jfa purple orange - act office of the senior … · web viewa public discussion paper prepared...
TRANSCRIPT

A public discussion paper prepared for the ACT Government, to assist public consultation
An overview of restrictive practices, and the key issues for consideration in relation
to the establishment of an Office of the Senior Practitioner

Acknowledgment
We gratefully acknowledge the assistance of the following persons who contributed ideas
and perspectives as part of a co-design process for the development of this paper.
Christina Ryan CEO, Advocacy For Inclusion
Fiona May - Chief Executive Officer, ADACAS
Helen Watchirs, President, ACT Human Rights Commission
Gabrielle McKinnon, ACT Human Rights Commission
Jan Kruger, Director, Imagine More
Robert Altomare, Executive Officer PWD ACT
Steve Fox Manager NDS in ACT
Simon Viereck - Executive Officer Mental Health Community Coalition ACT
Charlie Richardson, Mental Health Community Coalition ACT
Richard Bruggemann, Senior Practitioner, Disability SASue Salthouse - WWDACT
Susan Helyar Director, ACTCOSS
Agency details
JFA Purple Orange
104 Greenhill Road
Unley SA 5061 AUSTRALIA
Telephone: + 61 (8) 8373 8333
Fax: + 61 (8) 8373 8373
Email: [email protected]
Website: www.purpleorange.org.au
Facebook: www.facebook.com/jfapurpleorange
JFA Purple Orange is a non-government, social profit organisation. Anchored on dialogue with people living with disability, their families, service providers, government and other stakeholders, we seek to identify policy and practice that has the prospect of advancing peoples chances of a good life. Our work is anchored on the principles of Personhood and Citizenhood. Our work includes research, evaluation, capacity building, consultancy, and hosted initiatives.ISBN: 978-0-9804509-4-1January 2017.
1

Table of contents
1.0 Purpose of this discussion paper..................................................................32.0 Introduction to the issue..............................................................................33.0 Defining restrictive practice and its consequences......................................54.0 Who is affected by the use of Restrictive Practice.......................................85.0 Considering the alternatives........................................................................96.0 Variations across Australia in responses to restrictive practices................10
6.1 Victoria....................................................................................................116.2 Tasmania................................................................................................116.3 South Australia........................................................................................116.4 NSW........................................................................................................126.5 Queensland.............................................................................................126.6 NT...........................................................................................................136.7 WA..........................................................................................................13
7.0 The National Disability Insurance Scheme.............................................................138.0 The extent of the issue in the ACT.............................................................149.0 Considerations on how an ACT Office of the Senior Practitioner be might be arranged..............................................................................................................1710.0 Parameters for Public Consultation............................................................19
10.1 Principles underpinning the consultation................................................1910.2 Key elements of proposed consultation..................................................1910.3 Key questions to be explored through the consultation..........................20
11.0 Next steps..................................................................................................21
2

1.0 Purpose of this discussion paperThe purpose of this discussion paper is to assist a community consultation on how an Office of the Senior Practitioner might operate in the ACT. The discussion paper gives an overview of what is meant by restrictive practices, the extent to which such practices are an issue in the ACT, and how these issues might be addressed through an Office of the Senior Practitioner.
From late January to early March 2017 there will be a range of opportunities for people to give their views about this. It is hoped this discussion paper helps people to consider the issues and what they would like to say.
This discussion paper carries a range of detailed questions for the community consultation, that in
summary explore:
The ways that restrictive practices might be regulated in the ACT, so that they are reduced
and replaced by alternatives
The ways that organisations can develop their skills in using alternatives to restrictive prac-
tices
How an Office of the Senior Practitioner could help
Where an Office of the Senior Practitioner could be located (e.g. could it be standalone, or
attached to an existing organisation), and how it would link with existing arrangements in
the ACT that aim to protect people’s rights and safeguard people from harm
2.0 Introduction to the issue Some groups in the ACT community, including people with disability, older people, people living with mental illness, children and young people, and people intersecting with the justice system are more likely to be subjected to restrictive practices to manage behaviours that are perceived as challenging. Restrictive practices form a continuum of limitations of a person’s human rights and freedoms, with some restrictive practices such as seclusion, physical and mechanical restraint and the forcible giving of medication being of particular concern as they severely limit individuals’ rights and freedoms.
Except in emergency situations where necessary to prevent immediate harm to the person or oth-ers, seclusion and restraint are unlawful if used without legal authority. Current evidence indicates that the psychological and physical impact of seclusion and restraint is overwhelmingly negative. The need for these practices can be reduced and often eliminated through evidence-based, preventative approaches, along with increased support for services, and measures to improve their accountability and monitoring.
In relation to disability, the Commonwealth, State and Territory Disability Ministers endorsed the National Framework for Reducing and Eliminating the Use of restrictive practices in the Disability Service Sector at the Disability Reform Council meeting on 21 March 2014 (https://
3

