how do transplants fit in the current therapeutic schema?
DESCRIPTION
How do transplants fit in the current therapeutic schema?. Guenther Koehne, MD, PhD Adult Bone Marrow Transplant Service Division of Hematologic Oncology Department of Medicine Memorial Sloan-Kettering Cancer Center New York, New York. Autologous SCT. Who? When? How? Maintenance?. - PowerPoint PPT PresentationTRANSCRIPT

How do transplants fit in the current therapeutic schema?
Guenther Koehne, MD, PhDAdult Bone Marrow Transplant Service
Division of Hematologic OncologyDepartment of Medicine
Memorial Sloan-Kettering Cancer CenterNew York, New York

Autologous SCT
Who?When?How?
Maintenance?
Allogeneic SCT
Who?When?How?
Maintenance?

Multiple Myeloma Treatment Lines in Transplant-Eligible Patients
InductionConsolidationConditioning?
Frontline treatment
Maintenance
Maintenance
Rescue
Relapsed
Bz/DexBz/Dex/DoxBz/Thal/Dex
Len/DexRev/Len/Dex
CRd
SCT
ObservationThal
Thal/PredRev

Curr Opin Oncol, Sept 2012

Allogeneic Transplantation for Multiple Myeloma
Treatment with curative potential – Lack of myeloma cell contamination in graft– Graft vs. myeloma effect
Reserved for fit patients Conventional/Myeloablative studies: TRM >50% Non-myeloablative transplants – BMT CTN #0201
– No clear survival benefit – High rate of acute and chronic GVHD
GVHD, graft versus host disease; TRM, transplant-related mortality.

Allogeneic Vs. AutologousUS intergroup trial (S9321)
N = 813Induction Therapy
VAD
RANDOMIZE
n=261HD-CTX
collection
N=255HD-CTX
collection
n=213HDT
Mel/TBIautotransplant
n=211SDT
VBMCPautotransplant
n=39<55 years
HLA matched sibling
n= 36Mel/TBI
allotransplant
GVHD prophylaxis
x TRM:53%
HD-CTX, high-dose cyclophosphamide; HDT, high dose therapy; HLA, human leukocyte antigen; MEL, melphalan; SDT, standard dose therapy; TBI, total body irradiation; VAD, continuous infusion of vincristine and doxorubicin plus high-dose dexamethasone; VBMCP, vincristine, carmustine, melphalan, cyclophosphamide, and prednisone. Barlogie B, et al. J Clin Oncol. 2006; 24:929-936.

Summary of Recent Studies With Non-Myeloablative Conditioning for Multiple Myeloma
Study Conditioning Transplant (No. Pts)
PFS / OS TRM Acute GvHD Chronic GVHD
Bruno, et alN Engl J of Med 2007
TBI 200 cGy 80 36%
@ 3 y
80%
@ 3 y
10% 43%Grade II ‒IV
63%
Extensive – 32%
Rosiñol, et alBlood2008
Mel 140/FLU 25 Median not reached
Median not reached
16% 32%Grade II‒IV
66%
Vesole, et alBiol Blood Marrow Transplant2009
FC 31 58%
@ 3 y
78%
@ 3 y
8% 17%Grade III‒IV
57%
Extensive – 26%
Krishnan, et alLancet Oncol 2011
TBI 200 cGy SR: 189
HR: 37
43%
40%
@ 3 y
77%
59%
@ 3 y
11% 26%Grade II‒IV
54%
Björkstrand, et alJ Clin Oncol2011
TBI 200 cGy /FLU
108 35%
@ 5 y
65%
@ 5 y
12% 20%Grade II‒IV
54%
Extensive –23%
FC, fludarabine plus cyclophosphamide; FLU, fludarabine; HR, high risk; OS, overall survival; PFS, progression-free survival; SR, standard risk. Koehne G, Giralt S. Curr Opin Oncol. 2012;24:720-726.

Allogeneic SCT
Who?Risk stratification based on high-risk factors
When?Sooner than later
How & Where?TCD HSCT & MSKCC
Maintenance?Immunotherapeutic Approaches

Approaches to Allogeneic SCT for High-Risk Multiple Myeloma
Induction Consolidation/Conditioning
Maintenance
Relapse
# lines of treatmentVDT-PACE
2nd salvage auto SCT
Upfront
InductionAuto SCT
TCD HSCTImmunotherapy
DLIAntigen-specific CTLs
1.
2.

Cytogenetics and Disease High-risk cytogenetics: 25% of patients
– Deletion 17p: del(17p)• 10% of newly diagnosed patients
• Associated with aggressive disease and shorter overall survival
• No conclusive evidence that any currently available treatments are effective for patients with del17p
– Translocation of the immunoglobulin heavy chain (IgH) locus on chromosome 14
• t(4;14); t(14;16)
– Deletion 13q: del13q• Related to association with t(4;14) and del17p
– Hypodiploidy
High risk disease affects outcome and should therefore affect treatment
Current Study at MSKCC: TCD HSCT for Multiple Myeloma – IRB #10-051 Phase II study of TCD Allogeneic Transplantation for High-
Risk Multiple Myeloma– Principle Investigator: Guenther Koehne MD, PhD
Eligibility Criteria:– Relapsed multiple myeloma following ASCT High risk cytogenetics or relapse ≤ 15 months postASCT
At least PR to salvage therapy
Conditioning: Bu/Mel/Flu (+ ATG) TCD: CliniMacs device: CD34+ cells positively selected
ASCT, allogeneic hematopoietic stem cell transplantation; ATC, antithymocyte globulin; Bu: busulfan; FISH, fluorescent in situ hybridization; IRB, internal review board; MSKCC, Memorial Sloan-Kettering Cancer Center; TCD, T-cell depleted, VGPR, very good partial response.

