heat illness - information technology...
TRANSCRIPT
HEAT ILLNESS
Statistics
• High school athletes, especially males, are at the highest risk of suffering exertional heat illness requiring treatment in U.S. hospital emergency rooms.
• 31 high school players died of heat stroke complications between 1995 and 2009.
• 64.7% of football players sustaining a heat illness were either overweight or obese.
• The number of heat-related injuries from 1997 to 2006 increased 133 percent. Youth accounted for the largest proportion of heat-related injuries or 47.6 percent.
• 2/3 of kids show up for practice at least significantly dehydrated. • 2011 was one of the the worst heat-stroke period in 35 years with 5
heat related deaths.
HEAT STROKE
HEAT STROKE
• Core temperature rises (104) • Mental Status changes • May still be sweating • Seizures • Permanent brain injury • Death
Problem
• We are at high risk every day until November • High temperature and humidity • Play Station kids • Air Conditioning • Younger athletes at more risk than adults • Obesity • Nutrition • Hydration before participation

Prevention and Preparation
• Acclimation- at least seven exposures • Fluids and breaks • Use the shade • Immersion • Light colored clothing. Remove helmets when
possible • Preload with crushed ice • Monitor weights • Urine color • Sleep
Fluid replacement
• Hydration Before Exercise
• Drink about 15-20 fl oz, 2-3 hours before exercise • Drink 8-10 fl oz 10-15 min before exercise • Hydration During Exercise
Drink 8-10 fl oz every 10-15 min during exercise • If exercising longer than 90 minutes, drink 8-10 fl
oz of a sports drink (with no more than 8 percent carbohydrate) every 15 - 30 minutes.
Beware
• Illness • Sunburn • Medication • Diarrhea • Previous heat injury
Treatment
• Urgent Cooling. Time is brain. • 24 times faster in water than air • Ice water immersion is by far the most
effective • Cooling is more important than transporting.
Performance Decreases
• Concentration: keep hydrated and cool to teach
• Strength and speed – • Psalm 22:15 My strength is dried up like a
potsherd, and my tongue sticks to the roof of my mouth; you lay me in the dust of death.
• Endurance • Basketball decease in speed and shot
performance
Cramps: Keeping them in the game
• Salt • Bananas • Magnesium • Fluid, cool and flavored • Food • Anxiety
Sodium
• Fluid replacement. 1/2 tsp salt for ½ liter fluid sports drink
• Crampers lose more sodium. Up to 10 tsp in a day of 2 a day practice.
• Sodium loss ranges from 1 to 6 thousand mg/hr. Up to 24,000 mg in 4 hour practice.
• ¼ tsp salt is 590 mg sodium. • Can lose 2 liters fluid in one hour
New Rules coming soon
At minimum NCAA guidelines.
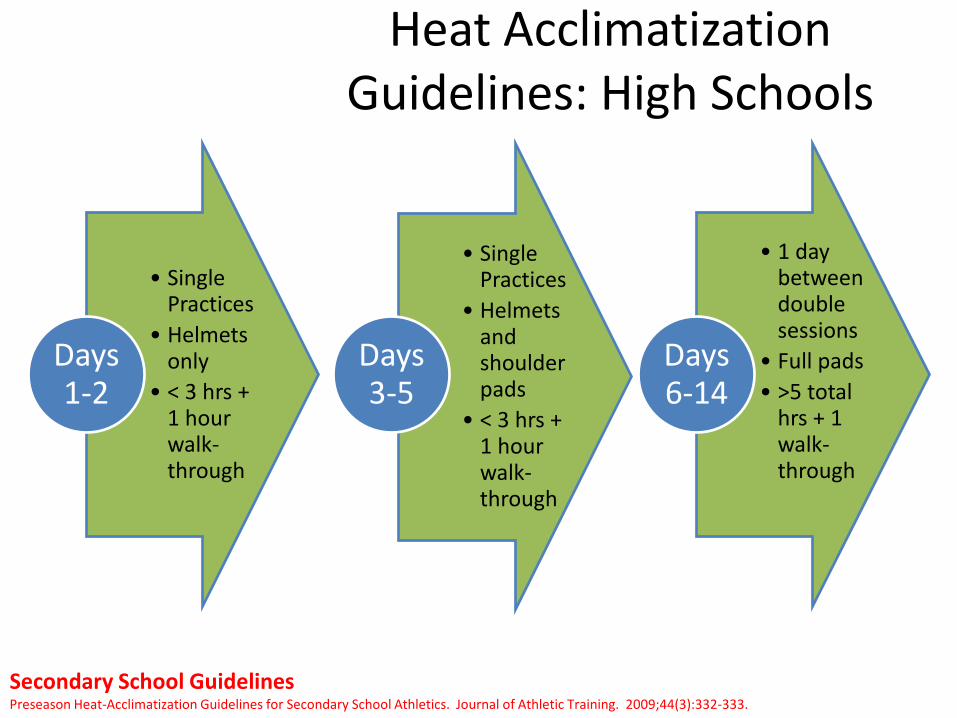
Heat Acclimatization Guidelines: High Schools
• Single Practices
• Helmets only
• < 3 hrs + 1 hour walk-through
Days 1-2
• Single Practices
• Helmets and shoulder pads
• < 3 hrs + 1 hour walk-through
Days 3-5
• 1 day between double sessions
• Full pads • >5 total
hrs + 1 walk-through
Days 6-14
Secondary School Guidelines Preseason Heat-Acclimatization Guidelines for Secondary School Athletics. Journal of Athletic Training. 2009;44(3):332-333.
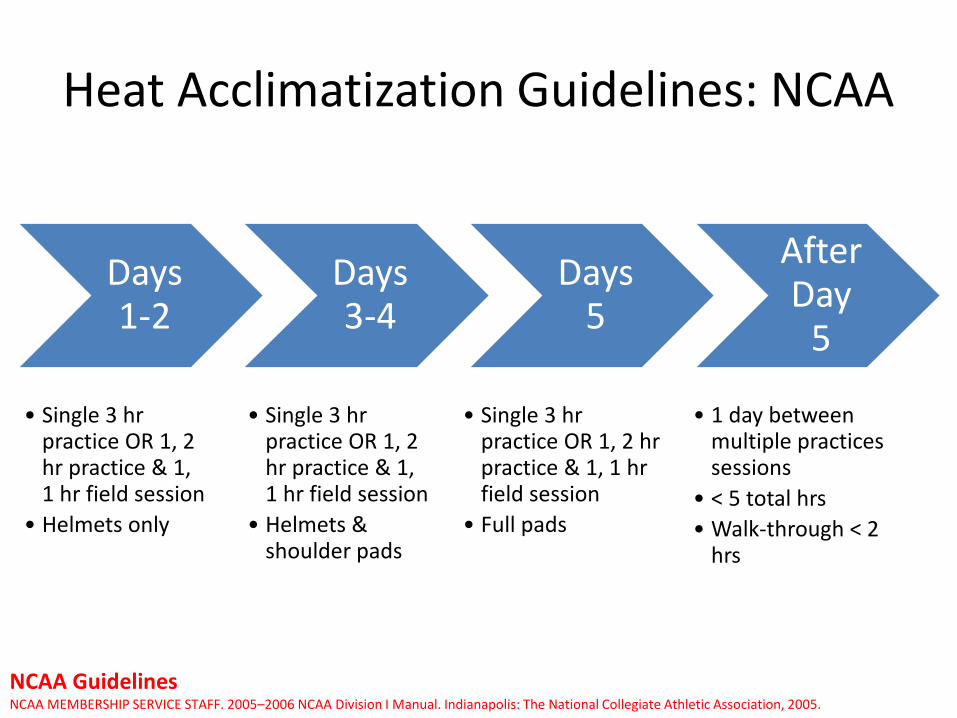
Heat Acclimatization Guidelines: NCAA
Days 1-2
• Single 3 hr practice OR 1, 2 hr practice & 1, 1 hr field session
• Helmets only
Days 3-4
• Single 3 hr practice OR 1, 2 hr practice & 1, 1 hr field session
• Helmets & shoulder pads
Days 5
• Single 3 hr practice OR 1, 2 hr practice & 1, 1 hr field session
• Full pads
After Day
5
• 1 day between multiple practices sessions
• < 5 total hrs • Walk-through < 2
hrs
NCAA Guidelines NCAA MEMBERSHIP SERVICE STAFF. 2005–2006 NCAA Division I Manual. Indianapolis: The National Collegiate Athletic Association, 2005.