www.dss.gov.au/sites/default/files/documents/04_2014/national_fraemwork_restricitive_prac-tices_0.pdf).
The National Framework focuses on the reduction of the use of restrictive practices in disability ser -vices that involves restraint (including physical, mechanical or chemical) or seclusion. It aims to con-tribute to the promotion and full realisation of all human rights for people with disability, including liberty and security of the person and freedom from exploitation, violence and abuse, in accordance with Articles 14 and 16 of the United Nations Convention on the Rights of Persons with Disabilities (CRPD).
The implementation of restrictive practice oversight functions in the ACT forms part of the commit-ment to the above framework, as well as to the National NDIA Quality and Safeguards Framework, currently under development by Commonwealth, State and Territory Governments.
The ACT Government is committed to improving the lives of people with a disability, as well as sup-porting and upholding their human rights. The ACT is the first jurisdiction to transition to the Na -tional Disability Insurance Scheme (NDIS), and by the end of 2016, will be at full scheme rollout. Alongside this important social policy shift to participant “choice and control” over their support ar -rangements, the ACT has strengthened its quality assurance and oversight functions, to ensure that participants can access high quality specialist disability support, and that support providers are com -pliant with national standards. This is achieved through the Disability Services Act 1991 (ACT), associ-ated regulations, and the establishment of the ACT Human Services Registrar. The second piece of work in supporting specialist quality services is the establishment of restrictive practices oversight within the ACT.
The ACT Government recognises that the proposed regulation of restrictive practices for people with disability represents additional oversight for providers of support and additional protection for people with disability.
Given the role of the ACT Human Services Registrar (HSR) in monitoring and oversight of specialist disability services in the ACT, the HSR will lead the development work for ACT Government. The HSR forms part of the Regulation, Oversight and Quality Services (ROQS) team in the Complaints, Quality and Regulation Branch of the ACT Government Community Services Directorate, and is responsible for a range of quality assurance, compliance and complaints monitoring functions.
While the NDIS has provided a large focus on what currently happens to people living with disability, including issues of quality and safeguarding, it is clear that the issue of restrictive practices extends to broader groups in the ACT. Therefore, it is important to contemplate the extent to which there are restrictive practices, and how these might be reduced, in relation to older people, people living with mental illness, and children and young people.
4

3.0 Defining restrictive practice and its consequences
Many people are living with increased vulnerability. These include people whose circumstances cre -ate concerns in others that the person’s actions may cause harm (or other types of perceived disrup -tion) to themselves or others.
In response, conventional service systems sometimes generate ‘support arrangements’ that involve restrictions on the person’s movements and decisions. These are referred to as restrictive practices.
In the NDIS Quality and Safeguarding Framework Consultation Report, the authors offer the follow -ing definition:
A restrictive practice is any intervention which restricts the rights or freedom of move-
ment of a person with disability who displays challenging behaviours, where the primary
purpose of that intervention is to protect them or others from harm.1
Also, the definition from the National Framework for Reducing and Eliminating the Use of Restrictive Practices in the Disability Service Sector is:
A “restrictive practice” is defined as any practice or intervention that has the effect of re-
stricting the rights or freedom of movement of a person with disability, with the primary
purpose of protecting the person or others from harm. 2
Given that restrictive practices can affect a broader population of vulnerable people than just those living with disability, the Government of South Australia offers this definition:
Restrictive practices refer to any practice, device or action that removes or restricts an-
other person’s freedom, movement or ability to make a decision. This includes detention,
seclusion, exclusion, aversive restraint, chemical restraint, physical restraint, mechanical
restraint, environmental restraint and psycho-social restraint. Restrictive practices do
not include therapeutic or safety devices/practices, where the device or practice is being
used for its intended purpose and the person is not resisting or objecting to its use3.
1 NDIS Quality and Safeguarding Framework DSS Consultation Report August 2016, https://engage.dss.gov.au/wp-content/uploads/2015/11/consultation_report_ndis_quality_safeguarding_framework.pdf
2 Australian Government (2013) National Framework for Reducing and Eliminating the Use of Restrictive Practices in the Disability Service Sector
3 SA Government DCSI Safeguarding People with Disability Overarching Policy DIS/366 – POL-SER-002-2013
5

