how to engage patients in necessary change: a dead simple
TRANSCRIPT
How To Engage Patients in Necessary Change:
A Dead Simple Roadmap
Robert R. Johnson, DOMedical Director, Amen Clinics
Diplomate, American Board of Addiction MedicineDiplomate, American Board of Psychiatry and Neurology
Agenda• Introduce the “Cycle of Renewal” and the 4 predictable
stages of change and transition• Discuss how to use this coaching model to call out vision,
engagement, and compliance in patients• Teach you some really simple and practical Motivational
Interviewing techniques that you can start using effectively on Monday!
“What if we had a few good maps that could support us through the changes, to show the way?”
William Bridges
Principle #1:
Life’s Greatest Illusion
If you were to graph it out, what would a healthy, mature,
successful adult life look like?
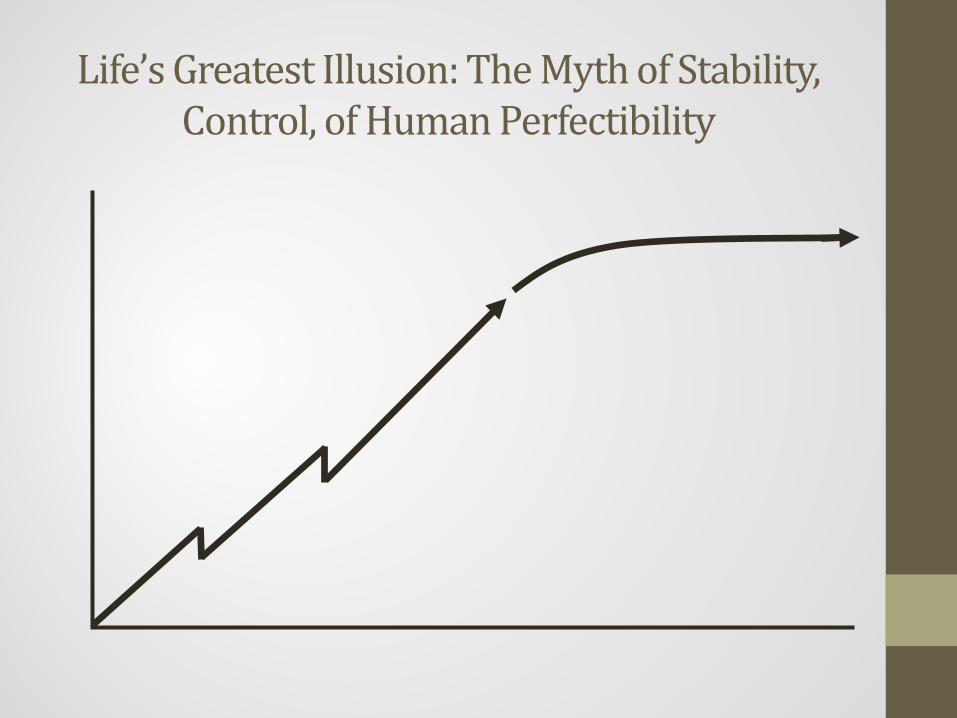
Life’s Greatest Illusion: The Myth of Stability, Control, of Human Perfectibility
If that’s an illusion, what does a healthy, mature, successful adult
life really look like?
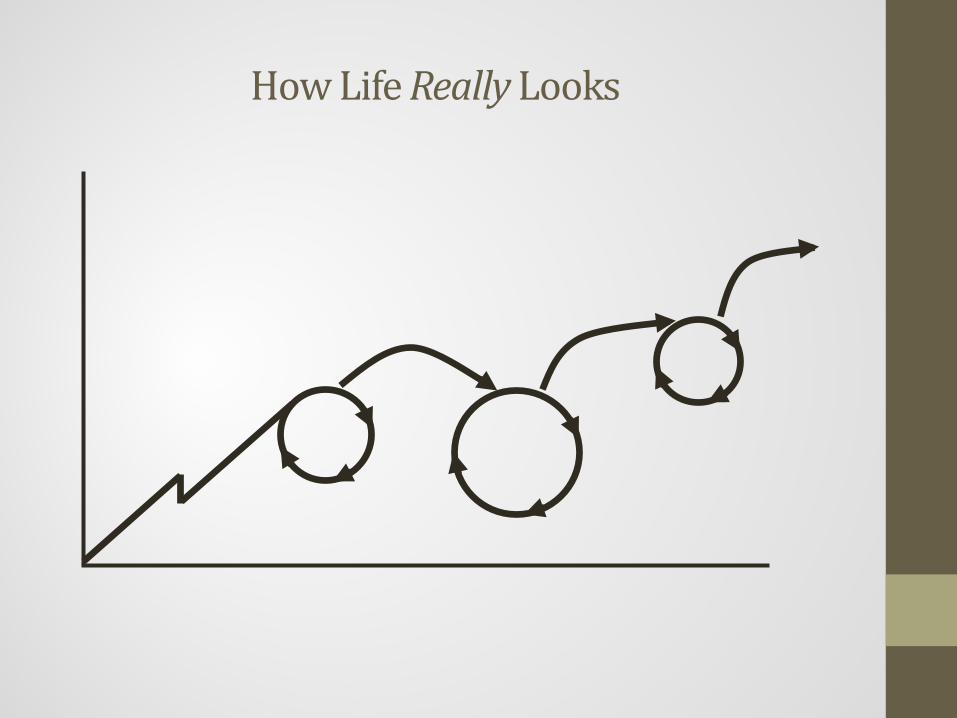
How Life Really Looks
The Truth: Life is more cyclical than linear
It’s amazing how much encouragement, hope, and direction this little change in perspective brings

Principle #2:
Life Chapters and Transitions Have Reliable Phases
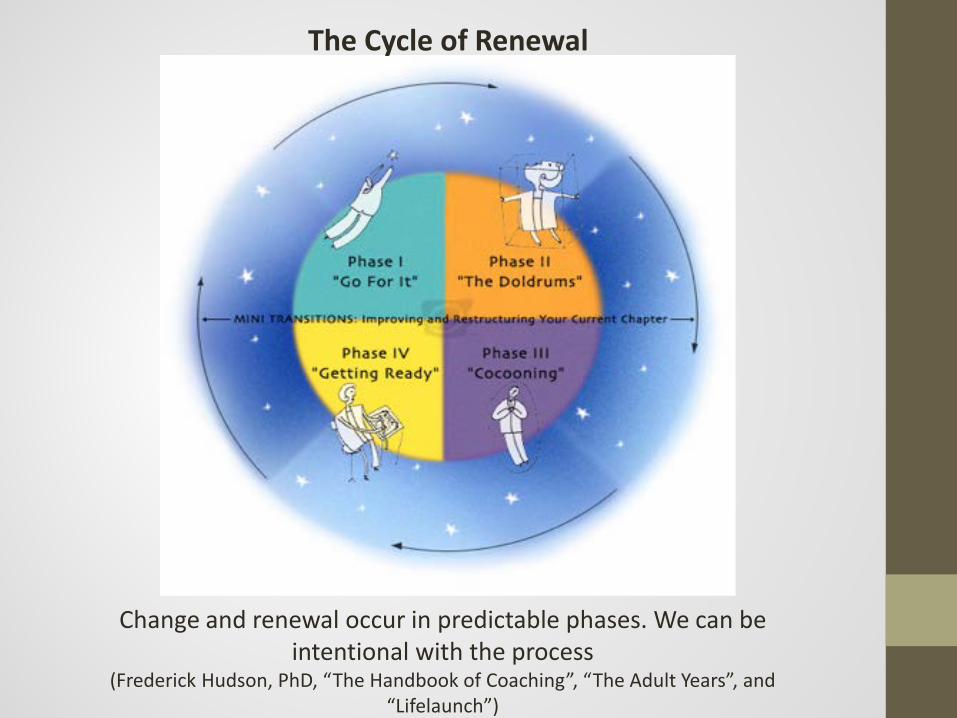
Change and renewal occur in predictable phases. We can be intentional with the process
(Frederick Hudson, PhD, “The Handbook of Coaching”, “The Adult Years”, and “Lifelaunch”)
The Cycle of Renewal
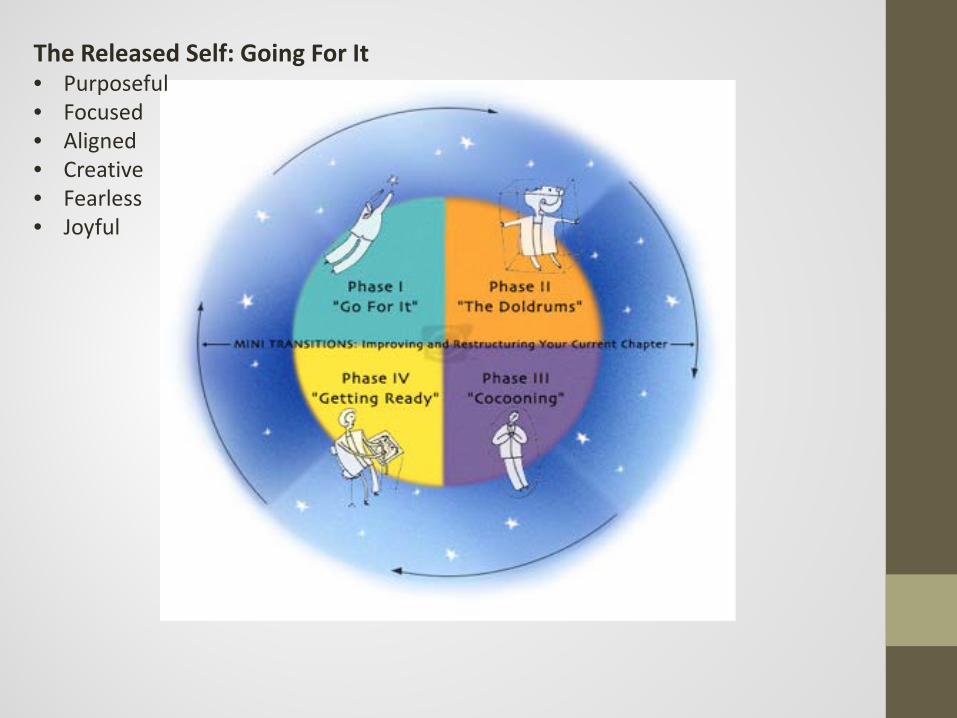
The Released Self: Going For It• Purposeful• Focused • Aligned• Creative • Fearless• Joyful
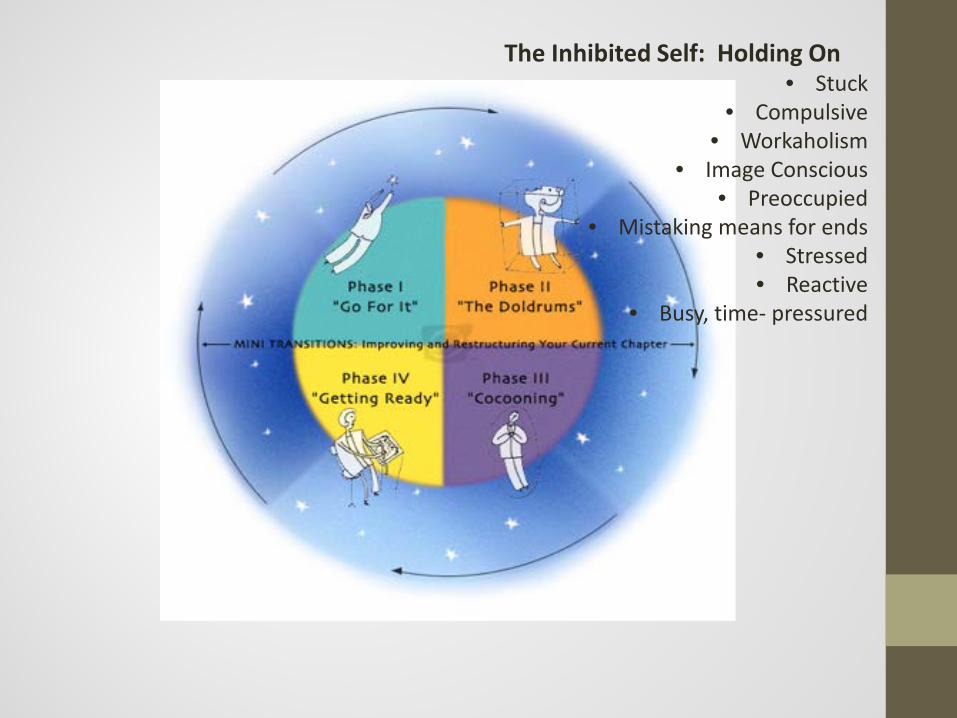
The Inhibited Self: Holding On• Stuck
• Compulsive• Workaholism
• Image Conscious• Preoccupied
• Mistaking means for ends• Stressed• Reactive
• Busy, time- pressured
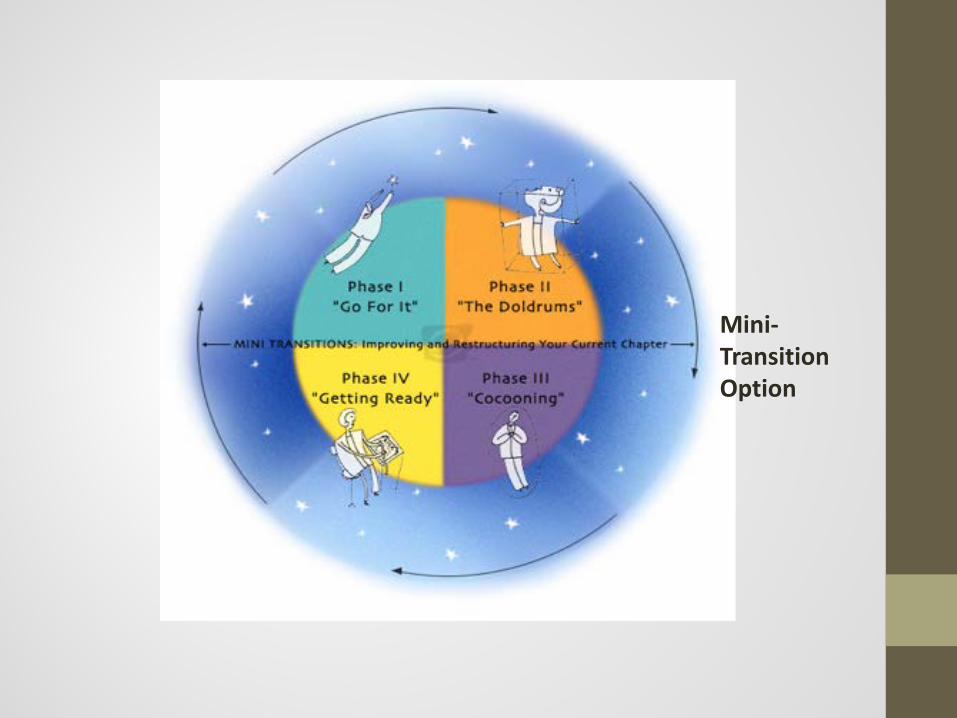
Mini-TransitionOption
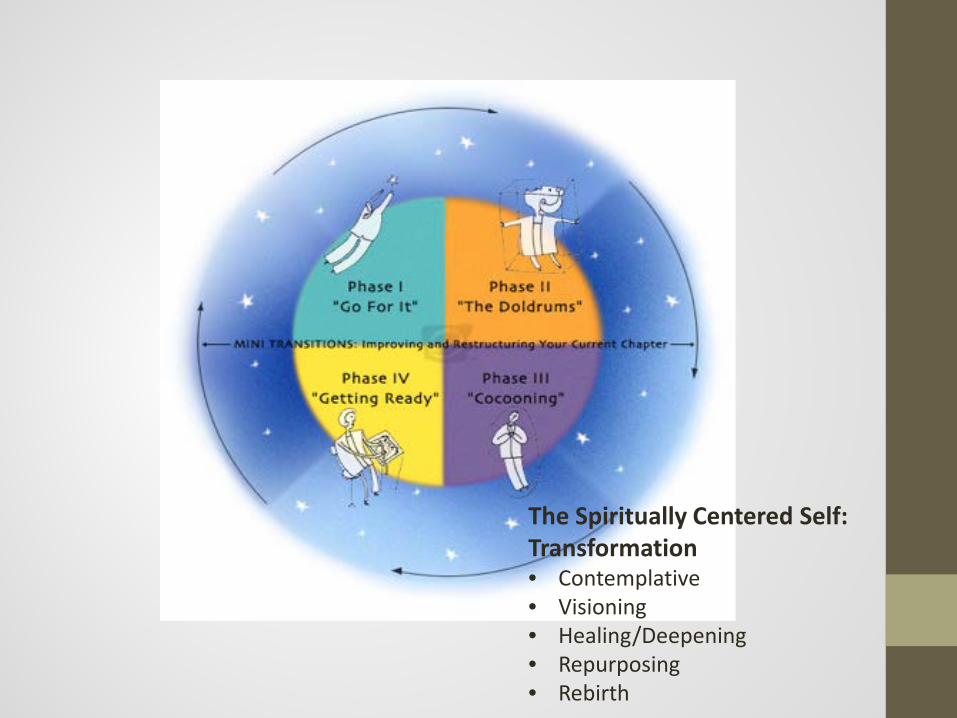
The Spiritually Centered Self: Transformation• Contemplative• Visioning• Healing/Deepening• Repurposing• Rebirth
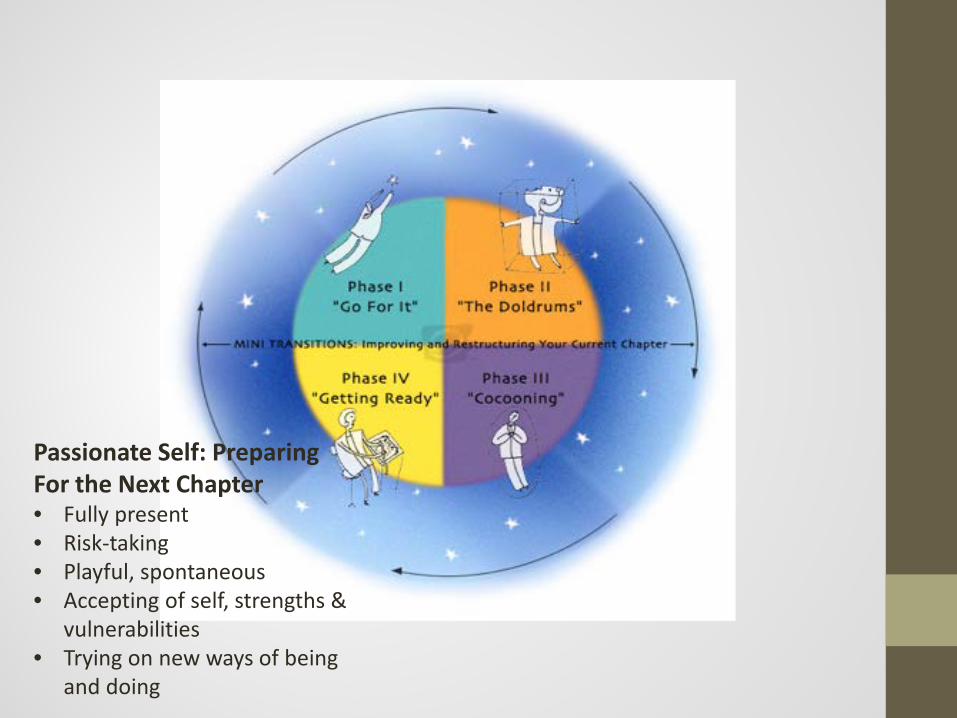
Passionate Self: Preparing For the Next Chapter• Fully present• Risk-taking• Playful, spontaneous• Accepting of self, strengths &
