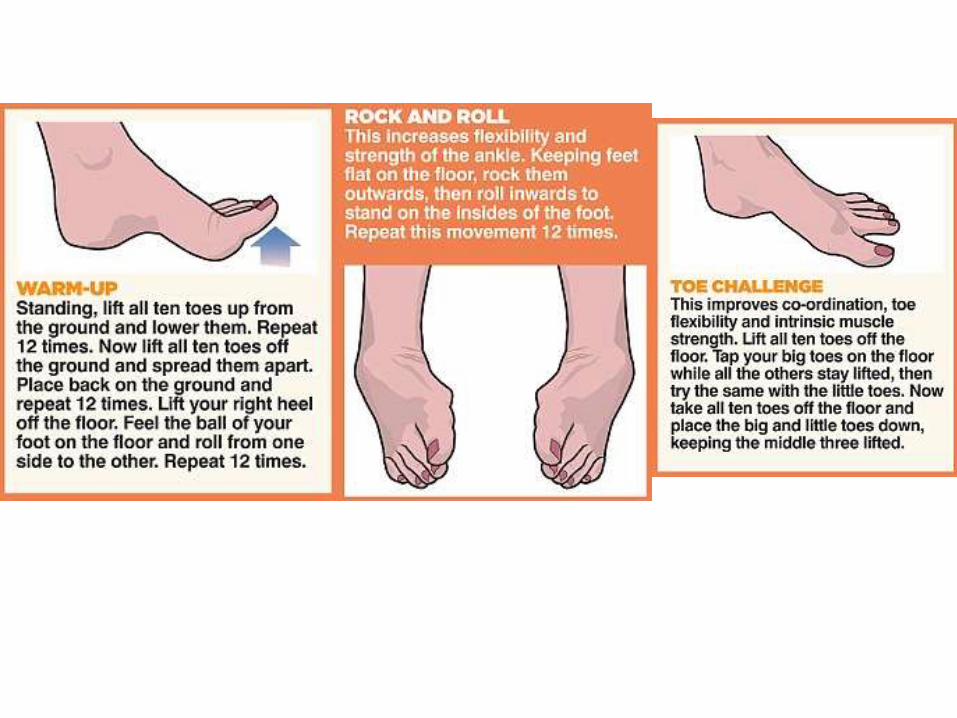
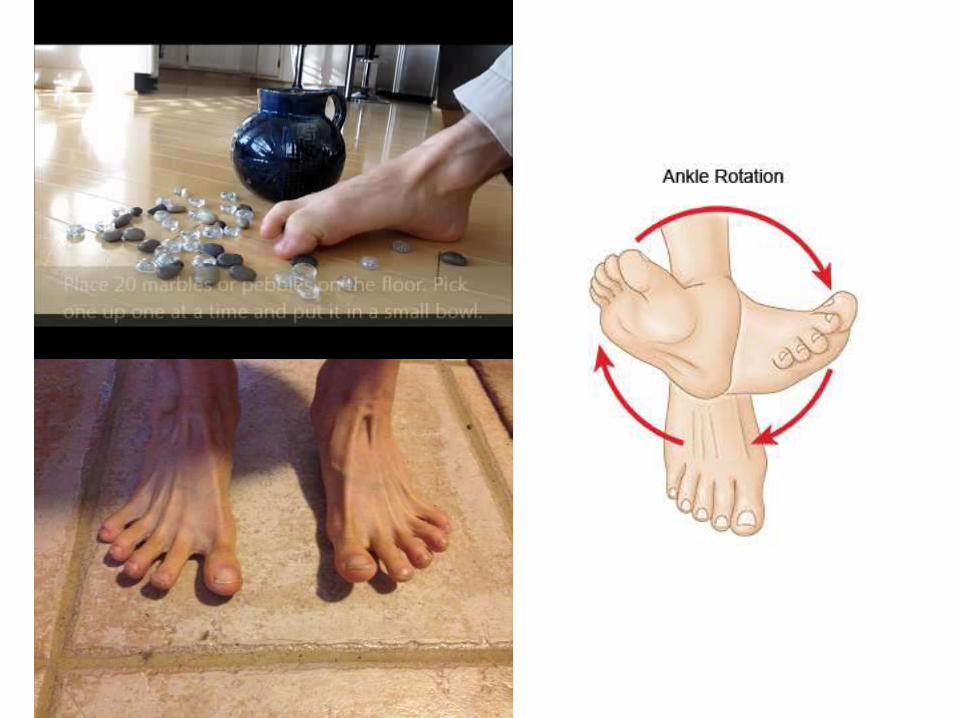
EXERCISES FOR FLAT FOOT
• Toe clawing• Toe spreading• Rising the inner border of forefoot closing – making fist with foot• Active foot rolling• Picking up small logs through foot• Standing on outer borders of foot• Toe flexion and extension while sanding on the edge of the stairs
with toes of the stairs.• Walk on a straight line• Walking on the lateral border of the foot• Curved foot walking• Heel walking • Toe walking
Complications and prognosis• Physiological pes planus (PP)
– It is generally stated that physiological PP is unlikely to cause significant foot problems.1,3 However, some authors suggest that excessive foot pronation (which usually occurs with PP) may contribute to the development of foot pain and foot problems such as:2
– Tibialis posterior dysfunction (because hyper-pronationstretches this tendon).
