heart failure update: tennessee acp annual … failure update: tennessee acp annual meeting 2016 ......
TRANSCRIPT

Heart Failure Update:Tennessee ACP Annual Meeting 2016
Stacy F. Davis, MDSt. Thomas Mid-town Comprehensive Heart Failure Center
Nashville, TN(615-329-5144)
Thomas Rowlandson, 1810Harvard Countway Medical LibraryBoston, MA
Heart Failure Therapy
Withering, William.“An account of the foxglove and some of its medical uses: with practical remarks on dropsy and other diseases.” London: J and J Robinson, 1785.

Optimal Heart Failure Therapy Pre 1980s: Non Pharmacologic Bed rest, inactivity,
Fluid restriction, Dig, Diuretics
1980s: Pharmacologic Dig, Diuretics, Vasodilators, Inotropes
1990s: Pharmacologic Dig, Diuretics, Neuro-humoral interventions
2000s: Device CRT, ICD, VADs
2010s: Cellular/Genetic Gene Therapy, Cell Regeneration, Xenotransplant

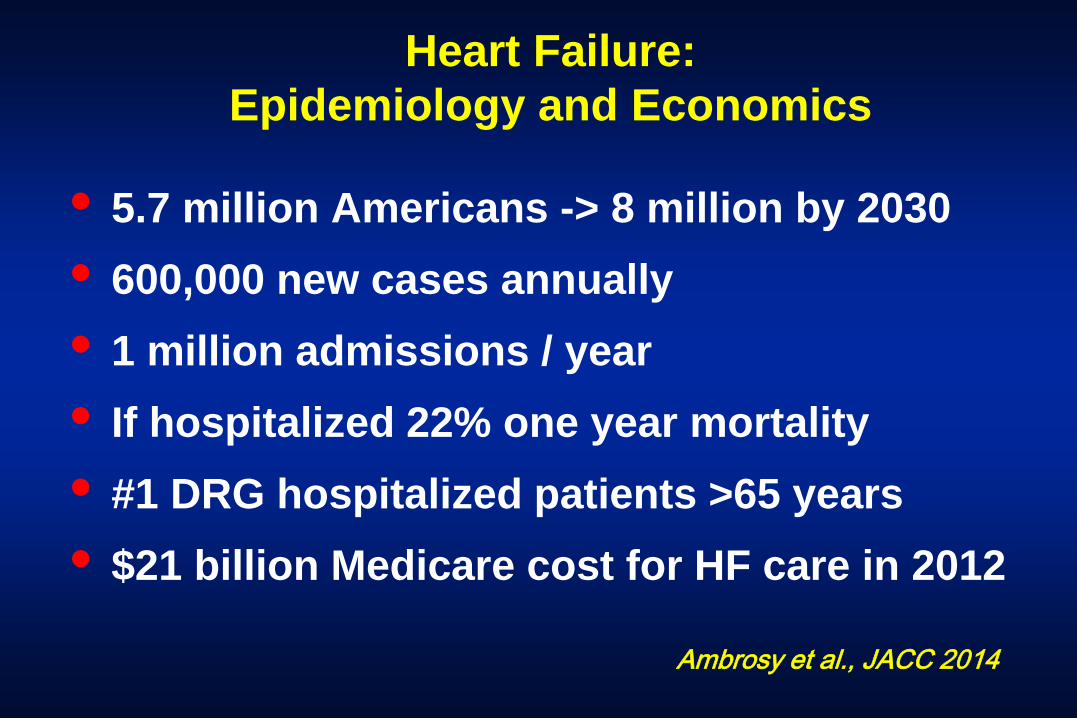
Heart Failure: Epidemiology and Economics
• 5.7 million Americans -> 8 million by 2030• 600,000 new cases annually• 1 million admissions / year • If hospitalized 22% one year mortality • #1 DRG hospitalized patients >65 years• $21 billion Medicare cost for HF care in 2012
Ambrosy et al., JACC 2014