vulnerabilities• Trying on new ways of being
and doing
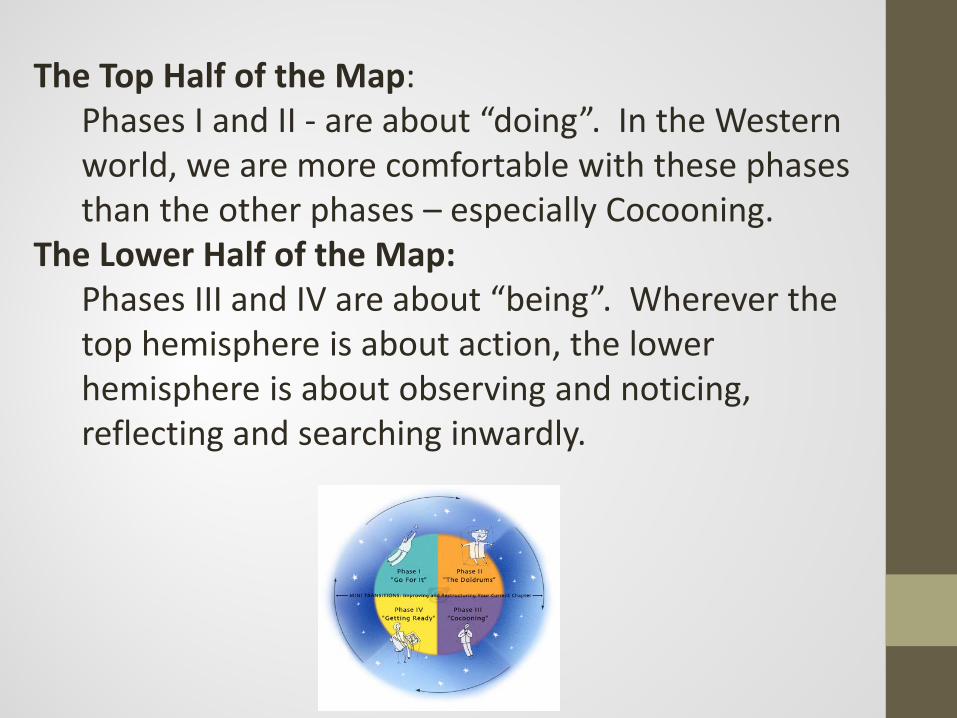
The Top Half of the Map:Phases I and II - are about “doing”. In the Western world, we are more comfortable with these phases than the other phases – especially Cocooning.
The Lower Half of the Map:Phases III and IV are about “being”. Wherever the top hemisphere is about action, the lower hemisphere is about observing and noticing, reflecting and searching inwardly.
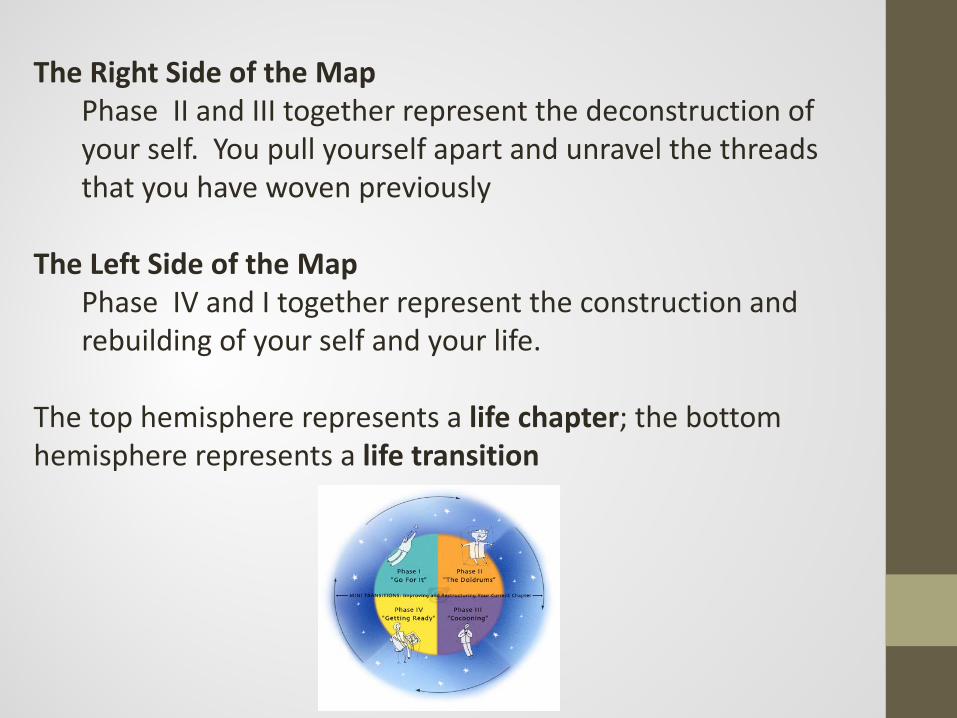
The Right Side of the MapPhase II and III together represent the deconstruction of your self. You pull yourself apart and unravel the threads that you have woven previously
The Left Side of the MapPhase IV and I together represent the construction and rebuilding of your self and your life.
The top hemisphere represents a life chapter; the bottom hemisphere represents a life transition
Principle #3:
Vision Trumps Vulnerabilities

"It's not what the vision is, it's what the vision does.”
Robert Fritz
Why Is Vision So Important?
Gap Diagram
"All the greatest and most important problems of life are fundamentally insoluble... They can never be solved, but only outgrown. This "outgrowth" proved on further investigation to require a new level of consciousness. Some higher or wider interest appeared on the patient's horizon, and through this broadening of his or her outlook the insoluble problem lost its urgency. It was not solved logically in its own terms but faded when confronted with a new and stronger life urge."
Carl Jung
Why Is Vision So Important?
What Is The Engine of Transformation?
“When people truly discover some aspect of their vision and have the opportunity to dedicate themselves to working on it, when they can tell the truth and focus on aspirations instead of on “being less bad”, when they can be themselves, then something changes. An inner alignment starts to develop that can release extraordinary energy and creativity... People can start to bring all of themselves to their endeavor.”
Peter Senge
It’s Not Enough to Simply Manage an Illness or Stop a Bad Habit
Health is not only the ability to say “NO” to all the options and voices that
are contrary to one’s values…
It is also the ability to say “YES” to something so completely that all other voices and values