– Hallux valgus (because more weight is borne by the medial metatarsals when the foot hyper-pronates).
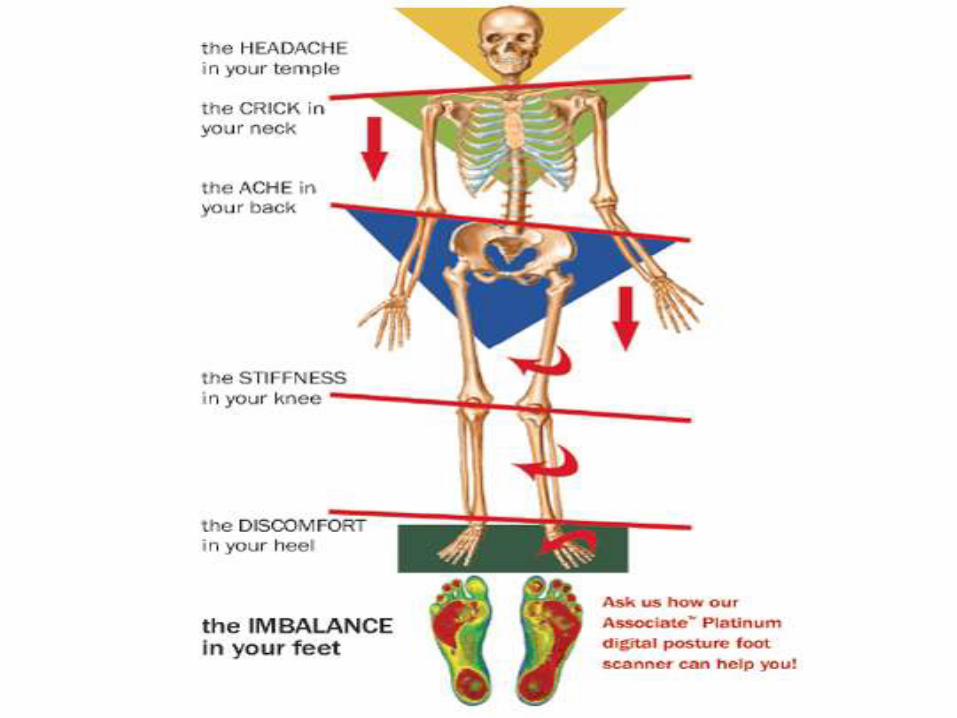
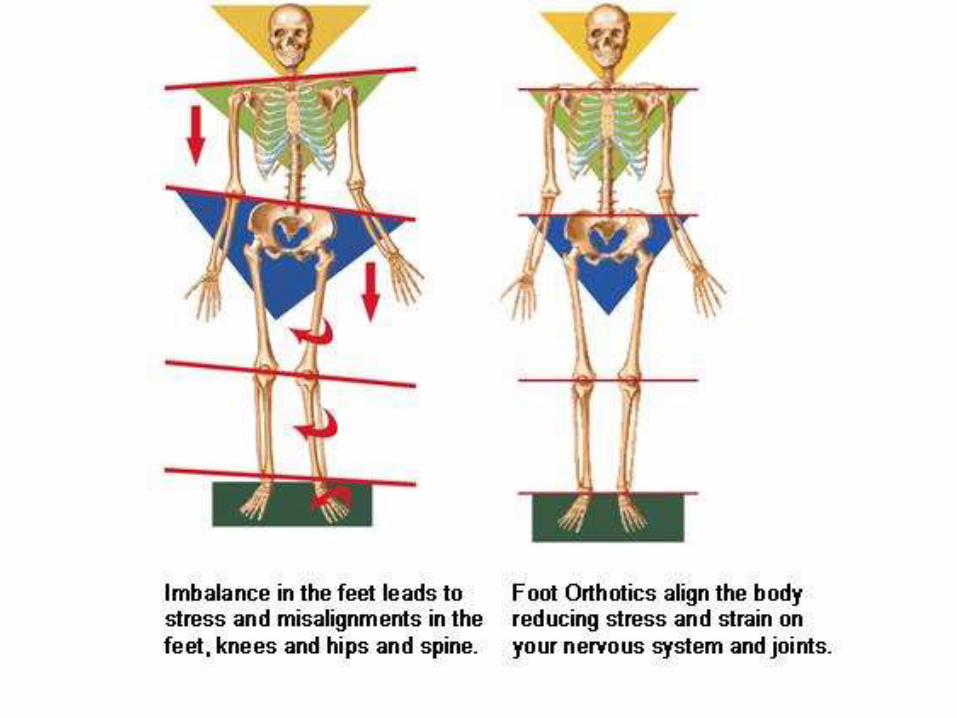
– Metatarsalgia (for the same reason).– Plantar fasciitis.– Knee pain– PP may reduce the shock-absorbing features of the foot,
potentially contributing to low back pain.3
PES CAVUS
• Deformity of a high arched.
• Occurs when metatarsals bone are planter-flexed relative to hind-foot – forefoot plantaris– which increases the height and curvature of the longitudinal arch.
• VARIANTS
pes equinocavovarus
pes calcaneovarus
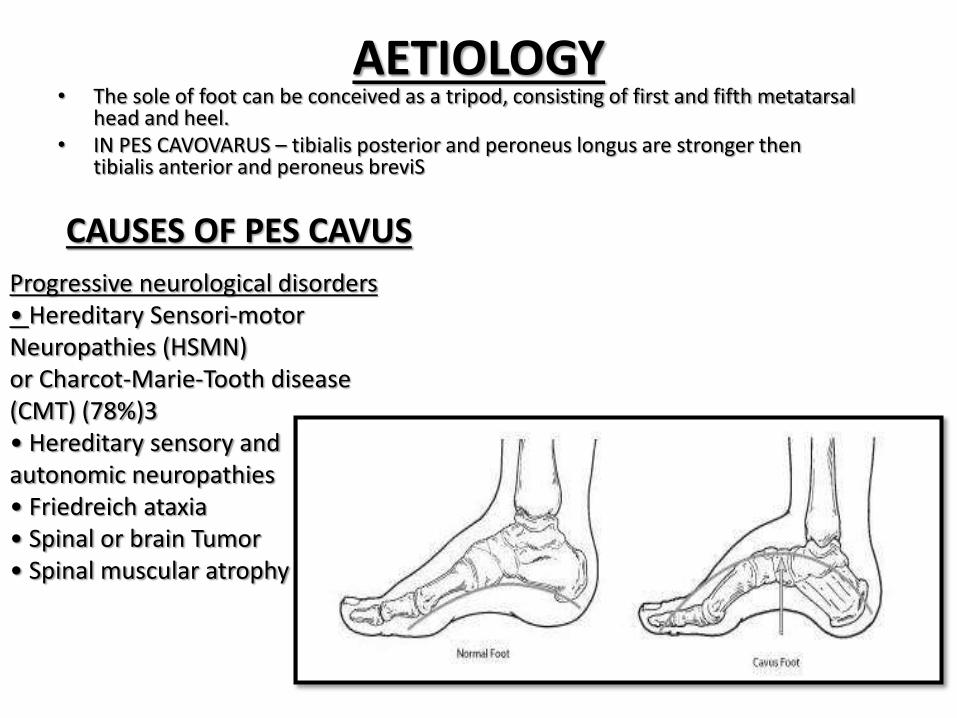
AETIOLOGY• The sole of foot can be conceived as a tripod, consisting of first and fifth metatarsal
head and heel.• IN PES CAVOVARUS – tibialis posterior and peroneus longus are stronger then
tibialis anterior and peroneus breviS
CAUSES OF PES CAVUS
