henrik grønborg, co-director rigshospitalet trauma center ... · development of acute cs in an...
TRANSCRIPT
Compartment syndromeDiagnostic difficulties & future developments
Henrik Grønborg, co-directorRigshospitalet Trauma Center
Copenhagen

• The past
• The present (difficulties)– Symptoms– Diagnosis
• The future ?

History
• Volkmann's ischaemic contracture
• Permanent flexion contracture• Claw-like deformity of the
hand and fingers
1830 - 1889

Development of acute CSIn an enclosed muscle (osteofascial) compartment:
Increase in volume of contentsand/or
Reduction in size of compartment
↓increased pressure within the compartment
↓compression of muscles, nerves & vessels
↓impaired blood flow
↓ischemia & necrosis

• Fracture (also open #’s)• Blunt trauma• Cast/dressing• Arterial injury• Post-ischemic
hyperperfusion• Burns/electrical injuries• Distorsion (ankle)• Tumour• Lithotomy position
• IM nailing (reaming)• Exertional states• Closure of fascial
defects• GSW / stabbings• IV & A-lines• Hemophil./coag.disorder• Intraosseous infusion• Snake bite
Numerous etiologies
……….and more

Symptoms
• Pain out of proportion• Pain on passive stretch• Paraesthesia• Paresis• Pulses present • Palpatory pain
• ACS is a surgical emergency !

20042008

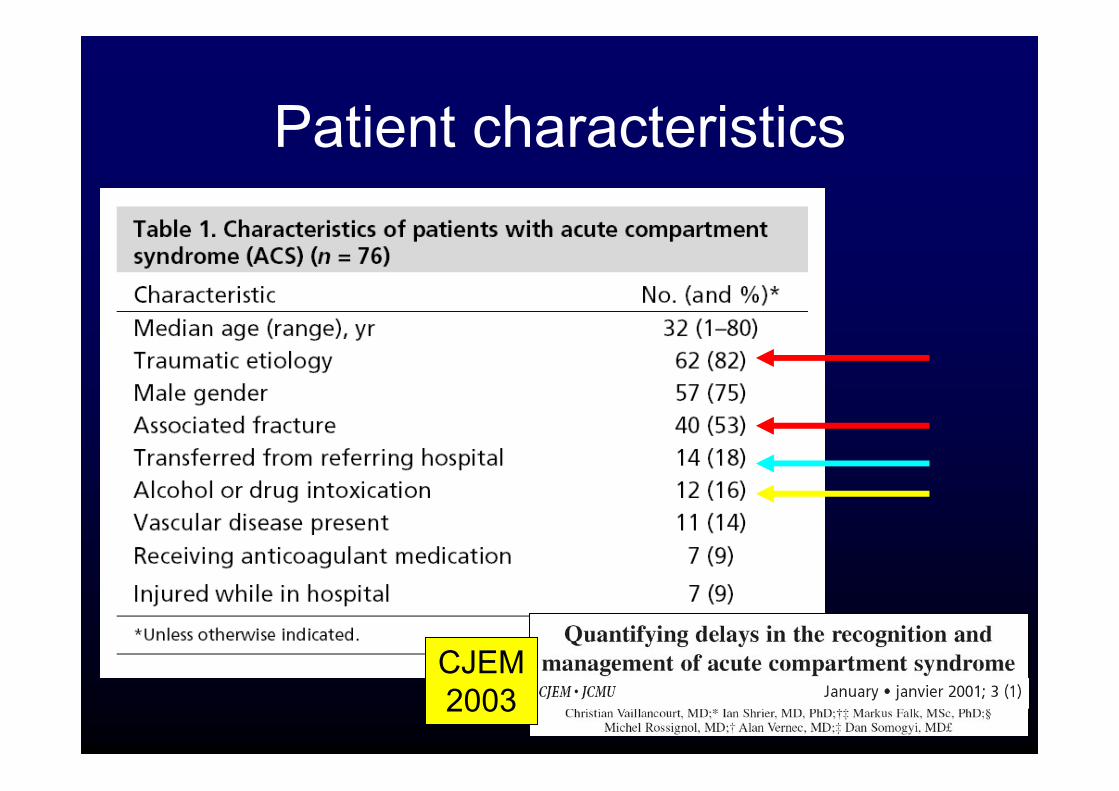
Patient characteristics
JBJS1996
Patient characteristics
CJEM 2003

• 17% of consultant anaesthetists• 9% of nonconsultant anaesthetistshad seen CS masked by regional anaesthesia !
Injury2006

