incomplete right bundle-branch block -...
TRANSCRIPT

Incomplete Right Bundle-Branch BlockAn Electrocardiographic Enigma and Possible Misnomer
By E. NEIL MooRE, D.V.M., PH.D., JoHN P. BOINEAU, M.D.,
AND DONALD F. PATTWSON, D.V.M., D.Sc.With James Alexander, M.D., and A. J. Kennel, M.D.
SUMMARYIncomplete right bundle-branch block (IRBBB) usually is thought to be associated
with abnormalities of the peripheral Purkinje system. This paper discusses the resultsof a study of six dogs from the same family and three nonrelated dogs with congenitalIRBBB. Cardiac catheterization data were normal, and no evidence or history of car-
diac disease was found before or after death. The depolarization sequence of ven-
tricular epicardial activation was determined, and delays in right ventricular (RV)epicardial activation times were observed. Multipoint intramural electrodes were usedto study intramural activation of the ventricular septum and free walls. The "electricalthickness" near the base of the RV mass was more than double that of the normal RVmass (9 vs 4 mm). Conduction along the right bundle branch (RBB) was analyzedduring cardiopulmonary bypass, and electrograms recorded simultaneously from sixsites along the RBB demonstrated that conduction velocity down the bundle was nor-
mal. The normal time of activation of the endocardial RV Purkinje fibers demonstratedthat conduction in the right peripheral Purkinje system also was normal. Therefore,IRBBB in these dogs did not result from conduction abnormalities within the RVspecialized conduction system. Interestingly, six of these dogs were members of the F1generation from a mating of a female beagle with pulmonary stenosis and a malebeagle with ventricular septal defect. Both defects as well as IRBBB were observedin the F2 generation. The present findings suggest that IRBBB may be a developmentalvariation in thickness of the RV free wall rather than an abnormality of the RV con-
duction system in cases without apparent heart disease. The developmental variantappears to have a genetic basis.
Additional Indexing Words:Cardiac developmental variant Conduction delayParietal block Right ventricular hypertrophy
INCOMPLETE RIGHT bundle-branch clinical andblock or "parietal block" describes the question ab
electrocardiographic abnormality associated ing incompwith a wide variety of heart diseases in which (IRBBB).-.it is presumed that an abnormality exists in of papers pi
the peripheral Purkinje conduction system. electrocardiiHowever, the fact that the same electrocardio- been foundgram is recorded in a variety of dissimilar
Focal hypertrophy
experimental conditions raises a
out the specific etiology underly-flete right bundle-branch block-10 There also have been a numberublished in which individuals withographic evidence of IRBBB haveto have no underlying cardiac
From the Comparative Cardiovascular Studies Unit,School of Veterinary Medicine, University of Pennsyl-vania, Philadelphia, Pennsylvania, and the Depart-ments of Pediatrics, Medicine, and Surgery, DukeUniversity Medical Center, Durham, North Carolina.
Supported in part by grants from the AmericanHeart Association and U. S. Public Health Service
678
grants HE-4885, HE-10995, HE-11307, HE-5372, andHE-11309.
Address for reprints: Dr. E. Neil Moore, Compara-tive Cardiovascular Studies Unit, School of VeterinaryMedicine, University of Pennsylvania, Philadelphia,Pennsylvania 19104.
Received April 5, 1971; revision accepted forpublication July 1, 1971.
Circulation, Volume XLIV, October 1971
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
INCOMPLETE RIGHT BUNDLE-BRANCH BLOCK
disease as demonstrated by clinical studiesand by postmortem histologic studies.1-' 5
The present paper concerns electrophysio-logic investigations on a family of dogs withdefinite electrocardiographic evidence ofIRBBB in which no evidence of cardiacdisease could be demonstrated, either ante-mortem or postmortem. Evidence is presentedthat the pattern of IRBBB resulted not fromconduction abnormalities within the atrioven-tricular specialized conduction system, butrather was due to focal hypertrophy of theright ventricle which was a congenital de-velopmental variant.
