gp buzz (oct - dec 2014)
DESCRIPTION
In this edition, we are pleased to share new and upcoming developments in Tan Tock Seng Hospital (TTSH) such as the soft launch of the Outpatient Pharmacy Automation System (OPAS) together with the official opening of the revamped Outpatient Pharmacy, and the commencement of the new Centre for Geriatric Medicine, designed to offer integrated and holistic care for elderly patients. In the cover story, GP BUZZ shares how bone conduction implants (BCIs) opened up new horizons for hearing rehabilitation options of hearing impaired patients. GP BUZZ is excited to introduce dance medicine, an area of medicine that promotes dance-related health and manages dance-related health problems. A new service offered by TTSH’s Sports Medicine and Surgery Clinic, GP BUZZ analyses the nature of dance injuries in the feature article, ‘Shall We Dance?’. The following Fitness section goes on to showcase a series of exercises to improve core strength for better execution of a dance routine and to minimise injuries in any professional or amateur dancers.TRANSCRIPT

A PUBLICATION FOR PRIMARY CARE PHYSICIANS
OCTOBER-dECEMBER 2014MCI (P) 088/03/2014
Scan the QR code using your iPhone or smart phone to view
GP BUZZ on the TTSHwebsite or visit
www.ttsh.com.sg/gp/.
Bone Conduction Implants –
New Horizons in Hearing
Rehabilitation
Preventing
Kidney StoneSNasal FRactuRe
cinnamon and Walnut
Baked apples
healthy recipe
iN eveRy issue
03 editor’s note
04 in the news
22 fitness
27 healthy recipe
iN tHis issue
07 Bone Conduction Implants – Opening New Horizons in Hearing Rehabilitation
10 Preventing Kidney Stones
14 Nasal Fracture: To Fix Or Not To Fix?
16 Straightening Out: The Facts on Peyronie’s Disease
19 Shall We Dance?
014 is drawing to a close with this October – December issue of GP BUZZ. With every end, a new beginning beckons.
In this edition, we are pleased to share new and upcoming developments in Tan Tock Seng Hospital (TTSH) such as the soft-launch of the Outpatient Pharmacy Automation System (OPAS) together with the official opening of the revamped Outpatient Pharmacy, and the commencement of the new Centre for Geriatric Medicine, designed to offer integrated and holistic care for elderly patients.
In the cover story, GP BUZZ shares how bone conduction implants (BCIs) opened up new horizons for hearing rehabilitation options of hearing impaired patients. GP BUZZ is excited to introduce dance medicine, an area of medicine that promotes dance-related health and manages dance-related health problems. A new service offered by TTSH’s Sports Medicine and Surgery Clinic, GP BUZZ analyses the nature of dance injuries in the feature article, ‘Shall We Dance?’. The following Fitness section goes on to showcase a series of exercises to improve core strength for better execution of a dance routine and to minimise injuries in any professional or amateur dancers.
In this issue, we also bring you management strategies to keep urinary stone disease at bay and to minimise recurrent episodes. Treatment for nasal fractures resulting from nasal trauma will also be discussed as well as the lesser known Peyronie’s disease, a condition in men characterised by the development of fibrous tunical plaque(s) and usually associated with some degree of penile curvature.
To celebrate the upcoming festive season, TTSH’s Nutrition and Dietetics Department in collaboration with the Hospitality and General Services Department (Kitchen) developed a special Cinnamon and Walnut Baked Apples recipe to end the year on a delicious note.
On behalf of the Editorial Team of GP BUZZ, we would like to thank our primary care partners and patients for your continued support in the year. You are our impetus to continue to produce quality content and develop fresher designs. We are humbled that our efforts paid off with GP BUZZ’s win of two gold awards in the international 2014 Content Marketing Awards.
Thank you and season’s greetings.
The GP BUZZ Editorial Team
2
editor’s notecontents
OCTOBER - dECEMBER 2014
HealtHy NeW you
tHe GP BuZZ editoRial team:Jessie Tay
Evelyn TanTeo Puat Wen
Celine Ong
advisoRy PaNel:Emeritus Professor Feng Pao Hsii Associate Professor Thomas Lew
Associate Professor Chia Sing JooAssociate Professor Chin Jing Jih
Adjunct Assistant Professor Chong Yew Lamdr Tan Kok Leong
dr Pauline Yong
GP BUZZ is a magazine by Tan Tock Seng Hospital, designed by
We value your feedback on how we can enhance the content of GP BUZZ. Please send in your
comments and queries to [email protected].
© All rights reserved. No part of this publication may be reproduced, stored in
a database, retrieval system or transmitted in any form by any means without prior consent from the publisher.
Although the publisher and author have exercised
reasonable care in compiling and checking that the information is accurate at the time of publication, we
shall not be held responsible in any manner whatsoever for any errors, omissions, inaccuracies, misprint and/or
for any liability that results from the use (or misuse) of the information contained in this publication.
All information and materials found in this publication are for purposes of information only and are not meant
to substitute any advice provided by your own physician or other medical professionals. You should not use the
information and materials found in this publication for the purpose of diagnosis or treatment of a health condition or
disease or for the prescription of any medication. If you have or suspect that you have a medical problem, you should
promptly consult your own physician and medical advisers.
07
19
10 14
02 03

in the newsin the news
opening of revamped pharmacy and soft launch of opas by Mr Gan Kim yong, Minister for health (centre).
Mr yong Keng Kwang receives the president's award for nurses at the istana.
introducing automation in medication dispensing.
the invasive cardiac laboratory at ttsh.
eNHaNciNG tHe outPatieNt PHaRmacy exPeRieNce WitH automatioN
sHave miNutes oFF ‘dooR-to-BallooN’ time
On 15 September 2014, the revamped Outpatient Pharmacy of Tan Tock Seng Hospital (TTSH) was officially opened by Mr Gan Kim Yong, Minister for
Health. Mr Gan also unveiled the new Outpatient Pharmacy Automation System (OPAS), an integrated system that features automation, robotic and radio-frequency identification (RFID) technologies. The full OPAS system is expected to roll out in early 2015.
With this new system, patients coming in to the B2 Pharmacy of TTSH can now expect to collect their medication faster and safer, thus enhancing the outpatient pharmacy experience for them.
Tan Tock Seng Hospital (TTSH) has effectively reduced the average ‘door-to-balloon’
time to 60 minutes, 10 minutes faster than in 2010, through process streamlining efforts.
One such improvement by TTSH’s Department of Cardiology involves placing all required equipment for angioplasty into a single sealed bag for quick access, rather than in individually sealed pouches. These bags are placed on trolleys in the operating theatre, which further reduces the preparation steps and ‘door-to-balloon’ time.
The relocation of the Invasive Cardiac Laboratory (where angioplasties are performed) above the Emergency Department last year contributed to quicker ‘door-to-balloon’ time.
Additionally, the shift from transfemoral angioplasty to transradial angioplasty as the default route also helped in the time reduction, since the latter is done via the radial artery in the wrist. Transfemoral angioplasty is done through the major femoral artery at the groin, hence more time is required to prepare the patient to begin the angioplasty.
ttsH NuRsiNG diRectoR Receives PResideNt's aWaRd FoR NuRses
Mr Yong Keng Kwang, Director of Nursing of Tan Tock Seng Hospital (TTSH) received the President’s Award for
Nurses from President Tony Tan Keng Yam at the award ceremony held in the Istana on 30 July 2014.
The award is the highest accolade of the nursing profession and it celebrates the nation’s most outstanding nurses. Mr Yong is the third male to receive the award since its launch 15 years ago.