Diagnostic delay
CJEM 2003

JOT2002
The clinical findings

• Bayes’ theorem– Estimating the probability of a diagnosis based
on a series of clinical findings
– The likelihood ratio that compartmentsyndrome exists in a patient with a tibial shaft #
• based on pain, paresthesia, PPS, paresis:
JOT2002
JOT2002
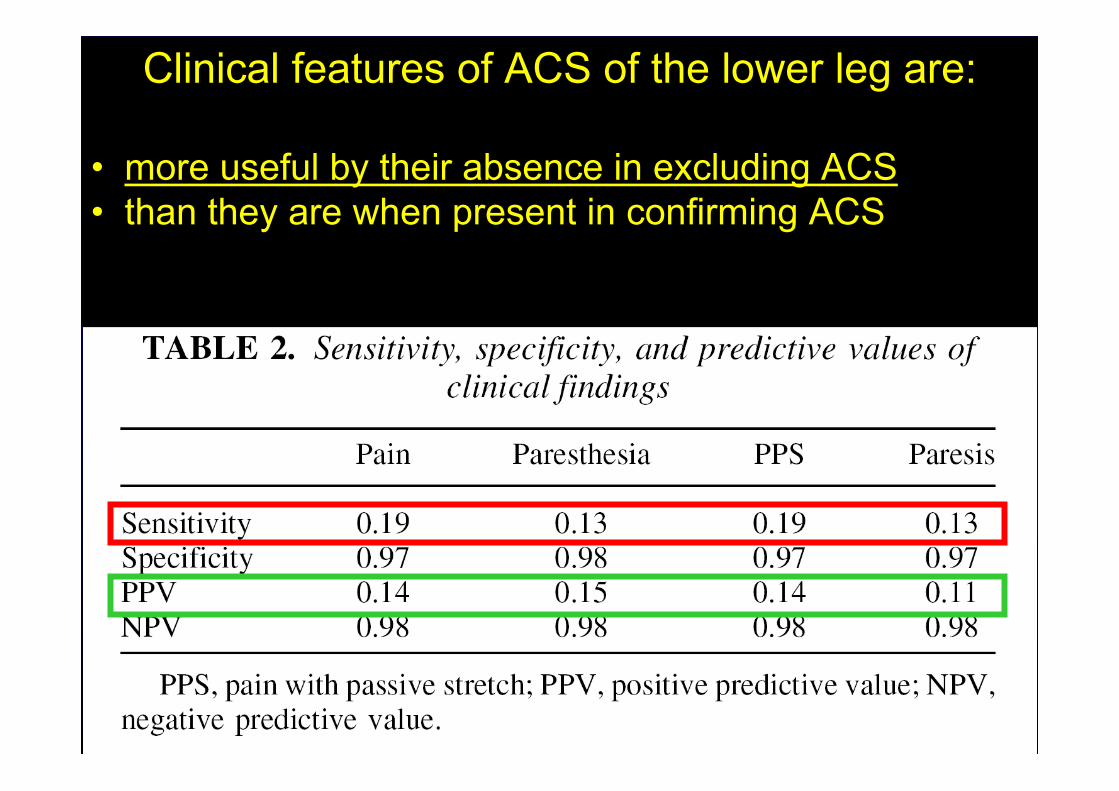
Clinical features of ACS of the lower leg are:
• more useful by their absence in excluding ACS• than they are when present in confirming ACS

