j. coyle, ph.d. april 2016; 04/06/2016 wvsha...
TRANSCRIPT

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 1
Pneumonia & Common Pulmonary Diseases in Adults
James L. Coyle, Ph.D., CCC‐SLP, BCS‐S
University of Pittsburgh 1
West Virginia Speech Language and Hearing Association Annual Conference, Bridgeport WV April, 2016
Disclosure
• University of Pittsburgh (salary)
• WVSHA honorarium
• NIH RO‐1 (25% effort)
• No products
• Lots of biases favoring my patients
2
What are pneumonitis and pneumonia?
3
J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 2
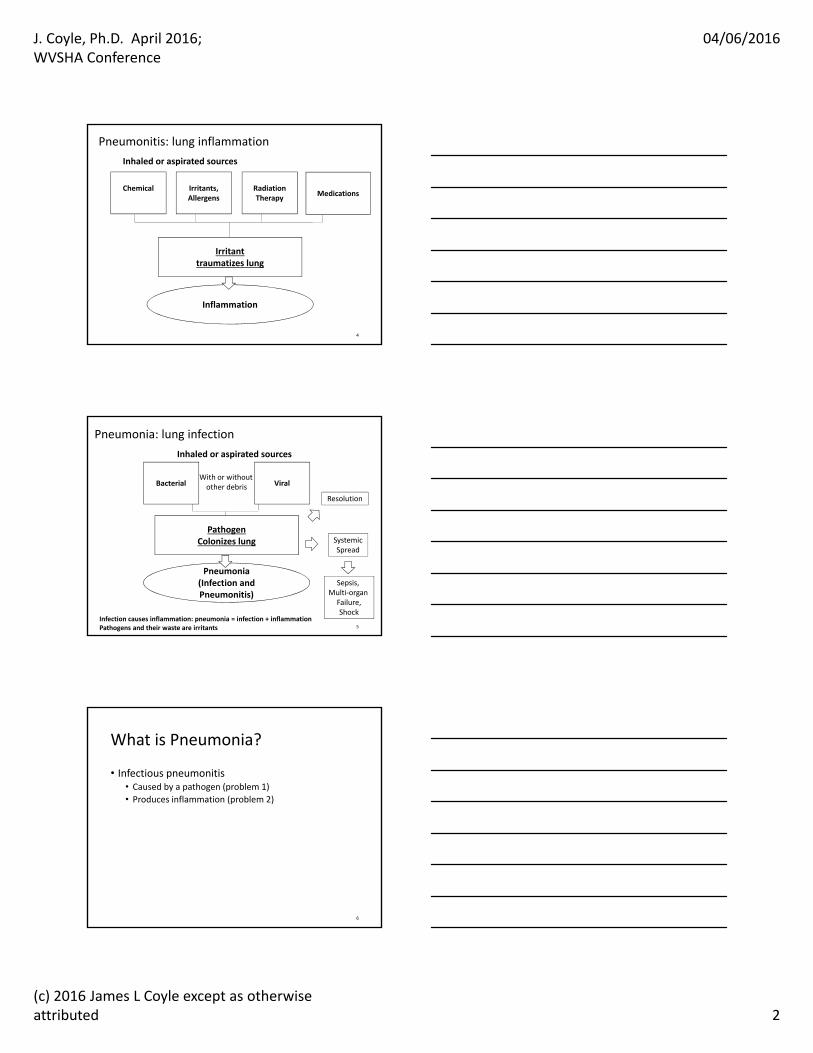
Pneumonitis: lung inflammation
Inflammation
ChemicalMedications
Irritanttraumatizes lung
Irritants,Allergens
RadiationTherapy
Inhaled or aspirated sources
4
Pneumonia: lung infection
Pneumonia (Infection andPneumonitis)
PathogenColonizes lung
Bacterial
Inhaled or aspirated sources
SystemicSpread
Resolution
Sepsis, Multi‐organ
Failure,Shock
ViralWith or withoutother debris
5
Infection causes inflammation: pneumonia = infection + inflammationPathogens and their waste are irritants
What is Pneumonia?
• Infectious pneumonitis• Caused by a pathogen (problem 1)
• Produces inflammation (problem 2)
6

