il$dolore$neoplastico$nei$secondarismi$ ossei$e ... · kaabencardino niguarda...
TRANSCRIPT

Ka#a Bencardino Niguarda Cancer Center, Grande Ospedale Metropolitano Niguarda, Milano, Italia
IL DOLORE NEOPLASTICO NEI SECONDARISMI OSSEI E SCRAMBLER THERAPY
Scrambler therapy
Scrambler Therapy is a non invasive neurocutaneous electrical pain intervention effective for the treatment of neuropathic pain It substitutes pain information with synthetic "non pain" information
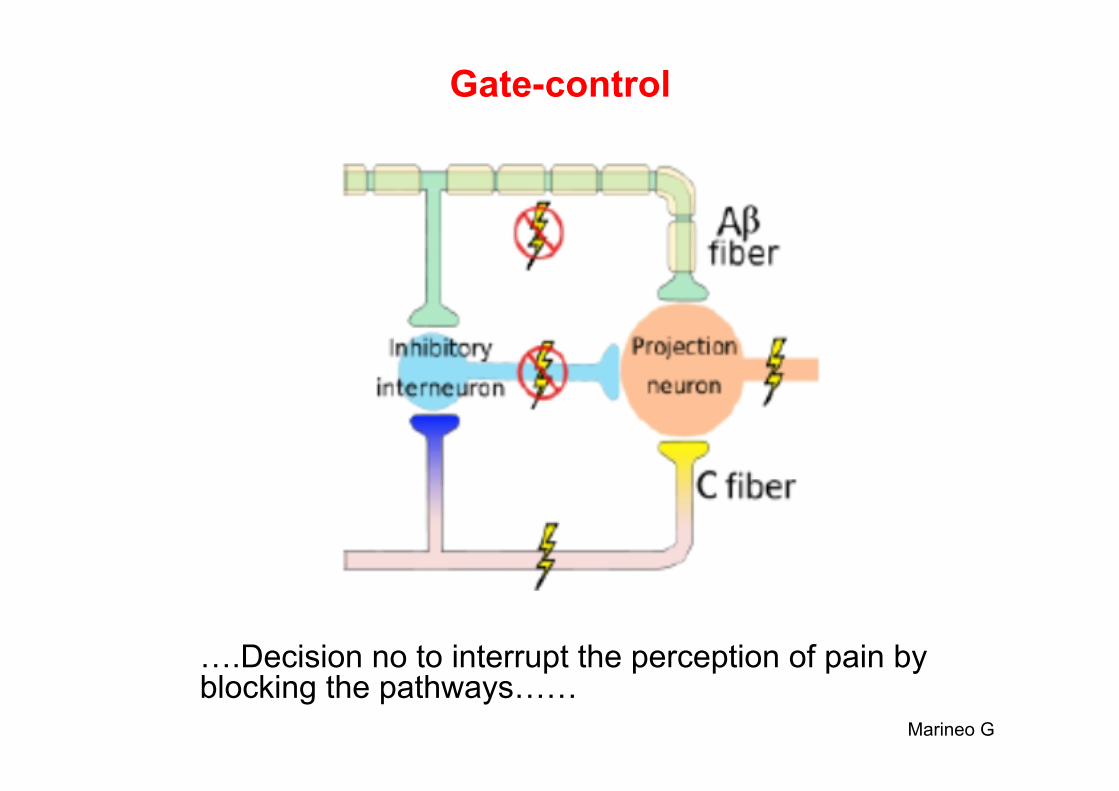
Gate-control
Marineo G
….Decision no to interrupt the perception of pain by blocking the pathways……
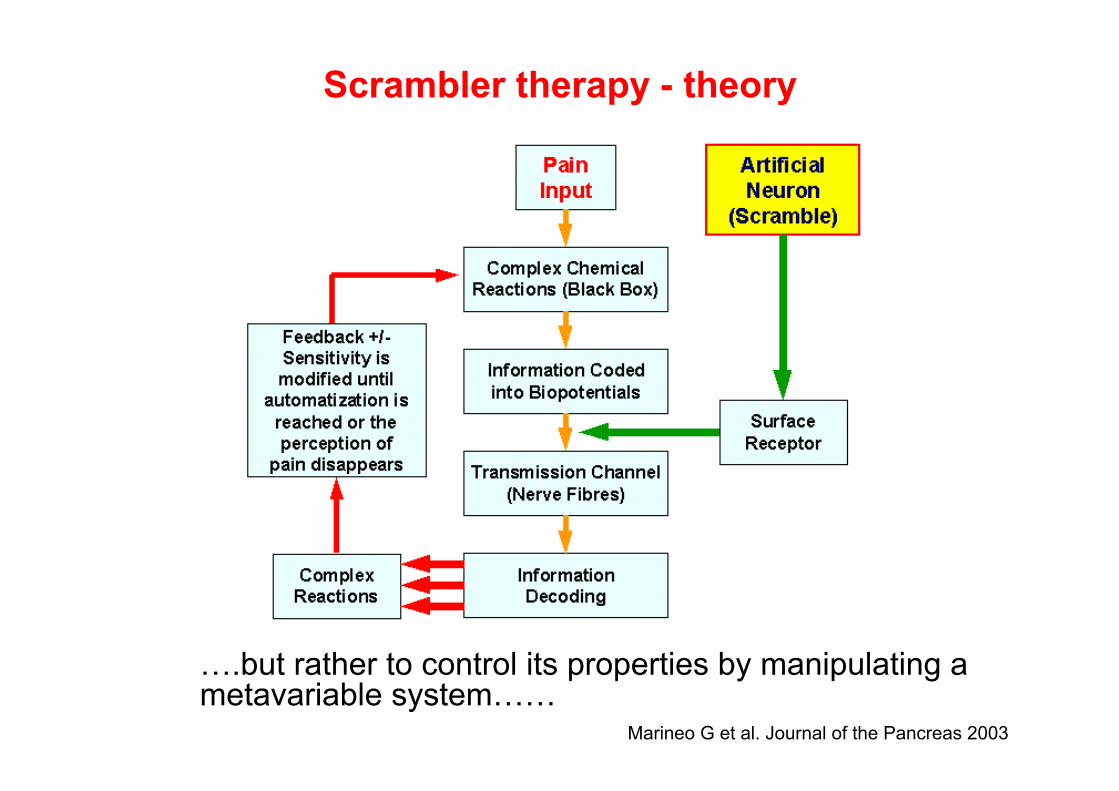
Scrambler therapy - theory
Marineo G et al. Journal of the Pancreas 2003
….but rather to control its properties by manipulating a metavariable system……
Scrambler therapy
• It consists on positioning electrodes bilaterally outside the pain area to the proximal and distant area and works converting a “pain” information in “non-pain” information via electrical stimulation to the central nerve system
