journal of cardiovascular pharmacology and …pbt.guc.edu.eg/repository/faculty/publications/55/alaa...
TRANSCRIPT
http://cpt.sagepub.com/
TherapeuticsJournal of Cardiovascular Pharmacology and
http://cpt.sagepub.com/content/early/2010/10/05/1074248410378506The online version of this article can be found at:
DOI: 10.1177/1074248410378506
published online 11 October 2010J CARDIOVASC PHARMACOL THERAlaaeldin I. Saleh, Sahar M. Abdel Maksoud, Shohda A. El-Maraghy and Mohamed Z. Gad
AspirinProtective Effect of L-Arginine in Experimentally Induced Myocardial Ischemia: Comparison With
Published by:
http://www.sagepublications.com
can be found at:Journal of Cardiovascular Pharmacology and TherapeuticsAdditional services and information for
http://cpt.sagepub.com/cgi/alertsEmail Alerts:
http://cpt.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
Protective Effect of L-Arginine inExperimentally Induced MyocardialIschemia: Comparison With Aspirin
Alaaeldin I. Saleh, MSc1, Sahar M. Abdel Maksoud, PhD1,Shohda A. El-Maraghy, PhD2, and Mohamed Z. Gad, PhD1
AbstractObjective: Coronary artery diseases including myocardial ischemia (MI) remain one of the leading causes of death worldwide.This study was designed to compare the protective effect of L-arginine versus aspirin from the biochemical changes associatedwith MI injury. Experimental design: Four groups of male New Zealand white rabbits were investigated. Normal group (n ¼ 8)rabbits were fed standard chow pellets, untreated MI group (n ¼ 16), where hypercholesterolemia was induced by feeding theanimals with a diet containing 2% cholesterol for 28 days, L-arginine group (n¼ 12) rabbits were fed a 2% cholesterol-enriched dietin conjunction with L-arginine (2.25 g %) in drinking water for 28 days, and aspirin group (n ¼ 12) rabbits were fed 2% cholesterol-enriched diet in conjunction with aspirin administered orally (0.7 mg/kg per d) for 28 days. After 28 days, MI was induced in all groups,except the normal group, by a single subcutaneous (sc) injection of isoproterenol hydrochloride (0.2 mg/kg body weight [bw]). Animalswere sacrificed 6 hours later. Results: Our results showed that L-arginine was more effective than aspirin in reducing platelet aggrega-tion, reducing low-density lipoprotein (LDL) oxidizability, preventing aortic intimal thickening, andmaintaining histological architectureof the myocardium. Both drugs, however, had similar positive effects on plasma fibrinogen levels and on the prevention of myocardialrelease of cardiac troponin I and creatine kinase-MB. The effect on hypercholesterolemia was insignificant for both drugs. Aspirinwas more effective than L-arginine in prolonging prothrombin time. Conclusion: L-arginine supplementation represents a potentiallynovel nutritional strategy for preventing and treating coronary artery diseases especially in cases of aspirin resistance and/orhypersensitivity.
Keywords
myocardial ischemia, hypercholesterolemia, isoproterenol, aspirin, L-arginine
Introduction
Myocardial ischemia (MI) is caused by an insufficient supply
of oxygen-rich blood to the myocardium caused by increased
myocardial substrate demand and/or the narrowing or closure
of coronary arteries.1 Lack of oxygen and metabolic substrates
rapidly decreases the energy available to the cell and leads to
cell injury that might be reversible or irreversible in nature.
One of the most widely used experimental models to study
MI and the therapeutic effects of drugs is isoproterenol-
induced MI.2 Isoproterenol (isoprenaline) hydrochloride is a
synthetic sympathomimetic amine that is structurally similar
to epinephrine but selective for b receptors, activating b1 and
b2 receptors equally, and exerting positive inotropic and chron-
otropic effects on the heart.3 Indeed, pathophysiological
changes following isoproterenol administration are comparable
to those taking place in human MI/infarction.4
L-Arginine is a semi-essential amino acid found in most
mammals. Under conditions of stress and injury, L-arginine is
considered an essential amino acid. It is the precursor of
endothelial nitric oxide (NO) that plays a critical role in cardi-
ovascular protection5 and in maintaining an active vasodilator
tone in healthy blood vessels.6 Several studies in humans and
experimental animals indicated that oral L-arginine intake has
multiple beneficial cardiovascular effects when taken in doses
larger than normally present in diet (reviewed in ref 7). The pos-
itive role of L-arginine in cardiovascular health is due to both
NO-dependent and NO-independent effects.8 It has been shown
that both oral and parenteral administration of L-arginine can
1 Biochemistry Department, Faculty of Pharmacy, German University in Cairo,
New Cairo, Egypt2 Biochemistry Department, Faculty of Pharmacy, Cairo University, Giza, Egypt
Corresponding Author:
Mohamed Z Gad, Biochemistry Department, Faculty of Pharmacy, The German
University in Cairo, El-Tagmoa El-Khamis, New Cairo, Egypt
Email: [email protected]
Journal of CardiovascularPharmacology and Therapeutics000(00) 1-10ª The Author(s) 2010Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/1074248410378506http://cpt.sagepub.com
1
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from

increase NO synthesis in various tissues.9 In hypercholesterole-
mia, the synthesis and/or release of NO is severely impaired,
