hematuria. epidemiology hematuria –defn- presence of excessive numbers of red blood cells (rbcs)...
TRANSCRIPT
Hematuria
Epidemiology
• Hematuria– Defn- presence of excessive numbers of red
blood cells (RBCs) in the urine• macroscopic-- gross
• microscopic-- visible with the aid of a microscope only
Epidemiology
• Hematuria– Normal patients can excrete 104 to 105 RBC in a
12-hr period– Corresponds to several RBCs in the sediment of
a randomly collected, centrifuged specimen under high power magnification
• therefore hematuria is >4 RBC/hpf of urine sediment
Epidemiology
• Hematuria– Children
• prevalence of microheme approximately 4%
• majority have normal UAs on f/u and do not develop urinary tract pathology
• therefore isolated microheme in children does not require extensive evaluation
Epidemiology
• Hematuria– recall
• dipsticks detect globin pigments-- not RBCs, therefore a positive dipstick must be validated by microscopy
– r/o myoglobinuria (rhabdomyolysis) and severe hemolysis

HematuriaGlomerulus
Tubule
ureter
prostate
bladder
urethra
penisvaginarectum
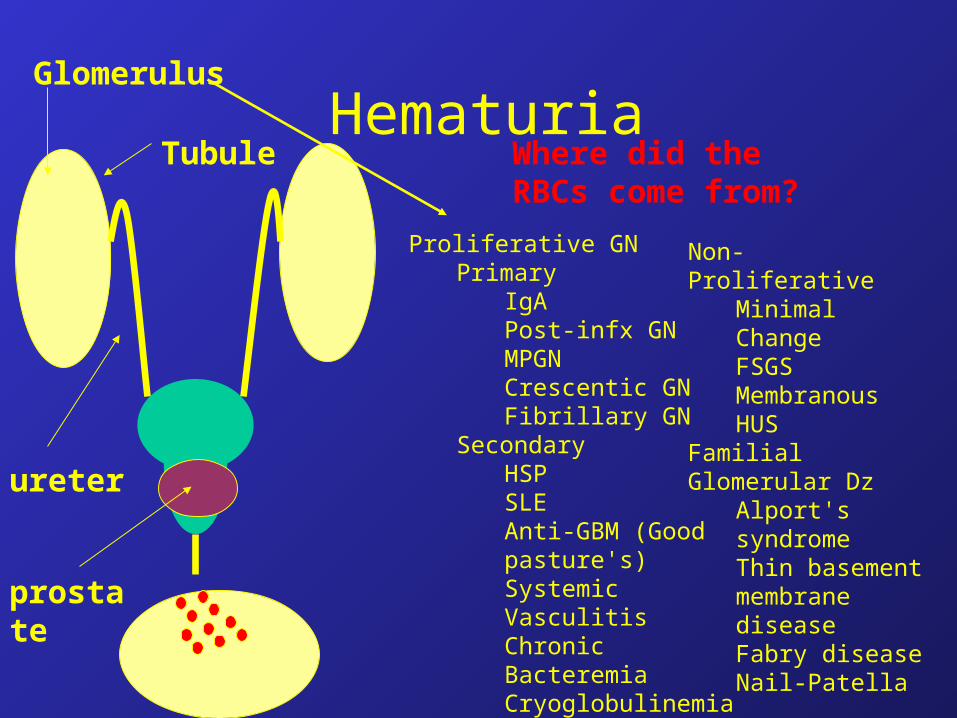