• The intensity of the electrodes is set to the maximum value
at which the patient doesn’t feel discomfort • Frequency: 43 to 52 Hz • 10 daily sessions of 30-40 minutes • The efficacy can be evaluated with pain scale (VAS-visual
analogue scale, NRS-numerical rating scale)
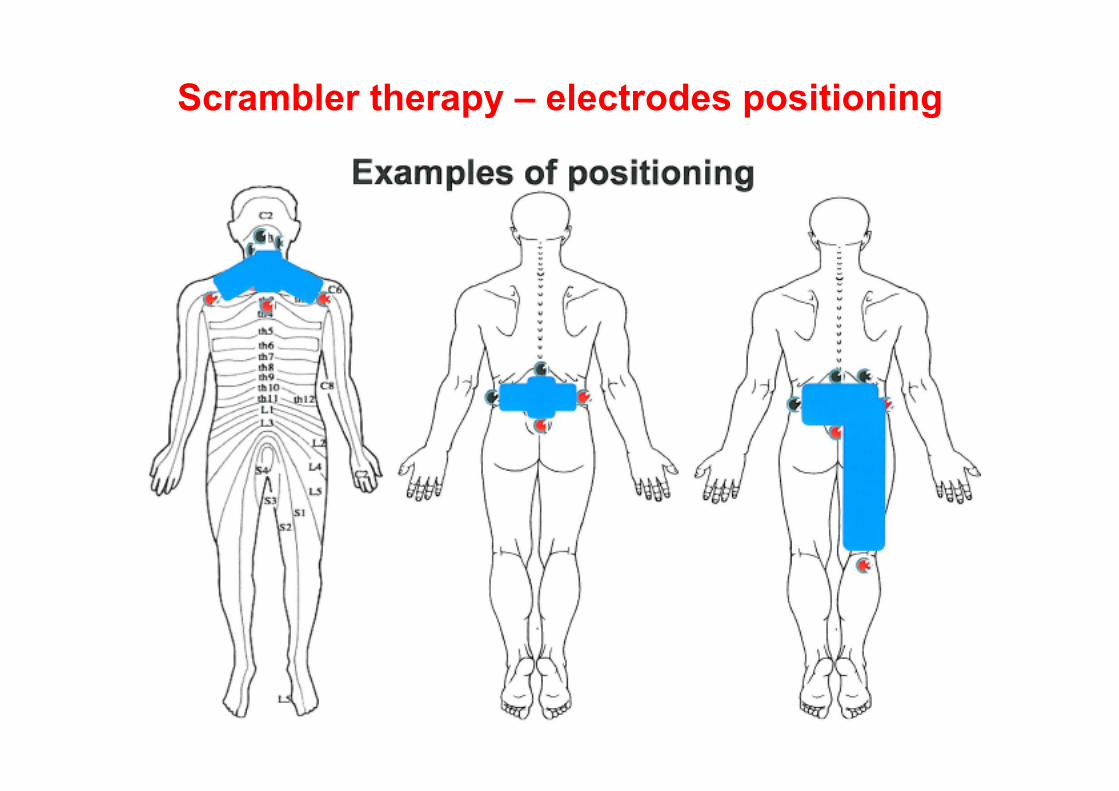
Scrambler therapy – electrodes positioning
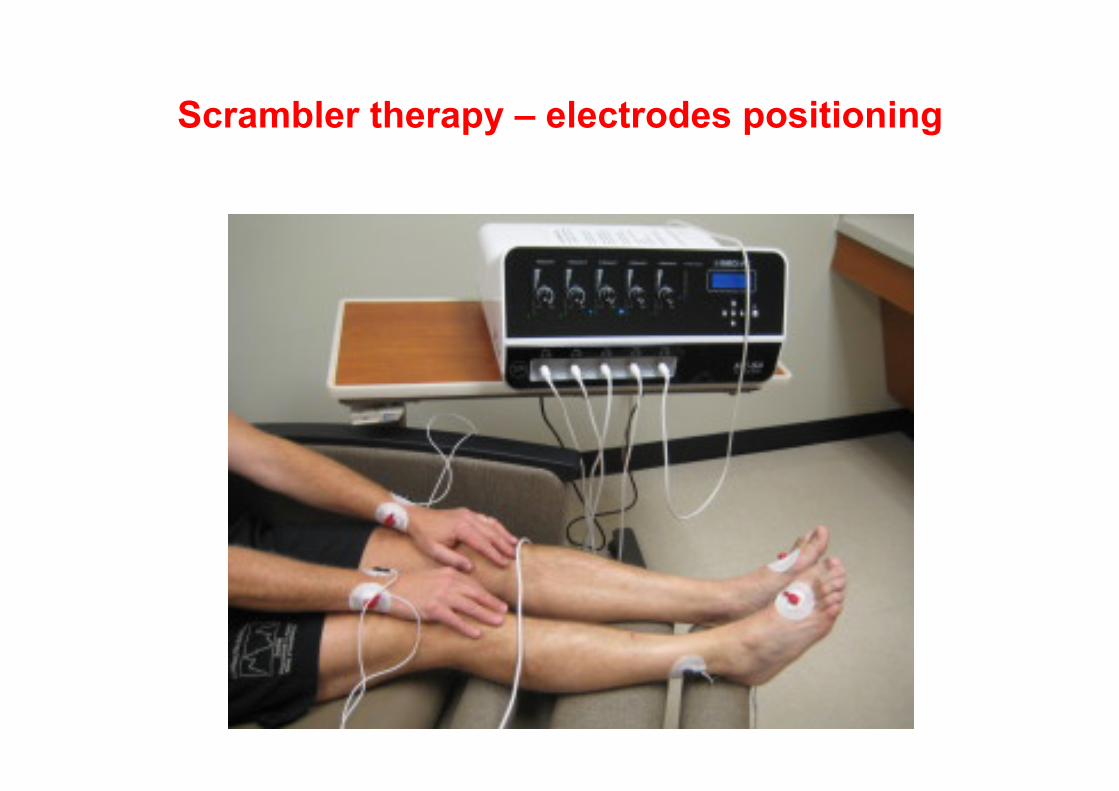
Scrambler therapy – electrodes positioning
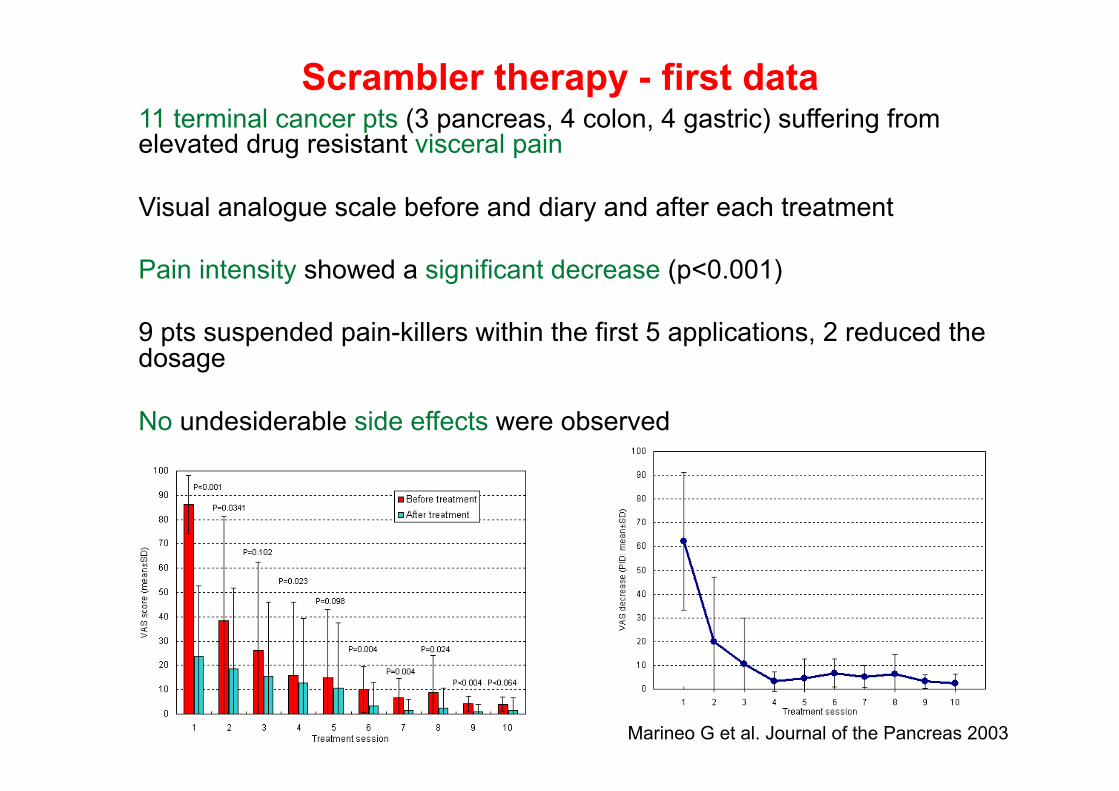
Scrambler therapy - first data
Marineo G et al. Journal of the Pancreas 2003
11 terminal cancer pts (3 pancreas, 4 colon, 4 gastric) suffering from elevated drug resistant visceral pain Visual analogue scale before and diary and after each treatment Pain intensity showed a significant decrease (p<0.001) 9 pts suspended pain-killers within the first 5 applications, 2 reduced the dosage No undesiderable side effects were observed
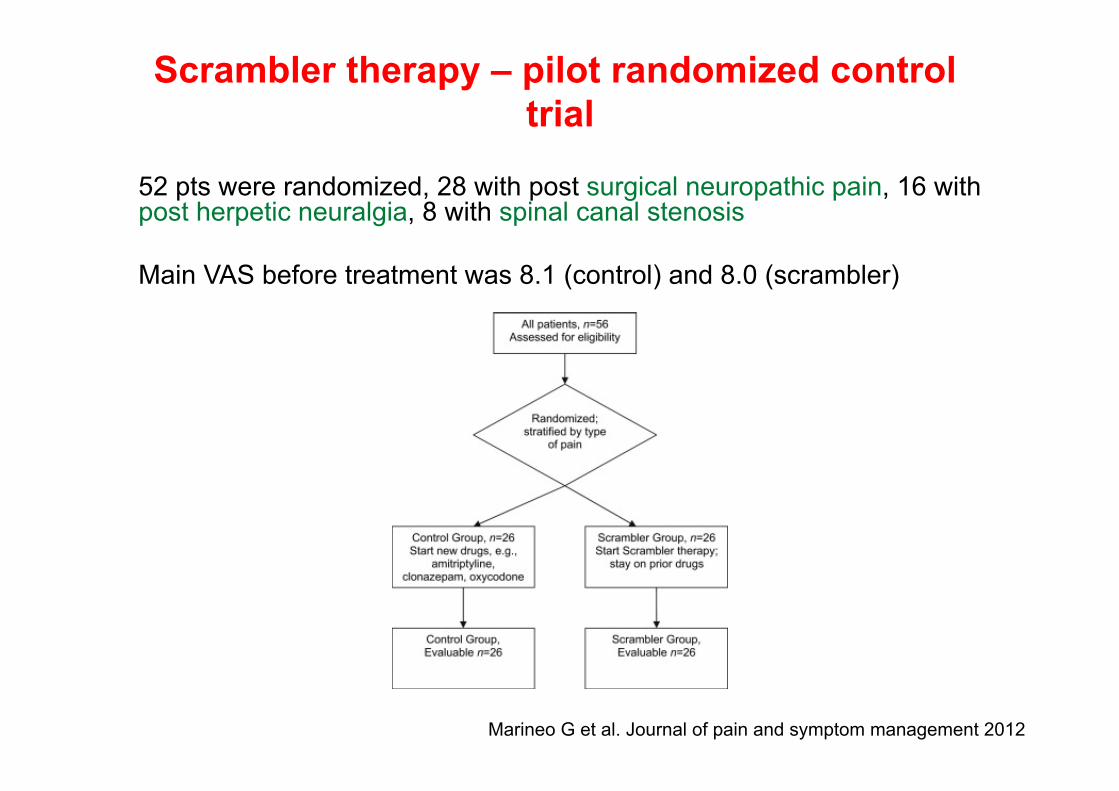
Scrambler therapy – pilot randomized control trial