leading to attenuated endothelium-dependent vasodilation,
enhanced platelet aggregation, intimal thickening, and subse-
quent development of atherosclerosis.10 The impairment of
endothelial NO liberation in hypercholesterolemia is related to
low-density lipoprotein (LDL) cholesterol uptake into the
endothelium,11 and both native and oxidized LDLs are reported
to interfere with the biological activity of NO in vitro.12
Evidence suggests that L-arginine may play a therapeutic role
in tissue preservation during reperfusion after a period of
hypoxia, as animal studies showed protective effects of
L-arginine administration against ischemia/reperfusion inju-
ries in several tissues, including the myocardium.13
Among the traditional medicines used for cardiovascular
disease (CVD) is aspirin, the prototype of traditional nonster-
oidal anti-inflammatory drugs (NSAIDs), which had been
officially approved by the US Food and Drug Administration
(FDA) in 1939. The history of aspirin use in protection from
CVD started in the 1950s, after the appearance of evidence
that aspirin prolongs prothrombin time (PT).14 During the
1960s, aspirin was found to inhibit thromboxane A2 synthesis
that enhances platelet aggregation.15 Today, use of low-
dosage aspirin is a common practice in the prophylaxis and
treatment of CVD.16 This study is among the few studies that
address the potential role of L-arginine in the prevention of
MI injury. The molecular mechanisms behind this prevention
were investigated and compared to the widely used cardiovas-
cular protective agent, aspirin.
Materials and Methods
Animals
A total of 48 male New Zealand white rabbits weighing 1.55 to
1.95 kg were used in the study. They were kept in standard rab-
bit cages in the animal house of the Faculty of Pharmacy, Cairo
University. The animals were adapted for 10 days prior to
experimental use. All rabbits were maintained at almost con-
stant environmental conditions throughout the study with free
access to food and water. The study protocol was approved
by the local ethics committee.
Drugs and Chemicals
L-Arginine powder (NOW FOODS, Bloomingdale, Illinois),
Cholesterol fine powder (Sigma-Aldrich, Germany), Isoprena-
line hydrochloride ampules (0.2 mg/mL, Monico SPA, Italy),
Aspirin tablets (acetylsalicylic acid 75 mg, CID, Egypt), and
Tween 80 (Adwic, Egypt) were used from the indicated manu-
facturers. All other reagents and chemicals were of high analy-
tical grade.
Experimental Protocol
After the initial adaptation, rabbits were divided into four
groups: group I, normal group of 8 rabbits fed standard chow
pellets; group II, myocardial ischemic (untreated MI) group
of 16 rabbits fed 2% cholesterol-enriched diet for 28 days17;
group III, L-arginine group of 12 rabbits fed 2% cholesterol-
enriched diet in conjunction with L-arginine in drinking water
(2.25 g %) for 28 days18; and group IV, aspirin group of 12 rab-
bits fed 2% cholesterol-enriched diet in conjunction with orally
administered aspirin (0.7 mg/kg per d) for 28 days.19 After
completion of the experimental period, animals in the untreated
MI, L-arginine, and aspirin groups were then injected with a
single bolus subcutaneous (sc) injection of isoproterenol hydro-
chloride (0.2 mg/kg body weight [bw])20 and sacrificed 6 hours
later. Control group rabbits were injected with vehicle and were
sacrificed 6 hours later. All animals were subjected to a
12-hour fast, with free access to water and were anesthetized
with intravenous injection of 20 mg/kg bw thiopental sodium21
before killing.
Sample Collection
Fasting blood samples from each rabbit ear vein were drawn
before killing, for the preparation of serum or plasma. Later,
hearts were removed and used for histopathological examina-
tion and determination of aorta intimal thickness.
Biochemical Analysis
Commercially available kits were used for the determination of
serum total cholesterol ([TC]; Diamond Diagnosis Co,
Germany),22 serum creatine kinase-MB activity ([CK-MB];
Greiner Diagnostics GmbH, Germany),23 cardiac Troponin
I ([cTnI]; DRG International Inc, Mountainside, New Jersey),24
PT, and fibrinogen measurements (Diagnostica stago,
France).25 Spectrophotometric measurements were performed
using a Jasco UV/VIS spectrophotometer (Japan) and a micro-
titer well reader Perkin Elmer (Perkin Elmer, Waltham, Massa-
chusetts). In the LDL oxidizability experiment, metal ion
copper was used for measuring the susceptibility of LDL and
very-low-density lipoprotein (VLDL) to become oxidized.26
Plasma was used for the determination of platelet aggregation
using a dual channel platelet aggregometer (Chrono-log,
Havertown, Pennsylvania).27
Histological Assessment
Autopsy samples were taken from the heart’s myocardium,
coronaries, and aorta of rabbits and fixed in 10% formol
saline. Samples were then subjected to histopathological
examination and intimal thickness measurement.28 For each
animal, 10 specimens from the aorta were subjected to
measurement of intimal thickness (mm) by a Leica image ana-
lyzer. The mean of the 10 sections represented the intimal
thickness of the animal. The average intimal thickness for all
animals of the group was then calculated to represent the mean
of intimal thickness for each group. These measurements were
done in the Histology department, Faculty of Medicine, Cairo
University.