Where did the RBCs come from?
HematuriaGlomerulus
Tubule
ureter
prostate
Where did the RBCs come from?
Proliferative GNPrimary
IgAPost-infx GNMPGNCrescentic GNFibrillary GN
SecondaryHSPSLEAnti-GBM (Good pasture's)Systemic VasculitisChronic BacteremiaCryoglobulinemiaHepatitis B/C
Non-Proliferative Minimal ChangeFSGSMembranousHUS
Familial Glomerular DzAlport's syndromeThin basement membrane diseaseFabry diseaseNail-Patella
Hematuria - Where did the RBCs come
from?Glomerulus
Tubule
ureter
prostate
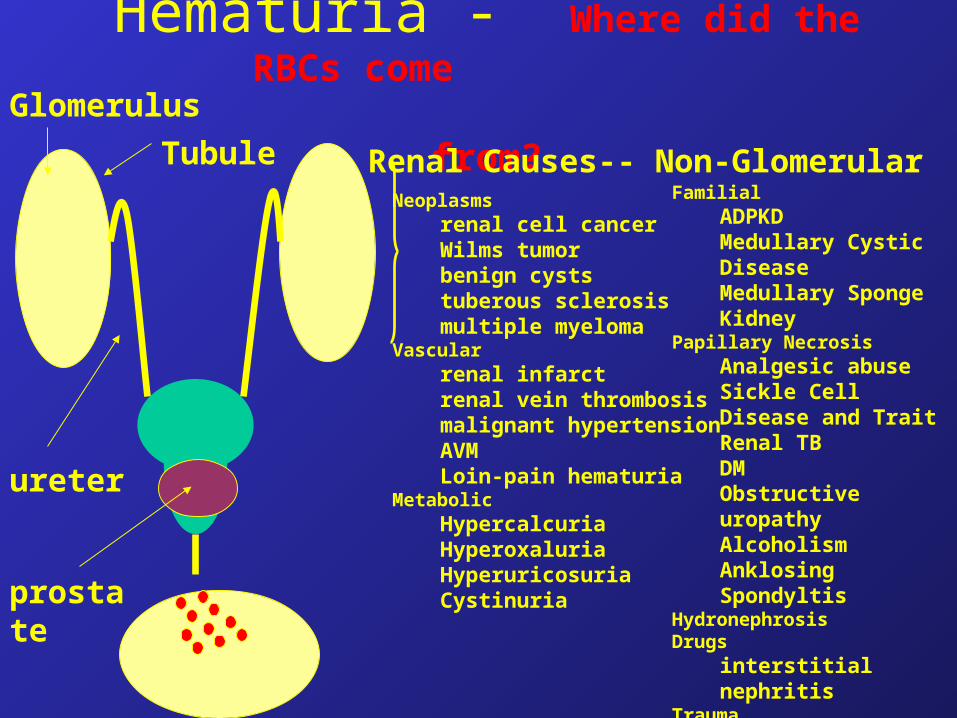
Renal Causes-- Non-GlomerularNeoplasms
renal cell cancerWilms tumorbenign cyststuberous sclerosismultiple myeloma
Vascularrenal infarctrenal vein thrombosismalignant hypertensionAVMLoin-pain hematuria
MetabolicHypercalcuriaHyperoxaluriaHyperuricosuriaCystinuria
FamilialADPKDMedullary Cystic DiseaseMedullary Sponge Kidney
Papillary NecrosisAnalgesic abuseSickle Cell Disease and TraitRenal TBDMObstructive uropathyAlcoholismAnklosing Spondyltis
HydronephrosisDrugs
interstitial nephritisTrauma
Renal Contusion or laceration Exercise hematuria