Ksi.uconn.edu

Preventing Sudden Death During Sport & Physical Activity
2011 book-Jones & Bartlett 16 Chapters, each focused on a
cause of death Each chapter written by
content expert NATA/AMSSM/ACSM members
well represented 15 ATC’s, 15 MD’s, 15 PhD’s
involved with writing
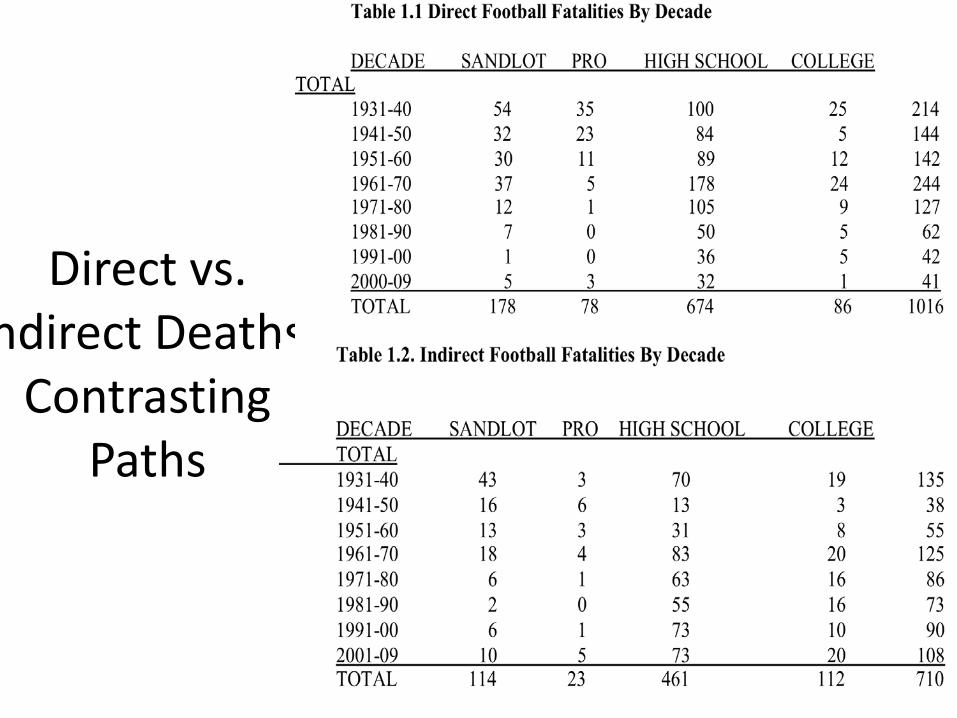
Direct vs. ndirect Deaths:
Contrasting Paths
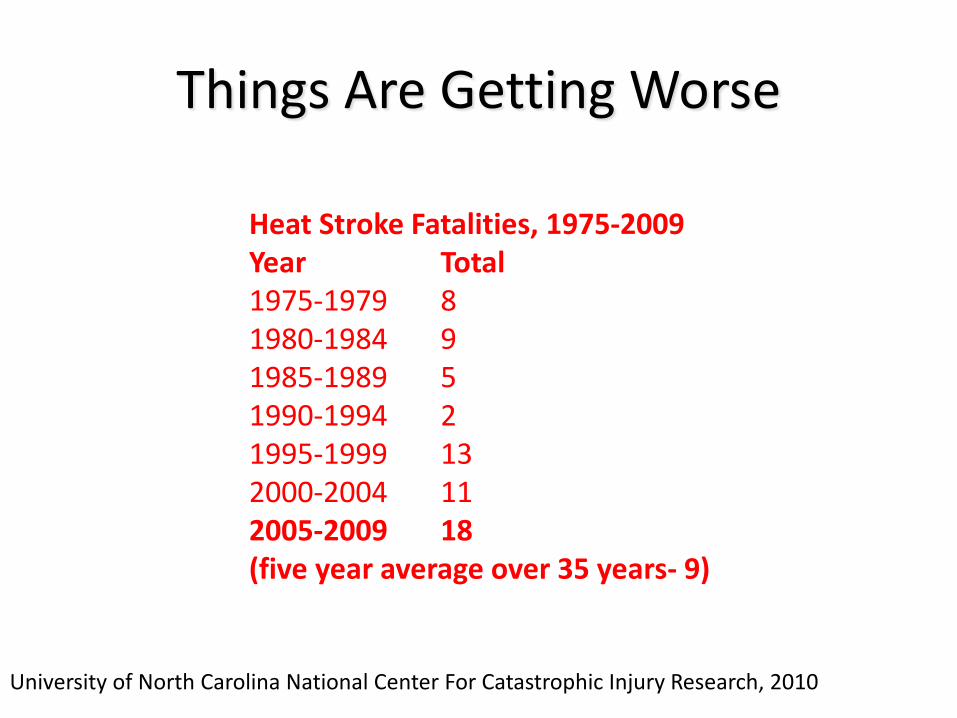
Things Are Getting Worse
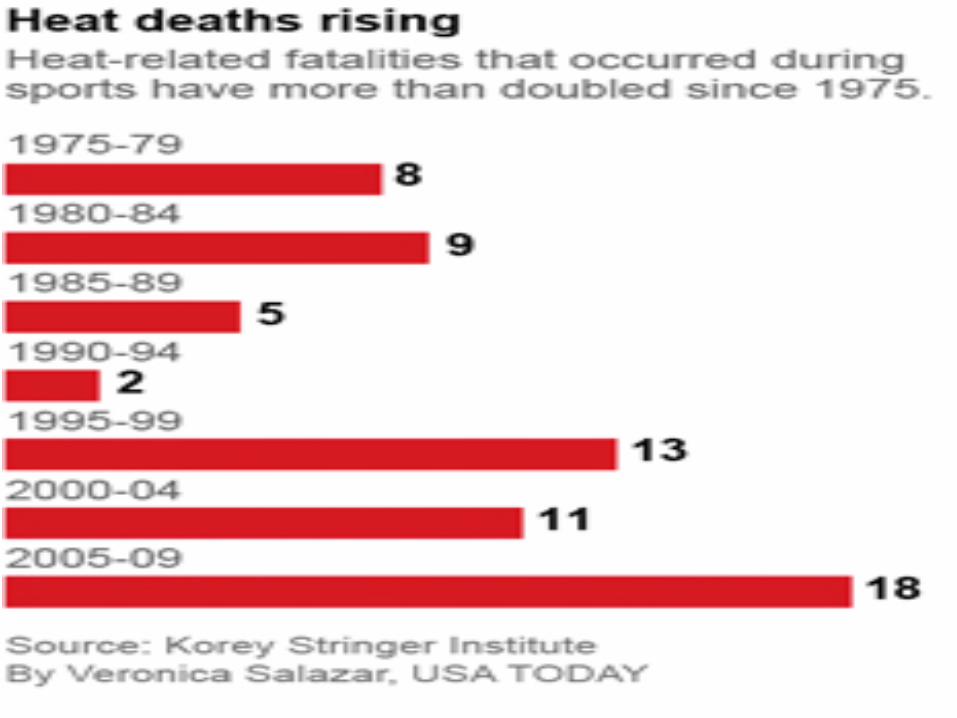
Heat Stroke Fatalities, 1975-2009 Year Total 1975-1979 8 1980-1984 9 1985-1989 5 1990-1994 2 1995-1999 13 2000-2004 11 2005-2009 18 (five year average over 35 years- 9)
University of North Carolina National Center For Catastrophic Injury Research, 2010
ITEM #10
Adapt Nationwide High School Heat Acclimatization Guidelines

