integrative medicine = good medicine
DESCRIPTION
Integrative Medicine = Good medicine. Kathi J. Kemper, MD, MPH Caryl J Guth Chair for Holistic and Integrative Medicine Professor of Pediatrics, Public Health Sciences, Family and Community Medicine Wake Forest University Health Sciences. CAM US History. - PowerPoint PPT PresentationTRANSCRIPT
Integrative Medicine = Good medicine
Kathi J. Kemper, MD, MPHCaryl J Guth Chair for Holistic
and Integrative MedicineProfessor of Pediatrics, Public Health Sciences, Family and
Community MedicineWake Forest University Health
Sciences
CAM US History• 1970’s American Holistic Medical Association• 1980’s popular books – Our Bodies, Our Selves• 1991 US Congress establishes Office of Alternative
Medicine at NIH ($2 million)• 1993 Eisenberg’s article in NEJM on common CAM
use in US (34% of US adults)• 1996 publication of The Holistic Pediatrician• 2000 CAHCIM• 2002 White House Commission on CAM report• 2005 Institute of Medicine report on CAM• 2005 AAP CHIM
CAM Clinical History US
• 1970’s and ’80’s – scattered MD clinics, eg Norm Shealy, Chris Northrup, Andy Weil, Hugh Riordan, Jim Gordon, Bob Anderson
• 1990’s –stand-alone multidisciplinary clinics; financially issues; growth of CAM in medical schools and CME 2000’s – integration into existing clinics; integration into hospital care –mind/body, massage, acupuncture, nutrition, hospital formulary policies; start of CAM education in residency education
• Financing – initially with philanthropy, wealthy self-pay; moving toward advocacy for insurance coverage (See John Weeks)
• Evidence-base
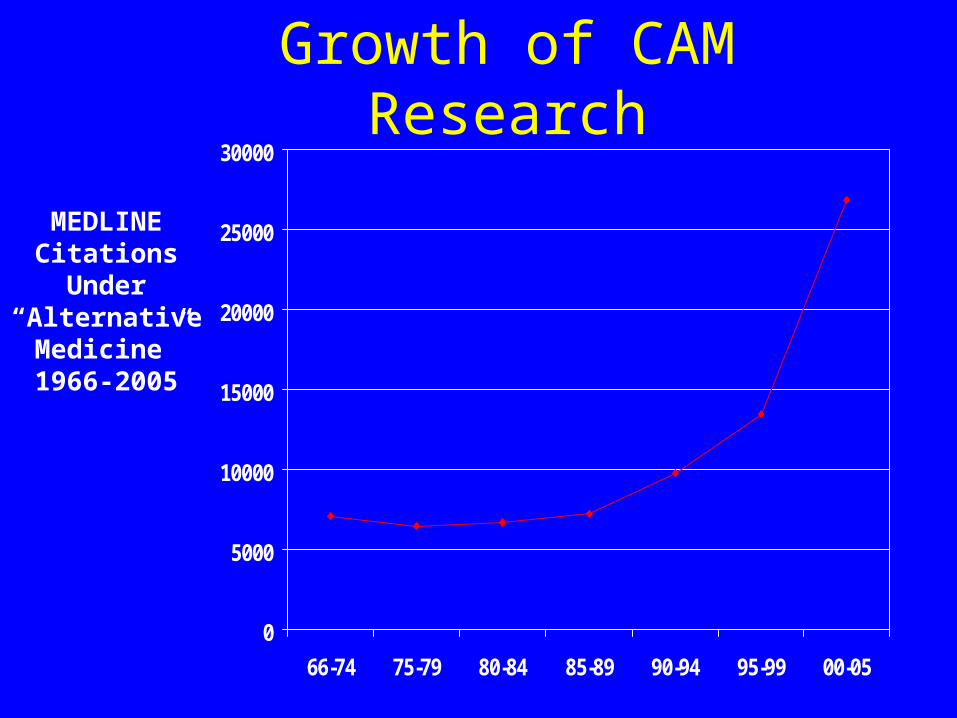
Growth of CAM Research
0
5000
10000
15000
20000
25000
30000
66-74 75-79 80-84 85-89 90-94 95-99 00-05
MEDLINECitations Under
“AlternativeMedicine”1966-2005
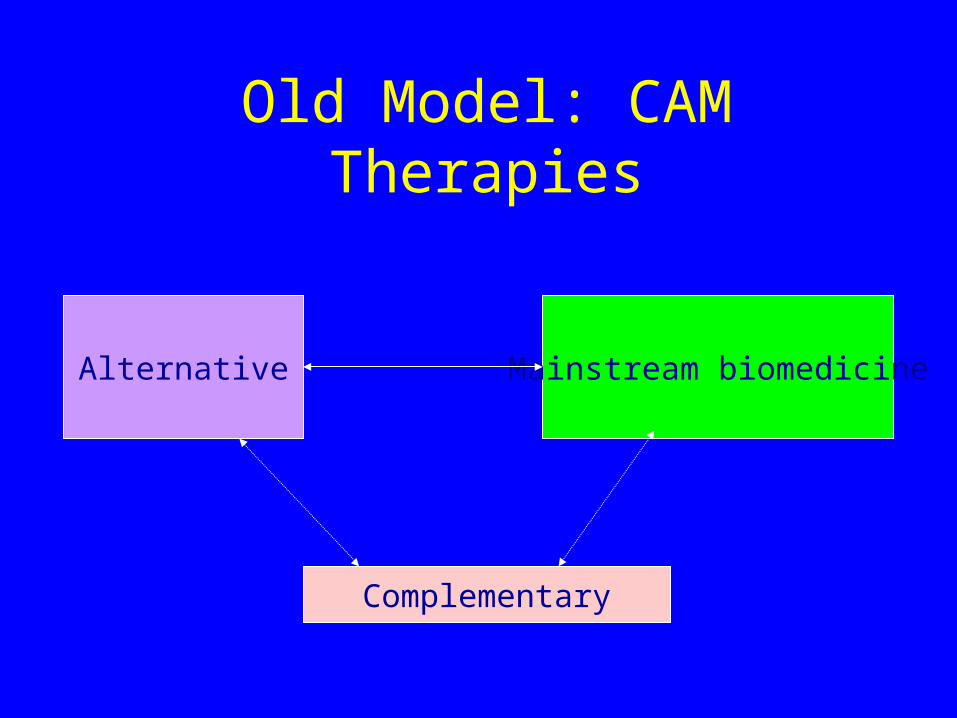
Old Model: CAM Therapies
Alternative Mainstream biomedicine
Complementary
Concerns about CAM
• Sylvia Millecam death from breast cancer following treatment with acupuncture, faith, psychic healers
• Unfounded treatments (NOT evidence-based)
• Poor oversight (poor coordination)
• NOT complementaryBMJ, 28 Feb 2004
Patient/Consumer Interest