are silenced.
What Will You Say “Yes” To?
Principle #4: “Positive Vision” vs. “Negative Vision”
“Ultimately, change strategies based on reacting to threats limit the commitment, imagination, and collective intelligence needed for ongoing growth and innovation. In short, fear cramps imagination.”
Peter Senge, The Necessary Revolution
How Are Your Goals Framed?
“Negative Vision”: Working against something, getting ‘less bad’ (“anti-smoking”, “anti-drugs”)“Positive Vision” (creating something new)
Doing less harm, while laudable, is not the same as working to create what we truly seek
If a car is heading south, slowing down does not cause it to head north...
Principle #5: The Goal is Disequilibrium
We don’t want to promote greater stability, we want to promote
disequilibrium in the service of our patients’ potential
Principle #6: The Truth About Anxiety
Anxiety is natural and normal. It is the actual feeling of growing. Anxiety denied leads to symptoms, anxiety embraced leads to growth. Anxiety suppressed weakens you, anxiety integrated gives you power.
Peter Koestenbaum
The Truth About Anxiety
Anxiety generates knowledge
Anxiety leads to action
Anxiety makes you a grown-up
Soren Kierkegaard
The Truth About Anxiety
Anxiety is not a disease, but the normal feeling of transitions.
William Bridges
Principle #7: The Role of An Imperfect, Messy Spirituality
People don’t talk about the central role of spirituality in health, sobriety, and accomplishment, because they don’t know how to demystify it, to make it practical
Also, many of us come to issues of religion and spirituality with old baggage...
The Role of An Imperfect, Messy Spirituality
“Religion is for people who are afraid of going to hell: spirituality is for those who have been there.”
Ross V., Member of Alcoholics Anonymous
The Role of An Imperfect, Messy Spirituality
Spirituality is lot like health. We all have health; we have good health or poor health but it is something we can’t avoid having. The same is true of spirituality: Every human being is a spiritual being. The question is not whether we “have spirituality” but whether the spirituality we have is a negative one that leads to isolation and self-destruction, or one that is more positive and life-giving.
Question: What’s Been Feeding YourSpirit?