Marineo G et al. Journal of pain and symptom management 2012
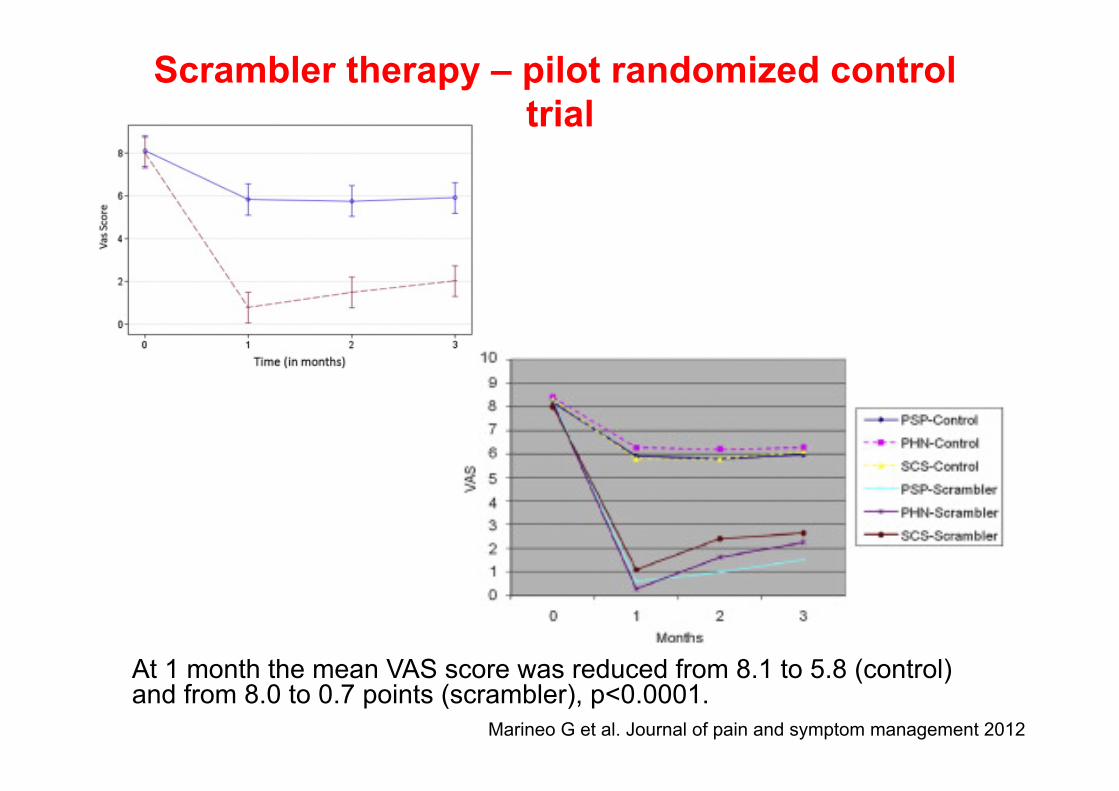
52 pts were randomized, 28 with post surgical neuropathic pain, 16 with post herpetic neuralgia, 8 with spinal canal stenosis Main VAS before treatment was 8.1 (control) and 8.0 (scrambler)
Scrambler therapy – pilot randomized control trial
Marineo G et al. Journal of pain and symptom management 2012
At 1 month the mean VAS score was reduced from 8.1 to 5.8 (control) and from 8.0 to 0.7 points (scrambler), p<0.0001.

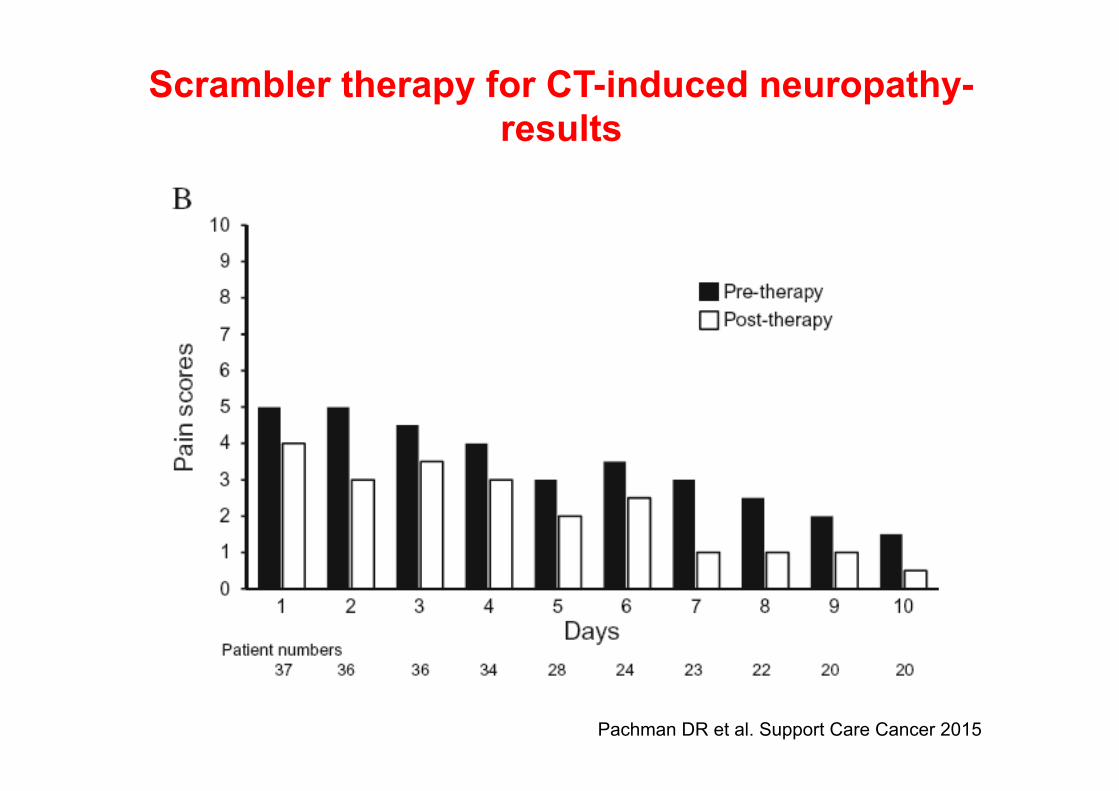
Pachman DR et al. Support Care Cancer 2015
Scrambler therapy for CT-induced neuropathy-
results
Scrambler therapy for CT-induced neuropathy
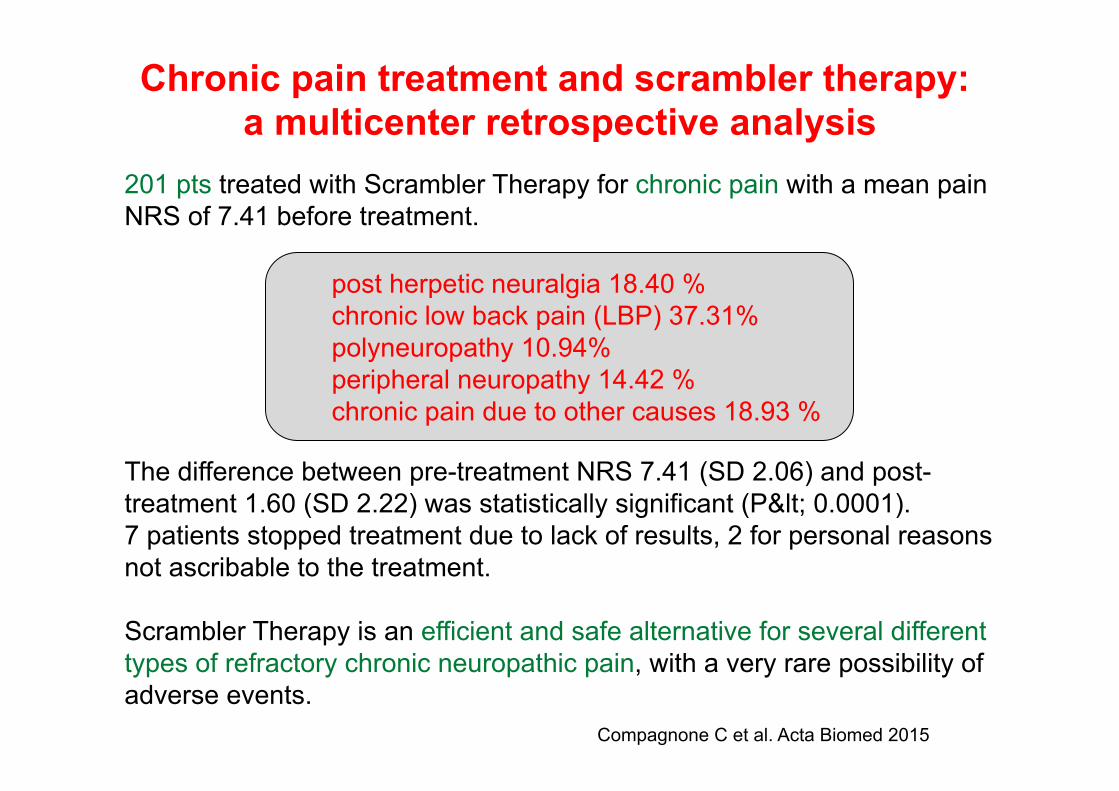
Chronic pain treatment and scrambler therapy: a multicenter retrospective analysis
Compagnone C et al. Acta Biomed 2015
201 pts treated with Scrambler Therapy for chronic pain with a mean pain NRS of 7.41 before treatment.