• Use is high; most use combinations
• 42% of Americans reported using (1997)
• Consumers self-paid $27 billion; this exceeds out of pocket expenses for hospital care
• Out of pocket payments highest for herbs and supplements, massage, acupuncture, fitness training
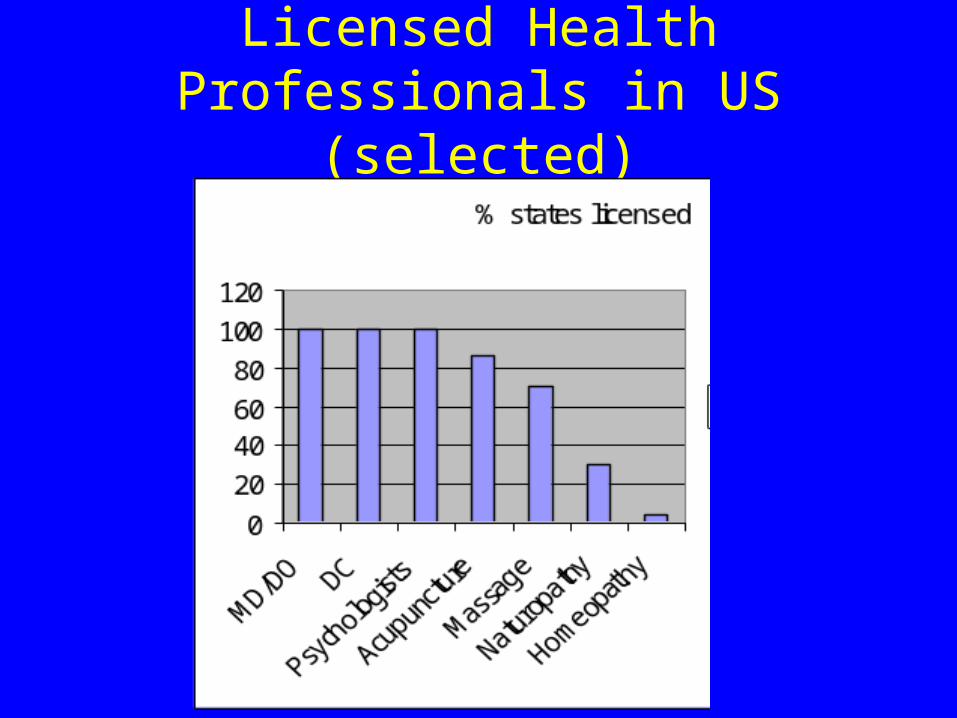
Licensed Health Professionals in US (selected)
Popularity leads to…eResources
• US Presidential Commission on CAM, chaired by James Gordon, MD http://www.whccamp.hhs.gov/
• Institute of Medicine report on CAM in the US, chaired by Professor Stuart Bondurant, MD; http://www.nap.edu/books/0309092701/html/
<>
eResource: NIH NCCAM
• Patient information sheets in English and Spanish
• Ongoing research projects/clinical trials
• Education and Training opportunities
• http://nccam.nih.gov
NCCAM Clearinghouse: (US) 1-888-644-
6226
eResource: NCI OCCAM
• Health information for patients
http://www.cancer.gov/cam/health_understanding.html
• Clinical trial information• Grant funding for
research projects
Highest CAM Users
• Well educated
• Upper income
• Women
• Chronically ill (pain fatigue, anxiety, depression)
Why use CAM?• Consistent with patient values (ecological, spiritual,
political)• Person-centered• Gentler• Empowering• Esthetic• Less drug dependent• Less technology dependent• Meaning – causes, what one can do• Lifestyle emphasis• Failures of medicine (antibiotic resistance; side effects,
costs; medical errors; limited access) poor success with chronic illnesses
Resource
• Founded in 2000• 38 academic health centers (Harvard, Yale,
Duke, Stanford, UAz, WFUSM, UMi, UMn, UNM, U Alberta, etc)
• International Research Conference• Collaborative research• Developing “best practices” clinical models• Education (residency and undergrad)• http://www.imconsortium.org/cahcim/about/home
.html
Definition: Integrative Medicine
Integrative Medicine is the practice of medicine that reaffirms the importance of the relationship between practitioner and patient, focuses on the whole person, is informed by evidence, and makes use of all appropriate therapeutic approaches, healthcare professionals and disciplines to achieve optimal health and healing.