Materials and MethodsGenetic Studies
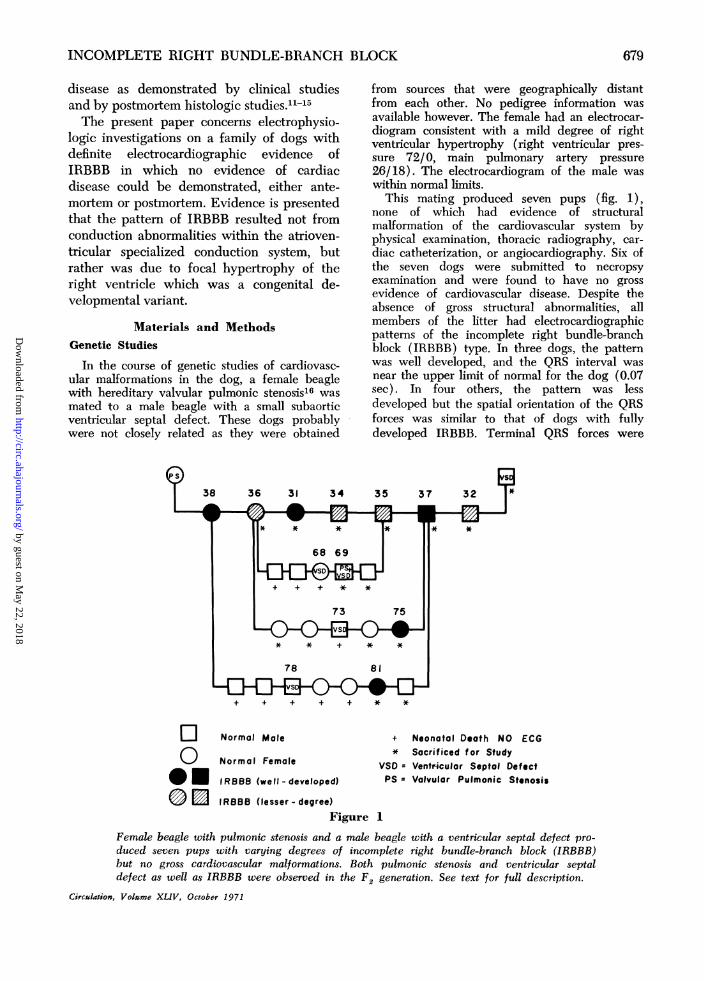
In the course of genetic studies of cardiovasc-ular malformations in the dog, a female beaglewith hereditary valvular pulmonic stenosis16 wasmated to a male beagle with a small subaorticventricular septal defect. These dogs probablywere not closely related as they were obtained
from sources that were geographically distantfrom each other. No pedigree information wasavailable however. The female had an electrocar-diogram consistent with a mild degree of rightventricular hypertrophy (right ventricular pres-sure 72/0, main pulmonary artery pressure26/18). The electrocardiogram of the male waswithin normal limits.
This mating produced seven pups (fig. 1),none of which had evidence of structuralmalformation of the cardiovascular system byphysical examination, thoracic radiography, car-diac catheterization, or angiocardiography. Six ofthe seven dogs were submitted to necropsyexamination and were found to have no grossevidence of cardiovascular disease. Despite theabsence of gross structural abnormalities, allmembers of the litter had electrocardiographicpatterns of the incomplete right bundle-branchblock (IRBBB) type. In three dogs, the patternwas well developed, and the QRS interval wasnear the upper limit of normal for the dog (0.07sec). In four others, the pattern was lessdeveloped but the spatial orientation of the QRSforces was similar to that of dogs with fullydeveloped IRBBB. Terminal QRS forces were
+ + + + + * *
Normal Male
Normal Femole
IRBBB (well - developed)
IROBB (lesser- degree)
+ Neonatal Deoth NO ECG* Sacrificed f or Study
VSD = Ventricular Septal DefectPS = Valvulor Pulmonic Stenosis
Figure 1
Female beagle with pulmonic stenosis and a male beagle with a ventricular septal defect pro-duced seven pups with varying degrees of incomplete right bundle-branch block (IRBBB)but no gross cardiovascular malformations. Both pulmonic stenosis and ventricular septaldefect as well as IRBBB were observed in the F2 generation. See text for full description.
Circulation, Volume XLlV, October 1971
El0em
679
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
MOORE ET AL.
directed ventrally, cranially, and to the right,producing R' waves in AVR and V1 and terminalS waves in leads V3, V6, and Vl0.Members of the litter were mated inter se to
produce an F2 generation consisting of 17 pups(fig. 1). Electrocardiograms were recorded inonly eight of the 17 members of the F2generation, since the remaining nine died in theearly neonatal period. Of the eight studiedelectrocardiographically, five had normal electro-cardiograms, one dog with pulmonic stenosis anda ventricular septal defect had electrocardiogra-phic signs of right ventricular hypertrophy, andtwo otherwise-normal dogs had an incompleteright bundle-branch block pattern.
This report deals with findings in six offspringof the F, generation which were studied byelectrophysiologic methods.
Electrophysiologic StudiesThe sequence of epicardial and intramural
activation of the ventricles was determined usinga bipolar electrode to scan 40 points on the rightand left ventricular epicardium, and multipoint,plunge electrodes to define intramural activation.These techniques have been previously describedin detail.'0 During the intramural activationstudies using plunge electrodes, special emphasiswas made to record from various right and leftPurkinje fibers both within the free ventricularwalls and septum. The onset of activation of thePurkinje fibers was correlated with the onset ofthe QRS complex. In addition, new techniqueswere developed to determine the sequence ofexcitation along the right bundle branch and His-Purkinje system.17 These investigations wereperformed after completing the epicardial-intra-mural activation studies. Both normal dogs anddogs with IRBBB were placed on cardiopulmo-nary bypass, and a right ventriculotomy was made.Then a 1.0- by 1.5-cm electrode plaque contain-ing 30 separate monopolar electrode sites locatedabout every 2 mm was gently sutured over theright bundle branch (RBB) (as indicated infigure 5 below). This electrode path enabledmultiple RBB electrograms to be recordedsimultaneously in either a bipolar or a unipolarmode. It was then possible to determine theconduction velocity along the RBB since thegeometry of the recording sites on the electrodepatch and the time of activation at these sameelectrodes was known. In 10 normal dogs, theconduction velocity along the RBB using thistechnique was 1-3 m/sec.17
Histologic StudiesThree dogs with electrophysiologically docu-
mented alterations of activation of the rightventricle (RV) had detailed histologic examina-
tions of the conduction system. Serial sections of6-8 g in thickness were made by the method ofPickett and Sommer.'8 Three dogs with normalelectrocardiographic findings were studied in alike manner. After fixation, multiple measure-ments were made of the thickness of the freewalls of the right ventricle, of the free walls of theleft ventricle, and of the septum. The weight ofthe free wall of the right ventricle was determinedas a percentage of the total ventricular weightand compared with normal values obtained byKnight.'9The following portions of the atrioventricular
conduction system were examined in each case:portions of the interatrial septum including theapproaches to the atrioventricular (A-V) node,the A-V node, the penetrating and bifurcatingportions of the common A-V bundle (Hisbundle), the proximal 1 cm of the left bundlebranch, the entire right bundle branch from itsorigin at the bifurcation to its termination at thebase of the septal papillary muscle, the free-running false tendons arising at the base of thepapillary muscle through their attachment to thefree wall of the right ventricle, that portion of theright ventricular free wall to which the free-running false tendons attached, and, finally,adjacent atrial as well as ventricular and valvularstructures.