Design of Study: TCD (CD34+ selection) HSCT for Multiple Myeloma
- DLI (5x105 CD3+/Kg) at earliest 5-6 months post SCT- DLI (5x105 CD3+/Kg) at earliest 8-9 months post SCT- DLI (1x106 CD3+/Kg) at earliest 12-13months post SCT
- DLI (1x105 CD3+/Kg) at earliest 5-6 months post SCT- DLI (5x105 CD3+/Kg) at earliest 1-3months post SCT, following the first infusion- DLI (1x106 CD3+/Kg) at earliest 3-4months post SCT, following the second infusion
Prophylactically in recipients of HLA-matched allografts
Preemptively in recipients of HLA-mismatched allografts
DLI, donor lymphocyte infusion.Courtesy of Koehne G, et al. MSKCC.
Busulfan:0.8 mg/kg x 10 dosesMelphalan:70 mg/m2 x 2 dosesFludarabine:25mg/m2 x 5 dATG: 2.5 mg/kg x 2 d
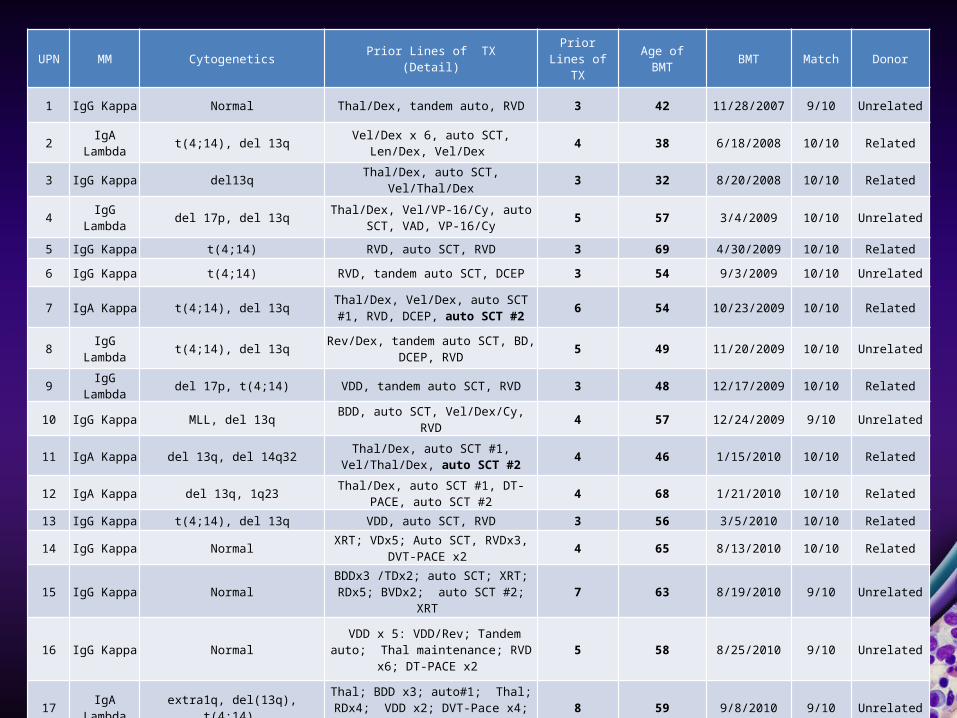
UPN MM Cytogenetics Prior Lines of TX (Detail) Prior Lines of TX Age of BMT BMT Match Donor
1 IgG Kappa Normal Thal/Dex, tandem auto, RVD 3 42 11/28/2007 9/10 Unrelated
2 IgA Lambda t(4;14), del 13q Vel/Dex x 6, auto SCT, Len/Dex, Vel/Dex 4 38 6/18/2008 10/10 Related
3 IgG Kappa del13q Thal/Dex, auto SCT, Vel/Thal/Dex 3 32 8/20/2008 10/10 Related
4 IgG Lambda del 17p, del 13q Thal/Dex, Vel/VP-16/Cy, auto SCT, VAD, VP-16/Cy 5 57 3/4/2009 10/10 Unrelated
5 IgG Kappa t(4;14) RVD, auto SCT, RVD 3 69 4/30/2009 10/10 Related
6 IgG Kappa t(4;14) RVD, tandem auto SCT, DCEP 3 54 9/3/2009 10/10 Unrelated
7 IgA Kappa t(4;14), del 13q Thal/Dex, Vel/Dex, auto SCT #1, RVD, DCEP, auto SCT #2 6 54 10/23/2009 10/10 Related
8 IgG Lambda t(4;14), del 13q Rev/Dex, tandem auto SCT, BD, DCEP, RVD 5 49 11/20/2009 10/10 Unrelated
9 IgG Lambda del 17p, t(4;14) VDD, tandem auto SCT, RVD 3 48 12/17/2009 10/10 Related
10 IgG Kappa MLL, del 13q BDD, auto SCT, Vel/Dex/Cy, RVD 4 57 12/24/2009 9/10 Unrelated
11 IgA Kappa del 13q, del 14q32 Thal/Dex, auto SCT #1, Vel/Thal/Dex, auto SCT #2 4 46 1/15/2010 10/10 Related
12 IgA Kappa del 13q, 1q23 Thal/Dex, auto SCT #1, DT-PACE, auto SCT #2 4 68 1/21/2010 10/10 Related
13 IgG Kappa t(4;14), del 13q VDD, auto SCT, RVD 3 56 3/5/2010 10/10 Related
14 IgG Kappa Normal XRT; VDx5; Auto SCT, RVDx3, DVT-PACE x2 4 65 8/13/2010 10/10 Related
15 IgG Kappa Normal BDDx3 /TDx2; auto SCT; XRT; RDx5; BVDx2; auto SCT #2; XRT 7 63 8/19/2010 9/10 Unrelated
16 IgG Kappa Normal VDD x 5: VDD/Rev; Tandem auto; Thal maintenance; RVD x6; DT-PACE x2 5 58 8/25/2010 9/10 Unrelated
17 IgA Lambda extra1q, del(13q), t(4:14) Thal; BDD x3; auto#1; Thal; RDx4; VDD x2; DVT-Pace x4; auto #2 8 59 9/8/2010 9/10 Unrelated