Hematuria-- non renalGlomerulus
Tubule
ureter
prostate
bladder
urethra
penisvaginarectum
Calculiureter, bladder, prostate
NeoplasmsTCCprostate Ca/BPHsquamous cell
Infectionscystitis, prostatitis, urethritisTBSchistosomiasis
Drugscyclophosphamideanticoagulants
TraumaContusion/lacerationexercise induced hematuriaforeign bodydecompression of severely distended bladder
Genital or anal bleeding

Hematuria
• History– frequency/dysuria - UTI– hesitancy, weak stream, and dribbling - bladder
obstruction 2nd stone/tumor/ prostate– colicky flank pain that radiates to groin-- stone or
renal papillary necrosis– arthralgia/arthritis/rash - systemic inflammatory
disorder-- HSP, SLE, or other systemic vasculitis– s/p bloody diarrhea -- think HUS

Hematuria
• History– 1-2 weeks s/p pharyngitis/skin infection - post-
strep GN– family h/o deafness/hematuria/renal failure -
Alport's syndrome (hereditary nephritis)– transient hematuria s/p exertion– foreign travel--Schistosoma haematobium
Hematuria
• Type of bleeding– Color
• brown or cola-colored-- usually kidney
• pink or red usually suggests extra-renal
– Clots• usually indicated a non-renal source
Hematuria
• Physical Exam– Vitals-- hypertension-- esp new c/w renal pathology
– HEENT-
– CV-
– Resp-
– Abd--
– Ext-- edema more c/w renal pathology
• arthritis-- SLE/inflammatory d/o
– GU-- vaginal/rectal source of blood. BPH?
– Skin-- rash
Hematuria
• UA– proteinuria accompanying hematuria is
glomerular disease until proven otherwise• don’t send to Urology to r/o stones/TCC
• Potential error-- HgB is a protein -- nl Hgb (12grams/dl), therefore hematuria (if hemolyzed) can easily cause measurable proteinuria
– Pyuria-- frequently seen with UTI/STDs
Hematuria
• Urine microscopy– Crystals– Casts-- presence also points toward renal
pathology– dysmorphic RBCs
• presence confirms glomerular disease, absence has no diagnostic implications
HematuriaGlomerular
• Labs– Chem 7– serum complement
• low-- MPGN, SLE, cryoglobulinemia– ASO and anti-Dnase B– HepBsAG, anti-HC– ANA– Other (depending upon clinical scenario)
• anti-gbm-- pulm hemorr or rpgn• anca- s/s of vasculitis• cryoglobulins• pt/ptt• sickle screen
HematuriaGlomerular
• Additional studies/info– r/o hereditary nephropathy
• Alport’s, Thin Basement Membrane Disease (AKA benign familial hematuria), and ADPKD
• screen all available family members with UA
– if Alport’s suspected• audiologic examination
– anterior lenticonus, yellowish perimacular flecks
HematuriaGlomerular
• Biopsy– considered on a case by case basis
• risks-- 1/2000 - 1/5000 risk of death, defining disease often will NOT result in a change in therapy
• avoid if s/p recent sore throat, acute nephritis, and low complements
• usually performed if associated with renal insufficiency, proteinuria, or low complement
HematuriaNonglomerular Hematuria
• If pyuria-– urine culture
– STD screen
• African-American– consider SICKLE CELL TRAIT OR DISEASE
• h/o cytoxan therapy– hemorrhagic cystitis
HematuriaNon-glomerular Hematuria
• If initial evaluation unremarkable:– renal US
– KUB
– and >40yo, consider urology referral• urine cytology
• cystoscopy
Initial Evaluation• Rule out obvious benign causes
– Infection• Irritative sx’s or WBCs on U/A Culture• Treat appropriately
– Men – 30 days of quinolone & consider GU evaluation
• Repeat U/A in 6 weeks
– Activity• Vigorous exercise, sex, virus, trauma, menses• Repeat U/A 48+ hours after cessation
– External lesions• Examine penis or perineum & vagina

Initial Evaluation• Rule out nephrologic hematuria
– Proteinuria• 1+ on dipstick, >500-1000 mg on 24 hr urine
– RBC Casts• Pathognomonic for glomerular bleeding
– Dysmorphic RBCs• Variation in size & shape, irregular/distorted outline• Predominance suggest glomerular origin
– Renal insufficiency• New rise in creatinine
General Evaluation
• Imaging upper tracts
• Cytology
• Cystoscopy
• Modify based on risk factors

Imaging
• Looking for:– Renal tumors– Collecting system tumors– Stones– Other – UPJO, infection
Imaging
• IVP– Old standard
– Misses smaller stones and masses
• Ultrasound– Misses smaller solid masses
– Operator & body habitus dependent
– OK for screening low-risk pts
– Good in combo with retrograde pyelograms for contrast allergic pts.

Imaging• CT
– Current “Gold Standard”• Stones: 94-99% sensitive
• Masses: excellent down to ~1 cm
– “Hematuria protocol”• No oral or rectal contrast
• Non-contrast spiral CT full GU tract
• Renal dedicated IV contrast view(s)– Early (arterial) and nephrographic
• Excretory phase of full GU tract
Imaging• CT
– How to order• 3 separate orders
– CT, ABDOMEN WO/W CONTRAST 74170 8120
– CT, PELVIS WO/W CONTRAST 72194 8142
– CT, KIDNEYS W/WO CONTRAST 74170 8114
• “Hematuria protocol” in comments at NNMC– ?? CHCS order line coming soon ??
Imaging
• Retrograde pyelogram– Collecting system anatomy only– In conjunction with non-contrast CT or
ultrasound for contrast allergic patients– To confirm abnormality on initial imaging– Performed at the the time of clinic cystoscopy
• !! Best to have imaging results prior to cystoscopy
Cytology
• Examination of exfoliated cells in the urine– Looking for malignant cells
• Sensitivity for urothelial cancer– Excellent (90+%) for high-grade– Poor (40%) for low-grade
• “Reactive” cells often suggest a stone• “Atypical” or “Suspicious”
– Only 15% truly malignant
Cytology
• How to order– Lab
• CYTOLOGIC NON-GYN– # Container Specimen Description Frozen
– = ====== =================== ======
– 1 A Voided urine NO
– 2 B Voided urine NO
– 3 C Voided urine NO