2 Journal of Cardiovascular Pharmacology and Therapeutics 000(00)
2
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
Statistical Analysis
Results are expressed as mean + standard error of the mean
(SEM). For statistical analysis of the data, multiple compari-
sons were carried out using 1-way analysis of variance
(ANOVA) followed by Tukey-Kramer test for post hoc analy-
sis. Statistical significance was accepted for a level of P < .05.
Results
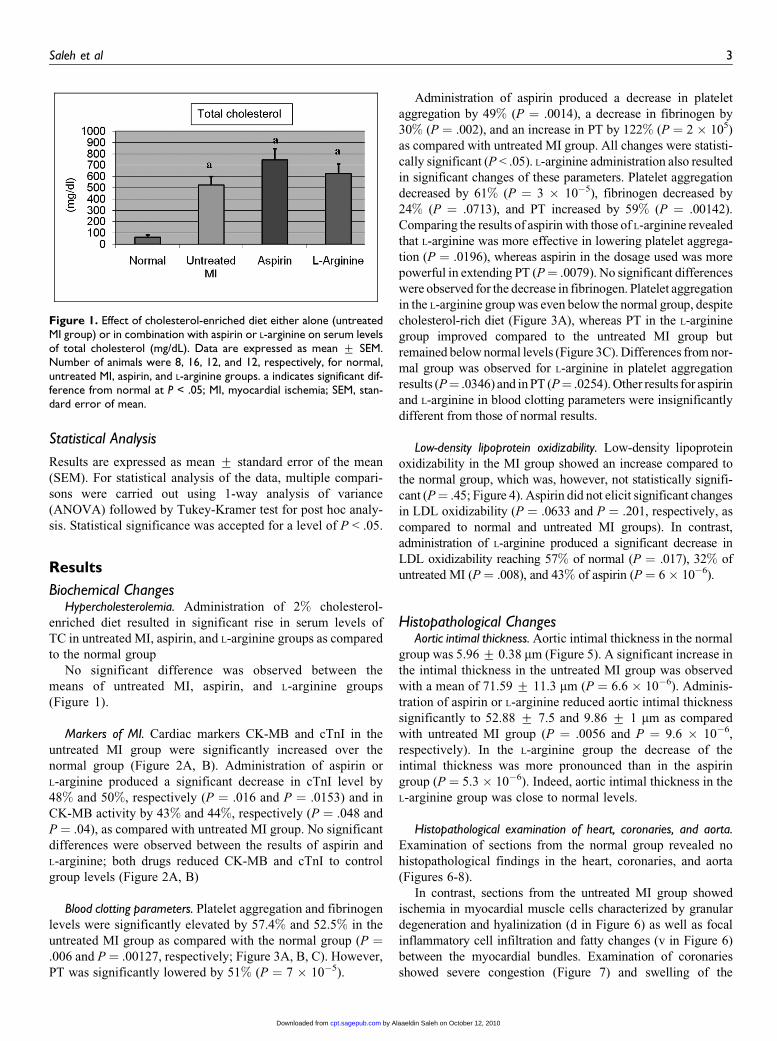
Biochemical ChangesHypercholesterolemia. Administration of 2% cholesterol-
enriched diet resulted in significant rise in serum levels of
TC in untreated MI, aspirin, and L-arginine groups as compared
to the normal group
No significant difference was observed between the
means of untreated MI, aspirin, and L-arginine groups
(Figure 1).