2009
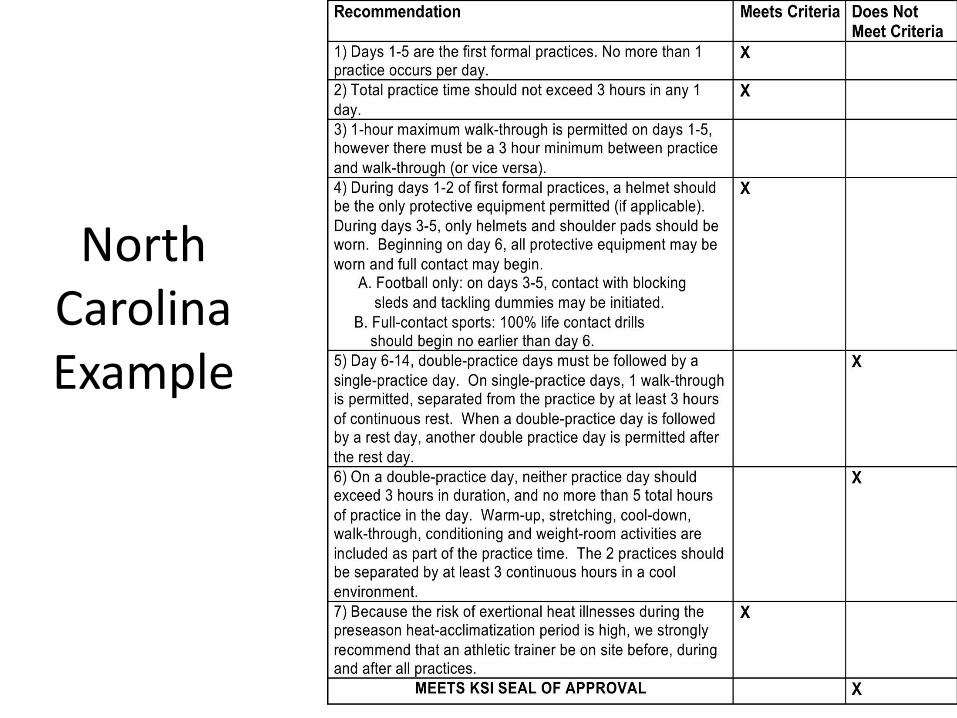
North Carolina Example
ITEM #8
Accurate Body Temperature Assessment at Point of Care for
Collapsed Athlete
2 Basic Rule-In Considerations
Excessive exercise induced hyperthermia Generally greater than >105oF at time of collapse But, a temp above this does not always mean EHS
CNS dysfunction But, absence of CNS problem does not rule out EHS,
remember possible lucid interval (CNS will show itself)
Options for Assessing Core Temperature
• Axillary • Oral • Tympanic • Temporal Artery • Forehead Sticker • Ingestible Thermistor • Esophageal • Rectal
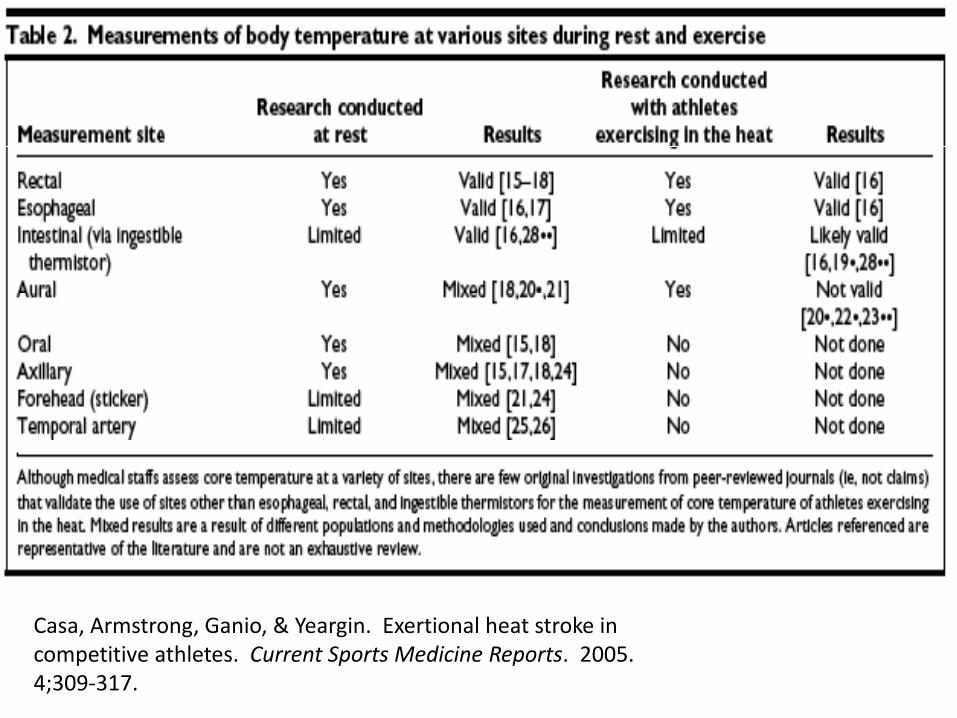
Casa, Armstrong, Ganio, & Yeargin. Exertional heat stroke in competitive athletes. Current Sports Medicine Reports. 2005. 4;309-317.