NYHA Class: One Year Mortality
Stevenson, Circulation 2005
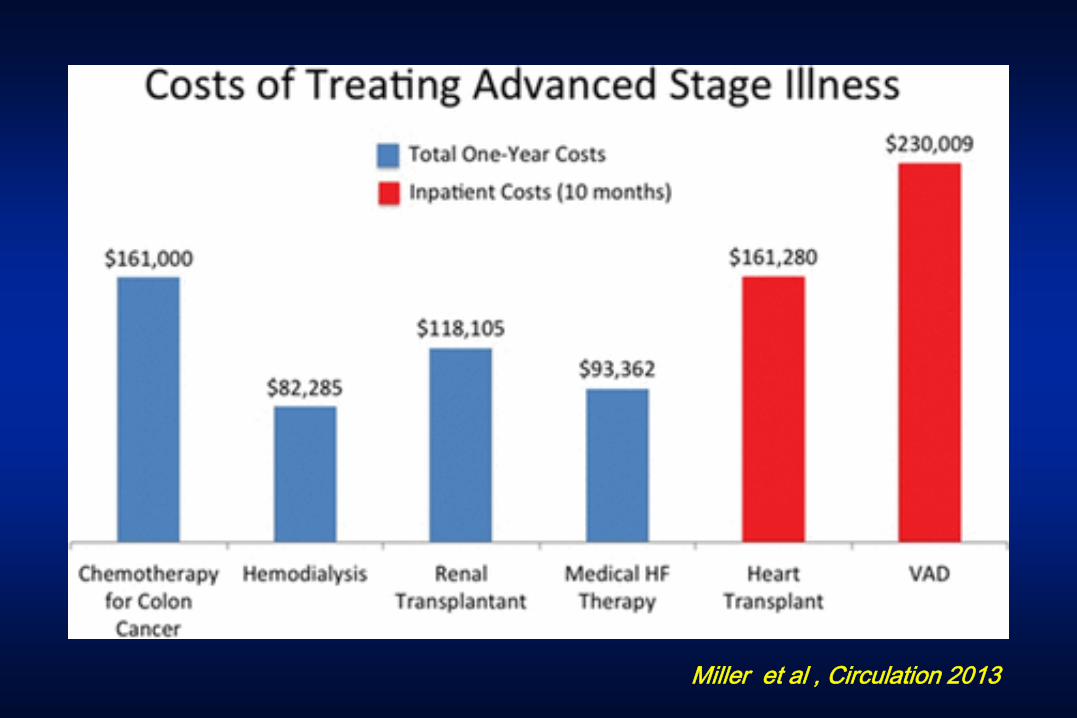
Miller et al , Circulation 2013
Case History
ID: 58 year old woman with diabetesand paroxysmal atrial fibrillation admitted for total knee replacement
HPI: Day #1
Seen immediately post-op with dyspnea after volume replacement for hypotension.

Case HistoryExam: Afebrile, tachycardic, pale, wheezing,
RUQ tenderness
CXR: “Infiltrate – Bilateral pneumonia”
Labs: AST = 1261; ALT = 1311; LDH = 1566; TB = 1.7; DB = 1.4, Troponin I <0.05Glucose =150, WBC = 10.1
ABG: 7.47 / 109 / 17 / 13 (2L)

12 Lead ECG
Sinus tachycardia, LVH repolarization changes, biatrial enlargement

Case History
You primary concern is:
(a) Pulmonary embolus(b) Aspiration pneumonia(c) Heart failure(d) Atrial fibrillation(e) All of the above

Case HistoryYour next step is to transfer to the SICU and:
(a) Treat pneumonia with antibiotics and COPD with nebulizer therapy.
(b) Evaluate for cholecystitis and obtain an abdominal ultrasound.
(c) Suspect CHF, begin diuretics and request an echocardiogram.
(d) Consider a pulmonary embolus and schedule a high resolution chest CT scan.

CHF on CT Scan
Cardiomegaly, pulmonary congestion

Heart Failure: MRI

Echocardiography and CHF
Global LV Hypokinesis; LVEF = 10%; LVEDD=6.7, biatrial enlargement

Case History
Are there other helpful lab tests?
(a) FT4, TSH(b) BNP(c) Ferritin(d) Viral titres(e) All of the above

Case History
Lab Results:
BNP: 1200FT4: 1.1TSH: 2.8Ferritin: <300Viral titres: pending