Along with the other three nursing award recipients, Mr Yong is lauded for his significant contributions to nursing. With 18 years of experience in nursing, Mr Yong introduced the
Shared Governance Council in TTSH, which allows nurses to elect council members, participate in policy recommendations and make decisions relating to nursing in the hospital.
Mr Yong was appointed in 2013 as the Chairperson of the National Nursing Taskforce Workgroup on Redefining the Role of Nurses. He also serves on the National Medical Ethics Committee, is an active member of the Singapore Nursing Board and several of its committees, and the Assistant Honorary Treasurer for the Singapore Nurses’ Association.
tWo toP coNteNt maRketiNG aWaRds FoR GP BuZZ maGaZiNe
GP BUZZ magazine, by Tan Tock Seng Hospital, has been awarded two gold awards in the international 2014 Content Marketing Awards.
The awards were conferred to the Health City Novena issue (October - December 2013) of GP BUZZ magazine, under the Digital Publication categories of 'Most Improved Editorial' and 'Most Improved Design'.
Now in its 11th year, the Content Marketing Awards is the leading awards programme for organisations that create branded or custom content, in print or electronic form (sometimes referred to as ‘content marketing’). All entries are judged
on a long list of criteria such as information value, quality of copywriting, appropriateness for the audience and visual appeal.
04 05

in the news
Tan Tock Seng Hospital (TTSH)’s new Centre for Geriatric Medicine was officially opened by Mr Gan Kim Yong, Minister for Health on 25 July
2014, the 170th anniversary of the hospital’s founding.
Drawing on 26 years of experience in geriatric care, TTSH designed and developed this 1,200 square feet,
NeW ceNtRe FoR GeRiatRic mediciNe desiGNed to oFFeR iNteGRated aNd Holistic caRe FoR tHe eldeRly
MoU signing between ttsh’s iGa and ntU.
opening of the centre for Geriatric Medicine by Mr Gan Kim yong, Minister for health with Madam Kay Kuok, chairman of national healthcare Group and the senior management team of tan tock seng hospital.
cover story
BoNe coNductioN imPlaNts – OPENING NEW HORIZONS IN HEARING REHABILITATIONUntreated hearing impairment can result in disability and handicap, which ultimately reduces a patient’s quality of life. Some patients have conductive pattern hearing loss and are unable to wear conventional hearing aids due to chronic ear diseases.
Bone conduction implants (BCIs) are a type of implantable hearing aid that have opened up new horizons for hearing rehabilitation options in these patients. Another group of patients who can benefit from BCIs are those with unilateral hearing loss.
purpose-built geriatrics care hub to provide our elderly patients with one-stop and multidisciplinary outpatient care in an elder-friendly environment.
Differing from a typical outpatient clinic, the new Centre boasts a mock geriatric-friendly home environment, which allows the occupational therapist
to advise the elderly patient or caregiver on the appropriate use of furniture. A sensory garden designed for dementia patients (which make up a quarter of the Centre’s patient load), helps to stimulate and enhance patients’ senses.
Geriatric care is also integrated into the Centre, with the co-location of the rehabilitation gymnasium and pharmacy within the clinic’s premises. Patients could then make same-day clinic consultation and rehabilitation sessions, thus cutting down travel time for them.
Alongside the opening of the Centre for Geriatric Medicine, a Memorandum of Understanding (MOU) was also signed between TTSH’s Institute of Geriatric and Active Ageing (IGA) and Nanyang Technological University (NTU). Under this agreement, IGA and NTU will be partnering on geriatric research and innovation to enhance the delivery of care to the elderly.
06 07

cover story
Much of our day-to-day communication is verbal. Communication is dependent on our ability to verbalise and understand spoken
language. Both of these functions are actually dependent on our ability to hear with our ears. Development of our speech and language was possible because of our ability to hear, listen and understand in early childhood.
Hearing impairment, if left untreated, will result in communication difficulty. This disability can lead to decreased participation and opportunities in life, for example, in education and employment, with a consequent reduction in quality of life.
Most patients with hearing impairment can benefit from the use of conventional hearing aids. Conventional hearing aids work by amplifying sounds before they get to our cochlear or inner ear.
deFiNiNG HeaRiNG aNd HeaRiNG imPaiRmeNtSound travels as a form of kinetic energy through the air. Our cochlear is actually a fluid-containing organ.
Sound is captured and amplified by our ear drum and ossicular chain and sound kinetic energy in the air is converted into sound kinetic energy in the fluid of the cochlear. Within the cochlear, sound kinetic energy is converted into electrical signals that our brains can decipher.
There are two main types of hearing impairment, sensorineural and conductive. Sensorineural hearing impairment is the most common type and a manifestation of any decline in the function of our cochlear or its nerve supply. This can occur due to ageing, ototoxicity, excessive noise exposure, infection, inflammation or trauma.
Conductive hearing impairment occurs when there is compromised transfer of sound energy from air to the fluid of the cochlear. Conductive hearing loss can be caused by problems with the external ear canal, ear drum and/or ossicular chain. Ear canal problems include narrowing or atresia of the ear canal, which can be either congenital or acquired. Ear drum problems include perforation, retraction, fluid accumulation, abnormal thickening or scarring. Ossicular chain problems include ossicular chain discontinuity or stiffening secondary to infection, inflammation or trauma.
Some patients may experience a combination of sensorineural and conductive hearing impairment.
imPlaNtaBle HeaRiNG aidsConventional hearing aids tend to work well for patients with pure sensorineural hearing impairment, but less so for patients with conductive or mixed pattern hearing impairment. The ear abnormalities responsible for the conductive hearing loss actually act as physical barriers for the efficient transfer of sound kinetic energy in the air to the fluid within the cochlear.
Bone conduction implants (BCIs) are implantable hearing aids that work by transferring sound air kinetic energy into sound kinetic energy within the bone. We are familiar with the concept of the bone being an excellent sound conductor during tuning fork tests.
This bone kinetic energy is then converted into fluid kinetic energy within the cochlear, with subsequent conversion into electrical signals. Hence, BCIs work by bypassing the ear canal, ear drum and ossicular chain.
Some patients are unable to wear conventional hearing aids due to recurrent ear infections and they too can benefit from BCIs. BCIs can also help patients who have deafness in one ear only, that is, unilateral hearing loss. BCIs can route the sound from the deaf side to the working cochlear in the contralateral ear, hence enabling patients to regain some hearing in their deaf side.
There are two main types of BCIs in Singapore.
The Bone Anchored Hearing Aid (BAHA) utilises osseointegration and was invented by the same person who invented dental implants. Osseointegration refers to the biological fusion of titanium implants with patients’ bone to form a very stable and secure fixation. This facilitates the efficient transfer of amplified sound from the air to bone via a tiny implant footprint.
cover story
The second device is called the Bonebridge, which is more aesthetically pleasing as it utilises a transcutaneous coupling system. The traditional BAHA has a percutaneous coupling system but the latest generation offers a transcutaneous option.
Every patient needs to be carefully assessed to ensure they meet the anatomical and audiological criteria for either device.
Both BAHA and Bonebridge require an operation for implant placement. The operations are relatively straightforward, with very low rates of complication.
multidisciPliNaRy HeaRiNG cliNicIn Tan Tock Seng Hospital, we initiated the multidisciplinary Combined Hearing Clinic two years ago, to assess patients with complex hearing difficulties who may benefit from various new hearing technologies. Since then, we have implanted more than a dozen BCIs. Many of these patients have struggled with their hearing impairment for a long time.