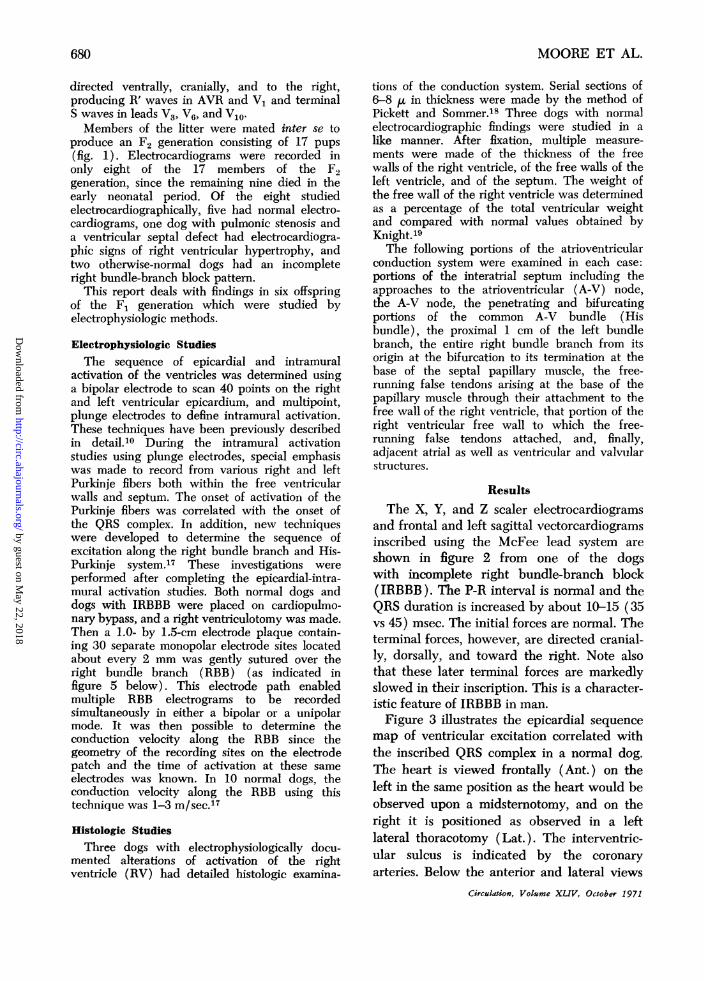
ResultsThe X, Y, and Z scaler electrocardiograms
and frontal and left sagittal vectorcardiogramsinscribed using the McFee lead system areshown in figure 2 from one of the dogswith incomplete right bundle-branch block(IRBBB). The P-R interval is normal and theQRS duration is increased by about 10-15 (35vs 45) msec. The initial forces are normal. Theterminal forces, however, are directed cranial-ly, dorsally, and toward the right. Note alsothat these later terminal forces are markedlyslowed in their inscription. This is a character-istic feature of IRBBB in man.Figure 3 illustrates the epicardial sequence
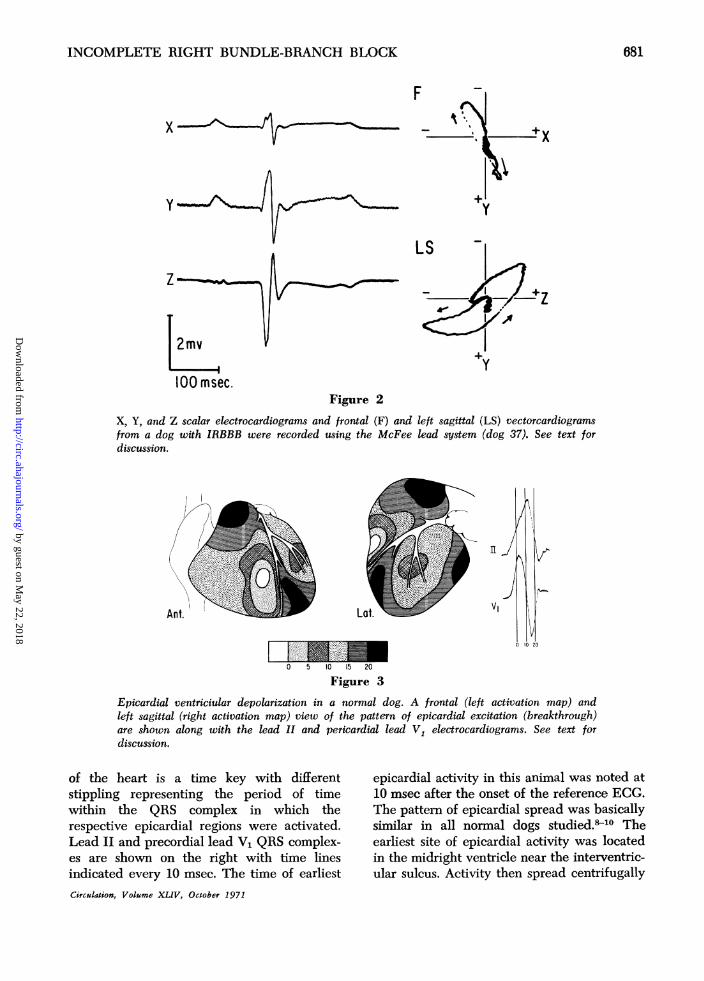
map of ventricular excitation correlated withthe inscribed QRS complex in a normal dog.The heart is viewed frontally (Ant.) on theleft in the same position as the heart would beobserved upon a midsternotomy, and on theright it is positioned as observed in a leftlateral thoracotomy (Lat.). The interventric-ular sulcus is indicated by the coronaryarteries. Below the anterior and lateral views
Circulation, Volume XLIV, October 1971
680
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
INCOMPLETE RIGHT BUNDLE-BRANCH BLOCK
F
X
y
zLS
'ZorA
2mv
100 msec.Figure 2
X, Y, and Z scalar electrocardiograms and frontal (F) and left sagittal (LS) vectorcardiogramsfrom a dog with IRBBB were recorded using the McFee lead system (dog 37). See text fordiscussion.
K
Ant.
II
V,Lot.
vs
21
0 5 10 15 20
E?igure 3
Epicardial ventriciular depolarization in a normal dog. A frontal (left activation map) andleft sagittal (right activation map) view of the pattern of epicardial excitation (breakthrough)are shown along with the lead II and pericardial lead V1 electrocardiograms. See text fordiscussion.
of the heart is a time key with differentstippling representing the period of timewithin the QRS complex in which therespective epicardial regions were activated.Lead II and precordial lead V1 QRS complex-es are shown on the right with time linesindicated every 10 msec. The time of earliestCirculation, Volume XLIV, October 1971
epicardial activity in this animal was noted at10 msec after the onset of the reference ECG.The pattern of epicardial spread was basicallysimilar in all normal dogs studied.-10 Theearliest site of epicardial activity was locatedin the midright ventricle near the interventric-ular sulcus. Activity then spread centrifugally
681
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

MOORE ET AL.