Case HistoryDay #2: IV diuretics started, but she does not improve.
VS: BP = 108/66; P = 122; RR = 26; T = 98.6Neck: JVP = 15 cm; No carotid bruitsCV: Stach, S1, S2, S3, 2/6 hsm LSB to apex
PMI diffuse, lat displaced, RV heave Pulm: Decreased breath sounds, dull at basesAbd: Liver 12 cm, RUQ tender, no massesExt: 1+ pedal, presacral edema, pulses 2+
No cyanosis or clubbing
Case History
Day #2: Additional test results
Labs: Na = 130; K = 3.3; BUN / Cr = 42 / 1.9;ALT = 225; AST = 76; LDH = 328;
Viral Titres: Toxo, Cocksackie, Echovirus (-)(+) IgG HAV; (-) HBV
CXR: Cardiomegaly, pulmonary vascularcongestion, large pleural effusions

Case HistoryThe next step is:
(a) Tap the large pleural effusions
(b) Discontinue furosemide
(c) Right Heart Catheterization
(d) Coronary Angiography
(e) Cardiac Resynchronization Therapy
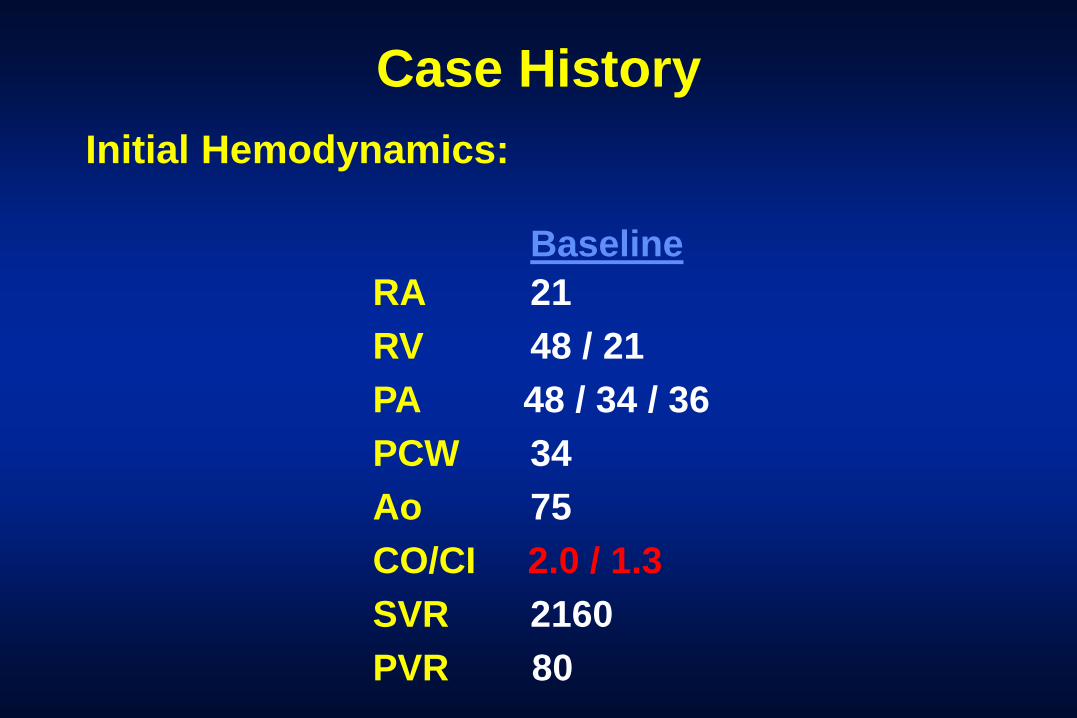
Case HistoryInitial Hemodynamics:
BaselineRA 21RV 48 / 21PA 48 / 34 / 36PCW 34Ao 75CO/CI 2.0 / 1.3SVR 2160PVR 80
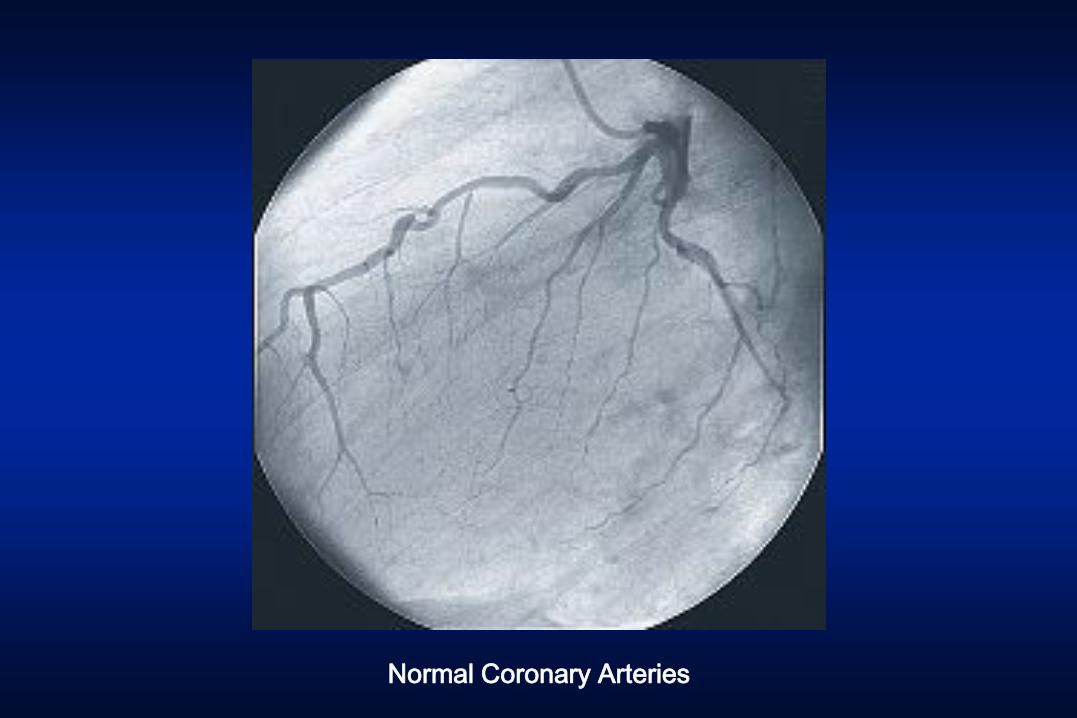
Normal Coronary Arteries
Case History
Days 3-5: The patient receives IV diuretics and inotropes. Her symptoms improve.
Day 6: She is transitioned to oral furosemide, enalapril, carvedilol, and spironolactone. She is ready for discharge.
Case History
Important maneuvers to avoid readmission:
(a) Outpatient appointment in one week(b) Teach self-monitoring of weight, fluid and
sodium intake (c) Establish system for outpatient monitoring(d) Address compliance issues pre-discharge(e) All of the above
Heart Failure: Major Clinical Problems
• Exercise intolerance• Fluid retention • Recurrent hospitalization• Arrhythmias• Increased mortality