UPN MM Cytogenetics Prior Lines of TX (Detail) Prior Lines of TX Age of BMT BMT Match Donor
18 IgG Kappa del(13q), der(1) Thal/Dex x5, tandem auto, Thal/Dex, XRT, Vel/Dox; RVD; RD; DCEP x5 8 61 11/10/2010 9/10 Unrelated
19 IgG Lambda Normal Cy/Dex x2; VD x2; Auto #1; VD; RD/Mel; Auto #2 6 57 12/2/2010 10/10 Related
20 IgG Kappa Normal Thal/Dex x4; RVD x5, Auto #1; RVD 4 54 12/10/2010 10/10 Unrelated
21 IgG Kappa p53, tri 17, 5p, 11, 15, BiRD x5; Auto SCT #1; RVD; maintenance Rev; VD-Cy x5; VDT-PACE x2; Auto #2 6 37 3/2/2011 10/10 Unrelated
22 IgG Kappa NormalBDDx3 /TDx2, Auto #1; maintenance Rev; Auto #2; maintenance Rev; VDT-PACE x2;
RVD-Cyx3 5 49 4/14/2011 10/10 Unrelated
23 Nonsecretory del(20q), del(13q), del(17p), p53 BDDx4; BDx5 Auto#1; VD; RD; Auto #2; BiRD 7 63 4/20/2011 10/10 Related
24 IgG Kappa MLL, del(13q), IgH, p53 BBD x2; Thal/Dex x2; tandem auto SCT; maintenance thal; XRT;RVD x 10 5 45 5/26/2011 10/10 Unrelated
25 IgG Lambdaextra 1q23 and 19p13, IgH, MLL, del
p53, extra of 1q, 1p, del(13) and del(17p), extra 4,11, and 14
Thal/Dex x 3 ; VD x3; RD, VD-PACEx1; VD-PACE x3;Auto #1; Bortez maintenance 6 60 6/3/2011 10/10 Unrelated
26 IgG Lambda extra 1q25, mono 13, Der3, I5p, I5q, trans IgH locus, del(17p)
Thal/Dex x1; RD x4; Auto #1 XRT/Dex followed by RD x6; Auto #2; maintenance
Rev; VD-Cy x5 7 62 8/31/2011 10/10 Unrelated
27 IgG LambdaDup(1q), del(4p), 1q25, tri(9), mono (13), tri 15, mono 16, loss p53 gene,
MLL
RVD x 4, Auto #1 ; RVD; DCEPx3 with RVD between cycles; VD-Bendamustine; VDT-
PACE x1; Auto #2 8 56 9/21/2011 9/10 Unrelated
28 IgG Kappadel(1)(p13p22), +3,+5+9,+11,del(13),
(q12q14), del(14)(q24), der(16), t(11;16), (p13.1;q24
RVD x9; XRT; Auto #1; VD x 4; VDT-PACE x3; Auto #2 6 61 10/21/2011 9/10 Unrelated
29 Lambda LC Normal Thal/Dex,auto SCT, Len main., RevDex, RVDx1 -->BDx6 4 56 12/29/2011 10/10 Unrelated
30 IgG Lambda NormalRVDx6, Cytoxan --> Mel + auto SCT #1, PomCLARx5, Carfilzomib x3, VDT-PACE,
salvage MEL + auto SCT #27 50 2/1/2012 10/10 Related
31 IgG Kappa extra 1q25, trisomy 5,9,15; del12p1q RXT, BDx2, BDDx2, CTX; MEL + auto SCT, main. Len, CyBorDx4, VDT-PACE x3 5 59 4/20/2012 9/10 Unrelated
32 Nonsecretory mono 13, t(11;14)Thal/Dex x3, Bortez + Thal/Dex x2,, tandem
auto SCT, RevDex,lorvotuzumab/mertansine x 9, BD
x44 52 8/1/2012 10/10 Unrelated
33 Kappa LC Normal RVD x 4, auto SCT, Bortez/Rev main., Cytoxan/Velcade x2 3 48 9/5/2012 10/10 Unrelated
34 IgG Lambda del13q, del20q, extra 1q25, del 4,12,16
RVD x4, auto SCT #1, CyBorD x4, Bortez/Mel, Auto SCT #2 5 44 12/28/2012 10/10 Unrelated

