impact of a bronchiolitis guideline on ed resource...
TRANSCRIPT
Impact of a Bronchiolitis Guideline on ED ResourceUse and Cost: A Segmented Time-Series Analysis
abstractOBJECTIVE: Bronchiolitis is a major cause of infant morbidity and con-tributes to millions of dollars in health care costs. Care guidelines maycut costs by reducing unnecessary resource utilization. Through theimplementation of a guideline, we sought to reduce unnecessary re-source utilization and improve the value of care provided to infantswith bronchiolitis in a pediatric emergency department (ED).
METHODS: We conducted an interrupted time series that examined EDvisits of 2929 patients with bronchiolitis, aged 1 to 12 months old, seenbetween November 2007 and April 2013. Outcomes were proportionhaving a chest radiograph (CXR), respiratory syncytial virus (RSV) test-ing, albuterol or antibiotic administration, and the total cost of care.Balancing measures included admission rate, returns to the ED result-ing in admission within 72 hours of discharge, and ED length of stay(LOS).
RESULTS: There were no significant preexisting trends in the outcomes.After guideline implementation, there was an absolute reduction of23% in CXR (95% confidence interval [CI]: 11% to 34%), 11% in RSVtesting (95% CI: 6% to 17%), 7% in albuterol use (95% CI: 0.2% to13%), and 41 minutes in ED LOS (95% CI: 16 to 65 minutes). Mean costper patient was reduced by $197 (95% CI: $136 to $259). Total costsavings was $196 409 (95% CI: $135 592 to $258 223) over the 2 bronchi-olitis seasons after guideline implementation. There were no significantdifferences in antibiotic use, admission rates, or returns resulting inadmission within 72 hours of discharge.
CONCLUSIONS: A bronchiolitis guideline was associated with reduc-tions in CXR, RSV testing, albuterol use, ED LOS, and total costs in a pe-diatric ED. Pediatrics 2014;133:e227–e234
AUTHORS: Ayobami T. Akenroye, MBChB, MPH,a,b Marc N.Baskin, MD,a,b Mihail Samnaliev, PhD,b,c and Anne M. Stack,MDa,b
aDivision of Emergency Medicine and cClinical ResearchProgram, Boston Children’s Hospital, Boston, Massachusetts; andbDepartment of Pediatrics, Harvard Medical School, Boston,Massachusetts
KEY WORDSbronchiolitis, guidelines, pediatric emergency, resourceutilization, costs
ABBREVIATIONSAAP—American Academy of PediatricsCI—confidence intervalCXR—chest radiographED—emergency departmentLOS—length of stayQI—quality improvementRSV—respiratory syncytial virus
Dr Akenroye was involved in the conceptualization of the study,development of the initial study design, data analyses, anddrafted the initial manuscript; Dr Baskin was involved in thedevelopment of the final study design, contributed to theinterpretation of the data, and provided critical revisions of themanuscript; Dr Samnaliev was involved in the development ofthe final study design and data analyses, retrieved the financialdata, and provided critical revisions of the manuscript; Dr Stackwas involved in the conceptualization of the study anddevelopment of the initial study design, contributed to theinterpretation of the data, and provided critical revisions of themanuscript; and all authors approved the final manuscript assubmitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1991
doi:10.1542/peds.2013-1991
Accepted for publication Sep 30, 2013
Address correspondence to Ayobami Akenroye, MBChB, MPH,Division of Emergency Medicine, Boston Children’s Hospital, 300Longwood Ave, Boston, MA 02115. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: This study was supported by the Boston Children’sHospital Department of Medicine Quality ImprovementPublication (QIPub) grant.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
PEDIATRICS Volume 133, Number 1, January 2014 e227
QUALITY REPORT
by guest on August 30, 2018www.aappublications.org/newsDownloaded from

Bronchiolitis is a major reason for am-bulatory visits and hospitalizations inpatients,2 years old.1–3 It is 1 of the top10 emergency department (ED) diag-noses during the late fall and winter.Viral bronchiolitis, although self-limitedwith testing and/or therapies offeringlittle or no benefit for most healthyinfants, contributes to millions of dol-lars in annual health care costs.2,4–10
Thehighcostofhealthcare in theUnitedStates, currently .17% of gross do-mestic product, continues to promoteextensive discussion among policymakers, payers, health care providers,and consumers.11,12 Evidence suggeststhat .30% of health care utilization isunnecessary and avoidable and in-cludes frequent overuse of screening ordiagnostic services.12,13 Whereas manyapproaches have been suggested torein in health care costs, reduction inthe use of unnecessary services hasbeen a recurring theme14. However, toidentify what services are unnecessary,and to avoid the potential problem ofreducing the quality of medical carewhile reducing costs, it is importantthat providers are equipped with theright evidence based on well-executedresearch. Care guidelines provide away of integrating best-available knowl-edge into a concise format and maymake it easier for individual providersto use best practices.