Kannel et al., British Heart Journal 1994
During 10 years Heart Failure develops in:18% of women with diabetes16% of men with diabetes
8% of women with high blood pressure12% of men with high blood pressure
30% of women after heart attack30% of men after heart attack
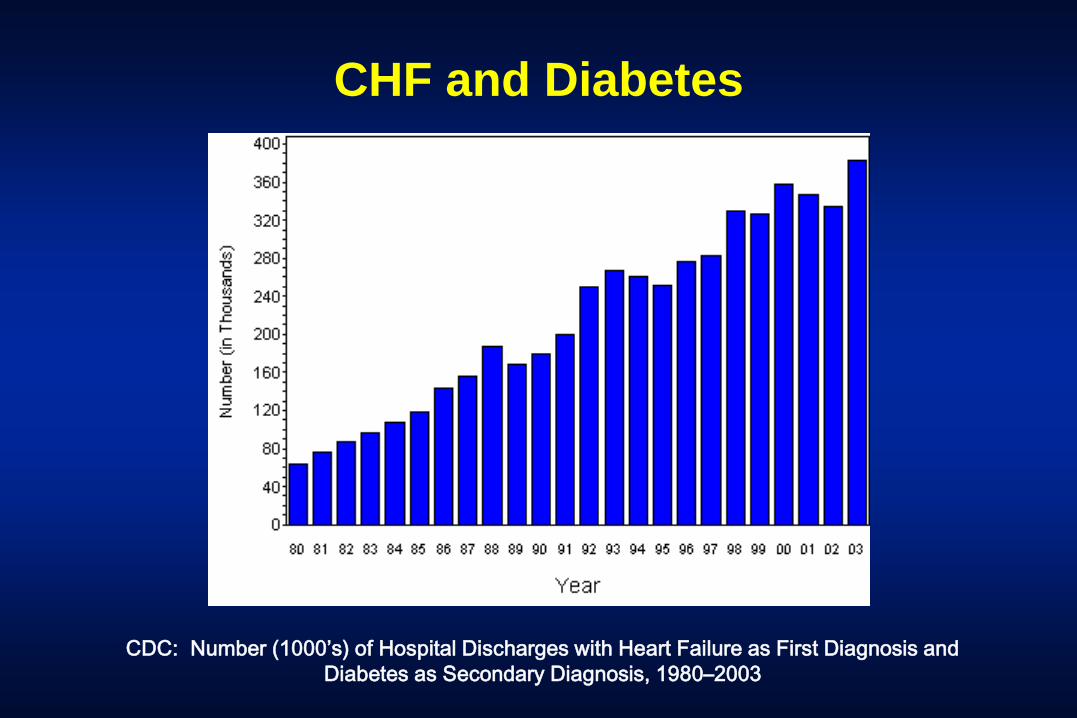
CHF and Diabetes
CDC: Number (1000’s) of Hospital Discharges with Heart Failure as First Diagnosis and Diabetes as Secondary Diagnosis, 1980–2003