Consortium of Academic Health Centers for Integrative Medicine,
5/05
Integrative Medicine = Good Medicine
Sustainable, Healing
Environment
Holistic Patient-
Centered Care
Wellness Orientation
Comprehensive Therapeutic
Options
*
Patient-centered care = holistic
Caring for whole person - body, mind, emotions, spirit, relationships -- in the context of family, culture and community
Biopsychosocial model
Culturally sensitive care
Can a surgeon be holistic? YES
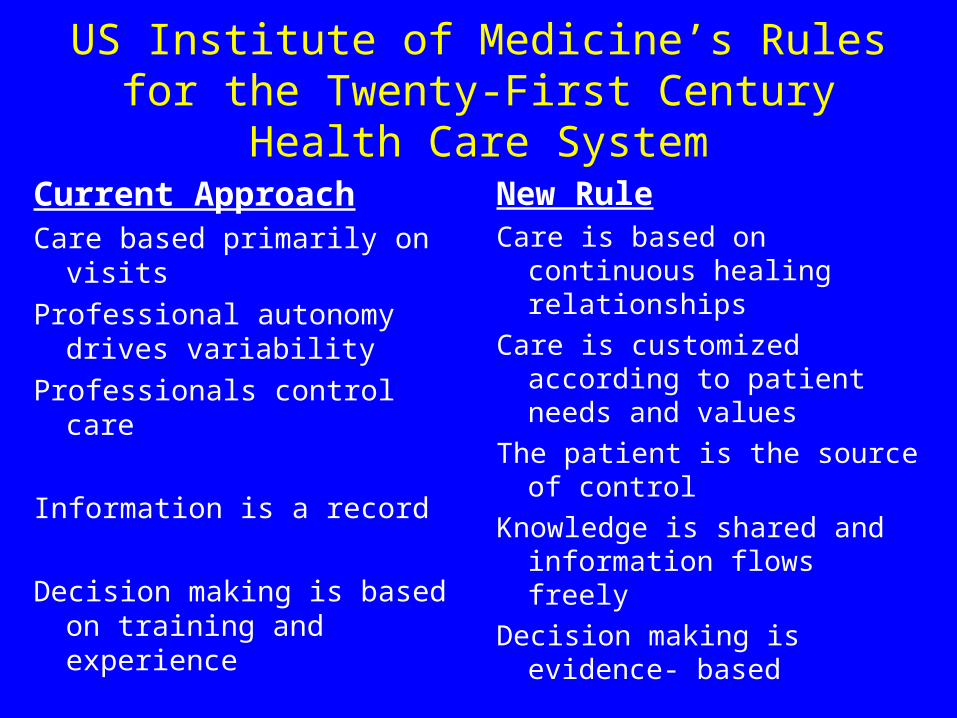
US Institute of Medicine’s Rules for the Twenty-First Century Health Care System
Current ApproachCare based primarily on visits
Professional autonomy drives variability
Professionals control care
Information is a record
Decision making is based on training and experience
New RuleCare is based on continuous
healing relationships
Care is customized according to patient needs and values
The patient is the source of control
Knowledge is shared and information flows freely
Decision making is evidence- based
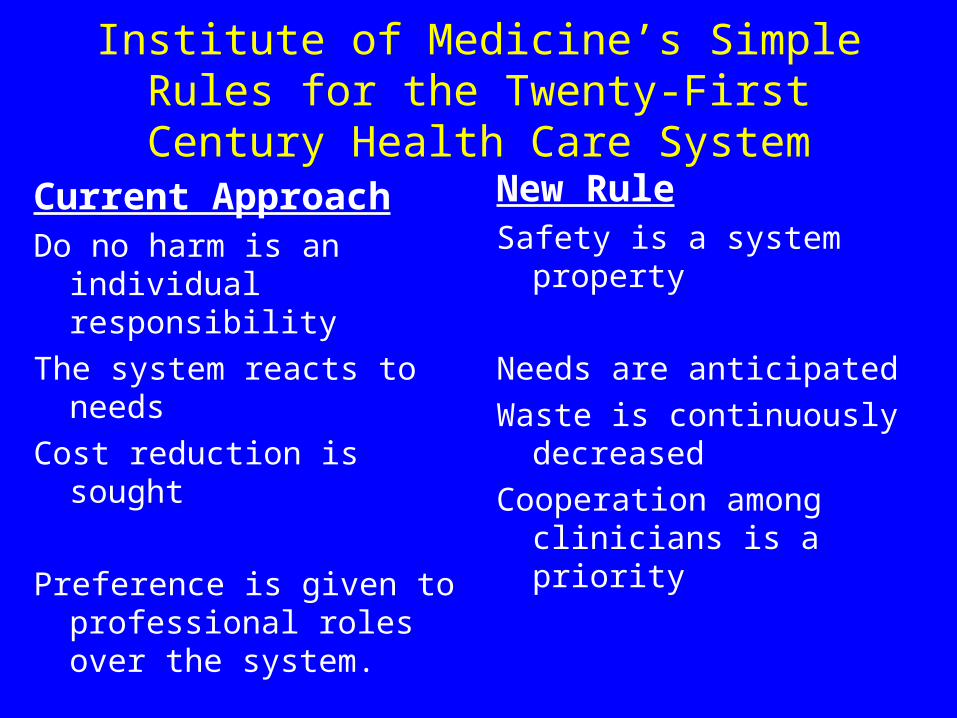
Institute of Medicine’s Simple Rules for the Twenty-First Century Health Care System
Current ApproachDo no harm is an individual
responsibility
The system reacts to needs
Cost reduction is sought