Acute GVHD (grade II – IV) at 12 months (N = 34)
Transplant-related Mortality (at 12 months) (N = 34)
Courtesy of Koehne G, et al. MSKCC.
0.09 (0.02-0.23)0.06 (0.01-0.17)
Chronic GVHD Graft failure or rejection
Courtesy of Koehne G, et al. MSKCC.
None observed
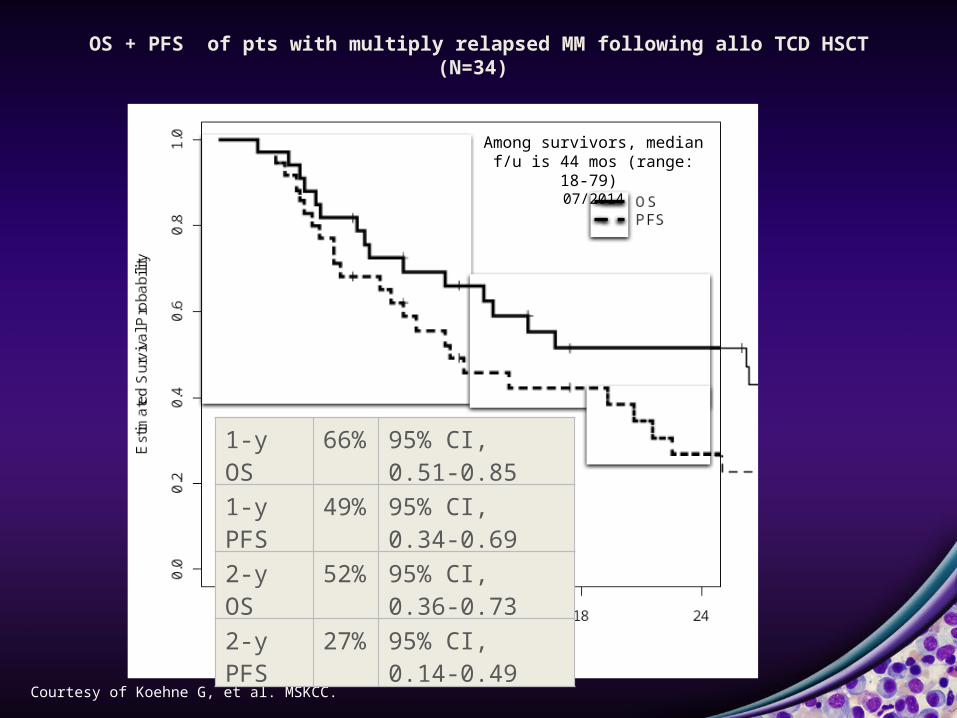
OS + PFS of pts with multiply relapsed MM following allo TCD HSCT(N=34)
Courtesy of Koehne G, et al. MSKCC.
Among survivors, median f/u is 44 mos (range: 18-79)
07/2014
1-y OS 66% 95% CI, 0.51-0.85
1-y PFS 49% 95% CI, 0.34-0.69
2-y OS 52% 95% CI, 0.36-0.73
2-y PFS 27% 95% CI, 0.14-0.49

OS (a) + PFS (b) of pts with multiply relapsed MM by previous lines of therapy prior to allo TCD HSCT
a. b.
p = 0.02 p = 0.05
Courtesy of Koehne G, et al. MSKCC.

OS (a) and PFS (b) of pts with multiply relapsed MM with < 6 previous lines of therapy prior to allo TCD HSCT based on donor selection
(related vs. unrelated)
Courtesy of Koehne G, et al. MSKCC.
b.
At 2yrs
Related:0.30 (0.12-0.77)Unrelated:0.36 (0.17-0.76)
At 2yrs
Related: 0.60 (0.36-0.99)Unrelated:
0.72 (0.51-0.99)
a.

OS (a) + PFS (b) of pts with multiply relapsed MM by previous lines of therapy prior to allo TCD HSCT
G. Koehne et al. MSKCC.

Post-salvage tx/ Pre-allo SCT
30d 100d
49 49 48
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
deathPDRelapse from CRSDPRVGPRCR
Clinical responses induced by Bu/Mel/Flu conditioning chemotherapy

Post-salvage tx/ Pre-allo SCT
30d 100d
49 49 48
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
deathPDRelapse from CRSDPRVGPRCR
Post-salvage tx/ Pre-allo SCT
30d 100d
34 34 33
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
deathPDRelapse from CRSDPRVGPRCR
Clinical responses induced by Bu/Mel/Flu conditioning chemotherapy

Clinical responses after initial DLIs (when receiving at least 2 doses) given for relapsed or residual MM
At DLI initiation 30d s/p DLI completion 100d s/p DLI completion 6m s/p DLI completion 1y s/p DLI completion14 13 12 10 10
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
deathPDSDPRVGPRRelaspe from CRCR

Single Patient Response
DLI 5x10e5/kg 06/09
July -1, 2
014
65 months in CR72 months post allo BMT
39-year-old male dx stage III IgA lambda, multiple myeloma (MM) high-risk cytogenetics (del 13; t(4;14).
Bortezomib /Dexamethasone (Dex) x 6, autoSCT 9/07 with relapse disease 12/07, Lenalidomide/Dex x1, Bort/Dex x2, alloHSCT from matched related donor (10/10) in 06/08, in
complete remission (CR) since 5/09.