The difference between pre-treatment NRS 7.41 (SD 2.06) and post-treatment 1.60 (SD 2.22) was statistically significant (P< 0.0001). 7 patients stopped treatment due to lack of results, 2 for personal reasons not ascribable to the treatment. Scrambler Therapy is an efficient and safe alternative for several different types of refractory chronic neuropathic pain, with a very rare possibility of adverse events.
post herpetic neuralgia 18.40 % chronic low back pain (LBP) 37.31% polyneuropathy 10.94% peripheral neuropathy 14.42 % chronic pain due to other causes 18.93 %
2015
Scrambler therapy for cancer pain
• We investigated its efficacy in control of cancer pain that
failed the previous standard treatments, including pharmacological therapies and locoregional tratment, such as radiotherapy
• The efficacy was evaluated with pain numerical rating
scale (NRS), at baseline, before and after each treatment session

Patients’ characteristics Median age 61y (32-85y) Male/Female: 15 (60%)/10 (40%) 22 solid tumors (5 lung cancers, 5 colorectal cancers, 5 pancreatic cancers, 1 sarcoma, 3 urothelial carcinomas, 1 pharyngeal cancer, 1 prostatic cancer, 1 breast cancer) 3 hematologic malignancies (2 mieloma, 1 NHL) 17 (68%) with bone metastases (14 from solid tumors, 3 from hematologic malignancies) 5 with visceral metastases or primitive tumors (1 parapharingeal mass, 1 lung mass, 3 pancreatic cancer)
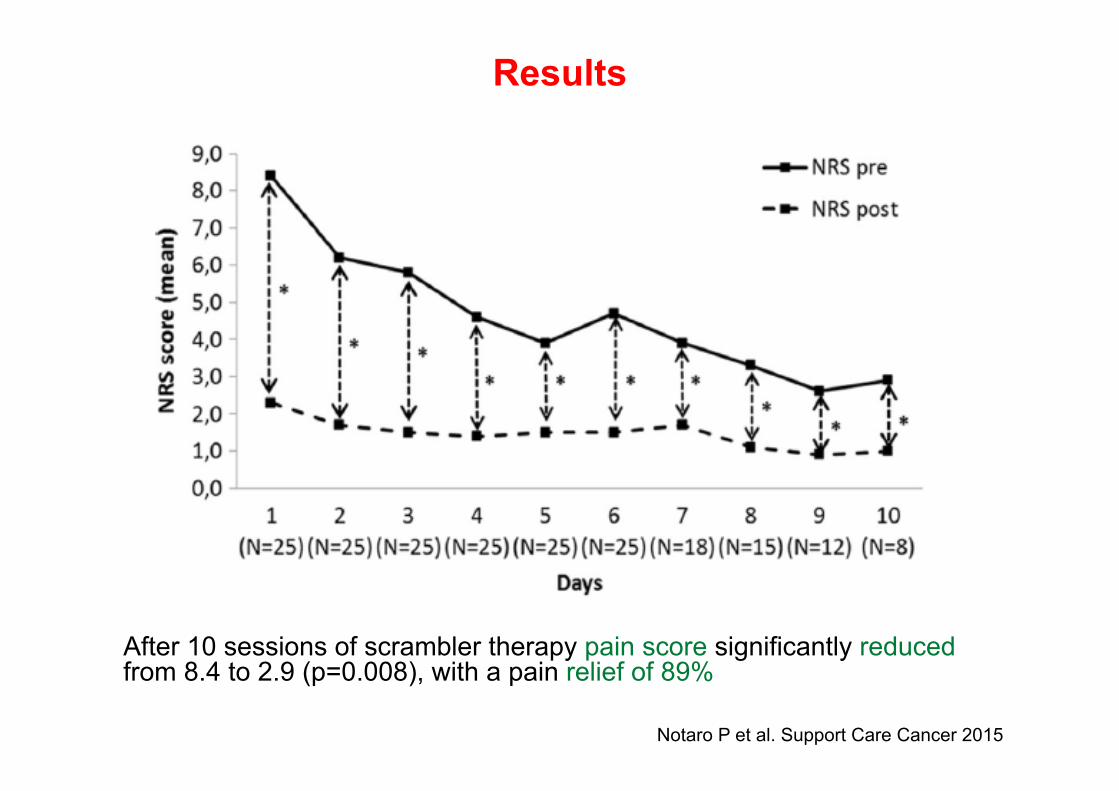
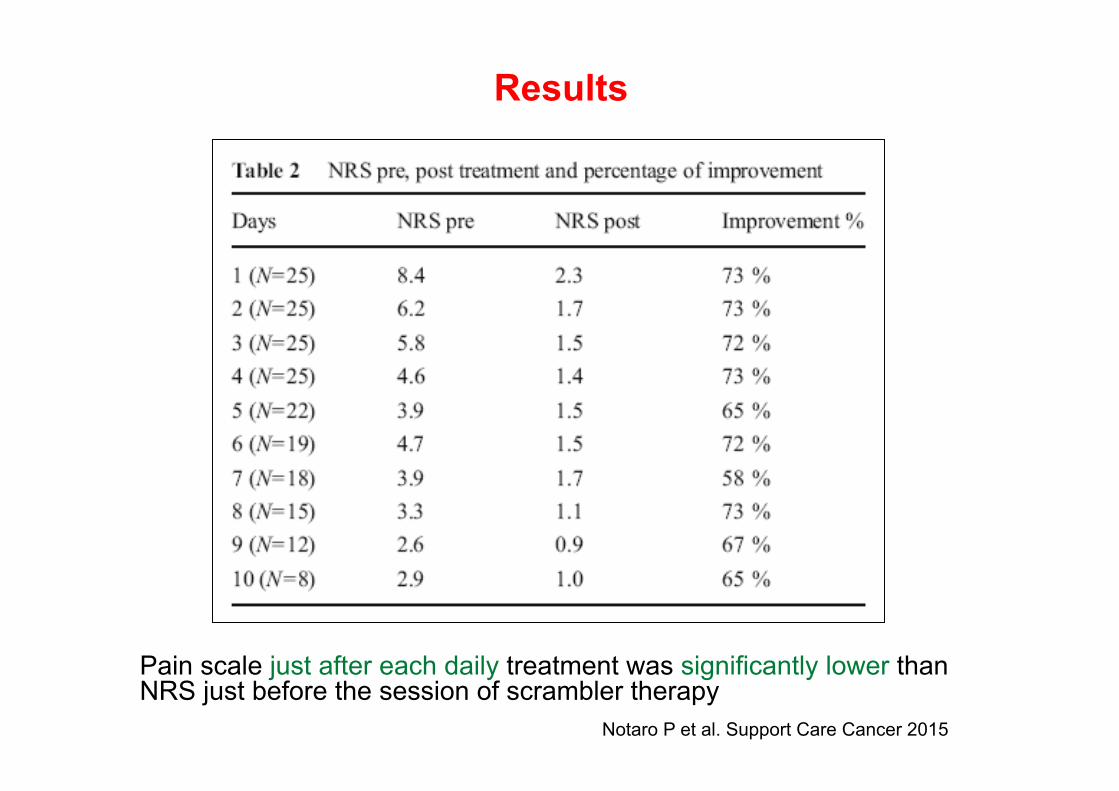
Results
After 10 sessions of scrambler therapy pain score significantly reduced from 8.4 to 2.9 (p=0.008), with a pain relief of 89%
Notaro P et al. Support Care Cancer 2015
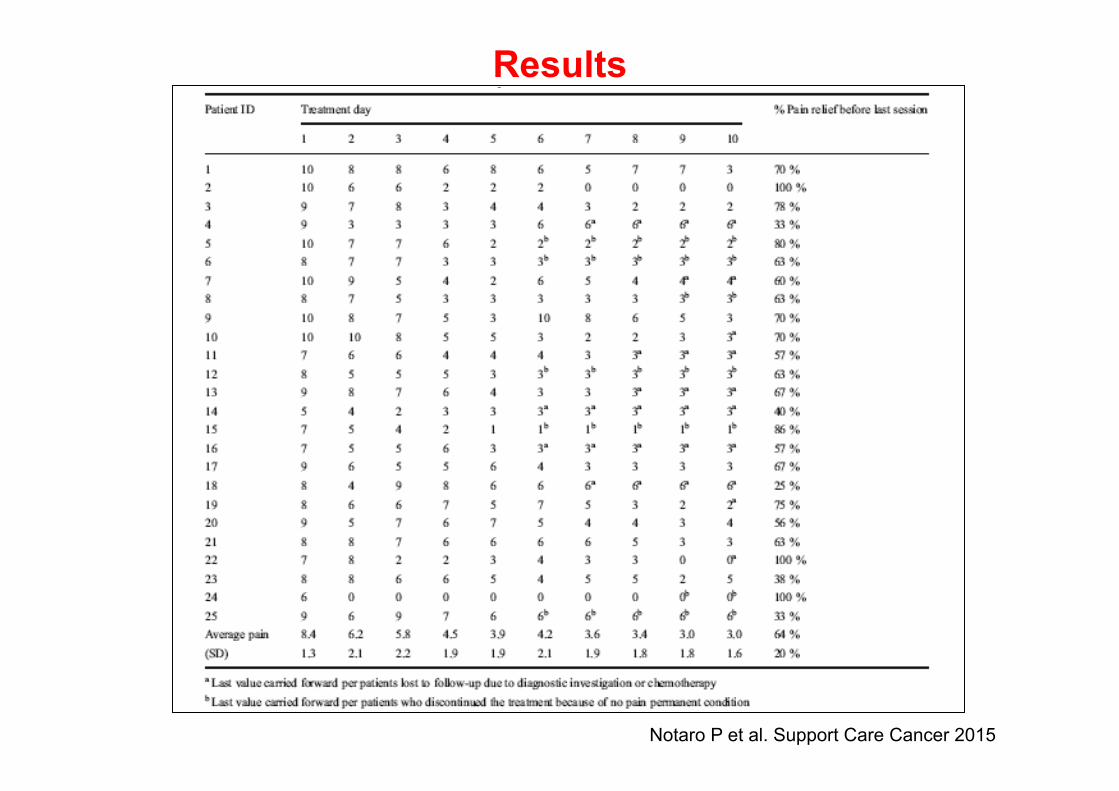
Results
Notaro P et al. Support Care Cancer 2015
Pain scale just after each daily treatment was significantly lower than NRS just before the session of scrambler therapy
Results
Notaro P et al. Support Care Cancer 2015
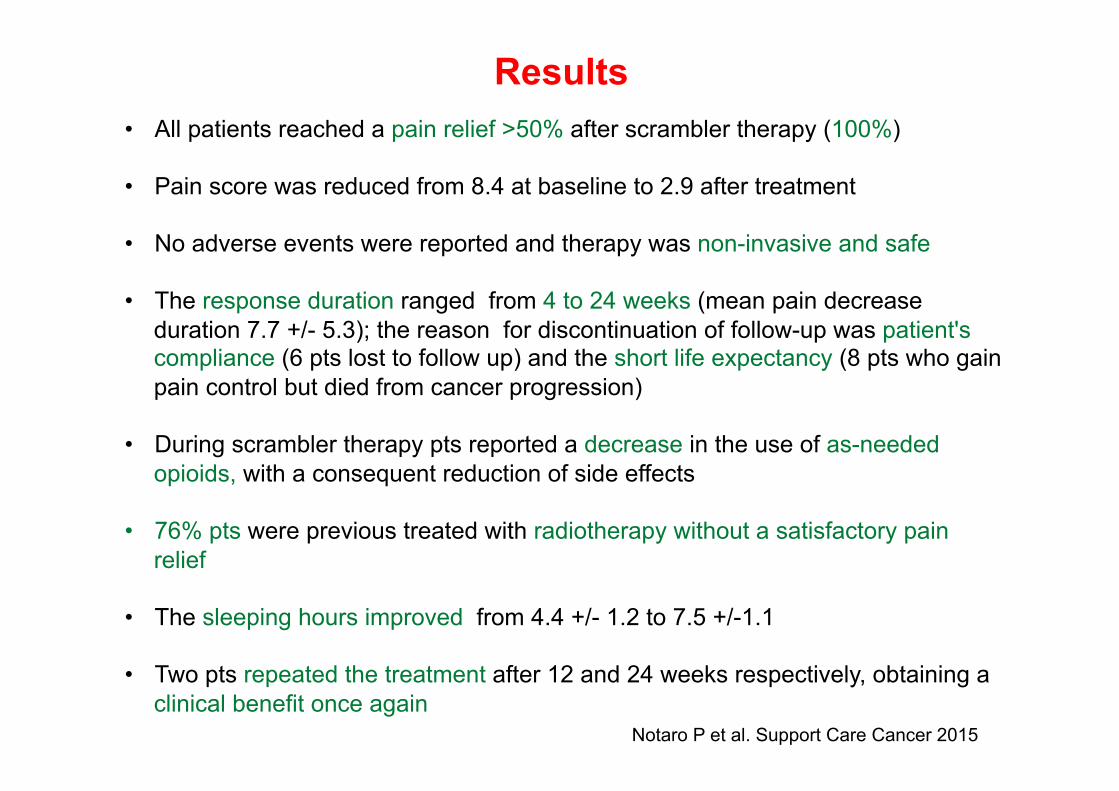
• All patients reached a pain relief >50% after scrambler therapy (100%)
• Pain score was reduced from 8.4 at baseline to 2.9 after treatment
• No adverse events were reported and therapy was non-invasive and safe