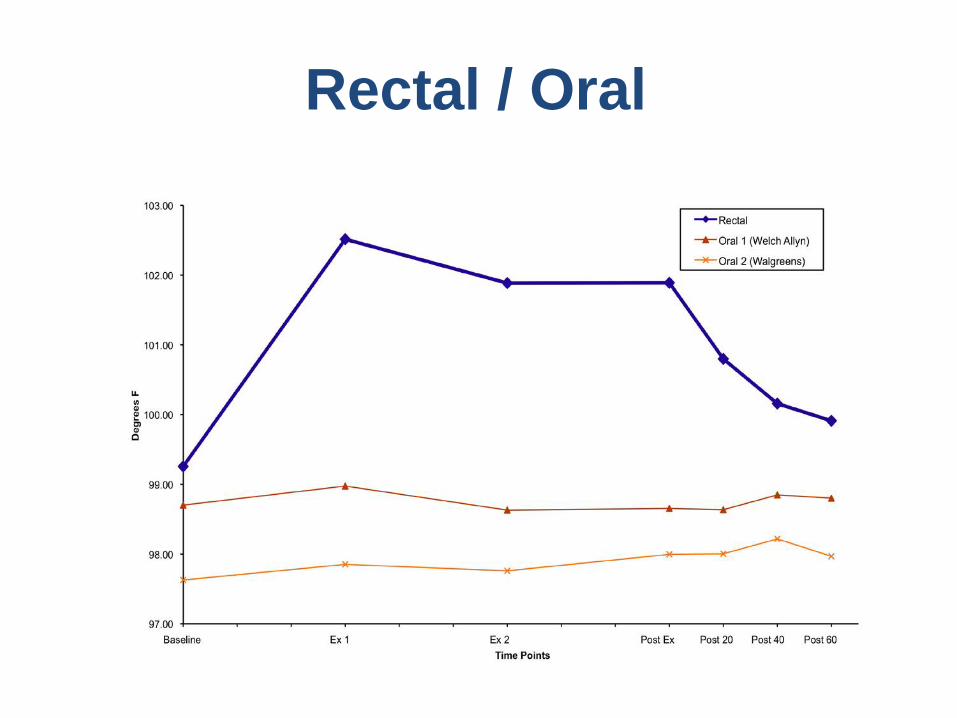
Rectal / Oral
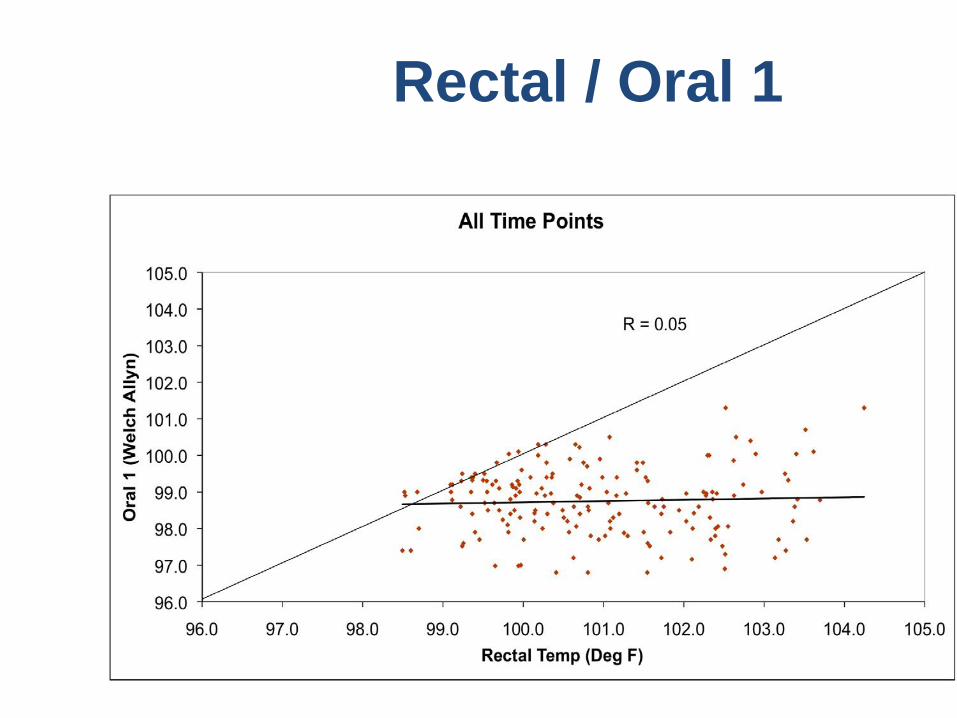
Rectal / Oral 1

Rectal / Tympanic
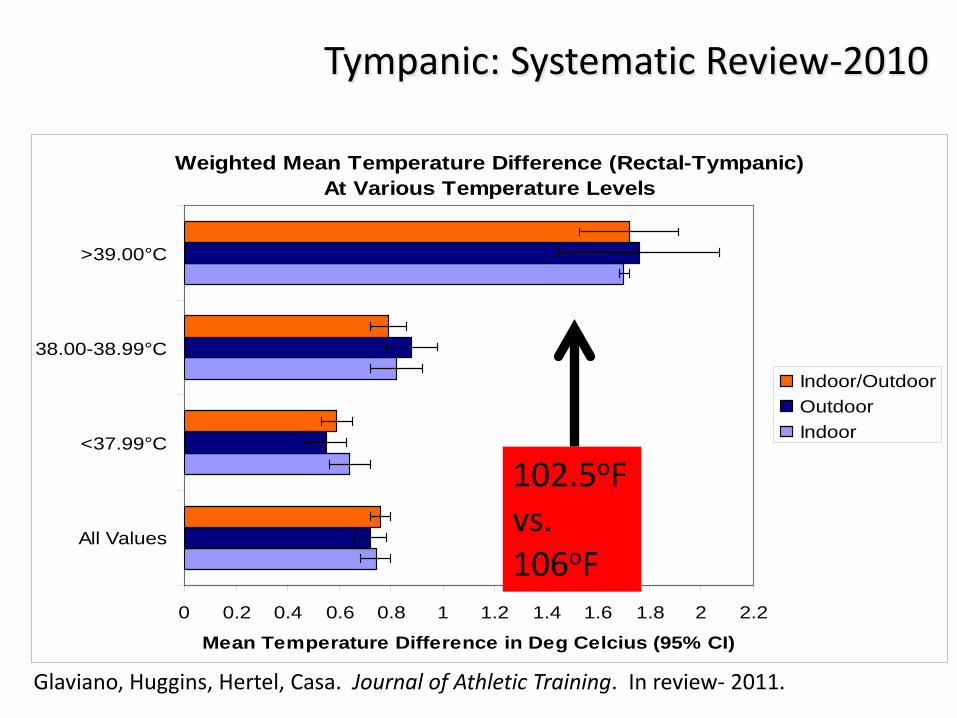
Tympanic: Systematic Review-2010
Weighted Mean Temperature Difference (Rectal-Tympanic) At Various Temperature Levels
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 2 2.2
All Values
<37.99°C
38.00-38.99°C
>39.00°C
Mean Temperature Difference in Deg Celcius (95% CI)
Indoor/OutdoorOutdoorIndoor
102.5oF vs. 106oF
Glaviano, Huggins, Hertel, Casa. Journal of Athletic Training. In review- 2011.