toward the atrioventricular groove, the inflowand outflow (conus) regions of the rightventricle (RV), and leftward across theinterventricular sulcus. The left ventricular(LV) epicardium was also activated in acentrifugal fashion with earliest activity beingobserved in the midregions and late activityoccurring at both the base and a small regionnear the anterior interventricular sulcus an-teriorly. The late activity in the RV conus,which occurred during the same period of theQRS complex as did late activity in the LVbase and anterior apex, resulted in considera-ble cancellation and a normal QRS complexbeing inscribed.The epicardial activation sequence maps
and lead II and V, QRS complexes in figure 4were recorded in a dog with IRBBB. The timekey below the activation maps containsstippling corresponding to the time of activa-tion of the respective regions of the epicar-dium. The rSR' QRS complex in the precordiallead V1 is characteristic of IRBBB. The frontalview of the dog's heart is shown on the left,and the left lateral view of the heart ispresented on the right. In contrast to thenormal dog (fig. 3) early activity wasobserved on the right epicardium near theinterventricular sulcus and simultaneously atthe apex of the LV indicating relatively laterthan normal RV breakthrough. Activity duringthe initial inscription of the R' wave in the
precordial lead V1 (10-15 msec) occurred atthe right and left ventricular bases. However,unlike the activation sequence in normal dogs,there was a late 10-msec period of time at20-30 msec in which activation occurred onlyin the outflow tract of the RV (conus) withoutany activity being recorded on the LVepicardium. The peak of the R' wavecoincided in time with this unopposed surfaceof activation in the RV. There are severalpossible causes of delayed activation of theRV conus region including alterations inconduction velocity of the right His-Purkinjesystem as well as possible variation in wallthickness of the RV free wall. Even withnormal radial conduction velocity, the in-creased thickness of the RV free wall couldresult in delayed activation of the thick regiondue to increased time for epicardial break-through. To investigate the mechanism ofdelayed epicardial activation, intramural acti-vation was analyzed using plunge electrodes.
Figure 5 contains simultaneously recordedintramural RV electrograms obtained from anormal dog (A), and from a dog with anelectrocardiogram characteristic of IRBBB(B). Using a constant reference electrogram,the lead II electrocardiogram was timenormalized with the simultaneously recordedintramural ventricular activation data as des-cribed previously. The intramural plungeelectrodes had 15 monopolar electrode sites
II1'
VIAnt.