For the purpose of this project, this discussion paper proposes the above definition be used.
Restrictions can include (but are not necessarily limited to):
mechanical, such as devices that limit a person’s movements (and this includes the removal
and/ or disengagement of mechanical supports that assist the person’s movements)
seclusion, such as the sole confinement of a person at any time in any room where the doors
and windows cannot be opened by that person
environmental, such as preventing free access to all parts of a person’s environment or
house (for example locking the refrigerators)
social, such as the imposition of sanctions that restrict the person’s access to relationships/
opportunities they value
chemical, such as medications that blunt the person’s emotions, cognition, and motor activ-
ity
physical, such as holding or ‘pinning down’ by another person
psycho-social restraints, such as power control strategies4 which might include threats,
intimidation, fear, coercion, discipline, or retaliation
organisational, such as excluding the person from activities, and restrictions to the person's
choice
communication restraint, such as switching off someone’s communication device
decision making restraint, such as failing to provide options for supported decision making
While taking action to avert a clear and present risk of harm is understandable, there are a number of problems with the imposition of restrictive practices. These include (but are not necessarily lim -ited to):
the negative consequences the restrictive practice by its nature can have on the person’s
progress towards good life chances, their general well-being, physically and psychologically
including the impact on self-esteem
4 Power-control strategies’ are defined in South Australia’s Safeguarding People with Disability Restrictive Practices Policy
as “the use of power-control strategies to influence a person’s behaviour. This includes but is not limited to directing the
person’s behaviour through voice tone, commands or threats and the use of punishment, including ignoring the person
and withholding basic human rights, such as positive social interaction, personal belongings or a favoured activity.”
6
restrictive practices that are focused on behaviour suppression as opposed to supporting
genuine positive behaviour change
restrictive practices that are focused on a negative reinforcement paradigm (the use of pun-
ishment to extinguish an unwanted behaviour, as opposed to positive reinforcement
paradigms that focus on rewarding the emergence of behaviour choices that can advance
the person’s life chances)
restrictive practices that are inadequate in terms of their conceptualisation and implementa-tion
restrictive practices that are inadequate in terms of a clearly defined timeframe and process
for review
restrictive practices that constitute an assault on the person’s human rights
restrictive practices that are crafted and/or executed by staff with inadequate skills and per-
spective.
It is recognised that the use of restrictive practices may not always be intentional but that actions taken, or not taken, inadvertently have the effect of restricting a person’s preferences and actions, and/or contravening their rights. The person using the restrictive practice may argue that there is no malicious intent and that it is just the way that things are done. However, this is not an adequate defence for the continuation of such practices.
While the imperative to reduce restrictive practices is relevant to a wide range of vulnerable people, we can by example look at specific signals for the disability community.
The United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) includes a num-ber of articles that each have clear implications for avoiding restrictive practices, including Article 12 (Equal Justice before the Law), Article 15 (Freedom from Torture or Cruel, Inhuman or Degrading Treatment or Punishment), Article 16 (Freedom from Exploitation, Violence and Abuse), Article 17 (Protecting the Integrity of the Person), Article 18 (Liberty of Movement and Nationality).
The United Nations Committee on the Rights of Persons with Disabilities has stated that it “is con-cerned that persons with disabilities, particularly those with intellectual impairment or psychosocial disability, are subjected to unregulated behaviour modification or restrictive practices such as chem-ical, mechanical and physical restraints and seclusion, in various environments, including schools, mental health facilities and hospitals.
The Committee recommends that “the State party take immediate steps to end such practices, in-cluding by establishing an independent national preventive mechanism to monitor places of deten -tion—such as mental health facilities, special schools, hospitals, disability justice centres and prisons—in order to ensure that persons with disabilities, including psychosocial disabilities, are not subjec-ted to intrusive medical interventions.”5
5 Committee on the Rights of Persons with Disabilities, above n 5, [35]–[36]. Referenced in Australian Law Reform Commission’s paper Equality, Capacity and Disability in Commonwealth Laws
7

This raises the question about what types of restrictive practices are acceptable, and in what circum -stances. There may be a range of views about what might constitute the threshold for using restrict-ive practices, what types of restrictive practices are permissible, and under what terms. In the NDIS landscape, it is critical that organisations understand the importance of implementing strategies to reduce the use of restrictive practices in human services, because restrictive practices by their nature reduce a person’s control and choice and impede a person’s access to valued roles in com -munity life.
Again considering specific circumstances the people living with disability, the National Framework for Reducing and Eliminating the Use of Restrictive Practices in the Disability Service Sector states that “Restrictive practices should only be used where they are proportionate and justified in order to protect the rights or safety of the person or others.”
The National Framework goes on to state, “disability service providers should seek to understand the nature and function of a person’s behaviour and to respond appropriately to that behaviour, ensur-ing the use of restrictive practices in very limited and specific circumstances and only as a last re -sort.” 6
It can be assumed that there are comparable imperatives for other vulnerable demographics.
4.0 Who is affected by the use of Restrictive Practice
There are a range of people within the ACT community who may be affected by the use of Restrictive practice. These include (but are not necessarily limited to), the following:
Children and adults living with disability Children and young people who have experienced trauma in the family home, or in
separation from the family home, or in settings that substitute the family home Older people People experiencing enduring and episodic mental illness People in justice-related custodial settings.
5.0 Considering the alternativesGiven the above challenges associated with the purpose and consequences of restrictive practices, there is a clear imperative to build a more positive context for how people are supported, particu-larly people most at risk of a service provider using restrictive practices in their support arrange -ments. Typically this is anchored on two main phases:
1) Understanding the reasons
https://www.alrc.gov.au/sites/default/files/pdfs/publications/whole_dp81.pdf6 Australian Government (2013) National Framework for Reducing and Eliminating the Use of Restrictive Practices in the Disability Service Sector
8