In 2006, the American Academy of Pe-diatrics (AAP) bronchiolitis guidelinewas introduced to aid clinician decision-making in the management of patientswith bronchiolitis.2 Despite publicationof the guideline, many studies acrossthe United States,10,15–19 have shownwide variation in resource utilizationand ED management of patients withbronchiolitis.
Through internal quality assuranceefforts, we found wide variation acrossproviders in the management of bron-chiolitis. To improve the management ofpatients with bronchiolitis in our setting,
we adapted the AAP recommendationsand implemented a bronchiolitis guide-line. We hypothesized that adherence toa well-implemented guideline would re-sult in reductions in resource utilizationand costs without a worsening of otheroutcomes.
METHODS
The study was approved by the hospi-tal’s institutional review board. An in-formed consent waiver was obtainedfor a quality improvement (QI) study.Data were deidentified and presentedon the aggregate level.
Study Design and Setting
This was a retrospective study of a QIintervention to standardize care forpatients with bronchiolitis. The settingwas the ED of a tertiary, university-affiliated pediatric hospital with 60000 annual visits. ED providers consistof 48 board-certified pediatric emer-gency medicine physicians, 26 generalpediatricians, up to 100 registerednurses or nurse practitioners, and.200 rotating residents and fellows.
Intervention
Description of the Guideline
Due to the variation and potential forimproved efficiency in themanagementof patients with bronchiolitis, a guide-line was developed. The guideline wasdeveloped by a team chaired by a pe-diatric emergency physician and nurseand occurred over the 9-month periodfrom October 2010 to June 2011.Implementation occurred at the start ofthe bronchiolitis season in November2011. Through an iterative process,early versions were evaluated by 5pediatric emergency medicine attend-ing physicians with a mean of 12 yearsof experience after subspecialty train-ing. The nurse provided support forinclusion of nursing-sensitive mea-sures. The major recommendations,
adapted fromtheAAPguideline,wereasfollows: no routine viral testing, chestradiograph (CXR), and albuterol orantibiotic administration. A trial ofbronchodilator to assess for effect wasan option.
Implementation of the Guideline
Implementation was led by the EDGuideline Implementation Team, madeup of 7 individuals: 2 physicians, 2nurses, a QI expert, a data analyst, andan administrator. Before implementa-tion, electronic order set and dischargeinstructions were created. In line withthe Pathman model,20 the goals of im-plementation were to stimulate aware-ness of the guideline, promote agreementwith recommendations, improve adop-tion, and support adherence. We usedmultifaceted strategies, which includedthe following:
� Guideline introduction and discus-sion of major recommendations atweekly division conference. At thiswell-attended conference, providerswere allowed to openly agree ordisagree with recommendations.The evidence supporting the guide-line recommendations was dis-cussed extensively.
� E-mail to ED providers highlightingthe major recommendations witha copy of the guideline algorithmattached.
� Display of copies of the algorithmin the ED charting area. Laminatedcopies of the algorithm and onlinecopies were also available.
� Monthly monitoring of performanceon the major recommendationswith the use of control charts.These were shared with the clinicalchief of the department, the nursemanager, and the guideline physi-cian and nurse leader. Controlcharts were shared at staff meet-ings every 2 to 3 months. Boosterdoses of reinforcement were sentto providers as appropriate.
e228 AKENROYE et al by guest on August 30, 2018www.aappublications.org/newsDownloaded from

� Annual feedback from the DivisionChief to individual attending physi-cians on their compliance with themajor recommendations. As partof this confidential report, individ-ual physicians were also able tocompare their performance with(deidentified) peers.
Other strategies included the use ofa pocket pamphlet outlining majorrecommendations, posters (eg, in-forming providers of the cost of a re-spiratory syncytial virus [RSV] test),graphical display of performance in theED conference room, and one-on-onediscussions with providers.
Data Collection
Eligible patientswere infants between 1and 12 months of age with a primarydiagnosis of bronchiolitis (InternationalClassification of Diseases, Ninth Re-vision, code 466.11 or 466.19) seen in theED during the months of Novemberthrough April 2007–2013. Patients werestudied during 6-month period becausethis is the peak bronchiolitis seasonin North America.21 The bronchiolitisguideline (Supplemental Fig 2) directedproviders in making a clinical diagnosisof bronchiolitis as well as indicatingpatients who should be excluded. Allpatients who presented to the ED wereeligible regardless of disposition at ini-tial visit. Data on utilization of resources,cost of services, and length of stay wereobtained from the administrative andfinancial databases of the hospital. Thehospital’s costing system integrates fi-nancial, clinical, and administrative in-formation and uses either internallydeveloped or industry-derived RelativeValue Units to accurately assign thecosts to individual procedures and ac-tivities. Total costs, in 2012 dollars, in-clude the cost of clinical care and thecost of supplies and materials (eg, thecosts of diagnostic tests, medications,and procedures and the cost of the EDvisit if discharged from the hospital and
the ED visit and inpatient costs if ad-mitted). We modeled the change in thetotal costs associated with the entireepisode of care to capture the overallimpact of the guideline.