The Role of An Imperfect, Messy Spirituality
“The spiritual life begins with the acceptance of our wounded self.”
Brennan Manning
The Role of An Imperfect, Messy Spirituality
The truth is, we are a mess. None of us is who we appear to be. We all have secrets. We all have issues. We all struggle from time to time. No one is perfect. The essence of an authentic spirituality is the refusal to pretend, to lie, or to allow others to believe we are something we are not. Coupled with the recognition that we can’t repair ourselves.
Charlie Brown
“Life is like a deck chair, Charlie”, Lucy says.
“On the cruise ship of life, some people place their deck chairs at the rear of the ship so they can see where they’ve been. Others place their deck chair at the front of the ship so they can see where they’re going.”
39
Charlie Brown (cont.)
The good ‘doctor’ looks at her puzzled client and asks, “Which way is your deck chair facing?” Without hesitating, Charlie replies glumly, “I can’t even get my deck chair unfolded.”
40
The Role of An Imperfect, Messy Spirituality
“Accepting the reality of our broken, flawed lives is the beginning of spirituality not because the spiritual life will remove our flaws but because we let go of seeking perfection and, instead, seek God, the one who is present in the tangledness of our lives. Spirituality is not about being fixed; it is about God’s being present in the mess of our unfixedness.”
Michael Yaconelli, “Messy Spirituality”
God and Higher Power
The Role of An Imperfect, Messy Spirituality
“Messy spirituality” breaks through the religious wall of secrecy and legitimizes faith that is unfinished, incomplete, and inexperienced
Messy spirituality speaks of a celebration of a spiritual life that is under construction
Spirituality and Addiction
“Addiction keeps a person in touch with God…at the very point of the vulnerability is where the surrender takes place—that is where God enters. God comes through the wound.”
Marion Woodman
Eric Clapton
“What am I? I’m an alcoholic, actually. My identity shifted when I got into recovery. That’s who I am now, and it actually gives me greater pleasure to have that identity than to be a musician or anything else, because it keeps me in a manageable size. When I’m down on the ground with my disease – which I’m happy to have – it gets me in tune. It gives me a spiritual anchor. Don’t ask me to explain.”
Have you had your Dylan moment?
What Is Your Dylan Moment?
“... it dawned on me that I might have to change my inner thought patterns… that I would have to start believing in possibilities that I wouldn’t have allowed before, that I had been closing my creativity down to a very narrow, controllable scale… that things had become too familiar and I might have to disorientate myself.”
What Is Your Dylan Moment?
“The thought occurred to me that maybe I’d have to write my own folk songs, ones that Mike didn’t know. That was a startling thought…it struck me that I’d never been there before…I wasn’t ready to act on it but knew somehow, though, that if I wanted to stay playing music, that I would have to claim a larger part of myself. I would have to overlook a lot of things – a lot of things that might even need attention – but that was all right…I had the map, could even draw it freehand if I had to. Now I knew I’d have to throw it away. Not today, not tonight, sometimes soon, though.”
Are you in transition in your life?
What’s still working for you?
What’s no longer working?
What phase in the Cycle of Renewal are you in?
How does it feel to be in the phase you are in?
Questions for Patients
What changes - inside or around you - have led you to your current phase?
Who are you, in this season of your life?
Who aren’t you any longer?
What matters most to you, now? What do you want to create in your life?
Questions for Patients
Questions for Patients
What are the changes you’re willing to make to align your life around the answers to those questions?
“Let’s talk about the structure and assistance you might need to create that alignment…”
What would a brain healthy, spiritually-grounded, purpose-focused life look like
for you in this next chapter of your life?
Role PlayEvaluation
What phase in the Cycle of Renewal are you in?
How does it feel to be in the phase you are in?
What changes - inside or around you - have led you to your current phase?
What matters most to you, now? What do you want to create in your life?
Intervention• What are the changes you’re willing to make to align
your life around the answers to those questions?
The Practical Use of Motivational Interviewing
When you meet a friend who…• Drinks too much, with no intention of quitting• Smokes a pack per day• Is obese• Doesn’t exercise• Has high blood pressure• But is unwilling to take your advice, change their lifestyle,
or comply with medication recommendations by their doctor
How do you feel?
When your adolescent, ADD son…• Refuses to turn down the music and do his
homework• Smells of cigarette smoke• Hangs out with friends who drink• Stops participating in healthy activities
How do you feel?
How do you feel?...• Sad• Helpless• Scared• Frustrated• Irritated • Unsure of how to help• Defeated before I start
So we respond with• (Internal) Judgment
• Unwanted advice• Scary stories of the risks they face• (Oh so subtle…) Efforts to elicit or coerce a
commitment to change their behavior• Withhold validation or encouragement until they
change their ways
… then repeat this advise, convince, prescribe, mandate, and subtle shaming approach at every opportunity
How’s that been working for you?
The Goal of This Session
To help you become more effective at facilitating real behavioral change in
yourself, your family, and your patients
How Will We Accomplish That?
Will teach you how to:• Perform rapid assessments of ones’ readiness for
change• Employ practical strategies to (a) enhance your
own and others’ motivation and (b) overcome barriers to change
Stages of Change
• The decision to make a lifestyle change is the result of a NATURAL process that takes place in STAGES over a certain period of time
• We’re going to talk about how to recognize, reinforce, and accelerate the natural process throughout these stages

Stages of Change
50%
20 - 30%
10 – 20%%
5 – 10 %%
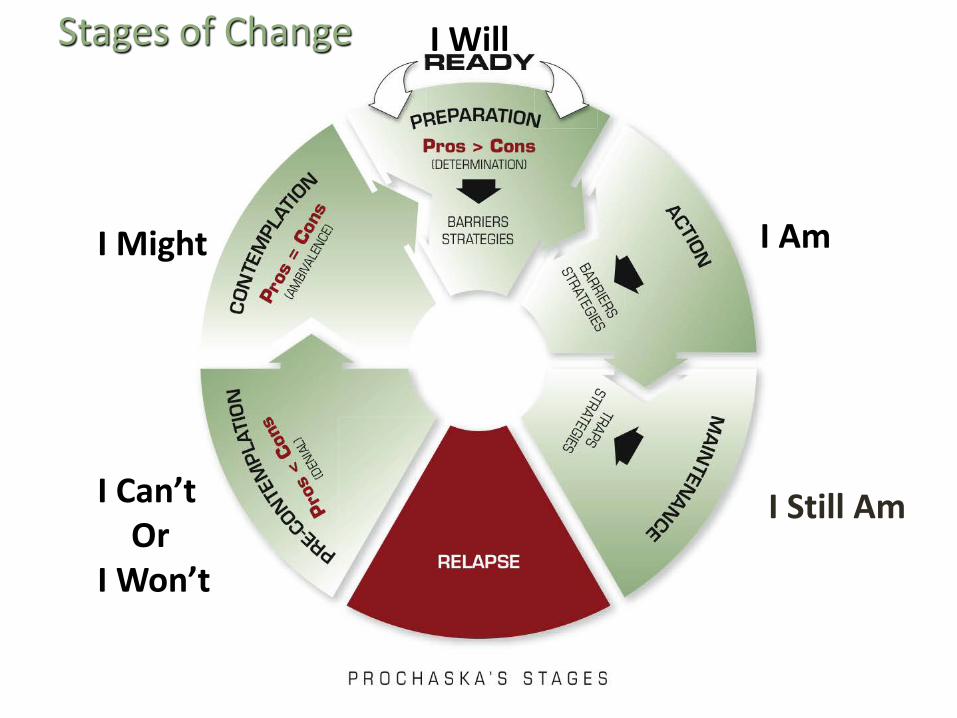
Stages of Change
I Can’tOr
I Won’t
I Might
I Will
I Am
I Still Am
“I have tried walking every day. The temperature is horrible in Buffalo! Do you think a stationary bike or a treadmill would be better?”
“I’ve lost 3 pounds in two months! On bad weather days, I go walking at the shopping mall…”
“I am always alone; all my children live far away. Smoking is all I have left!”
STAGES OF BEHAVIOURAL CHANGE
EXERCISES:
1.
2.
3.
“My grandfather died at the age of 94. He drank like a fish andsmoked like a chimney!”
“It’s not good to smoke, but if I quit, I gain weight. I’m replacing one problem with another!”
“Drinking Scotch may not be good for my high blood pressure butIt relaxes me coming back from work.”
STAGES OF BEHAVIOURAL CHANGE
EXERCISES:
3.
4.
5.
Determining the StageStages are evaluated by using the open-ended question: “What would you think about…?”• Quitting smoking?• Getting more exercise?• Changing your eating habits?• Cutting down or abstaining from alcohol?