Where a person may be at risk of a service agency putting restrictive practices in place, it is of critical importance the service agency deepen its understanding of the person. This is particularly so if there are concerns about the person placing themselves at risk, or placing others at risk, damaging property or being labelled in some way as disruptive.
It is important because people do things for a reason, and getting to know the person and their story will assist the agency in finding alternatives to restrictive practices.
Deeper insight to the person will better reveal the person’s choices and preferences, and will also re-veal the extent to which the person’s current daily life is missing the opportunities that are meaning -ful to the person which bring that person into valued membership of community.
In their nature, restrictive practices undermine a person’s choices and preferences, and can also un-dermine a person’s chances of rich and meaningful life.
Alternatives to restrictive practices might include making changes to the person’s support arrange-ments, home arrangements, etc, that better reflect the person’s choices and preferences.
2) Building a positive alternative
There may be circumstances where people remain concerned about the person even where support arrangements better reflect the person’s preferences and typical goals of community life, and where elements of restrictive practices are contemplated to manage acute situations where safety is a central issue.
In such situations, any restrictive practices need to be used sparingly, and always in the context of al-ternative types of support that preserve the person’s preferences and life chances.
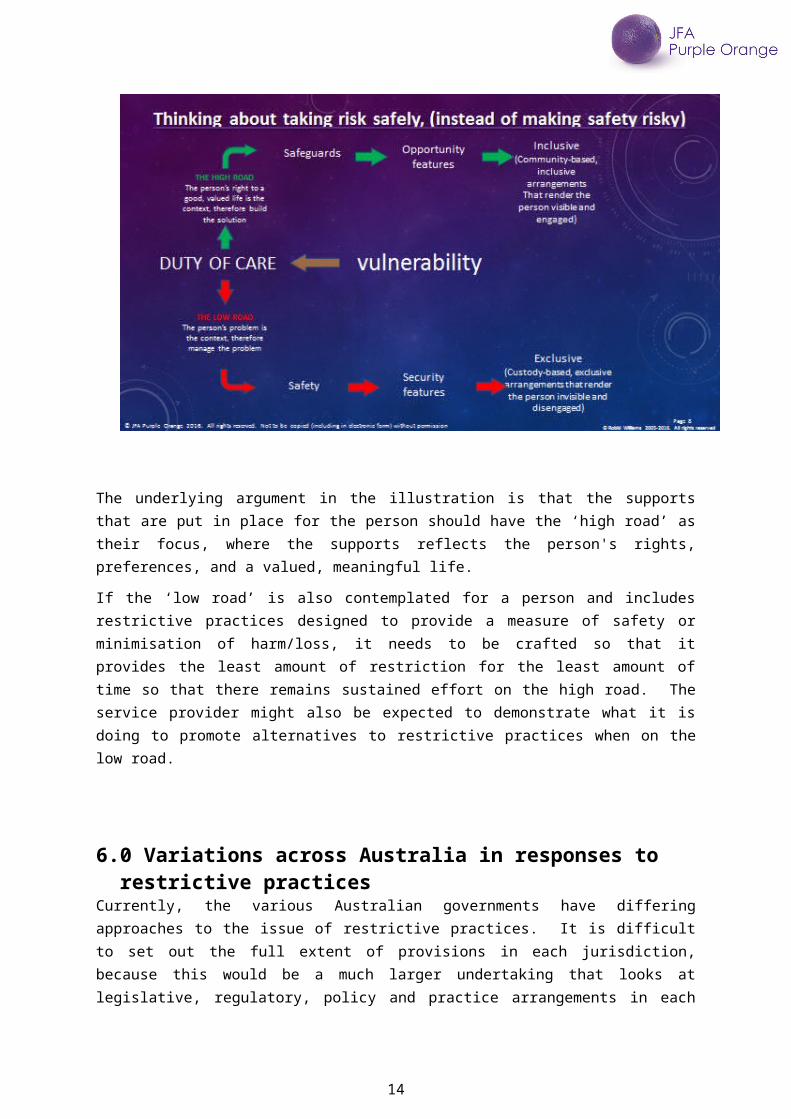
This is illustrated in the following slide, which sets out the ‘high road’ and ‘low road’ responses to perceived vulnerabilities.
9

The underlying argument in the illustration is that the supports that are put in place for the person should have the ‘high road’ as their focus, where the supports reflects the person's rights, prefer -ences, and a valued, meaningful life.
If the ‘low road’ is also contemplated for a person and includes restrictive practices designed to provide a measure of safety or minimisation of harm/loss, it needs to be crafted so that it provides the least amount of restriction for the least amount of time so that there remains sustained effort on the high road. The service provider might also be expected to demonstrate what it is doing to pro -mote alternatives to restrictive practices when on the low road.
6.0 Variations across Australia in responses to restrictive practices
Currently, the various Australian governments have differing approaches to the issue of restrictive practices. It is difficult to set out the full extent of provisions in each jurisdiction, because this would be a much larger undertaking that looks at legislative, regulatory, policy and practice arrangements in each jurisdiction. In addition, these arrangements would then need to be unpacked in terms of the extent to which they apply to one or more of different demographics such as mental-health, dis -ability, older persons, children and young people, people in touch with the justice system, and also across a range of public service areas such as human rights, education, health, etc. In short, there is complexity.
We note the Australian Law Reform Commission's recommendation that because of the range of variation across the Australian jurisdictions, there is a case for a common framework7.
7 Australian Law Reform Commission’s paper Equality, Capacity and Disability in Commonwealth Lawshttps://www.alrc.gov.au/sites/default/files/pdfs/publications/whole_dp81.pdf
10