Preference is given to professional roles over the system.
New RuleSafety is a system property
Needs are anticipated
Waste is continuously decreased
Cooperation among clinicians is a priority
CAM is a SUBSET of tools within Integrative Medicine
Integrative Medicine emphasizes
• wellness and healing of the whole person, • with special emphasis on patient participation, • and attention to mental and spiritual health;• Communication, empowerment, cultural awareness
The knowledge and use of Complementary and Alternative Medicine (CAM) is an important aspect of Integrative Medicine.
Section on Integrative Medicine, Internal Medicine, UNM
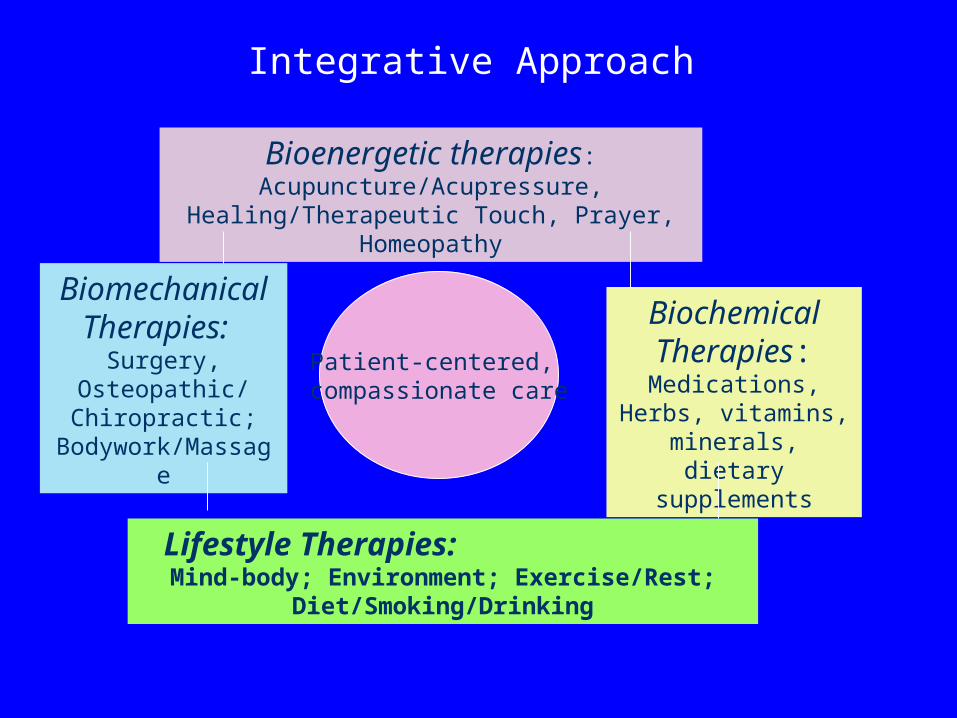
Patient-centered, compassionate care
Bioenergetic therapies: Acupuncture/Acupressure, Healing/Therapeutic
Touch, Prayer, Homeopathy
Biochemical Therapies:
Medications, Herbs, vitamins, minerals,
dietary supplements
Lifestyle Therapies: Mind-body; Environment; Exercise/Rest;
Diet/Smoking/Drinking
Biomechanical Therapies:
Surgery, Osteopathic/ Chiropractic;
Bodywork/Massage
Integrative Approach
eEducation about herbs / dietary supplements
• https://northwestahec.wfubmc.edu/learn/herbs_ce/index.cfm
What kinds of services do NC MDs want to provide in hospital?