Progressive neurological disorders• Hereditary Sensori-motor Neuropathies (HSMN)or Charcot-Marie-Tooth disease (CMT) (78%)3• Hereditary sensory and autonomic neuropathies• Friedreich ataxia • Spinal or brain Tumor• Spinal muscular atrophy
Other causes• Scarring of the deep posterior compartment
after compartment syndrome5
• Foot trauma
• Tarsal coalition
• Under-corrected congenital talipes equinovarus
• Iatrogenic (e.g. overzealous surgery for pes
planus)
• Idiopathic / familial
Static neurological disorders• Cerebral palsy• Stroke• Poliomyelitis• Spinal nerve root injury• Peroneal nerve injury4
• Spinal trauma• Syringomyelia• Myelodysplasia• Spinal dysraphism: spina bifida, spina bifidaocculta, diastematomyelia4• Muscular dystrophy
SYMPTOMSMetatarsal overload, heel pain. Stiffness, ankle sprain, ill fitting footwear, foot rubbing, ulceration
Reduce shock absorbance and diminish ability to balance on uneven surfaces
Hind-foot varus lead to increase moment on ankle, making ankle inversion injuries common eventually there may be dramatic varus tilting and secondary osteoarthritis.
Planter pain and callus formation may give way to ulceration particularly in patients with sensory loss.
With progression ---deformity and rigidity become more severe Lateral foot overload 5th metatarsal stress fracture.
Achilles tendon disorders, plantar fasciitis, and ankle impingement are also common.
DIAGNOSIS• HISTORY
• Family history
• Birth and early developmental history
• Previous trauma / illness / injury
• General examination may reveal features of neurological conditions such as path of hair over spine in spina bifida.
• Neurological examination - search for signs of peripheral, nervous disease, such as muscle wasting, weakness and sensory deficit, and signs of central nervous disease, such as pyramidal signs, cerebellar signs or cranial nerve abnormalities. Accurate serial recording of power in individual muscle groups.