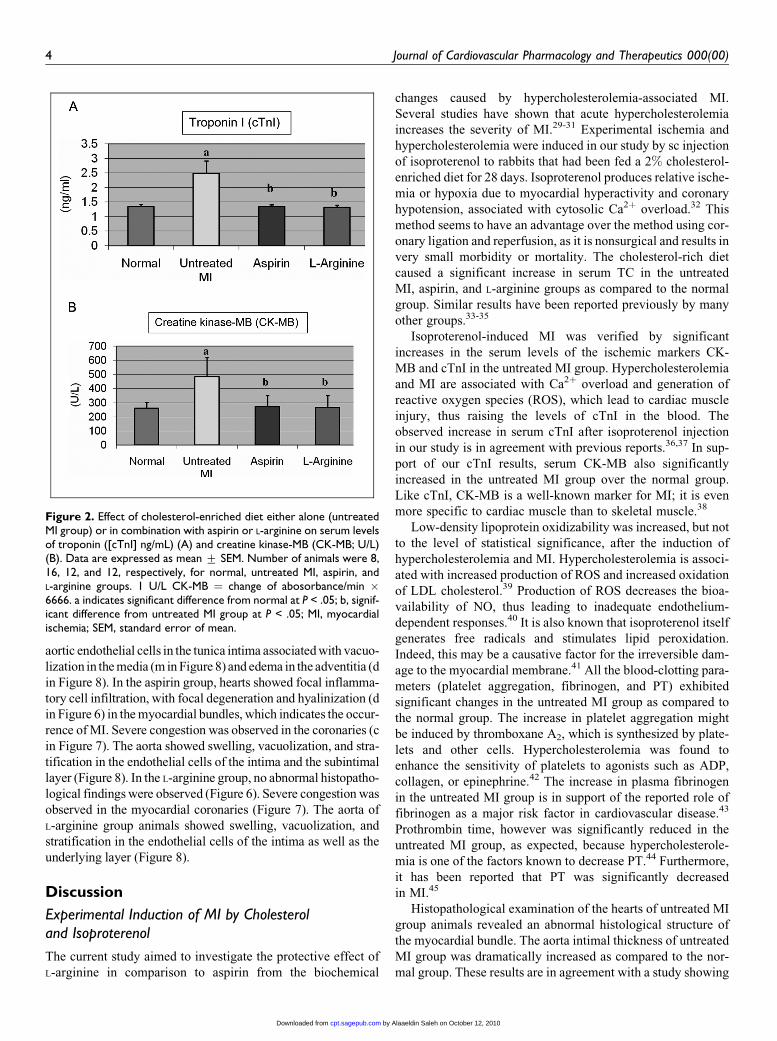
Markers of MI. Cardiac markers CK-MB and cTnI in the
untreated MI group were significantly increased over the
normal group (Figure 2A, B). Administration of aspirin or
L-arginine produced a significant decrease in cTnI level by
48% and 50%, respectively (P ¼ .016 and P ¼ .0153) and in
CK-MB activity by 43% and 44%, respectively (P ¼ .048 and
P ¼ .04), as compared with untreated MI group. No significant
differences were observed between the results of aspirin and
L-arginine; both drugs reduced CK-MB and cTnI to control
group levels (Figure 2A, B)
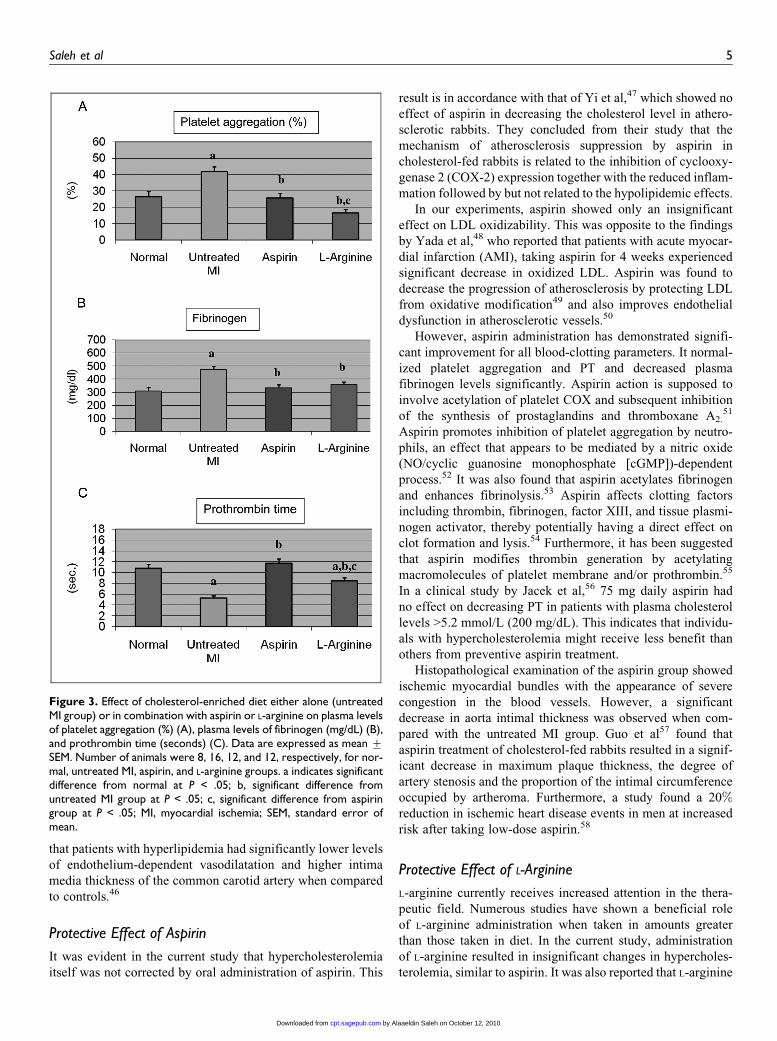
Blood clotting parameters. Platelet aggregation and fibrinogen
levels were significantly elevated by 57.4% and 52.5% in the
untreated MI group as compared with the normal group (P ¼.006 and P ¼ .00127, respectively; Figure 3A, B, C). However,
PT was significantly lowered by 51% (P ¼ 7 � 10�5).