Our primary outcomes, chosen a priori,were rates of CXR, RSV testing, admin-istration of antibiotic or albuterol, andtotal costof care.Albuterolwasbilledbydose (eg, a patient nebulized twice wasbilled for 2units). RSV tests includeboththepoint-of-care test and the laboratorydirect fluorescent antigen test. Balanc-ing measures, to identify unintendedconsequences of the guideline, wererates of admission at initial visit, returnED visit resulting in admission within 72hours of discharge, mortality rate, andthe ED length of stay (LOS). We did notdefine a clinically relevant change in theoutcome variables. Because the AAPrecommends against obtaining thesetests or prescribing albuterol and anti-biotics routinely, we considered anystatistically significant change in theprimary outcomes as a relevant change.For the balancing measures, we lookedfor a steadiness in these rates frompre– to post–guideline implementation.
Data Analysis and StatisticalMethods
Segmented regression analysis of inter-rupted time series was conducted toassess the impact of the bronchiolitisguideline. The model compares the pre-intervention with the postinterventionrates while accounting for preexistingtrends, the preintervention rates of theseoutcomes, and the magnitude of the de-crease. We adjusted for the followingcovariates: age, gender, race and eth-nicity, oxygen saturation, initial temper-ature, and disposition.
For all outcomes, the mean monthlyrates were modeled, with the exceptionof ED LOS for which the median wasmodeled due to its skewed distribution.Serial autocorrelation between errorterms was assessed by using the
Durbin-Watson statistic, and the Prais-Winsten transformation was appliedto adjust for first-order autocorrelationwhen evidence of autocorrelation wasfound. Stationarity of segments (inwhich trends are stable over a givenperiod) were assessed by using theaugmented Dickey-Fuller test.22,23
Cost savings after implementation ofthe guideline were estimated by mul-tiplying the average cost saved perpatient by the total number of patientsseen. We conducted subgroup analysesfor patients who were admitted com-pared with those who were not. Be-cause the estimated effects of theguideline on all outcomes and costswere in the same direction and ofsimilar magnitude, only the aggregateresults are presented. Analyses wereconducted in Stata version 12 (Stata-Corp, College Station, TX).
RESULTS
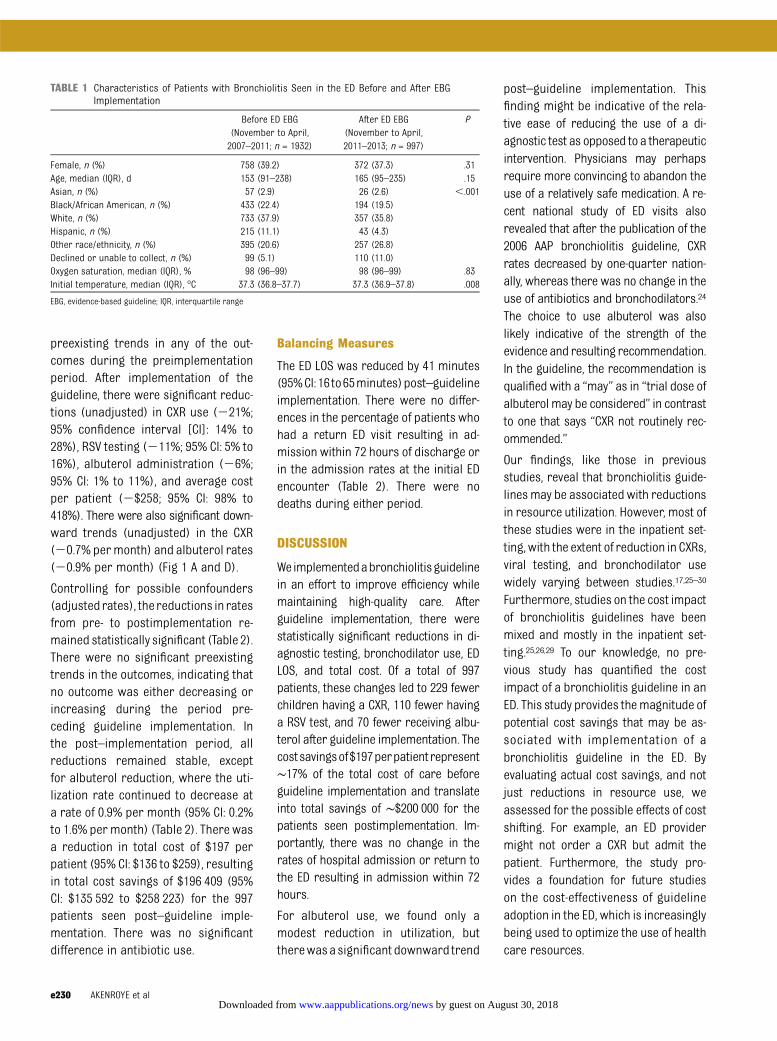
A total of 2929 patients with bronchio-litis were treated in the ED during the 6seasons studied (4 seasons pre– and 2seasons post–guideline implementa-tion). The groups of patients seenduring both periods were similar inbaseline characteristics, with the ex-ception of race and ethnicity and initialtriage temperature. Before guidelineimplementation, more than one-quarterof patients were categorized as having“other race/ethnicity.” We, however, be-lieve this difference is reflective of cod-ing adjustments in race/ethnicity options.The difference in temperature betweenthe patients seen before and afterguideline implementation, althoughstatistically significant, was not clini-cally meaningful (Table 1).