• Nutrition services – 84%• Fitness services – 80%• Stress management
services – 75%
Kemper K. BMC CAM 2007

***Mind-Body Therapies***
• Hypnosis• Guided imagery• Meditation• Autogenic training• Biofeedback• Journaling• Social Support• Psychological counseling• Peer support
Is it ETHICAL to integrate CAM therapies into conventional
practice?• Principles of ethics
– Beneficence / Do no harm– Autonomy– Justice
• Common Sense– Balance risks and benefits
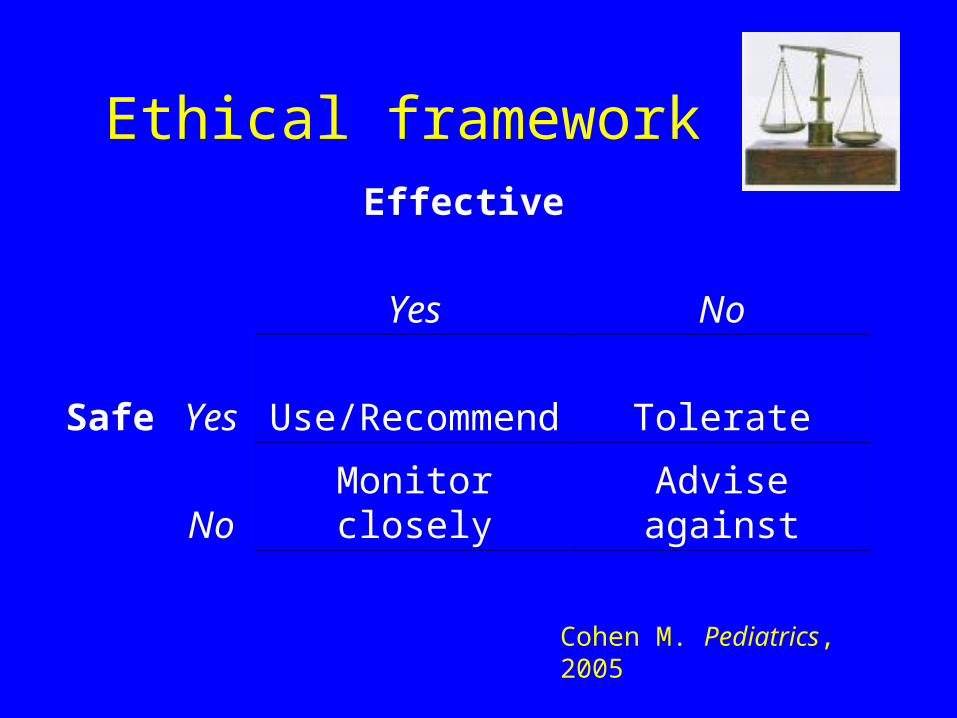
Ethical frameworkEffective
Yes No
Safe Yes Use/Recommend Tolerate
No Monitor closely Advise against
Cohen M. Pediatrics, 2005

Effective? Safe?
– What therapy? – For whom? – For what condition? (cancer,
colds)– Under what circumstances?– For what desired outcome?– When? immediate versus long-
term
Kemper. Arch Dis Child, 2001
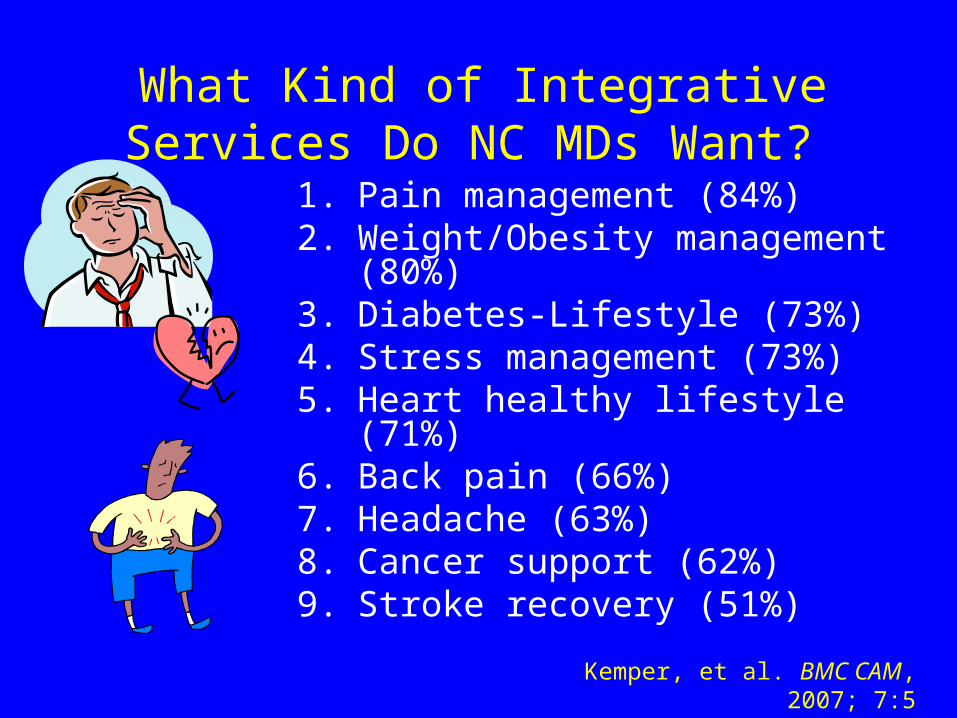
What Kind of Integrative Services Do NC MDs Want?