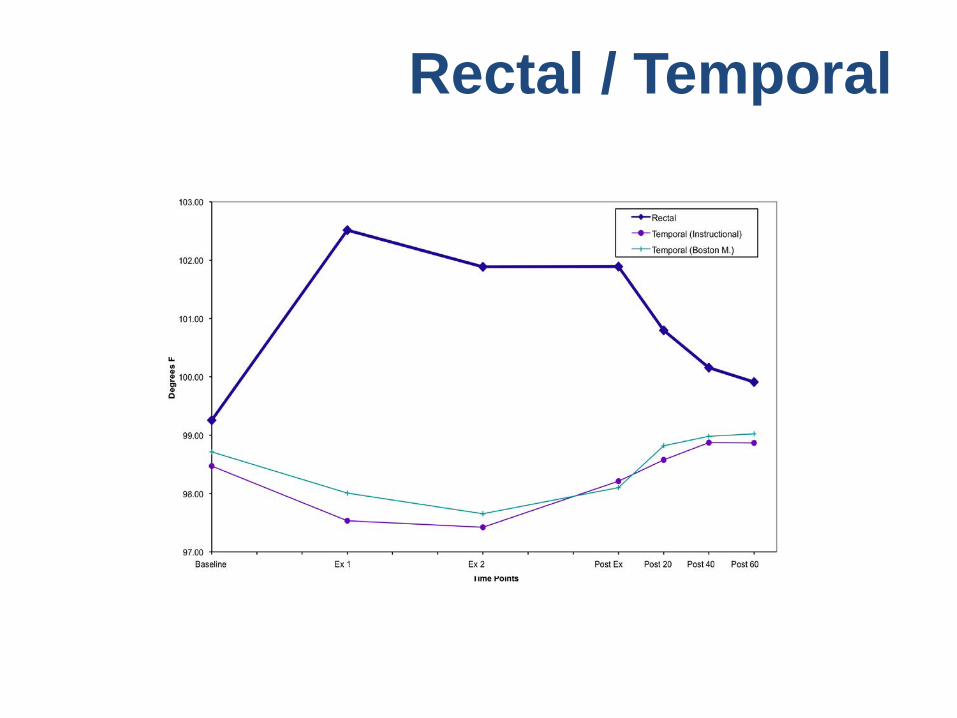
Rectal / Temporal
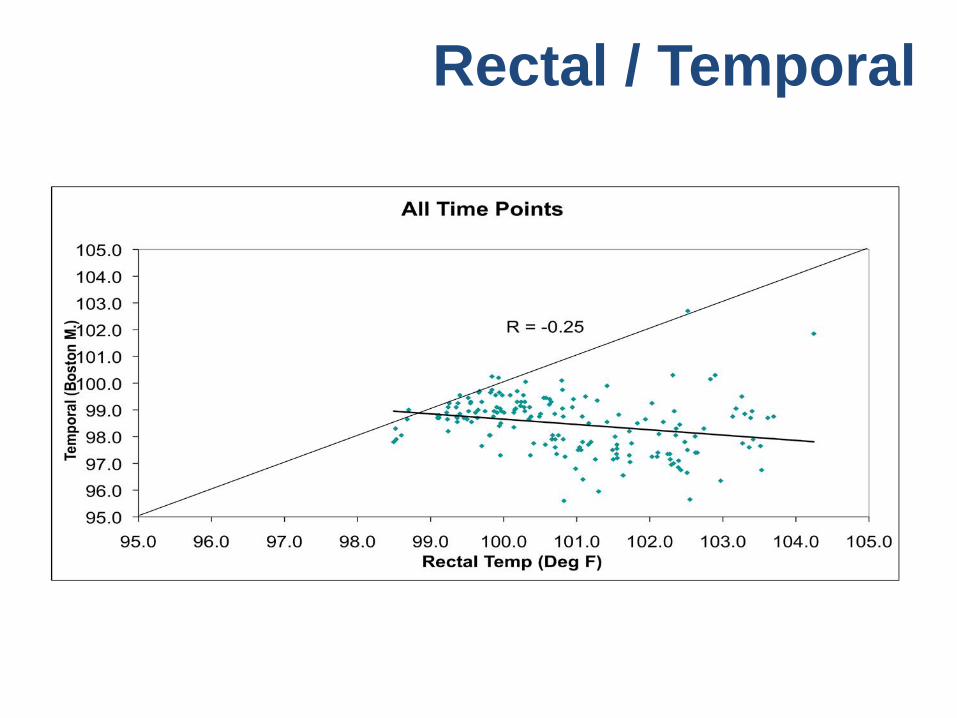
Rectal / Temporal
ITEM #7
The New NATA Educational Competencies
Fall 2012
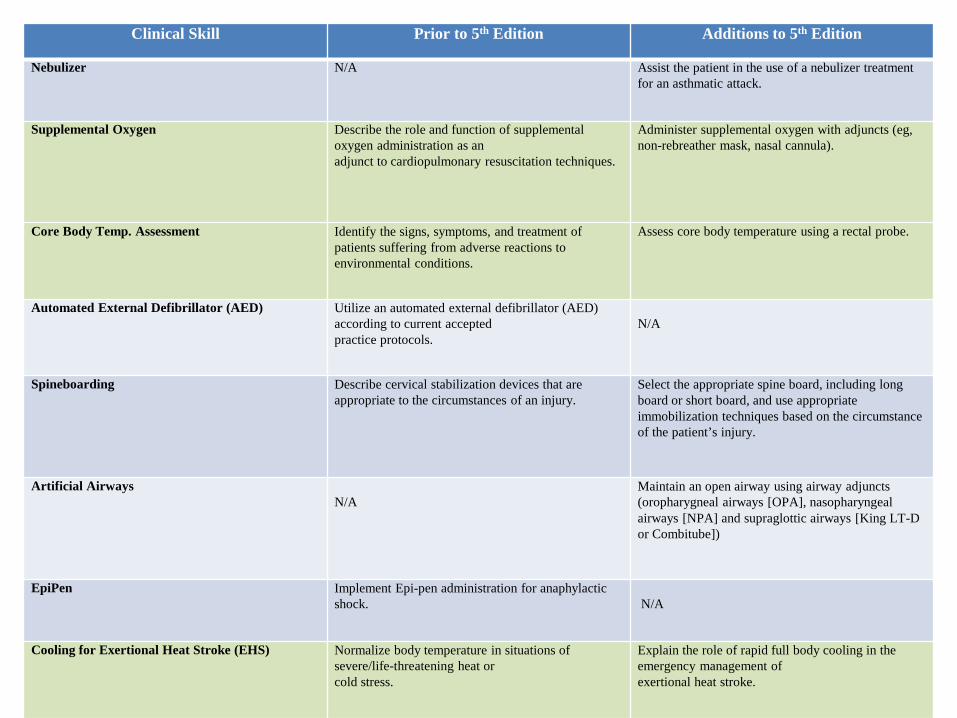
Clinical Skill Prior to 5th Edition Additions to 5th Edition
Nebulizer N/A Assist the patient in the use of a nebulizer treatment for an asthmatic attack.
Supplemental Oxygen Describe the role and function of supplemental oxygen administration as an adjunct to cardiopulmonary resuscitation techniques.
Administer supplemental oxygen with adjuncts (eg, non-rebreather mask, nasal cannula).
Core Body Temp. Assessment Identify the signs, symptoms, and treatment of patients suffering from adverse reactions to environmental conditions.
Assess core body temperature using a rectal probe.
Automated External Defibrillator (AED) Utilize an automated external defibrillator (AED) according to current accepted practice protocols.
N/A
Spineboarding Describe cervical stabilization devices that are appropriate to the circumstances of an injury.
Select the appropriate spine board, including long board or short board, and use appropriate immobilization techniques based on the circumstance of the patient’s injury.
Artificial Airways N/A
Maintain an open airway using airway adjuncts (oropharygneal airways [OPA], nasopharyngeal airways [NPA] and supraglottic airways [King LT-D or Combitube])
EpiPen Implement Epi-pen administration for anaphylactic shock.
N/A
Cooling for Exertional Heat Stroke (EHS) Normalize body temperature in situations of severe/life-threatening heat or cold stress.
Explain the role of rapid full body cooling in the emergency management of exertional heat stroke.