Factors that May Precipitate CHF
• Unrecognized fluid retention• Inadequate education / compliance• Recurrent ischemia• Tachyarrhythmia (AFib, VT)• Systemic viral infection• Heavy EtOH use • Endocrine abnormalities (thyroid)• Negative inotropes / NSAIDs / glitazones
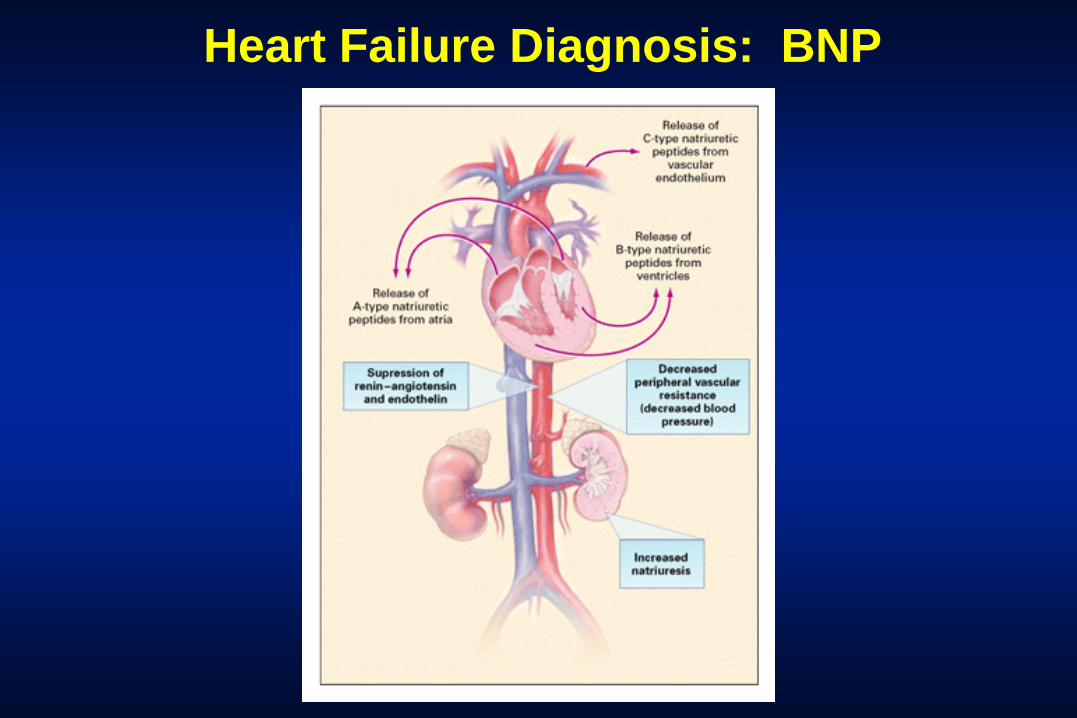
Heart Failure Diagnosis: BNP

Heart Failure: BNP
•Higher with more severe CHF and LV dysfunction
•Chronic CHF: Independent predictor of death
•Acute CHF: Independent predictor of CV mortality