JOT2002

Measurement ofintracompartmental
pressure

Pressure monitoring
Kodiag
Stryker
Whitesidetechnique

AJEM2003
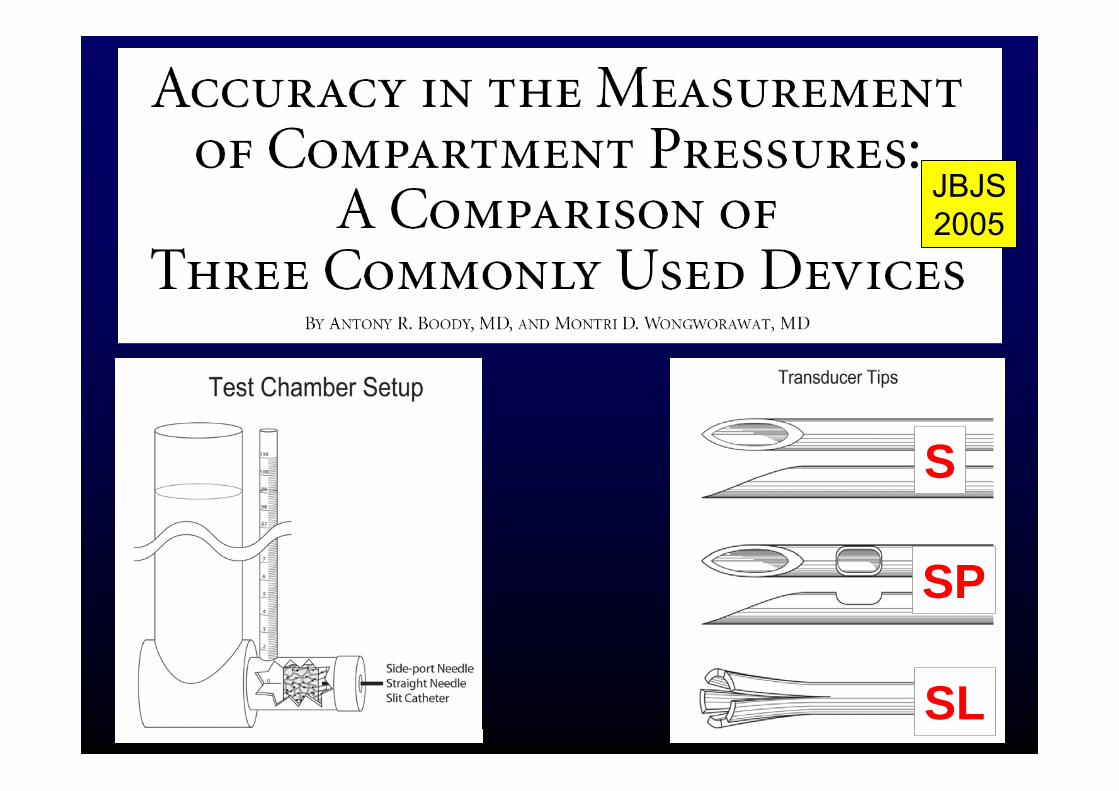
JBJS2005
SP
S
SL

• A-line manometer with:– side-port needle
or– slit catheter
• Available at ICU’s !
JBJS2005

Pressure measurementsshould be performed in:
1. both the anterior and the deepposterior compartments
2. at the level of the fracture+
3. at locations proximal and distalto the fracture zone
HeckmanJBJS-A, 1994

• A pressure threshold of 30 mmHg seemsto give an unacceptably high rate offasciotomies– ”Even if the absolute pressure limit had been
increased to 40 or 50 mmHg, we would have 19% or 14%, respectively”
Arch OrthopTrauma Surg
1998

– 116 patients with tibial #’s– Continuous monitoring of anterior tibial
compartment for 24 hrs– P=30 mmHg threshold for fasciotomy
• 3 patients (2.6%) fasc.• no missed cases
– If P=30mmHg• 50 patients (43%) fasc.
– If P=40mmHg• 27 patients (23%) fasc.
JBJS1996

95 patients with 97 tibial #’s• ICP > 30mmHg
or• PP = P = (DBP – ICP) <30 mmHg
– acceptable sensitivitybut
– poor specificity too many fasciotomies
• PP = P = (MAP – ICP) <30 mmHg, used in combinationwith clinical symptoms or a second measurement after 1hr– excellent specificity
but– low sensitivity too many missed CS’s
Injury2001

• ↑ fracture complexity => ↓ P• ↑ delay to diagnosis => ↓ P
• Open vs. closed # => ns diff. in P
• IM nail vs. Ex-Fix => ns diff. in P
JBJS1996

• CCPM is– invasive– requires hourly nursing attention– regular in-service training of nursing staff
• not cost effective
• CCPM is not indicated in alert patients who are adequately observed
JBJS1996

Management of acute compartmentsyndrome - how do we do it ?
Injury1998
ANZ J.Surg2007

• 100 questionaires to consultants at different centres
• 78 answers– 36/78 had equipment for pressure monitoring
• 12/36 used equipmet routinely• 24/36 used it selectively or not at all
Injury1998

Injury1998

• 264 valid responses– (29% of all eligible respondents).
• 78% of respondents regularly measuredcompartment pressure– 33% used an absolute P threshold– 28% used a P threshold– 39% took both into consideration
ANZ J.Surg2007

ANZ J.Surg2007

ANZ J.Surg2007

ANZ J.Surg2007

Immediate actions• Limb elevation =>↓ compartment pressure
BUT• BP ↓ in elevated limb• 53% ↓ in perfusion pressure
NO
Wiger & Styf, J Orthop Trauma. 1998
• Cut & spread plaster• Cut webril• Remove cast
YES

• Fasciotomy most efficacious when performed early• However, when performed late
– similar rates of limb salvage as compared to early fasc– but increased risk of infection
• Results support aggressive use of fasciotomyregardless of time of diagnosis
Surgery1997

• 5 patients• Average delay 56 hrs (35-96 hrs)• 9 fasciotomies in lower limbs
– 1 death of septicaemia and MOF– 4 required amputations
• If CP in a closed lower limb injury > 8 to 10 hours:– ICP recordings after an 8-hour period is not useful– Treatment of potential acute renal failure must be considered– Viable skin left intact; no exposure of necrotic muscle to infection– Late reconstructive procedures to correct muscle contractures
JOT1996

The future ?

JBJS 1999

Physiol Meas2004

J OrthopTrauma
2006

Identifying the patient at risk
• Unconsciousness• Intoxication• Concomitant nerve injury• Multiple injuries• Young children• Individual patients with equivocal
symptoms and signs • Epidural anaesthesia
”seek, and ye shall find”Matthew (ch. VII, v. 7-8)

Trauma 2007

Take home message• ACS is a surgical emergency• High level of suspicion (”seek, and ye shall find”)
• Classic clinical symptoms have:– low sensitivity & pos+ predictive value– high specificity & neg- predictive value
• ICP easily measured with A-line manometer• P=30 mmHg useful threshold for fasciotomy• Screening protocols for patients at risk• Non-invasive pressure monitoring is coming

This lecture is available at:
www.flims.dk