Here follows a brief summary of the extent to which other Australian states and territories have spe -cific provisions for managing restrictive practices.
6.1 VictoriaIn Victoria, the Senior Practitioner (Disability) is responsible, under the Disability Act 2006, for ensur-ing that the rights of persons who are subject to restrictive practice are protected and that appropri -ate standards are complied with.
The Senior Practitioner does this by way of:
educating service providers
facilitating knowledge and training
monitoring the use of restrictive practice in disability services.
The Senior Practitioner can:
visit and inspect any disability service
investigate any use of restrictive practice
direct a service provider to stop using a restrictive practice.
Victoria also has the Restrictive Intervention Data System (RIDS) which has been developed to record and report events of routine, PRN or emergency restrictive interventions such as chemical restraint, mechanical restraint or seclusion.
6.2 TasmaniaIn Tasmania the Senior Practitioner is appointed by the Secretary of the Department of Health and Human Services (DHHS) under the Disability Services Act 2011.
The Senior Practitioner gives:
advice to the Department and the Guardianship and Administration Board about the use of restrictive practice
develops guidelines and standards
provides accessible information about the rights of people with disability.
The Senior Practitioner can visit service providers and look at how and why a restrictive practice is being used.
6.3 South AustraliaIn South Australia, the Office of the Senior Practitioner sits within the Department of Communities and Social Inclusion (DCSI).
The Senior Practitioner works to reduce the use of restrictive practices through:
11

awareness raising and training
by promoting positive behaviour support practices.
It has a key focus on the minimisation and where possible, elimination of restrictive practices within disability services.
The Senior Practitioner is finalising procedures to ensure disability service providers are responsible for accurate recording and reporting of the use of restrictive practices by maintaining a register and recording every use of restrictive practice.
Under section 32 of the Guardianship and Administration Act 1993, an order by the SA Civil and Ad -ministrative Tribunal is required authorizing a restrictive practice where a person does not have mental capacity to consent.
6.4 NSWIn NSW the Office of the Senior Practitioner Ageing, Disability and Home Care sits within the Depart -ment of Family and Community Services NSW.
The Senior Practitioner provides leadership and coordination of services for people with complex needs and challenging behaviour.
The use of restrictive practices in NSW is essentially governed by the Department’s behaviour Sup-port Policy and Practice manual with main principles governing rights of people with disability in the Disability Inclusion Act 2014.
6.5 QueenslandQueensland does not have an Office of the Senior Practitioner. On 1 July 2014, new legislation (amendment to Disability Services act 2006) came in to place to ensure the use of positive behaviour support and to protect clients who may be subject to restrictive practices.
The new laws also make it easier for disability service providers to meet their legal obligations, while increasing their accountability around the use of restrictive practices. Additionally, the changes in -clude streamlined processes to allow service providers to focus on supporting their clients.
The new process entails five steps for disability service providers. The approvals process depends on what type of restrictive practice is being used and whether it is a short-term or long term response:
Step 1 – develop a positive behaviour support plan
Step 2 – identify any restrictive practices in use
Step 3 – provide the adult and stakeholders with a statement about the use of restrictive practices
Step 4 – make a short-term approval application(where there is an immediate and serious risk of harm) to the Public Guardian or the Chief Executive, Department of Communities, Child Safety and Disability Services
12

Step 5 – seek approval from Queensland Civil and Administrative Tribunal (QCAT) for long term use, implement and review the plan.
The Queensland Government has committed to delivering training programs throughout the state through the Centre of Excellence for Clinical Innovation and Behaviour Support.
6.6 NTThe Northern Territory does not currently have an Office of the Senior Practitioner. The regulation of restrictive practice is contained within the Disability Services Act 2015
6.7 WAWA does not have an Office of the Senior Practitioner. Regulation is through the Disability Services Act 1993 and the Code of Practice for the elimination of Restrictive Practices.
7.0 The National Disability Insurance SchemeWhile this paper contemplates a broader range of demographics, it is clear that restrictive practices are a significant concern to the disability sector and disability community, and so any arrangements in the ACT will need to contemplate the extent of any parallel arrangements emerging nationally in disability reform, especially in relation to the rollout of the National Disability Insurance Scheme (NDIS).
The Commonwealth Department of Social Services has been leading the consideration of NDIS Qual -ity and Safeguarding Framework. Arrangements are not yet resolved, however a consultation report from 2015 provides useful signals about stakeholder sentiments, and which could be considered in relation to an ACT Office of the Senior Practitioner.
The consultation report, National Disability Insurance Scheme Quality and Safeguarding Framework Department of Social Services Consultation Report, records the findings of the national consultation about a proposed structure for an NDIS Quality and Safeguarding Framework. The consultation, which included public meetings, other forums and written submission, included a number of ACT stakeholders.
The consultation report included a specific section on restrictive practices. This included considera-tion of how restrictive practices should be authorised. The authors noted there was strong support for there being an independent decision maker who would authorise the use of restrictive practices, and that this independent decision maker might be an independent officeholder such as a Senior Practitioner.
The consultation also explored how restrictive practices should be reported. Most stakeholders were in agreement there should be mandatory reporting of emergency use of restrictive practices and of one-off reporting where a support plan includes a restrictive practice. However, some stakeholders felt these arrangements should go further and include routine reporting on each occasion where physical, chemical, mechanical and secluding restrictive practices were being used.8
8 National Disability Insurance Scheme Quality and Safeguarding Framework Department of Social Services Consultation Report (2015) ARTD Consultants.
Accessed at https://engage.dss.gov.au/ndis-qsf/consultation-paper/
13
As such, the work to develop a NDIS Quality and Safeguarding Framework builds on previous work undertaken by the Disability Reform Council to develop a national framework for reducing and elim -inating the use of restrictive practices in the disability service sector. This included emphasis on hu-man rights and a person centred focus, and on the importance of a national approach. This in turn sets an imperative that an ACT Office of the Senior Practitioner will need to have clear links to na-tional arrangements relating to the oversight of restrictive practices.
The disability Reform Council document also emphasised the importance of accountability, collabor-ation, quality outcomes, safe workplaces, raising awareness, using data to inform practice, use of tools that reduce restrictive practices, and practice review.9
Though the above two documents were generated specifically in relation people living with disabil-ity, the themes are likely to resonate for a broader range of people, and are strongly relevant to the consideration of an ACT Office of the Senior Practitioner.
8.0 The extent of the issue in the ACTBased on initial commentary provided by persons within key stakeholder groups and sectors in the ACT, there are significant concerns in relation to the nature, extent and consequence of restrictive practices. Sentiments included the need for stronger protections, policy frameworks, and guidance about alternative practices.
This includes a consensus that the use of restrictive practices is more extensive than generally thought. The term ‘restrictive practices’ is not widely used or understood. Often other terms are used, such as ‘calming someone down’, ‘reducing stress’, ‘for their own safety’ and ‘behaviour man -agement’. The use of such language to explain restrictive practices emphasises the good intentions but is at risk of understating the adverse consequences that restrictive practices typically bring.
Significant concerns were raised that restrictive practices are over-utilised. However well-intended, there appears to be an entrenched culture in the use of restrictive practices – described as a ‘dino-saur’ culture by one stakeholder – where service providers do not have another avenue of response; not just to one-off crisis situations but to situations which occur day after day, week after week.
The above comments are not intended as an indictment on service providers, who may be in struggle because of a lack of capacity within the organisation, and perhaps more broadly in the in-dustry, for designing and delivering alternatives to restrictive practices.
Similarly, the comments are not intended as an indictment on families and other informal supports who are involved in such practices, because families can feel they are in very difficult situations espe-cially when there are no other supports available.
Nevertheless, the first step in moving forward is to name such practices for what they are, so that a collective focus can be built on finding better alternatives.
9 National Framework for Reducing and Eliminating the Use of Restrictive Practices in the Disability Service Sector (2014) Disability Reform Council
accessed at https://www.dss.gov.au/our-responsibilities/disability-and-carers/publications-articles/policy-research/national-framework-for-reducing-and-eliminating-the-use-of-restrictive-practices-in-the-disability-service-sector
14