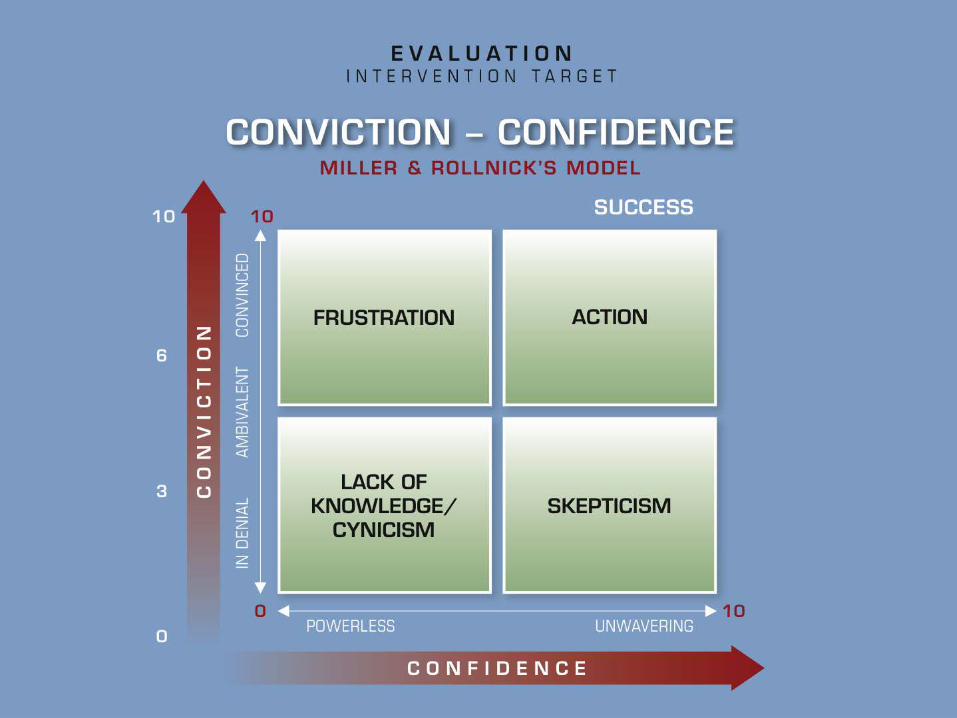
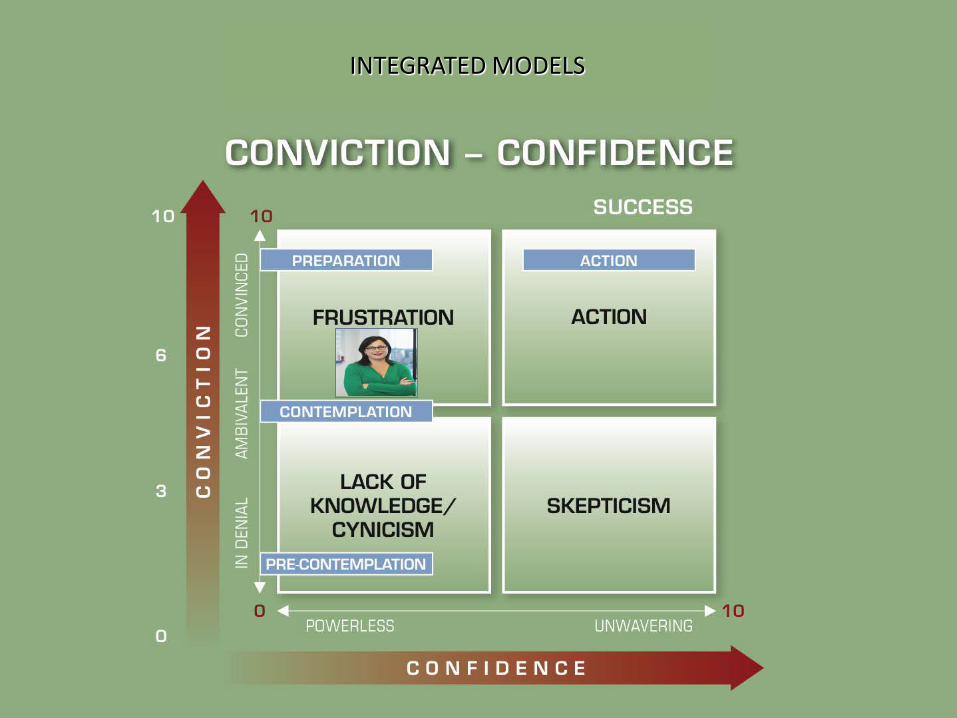
After Determining Stage:Assess whether your immediate goal is to increase:• CONVICTION: Perceiving the benefits that would result
from a behavior change• CONFIDENCE: Feeling capable of changing a behavior
“CONVICTION”:Recognizing the benefitsof changing a behavior.
Q: “If you decided to… how wouldthat benefit you?”
“CONFIDENCE”:Sense of our ability
to modify a behavior.
Q: “If you really decided to… do you think you could do it?”
MOYENNNE: ABSTRAIT (CONNAISSANCES)« Ma santé serait meilleure, je vivrais plus vieux… Mon risque de maladie diminuerait, mon risque d’infarctus serait plus petit,Mon taux de cholestérol serait meilleur. »
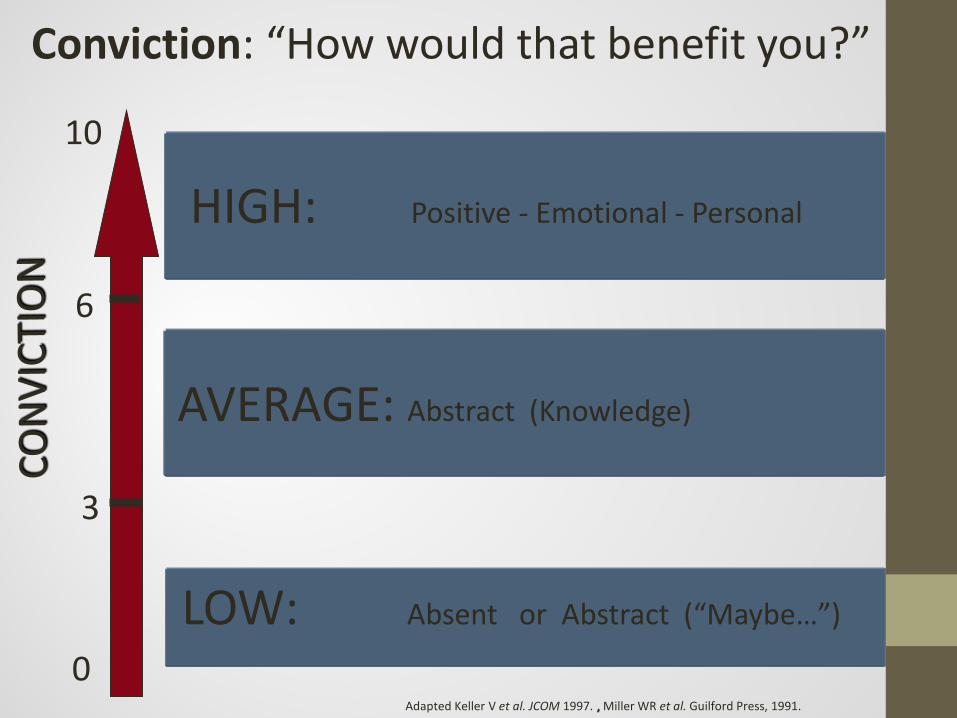
0
10
6
3
Conviction: “How would that benefit you?”
AVERAGE: Abstract (Knowledge)
HIGH: Positive - Emotional - Personal
LOW: Absent or Abstract (“Maybe…”)
Adapted Keller V et al. JCOM 1997. , Miller WR et al. Guilford Press, 1991.
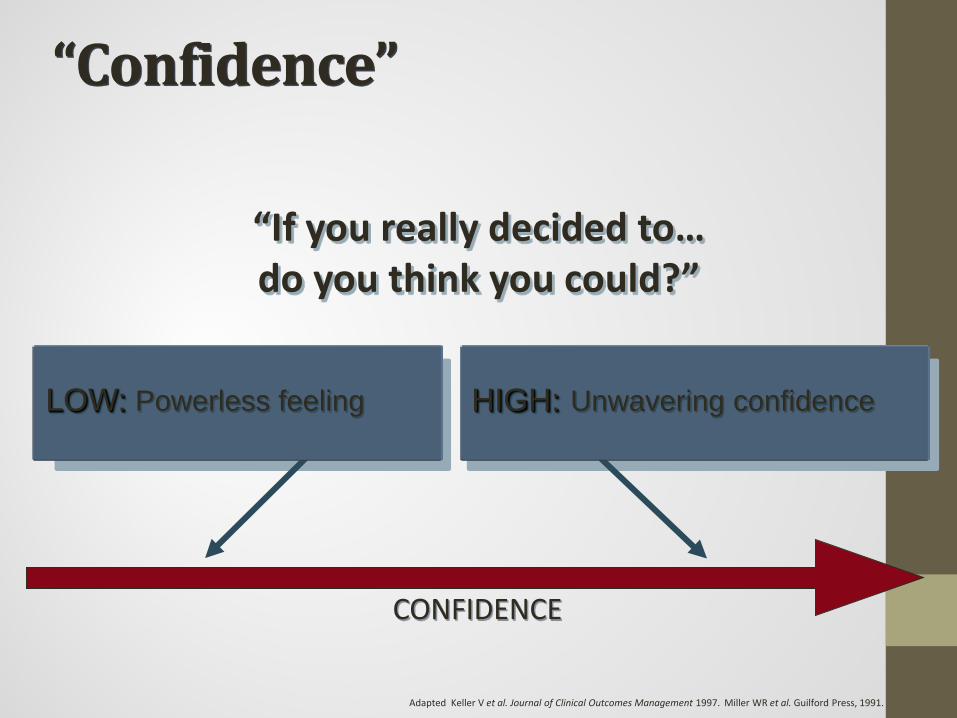
“Confidence”
CONFIDENCE
LOW: Powerless feeling
“If you really decided to…do you think you could?”
HIGH: Unwavering confidence
Adapted Keller V et al. Journal of Clinical Outcomes Management 1997. Miller WR et al. Guilford Press, 1991.