BCIs are more expensive than conventional hearing aids. We work closely with our Medical Social Workers to ensure that financial limitations do not limit patients' access to these devices.
BCIs have opened up new hearing rehabilitation options for patients whose conventional hearing aids had not been helpful previously.
Dr Ho Eu Chin Dr Ho Eu Chin is a Consultant in the Department of Otorhinolaryngology (ENT) in Tan Tock Seng Hospital. He completed his postgraduate ENT training in England. Dr Ho runs the Combined Hearing Clinic and Multidisciplinary Balance Clinic and has interests in providing holistic and individualised care to patients with complex hearing and balance problems. He devotes his time to teaching and research, and collaborates
closely with colleagues from Nanyang Technological University, Singapore.
Bone anchored hearing aid in an adult patient (photo used with permission from cochlear, australia)
Bonebridge in an adult patient (photo used with permission from Medel, austria)
08 09

preventing Kidney stones
feature feature
The treatment of urinary stone disease extends beyond the acute management of stones as this condition yields a high rate of recurrence.
Approaches for stone prevention includes both dietary interventions
and medication. The use of medication should be guided by the 24-hour urine analysis.
WHat caN a PatieNt do aBout BeiNG diaGNosed WitH stoNes?In one case, a patient, Mark (not his real name), was sleeping when he felt a severe pain in his left back. Upon seeking help, he discovered a stone in his kidney and underwent shockwave lithotripsy, which cleared the stone.
Urinary stone disease is a relatively common condition thought to affect 15% of the population and with a slowly increasing trend. This could be associated with heightened rates of diabetes and obesity. After treatment, there is a 25 to 50% chance of recurrence within five years. Thus, in many cases, urinary stone disease is a chronic condition. This is more so when the patient possesses risk factors for recurrence.
WHat caN Be doNe to PReveNt a RecuRReNce?1. evaluationFirst, patients with urinary stone disease should be evaluated. The baseline evaluation for this condition requires a proper medical and dietary history. Physical examinations should include blood tests to look for abnormalities in uric acid, calcium and kidney functions, and a urine dipstick test to detect infections and measure urinary pH levels.
For patients with a higher risk of recurrence (Table 1), a 24-hour urine test to look for abnormalities
should be obtained. In a pilot study conducted by Tan Tock Seng Hospital, it was found that 95% of patients with high risk of stone formation were found to possess abnormalities after undergoing the 24-hour urine analysis. The correction of these abnormal urine parameters can significantly reduce the recurrence of stones.
An added benefit of doing metabolic evaluations is that underlying systemic diseases that manifest as stone diseases can be detected. They may include conditions such as hyperparathyroidism, renal tubular acidosis and hyperoxaluria.
table 1. patients at risk of stone recurrence
• Previous history of stones • Multiple stones in kidney
• Previous weight loss surgery • Solitary kidney
• Presence of remnant stones • Family history of stones
• Onset of disease - before 25 years of age • Calcium phosphate stone
2. Management strategiesThe main aims of treatment are to improve the solubility of kidney stones, introduce inhibitors to stone formation and also normalise abnormal urinary levels of calcium and oxalate.
Improved solubility of the stones can be achieved by dilution and maintaining a neutral or slightly higher pH, while the main inhibitor of stone formation is citrate. Normalising urinary calcium and oxalate levels can be done through dietary and medical means.
(a) dietary ManagementThere are a number of dietary interventions that can be applied to reduce stone recurrence.
• Basic dietary ManagementFluidsFirst and foremost, patients with stone disease should be encouraged to drink more fluids to produce at least two litres of urine a day, unless contraindicated. A simple gauge of adequate fluid intake is in the colour of the urine. If it is dark, fluid intake is inadequate. Patients with stones should aim for very light to clear coloured urine.
A study by Borghi et al1 found that increasing fluid intake would reduce the risk of recurrent stone disease
by 50%. Lemonade and orange juice are recommended as the citrate in these juices helps to reduce stone recurrence. The citrate alkalises urine and can also combine with calcium to form a soluble salt, thus stopping stone precipitation. Soft drinks should be avoided as they have been shown to be associated with increased stone episodes2.
SaltPatients should also be on a salt restriction diet. They should aim to consume not more than 3g per day, which is equivalent to half a teaspoon of salt. This would help reduce urinary calcium excretion, which could precipitate as stones in the urinary system.
Animal ProteinAnimal proteins can lead to increased uric acid (via purine metabolism) in the blood and acidification of the urine, which will
increase the incidence of calcium oxalate and uric acid stones. Consumption of animal proteins should be limited to not more than 0.8 to 1g per kg of the body weight per day (e.g. egg: 7g, fillet of salmon: 22g, 100g of chicken: 26g). In a recent study, it was found that fish and chicken actually caused as much uric acid issues as beef3.
VegetablesFibre and vegetables should be encouraged as this raises pH levels and reduces incidence of stones by improving the solubility of stones. Citrate is also found in many fruits and vegetables.
SupplementsVitamin C consumption should be limited to 500mg per day, unless otherwise specified. Dosing more than 1g or more has been shown to be associated with increased calcium oxalate stone formation as the excess ascorbic acid is converted to oxalate4.
A normal calcium intake of 800mg per day should be adhered to5. This is because when calcium is taken together with high oxalate foods, it binds oxalate in the gut
preventing Kidney stones
10 11

feature
References 1. Borghi L, Meschi T, Amato F, Briganti A, Novarini A, Giannini A. Urinary volume, water and
recurrences in idiopathic calcium nephrolithiasis: a 5-year randomised prospective study. The Journal of urology. 1996;155(3):839-43.2. Shuster J, Jenkins A, Logan C, Barnett T, Riehle R, Zackson D, et al. Soft drink consumption
and urinary stone recurrence: a randomised prevention trial. Journal of clinical epidemiology. 1992;45(8):911-6.
3. Tracy CR, Best S, Bagrodia A, Poindexter JR, Adams-Huet B, Sakhaee K, et al. Animal protein and the risk of kidney stones: A comparative metabolic study of animal protein sources. The journal of urology. 2014.
4. Thomas LD, Elinder CG, Tiselius HG, Wolk A, Akesson A. Ascorbic acid supplements and kidney stone incidence among men: a prospective study. JAMA internal medicine. 2013;173(5):386-8.
5. Candelas G, Martinez-Lopez JA, Rosario MP, Carmona L, Loza E. Calcium supplementation and kidney stone risk in osteoporosis: a systematic literature review. Clinical and experimental rheumatology. 2012;30(6):954-61.
Dr Tan Yung Khan Dr Tan Yung Khan is a Consultant in the Department of Urology at Tan Tock Seng Hospital. He is also the Director of Endourology and Co-director of the Minimally Invasive Urology Fellowship and a clinical lecturer at National University of Singapore (NUS) School of Medicine. Dr Tan completed his Urology training in Singapore and received the National Medical Research Council (NMRC) scholarship to do advanced research in robotic surgery and minimally invasive surgery at University of
Texas Southwestern Medical Center, Dallas, Texas. He also matched in the Endourology Society training programme in the United States and spent a year at Columbia Medical Center, New York City focusing on endourology and the management of stone disease.
feature
• directed dietary ManagementWhen a proper dietary history and 24-hour urine test are done, we can tailor the dietary management to correct the abnormalities found in the urine test.
Oxalate restrictionOxalate restriction in the diet is controversial. This is because oxalate is found in a lot of vegetables that have beneficial effects in the prevention of stone formation and also cardiovascular health.