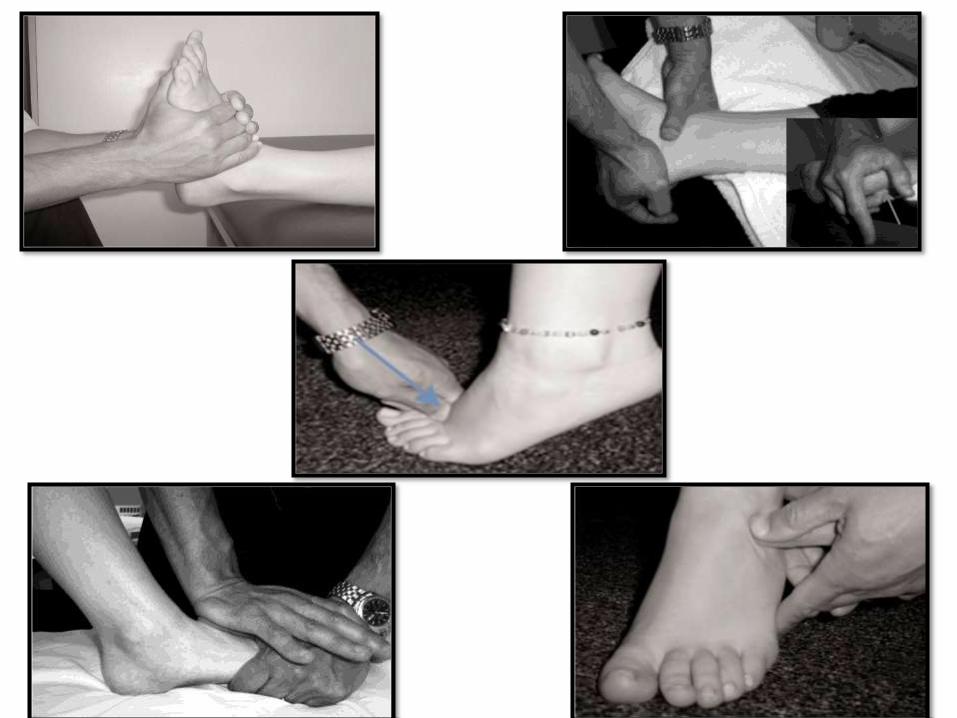
• FOOT EXAMINATION – to what extent deformities are fixed or flexible. Examination include :
inspection, palpation, passive and active movements, looking for joint contractures, ‘ COLEMAN BLOCK TEST’,
• INVESTIGATIONS : Radiographs, nerve conduction testing and EMG.
if onset is during adulthood or rapidly progressive a central disorder mus t be excluded by MRI of brain an spinal cord.
CONSERVATIVESuggested conservative management of patients with painful pes cavus typically involve :• Strategies to reduce and redistribute plantar pressure loading with foot orthoses and specialized cushioned footwear• Stretching and strengthening