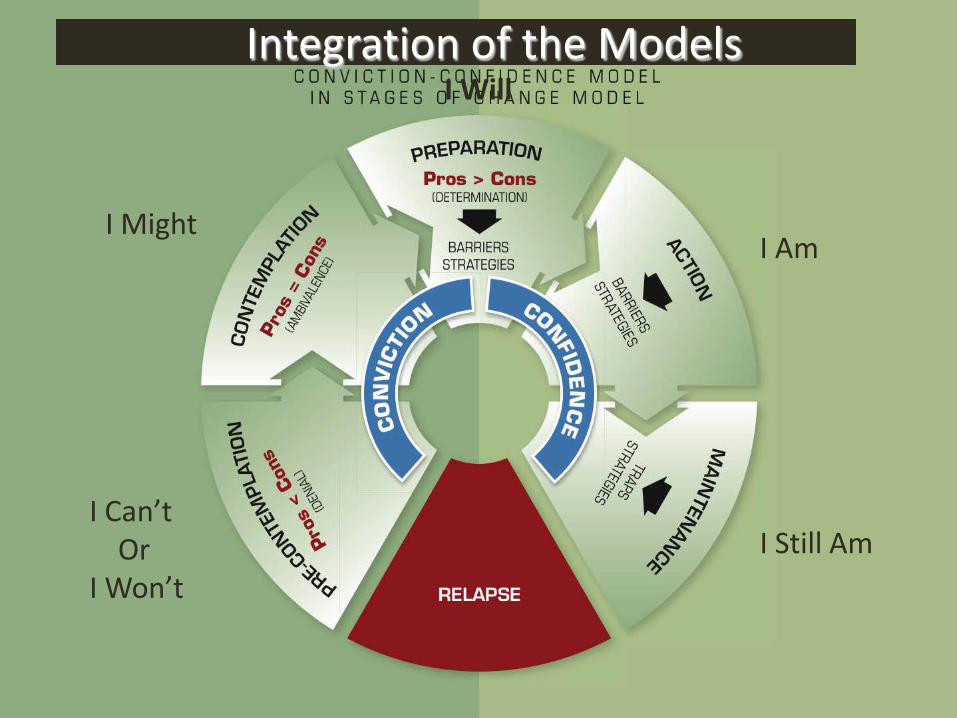
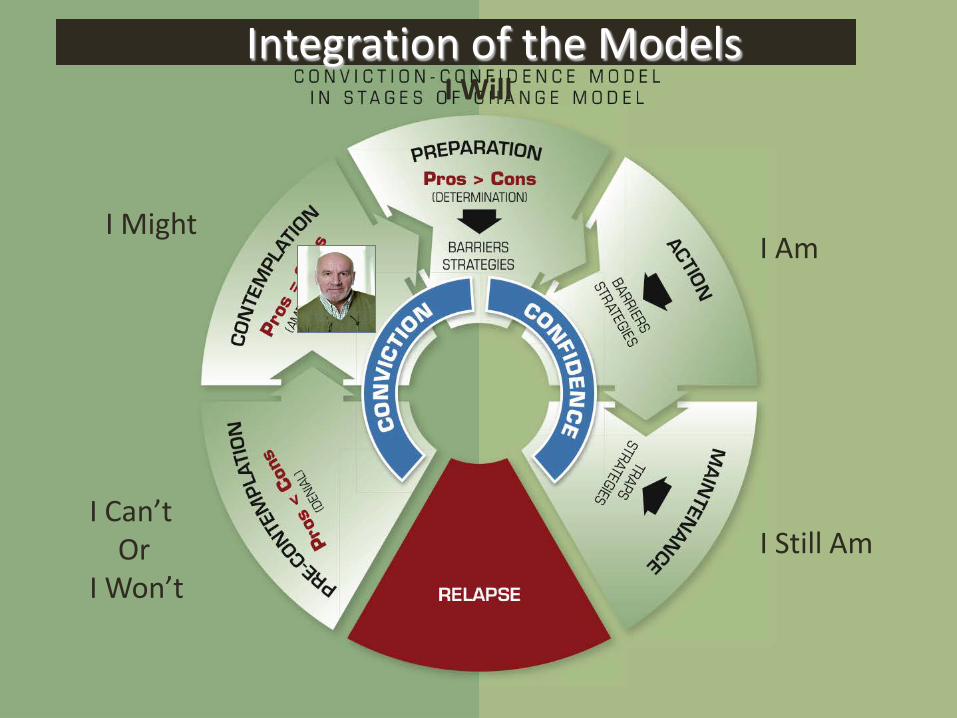
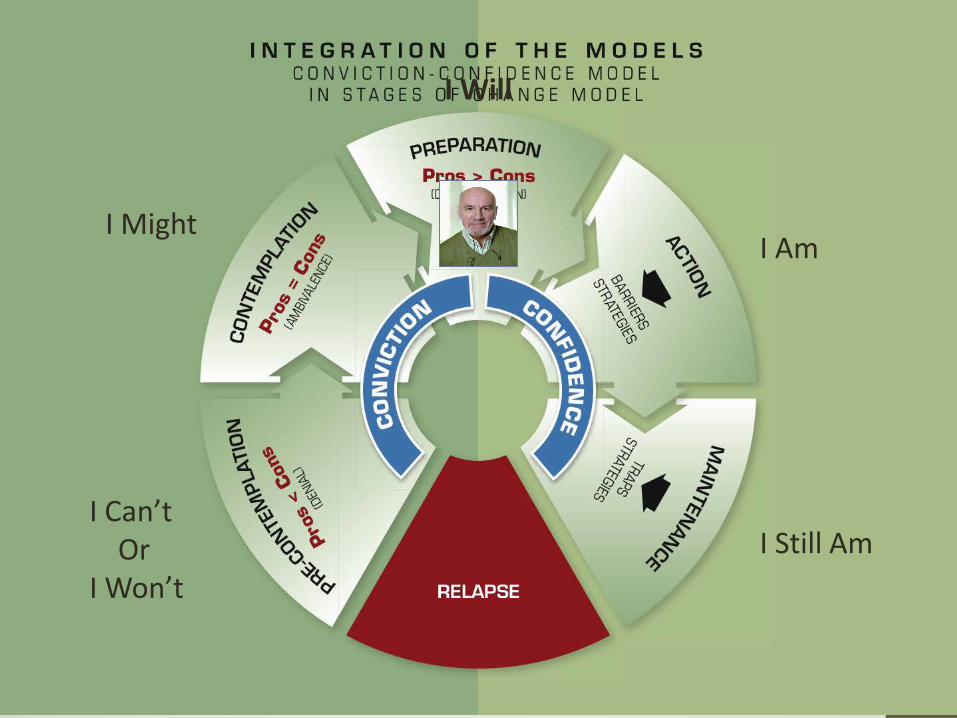
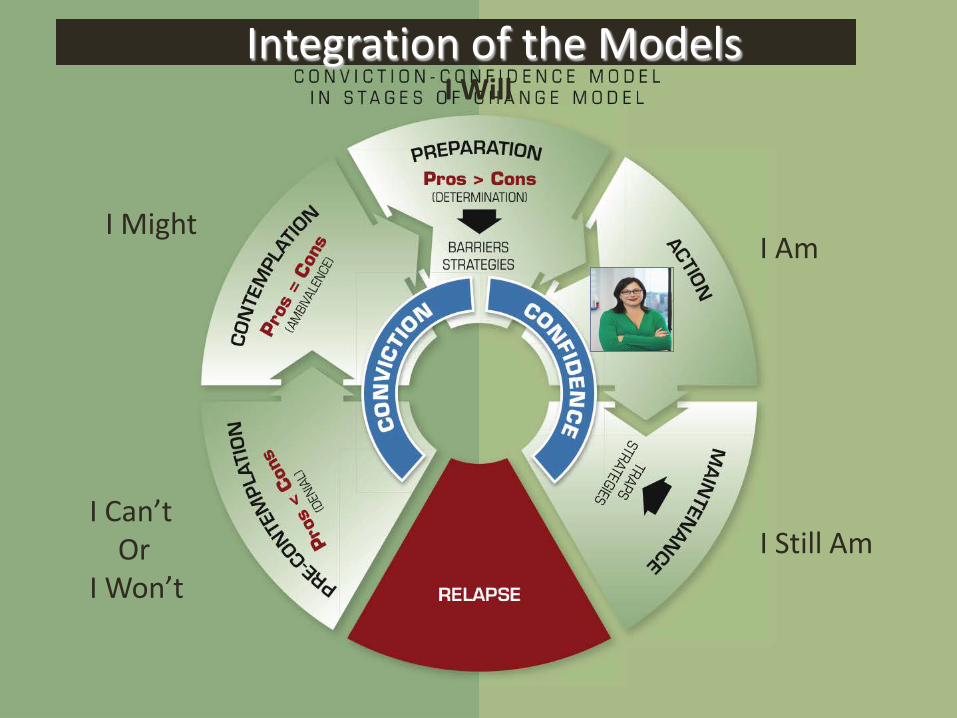
Integration of the Models
I Can’tOr
I Won’t
I MightI Am
I Still Am
I Will
Your Patient, Dan
1) 54 years old2) Obese3) Myocardial infarction 2005 4) Cholesterol and lipids elevated5) Chronic obstructive pulmonary disease (COPD)
Has smoked since age 12, and has never tried to quit
Quit drinking 4 years ago
DanSTAGE:You: “Have you ever thought about doing something about your smoking habit?”Dan: “I’ll probably quit someday, but I’m not ready now.”