Primary Outcomes
The unadjusted rates of CXR use, RSVtesting, albuterol or antibiotic admin-istration, and average cost per patientduring the study periods are shown inFig 1 A–E. There were no significant
QUALITY REPORT
PEDIATRICS Volume 133, Number 1, January 2014 e229 by guest on August 30, 2018www.aappublications.org/newsDownloaded from
preexisting trends in any of the out-comes during the preimplementationperiod. After implementation of theguideline, there were significant reduc-tions (unadjusted) in CXR use (221%;95% confidence interval [CI]: 14% to28%), RSV testing (211%; 95% CI: 5% to16%), albuterol administration (26%;95% CI: 1% to 11%), and average costper patient (2$258; 95% CI: 98% to418%). There were also significant down-ward trends (unadjusted) in the CXR(20.7% permonth) and albuterol rates(20.9% per month) (Fig 1 A and D).
Controlling for possible confounders(adjustedrates), the reductions in ratesfrom pre- to postimplementation re-mained statistically significant (Table 2).There were no significant preexistingtrends in the outcomes, indicating thatno outcome was either decreasing orincreasing during the period pre-ceding guideline implementation. Inthe post–implementation period, allreductions remained stable, exceptfor albuterol reduction, where the uti-lization rate continued to decrease ata rate of 0.9% per month (95% CI: 0.2%to 1.6% permonth) (Table 2). There wasa reduction in total cost of $197 perpatient (95% CI: $136 to $259), resultingin total cost savings of $196 409 (95%CI: $135 592 to $258 223) for the 997patients seen post–guideline imple-mentation. There was no significantdifference in antibiotic use.
Balancing Measures
The ED LOS was reduced by 41 minutes(95%CI:16to65minutes)post–guidelineimplementation. There were no differ-ences in the percentage of patients whohad a return ED visit resulting in ad-mission within 72 hours of discharge orin the admission rates at the initial EDencounter (Table 2). There were nodeaths during either period.
DISCUSSION
Weimplementedabronchiolitisguidelinein an effort to improve efficiency whilemaintaining high-quality care. Afterguideline implementation, there werestatistically significant reductions in di-agnostic testing, bronchodilator use, EDLOS, and total cost. Of a total of 997patients, these changes led to 229 fewerchildren having a CXR, 110 fewer havinga RSV test, and 70 fewer receiving albu-terol after guideline implementation. Thecostsavingsof$197perpatientrepresent∼17% of the total cost of care beforeguideline implementation and translateinto total savings of ∼$200 000 for thepatients seen postimplementation. Im-portantly, there was no change in therates of hospital admission or return tothe ED resulting in admission within 72hours.
For albuterol use, we found only amodest reduction in utilization, buttherewasasignificant downward trend
post–guideline implementation. Thisfinding might be indicative of the rela-tive ease of reducing the use of a di-agnostic test as opposed to a therapeuticintervention. Physicians may perhapsrequire more convincing to abandon theuse of a relatively safe medication. A re-cent national study of ED visits alsorevealed that after the publication of the2006 AAP bronchiolitis guideline, CXRrates decreased by one-quarter nation-ally, whereas there was no change in theuse of antibiotics and bronchodilators.24
The choice to use albuterol was alsolikely indicative of the strength of theevidence and resulting recommendation.In the guideline, the recommendation isqualified with a “may” as in “trial dose ofalbuterol may be considered” in contrastto one that says “CXR not routinely rec-ommended.”
Our findings, like those in previousstudies, reveal that bronchiolitis guide-linesmay be associated with reductionsin resource utilization. However, most ofthese studies were in the inpatient set-ting,with the extent of reduction in CXRs,viral testing, and bronchodilator usewidely varying between studies.17,25–30
Furthermore, studies on the cost impactof bronchiolitis guidelines have beenmixed and mostly in the inpatient set-ting.25,26,29 To our knowledge, no pre-vious study has quantified the costimpact of a bronchiolitis guideline in anED. This study provides themagnitude ofpotential cost savings that may be as-sociated with implementation of abronchiolitis guideline in the ED. Byevaluating actual cost savings, and notjust reductions in resource use, weassessed for the possible effects of costshifting. For example, an ED providermight not order a CXR but admit thepatient. Furthermore, the study pro-vides a foundation for future studieson the cost-effectiveness of guidelineadoption in the ED, which is increasinglybeing used to optimize the use of healthcare resources.