• The response duration ranged from 4 to 24 weeks (mean pain decrease duration 7.7 +/- 5.3); the reason for discontinuation of follow-up was patient's compliance (6 pts lost to follow up) and the short life expectancy (8 pts who gain pain control but died from cancer progression)
• During scrambler therapy pts reported a decrease in the use of as-needed opioids, with a consequent reduction of side effects
• 76% pts were previous treated with radiotherapy without a satisfactory pain relief
• The sleeping hours improved from 4.4 +/- 1.2 to 7.5 +/-1.1
• Two pts repeated the treatment after 12 and 24 weeks respectively, obtaining a clinical benefit once again
Results
Notaro P et al. Support Care Cancer 2015

Case Report (G.R.) • G.R. 06.05.1982 • April 2005: Surgery (RAR) for rectal adenocarcinoma pT3N2G2M0. KRAS mutation G12D. • May-July 2005: adjuvant chemoradiotherapy (c.i. 5-FU + RT). • July-December 2005: 6 courses of adjuvant chemotherapy with FOLFOX. Negative follow up until • July 2007: anastomotical relapse. Surgery (Miles rectal amputation and colostomy). • July 2007-January 2008: adjuvant CT with oral capecitabine. Negative follow up until • March 2010: paravaginal and lung metastases. • April-September 2010: 12 courses of CT with FOLFIRI + bevacizumab with PR. • October 2010-April 2011: 9 courses of maintenance therapy with capecitabine and bevacizumab. • May 2011: CT-scan: lung PD. 2 courses of FOLFOX, stopped for allergic reaction to oxaliplatin. • July-September 2011: 3 courses with Dacarbazine in DETECT trial. CT-scan: PD. • October 2011-March 2012: 9 courses of CT with FOLFIRI with SD. In december 2011 Radiotherapy on
left lung lesion (39 Gy + boost 7 Gy). • May 2012-October 2013: CT-scan (May 2012): lung PD. Therapy with Ragorafenib in Consign trial with
PR and SD. October 2012: pain on left inferior leg. MRI: metastasis of superior third of left thighbone. Radiotherapy on left thighbone (20 Gy in 5 fractions). Zometa. CT-scan (October 2013): PD. In september 2013 RT on paravaginal mass with benefit.