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 3
Pneumonia
• Most frequent infectious cause of death*
• 40% higher incidence in elderly ** • #2 nosocomial infection (UTI) in hospitals***
• High case fatality rate• 55% (elderly)• Leading cause of mortality in children under 5****
Marston, et al., 1997*; National Center for Health Statistics, 2003**; ***Niederman, et al., 2002;****Baine et al., 2001; Almirall, et al., 2000 7
What is Pneumonia?
Capillary – RBC, WBC
O2
O2
O2
O2
O2O2
O2
CO2
CO2
CO2
CO2
O2 enters alveoli, diffuses to blood
CO2 diffuses to alveoli, is exhaled
Pathogen enters alveoli
Pathogen adheres to epithelium,produces waste, reproduces. Wasteproducts are irritants
Inflammation: alveoli become thick,noncompliant.
1. Inoculation, infection
8
Capillary – RBC, WBC
O2
O2
O2
O2
O2
O2
O2
CO2
CO2
CO2
CO2
Inflammation traumatizes respiratorymembrane making it excessively permeable.
Red blood cells leak into alveoli.
Volume of debris in alveoli increases
2. Inflammation, RBC leakage
9
J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 4
capillary
O2O2
O2
O2
O2
O2
O2
CO2
CO2
CO2
CO2
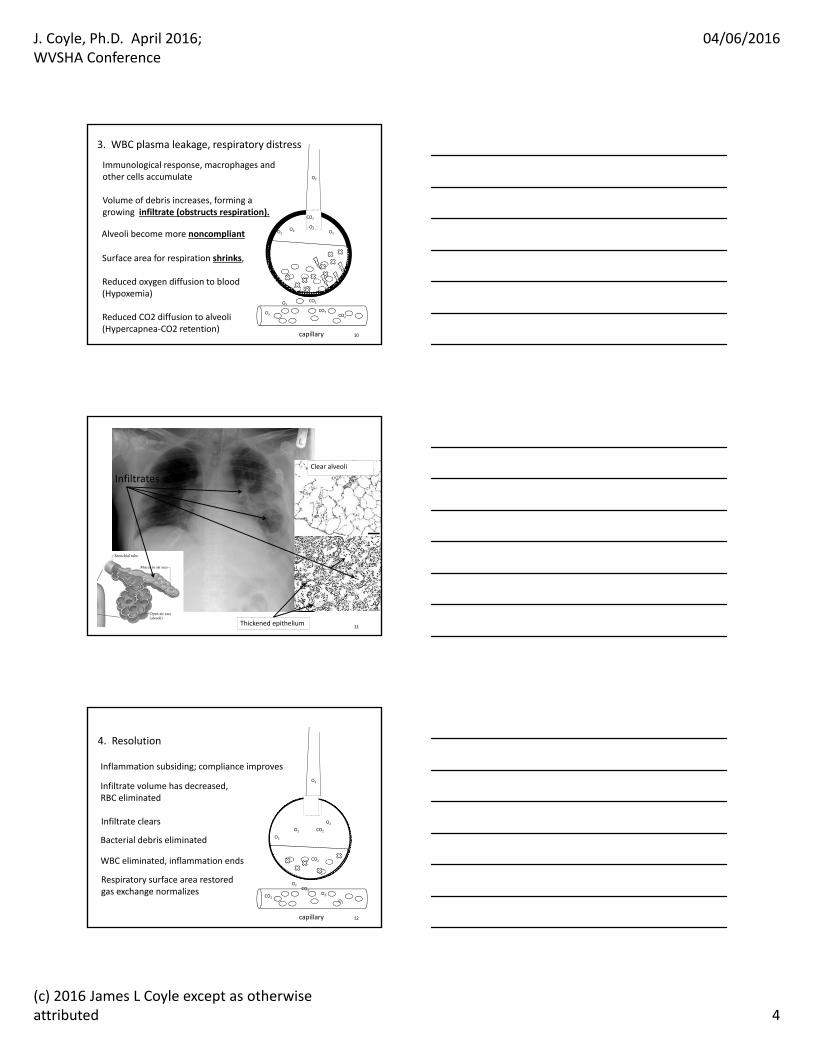
Alveoli become more noncompliant
Immunological response, macrophages and other cells accumulate
Volume of debris increases, forming a growing infiltrate (obstructs respiration).
Surface area for respiration shrinks,
Reduced oxygen diffusion to blood (Hypoxemia)
Reduced CO2 diffusion to alveoli(Hypercapnea‐CO2 retention)
3. WBC plasma leakage, respiratory distress
10
Clear alveoli
Thickened epithelium
Infiltrates
11
capillary
O2
O2
O2
O2
O2
O2
O2
CO2
CO2
CO2
CO2
Infiltrate volume has decreased,RBC eliminated
Inflammation subsiding; compliance improves
Respiratory surface area restoredgas exchange normalizes
WBC eliminated, inflammation ends
Infiltrate clears
4. Resolution
Bacterial debris eliminated
12