Oxalate restriction should be done in moderation and options like consuming calcium at the time of a high oxalate meal may be a better option. In the event that oxalate restriction is used, it is usually suggested to remove the most prominent source of oxalate, commonly found in spinach.
(b) MedicationsIn situations where there are significant abnormalities in the 24-hour urinalysis that cannot be corrected by diet alone, medications can be started to help correct the abnormalities. These can range from the use of potassium citrate, thiazide diuretics and allopurinol, depending on the abnormalities found.
Potassium citrate has the ability to alkalise the urine and also reduce the formation of calcium oxalate and calcium phosphate stones. It is used when increasing citrate with dietary interventions are insufficient. Thiazides also help to reduce calcium-based stones by increasing renal tubular reabsorption of calcium
and prevents oxalate absorption. Hence, a low calcium diet would lead to excessive absorption of oxalate and subsequently increase the incidence of calcium oxalate stones.
It is advisable for patients to take a 300mg tablet of calcium along with high oxalate meals, to try and ameliorate the effects of oxalate. Calcium supplementation in the form of calcium citrate is a better alternative as one would enjoy the benefits of calcium and citrate intakes.
DietsSpecific dietary plans can have effects on stone disease. The Atkins diet and ketogenic diets are more likely to cause stones, whereas the Dietary Approaches to Stop Hypertension (DASH) and vegetarian diets tend to reduce stone formation. This is expected as the Atkins diet, with a high animal protein load, tends to lead to acidic urine, which promotes the precipitation of kidney stones. Increased purine loads from the diet may also make the patient prone to uric acid stones.
and thus lowering urinary calcium levels.
Mark was also noted to have bilateral small stones and his 24-hour urinalysis was found to have a citrate deficit. As it was mild, apart from basic dietary advice, he was advised to increase his intake of citrate in the form of orange juice and lemonade. A repeat 24-hour urinalysis showed that this corrected his citrate deficit. Today, Mark has not had a recurrence of stone disease in the past five years.
Urinary stone disease is a chronic condition. Recurrent stone disease can be prevented if a suitable approach is taken to prevent recurrence.
1312

featurefeature
Dr Chua Yu Khim, Dennis Dr Dennis Chua is an Associate Consultant in the Department of Otorhinolaryngology (ENT) in Tan Tock Seng Hospital. He completed his subspecialty in facial plastic surgery
at the University of Virginia, United States of America (USA) in 2013. He is passionate about research and has presented in conferences globally. Besides having published in international peer reviewed journals, he also co-authored book chapters on functional nasal surgery and facial trauma.
The nose is the most commonly traumatised structure on the face due to its prominence. A nasal septal hematoma is a feared complication that should be picked up as soon as possible, and the hematoma should be evacuated within 12 hours due to the potential of septal cartilage necrosis. Nasal septal cartilage necrosis can result in a saddle nose deformity with nasal obstruction. Nasal trauma can also result in a nasal fracture with resultant nasal obstruction and/or cosmetic deficits such as a saddle or crooked nose.
The critical window for a closed nasal reduction for treatment of nasal fracture is before two weeks in adults and before one week in pediatric patients. The treatment for persistent nasal deformities beyond one month after injury may require a functional septorhinoplasty.
The nose is frequently traumatised in facial injuries and this often results from
motor vehicle accidents, sports-related injuries and altercations. When the injury is significant, this can result in nasal fractures with its accompanying nasal deformity.
There are two main problems that nasal trauma can result in: a nasal septal hematoma or nasal fracture with nasal obstruction or nasal deformities.
nasal fracture: to fix or not to fix?
● If the nose is bleeding, apply digital pressure over the lower half of the soft fleshy part of the nose for 15 minutes to slow down bleeding.
● The head should be tilted forward during this time to prevent aspiration of the blood into the lungs.
● Place ice wrapped in a cloth or a bag of frozen peas over the nose for about 15 minutes at a time. This process can be repeated hourly throughout the day. Using ice packs at the time of injury and for one to two days afterward helps to reduce pain, swelling and nose bleeds. Take breaks between applications and do not apply the ice directly to the skin.
● Take paracetamol or non-steroidal anti-inflammatory drugs (NSAIDs) to reduce pain. The pain is usually worse in the first five days after the injury.
● Nasal decongestants such as oxymetazoline can be used to help with the nasal obstruction. However, these should not be used beyond five days.
● Elevate the head, especially when sleeping, to avoid increased swelling of the nose. Prop the head up with pillows or lift the head of the bed by placing large blocks or phone books under the mattress.
A closed nasal reduction can be attempted within three hours of injury, before swelling sets in or between three to fourteen days
figure 1: a closed nasal reduction being performed in the clinic with the patient awake with nose deviated to left. an elevator is used on the right side and digital pressure is simultaneously applied on the left to reduce the fracture.
Nasal sePtal HematomaA nasal septal hematoma is one of the most feared complications that can occur through nasal trauma. Though uncommon, a septal hematoma can lead to complications such as septal abscess, septal perforation and cartilage necrosis with potential saddle nose deformity.
A nasal septal hematoma can usually be diagnosed with a careful clinical examination, using a good light source with a nasal speculum. If a fluctuant reddish-blue swelling is noted on the anterior part of the nasal septum, drainage of the hematoma should be performed urgently to prevent complications as mentioned above.
Nasal FRactuReA nasal fracture can be diagnosed clinically if there is gross deviation of the nose from its pre-injury appearance. An x-ray, though frequently performed may not always be necessary as it does not change the management.
You may apply the following first aid measures when a nasal fracture is diagnosed.
when the swelling has improved. This helps in the evaluation of the precise nasal deformity that the patient is suffering from. This procedure can be performed under local anaesthesia and is usually painless.
A satisfying “click” can usually be felt or even heard when the nasal fracture is pushed back in place (Refer to Figure 1). There is usually increased swelling over the nose and some periorbital bruising may sometimes occur post nasal reduction. Small amounts of nose bleeding is usually expected in the first 48 hours after a nasal reduction. A nasal cast is usually applied over the next week to protect the reduced nasal fragments. It is important that the patient avoids all contact sports (e.g. basketball, football) for the next six weeks following a closed
nasal reduction, till the nasal fragments are healed in place.
Nasal deFoRmities Subsequently, post-traumatic nasal deformity is one of the most common reasons that patients seek consultation in the doctor’s clinic. Depending on the type of nasal deformity, this can result in functional impairment and aesthetic problems. Two challenging problems to be addressed in the post-traumatic nose are the crooked nose and saddle nose deformities. The only definitive treatment for these conditions would be a functional septorhinoplasty, if it continues to trouble the patient.
14 15

featurefeature
stRaiGHteNiNG out:
tHe Facts oN PeyRoNie’s
diseasePeyronie’s disease (PD) does not spell the end for men who suffer from this condition. With a greater knowledge of its symptoms and range
of treatment options available, primary care practitioners can all play a part to improve the
sexual well-being of their patients.
aBout PeyRoNie’s diseaseOriginally known as induration penis plastica, Peyronie’s disease (PD) was described and eponymously named after François Gigot de La Peyronie in 1743.
PD is characterised by the development of fibrous tunical plaque(s) and is usually associated with some degree of penile curvature. There is a significant psychological component in patients suffering from PD as approximately 48% of PD patients are affected by resulting clinical depression. The prevalence of PD is reported to range from 3% to 9% in the adult male population and PD frequently presents in men when they are 50 years old and above.