• October 2013-January 2014: 6 courses of CT with FUFA De Gramont. CT-scan (January 2014): PD. • January-July 2014: 9 courses of CT with FOLFOX with SD/initial PD.
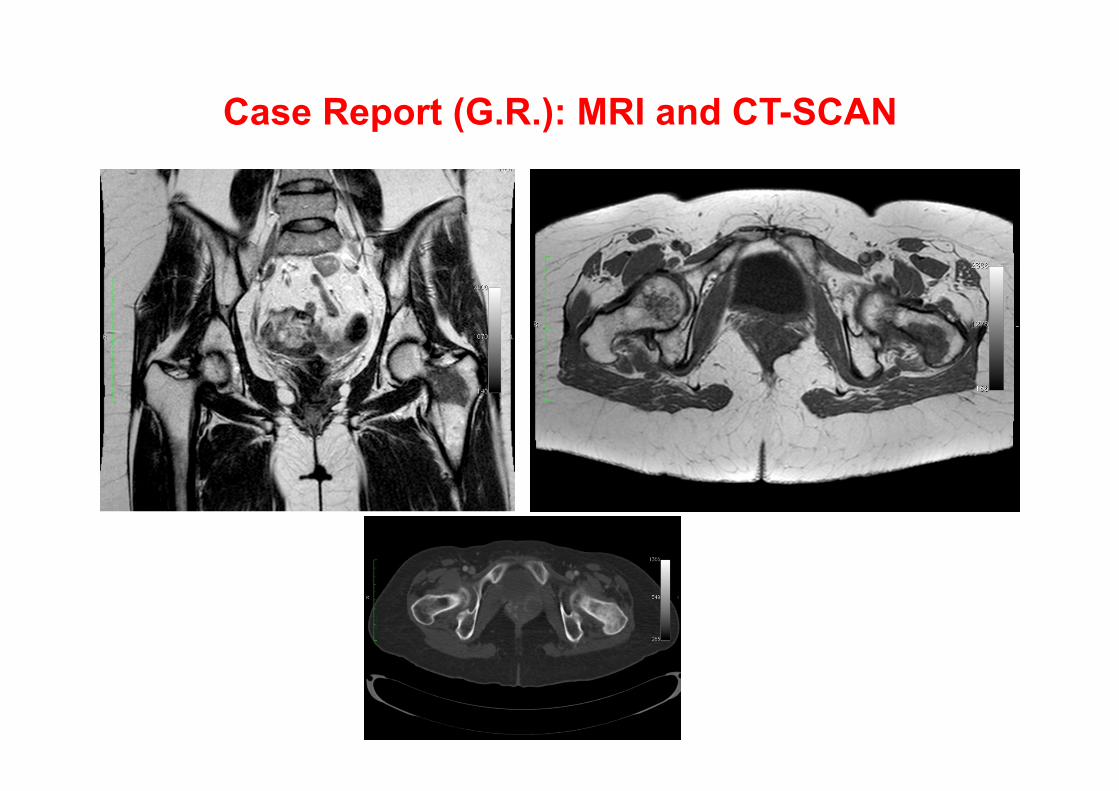
Case Report (G.R.): MRI and CT-SCAN
Case Report (G.R.)
• October 2012: pain on left inferior leg treated with opioids, fans and neuroleptic drugs (matrifen, oxycontin, abstral, depalgos, actiq, toradol, rivotril, lyrica) with poor benefit. MRI: metastasis of superior third of left thighbone. Radiotherapy on left thighbone (20 Gy in 5 fractions) with response. After 3 months from the end of RT pain recurrence.
• April 2013-February 2014: many modifications of analgesic drugs and locoregional injections with lidocaine and steroids for intense pain on inferior left leg. In May 2013 hospitalization for bowel obstruction due to constipation from opioids.
• February 2014: Scrambler therapy on left inferior leg (9 sessions) with immediate benefit (NRS 10 0). Improvement in quality of life (she was able to work standing for several hours).
• August 2014: pain recurrence on left inferior leg. Scrambler therapy on left inferior leg (10 sessions) with immediate benefit (NRS 10 0).
• November 2014: brain metastases. RT and best supportive care. • December 2014: death
Conclusions
• Non-invasive and safe technique • No side effects • High and fast responses • Repeatable technique • Useful choice in case of antalgic RT failure • Reduction of opioids use and relative side effects • Quality of life improvement • Limited duration of response due to advanced diseases • Treatment can be associated with medical oncologic therapy
(chemotherapy), without interfering with the oncologic program, unlike of RT
• The scrambler session can be applied both as outpatient and inpatient setting, potentially reducing the lengthening of hospitalization
Future directions
• Use of scrambler therapy in pts selected for site of disease (i.e. bone metastases, primitive pancreatic cancer) with a prospective randomized trial
• Use of scrambler therapy in pts with higher life
expectancy in order to detect the real duration of response

partnerships with big-‐, medium-‐, and small-‐size pharma
Laboratory of Cancer Genetics
Friday 20 April 2012
at 2.30 P.M. – Aula Cappa
““““Receptor trafficking and Receptor trafficking and Receptor trafficking and Receptor trafficking and
signaling:govsignaling:govsignaling:govsignaling:governance by ubiquitin and ernance by ubiquitin and ernance by ubiquitin and ernance by ubiquitin and
phosphorylation.phosphorylation.phosphorylation.phosphorylation.””””
Prof. Michael Clague
Cell Signaling Laboratory at the University of Liverpool, UK
Cancer Res UK
IRCC- Strada Provinciale 142, 10060 Candiolo-Torino-Italy www.ircc.it
Grazie per l’attenzione!