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 5
What is aspiration and how do lungs respond to aspiration?
13
Pneumonia/Pneumonitis
• Setting in which it began
• Pathogenic origin
• Mechanism• Aspiration
• Dysphagia‐related
• Non dysphagia‐related
• Hematogenous
• Iatrogenic: Direct Inoculation vs. Ventilator associated• Health care workers vs. sterilization errors
14
Pneumonia classification
• By setting• Community acquired pneumonia
• Aspiration, influenza, bug of the month
• Health care associated pneumonia• Aspiration, ventilator associated, HCW, contaminated equipment
15

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 6
Pneumonia classification
• By pathogen causing infection• Bacterial
• Streptococcal, staphylococcal, etc.
• Viral• Influenza, etc.
• Fungal, etc.
16
Pneumonia classification
• By anatomy• Bronchopneumonia• Lobar pneumonia
• Multilobar
• Diffuse, focal
17
Pneumonia classification
• By mechanism• Indirect ‐ HCW inoculation• Direct ‐ equipment contamination
• Hematogenous• Lung infected through circulatory system (sepsis)
• Aspiration• Dysphagia‐related• Non‐dysphagia‐related
18

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 7
Aspiration Pneumonia 15.5%
>Oropharyngeal>Gastric
DAPNon‐DAP
Typical
Pneumonia100%
CAPHospital Acquired
Pneumonia
VAPAtypical
Inhaled Pathogen
AspiratedPathogen
Non‐VAP
Inhaled Pathogen
19PEOPLE CAN ASPIRATE ANYWHERE: AP IS NOT SETTING SPECIFIC!Baine et al., 2001
Aspiration
• Solid or liquid matter• Not airborne, inhaled pathogen
• Courses by gravity, to its destination
• Crosses plane of true vocal folds
20
Aspiration‐destination• Entrance of liquid or solid matter into the respiratory system, below the vocal folds• Not airborne
• Aspirated material is gravity dependent
• Airborne is not
R L
RL
21

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 8
Lung response to aspiration: water
Inside alveolus
Plasma containing water inside capillary
RespiratoryMembrane
Water
H2O
H2O
H2O
H2O
RBC’s
WBC’s
Toward (L) heartFrom (R) heart
Capillary membrane
Alveolar membrane
Effros, et al., 2000 22
Inside alveolus
RespiratoryMembrane
Chemical irritant
Lung response to aspiration: pathogens and particulate matter
RBC’s
WBC’s
Plasma containing water inside capillary
Toward (L) heartFrom (R) heart
H2O H2O plasma H2O
Capillary membrane
Alveolar membrane
infiltrate
Chemical pneumonitis 23
Dysphagia‐related Aspiration Destinations
Aspiration produces pneumonitis or pneumonia in gravity dependent portions of lung(s).“Dependence” depends on posture when aspiration occurs, density & volume aspirated.
(R) Basilar infiltrates (R) Upper lobe infiltrates
24Marik, 2001