Maisel A et al., NEJM 2002
Heart Failure: BNP

Heart Failure: BNP
<100 CHF unlikely (<2%)COPD, PE, Asthma, Pneumonia, Sepsis100-500 CHF possible (90%)Stable LV dysfunction, RV failure due to pulmonary hypertension, Renal failure
>500 CHF very likely (95%)
BNP Consensus Panel 2004

Heart Failure: BNP
Maisel et al., NEJM 2002

Heart Failure: BNP
• In volume overload states, drop in BNP occurs with diuresis
•Doesn’t always correlate with PCW•Draw on admit, to assess treatment
effect, at discharge, not daily•Failure to fall suggests poor prognosis
BNP Consensus Panel 2004

Elevated BNP: False Positives
• Elderly• Females• HOCM• Pulmonary embolism (30%)• COPD, Asthma• Renal insufficiency (normal <200)
Low BNP: False Negatives
• Acute CHF (1-2 hours)• Acute MR • Flash pulmonary edema• Obesity (BMI > 30%)


Optimal Heart Failure Therapy: Treatments that Improve Survival
• ACE Inhibitors
• Beta Blockers
• Aldosterone Antagonists
• Angiotensin - Neprilysin Inhibitor
• Implantable Cardioverter – Defibrillator
• Cardiac Resynchronization
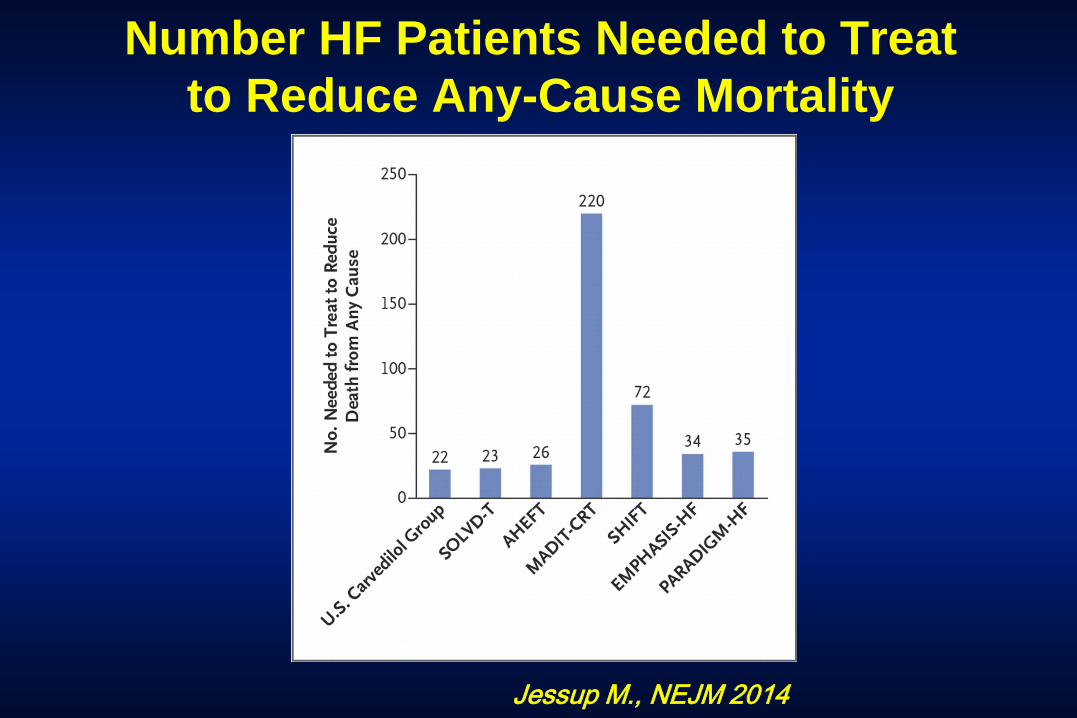
Jessup M., NEJM 2014
Number HF Patients Needed to Treat to Reduce Any-Cause Mortality
Optimal Heart Failure Therapy: Angiotensin - Neprilysin Inhibitor
• PARADIGM HF: Sacubitril-Valsartan vs. Enalapril + standard therapy
• NYHA Class II-IV, LVEF < 40%
• Primary Composite Endpoint: CV death or HF Hospitalization
McMurray et al. , NEJM 2014
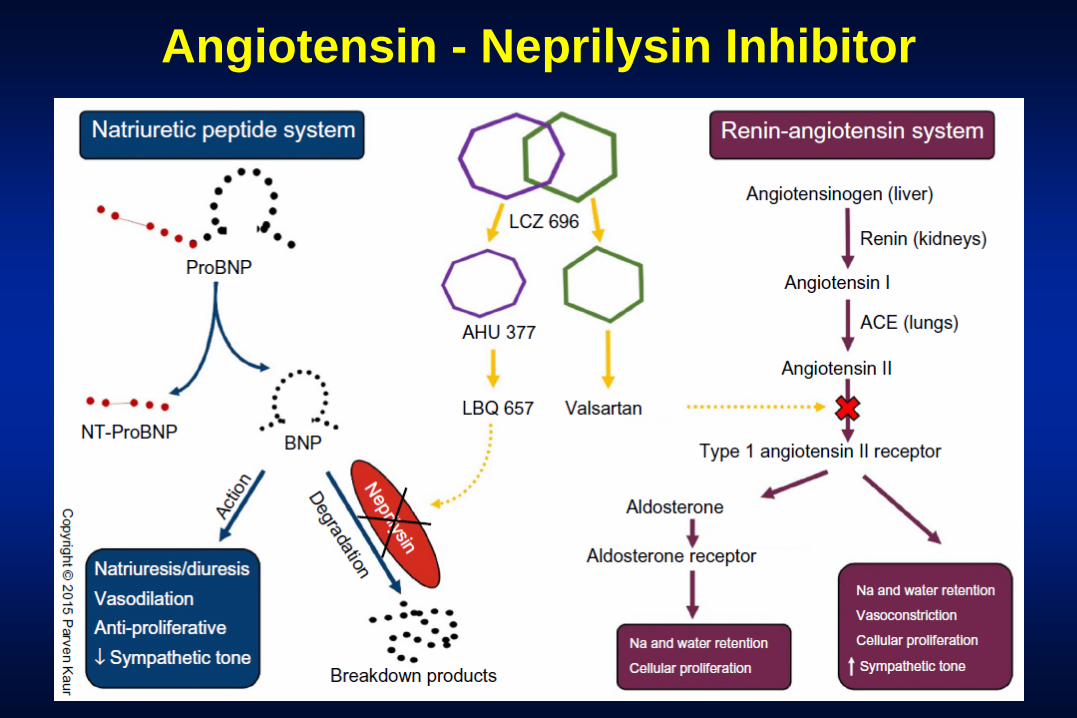
Angiotensin - Neprilysin Inhibitor