PD is often associated with prior penile trauma but this history is not universal. The uncertainty about the pathogenesis and natural history of PD adds to the difficulty of managing men who present this condition. causes oF PeyRoNie’s diseaseRecently, PD has been categorised as a wound healing disorder. A common presentation is a fibrous and inelastic scar or plaque of the tunica albuginea that appears, following trauma to the penis. It is postulated that trauma causes increased transforming growth factor beta 1 (TGF-β1) levels, which results in an intense pro-inflammatory and pro-fibrotic cascade with subsequent deposition of collagen, resulting in the hallmark of the disease: plaque formation and penile curvature.
Studies have shown that inducible nitric oxide levels are quenched by reactive oxygen species (ROS), creating peroxynitrite, a highly toxic and pro-fibrotic compound. Although the pathophysiology of PD is still poorly understood, attempts at manipulating the levels of TGF-β1 and ROS could theoretically alter the natural history of PD, which form the basis of many of our current medical therapies.
As a general rule, the aim of medical management of PD is to alter the wound healing process and prevent plaque formation.
diaGNosiNG PeyRoNie’s diseasePlaque formations along the penile shaft are commonly found upon examination of the stretched and non-erect penis. The most common
The main problems with PD are penile curvature interfering with sexual activity and penile shortening, which can be embarrassing symptoms for the affected men. Since PD affects the private parts of a patient’s body, it can be difficult for affected men to present themselves to doctors. As such, the reported prevalence of PD in literature may not be accurate.
When considering the natural history of PD one year post-diagnosis, it is found that about 40% of men with PD reported penile curvature that remained unchanged. Approximately 45% of them reported progressive penile curvature and less than 15% reported spontaneous resolution.
plaque volume through the use of pentoxifylline (PTX) and Coenzyme Q10 (CoQ10).
PTX is a non-selective phosphodiesterase inhibitor with anti-inflammatory properties. It is shown to inhibit fibroblast proliferation and attenuate both collagen fibre deposition as well as elastogenesis in vitro. PTX downregulates TGF-β and increases fibrinolytic activity.
A retrospective cohort study showed that treatment with PTX appeared to stabilise or reduce calcium content in PD plaque. In a random trial, administering PTX sustained-release of 400mg twice daily for six months significantly improved penile curvature and plaque volumes, as compared to the placebo results. The authors also concluded that PTX is moderately effective in reducing penile curvature and plaque volume in patients with early chronic PD.
location would be over the dorsal aspect of the penile shaft, since dorsal curvature is far more common than ventral ones.
Some men would present photos of their erect penis, showing the penile deformity that they are concerned about. The investigative method of choice is a penile Doppler ultrasound. Prior to the ultrasound, the patient would be administered with intracavernosal alprostadil, which is a Prostaglandin E1 (PGE1) analogue, to induce an artificial erection. The penile curvature could then be measured with a goniometer and documented as a baseline prior to the administration of any form of treatment. At the same time, the erectile function would be assessed with the ultrasound. tReatmeNts FoR PeyRoNie’s diseaseMedical therapy for PD (or minimally invasive management) can be sub-divided into oral, topical, iontophoretic, intralesional, radio therapeutic, shockwave therapy, penile traction or any combination of the above. There is also a recent interest in including stem cells for the treatment of PD. The current literature only supports the use of oral therapy as well as intralesional therapy.
(a) oral therapyOral therapy has been shown in randomised controlled trials to significantly improve penile curvature and
16 17

feature
Omega-3 is a polyunsaturated fatty acid that stimulates the production of collagenase. The only prospective, randomised, double-blind, placebo-controlled study that evaluates the efficacy of Omega-3 fatty acids in PD was performed by Safarinejad. The study has shown no significant improvements in penile curvature, penile pain during erection, or erectile function with the use of Omega-3 fatty acids.
CoQ10 is a very potent antioxidant. In a double-blinded, placebo-controlled study, early chronic PD patients taking 300mg of CoQ10 daily for 24 weeks demonstrated statistically significant reductions in plaque size as well as improvements in both penile curvature and erectile function.
(b) intralesional therapyMen with PD should be referred to urologists with subspecialty interests in andrology and urological prosthetic surgery, should they fail to respond to oral medication. Intralesional therapy with or without penile traction therapy has been shown to be efficacious. The newest intralesional therapy that is approved by the Food and Drug Administration (FDA) in the United States, is the use of collagenase clostridium histolyticum (CCh). This drug has been shown to reduce contractures and improve the range of motion in joints affected by advanced Dupuytren’s contracture (a disease that is characterised by development of palmar fibrous plaque).
Findings from IMPRESS I and II, which are two independent, double-blind, placebo-controlled studies, reveal the efficacy and tolerability of CCh in improving the
co-primary outcomes of physical penile curvature and psychological bother domains. This intralesional drug is currently not available in Singapore, but has been shown to bring about meaningful change in the penile curvature of men stricken with PD.
(c) surgical optionsSurgical therapy includes plication procedures, incision and grafting, as well as the insertion of inflatable penile prosthesis with manual modeling.
Surgical procedures for correcting penile curvature in men with PD range from penile plication procedures to insertion of penile prosthesis. The type of surgical procedure is determined by the erectile function of the patient. Men with good erections can undergo simple procedures like penile plication, to correct the angle of curvature. The shortcoming of this procedure is penile shortening.
In patients with more severe curvatures, incision and grafting on the plaque with pericardial grafts have shown success. This surgical procedure should only be carried out by urologists who are experienced in the surgical management of PD, as erectile function can be adversely affected by merely incising the tunica albuginea.
The gold standard treatment for men who exhibit both PD and erectile dysfunction is the insertion of an inflatable penile prosthesis with manual modeling. Not only will the patient have no problems with erections after placement of the penile prosthesis, the problem of progressive penile shortening due to
the natural history of PD would also be dealt with.
It would seem that PD is rarely seen locally, but this could be due to a stigma in local culture regarding such treatment, and a lack of awareness on disease diagnosis and management among many physicians.
While PD is a benign condition, the loss of penile length is distressing to most if not all men. The unwanted penile curvature may also create discomfort during sex. A greater awareness of PD could help straighten things out in the bedroom for these men and their partners, enabling them to have a healthier sex life.
feature
References 1. Ronny BW Tan, Premsant Sangkum, Gregory C Mitchell,
Wayne JG Hellstrom. Update on medical management of Peyronie’s disease. Curr Urol Rep. 2014; 15 (6):415. doi: 10.1007/s11934-014-0415-4.
2. Eric J Shaw, Gregory C Mitchell, Ronny BW Tan, Premsant Sangkum, Wayne JG Hellstrom. The non-surgical treatment of Peyronie’s Disease: 2013 update. World J Mens Health. 2013 Dec;31(3):183-92. doi: 10.5534/wjmh.2013.31.3.183. Epub 2013 Dec 24
Dr Tan Ban Wei, Ronny Dr Ronny Tan is a Consultant from the Department of Urology in Tan Tock Seng Hospital. He graduated with MBBS from National University of Singapore (NUS), was elected a Member of
the Royal College of Surgeons (Edinburgh) and conferred a Masters of Medicine (Surgery) from NUS. He completed his Advanced Specialist Training (Urology), board-certified in 2012 and became a Fellow of the Academy of Medicine, Singapore. He received the National Healthcare Group-Health Manpower Development Programme award and undertook his clinical fellowship in andrology, sexual medicine and urology prosthetic surgery with Professor Wayne Hellstrom at Tulane University (USA). He is an executive committee member of the Society for Men’s Health Singapore and a member of the International Society for Sexual Medicine.
shall we dance?
an introduction to dance injuries and the profile of the singapore dancer
What is dance medicine? In simple terms, it is an area
of medicine that focuses on dance-related health and
management, including the prevention and treatment of dance-related injuries.