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 9
What is aspiration pneumonia?
• …and what other types of pneumonia are there?
25
Aspiration Pneumonias
• Dysphagia‐related AP (DAP)• Pathogen in solid or liquid matter• Courses by gravity, to its destination• Not airborne, inhaled pathogen• Incidence: 11%; 15.5%, 22% (*)• Dysphagia!• Oral pathogens typically
• Colonization of oral cavity
26Robbins et al., 2008; Baine et al., 2001; Langmore et al., 1998
Other Aspiration Pneumonias
• Non‐dysphagia related AP (NDAP)• Aspiration pneumonia NOT FROM THE MOUTH
• Colonized emesis
• Gastroesophageal esophagopharyngeal reflux
• Esophageal motility disorder
• Oral pathogens • that survive in stomach
• Or from esophagus
27

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 10
Community Acquired Pneumonia (CAP)
• Pneumonia not acquired in a health care facility• Mechanism: aspiration or other
• 4‐5 million cases per year* **• 600,000 hospitalizations, 45,000 deaths**
• Incidence**• 12 per 1000 persons• 20 per 1000 elderly persons (60% greater)
• Common pathogens• Typical: Streptococcus, Klebsciella pneumoniae
• Atypical *: H. influenzae, RSV, Legionella, E. coli, Staph. aureus, others
*Niederman, 2002; **Mandell & Wunderink, 200728
Other Types of Pneumonia• Ventilator Associated Pneumonia
• Exposure to mechanical ventilation• Contaminated respiratory circuits
• Contaminated suction, bronchoscopic equipment
• Aspiration of oral secretions while sedated
• Gastroesophageal reflux common in ventilation• Early, late onset
• Early: typically CAP pathogens• Late: MRSA, other drug‐resistant pathogens
29
Other Types of Pneumonia
• Respiratory Syncitial virus (RSV)• Viral, common in children (day care)
• Legionella pneumonia
• Hematogenous pneumonia: sepsis• AKA SIRS
• Systemic inflammatory response syndrome
• Lung infected by bloodborne pathogen
30

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 11
Sepsis
Infection and sepsis
• Infection• Pathogenic Organism…
• Organism that causes disease in host organ
• … enters and occupies host organ/tissue …
• … draws nutrients from host and damages tissue …
• … reproduces and generates metabolic waste …
• … organism, offspring, waste, are all IRRITANTS …
• … blood organ barrier disrupted …
• … organism enters circulatory system = SEPSIS
• … process repeats in other organs …
• Depending on organ … effects of infection … ???
32
Infection and sepsis
• Sepsis = septicemia = bacteremia (if bacterial)• Pathogen Damage to vascular structures, organs
• Leakage of fluid from blood vessels
• Hypotension • Organs need adequate blood pressure to function
• Organ metabolic failure
• Hypotensive shock• Multi‐organ hypotensive failure (high mortality)
• Organism infecting other organs• Example: UTI sepsis hematogenous pneumonia
33

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 12
Infection and sepsis
• Typical scenarios• 1. Urinary tract infection
• Bladder ureters kidneys blood spread
• 2. Pneumonia• Airway alveoli pulmonary capillaries spread
• 3. Wound infection• Local wound tissue capillaries blood spread
• Progression• Typically insidious in first days
• Patient may not develop sudden signs
34
Infection and sepsis
• Effects of sepsis• Depends on organs affected: Examples …• Brain and CNS
• Progressive lethargy reduced oral intake dehydration more lethargy more reduced intake more dehydration …
• Urinary system• Impaired filtration accumulated [organ] metabolic waste impaired nervous system and other organ function• Metabolic acidosis
• Example to illustrate• E. coli, pneumococcus in blood culture
35
Sepsis
• The challenge in sepsis…• Acute mental status changes affect sensorimotor function
• Patient is impaired
• SLP examines patient• Patient performs poorly; diagnoses “dysphagia”
• Pulmonary infection now presumed to be ASPIRATION‐RELATED
• Association sticks and becomes a permanent part of the record
• Patient has permanent “history of aspiration pneumonia”
36