ITEM #6
Hold Companies/Organizations Accountable for
False/ Misleading Claims & Negligent Behavior
And The Best Yet----NATA 2007
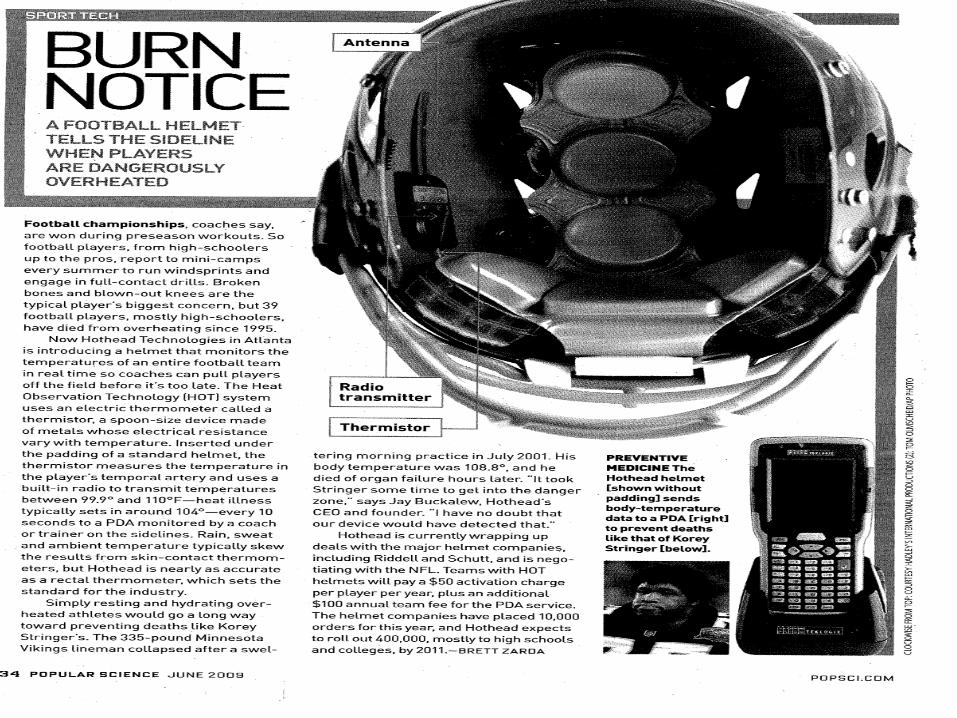
HotHead
“We are out evangelize athletic trainers to this product”
“We are first getting the word out about the product, and then we plan on conducting research
(to see if it works)” Are you serious or am I hallucinating?
Website- A) 167 heat related deaths in football since 2000!!!!!!!
B) The patent pending technology that reduces the risk of heat-related injury or death by monitoring a players temperature.
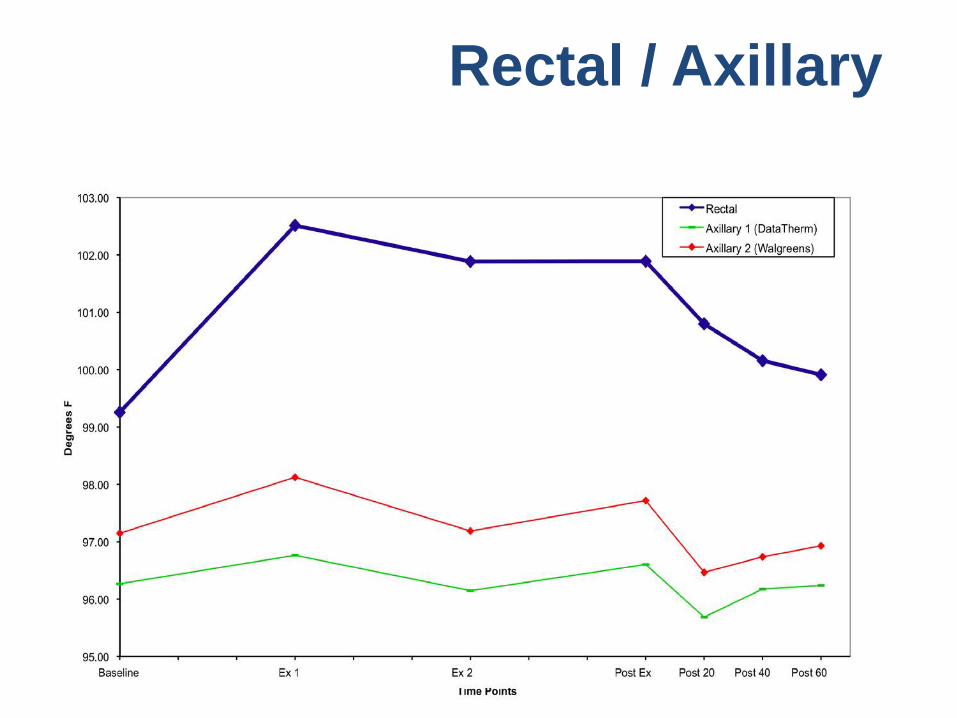
Rectal / Axillary
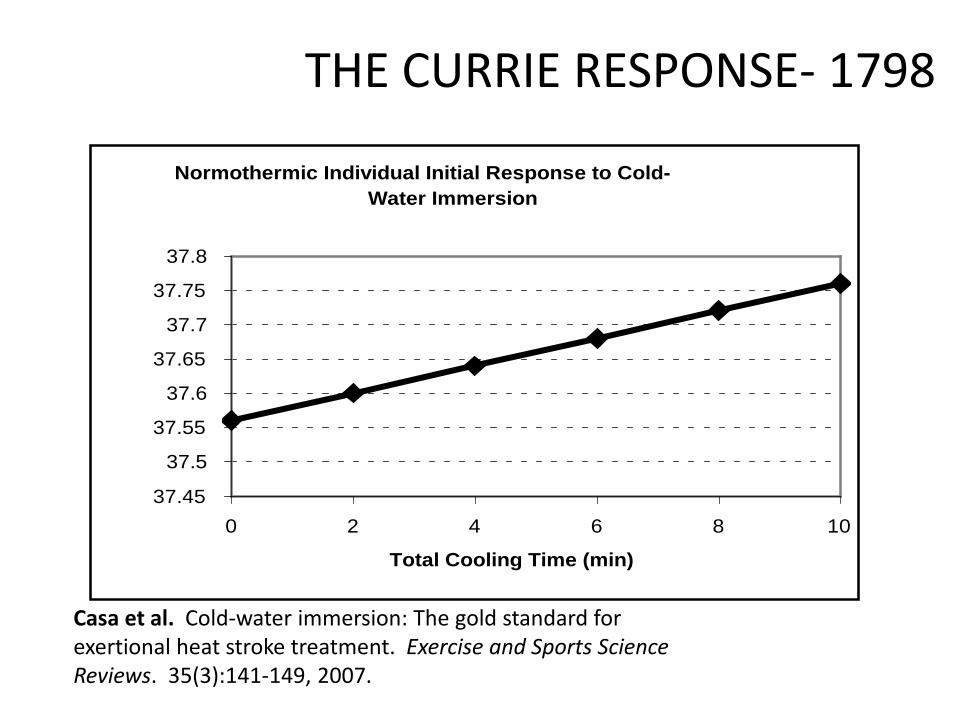
Normothermic Individual Initial Response to Cold-Water Immersion
37.45
37.5
37.55
37.6
37.65
37.7
37.75
37.8
0 2 4 6 8 10
Total Cooling Time (min)
THE CURRIE RESPONSE- 1798
Casa et al. Cold-water immersion: The gold standard for exertional heat stroke treatment. Exercise and Sports Science Reviews. 35(3):141-149, 2007.