DLI and Disease Course
55-year-old male dx stage III IgG lambda, MM high-risk cytogenetics (del 17p by FISH, del 13q by karyo).
Thalidomide/Dex x 4 months with PD + ARF, Bort–MI–CAGB with EF 35%, VP-16 + cyclophosphamide (CY) with PR, auto SCT 08/07 with relapse disease 08/08, VAD with PD, VP-16
+ CY x 3, allo HSCT from matched unrelated donor (10/10) in 03/09.
3830
4
3833
2
3835
9
3838
0
3838
8
3840
1
3844
4
3847
2
3851
4
3854
1
3855
5
3858
3
3860
4
3865
3
3869
5
3872
2
3874
3
3877
8
3883
4
3886
2
3890
4
3895
3
3898
1
3906
5
3914
9
3925
3
3931
0
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
M protein
M protein
M p
rote
in g
/dL
Allo BMT
DLI 5x10e5/kg
DLI 5x10e5/kg
DLI 1x10e6/kg
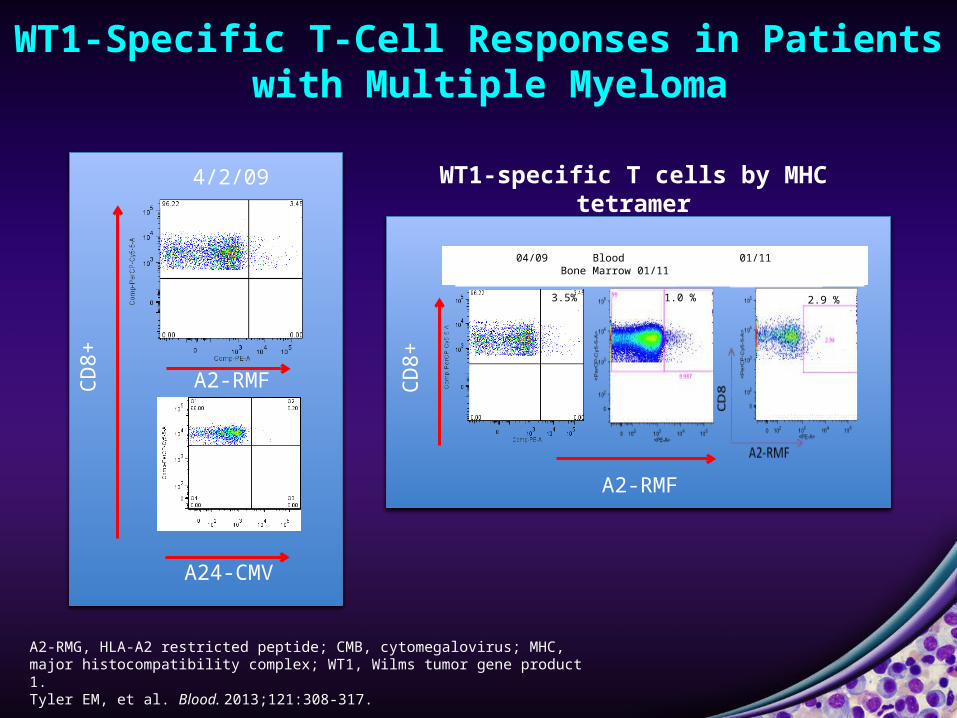
WT1-Specific T-Cell Responses in Patients with Multiple Myeloma
A2-RMG, HLA-A2 restricted peptide; CMB, cytomegalovirus; MHC, major histocompatibility complex; WT1, Wilms tumor gene product 1. Tyler EM, et al. Blood. 2013;121:308-317.
WT1-specific T cells by MHC tetramer
A24-CMV
A2-RMF
4/2/09
04/09 Blood 01/11 Bone Marrow 01/11
3.5% 1.0 % 2.9 %
A2-RMF
CD8+
CD8+

WT1—A Potential Target for Multiple Myeloma?
WT1: zinc finger transcription factor— Roles in cell proliferation, differentiation, apoptosis and organ development
Preferentially expressed during embryogenesis, but also at low levels in kidney, ovary, endometrium, testis and spleen of adults
Frequently overexpressed in a number of solid and hematologic malignancies— Expression correlates with disease progression in MDS, ALL, & CML— Molecular marker for risk assessment
Emergence of WT1-specific T cells correlates with better relapse-free survival post allogeneic transplant in leukemia1
MM cells are efficiently lysed by WT1-specific cytotoxic T lymphocytes2
WT1 expression in the BM of myeloma patients correlates with disease stage3
ALL, acute lymphocytic leukemia; CML, chronic myeloid leukemia; MDS, myelodysplastic syndrome.1. Rezvani K, et al. Blood. 2007;110:1924-1932; 2. Azuma T, et al. Clin Cancer Res. 2004;10:7402-7412; 3. Hatta Y, et al. J Exp Clin Cancer Res. 2005;24:595-599.