Administration of aspirin produced a decrease in platelet
aggregation by 49% (P ¼ .0014), a decrease in fibrinogen by
30% (P ¼ .002), and an increase in PT by 122% (P ¼ 2 � 105)
as compared with untreated MI group. All changes were statisti-
cally significant (P < .05). L-arginine administration also resulted
in significant changes of these parameters. Platelet aggregation
decreased by 61% (P ¼ 3 � 10�5), fibrinogen decreased by
24% (P ¼ .0713), and PT increased by 59% (P ¼ .00142).
Comparing the results of aspirin with those of L-arginine revealed
that L-arginine was more effective in lowering platelet aggrega-
tion (P ¼ .0196), whereas aspirin in the dosage used was more
powerful in extending PT (P¼ .0079). No significant differences
were observed for the decrease in fibrinogen. Platelet aggregation
in the L-arginine group was even below the normal group, despite
cholesterol-rich diet (Figure 3A), whereas PT in the L-arginine
group improved compared to the untreated MI group but
remained below normal levels (Figure 3C). Differences from nor-
mal group was observed for L-arginine in platelet aggregation
results (P¼ .0346) and in PT (P¼ .0254). Other results for aspirin
and L-arginine in blood clotting parameters were insignificantly
different from those of normal results.
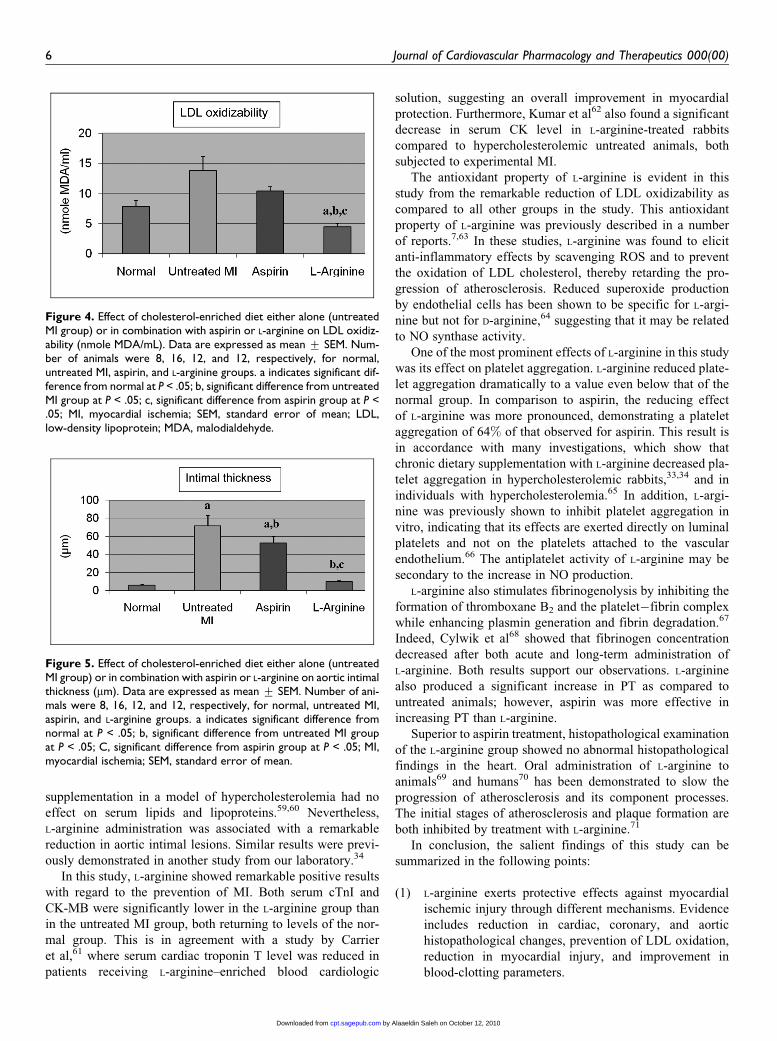
Low-density lipoprotein oxidizability. Low-density lipoprotein
oxidizability in the MI group showed an increase compared to
the normal group, which was, however, not statistically signifi-
cant (P¼ .45; Figure 4). Aspirin did not elicit significant changes
in LDL oxidizability (P ¼ .0633 and P ¼ .201, respectively, as
compared to normal and untreated MI groups). In contrast,
administration of L-arginine produced a significant decrease in
LDL oxidizability reaching 57% of normal (P ¼ .017), 32% of
untreated MI (P¼ .008), and 43% of aspirin (P ¼ 6� 10�6).
Histopathological ChangesAortic intimal thickness. Aortic intimal thickness in the normal
group was 5.96 + 0.38 mm (Figure 5). A significant increase in
the intimal thickness in the untreated MI group was observed
with a mean of 71.59 + 11.3 mm (P ¼ 6.6 � 10�6). Adminis-
tration of aspirin or L-arginine reduced aortic intimal thickness
significantly to 52.88 + 7.5 and 9.86 + 1 mm as compared
with untreated MI group (P ¼ .0056 and P ¼ 9.6 � 10�6,
respectively). In the L-arginine group the decrease of the
intimal thickness was more pronounced than in the aspirin
group (P ¼ 5.3 � 10�6). Indeed, aortic intimal thickness in the
L-arginine group was close to normal levels.