DanSTAGE: ContemplationYou: “Have you ever thought about doing something about your smoking habit?”Dan: “I’ll probably quit someday, but I’m not ready now.”
DanYou: “How do you think quitting smoking would benefit you?”Dan: “I think I’d be healthier.”
Conviction: Moderate and Impersonal
You: “If you decided to quit smoking, do you think you could do it?”Dan: “If I decided to quit, I wouldn’t have any problem. I quit drinking four years ago and I’ve never fallen off the wagon.
Confidence: High and Personal
Dan• “I’ll stop smoking eventually but I’m not ready yet.”
• Stage: Contemplation• “My health would be better.”
• Conviction: Moderate and Impersonal• “Hey, I quit drinking 4 years ago. I know I could do it if I
set my mind to it.”• Confidence: High and Personal
Goal: Dan is at the Contemplation stage with moderate conviction and high confidence. So the goal for the intervention should be to increase his level of motivation, in order to get him to the Preparation stage.
Integration of the Models
I Can’tOr
I Won’t
I MightI Am
I Still Am
I Will
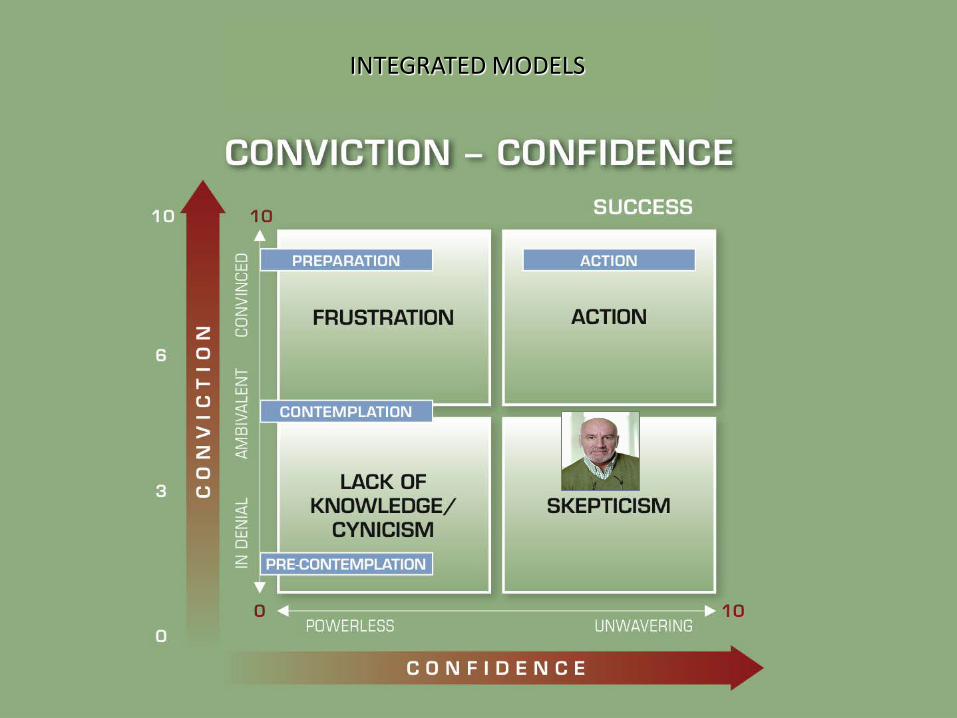
INTEGRATED MODELS
DanIntervention: What do you do now?
DanInterventionAsk open-ended questions that encourage Dan to express himself about the benefits of changing his behavior (don’t try to answer for him).
Then mirror back Dan’s responses to lead him to talk about personal advantages, with an emotional content
DanInterventionYou: “How do you think quitting smoking would benefit you?”Dan: “I think I’d be healthier.” (abstract benefit: low conviction)You: “How specifically would it improve?”Dan: “I wouldn’t cough as much and I wouldn’t be so short of breath” (Benefits are more personal. Pain and discomfort are not abstract concepts: moderate conviction)
DanYou: “If you weren’t so short of breath, what else could you do?”Dan: “Well, I guess my quality of life would be much better. For instance, just the other day I tried to play with my grandchildren. I had to stop after 30 seconds because I was just so short of breath. I could be much closer to my grandchildren. I could do more things with them, maybe take them on trips.” (The benefits are now very personal and highly emotionally charged. “Play with grandchildren”: high conviction)
DanReinforcement
You: “So, it would be great if you weren’t so short of breath. You could really enjoy life and be closer to your grandchildren?”
Once the person has reached the Preparation (“I Will”) stage (high Motivation), this is the time to boost their Confidence by switching to open-ended questions that encourage the person to identify Obstacles and Strategies with goal of action stage.Dan is already strong in Confidence.
I Can’tOr
I Won’t
I MightI Am
I Still Am
I Will
Concluding the Interaction:3 Options:• Offer the person information
(oral information or literature)• Raise questions that give the person food for thought
• “If you were to rate your motivation to quit smoking on a 1-10 scale, where would you rate it?”
• If Dan says “4”, what would you say?
Case #2: Rene’s Health & Weight Loss Goals
(working on Confidence issues identifying barriers and effective strategies)
Intervention to Increase Confidence
• 1• If you really decide to…
do you think you could do it?
• 2• What would prevent you from…?
« BARRIERS»
• 3• How do you think you can start..?
« STRATEGIES »
Your Patient, ReneRene, 36-year-old customer service rep• Has been unable to lose the 40 pounds gained over
the course of her two pregnancies; now weighs 175 pounds
• Tries to eat healthy foods• Was an avid athlete prior to marriage and
subsequent divorce, now claims she has no time for regular exercise
• No hormone issues• Wakes up at 5:30 AM, is at work by 7 AM, then
works non-stop until 7 PM. • Back home she eats and goes to bed early, “totally
exhausted”
ReneSTAGE:You: “Have you thought about increasing your level of physical activity?”Rene: “I’d love to be more active and hopefully I will be in a few months when I have found someone to help out with the housework.”
ReneSTAGE: PreparationYou: “What do you think about your level of physical activity?”Rene: “I’d love to be more active and hopefully I will be in a few months when I have found someone to help out with the housework.”
ReneConviction:You: “What benefits do you see in becoming more physically active?”Rene: “I used to be really active and I’d like to get back into shape. I wouldn’t feel exhausted at the end of the day. Then I could finally lose this weight, get in shape and have more energy.”
ConfidenceYou: “Do you think you could do it?”Rene: “Right now I get up early with the kids, work all day and collapse after I get them into bed. I don’t see how I could do it right now.”
ReneConviction: High ConvictionYou: “What benefits do you see in becoming more physically active?”Rene: “I used to be really active and I’d like to get back into shape. I wouldn’t feel exhausted at the end of the day. Then I could finally lose this weight, get in shape and have more energy.”
Confidence: Very Low ConfidenceYou: “Do you think you could do it?”Rene: “Right now I get up early with the kids, work all day and collapse after I get them into bed. I don’t see how I could do it right now.”
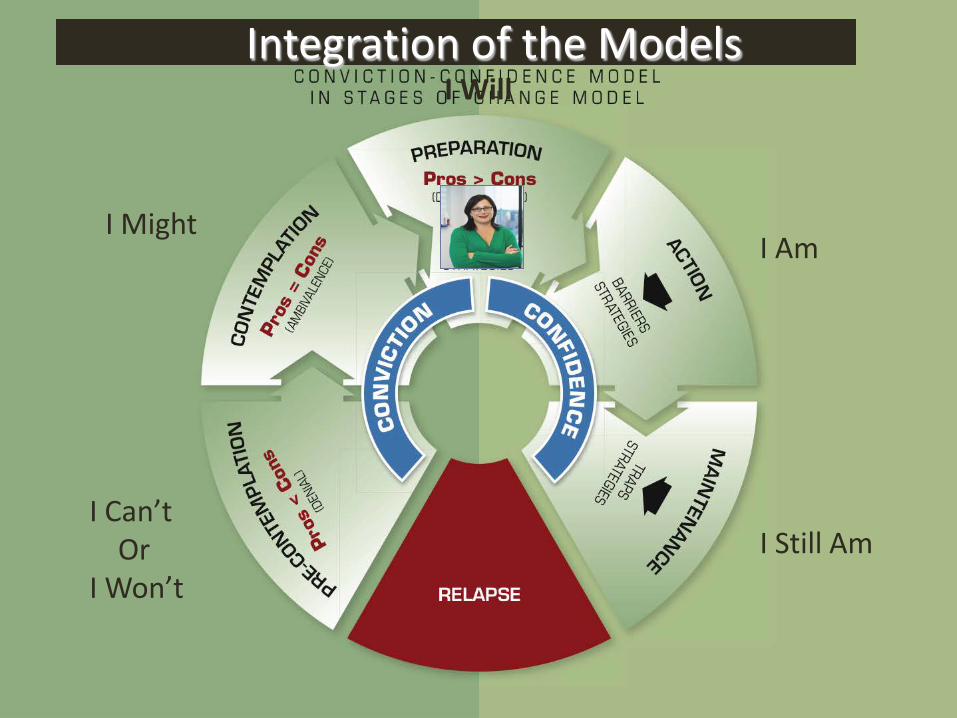
Integration of the Models
I Can’tOr
I Won’t
I MightI Am
I Still Am
I Will
INTEGRATED MODELS
ReneIntervention: What do you do now?