WT1-Specific T Cells and Disease Course

WT1-Specific T Cells and Disease Course
55-year-old male dx stage III IgG lambda, MM high risk cytogenetics (del 17p by FISH, del 13q by karyo).
Thal/Dex x 4 months with PD + ARF, Bort – MI – CAGB with EF 35%, VP-16 + CY with PR, auto SCT 08/07 with relapse disease 08/08, VAD with PD, VP-16 + CY x 3,
allo HSCT from MUD (10/10) in 03/09.
3830
438
332
3835
938
380
3838
838
401
3844
438
472
3851
438
541
3855
538
583
3860
438
653
3869
538
722
3874
338
778
3883
438
862
3890
438
953
3898
139
065
3914
939
253
3931
0
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0
5
10
15
20
25
30
35
40
M proteinAbs # CD8+ IFN-y+Abs # CD4+ IFN-y+
M p
rote
in g
/dL
Absolute num
ber WT1-specific T cells/ μL
IF neg
Allo BMT
DLI 5x10e5/kg
DLI 5x10e5/kg
DLI 1x10e6/kg
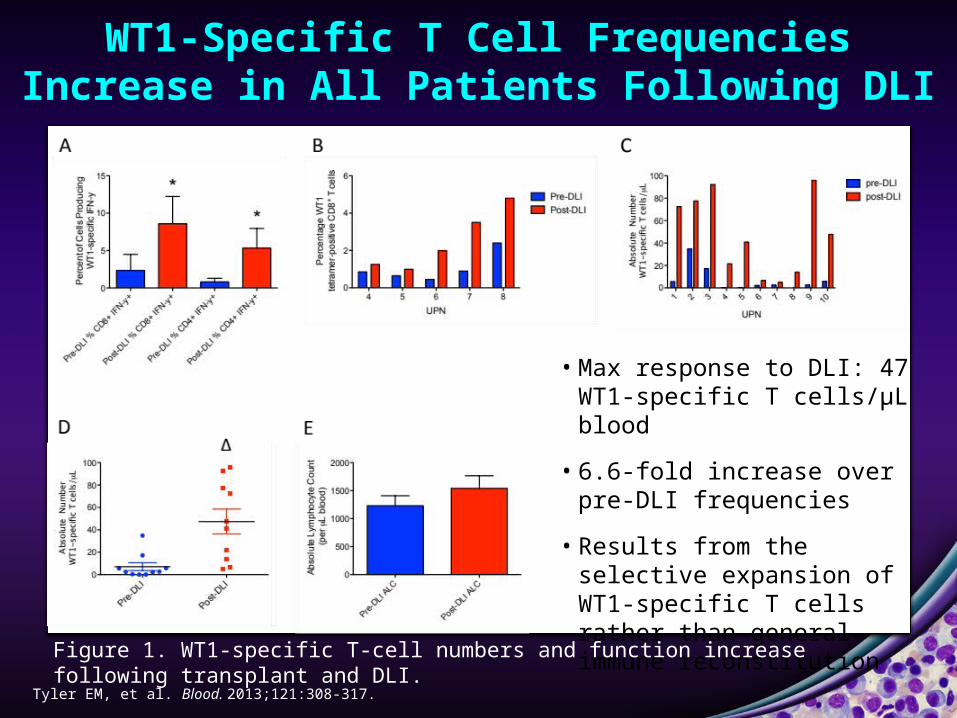
WT1-Specific T Cell Frequencies Increase in All Patients Following DLI
• Max response to DLI: 47 WT1-specific T cells/μL blood
• 6.6-fold increase over pre-DLI frequencies
• Results from the selective expansion of WT1-specific T cells rather than general immune reconstitution
Figure 1. WT1-specific T-cell numbers and function increase following transplant and DLI.
Tyler EM, et al. Blood. 2013;121:308-317.

IHC With WT1 mAb 6F-H2
CD138 (brown)/ WT1 (red) co-staining of BM biopsy
WT1 (red) co-staining of kidney biopsy CD138 (brown) staining of BM biopsy
BM, bone marrow; IHC, immunohistochemistry.Tyler EM, et al. Blood. 2013;121:308-317.

IHC Analyses of WT1 Expression in the BM of MM pts
++++ +++CD138 (MI15; DAB) = brown; WT1 (6F-H2, nFu) = red
++
Focal Negative Grading
Neg 0Focal < 5%+ < 25%++ 25 – 50%+++ 50 – 75%++++ > 75%
90% PC’s by biopsy
50 -60 % PC’s by
biopsy
45% PC’s by biopsy
5% PC’s by biopsy No PC’s by biopsy
DAB 3,3-diaminobenzidine; nFU, nFu1 antibody; PC, plasma cell. Tyler EM, et al. Blood. 2013;121:308-317.

Phase I Trial #IRB 12-175:TCD (CD34+ selection) Allo SCT Followed by WT1-Specific T-Cell
Infusions for Patients With Relapsed/Refractory Multiple Myeloma or Plasma Cell Leukemia
Busulfan:0.8 mg/kg x 10 dosesMelphalan:70 mg/m2 x 2 dosesFludarabine:25mg/m2 x 5 dATG: 2.5 mg/kg x 2 d
WT
WWT1-specific CTLs
WT1 CTLs - Dose levels 1, 3 and 5 x10e6/ kg; -3 doses/recipient of HLA-matched and HLA-mismatched allografts. - First dose at 6-10 weeks post transplant. - The second dose will be given 4-8 weeks following the first infusion and a third dose will
be administered 4-8 weeks following the second infusion. - The second and third dose will only be administered in the absence of grade III-IV toxicity
and grade II-IV acute GvHD following the preceding T-cell dose.
CTL, cytotoxic T lymphocytes.Courtesy of Koehne G, et al. MSKCC.