TABLE 1 Characteristics of Patients with Bronchiolitis Seen in the ED Before and After EBGImplementation
Before ED EBG(November to April,2007–2011; n = 1932)
After ED EBG(November to April,2011–2013; n = 997)
P
Female, n (%) 758 (39.2) 372 (37.3) .31Age, median (IQR), d 153 (91–238) 165 (95–235) .15Asian, n (%) 57 (2.9) 26 (2.6) ,.001Black/African American, n (%) 433 (22.4) 194 (19.5)White, n (%) 733 (37.9) 357 (35.8)Hispanic, n (%) 215 (11.1) 43 (4.3)Other race/ethnicity, n (%) 395 (20.6) 257 (26.8)Declined or unable to collect, n (%) 99 (5.1) 110 (11.0)Oxygen saturation, median (IQR), % 98 (96–99) 98 (96–99) .83Initial temperature, median (IQR), °C 37.3 (36.8–37.7) 37.3 (36.9–37.8) .008
EBG, evidence-based guideline; IQR, interquartile range
e230 AKENROYE et al by guest on August 30, 2018www.aappublications.org/newsDownloaded from

Previous studies have shown thatguideline adoption is usually slower andmore challenging in outpatient com-pared with inpatient settings.31,32 We
believe the speed of adoption of theguideline recommendations after im-plementation and the sustainability ofimprovements in our ED are probably
indicative of the robustness of ourimplementation strategy. Despite simi-lar ED volumes during both periods, EDLOS also decreased by 41 minutes. One
FIGURE 1Utilization of CXR (A), RSV testing (B), antibiotics (C), and albuterol (D) andaverage cost perpatient (E). Vertical reddashed lines represent thepoint atwhich thebronchiolitis guideline was implemented. The x axis shows the 6 seasons studied (November to April 2007–2013). Labels for alternate monthswere eliminatedfor better display.
QUALITY REPORT
PEDIATRICS Volume 133, Number 1, January 2014 e231 by guest on August 30, 2018www.aappublications.org/newsDownloaded from

reason for the reduction in LOS couldbe avoidance of the delay associatedwith the testing or therapy, such as theavoidance of the wait to have a CXRperformed and evaluated.
Our findingsmust be viewed in the lightofseveral limitations.First, this isasingle-center studyandothercontextual factorsmight have aided successful implemen-tation. However, our implementationstrategies are clear and could be easilytranslated to other EDs. Second, althoughinterrupted time-series analyses areconsidered a strong quasi-experimentaldesign,22 changes occurring at thesame time as the bronchiolitis guidelinecould have affected our outcomes. How-ever, to our knowledge, there were nointerventions that could have accountedfor the magnitude and consistency inchange across these outcomes. Third,we did not perform chart reviews toidentify patients with significant comor-bidities or instances when the utilizationof the tests or therapieswas justified. Werealize that bronchiolitis is a heteroge-neous disease with different viral causesand a subset of patients may have be-nefited from further testing and/ortherapies: for instance, patients withhuman rhinovirus–associated bronchio-litis have been shown to have a differentclinical course33 and may convey ahigher risk of childhood asthma34–36
than those with RSV-induced bronchioli-tis. These patients could therefore ben-efit from further testing. However, we donot expect the percentage of instanceswhen these tests were justified to havechanged significantly from pre– to post–guideline implementation given the sim-ilar patient populations as well as themultivariate adjustment for patient-levelcovariates. Fourth, we do not account forthe initial costs of developing or imple-menting the guideline. However, thesewere relatively small and entirely in kind.Finally, we rely on only a few quantifiablebalancing measures. Health care qualitymay have been affected in otherways notcaptured in this evaluation. For instance,patients may have presented to anotherhospital for a return visit.
The cost savings, although they appear tobe associated with the specific guidelinerecommendations, may be indirectlylinked to reductions in additional re-source utilization. For example, patientswho have a CXR may be more likely toreceive additional therapies such asantibioticsduetofindingsontheCXRsthatmaybemorerepresentativeofatelectasisthan bacterial pneumonia.2,5,37,38 Reduc-tion in unnecessary utilization maytherefore have an impact far beyond thedirect savings from the specific resource.