Initial consultation revealed that service providers (in community services, education, etc) want to use less restrictive practices but staff do not have the time, skills or resources to implement least re-strictive alternatives. Restrictive practices may initially be seen as a temporary measure, however without organisational skill development to provide alternatives, these temporary measures con-tinue. For similar reasons, although positive behaviour support plans may exist, they may not be im -plemented.
Stakeholders felt that when concerns about the use of restrictive practices are raised, they may not be addressed appropriately. Service providers across the social services sector have varied policies and procedures in place to deal with such issues, but with no broad accountability requirements, service responses are variable and inconsistent.
Stakeholders outlined a range of restrictive practices known to be used in the ACT which restrict the rights and freedom of individuals. A small sample of these included:
Separation/isolation /timeout (keeping someone in or out of a room) Chemical restraint to modify behavior and make people more passive Physical restraint (being tied to a bed or chair; battery removed from wheelchair) Not allowing social contact with persons of their choice or being forced to socialise with peo-
ple) Sanctions (for example, not being allowed to attend something if behavior is not approved,
or being required to leave school early/attend part-time/suspend attendance) Access to food and water restricted Not being able to live with whom they choose Being required to live in a certain setting to receive services Highly controlled environments (e.g. in congregate accommodation).
Also, there was a clear sentiment that people deserve to have supports that are proactive, where the focus is on assisting the person into the features of an ordinary, valued life, as opposed to supports that are reactive, that focus on managing crisis.
The ACT Government has commissioned a range of reports that in various ways reveal there are sig-nificant issues in relation to restrictive practices.
These include:
Report Of The Expert Panel On Students With Complex Needs And Challenging Behaviour (November 2015) and ResponseThis report, prepared by the Expert Panel on Students with Complex Needs and Challenging Behaviours, raises a range of relevant issues, including for example suspensions, part-time schooling, and locked seclusion. The report identified 50 recommendations across a com-prehensive range of systemic elements, including issues of restrictive practices and positive behaviour supports.In its response, the ACT government agreed to 43 recommendations, and agreed-in-principle to the remaining seven. (http://www.det.act.gov.au/__data/assets/pdf_file/0009/795186/62074-Expert-Panel-Re-port-Web.pdf)(http://www.det.act.gov.au/__data/assets/pdf_file/0010/793981/Expert-Panel-Response-fi-nal.pdf)
15