Plasma Cell Leukemia
Overall Survival (OS) in pPCL and sPCL, showing superior survival of pPCL vs sPCL from the time of leukemia diagnosis.
pPCL, primary plasma cell leukemia; sPCL, secondary plasma cell leukemia.Albarracin F, Fonseca R. Blood Rev. 2011;25:107-112.

Case―61-Year-Old AA Female With Secondary Plasma Cell LeukemiaUndergoing TCD HSCT Followed by WT1 CTLs
Residual Disease Post VDT-PACE, but HLA-Matched Brother
TCD HSCT02/13/12
WT1 #1 1x10e6/kg04/18/12
WT1 #2 1x10e6/kg05/16/12
WT1 #3 1x10e6/kg06/13/12
0
10
20
30
40
50
60
70
Donor PHA Blasts
Donor DC Donor DC Pulsed
K562
% C
ytot
oxic
ity
E:T
25:1
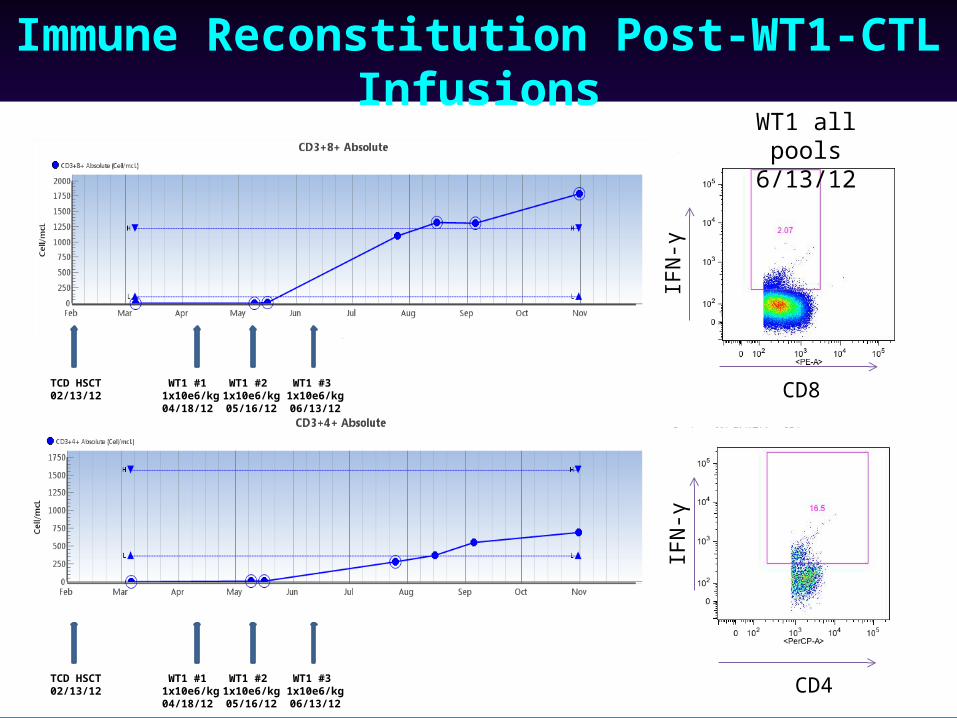
Immune Reconstitution Post-WT1-CTL Infusions
TCD HSCT02/13/12
WT1 #1 1x10e6/kg04/18/12
WT1 #2 1x10e6/kg05/16/12
WT1 #3 1x10e6/kg06/13/12
IFN
-γ
CD8
CD4IF
N-γ
TCD HSCT02/13/12
WT1 #1 1x10e6/kg04/18/12
WT1 #2 1x10e6/kg05/16/12
WT1 #3 1x10e6/kg06/13/12
WT1 all pools6/13/12