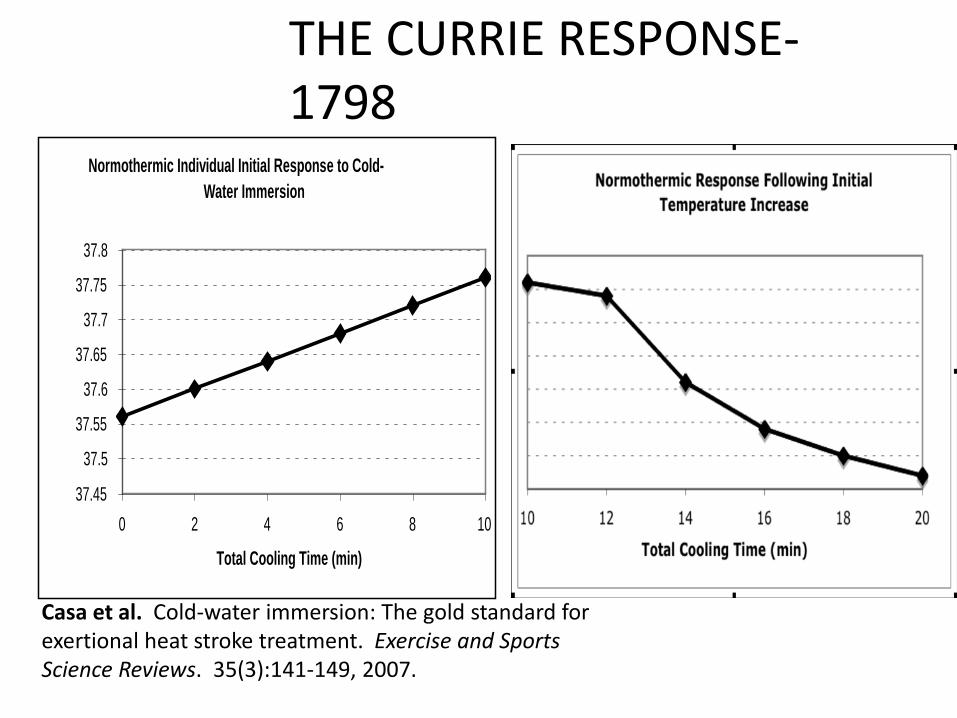
Normothermic Individual Initial Response to Cold-Water Immersion
37.45
37.5
37.55
37.6
37.65
37.7
37.75
37.8
0 2 4 6 8 10
Total Cooling Time (min)
THE CURRIE RESPONSE- 1798
Casa et al. Cold-water immersion: The gold standard for exertional heat stroke treatment. Exercise and Sports Science Reviews. 35(3):141-149, 2007.
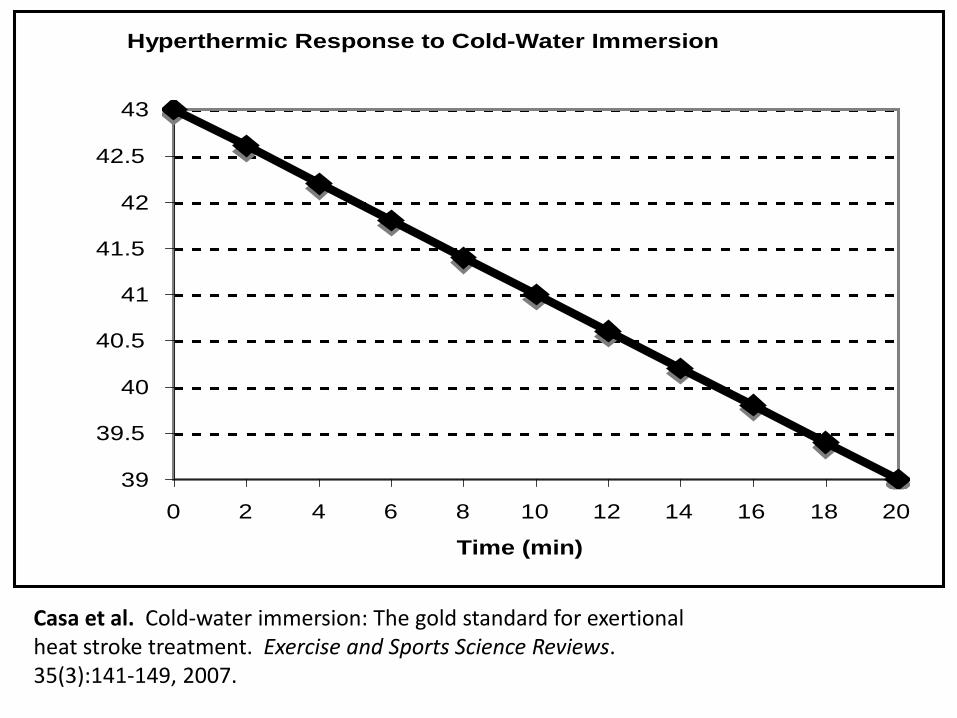
Hyperthermic Response to Cold-Water Immersion
39
39.5
40
40.5
41
41.5
42
42.5
43
0 2 4 6 8 10 12 14 16 18 20
Time (min)
Casa et al. Cold-water immersion: The gold standard for exertional heat stroke treatment. Exercise and Sports Science Reviews. 35(3):141-149, 2007.
ITEM #5
Cool First-Transport Second (the exertional heat stroke survival
mantra)
From The Inter-Association Task-Force on Exertional Heat Illnesses Consensus Statement,
2003
• “Provided that adequate emergency medical care is available on-site (i.e. ATC, EMT, or physician), it is recommended to cool first via cold water immersion, then transport second”
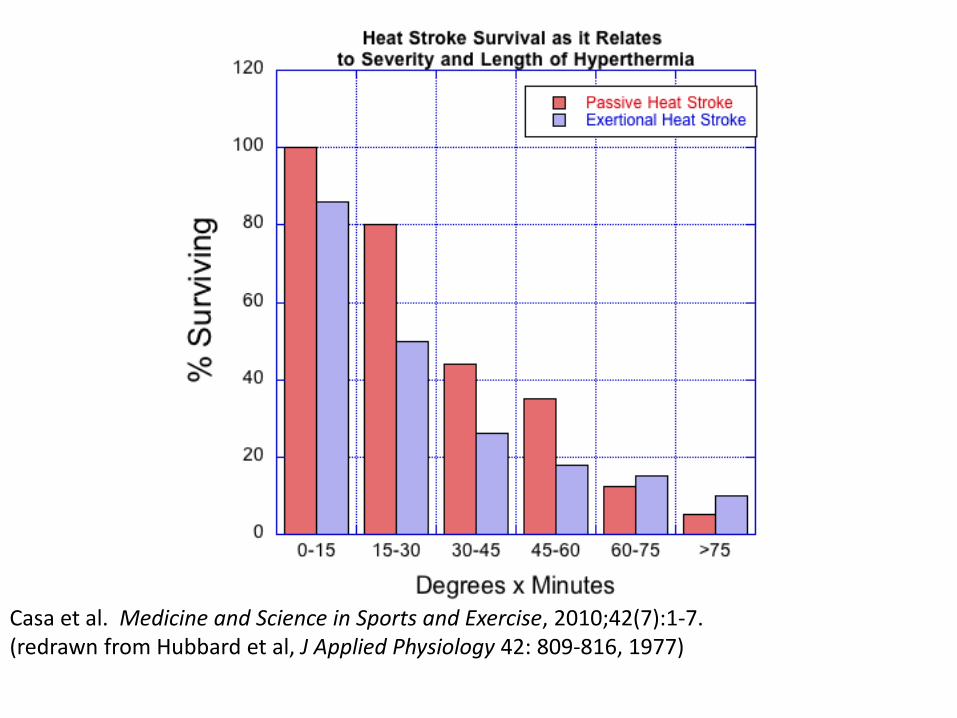
Casa et al. Medicine and Science in Sports and Exercise, 2010;42(7):1-7. (redrawn from Hubbard et al, J Applied Physiology 42: 809-816, 1977)
ITEM #4
Utilize cold/Ice Water When Cooling An
Exertional Heat Stroke Victim
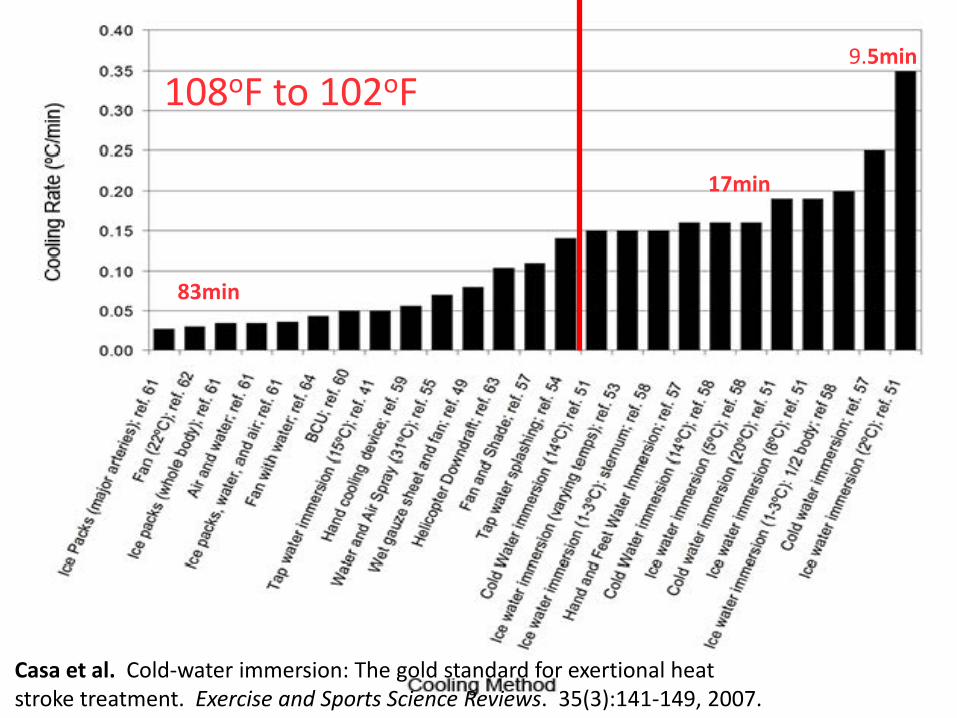
9.5min
17min
83min
108oF to 102oF
Casa et al. Cold-water immersion: The gold standard for exertional heat stroke treatment. Exercise and Sports Science Reviews. 35(3):141-149, 2007.