18 19

feature
dance vs. sportsIn specialised centres such as the Harkness Centre for Dance Injuries at the New York University Langone Medical Center, United States, medical care follows a multidisciplinary model comprising physiotherapists, athletic trainers, kinesiologists as well as surgeons and physicians with training in manning sports and dance-related injuries.
While the treatment of dance injuries shares similarities with the treatment of sports injuries such as those from artistic gymnastics, there are crucial differences between the two. In dance, the choreography often requires movements, which are atypical of those from athletic endeavours, thus resulting in different injury patterns.
dance activity PatternsAn understanding of the physical demands of the dancer as well as the training regime is crucial to the management of dance injuries. In dance classes, where the emphasis is on defining technique, the nature of the exertion demands short periods of activity, interspersed by short periods of rest. This intermittent pattern is carried over to rehearsals and performances, and under longer periods of activity.
Contemporary dance tends to have longer periods of continuous activity, while periods of activity in ballet can be more intense. As such, a dancer’s aerobic fitness falls into the range as athletes undertaking intermittent sports. Fatigue is a risk factor for dance injuries, which occurs more during rehearsals, performances and also deep into training seasons.
(a) BalletBallet emphasises balance and maintaining a vertical alignment, lower limb, trunk flexibility and lower limb explosive strength, to convey lightness in jumps. There is a preponderance of injuries to the lower limb especially on the ankles and knees as well as on the lower back.
The aesthetic emphasis of turn-out (external rotation in the hips) often means that dancers who lack this faculty might be tempted to increase the range with torsion at the knees and even at the foot and ankle. These often contribute to knee pain and stresses to the soft tissue around the medial arch. The amount of time spent perfecting balance on demi-pointe (balancing on the balls of the feet) and en-pointe (on the tips of the toes) can lead to posterior ankle impingement and metatarsalgia.
(b) modern and contemporary danceIn modern dance, certain patterns of movements might predominate in each school, for instance, torso contraction in the Graham technique. However, when we move into contemporary dance, the movement becomes too varied to be codified and often, we have to depend on the dancer to describe or demonstrate aggravating movements.
A typical feature of contemporary dance is ground movements, involving contact between various parts of the body and the ground, hence the occurance of prepatellar bursitis is not uncommon among contemporary dancers.
Dance instruction often depends on visual imagery and kinaesthetic awareness of effectively elicit movements with the correct qualities and they often do not translate into anatomical terms. Many a times, rehabilitation exercises have to be modified, in order to suit dance requirements and instructions translated into kinaesthetic terms to elicit proper muscle activation patterns.
managing dance injuriesA good command of dance movements and requirements not only hastens diagnosis, it also allows for a more graduated return to dance, so that the dancer may maintain her technical expertise without incurring the risk of re-injury.
In a 2012 survey on recreational dancers in Singapore1, it is shown that approximately half of the dancers have existing dance-related injuries. Many are nursing multiple recurrent injuries. Only a third of those seek medical attention and the rest choose to depend on self-care. More troubling is that dancers often see the injuries and pain as part and parcel of dance.
Most injuries are overuse-related and involve the legs, particularly in the areas of the foot and ankle, followed by the knees and finally the back. The pattern of recurrence suggests that technical factors and factors intrinsic to the dancer such as strength or flexibility and inadequate treatment of previous injuries, might be the risk factors.
Interestingly, only a minority of dancers spend time physically
References (1) Survey on Dance Practices and Injury Patterns amongst Singaporean Dancers. Presented in the 22nd Annual General
Meeting of International Association of Dance Medicine and Science in 2012.
dance Medicine workshop series: Movement session for healthcare professionals As part of the initiative to improve healthcare for dancers in Singapore and develop dance medicine in Singapore, the Sports Medicine and Surgery Clinic of Tan Tock Seng Hospital (TTSH), in collaboration with the National Arts Council, conducted a movement session on 2 August 2014.
Hosted at the Singapore Dance Theatre, the session was attended by physiotherapists and sports physicians. The movement session, facilitated by Ms Christina Chan from Frontier Danceland and Dr Jason Chia, Head of Sports Medicine and Surgery Clinic in TTSH, brought the participants through fundamental dance movements in ballet and contemporary dance, accompanied by anatomical demonstrations by Dr Jason Chia.
The programme aims to equip healthcare professionals with an understanding of the anatomical basis of basic dance movement as well as the pedagogy of techniques in dance. The programme also facilitates communication between healthcare professionals and dance patients, thus improving treatment for dance injuries. A second session for healthcare professionals and third session for dancers will be held in the later part of 2014.
dance Medicine workshop in collaboration with the national arts council.
feature
conditioning aspects of their physique other than flexibility. This is despite the fact that dance is essentially a physically demanding discipline.
Clearly, dancers would benefit from access to healthcare professionals with a special interest and training to manage dance-related injuries. While dance medicine is in its infancy, some steps are being made to increase awareness in this field (please see insert on the right) and in the education of healthcare professionals and dancers alike.
Apart from managing injuries when they have already occurred, dance-specific screening is a way where underlying injuries that have not been recovered fully, can be picked up and treated.
Dr Jason Chia Dr Jason Chia is the Head and Senior Consultant of the Sports Medicine and Surgery Clinic of Tan Tock Seng Hospital. He graduated from the National University of Singapore and obtained his Masters
of Sports Medicine from Australia in 2002. He is involved in sports injury management, fitness testing and exercise prescription, weight management, and extracorporeal shockwave therapy (ESWT) as well as gait analysis. He has also written and published a handbook for exercise prescription for general practitioners. Dr Chia’s areas of clinical research include ESWT as well as biomechanical research.