Cytology
• Patient instructions– Well hydrated & active– Not first morning void– Fill container– Refrigerate immediately– Turn in <24 hrs
Cystoscopy
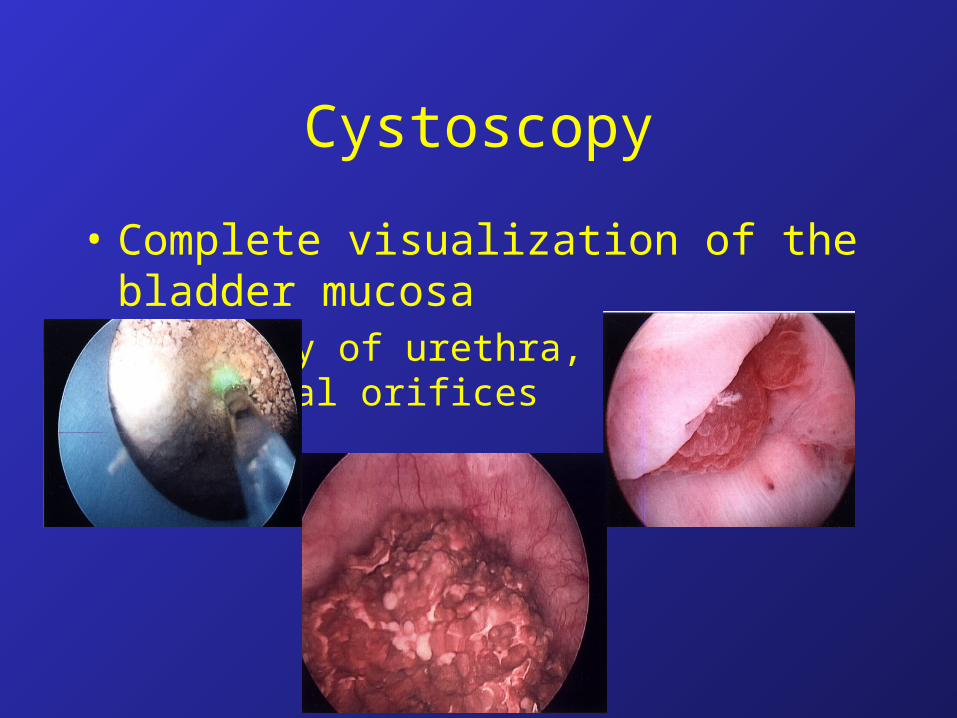
• Complete visualization of the bladder mucosa– Anatomy of urethra, prostate, ureteral orifices
Low-Risk Evaluation
• No risk factors
• CT– Stop after non-contrast phase if cause found– Ultrasound also reasonable
• Either cystoscopy or cytology
Benign Hematuria
• Benign/Isolated/Idiopathic Hematuria
• Negative full workup– ~2/3 have mild structural abnormality if
biopsied– At risk for mild nephropathy with low risk of
progression– <3% have missed malignancy
Follow-Up
• Follow-Up Protocol
• Annual– Urinalysis– Cytology x1– BP– Start in 6 months, continue for three years
• Modify based on risk
Follow-Up
• Re-evaluate if:– Significant increase in hematuria
• Ex. 5-10 now 25-50 RBC/HPF
– Abnormal urinary cytology– Irritative voiding symptoms develop in the
absence of infection
• Nephrology Evaluation– HTN, Proteinuria, RBC Casts, Dysmorphic
RBCs
Take Home Messages
• Dx: 3 RBC/HPF, 2/3 samples, properly collected
• R/o benign & nephrologic causes• Begin w/u with CT & cytology x3• Consult Urology
– Cystoscopy
• F/u yearly for 3 years with Hx, BP, U/A, cytology
HematuriaPearls
• Hematuria (<4rbc/phpf) is normal• Strenuous exercise can induce hematuria• Hematuria accompanied by proteinuria usually represents
a renal source• Only RBC casts or dysmorphic RBCs reliably localize
hematuria to the kidney• Microheme is the most common presentation of sickle
trait