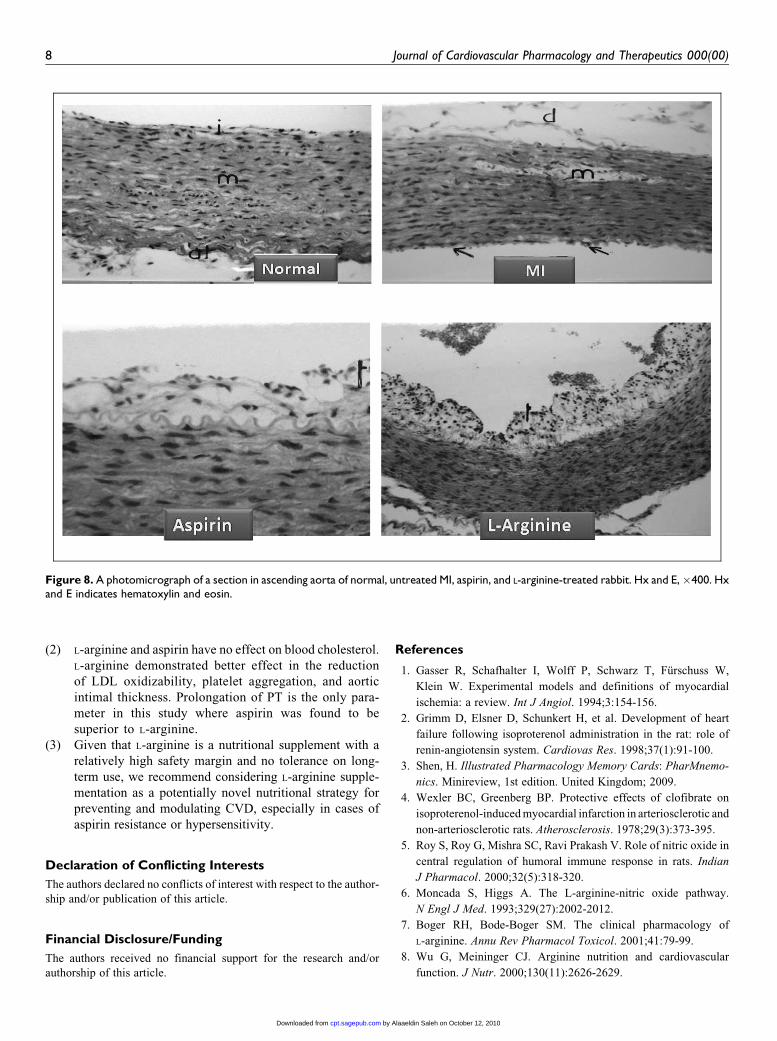
Histopathological examination of heart, coronaries, and aorta.Examination of sections from the normal group revealed no
histopathological findings in the heart, coronaries, and aorta
(Figures 6-8).
In contrast, sections from the untreated MI group showed
ischemia in myocardial muscle cells characterized by granular
degeneration and hyalinization (d in Figure 6) as well as focal
inflammatory cell infiltration and fatty changes (v in Figure 6)
between the myocardial bundles. Examination of coronaries
showed severe congestion (Figure 7) and swelling of the
Figure 1. Effect of cholesterol-enriched diet either alone (untreatedMI group) or in combination with aspirin or L-arginine on serum levelsof total cholesterol (mg/dL). Data are expressed as mean + SEM.Number of animals were 8, 16, 12, and 12, respectively, for normal,untreated MI, aspirin, and L-arginine groups. a indicates significant dif-ference from normal at P < .05; MI, myocardial ischemia; SEM, stan-dard error of mean.
Saleh et al 3
3
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
aortic endothelial cells in the tunica intima associated with vacuo-
lization in the media (m in Figure 8) and edema in the adventitia (d
in Figure 8). In the aspirin group, hearts showed focal inflamma-
tory cell infiltration, with focal degeneration and hyalinization (d
in Figure 6) in the myocardial bundles, which indicates the occur-
rence of MI. Severe congestion was observed in the coronaries (c
in Figure 7). The aorta showed swelling, vacuolization, and stra-
tification in the endothelial cells of the intima and the subintimal
layer (Figure 8). In the L-arginine group, no abnormal histopatho-
logical findings were observed (Figure 6). Severe congestion was
observed in the myocardial coronaries (Figure 7). The aorta of
L-arginine group animals showed swelling, vacuolization, and
stratification in the endothelial cells of the intima as well as the
underlying layer (Figure 8).
Discussion
Experimental Induction of MI by Cholesteroland Isoproterenol
The current study aimed to investigate the protective effect of
L-arginine in comparison to aspirin from the biochemical
changes caused by hypercholesterolemia-associated MI.