ZwEEE0 5 10 15 20 25 30
Figure 4
_1Epicardial ventricular depolarization in incomplete right bundle-branch block (IRBBB).Frontal (Ant.) and left sagittal (Lat.) activation maps are presented along with the lead IIand precordial lead V1 electrocardiogram (dog 37). See text for discussion.
Circulation, Volume XLIV, October 1971
682
I6 ,,'
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

INCOMPLETE RIGHT BUNDLE-BRANCH BLOCK
A B
Lead II V '
1-2
Pj2-3
3-4 -
4-5
100 msec.
Lead II
1-2
2-3
3-44-5
-- 5-6
6-7
7-88-9
Figure 5A and B contain simultaneously recorded ventricular intramural electrograms recorded usingplunge-type electrodes. The lead II ECG was time normalized with the simultaneously re-corded ventricular electrograms. A was recorded from the base of the right ventricle in anormal dog. B was recorded in a dog with incomplete right bundle-branch block (IRBBB)(dog 37). See text for discussion.
located at 1-mm intervals along the electrodeshaft. In A, recorded from a normal dog, itcan be observed that four bipolar electro-grams were recorded between five monopolarelectrodes sites, and the "electrical thickness"of the RV free wall at this conus regiontherefore was 4 mm. Note also that thePurkinje depolarization spike denoted by Pj infigure 5 recorded on the endocardial surface ofthe RV free wall occurred at the onset of theinscription of the R wave in the lead II ECG.The activation sequence was also from endo-cardium to epicardium as indicated by theprogressive delay in onset of activation ofbipolar site 1-2 to bipolar site 4-5.
In figure 5B, the endocardial bipolarelectrode site 1-2 was activated earliest. Asmall Purkinje spike was recorded in thiselectrogram (Pj) and the onset of depolariza-Circulation, Volume XLIV, October 1971
tion of the Purkinje fiber was again at theinitiation of the R wave as normally observed.The "electrical thickness" of the RV free wallin this dog with IRBBB varied between 8 and9 mm in the basilar regions and pulmonaryconus region. This is nearly double the normal"electrical thickness" in this region as deter-mined in over 30 normal dogs. The spread ofactivation radially through the free walloccurred at a normal conduction velocity.Note that the endocardial site (site 1-2) wasactivated during the R wave in the lead IIECG while the outermost epicardial site (site8-9) was activated during the S wave. Similarincreased thickness of the RV free wall in theconus region was observed in eight other dogswith electrocardiographic manifestation ofIRBBB.
683
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
MOORE ET AL.
EKG
2
TV,3
~4
~~~~~~5
20 msec.
Figure 6
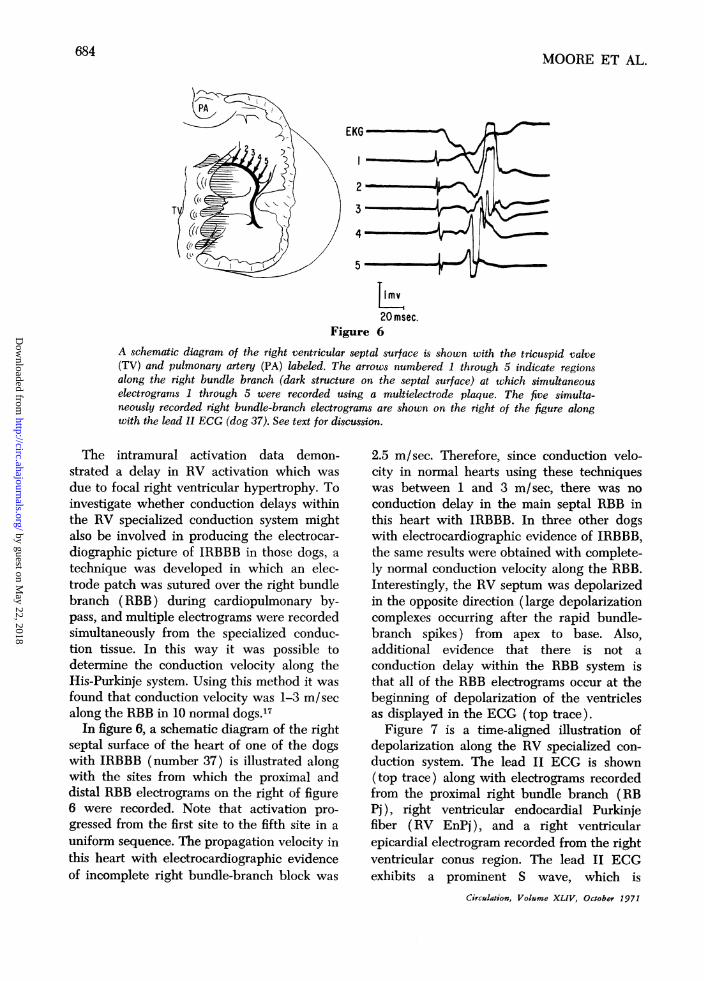
A schematic diagram of the right ventricular septal surface is shown with the tricuspid valve(TV) and pulmonary artery (PA) labeled. The arrows numbered 1 through 5 indicate regionlsalong the right bundle branch (dark structure on the septal surface) at which simultaneouselectrograms 1 through 5 were recorded using a multielectrode plaque. The five simulta-neously recorded right bundle-branch electrograms are shown on the right of the figure alongwith the lead II ECG (dog 37). See text for discussion.