Although these savings could be consid-eredrelativelymodest, cost reductionsat
the microsystem level (hospitals, clinics,etc) may translate into large savings ifimplementedmore broadly. In the UnitedStates, children,2 years old represent.200 000 ED visits for bronchiolitis an-nually.39,40 Successful implementation ofbronchiolitis guidelines in ED settingswith similar cost savings could thereforesave up to $40 million annually. This es-timate, however, could be conservativebecause several studies have shownthat, in general, regardless of severity,patients with bronchiolitis are morelikely to receive resource-intensive andcostly care (eg, have a CXR and be pre-scribed antibiotics) if seen in a generalED as opposed to the ED of a children’shospital.41–43
From this effort, we have learned thatguideline implementation can be suc-cessful even in a busy setting such asthe ED. More important, we found thatprovider buy-in is crucial to successfulimplementation. Toseekagreementwithrecommendations, the evidence sup-portingeachguideline recommendationwas discussed extensively. As in thisstudy, it is also important to note thatclinical outcomes might not necessarilychange after improvement activities,especially in instances in which effec-tiveness of care is optimal before theimprovement activity. Nonetheless, evenif outcomes are perfect, because higher
TABLE 2 Association of the ED Bronchiolitis Guideline with Outcomes: Multivariate Interrupted Time-Series Analysis
Pre-EBG Utilizationand Costs (Adjusted)
Change in Utilization and CostsFrom Pre- to Post-EBG (95% CI)
Pre-EBG Trend perMonth (95% CI)a
Change in Trend per MonthFrom Pre- to Post-EBG (95% CI)b
Primary outcomesCXR utilization, % 39 223 (211 to 234)* +0.2 (20.2 to 0.6) 20.3 (21.3 to 0.6)RSV testing, % 33 211 (26 to 217)* 20.2 (20.5 to 0.1) 20.2 (20.5 to 0.9)Antibiotics utilization, % 11 24 (29 to 0.7) +0.02 (20.5 to 0.1) 20.4 (21.1 to 0.3)Albuterol utilization, % 54 27 (20.2 to 213)* +0.2 (20.2 to 0.5) 20.9 (20.2 to 21.6)*Total cost per patient, $ 1178 2197 (2136 to 2259)* 25 (211 to 1.3) 28 (24 to 20)
Balancing measuresc
Admission rate, % 26 +0.8 (22 to 3) +0.1 (20.1 to 0.3) 20.2 (20.5 to 0.2)Return ED visit rate, % 2 21.1 (23.9 to 1.7) +0.1 (20.1 to 0.3) 20.1 (20.4 to 0.3)ED LOS, min 240 241 (216 to 265)* 20.6 (22.2 to 1.1) +1.7 (21.3 to 4.7)
Covariates were adjusted for age, gender, race/ethnicity, oxygen saturation, initial temperature, and disposition. EBG, evidence-based guideline. *Significant (P value,.05) after adjustmentfor preexisting trends and covariates.a Trend (slope): “+” indicates increasing trend; “2” indicates decreasing trend.b “Change in trend” indicates testing for a significant difference between the pre-EBG and post-EBG slopes. For instance, the albuterol utilization rate revealed no significant pre-EBG trend. Post-EBG, however, the rate decreased at an additional 0.9% per month.c No deaths occurred during either period.
e232 AKENROYE et al by guest on August 30, 2018www.aappublications.org/newsDownloaded from

value health care should be the goal(improvedquality, lowercosts),wecouldstrive for improved performance inother areas of care, such as efficiencyand costs, without jeopardizing theoutcomes of care.
Other EDs could improve the uptake ofvarious evidence-based guidelines toimprove care in their setting by apply-ing similar principles of implementa-tion as we have done here, such asvisible leadership involvement, fos-tering peer support, and leveragingavailable resources. However, whenembarkingon improvementactivities, itis important toconsiderwhat is feasible.In our case, it was easier to significantlyreduce a commonly used diagnostic testthan toreduceantibioticswhere the rate
was already relatively low (10%) andpossibly justified before guidelineimplementation, such as for treatmentof concomitant otitis media. It is alsoharder to increase a high-performanceintervention. These floor and ceilingeffects might therefore affect QI activi-ties. Also, associated cost savings afterimplementation of a bronchiolitisguideline will depend on the number ofpatientswithbronchiolitisseen.EDswithlowutilizationof these tests or therapiesand/or with fewer patients with bron-chiolitis might not be able to demon-strate significant reductions in resourceutilization and costs.
To summarize, in the ED setting, a suc-cessfully implemented bronchiolitisguideline can help reduce costs through
the reduction of unnecessary utilizationof testing and treatment, without a re-duction in the quality of care. With thesavings of ∼$200 per patient, theremay be potential for substantial sav-ings in the management of bronchioli-tis across the United States, especiallyin centers with high utilization of test-ing and/or therapies.
ACKNOWLEDGMENTSWe thank Nicole Nutting, RN, the EDBronchiolitis Guideline nursing cham-pion;MichaelMonuteaux, ScD, and FangZhang, PhD, for their statistical guid-ance; andDennisFulton forhishelpwithretrieving the administrative portion ofthe data.