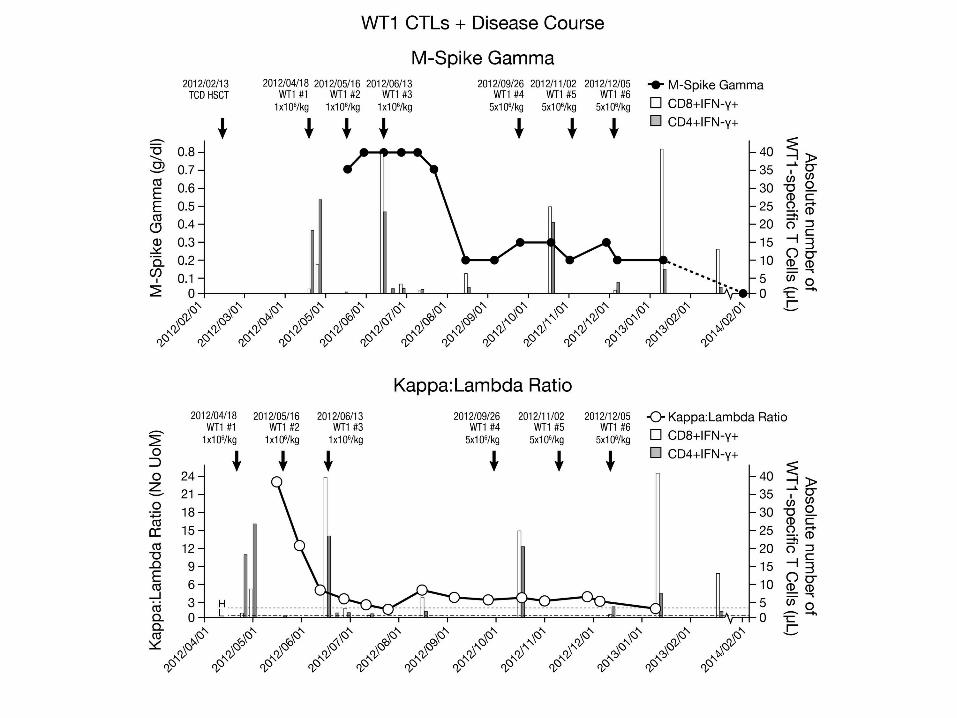
WT1 CTLs + Disease Course
WT1 #3 1x10e6/kg06/13/12
WT1 #2 1x10e6/kg05/16/12
WT1 #1 1x10e6/kg04/18/12
WT1 #4 5x10e6/kg09/26/12
WT1 #5 5x10e6/kg11/02/12
WT1 #6 5x10e6/kg12/05/12
TCD HSCT02/13/12
WT1 #1 1x10e6/kg04/18/12
WT1 #2 1x10e6/kg05/16/12
WT1 #3 1x10e6/kg06/13/12
WT1 #4 5x10e6/kg09/26/12
WT1 #5 5x10e6/kg11/02/12
WT1 #6 5x10e6/kg12/05/12
M-Spike Gamma
Kappa: Lambda Ratio
Feb 2014
Feb 2014
#
#

IHC With CD138 + WT1 mAb 6F-H2
Relapse11/11
Post allo BMT + WT1 CTL #1
05/16/12
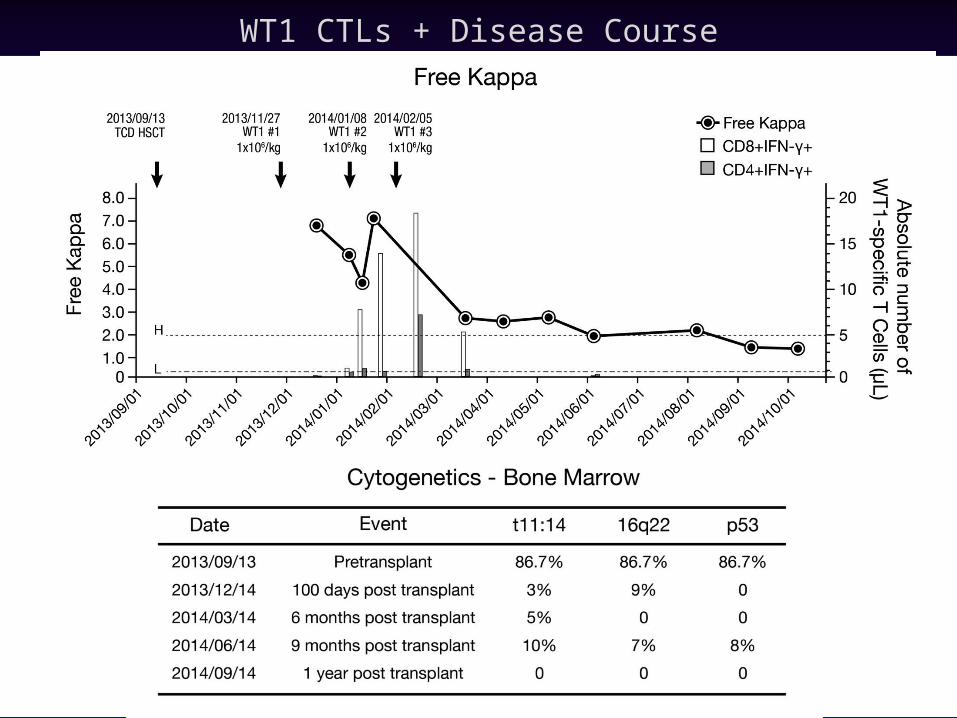
WT1 CTLs + Disease Course

Future Approaches to Treatment for High-Risk Multiple Myeloma
Induction Conditioning Maintenance
Relapse
UpfrontTCD HSCT
Suicide-gene modified DLI
WT1-specific CTLs
1.
2. Do we need an auto SCT? CRD x 6 cycles TCD HSCT WT1 CTLs ?
3. Do we need an allo SCT? Induction auto SCT MM-specific CARS?

AcknowledgementResearch Team
Eleanor Tyler, PhD, Cornell Weill CollegeAchim Jungbluth, MD, Pathology, MSKCCDenise Frosina, Senior Research TechnicianSean Devlin, PhD, Biostatistics, MSKCCEvelyn Orlando, RSA
Eric Smith, MD, PhDSatya Kosuri, MD
Adoptive Immune Cell Therapy Facility (AICT lab)
Ekaterina Doubrovina MD PhDRichard O’Reilly, MD
Myeloma Service
Heather Landau MD Hani Hassoun MD Alex Lesokhin MD Nikoletta Lendvai MD PhDDavid Chung MD, PhD Sergio Giralt MDOla Landgren, MD
Otsuka Pharmaceutical Co, Ltd – for generous research support