ACT’s Mental Health Act 2015 Developed as a result of a multi-year review process, this legislation is designed to reflect the Convention on the Rights of Persons with disabilities and the ACT Human Rights. It em-phasises recovery as context, and Act Key points from review leading to updated Mental Health Act (2015) which focuses on recovery, and providing the least restrictive care. It also emphasises the role of supported decision making(http://www.health.act.gov.au/our-services/mental-health/mental-health-act-2015)
ACT Law Reform Advisory Council Guardianship Report (July 2016)This report carries a series of recommendations that together constitute a systemic shift away from ‘best-interests’-based decision making towards rights-based decision-making. By their nature, these recommendations suggest that ACT stakeholders are not content with current arrangements relating to guardianship and substitute decision-making. Given many restrictive practices are undertaken against the will of the person being restricted, and are permitted or asserted by persons holding guardianship, then the recommended new ar-rangements create imperatives for new arrangements to reduce use of restrictive practices.(http://cdn.justice.act.gov.au/resources/uploads/JACS/Reviews/submissions/Guardianship_review/Guardianship_Report-Final.pdf).
ACT is one of only two States and Territories in Australia to have a legislative charter of rights, the Human Rights Act 2004, which provides that public authorities (including non-government agencies carrying out functions of government) must take human rights into account in decision making and must act consistently with human rights.
Use of restrictive practices in many contexts may be inconsistent with human rights including the right to be free from inhuman and degrading treatment, the right to liberty and security of person, freedom of movement and freedom of association, and so it is important that these human rights obligations are taken into account in any proposed model of oversight in the ACT.
In addition, the design and implementation of the NDIS includes the current development of a Na-tional Framework for Quality and Safeguards to help guide the suitability of support arrangements for NDIS participants (which includes children and adults living with disability, including psychosocial disability).
16
9.0 Considerations on how an ACT Office of the Senior Practitioner be might be arranged
Feedback from the initial consultation indicated that an Office of the Senior Practitioner might need to be premised on the broadest understandings of restrictive practices. If so, this signals a large and complex task in seeking to establish a regulatory, practice-shaping environment that reaches across a wide range of demographics and a wide range of service settings, such as schools and other educa-tion settings, disability service settings, hospitals and other health settings, mental health service settings, aged care settings, , and justice-related custodial settings. This poses a significant challenge in defining the role of the Office of Senior Practitioner.
The ultimate aim of an Office of the Senior Practitioner should be to eliminate restrictive practices not merely reduce or minimise the use of them, as it is the most vulnerable people, affected by signi -ficant power imbalances, who are most likely to be subject to restrictive practices.
Generally, initial stakeholder feedback considered that an Office of the Senior Practitioner would need to be high profile, with appropriate staffing and resources to undertake investigations, make strong recommendations, gather data and provide reports; plus have an educative function about what constitutes restrictive practices and how these practices can be replaced by positive alternat-ives.
This in turn raises the question about where the primary focus might be for the work of an Office of the Senior Practitioner. At least three areas of focus were identified:
Evolving support practices
This suggests investment in raising awareness, identifying best practice alternatives, and leading professional development in the sector.
Strengthening scrutiny arrangements
This suggests investment in strengthening the visibility of services and their practices, to make it easier to identify, investigate and respond to issues of concern. This may include a process to approve or deny proposed restrictive practices.
Imposing sanctions
This suggests investment in arrangements that apply sanctions or penalties to organisations who operate unauthorised restrictive practices.
If the goal of an ACT Office of the Senior Practitioner is to influence the reduction in the use of re-strictive practices in favour of positive alternatives, this gives rise to a number of considerations about how an ACT Office of the Senior Practitioner might operate, including, but not necessarily lim -ited to, the following:
Legislation that sets out the purpose and extent of the Office of the Senior Practitioner’s powersWould it be helpful for the ACT to have specific legislation that sets out the role and powers of an Office of the Senior Practitioner, and how would it relate to other relevant legislation in relation to mental-health, guardianship, etc?
Regulatory role to approve/deny proposed restrictive practice arrangements
17

Would it be helpful for there to be regulations that say who can approve/deny restrictive practice arrangements, and how those practices are reviewed? Might this be an ACT Office of the Senior Practitioner, or someone else?
Maintenance of a Register of approved/declared restrictive practicesWould it be helpful for an ACT Office of the Senior Practitioner to run a register detailing which people are currently being subjected to restrictive practices, by whom, for what pur-pose and for how long? And, while protecting the identities of those being restricted, should the register be reported, to whom and how often?
Awareness-raising across a range of stakeholder groups on the problems of restrictive practicesCould an ACT Office of the Senior Practitioner lead the systematic awareness-raising across all stakeholders about the problems of restrictive practices?
Leading the understanding of best practice in applied behaviour analysis and positive be-haviour supportsCould an ACT Office of the Senior Practitioner be the place that leads the understanding of best practice about the alternatives to restrictive practices?
Training and information to service providers and related stakeholders to increase capa-city for providing alternatives to restrictive practicesCould an ACT Office of the Senior Practitioner be the place that leads the training and devel-opment of alternatives to restrictive practices?
Accreditation of professionals allowed to develop behaviour support plans where restrict-ive practices might be contemplatedCould an ACT Office of the Senior Practitioner be the place that provides accreditation for professionals who are allowed to develop and/or sign-off support arrangements that include restrictive practices?
Stimulating sector development to assist adequate supply of such professionalsCould an ACT Office of the Senior Practitioner take a lead role in ensuring that the ACT hu-man services sector has enough accredited professionals to support the regulating of re-strictive practices and the development of alternatives?
Alignment with other relevant ACT legislation, regulations and frameworks?How would an ACT Office of the Senior Practitioner need to operate so that it aligns with other relevant ACT legislation and regulations. For example, how could an ACT Office of the Senior Practitioner support the coherence in practice of the Mental Health Act 2015, the im-plemented recommendations from Law Reform Advisory Council Guardianship Report, and the implemented recommendations from the Report Of The Expert Panel On Students With Complex Needs And Challenging Behaviour.
Alignment with other relevant Commonwealth legislation, regulations and frameworksHow might an ACT Office of the Senior Practitioner align, for example, with the NDIS Na-tional Quality and Safeguards Framework, and with Commonwealth arrangements for older persons and the children and young people
Organisational location of an ACT Office of the Senior Practitioner
18