Several studies have shown that acute hypercholesterolemia
increases the severity of MI.29-31 Experimental ischemia and
hypercholesterolemia were induced in our study by sc injection
of isoproterenol to rabbits that had been fed a 2% cholesterol-
enriched diet for 28 days. Isoproterenol produces relative ische-
mia or hypoxia due to myocardial hyperactivity and coronary
hypotension, associated with cytosolic Ca2þ overload.32 This
method seems to have an advantage over the method using cor-
onary ligation and reperfusion, as it is nonsurgical and results in
very small morbidity or mortality. The cholesterol-rich diet
caused a significant increase in serum TC in the untreated
MI, aspirin, and L-arginine groups as compared to the normal
group. Similar results have been reported previously by many
other groups.33-35
Isoproterenol-induced MI was verified by significant
increases in the serum levels of the ischemic markers CK-
MB and cTnI in the untreated MI group. Hypercholesterolemia
and MI are associated with Ca2þ overload and generation of
reactive oxygen species (ROS), which lead to cardiac muscle
injury, thus raising the levels of cTnI in the blood. The
observed increase in serum cTnI after isoproterenol injection
in our study is in agreement with previous reports.36,37 In sup-
port of our cTnI results, serum CK-MB also significantly
increased in the untreated MI group over the normal group.
Like cTnI, CK-MB is a well-known marker for MI; it is even
more specific to cardiac muscle than to skeletal muscle.38
Low-density lipoprotein oxidizability was increased, but not
to the level of statistical significance, after the induction of
hypercholesterolemia and MI. Hypercholesterolemia is associ-
ated with increased production of ROS and increased oxidation
of LDL cholesterol.39 Production of ROS decreases the bioa-
vailability of NO, thus leading to inadequate endothelium-
dependent responses.40 It is also known that isoproterenol itself
generates free radicals and stimulates lipid peroxidation.
Indeed, this may be a causative factor for the irreversible dam-
age to the myocardial membrane.41 All the blood-clotting para-
meters (platelet aggregation, fibrinogen, and PT) exhibited
significant changes in the untreated MI group as compared to
the normal group. The increase in platelet aggregation might
be induced by thromboxane A2, which is synthesized by plate-
lets and other cells. Hypercholesterolemia was found to
enhance the sensitivity of platelets to agonists such as ADP,
collagen, or epinephrine.42 The increase in plasma fibrinogen
in the untreated MI group is in support of the reported role of
fibrinogen as a major risk factor in cardiovascular disease.43
Prothrombin time, however was significantly reduced in the
untreated MI group, as expected, because hypercholesterole-
mia is one of the factors known to decrease PT.44 Furthermore,
it has been reported that PT was significantly decreased
in MI.45
Histopathological examination of the hearts of untreated MI
group animals revealed an abnormal histological structure of
the myocardial bundle. The aorta intimal thickness of untreated
MI group was dramatically increased as compared to the nor-
mal group. These results are in agreement with a study showing
Figure 2. Effect of cholesterol-enriched diet either alone (untreatedMI group) or in combination with aspirin or L-arginine on serum levelsof troponin ([cTnI] ng/mL) (A) and creatine kinase-MB (CK-MB; U/L)(B). Data are expressed as mean + SEM. Number of animals were 8,16, 12, and 12, respectively, for normal, untreated MI, aspirin, andL-arginine groups. 1 U/L CK-MB ¼ change of abosorbance/min �6666. a indicates significant difference from normal at P < .05; b, signif-icant difference from untreated MI group at P < .05; MI, myocardialischemia; SEM, standard error of mean.
4 Journal of Cardiovascular Pharmacology and Therapeutics 000(00)
4
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
that patients with hyperlipidemia had significantly lower levels
of endothelium-dependent vasodilatation and higher intima
media thickness of the common carotid artery when compared
to controls.46
Protective Effect of Aspirin
It was evident in the current study that hypercholesterolemia
itself was not corrected by oral administration of aspirin. This
result is in accordance with that of Yi et al,47 which showed no
effect of aspirin in decreasing the cholesterol level in athero-
sclerotic rabbits. They concluded from their study that the
mechanism of atherosclerosis suppression by aspirin in
cholesterol-fed rabbits is related to the inhibition of cyclooxy-
genase 2 (COX-2) expression together with the reduced inflam-
mation followed by but not related to the hypolipidemic effects.
In our experiments, aspirin showed only an insignificant
effect on LDL oxidizability. This was opposite to the findings
by Yada et al,48 who reported that patients with acute myocar-
dial infarction (AMI), taking aspirin for 4 weeks experienced
significant decrease in oxidized LDL. Aspirin was found to
decrease the progression of atherosclerosis by protecting LDL
from oxidative modification49 and also improves endothelial
dysfunction in atherosclerotic vessels.50
However, aspirin administration has demonstrated signifi-
cant improvement for all blood-clotting parameters. It normal-
ized platelet aggregation and PT and decreased plasma
fibrinogen levels significantly. Aspirin action is supposed to
involve acetylation of platelet COX and subsequent inhibition
of the synthesis of prostaglandins and thromboxane A2.51
Aspirin promotes inhibition of platelet aggregation by neutro-
phils, an effect that appears to be mediated by a nitric oxide
(NO/cyclic guanosine monophosphate [cGMP])-dependent
process.52 It was also found that aspirin acetylates fibrinogen
and enhances fibrinolysis.53 Aspirin affects clotting factors
including thrombin, fibrinogen, factor XIII, and tissue plasmi-
nogen activator, thereby potentially having a direct effect on
clot formation and lysis.54 Furthermore, it has been suggested
that aspirin modifies thrombin generation by acetylating
macromolecules of platelet membrane and/or prothrombin.55
In a clinical study by Jacek et al,56 75 mg daily aspirin had
no effect on decreasing PT in patients with plasma cholesterol
levels >5.2 mmol/L (200 mg/dL). This indicates that individu-
als with hypercholesterolemia might receive less benefit than
others from preventive aspirin treatment.