1. Pain management (84%)2. Weight/Obesity management
(80%)3. Diabetes-Lifestyle (73%)4. Stress management (73%)5. Heart healthy lifestyle (71%)6. Back pain (66%)7. Headache (63%)8. Cancer support (62%)9. Stroke recovery (51%)
Kemper, et al. BMC CAM, 2007; 7:5
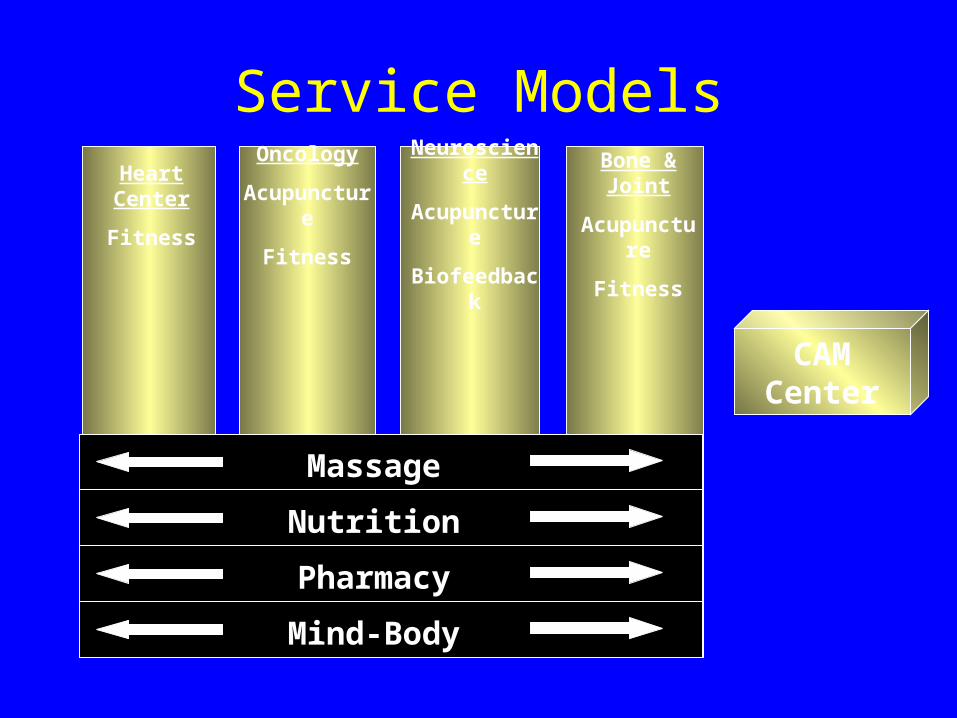
Service Models
Heart Center
Fitness
Oncology
Acupuncture
Fitness
Neuroscience
Acupuncture
Biofeedback
Bone & Joint
Acupuncture
Fitness
Mind-Body
Nutrition
Pharmacy
Massage
CAM Center
Sustainability
• Consistent with cultural values, e.g., evidence-based, compassionate, comprehensive, common sense, cost-effective – strengthens and restores the heart and soul of medicine
• Insurance coverage• Collaborative with public health, community of
health care providers, patient advocacy groups• Integrated, not marginalized
THANK YOU!