Given the potential breadth of the Office of the Senior Practitioner role, and the question of how it links to other existing arrangements in the ACT, options might include it being an in-dependent statutory authority, or located within another existing entity such as the Human Services Regulator, the Human Rights Commission, the ACT Ombudsman, or a specific ACT government directorate.
10.0 Parameters for Public ConsultationWhile it can be argued that community stakeholders may have accrued consultation fatigue in re -cent times because of a range of important conversations relating to disability, mental health, and education, the issue of restrictive practices is a sufficiently important issue to seek the views of a wide range of stakeholders.
10.1Principles underpinning the consultation importance of making sure a wide range of stakeholders have their say importance of making it as easy as possible for stakeholders to give their views (to balance
thoroughness with consultation fatigue) importance of a wide range of channels, in support of the above, so each stakeholder can
choose which ever channel works best for them importance of ensuring sufficient flexibility in the line of enquiry, to minimise the risk of in-
advertently missing issues of concern to stakeholders that are not covered by consultation questions
importance of collaboration with a range of ACT community agencies, such as peak bodies and member-based organisations, whose current relationship with their stakeholders means they might be best placed to host a consultation event/channel
scheduling the consultation to meet the ACT government’s deadline of 31 March 2017 for a report on consultation findings
10.2Key elements of proposed consultationTo give effect to the above principles, we propose the following elements:
Target consultation period covering 7 week period from 30 January to 17 March Development of a web presence as hub for the consultation schedule, and for the project
overall, so stakeholders can get relevant information easily and quickly Development of a range of consultation channels, including:
o online surveyso a wide range of stakeholders can give their views at a time of their convenience.
o 1:1 telephone interviewfor individual stakeholders who would prefer this approach.
o Email submissionin response to the matters raised in this Discussion Paper.
o Easy-English summariesto assist stakeholders with differing cognitive capacity to engage the issues.
o Focus groupsIncluding those held in collaboration with, or via, local peak bodies and membership-based groups.
o Public forumsfor a broader range of stakeholders to contribute.
19
None of these are mutually exclusive; a stakeholder can access as many different channels as they feel will assist their voice to be heard.
10.3Key questions to be explored through the consultationMindful of the considerations listed in section 9 of this document, and to serve as focal points for stakeholders to consider their views, the consultation is anchored on the following questions:
Are there any situations where restrictive practices are ok?
Should there be a law or regulation that only allows restrictive practices to happen in certain circumstances?
o If so, what things would be in that law or regulation?
o If not, what else could help?
How do you feel about disability service providers, mental health service providers, schools, hospitals, and older persons’ service providers, needing to get external permission before they can use restrictive practices on someone?
o Should it be a new ACT Office of the Senior Practitioner (ACT Office of the Senior Practitioner) who is in charge of giving that permission, and what skills and experi -ence should they have?
o If you think there should be external permission, but not an ACT Office of the Senior Practitioner, is there some other ACT or national agency that could do this?
o If you think there does not need to be external permission, who should be in charge of such decisions inside the service agency, and what skills and experience should they have?
How important do you think it would be to have a register of every person who is being sub -jected to restrictive practices?
o If so, how do you think that register should work, including how it is reported?
o Do you think an ACT Office of the Senior Practitioner could run the register, or someone else?
How important is it to you that there is a strategy to raise awareness of the problems of re-strictive practices?
o If so, do you think an ACT Office of the Senior Practitioner could do this or do you think there is some other ACT or national agency that could do this?
o What would be the priorities in that strategy for raising awareness?
How important do you think it would be to have a strategy to build capacity for best practice within the health, education and community services sectors, so that more staff know how to provide alternatives to restrictive practices?
o If so, do you think an ACT Office of the Senior Practitioner could do this or do you think there is some other ACT or national agency that could do this?
20

o What would be the priorities in that strategy for capacity-building?
Which other ACT and national laws, regulations and frameworks do you think an ACT Office of the Senior Practitioner needs to link to (to avoid duplication, gaps, etc), and how do you think this should happen?
o How might an ACT Office of the Senior Practitioner link in for example with care and protection legislation and services, official visitor schemes, human rights legislation and complaints, ACAT treatment orders, the ACT Ombudsman, and the offices within the ACT Human Rights Commission, including the Discrimination, Health Services, and Disability & Community Services Commissioner, and the Public Advocate and Children and Young People Commissioner
These questions serve as a focus for consultation, and do not preclude the possibility of other themes and comments emerging during the consultation process.
Also, consultation will need to be framed in ways that support as many people as possible to give their views. This includes those people who are vulnerable to having restrictive practices imposed on them, such as children and young people, people living with disability, people living with mental illness, people connecting with the Justice system, and older people.
11.0 Next stepsThe ACT government has asked the community agency called JFA Purple Orange to lead the con -sultation.
You can go to JFA Purple Orange’s dedicated website (http://www.actosp.org.au) for further information about the project, including timelines, latest news, community consultation events, and other ways you can give your views. You can also download further copies of this discussion paper and other papers as and when they are released.
You can also contact JFA Purple Orange on1300 857 327 or via [email protected] if you have any questions about the consultation project.
End of document
21