REFERENCES
1. Mansbach JM, Pelletier AJ, Camargo CA Jr.US outpatient office visits for bronchiolitis,1993-2004. Ambul Pediatr. 2007;7(4):304–307
2. American Academy of Pediatrics Sub-committee on Diagnosis and Managementof Bronchiolitis. Diagnosis and manage-ment of bronchiolitis. Pediatrics. 2006;118(4):1774–1793
3. Hall CB, Weinberg GA, Iwane MK, et al. Theburden of respiratory syncytial virus in-fection in young children. N Engl J Med.2009;360(6):588–598
4. Hall CB. Managing bronchiolitis and re-spiratory syncytial virus: finding the yellowbrick road. Arch Pediatr Adolesc Med. 2004;158(2):111–112
5. Zorc JJ, Hall CB. Bronchiolitis: recent evi-dence on diagnosis and management. Pe-diatrics. 2010;125(2):342–349
6. Bordley WC, Viswanathan M, King VJ, et al.Diagnosis and testing in bronchiolitis:a systematic review. Arch Pediatr AdolescMed. 2004;158(2):119–126
7. King VJ, Viswanathan M, Bordley WC, et al.Pharmacologic treatment of bronchiolitisin infants and children: a systematic re-view. Arch Pediatr Adolesc Med. 2004;158(2):127–137
8. Schuh S, Lalani A, Allen U, et al. Evaluation ofthe utility of radiography in acute bron-chiolitis. J Pediatr. 2007;150(4):429–433
9. Paramore LC, Ciuryla V, Ciesla G, Liu L.Economic impact of respiratory syncytial
virus-related illness in the US: an analysisof national databases. Pharmacoeconomics.2004;22(5):275–284
10. Conway PH, Edwards S, Stucky ER, ChiangVW, Ottolini MC, Landrigan CP. Variations inmanagement of common inpatient pediat-ric illnesses: hospitalists and communitypediatricians. Pediatrics. 2006;118(2):441–447
11. Orszag PR, Ellis P. Addressing rising healthcare costs—a view from the CongressionalBudget Office. N Engl J Med. 2007;357(19):1885–1887
12. Young PL, Olsen L. The Healthcare Impera-tive: Lowering Costs and Improving Outcomes:Workshop Series Summary. Washington,DC: The National Academies Press; 2010
13. Qaseem A, Alguire P, Dallas P, et al. Appro-priate use of screening and diagnostictests to foster high-value, cost-consciouscare. Ann Intern Med. 2012;156(2):147–149
14. Baker DW, Qaseem A, Reynolds PP, GardnerLA, Schneider EC. Design and use of per-formance measures to decrease low-valueservices and achieve cost-conscious care.Ann Intern Med. 2013;158(1):55–59
15. Landrigan CP, Conway PH, Stucky ER, ChiangVW, Ottolini MC. Variation in pediatric hos-pitalists’ use of proven and unproventherapies: a study from the Pediatric Re-search in Inpatient Settings (PRIS) net-work. J Hosp Med. 2008;3(4):292–298
16. Mansbach J, Kunz S, Acholonu U, Clark S,Camargo CA Jr. Evaluation of compliancewith palivizumab recommendations ina multicenter study of young childrenpresenting to the emergency departmentwith bronchiolitis. Pediatr Emerg Care.2007;23(6):362–367
17. Ralston S, Garber M, Narang S, et al. De-creasing unnecessary utilization in acutebronchiolitis care: results from the value ininpatient pediatrics network. J Hosp Med.2013;8(1):25–30
18. Tarini BA, Garrison MM, Christakis DA. In-stitutional variation in ordering completeblood counts for children hospitalized withbronchiolitis. J Hosp Med. 2007;2(2):69–73
19. Van Cleve WC, Christakis DA. Unnecessarycare for bronchiolitis decreases with in-creasing inpatient prevalence of bronchioli-tis. Pediatrics. 2011;128(5). Available at: www.pediatrics.org/cgi/content/full/128/5/e1106
20. Pathman DE, Konrad TR, Freed GL, FreemanVA, Koch GG. The awareness-to-adherencemodel of the steps to clinical guidelinecompliance: the case of pediatric vaccinerecommendations. Med Care. 1996;34(9):873–889
21. Centers for Disease Control and Prevention.Respiratory syncytial virus—United States,July 2007-June 2011. MMWR Morb MortalWkly Rep. 2011;60(35):1203–1206
22. Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented regression analysis
QUALITY REPORT
PEDIATRICS Volume 133, Number 1, January 2014 e233 by guest on August 30, 2018www.aappublications.org/newsDownloaded from

of interrupted time series studies in med-ication use research. J Clin Pharm Ther.2002;27(4):299–309
23. Dickey DA, Fuller WA. Distribution of theestimators for autoregressive time serieswith a unit root. J Am Stat Assoc. 1979;74(366):427–431
24. Johnson LW, Robles J, Hudgins A, Osburn S,Martin D, Thompson A. Management ofbronchiolitis in the emergency department:impact of evidence-based guidelines? Pe-diatrics. 2013;131(suppl 1):S103–S109
25. Barben J, Kuehni CE, Trachsel D, Hammer J;Swiss Paediatric Respiratory ResearchGroup. Management of acute bronchiolitis:can evidence based guidelines alter clinicalpractice? Thorax. 2008;63(12):1103–1109
26. Kotagal UR, Robbins JM, Kini NM, SchoettkerPJ, Atherton HD, Kirschbaum MS. Impact ofa bronchiolitis guideline: a multisite dem-onstration project. Chest. 2002;121(6):1789–1797