The intramural activation data demon-strated a delay in RV activation which was
due to focal right ventricular hypertrophy. Toinvestigate whether conduction delays withinthe RV specialized conduction system mightalso be involved in producing the electrocar-diographic picture of IRBBB in those dogs, a
technique was developed in which an elec-trode patch was sutured over the right bundlebranch (RBB) during cardiopulmonary by-pass, and multiple electrograms were recordedsimultaneously from the specialized conduc-tion tissue. In this way it was possible todetermine the conduction velocity along theHis-Purkinje system. Using this method it wasfound that conduction velocity was 1-3 m/secalong the RBB in 10 normal dogs.'7
In figure 6, a schematic diagram of the rightseptal surface of the heart of one of the dogswith IRBBB (number 37) is illustrated alongwith the sites from which the proximal anddistal RBB electrograms on the right of figure6 were recorded. Note that activation pro-
gressed from the first site to the fifth site in a
uniform sequence. The propagation velocity inthis heart with electrocardiographic evidenceof incomplete right bundle-branch block was
2.5 m/sec. Therefore, since conduction velo-city in normal hearts using these techniqueswas between 1 and 3 m/sec, there was noconduction delay in the main septal RBB inthis heart with IRBBB. In three other dogswith electrocardiographic evidence of IRBBB,the same results were obtained with complete-ly normal conduction velocity along the RBB.Interestingly, the RV septum was depolarizedin the opposite direction (large depolarizationcomplexes occurring after the rapid bundle-branch spikes) from apex to base. Also,additional evidence that there is not a
conduction delay within the RBB system isthat all of the RBB electrograms occur at thebeginning of depolarization of the ventriclesas displayed in the ECG (top trace).
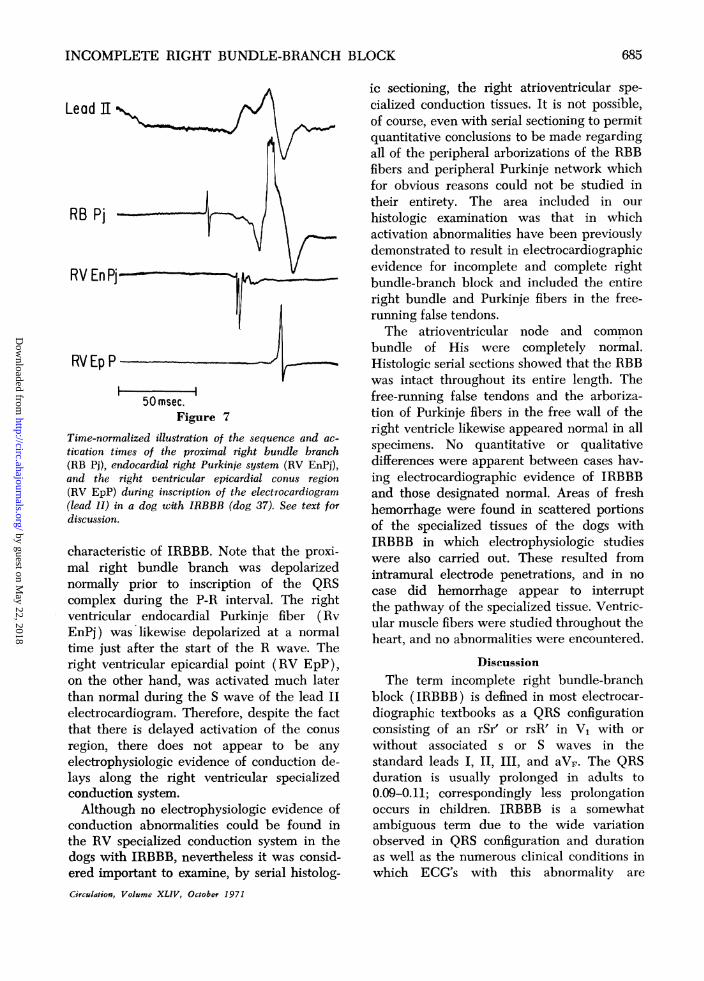
Figure 7 is a time-aligned illustration ofdepolarization along the RV specialized con-duction system. The lead II ECG is shown(top trace) along with electrograms recordedfrom the proximal right bundle branch (RBPj), right ventricular endocardial Purkinjefiber (RV EnPj), and a right ventricularepicardial electrogram recorded from the rightventricular conus region. The lead II ECGexhibits a prominent S wave, which is
Circulation, Volume XLIV, October 1971
684
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
INCOMPLETE RIGHT BUNDLE-BRANCH BLOCK
Lead ]I
RB Pj
RV EnPj
RV Ep P
50 msec.Figure 7
Time-normalized illustration of the sequence and ac-tivation times of the proximal right bundle branch(RB Pj), endocardial right Purkinje system (RV EnPj),and the right ventricular epicardial conus region(RV EpP) during inscription of the electrocardiogram(lead II) in a dog with IRBBB (dog 37). See text fordiscussion.