WHO 2000 ranking
• Netherlands is #17 for quality of health services (US is #37)
• Problems– Waiting times– Labor shortages
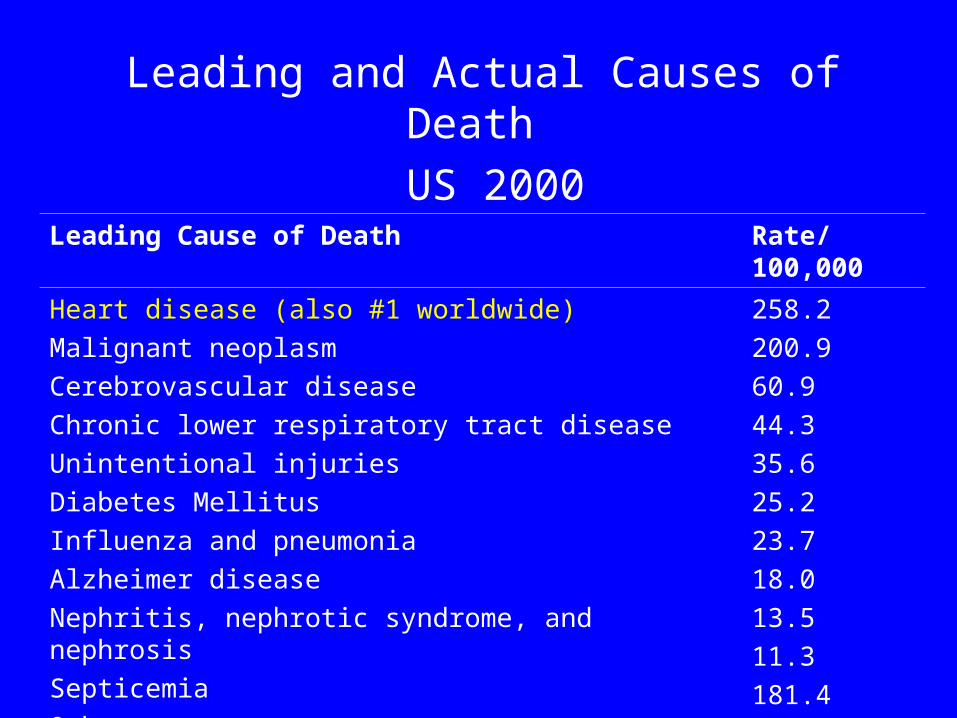
Leading and Actual Causes of Death
US 2000Leading Cause of Death Rate/100,000
Heart disease (also #1 worldwide)
Malignant neoplasm
Cerebrovascular disease
Chronic lower respiratory tract disease
Unintentional injuries
Diabetes Mellitus
Influenza and pneumonia
Alzheimer disease
Nephritis, nephrotic syndrome, and nephrosis
Septicemia
Other
Total
258.2
200.9
60.9
44.3
35.6
25.2
23.7
18.0
13.5
11.3
181.4
873.1
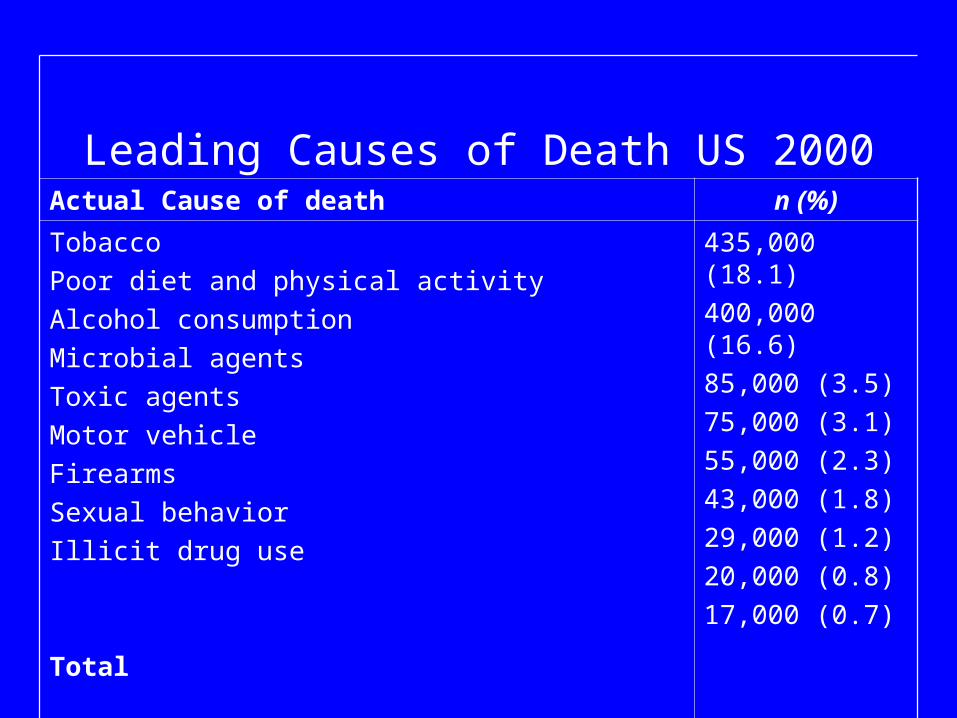
Leading Causes of Death US 2000Actual Cause of death n (%)
Tobacco
Poor diet and physical activity
Alcohol consumption
Microbial agents
Toxic agents
Motor vehicle
Firearms
Sexual behavior
Illicit drug use
Total
435,000 (18.1)
400,000 (16.6)
85,000 (3.5)
75,000 (3.1)
55,000 (2.3)