McMurray et al. , NEJM 2014
PARADIGM HF: Sacubitril - Valsartan

Angiotensin - Neprilysin Inhibitor: Sacubutril- Valsartan vs. Enalapril
• Composite Endpoint: 21.8% vs. 26.5% (p < 0.001)
• Lower Proportion CV Deaths: 13.3% vs. 16.5% (p< 0.001)
• Reduced Risk of HF Hospitalization by 21% (p <0.001)
• Decreased Symptoms and HF Limitations (p = 0.001)
McMurray et al. , NEJM 2014

McMurray et al. , NEJM 2014
Angiotensin - Neprilysin Inhibitor: Sacubutril- Valsartan vs. Enalapril
• Higher % hypotension and angioedema
• Lower % renal impairment, cough, and hyperkalemia
• Number needed to treat to prevent one CV death (21 vs. 32)

Implantable Cardioverter-Defibrillators

ICDs and CHF: SCD HeFT
Bardy et al., NEJM 2005

Cardiac Resynchronization

Cardiac Resynchronization
Abraham et al., NEJM 2002

Optimal Heart Failure Therapy: Other Considerations
• Angiotensin-2 Receptor Blockers
• Isorbide Dinitrate and Hydralazine
• Digoxin
• Diuretics
• Ivabradine
Heart Failure and Heart Rate Lowering: Ivabradine
• SHIFT: Ivabradine vs. Placebo + standard HF therapy
• “Symptomatic HF”, LVEF < 35%, one HF admit prior year
• NSR with heart rate > 70 bpm
• Primary Composite Endpoint: CV death or HF Hospitalization
Swedberg et al. , Lancet 2010