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 13
Sepsis• Assessment considerations
• Stage of recovery
• Organs affected
• Pulmonary damage: alveolar noncompliance, debris from infiltrates ALL • Increase respiratory rate
• Muscle damage• weakness, increased respiratory rate
• Brain damage• Cognitive impairments after sepsis
• Patient endurance
• Weakness
• Effects of prolonged mechanical ventilation
• Depends on what organs suffered what damage…
Aspiration Pneumonitis(chemical pneumonitis)
• Non‐Infectious‐chemical trauma• Acute Lung Injury: caustic or particulate aspiration
• Inflammation of alveoli by effects of irritants• No primary infection
• Inflammatory edema reduces surface area
• Gastric contents• Sterile, acidic, caustic• Damage to airways, alveoli
39

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 14
ARDS
Ware & Matthay, 2000
Normal acute resolution
40
Other Respiratory Diseases
41
Categories
• Obstructive Diseases• Inspired air is obstructed from the respiratory membrane• Obstructed gas exchange• Respiratory pump works
• Restrictive Diseases• Airflow or volume is mechanically restricted• Gas exchange is intact• Patient cannot inhale sufficient volume
42
J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 15
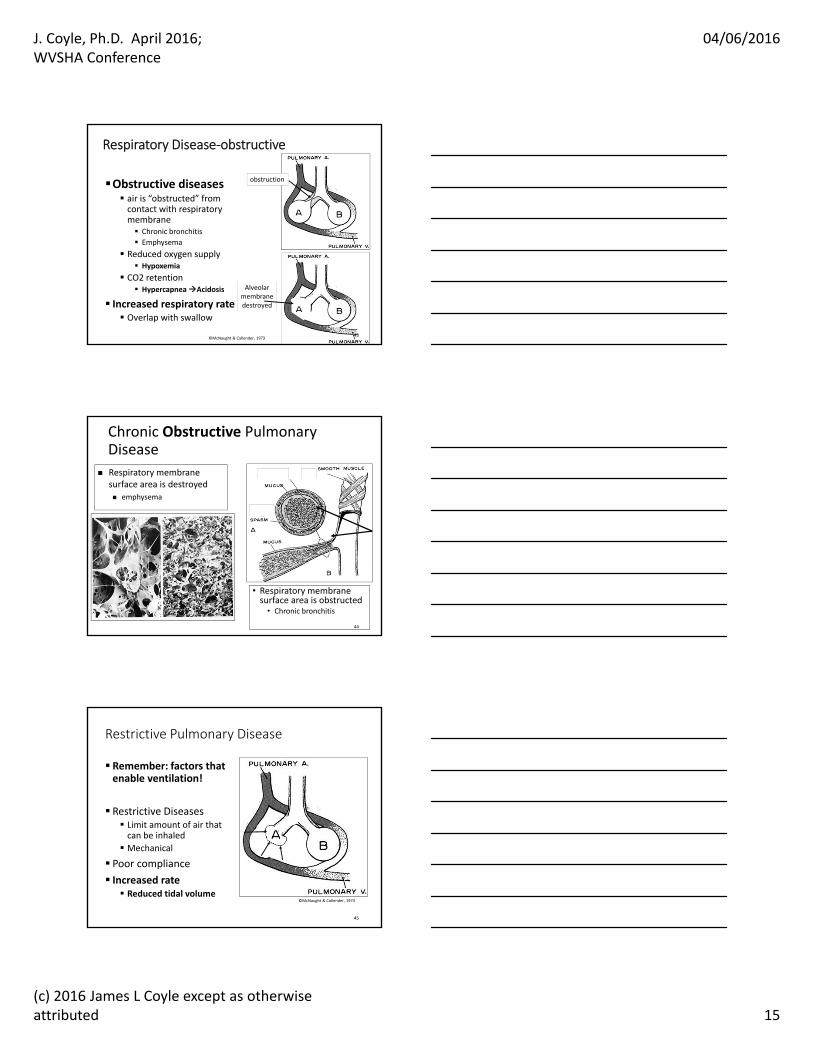
Respiratory Disease‐obstructive
Obstructive diseases air is “obstructed” from contact with respiratory membrane Chronic bronchitis
Emphysema
Reduced oxygen supply Hypoxemia
CO2 retention HypercapneaAcidosis
Increased respiratory rate Overlap with swallow
obstruction
Alveolarmembranedestroyed
43©McNaught & Callender, 1973
Chronic Obstructive Pulmonary Disease
• Respiratory membrane surface area is obstructed• Chronic bronchitis
Respiratory membrane surface area is destroyed emphysema
44
Restrictive Pulmonary Disease
Remember: factors that enable ventilation!
Restrictive Diseases Limit amount of air that can be inhaled
Mechanical
Poor compliance
Increased rate Reduced tidal volume
45
©McNaught & Callender, 1973