characteristic of IRBBB. Note that the proxi-mal right bundle branch was depolarizednormally prior to inscription of the QRScomplex during the P-R interval. The rightventricular endocardial Purkinje fiber (RvEnPj) was likewise depolarized at a normaltime just after the start of the R wave. Theright ventricular epicardial point (RV EpP),on the other hand, was activated much laterthan normal during the S wave of the lead IIelectrocardiogram. Therefore, despite the factthat there is delayed activation of the conusregion, there does not appear to be anyelectrophysiologic evidence of conduction de-lays along the right ventricular specializedconduction system.Although no electrophysiologic evidence of
conduction abnormalities could be found inthe RV specialized conduction system in thedogs with IRBBB, nevertheless it was consid-ered important to examine, by serial histolog-
ic sectioning, the right atrioventricular spe-cialized conduction tissues. It is not possible,of course, even with serial sectioning to permitquantitative conclusions to be made regardingall of the peripheral arborizations of the RBBfibers and peripheral Purkinje network whichfor obvious reasons could not be studied intheir entirety. The area included in ourhistologic examination was that in whichactivation abnormalities have been previouslydemonstrated to result in electrocardiographicevidence for incomplete and complete rightbundle-branch block and included the entireright bundle and Purkinje fibers in the free-running false tendons.The atrioventricular node and common
bundle of His were completely normal.Histologic serial sections showed that the RBBwas intact throughout its entire length. Thefree-running false tendons and the arboriza-tion of Purkinje fibers in the free wall of theright ventricle likewise appeared normal in allspecimens. No quantitative or qualitativedifferences were apparent between cases hav-ing electrocardiographic evidence of IRBBBand those designated normal. Areas of freshhemorrhage were found in scattered portionsof the specialized tissues of the dogs withIRBBB in which electrophysiologic studieswere also carried out. These resulted fromintramural electrode penetrations, and in nocase did hemorrhage appear to interruptthe pathway of the specialized tissue. Ventric-ular muscle fibers were studied throughout theheart, and no abnormalities were encountered.
DiscussionThe term incomplete right bundle-branch
block (IRBBB) is defined in most electrocar-diographic textbooks as a QRS configurationconsisting of an rSr' or rsR' in V1 with orwithout associated s or S waves in thestandard leads I), II III, and aVF. The QRSduration is usually prolonged in adults to0.09-0.11; correspondingly less prolongationoccurs in children. IRBBB is a somewhatambiguous term due to the wide variationobserved in QRS configuration and durationas well as the numerous clinical conditions inwhich ECG's with this abnormality are
Circulation, Volume XLIV, October 1971
68-05
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
MOORE ET AL.
encountered. The term IRBBB implies thatthere is block in the peripheral right Purkinjesystem, and cases of IRBBB associated withacquired, congenital, or experimental lesionswithin the right ventricular Purkinje networkhave been clearly demonstrated. However,other instances of IRBBB without demonstra-ble cardiovascular lesions have also beenreported. Thus, there is clearly a need toexamine the right bundle branch-Purkinjesystem using direct electrophysiologic tech-niques to determine the sequence of rightventricular myocardial activation, as well asactivation studies on the right ventricularspecialized conduction system in cases ofIRBBB. These types of investigations aredifficult and, in many instances, impossible toperform in patients. The present investigationsafforded an unusual opportunity to examinethe basis of spontaneous IRBBB in a group ofbeagle dogs which were siblings of an F1breeding of two dogs with congenital heartdisease (fig. 1).
In the present study, six canine siblingswere found to have an electrocardiographicpattern of IRBBB, but no cardiovascularabnormalities could be found on clinicalexamination or upon histologic examination ofthe heart. The etiology of the IRBBB patternwas a focal hypertrophy of regions of the rightventricular free wall near the atrioventricularmargin and pulmonary conus. Myocardialconduction velocity through these thickenedregions of right ventricular myocardium wasfound to be normal; however, the longerdistance that the wavefront had to travel fromthe endocardium to epicardium resulted indelay in the onset of activation of the rightventricular epicardium at these hypertrophiedregions. Therefore, IRBBB resulted from aprolonged phase of activation in certainregions of the right ventricular free wallcaused by focal hypertrophy, rather than fromdelay caused by conduction abnormalitieswithin the peripheral right ventricularPurkinje system.Of course, the explanation for the surface
ECG pattern of IRBBB in these animalscannot be generalized to explain all cases of
IRBBB in man. However, they do indicate atleast one basis for this electrocardiographicpattern other than the classically acceptedtheory of parietal block of the right Purkinjenetwork. Strong additional support for focalregions of right ventricular hypertrophy givingrise to an ECG pattern of IRBBB is the factthat two other unrelated dogs of differentbreeds (keeshond and a mongrel) also had afocal right ventricular hypertrophy associatedwith an electrocardiographic pattern ofIRBBB. It should be mentioned that when theratio of the total weight of the rightventricular free wall was compared to totalheart weight in these dogs, the ratio was at theupper limits of normal found by Knight in aseries of 38 normal dogsl9 (24% of total heartweight in IRBBB dogs vs an average of 22% innormal dogs). The fact that there was not asignificant increase in right ventricular wallweight as determined by this method pointsout that activation delays in only a smallregion of the right ventricle can result inchanges in phase relationships of a sufficientdegree to alter the usual balance of forces,thereby permitting delayed right ventricularactivation to be expressed as IRBBB. Thethickened right ventricular wall not onlyresults in phasic changes in right and leftventricular activation, but also permits theactivation wavefront to occupy a greater areaof the right ventricular wall, thereby causingthe amplitude of the late right ventricularforces to be increased in the electrocardio-gram.20
Perhaps of greater significance is the findingthat mild localized right ventricular hyper-trophy was present in the family of beagles inthe absence of any obvious hemodynamicstimulus. This suggests that the distribution ofright ventricular mass is determined not onlyby the hemodynamic state, but also by geneticfactors which govern the morphogenesis of theventricular walls. Such intrinsic mechanismsmay determine to some extent the capacity ofthe individual to react to hemodynamic loadsand may account for the variation in rightventricular hypertrophy encountered in pa-tients with similar degrees of hemodynamic
Circulation, Volume XLIV, October 1971
686
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
INCOMPLETE RIGHT BUNDLE-BRANCH BLOCK
overload. Also, the present findings suggestthat the frequent occurrence of late anterior-rightward QRS forces (rSr' and S1S2S3) inapparently healthy people may in part repre-sent normal variation in thickness and distri-bution of the RV mass.