Core temperature diminution during three methods of post-hyperthermic cooling
40
40.5
41
41.5
42
42.5
43
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96100
Time in minutes
Core
tem
pera
ture
dec
reas
e du
ring
cool
ing
(deg
rees
Cel
sius
) Cooling rate 0.03
Cooling rate 0.10
Cooling rate 0.20
Casa et al. Cold-water immersion: The gold standard for exertional heat stroke treatment. Exercise and Sports Science Reviews. 35(3):141-149, 2007.
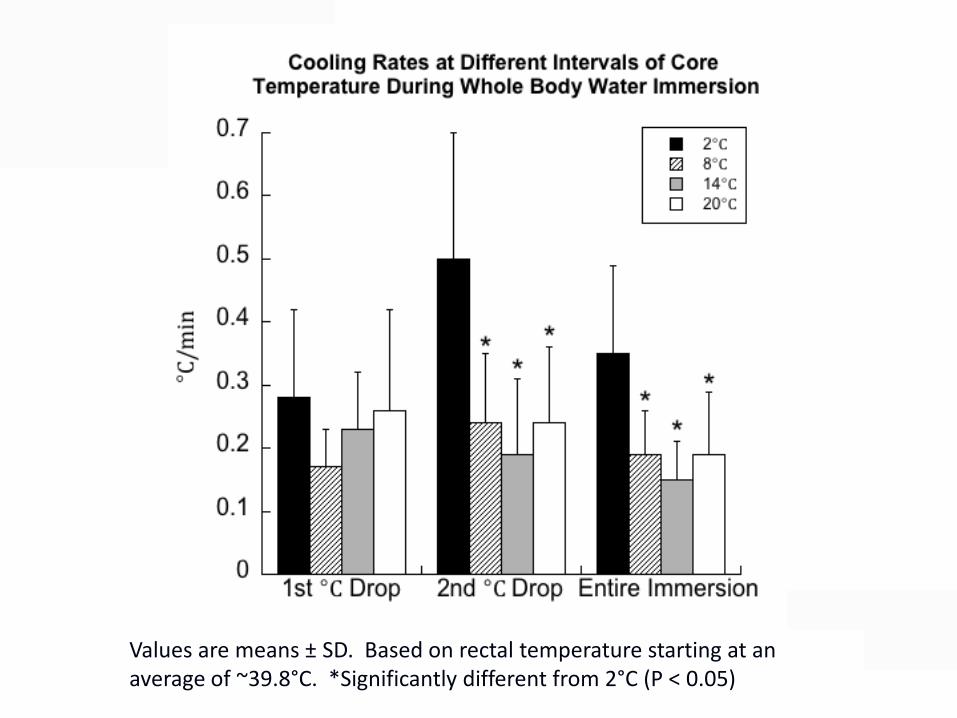
Values are means ± SD. Based on rectal temperature starting at an average of ~39.8°C. *Significantly different from 2°C (P < 0.05)

ITEM #3
An Athletic Trainer at Every High School
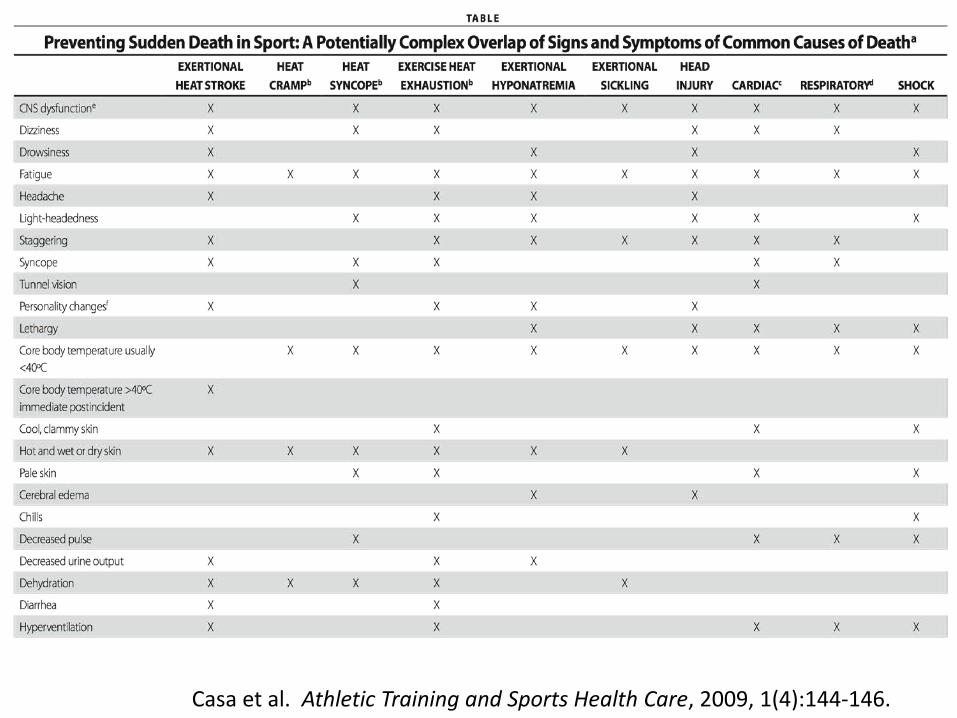
Casa et al. Athletic Training and Sports Health Care, 2009, 1(4):144-146.
ITEM #1
DEVELOP GREAT POLICIES (EAP’s) & FOLLOW THEM IN TIMES OF
CRISIS (The Checklist Manifesto)
All Medical Staff Can Intervene on Behalf of Patient’s Best Interests