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 16
Mechanically restrictive
• Disable expansion of alveoli• Pulmonary non‐compliance
• Pulmonary fibrosis
• Atelectasis• Pneumothorax
• Reduced surfactant production
• Disable expansion of thoracic cavity• Kyphosis
• Abnormally flexed thoracic spine, compressed thorax
• Tough, leathery segments tether adjacent segments
• Paralysis
46
Kyphosis
47
Pneumothorax
• Perforation of pleural membrane• Destroys intrapleural vacuum that holds lung open
Subatmospheric pressure
Pleural cavity
Atmospheric pressure48

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 17
Pneumothorax
© en:User:Clinical Cases
© Hellerhoff
49
Atelectasis Areas of collapsed alveoli Compressive, dependent, adhesive, obstructive
Restrictive Pulmonary Disease
50
CHF
• Both obstructive…• Pulmonary edema
• Fluid leaks into alveoli due to pulmonary hypertension
• Obstructs respiratory membrane diffusion
• And restrictive components• Pleural effusions• Fluid surrounds lung, prevents inflation
51

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 18
Pleural effusion• Fluid filling parts of pleural cavity
• Preventing lung expansion during inspiration
• Gravity dependent “bag of water”
Pleural cavity
52
CHF (transudative), Inflammatory (exudative)53
Pleural Effusion
Pulmonary vascular congestion
• Incoming arterial flow obstructed
• Blood “backs up” – casts shadow on image
Pulmonary hypertension54
Pulm. artery Pulm. vein
Obstructed flow

J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 19
Pulmonary edema
Pulmonary hypertension55
Pulmonary Edema
56
Iatrogenic causes of respiratory conditions
• Iatrogenic condition: a disease cause by treatment of another disease• Sedation (restrictive)
• CNS depression
• Disruption of pleural linkage (restrictive)• Cardiothoracic surgery
• Phrenic nerve injury (restrictive)• Cardiothoracic surgery
• Vagal injury (obstructive: vocal fold paralysis)
57
J. Coyle, Ph.D. April 2016; WVSHA Conference
04/06/2016
(c) 2016 James L Coyle except as otherwise attributed 20
Summary
• Pulmonary disease affects swallow/breathing coordination
• Pulmonary disease can cause dysphagia• Mainly characterized by disruption of swallow‐respiratory coordination
• Pulmonary disease can be caused by dysphagia
• Pneumonia and dysphagia are related but not married!
58
59
Questions?
Thank you!