of tight and weak muscles• Debridement of plantar callosities• Osseous mobilization• Massage• manipulation of the foot and ankle and strategies to improve balance
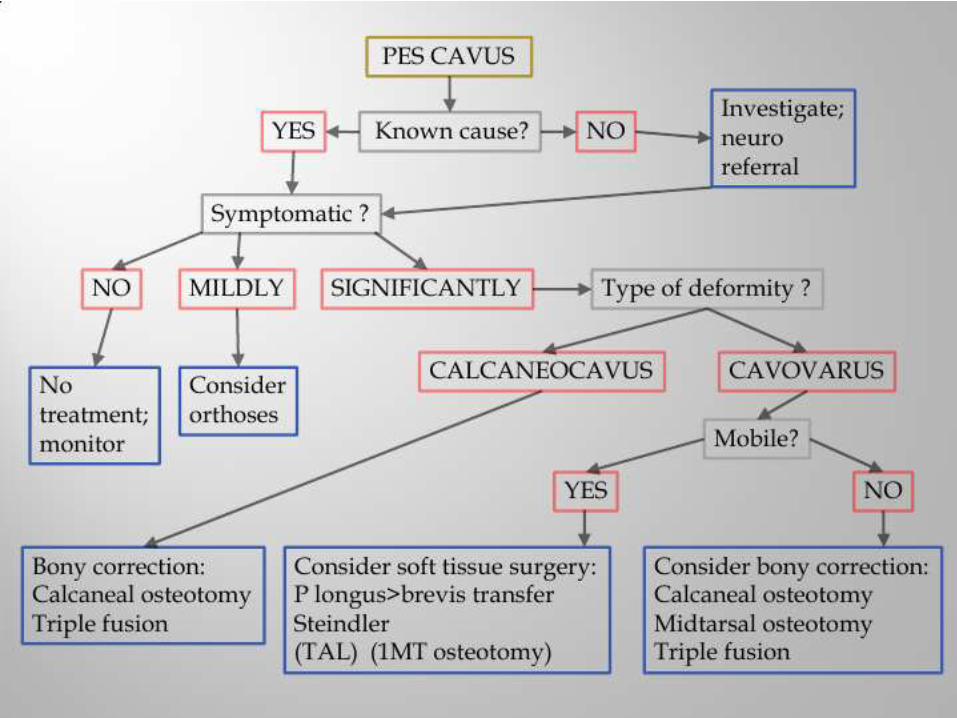
DIVIDED INTO 2 CATEGORIES1. non Surgical (conservative)2. surgical
TREATMENT
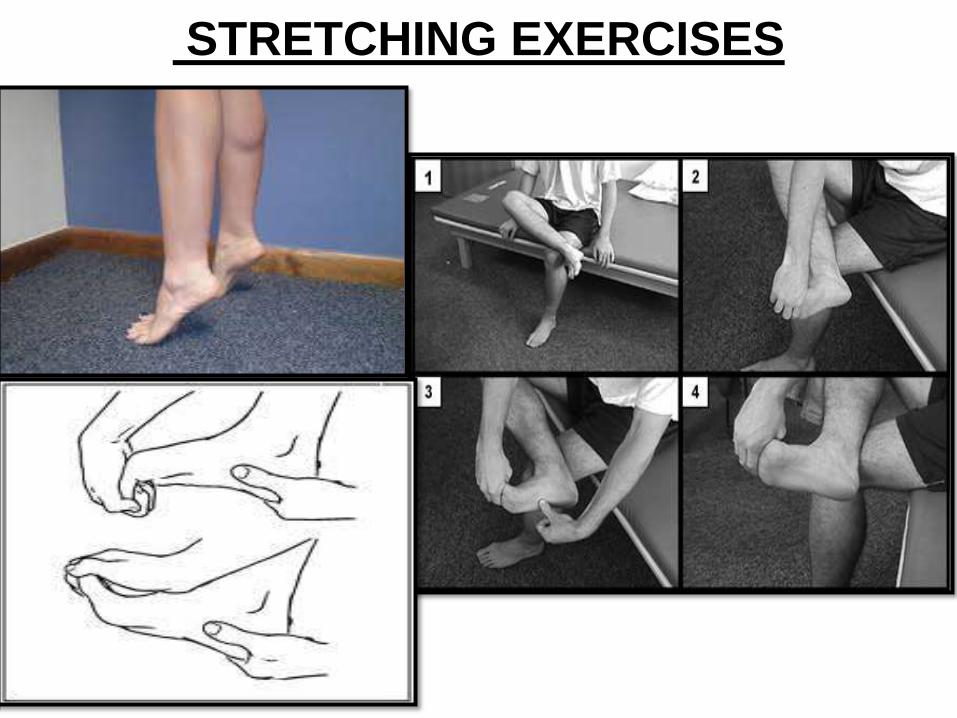
STRETCHING EXERCISES
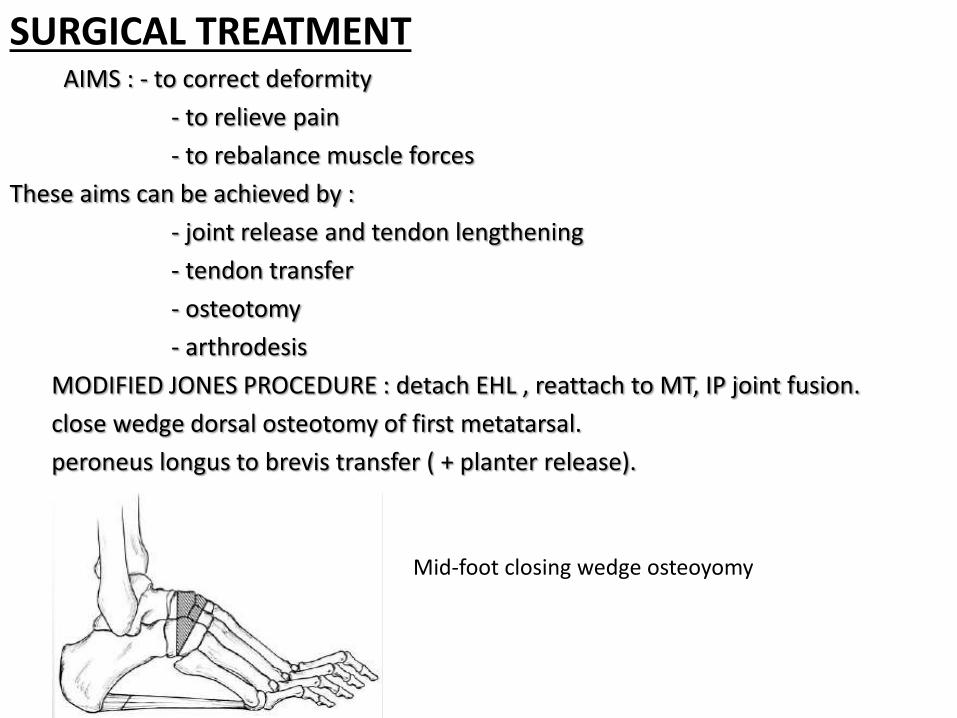
SURGICAL TREATMENTAIMS : - to correct deformity
- to relieve pain
- to rebalance muscle forces
These aims can be achieved by :
- joint release and tendon lengthening
- tendon transfer
- osteotomy
- arthrodesis
MODIFIED JONES PROCEDURE : detach EHL , reattach to MT, IP joint fusion.