20 21
fitness
core strength for dancers
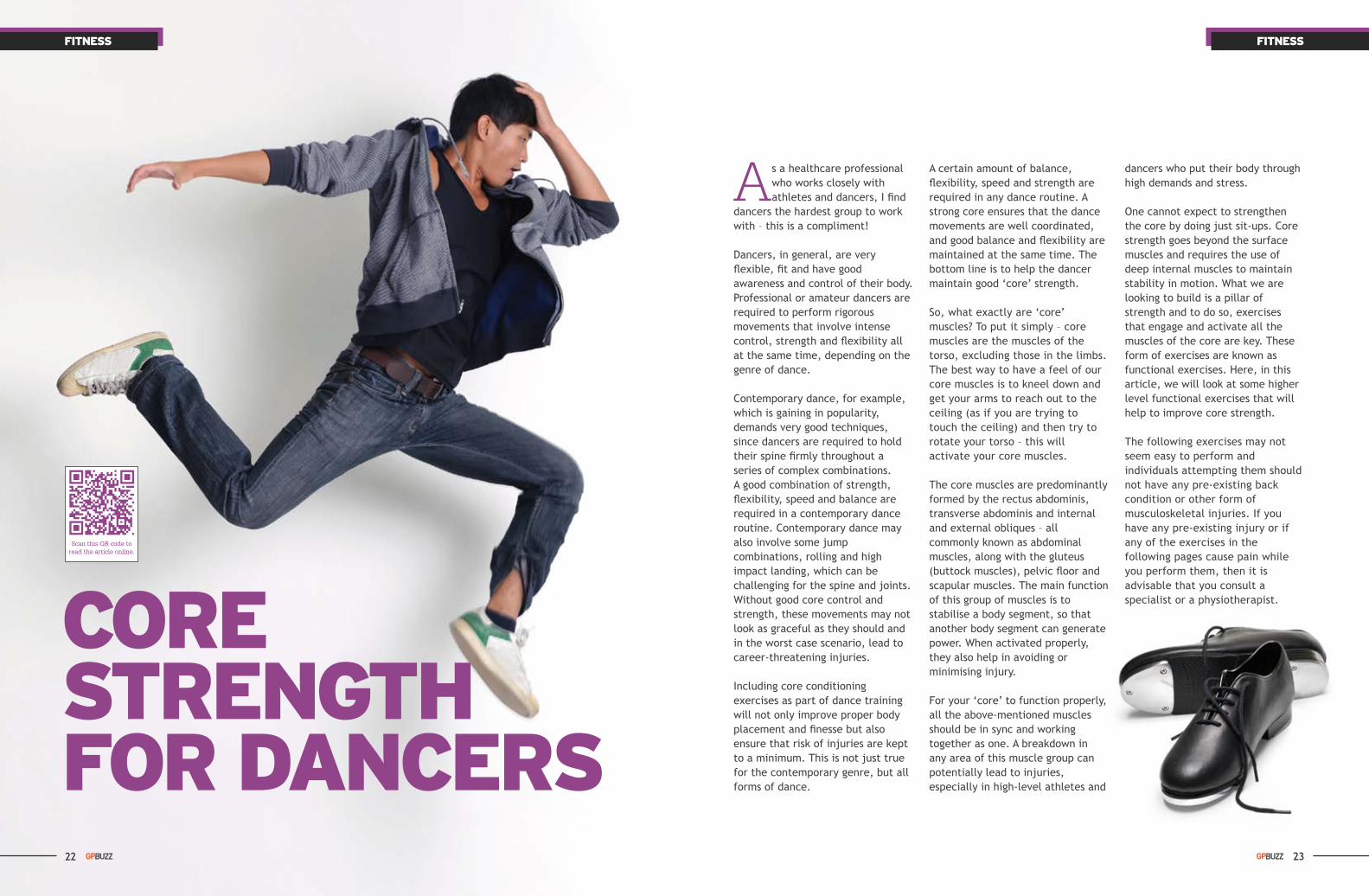
As a healthcare professional who works closely with athletes and dancers, I find
dancers the hardest group to work with – this is a compliment!
Dancers, in general, are very flexible, fit and have good awareness and control of their body. Professional or amateur dancers are required to perform rigorous movements that involve intense control, strength and flexibility all at the same time, depending on the genre of dance.
Contemporary dance, for example, which is gaining in popularity, demands very good techniques, since dancers are required to hold their spine firmly throughout a series of complex combinations. A good combination of strength, flexibility, speed and balance are required in a contemporary dance routine. Contemporary dance may also involve some jump combinations, rolling and high impact landing, which can be challenging for the spine and joints. Without good core control and strength, these movements may not look as graceful as they should and in the worst case scenario, lead to career-threatening injuries.
Including core conditioning exercises as part of dance training will not only improve proper body placement and finesse but also ensure that risk of injuries are kept to a minimum. This is not just true for the contemporary genre, but all forms of dance.
fitness
A certain amount of balance, flexibility, speed and strength are required in any dance routine. A strong core ensures that the dance movements are well coordinated, and good balance and flexibility are maintained at the same time. The bottom line is to help the dancer maintain good ‘core’ strength.
So, what exactly are ‘core’ muscles? To put it simply – core muscles are the muscles of the torso, excluding those in the limbs. The best way to have a feel of our core muscles is to kneel down and get your arms to reach out to the ceiling (as if you are trying to touch the ceiling) and then try to rotate your torso – this will activate your core muscles.
The core muscles are predominantly formed by the rectus abdominis, transverse abdominis and internal and external obliques – all commonly known as abdominal muscles, along with the gluteus (buttock muscles), pelvic floor and scapular muscles. The main function of this group of muscles is to stabilise a body segment, so that another body segment can generate power. When activated properly, they also help in avoiding or minimising injury.
For your ‘core’ to function properly, all the above-mentioned muscles should be in sync and working together as one. A breakdown in any area of this muscle group can potentially lead to injuries, especially in high-level athletes and
dancers who put their body through high demands and stress.
One cannot expect to strengthen the core by doing just sit-ups. Core strength goes beyond the surface muscles and requires the use of deep internal muscles to maintain stability in motion. What we are looking to build is a pillar of strength and to do so, exercises that engage and activate all the muscles of the core are key. These form of exercises are known as functional exercises. Here, in this article, we will look at some higher level functional exercises that will help to improve core strength.
The following exercises may not seem easy to perform and individuals attempting them should not have any pre-existing back condition or other form of musculoskeletal injuries. If you have any pre-existing injury or if any of the exercises in the following pages cause pain while you perform them, then it is advisable that you consult a specialist or a physiotherapist.
22 23
fitness fitness
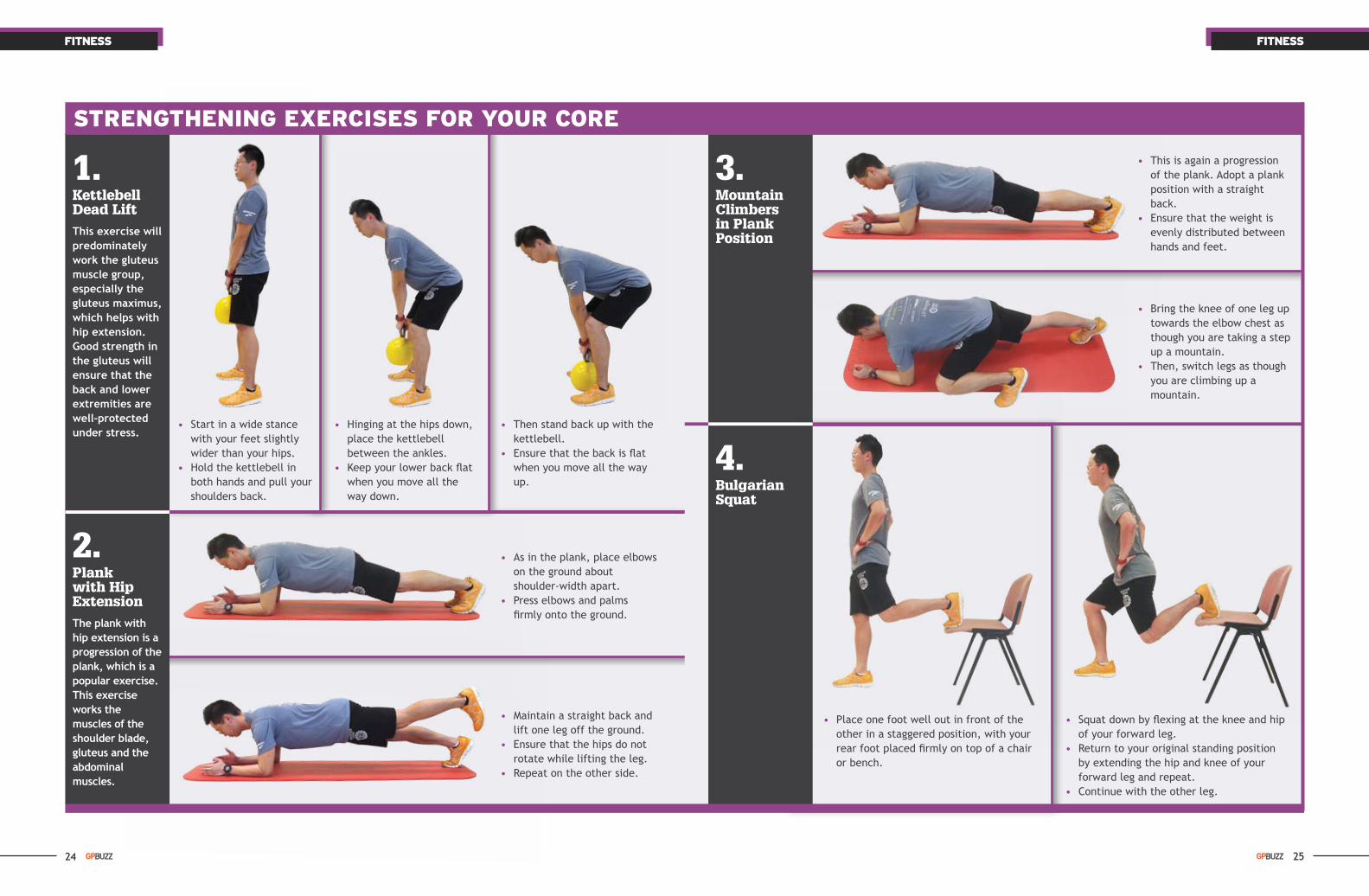
3. mountain climbers in Plank Position
2. Plank with Hip extensionThe plank with hip extension is a progression of the plank, which is a popular exercise. This exercise works the muscles of the shoulder blade, gluteus and the abdominal muscles.