Swedberg et al., Lancet 2010
HF and Heart Rate Lowering : Ivabradine
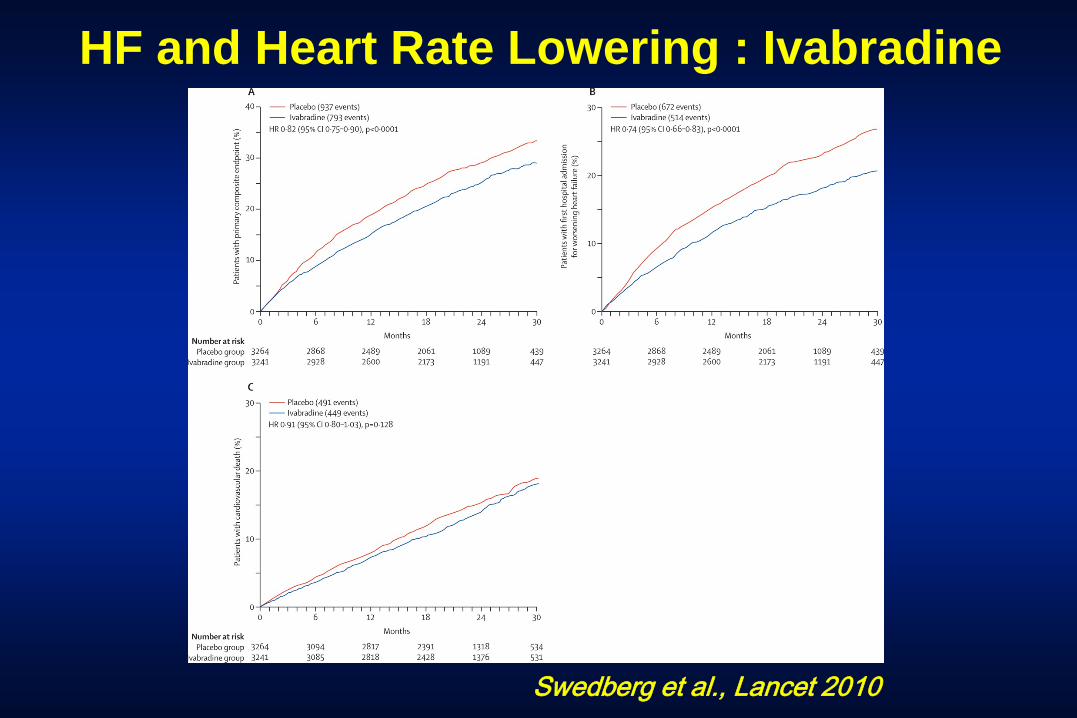
Swedberg et al., Lancet 2010
HF and Heart Rate Lowering : Ivabradine
SHIFT: HF and Heart Rate LoweringIvabradine vs. Placebo
• Composite Endpoint Death or HF Admission: 24% vs. 27% (p < 0.0001)
• Reduced Risk Admission Worse HF: 16% vs. 21% (p <0.001)
• Reduced Death Due to HF: 3% vs. 5% (p=0.14)
• Fever Serious Events (p=0.025)
• More Symptomatic Bradycardia: 5% vs. 1% (p< 0.001) Swedberg et al. , Lancet 2010

Heart Failure: A Continuum of Options
Heart Failure New Drug Therapies PreventiveOptimization Cardiology
Pacemakers / ICDs High Risk Revascularization
Mechanical Assist Devices Surgical / Cath Alternatives
Cardiac or Cell Transplantation
Man & His Machines

Summary
• Heart failure is common
• Look for signs and symptoms
• Most patients improve with therapy
• Treat reversible processes
• Initiate optimal medical therapy
• Educate the patient and family

Heart Failure: When to Refer
• Optimize medical therapy• Heart failure of uncertain cause• Close follow-up and intensive education• Frequent readmissions• Pacemaker / ICD to improve survival or QOL• Consider inotropic therapy• Evaluate for transplant or VAD
St. Thomas Heart Mid-Town Comprehensive Heart Failure Program
(615-329-5144)
• Dr. Stacy F. Davis CHF / Transplant / VAD• Teresa Jackson, NP CHF Outpatient NP• Sandra Byrd, NP CHF Inpatient NP• Kathy Norton, CCRN CHF Nurse Educator• Debbie Glover, CCRN CHF Nurse Educator