close wedge dorsal osteotomy of first metatarsal.
peroneus longus to brevis transfer ( + planter release).
Mid-foot closing wedge osteoyomy
REFERENCES1. Sachithanandam V, Joseph B. The influence of footwear on the prevalence of flatfoot: a survey
of 1846 skeletally mature persons. J Bone Joint Surg Br 77(2):254, 1995.
2. Burns J, Crosbie J, Hunt A, Ouvrier R. The effect of pes cavus on foot pain and plantar pressure. Clin Biomech 20(9):877-882, 2005.
3. Ibrahim K. Pes cavus in surgery of the musculoskeletal system, Everts (CM, ed.), Churchill
Livingston, New York, 1990.
4. Brewerton DA, Sandifer PH, Sweetnam DR. “Idiopathic” pes cavus. Bristish Med J 2(5358):659-61, 1963.
5. Cavanaugh PR, Morag E, Boulton AJ, Young MJ, Deffner KT, Pammer SE. The relationship of static Foot structure to dynamic foot function. J Biomech 30(3):243-50.
6. Walker M, Fan HJ. Relationship between foot pressure pattern and foot type. Foot Ankle Int
19(6):379-83, 1998.
7. Redmond AC, Crosbie J, Ouvrier. Development and validation of a novel rating system for scoring standing foot posture: the Foot Posture Index. Clin Biomech 21(1):89-98, 2006.
8. Benedetti MG, Catani F, Ceccarelli F, Sioncini L, Giannini S, Leardini A. Gait analysis in pes cavus. Gait Posture 5(2):169, 1997. 9. Williams DS, McClay IS, Hammill J. Arch structure and injury patterns in runners. Clin Biomech16(4):341-47, 2001. 10. Williams DS, McClay IS. Measurements used to characterize the foot and the medial longitudinal arc: reliability and validity. Phys Ther 80(9):864-71, 2000. 11. Chalmers AC, Busby C, Goyert J, Porter B, Schulzer M. Metatarsalgia and rheumatoid arthritis-a randomized, single blind, sequential trial comparing two types of foot orthoses and supportive shoes. J Rheumatology 27(7):1643-7, 2000. 12. Mueller MJ, Lott DJ, Hastings MK, Commean PK, Smith KE, Pilgram TK. Efficacy and mechanism of orthotic devices to unload metatarsal heads in people with diabetes and a history of plantar ulcers. Phys Ther 86(6):833-42, 2006. 13. Crosbie J, Burns J. Are in-shoe pressure characteristics in symptomatic idiopathic Pes Cavusrelated to the location of foot pain? Gait Posture 27(1):16-22, 2008. 14. Bennett PJ, Patterson C, Wearing S. Baglioni T. Development and validation of a questionnaire designed to measure foot-health status. JAPMA 88(9):419-428, 1998. 15. Kirby K. Foot and Lower Extremity Biomechanics: A Ten Year Collection of Precision IntricastNewsletters. Precision Intricast 23-24, 1997.