• As in the plank, place elbows on the ground about shoulder-width apart.
• Press elbows and palms firmly onto the ground.
• This is again a progression of the plank. Adopt a plank position with a straight back.
• Ensure that the weight is evenly distributed between hands and feet.
• Then stand back up with the kettlebell.
• Ensure that the back is flat when you move all the way up.
• Maintain a straight back and lift one leg off the ground.
• Ensure that the hips do not rotate while lifting the leg.
• Repeat on the other side.
• Bring the knee of one leg up towards the elbow chest as though you are taking a step up a mountain.
• Then, switch legs as though you are climbing up a mountain.
1. kettlebell dead liftThis exercise will predominately work the gluteus muscle group, especially the gluteus maximus, which helps with hip extension. Good strength in the gluteus will ensure that the back and lower extremities are well-protected under stress.
strengthening exercises for your core
• Start in a wide stance with your feet slightly wider than your hips.
• Hold the kettlebell in both hands and pull your shoulders back.
• Hinging at the hips down, place the kettlebell
between the ankles. • Keep your lower back flat
when you move all the way down.
• Place one foot well out in front of the other in a staggered position, with your rear foot placed firmly on top of a chair or bench.
4. Bulgarian squat
• Squat down by flexing at the knee and hip of your forward leg.
• Return to your original standing position by extending the hip and knee of your forward leg and repeat.
• Continue with the other leg.
24 25

healthy recipe
cinnamon and Walnut Baked apples
Cinnamon and Walnut Baked Apples
(Serves 4)
Ingredients
4 apples (green or red)½ cup walnuts, roughly chopped½ teaspoon cinnamon powder1 tablespoon honey 1 tablespoon margarineLow fat/fat-free vanilla yoghurt
Methods
1. Pre-heat the oven to 180°C.2. Wash and core the apples with an
apple corer, removing all the seeds but leaving the apples whole.
3. Place the apples in an ovenproof dish.
4. Separately, melt the margarine and mix in the walnuts, cinnamon powder and honey.
5. Stuff the mixture into the cored apples.
6. Bake the stuffed apples for 25 to 30 minutes until the apples are soft but do not fall apart.
7. Serve the apples hot, topped with the yoghurt.
Nutrition Information Panel Per ServingEnergy (kcal) 155
Protein (g) 3.9
Total fat (g) 8.1
Carbohydrate (g) 19.4
Sodium (mg) 30.0
Calcium (mg) 41.2
fitness
5. Bear crawlsThe bear crawl strengthens your midsection and improves your ability to stabilise your spine.
strengthening exercises for your core
• Get on to your hands and knees and lift hips slightly to raise knees off the floor. Make sure to brace your abs.
• Your knees and hands should be directly under your hips and shoulders respectively.
• Step forward using your left hand and right foot to propel yourself forward.
• Do the same with the right hand and left foot immediately and so on.
Haris Mohamed Mr Haris Mohamed is the Principal Physiotherapist from the Department of Physiotherapy in Tan Tock Seng Hospital. He also helms the musculoskeletal outpatient team. Haris has extensive
experience in musculoskeletal and sports physiotherapy and has been working in the outpatient setting since 1999.
He has a special interest in dance injuries and works closely with dancers, especially contemporary dancers. He conducts screening for dancers to identify potential injuries and helps them in injury management.
26

CliniC B1B– Orthopaedic Surgery
• Hand Procedure Suite
– Rheumatology, Allergy and Immunology
• Intravenous Infusion Day Facility
CliniC 2B– Gastroenterology and
Hepatology Our sub-specialties include: • General Gastroenterology • Hepatology (Liver) Service • Inflammatory Bowel Disease • Gastrointestinal Endoscopy • Pancreato-biliary Diseases • Upper Gastrointestinal Motility • Nutrition
– General Surgery Our sub-specialties include: • General Surgery • Colorectal Service • Bariatric and Weight
Management Services • Upper Gastrointestinal Service • Head and Neck Surgical
Services • Endocrine Service
• Liver, Pancreas and Biliary Services
• Vascular Service • Veins Service • Thoracic Service • Plastics, Reconstructive and
Aesthetics Services
– Urology Our sub-specialties include: • General Urology • Andrology and Men’s Health • Adrenal Surgery • Continence and Voiding
Dysfunction • Endo-urology and Stone
Surgery • Female Urology • Minimally Invasive Surgery and Laparoscopic Surgery • Neuro-urology • Prostate Surgery • Reconstructive Urology • Robotic Surgery • Subfertility and Sexual
Dysfunction • Urologic Cancer Surgery
– Endoscopy• Colonoscopy• Flexible Cystoscopy• Gastroscopy
CliniC 4B
– Diabetes and Endocrinology – General Medicine – Haematology – Psychological Medicine – Renal Medicine – Respiratory and Critical
Care Medicine– Travellers' Health and
Vaccination Clinic (THVC)
CliniC 6B
- Complementary Integrative Medicine• Acupuncture• Cupping• Dietary Advice• Pain-relief Physiotherapy
- DentalOur specialist services include:• Braces• Root Canal Treatment• Wisdom Tooth Surgery• Dental Implants
Multi-DisCiplinary speCialist CareTTSH PEARL’s suite of clinics and services is guided by the four pillars of care through Evidence Care, Destination Care, Team Care and Personalised Care. We remain committed to delivering a higher level of patient care as we value our patients most.
CliniC B1BOrthopaedic Surgery Tel: (65) 6889 4055 Email: [email protected]
Rheumatology, Allergy and Immunology Tel: (65) 6889 4027 Email: [email protected]
CliniC 2BTel: (65) 1800-PEARL-00
(65) 1800-73275-00 Email: [email protected]
CliniC 4BTel: (65) 1800-PEARL-00
(65) 1800-73275-00 Email: [email protected]
CliniC 6BComplementary Integrative MedicineTel: (65) 6889 4628 Email: [email protected]
DentalTel: (65) 6889 4627 Email: [email protected]