27. Perlstein PH, Kotagal UR, Schoettker PJ,et al. Sustaining the implementation of anevidence-based guideline for bronchiolitis.Arch Pediatr Adolesc Med. 2000;154(10):1001–1007
28. Todd J, Bertoch D, Dolan S. Use of a largenational database for comparative evalua-tion of the effect of a bronchiolitis/viralpneumonia clinical care guideline on pa-tient outcome and resource utilization.Arch Pediatr Adolesc Med. 2002;156(11):1086–1090
29. Wilson SD, Dahl BB, Wells RD. An evidence-based clinical pathway for bronchiolitis
safely reduces antibiotic overuse. Am JMed Qual. 2002;17(5):195–199
30. Perlstein PHKU, Kotagal UR, Bolling C, et al.Evaluation of an evidence-based guideline forbronchiolitis. Pediatrics. 1999;104(6):1334–1341
31. Jerardi KE, Elkeeb D, Weiser J, BrinkmanWB. Rapid implementation of evidence-based guidelines for imaging after firsturinary tract infection. Pediatrics. 2013;132(3). Available at: www.pediatrics.org/cgi/content/full/132/3/e749
32. Cohen AL, Rivara FP, Davis R, Christakis DA.Compliance with guidelines for the medicalcare of first urinary tract infections ininfants: a population-based study. Pediat-rics. 2005;115(6):1474–1478
33. Mansbach JM, McAdam AJ, Clark S, et al.Prospective multicenter study of the viraletiology of bronchiolitis in the emergencydepartment. Acad Emerg Med. 2008;15(2):111–118
34. Kotaniemi-Syrjänen A, Vainionpää R, ReijonenTM, Waris M, Korhonen K, Korppi M.Rhinovirus-induced wheezing in infancy—the first sign of childhood asthma? J Al-lergy Clin Immunol. 2003;111(1):66–71
35. Lemanske RF Jr, Jackson DJ, Gangnon RE,et al. Rhinovirus illnesses during infancypredict subsequent childhood wheezing.J Allergy Clin Immunol. 2005;116(3):571–577
36. Kusel MM, de Klerk NH, Holt PG, Kebadze T,Johnston SL, Sly PD. Role of respiratoryviruses in acute upper and lower re-spiratory tract illness in the first year oflife: a birth cohort study. Pediatr Infect DisJ. 2006;25(8):680–686
37. Christakis DA, Cowan CA, Garrison MM,Molteni R, Marcuse E, Zerr DM. Variation ininpatient diagnostic testing and manage-ment of bronchiolitis. Pediatrics. 2005;115(4):878–884
38. Yong JH, Schuh S, Rashidi R, et al. A costeffectiveness analysis of omitting radiog-raphy in diagnosis of acute bronchiolitis.Pediatr Pulmonol. 2009;44(2):122–127
39. Knapp JF, Simon SD, Sharma V. Quality ofcare for common pediatric respiratory ill-nesses in United States emergency depart-ments: analysis of 2005 National HospitalAmbulatory Medical Care Survey Data. Pe-diatrics. 2008;122(6):1165–1170
40. Mansbach JM, Emond JA, Camargo CA Jr.Bronchiolitis in US emergency depart-ments 1992 to 2000: epidemiology andpractice variation. Pediatr Emerg Care.2005;21(4):242–247
41. Johnson DW, Adair C, Brant R, Holmwood J,Mitchell I. Differences in admission rates ofchildren with bronchiolitis by pediatric andgeneral emergency departments. Pediat-rics. 2002;110(4). Available at: www.pediat-rics.org/cgi/content/full/110/4/e49
42. Isaacman DJ, Kaminer K, Veligeti H, JonesM, Davis P, Mason JD. Comparative practicepatterns of emergency medicine physiciansand pediatric emergency medicine physi-cians managing fever in young children.Pediatrics. 2001;108(2):354–358
43. Knapp JF, Hall M, Sharma V. Benchmarks forthe emergency department care of childrenwith asthma, bronchiolitis, and croup.Pediatr Emerg Care. 2010;26(5):364–369
e234 AKENROYE et al by guest on August 30, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-1991 originally published online December 9, 2013; 2014;133;e227Pediatrics
Ayobami T. Akenroye, Marc N. Baskin, Mihail Samnaliev and Anne M. StackTime-Series Analysis
Impact of a Bronchiolitis Guideline on ED Resource Use and Cost: A Segmented
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/133/1/e227including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/133/1/e227#BIBLThis article cites 40 articles, 13 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/bronchiolitis_subBronchiolitishttp://www.aappublications.org/cgi/collection/pulmonology_subPulmonologyhttp://www.aappublications.org/cgi/collection/trauma_subTraumasubhttp://www.aappublications.org/cgi/collection/emergency_medicine_Emergency Medicinefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on August 30, 2018www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2013-1991 originally published online December 9, 2013; 2014;133;e227Pediatrics
Ayobami T. Akenroye, Marc N. Baskin, Mihail Samnaliev and Anne M. StackTime-Series Analysis
Impact of a Bronchiolitis Guideline on ED Resource Use and Cost: A Segmented
http://pediatrics.aappublications.org/content/133/1/e227located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2013/12/03/peds.2013-1991.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on August 30, 2018www.aappublications.org/newsDownloaded from