43,000 (1.8)
29,000 (1.2)
20,000 (0.8)
17,000 (0.7)
1,159,000 (48.2)
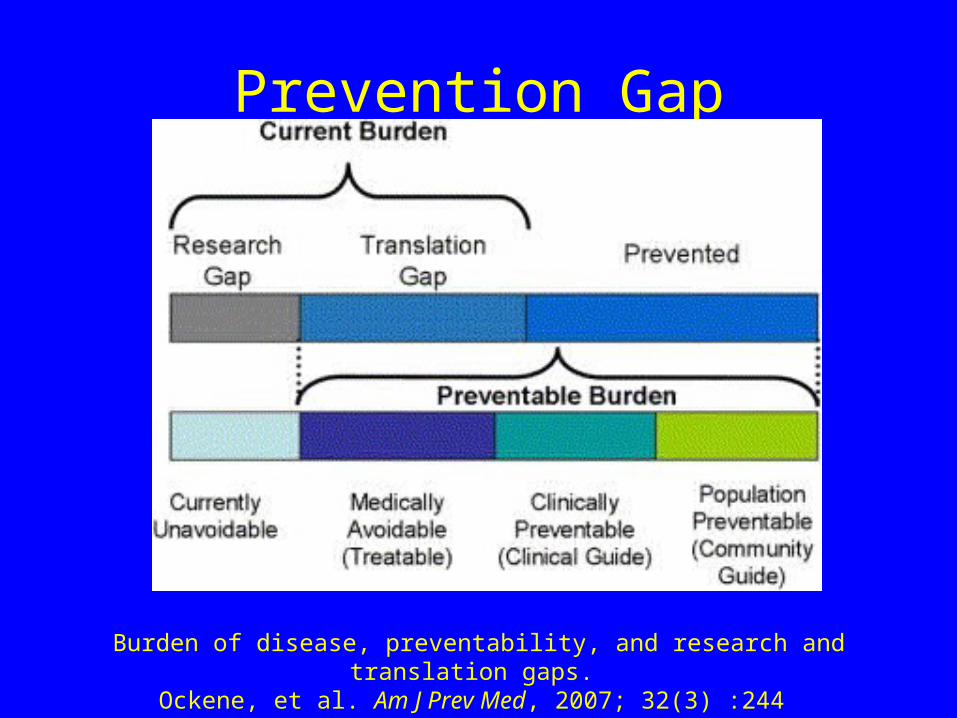
Prevention Gap
Burden of disease, preventability, and research and translation gaps. Ockene, et al. Am J Prev Med, 2007; 32(3) :244
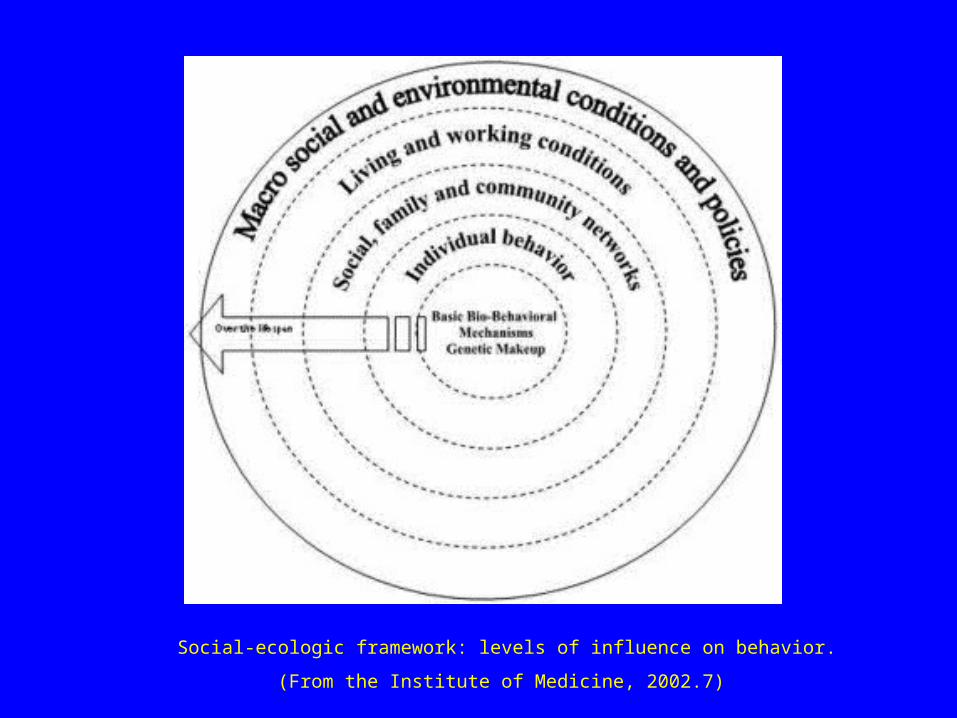
Social-ecologic framework: levels of influence on behavior.
(From the Institute of Medicine, 2002.7)
Payment for Health Services - US
• Public (26%)– Medicare (>65; 14%)– Medicaid (poor, disabled; 12% )
• Private – variety, diverse coverage; usually employer-based; (58% of Americans)
• Uninsured (16% of Americans)
Burden of Disease: 2020 Expected in Developed Countries
1. Ischemic heart disease2. Cerebrovascular disease3. Unipolar major depression4. Trachea, bronchi, lung cancers5. Road traffic injuries6. Alcohol misuse7. Osteoarthritis8. Dementia and related….
Murray CJL. Lancet, 1997
Pharma Promises…