Acknowledgments
The authors wish to thank Ralph Iannuzzi, WilliamSchnarr, J. H. Kasell, and C. B. Clark for invaluabletechnical assistance.
References
1. GRANT RP: Clinical Electrocardiography, theSpatial Vector Approach. New York, McGraw-Hill Book Co., Inc., 1957
2. LEDBETTER MK, CANNON AB, COSTA AF: Theelectrocardiogram in diphtheritic myocarditis.Amer Heart J 68: 599, 1964
3. BiRiNiK AJ, NEILL CA: The electrocardiogram incongenital heart disease. Circulation 12: 604,1955
4. HuTH ES, SQUIRES RD: The relation of cardio-vascular phenomena to metabolic changes ina patient with chronic hypokalemia. Circula-tion 14: 60, 1965
5. PAYNE CA, GREENFIELD JC: Electrocardiograph-ic abnormalities associated with myotonicdystrophy. Amer Heart J 65: 436, 1963
6. GRANT RP: Left axis deviation. Circulation 14:233, 1956
7. UHLEY HN, RIVKIN L: Electrocardiographicpatterns following interruption of main andperipheral branches of the canine right bundleof His. Amer J Cardiol 7: 810, 1961
8. MOORE EN, HOFFMAN BF, PATTERSON DF,STJUCKEY JH: Electrocardiographic changesdue to delayed activation of the wall of theright ventricle. Amer Heart J 68: 347, 1964
9. WATT TB, PRurrr RD: Electrocardiographicfindings associated with experimental arboriza-tion block in dogs. Amer Heart J 69: 642,1965
10. BOINEAU JP, SPACH MS, AYREs CR: Genesis ofthe electrocardiogram in atrial septal defect.Amer Heart J 68: 637, 1964
11. STEWART CB, MANNING GW: A detailed analysisof electrocardiograms of 500 R.C.A.F. air crew.Amer Heart J 27: 502, 1944
12. PACKARD JM, GRAETrINGER JS, GRAYBIEL A:Analysis of the electrocardiogram obtainedfrom 1,000 young healthy aviators. Circulation10: 384, 1954
13. Hiss RG, LAMB LF, ALLEN MF: Electrocardio-graphic findings in 67,375 asymptomaticsubjects: Normal values. Amer J Cardiol 6:209, 1960
14. ELIOT RS, MILLHAM WA, MILLHAM J: Theclinical significance of marked left axisdeviation in man without known disease. AmerJ Cardiol 12: 767, 1963
15. ENTMAN ML, ESTES EH, HACKEL DB: Thepathologic basis of the electrocardiographicpattern of parietal block. Amer Heart J 74:202, 1967
16. PATTERSON DF: Epidemiologic and geneticstudies of congenital heart disease in the dog.Circ Res 23: 171, 1968
17. WALSTON A, BOINEAU JP, ALEXANDER JA, SEALYWC: A study of functional dissociation in theright bundle branch. In preparation
18. PICKETT JP, SOMMER JR: Thirty-five mm film asmounting base and plastic spray as cover glassfor histologic sections. Arch Path (Chicago)69: 239, 1960
19. KNIGHT DH: Effects of spontaneous cor pulmo-nale in dogs (Dirofilaria immitis infestation)on the gross morphology and hemodynamics ofthe lung circulation and ventricles. Mastersthesis, University of iPennsylvania
20. BOINEAU JP, HILL EN, SPACH MS, MOORE EN:Basis of the electrocardiogram in rightventricular hypertrophy: Relationship betweenventricular depolarization and body surfacepotentials in dogs with spontaneous RVH-con-trasted with normal dogs. Amer Heart J 76:605, 1968
Circulation, Volume XLIV, October 1971
687
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from
Alexander and A. J. KennelE. NEIL MOORE, JOHN P. BOINEAU, DONALD F. PATTERSON, James
Possible MisnomerIncomplete Right Bundle-Branch Block: An Electrocardiographic Enigma and
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1971 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.44.4.6781971;44:678-687Circulation.
http://circ.ahajournals.org/content/44/4/678located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from