Intervention to Increase Confidence• To increase confidence, ask 3 questions in a row
to encourage Rene to express how she sees her own obstacles and solutions
Intervention to Increase Confidence
• 1• If you really decide to…
do you think you could do it?
• 2• What would prevent you from…?
« BARRIERS»
• 3• How do you think you can start..?
« STRATEGIES »
ReneIdentification of obstaclesYou: “If you really decided to get more exercise, do you think you could?”Rene: “I guess so, but it would be pretty tough.” You: “What would prevent you from getting more exercise?”Rene: “Time and energy.”
The obstacles are time and energy.
ReneIdentification of solutionsYou: “How do you think you could work around this?”Rene: “I guess I could start by taking the kids for a walk after I’m finished with work.” You: “From a practical point of view, do you know how you could start doing this?”Rene: “Yes, I could walk for 30 minutes three times a week.”
Intervention to Increase Confidence• Once the person has expressed their perceived obstacles
and solutions, the conversation concludes with an agreement on steps to be taken (actions) before your next interaction
• This action is realistic because it is based on solutions put forward by the individual themselves.
• Even if it is only partially successful, it can be a first step toward building the person’s confidence and serving as a foundation for the next stage.
ReneConclusion: negotiating concrete actionYou: “Are you saying you’ve decided today to walk 30 minutes three times a week? If so I’ll check in with you next week to see how it’s going.”Rene: “OK, I agree. I’ll start tomorrow. Let’s see how it goes!”
This is how the process begins. This realistic strategy (small step: 30 mins of physical activity three times a week) has every chance of succeeding. Encouraged by this partial success and improved well-being, Rene will be more inclined to take the next step, i.e., to increase the duration and intensity of her daily workouts.
Integration of the Models
I Can’tOr
I Won’t
I MightI Am
I Still Am
I Will
Dr. J, Last Week: Patient Jeff
• 21 y/o male with Major Depressive Disorder, PTSD, Alcohol and Nicotine Dependence
• “I’ve used alcohol since I was fourteen to cope with depression and anxiety”.
• First time he drank “I experienced a sense of ease I had never felt before… I felt I finally clicked with society”, and “I’ve not found a reason to quit.”
• At Initial Evaluation was drinking heavily, averaging 15-20 beers/day plus occasional hard liquor, and would binge drink for weeks at a time.
• Single DUI, and history of fighting when drunk.
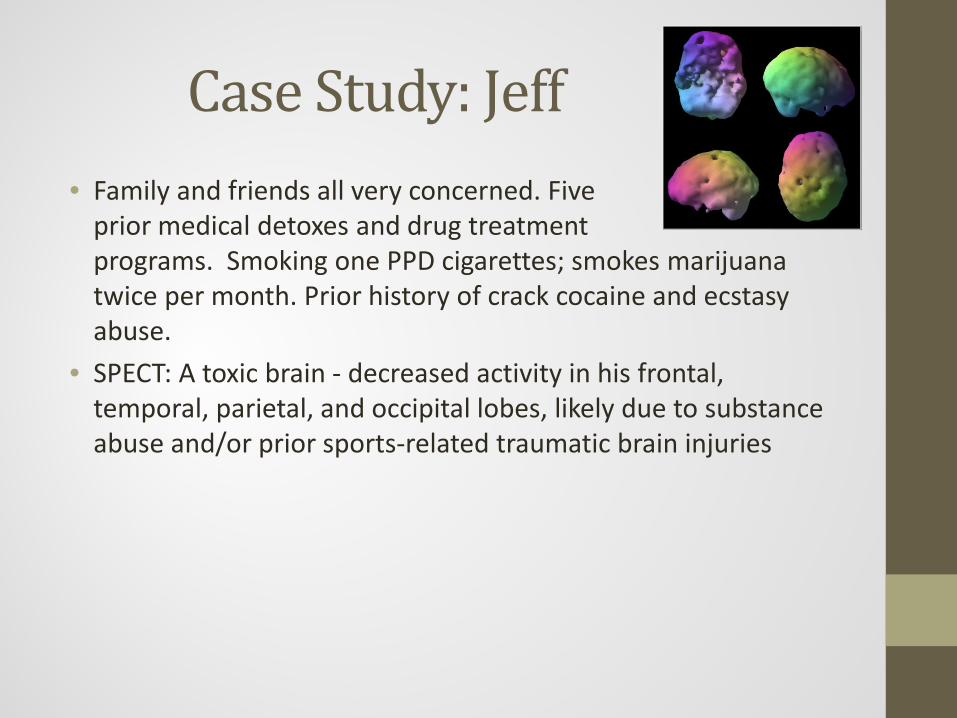
Case Study: Jeff• Family and friends all very concerned. Five
prior medical detoxes and drug treatment programs. Smoking one PPD cigarettes; smokes marijuana twice per month. Prior history of crack cocaine and ecstasy abuse.
• SPECT: A toxic brain - decreased activity in his frontal, temporal, parietal, and occipital lobes, likely due to substance abuse and/or prior sports-related traumatic brain injuries
Case Study: JeffFollowing Initial Motivational Interviewing Intervention:• 3rd follow-up session: now 115 days abstinent from alcohol, a full-
time student, states “It feels really good to be sober!”• Friends are still drinking, “But it’s not attractive to me anymore…
they’re not doing anything with their lives… I feel I’ve changed in terms of what I want to do with my life. Before I was comfortable with not doing anything, but not any longer.”
• Dr. J: “What contributed to this shift in motivation and drive?”• Jeff: “Just getting sober and having a good understanding of what’s
going on, through you guys. That was a big thing when we took a look at my brain and figured out what was happening. That was the biggest thing. Now I just need to quit smoking.”

“Now I just need to quit smoking”
Staging his stage of change, conviction, and confidence:
• Dr. J: “If you were to cut back or quit, how would that benefit you?”
• Jeff: “It puts me as close to the old days as I want to be… quitting would kind of remove those ties completely.”
• Dr. J: “Cutting those ties would do what for you, personally?”• Jeff: “It might help close off that self-destructive part of
myself… and I really want to be a role model for my nephews, and for my friends.”
• Dr. J: “So if you quit smoking you could be the role model you’ve wanted to be for your friends and family, and it would represent the next step in leaving your old life behind?”
• Jeff: “You got it!”
“I just need to quit smoking”• Dr. J: “If you decided to quit, do you think you
could do it?”• Jeff: “I don’t know… that’s a tough one. I’ve
never tried to quit before.” • Dr. J: “What hurdles would you anticipate
running into?”• Jeff: “I don’t really know.”
Case Study: JeffMotivation Level: ContemplationCommitment: Moderate to High (emotional, and personal)Confidence: Low to Moderate
“I just need to quit smoking”• Dr. J: “If you were to try, what first steps would you take?”• Jeff: “I would keep the patches handy.”• Dr. J: “So you’d keep the Nicorette patches handy, in case you
felt the craving for a cigarette?”• Jeff: “Yes”• Dr. J: “What have you learned about your triggers or cues for
smoking? What are your high risk times and places?”• Jeff: “Usually after eating, for sure when I wake up, and when I
listen to classic rock music.” • Dr. J: “So you tend to get a craving to smoke when you wake
up in the morning, after meals, and when you listen to rock, so you’d be intentional about having a Nicoderm patch handy during those times, and would use one instead of smoking? Am I hearing you right?”
“I just need to quit smoking”• Dr. J: “What would your initial goal be?”• Jeff: “Maybe cutting back by 5 cigarettes per week.”• Dr. J: “So you’d cut down by 5 cigarettes per week, which
would mean that you would be off altogether in 3 weeks? Would that pace feel workable for you?”
• Jeff: “Yep, I think I can do that!”• Dr. J: “How about if we schedule our next appointment for
the week after you’ve gotten off cigarettes, and see how you’re doing? And could you email me at the end of each of the next two weeks to let me know how your plan is working?”
• Jeff: “Absolutely.”
Take Home Message
“ASK, DON’T TELL!”
Help others convince themselves of the need to change and own the strategy
they choose
Role PlayEvaluation• Determine the Stage• Determine the level of Conviction and level of Confidence
(target of intervention)Intervention (target)• For Conviction: provoke their perception of the advantages
(personal and emotional)• For Confidence: provoke identification of the barriers and
solutions
Start The Timer!
Questions to Determine:• Stage of Change: “What would you think
about…”• Conviction: “If you decided to… how would that
benefit you?”• Develop more personal and emotional conviction
• Confidence: “If you really decided to… do you think you could do it?”• Barriers: “What would prevent you from…?• Strategies: “How do you think you could start…?”
• Agreement on Action (if ready)
Let’s See Where We’ve Come
We started with…
When you meet a friend who…• Drinks too much, with no intention of quitting• Smokes a pack per day• Is obese• Doesn’t exercise• Has high blood pressure• But is unwilling to take your advice, change their lifestyle,
or comply with medication recommendations by their doctor
How do you feel?
How do you feel?• Sad…• Helpless• Scared• Irritated• Unsure of how to help• Defeated before I start
The Goal of This Session
Was to help you become more effective at facilitating real behavioral change in
yourself, your family, and your friends
How do you feel now?Do you feel more equipped?
Must practice this simple process until it becomes automatic…
until it becomes your way of being with your patients, peers, spouse, and kids
How To Engage Patients in Necessary Change:
A Dead Simple Roadmap
Robert R. Johnson, DOMedical Director, Amen Clinics
Diplomate, American Board of Addiction MedicineDiplomate, American Board of Psychiatry and Neurology