Histopathological examination of the aspirin group showed
ischemic myocardial bundles with the appearance of severe
congestion in the blood vessels. However, a significant
decrease in aorta intimal thickness was observed when com-
pared with the untreated MI group. Guo et al57 found that
aspirin treatment of cholesterol-fed rabbits resulted in a signif-
icant decrease in maximum plaque thickness, the degree of
artery stenosis and the proportion of the intimal circumference
occupied by artheroma. Furthermore, a study found a 20%reduction in ischemic heart disease events in men at increased
risk after taking low-dose aspirin.58
Protective Effect of L-Arginine
L-arginine currently receives increased attention in the thera-
peutic field. Numerous studies have shown a beneficial role
of L-arginine administration when taken in amounts greater
than those taken in diet. In the current study, administration
of L-arginine resulted in insignificant changes in hypercholes-
terolemia, similar to aspirin. It was also reported that L-arginine
Figure 3. Effect of cholesterol-enriched diet either alone (untreatedMI group) or in combination with aspirin or L-arginine on plasma levelsof platelet aggregation (%) (A), plasma levels of fibrinogen (mg/dL) (B),and prothrombin time (seconds) (C). Data are expressed as mean +SEM. Number of animals were 8, 16, 12, and 12, respectively, for nor-mal, untreated MI, aspirin, and L-arginine groups. a indicates significantdifference from normal at P < .05; b, significant difference fromuntreated MI group at P < .05; c, significant difference from aspiringroup at P < .05; MI, myocardial ischemia; SEM, standard error ofmean.
Saleh et al 5
5
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
supplementation in a model of hypercholesterolemia had no
effect on serum lipids and lipoproteins.59,60 Nevertheless,
L-arginine administration was associated with a remarkable
reduction in aortic intimal lesions. Similar results were previ-
ously demonstrated in another study from our laboratory.34
In this study, L-arginine showed remarkable positive results
with regard to the prevention of MI. Both serum cTnI and
CK-MB were significantly lower in the L-arginine group than
in the untreated MI group, both returning to levels of the nor-
mal group. This is in agreement with a study by Carrier
et al,61 where serum cardiac troponin T level was reduced in
patients receiving L-arginine–enriched blood cardiologic
solution, suggesting an overall improvement in myocardial
protection. Furthermore, Kumar et al62 also found a significant
decrease in serum CK level in L-arginine-treated rabbits
compared to hypercholesterolemic untreated animals, both
subjected to experimental MI.
The antioxidant property of L-arginine is evident in this
study from the remarkable reduction of LDL oxidizability as
compared to all other groups in the study. This antioxidant
property of L-arginine was previously described in a number
of reports.7,63 In these studies, L-arginine was found to elicit
anti-inflammatory effects by scavenging ROS and to prevent
the oxidation of LDL cholesterol, thereby retarding the pro-
gression of atherosclerosis. Reduced superoxide production
by endothelial cells has been shown to be specific for L-argi-
nine but not for D-arginine,64 suggesting that it may be related
to NO synthase activity.
One of the most prominent effects of L-arginine in this study
was its effect on platelet aggregation. L-arginine reduced plate-
let aggregation dramatically to a value even below that of the
normal group. In comparison to aspirin, the reducing effect
of L-arginine was more pronounced, demonstrating a platelet
aggregation of 64% of that observed for aspirin. This result is
in accordance with many investigations, which show that
chronic dietary supplementation with L-arginine decreased pla-
telet aggregation in hypercholesterolemic rabbits,33,34 and in
individuals with hypercholesterolemia.65 In addition, L-argi-
nine was previously shown to inhibit platelet aggregation in
vitro, indicating that its effects are exerted directly on luminal
platelets and not on the platelets attached to the vascular
endothelium.66 The antiplatelet activity of L-arginine may be
secondary to the increase in NO production.
L-arginine also stimulates fibrinogenolysis by inhibiting the
formation of thromboxane B2 and the platelet�fibrin complex
while enhancing plasmin generation and fibrin degradation.67
Indeed, Cylwik et al68 showed that fibrinogen concentration
decreased after both acute and long-term administration of
L-arginine. Both results support our observations. L-arginine
also produced a significant increase in PT as compared to
untreated animals; however, aspirin was more effective in
increasing PT than L-arginine.
Superior to aspirin treatment, histopathological examination
of the L-arginine group showed no abnormal histopathological
findings in the heart. Oral administration of L-arginine to
animals69 and humans70 has been demonstrated to slow the
progression of atherosclerosis and its component processes.
The initial stages of atherosclerosis and plaque formation are
both inhibited by treatment with L-arginine.71
In conclusion, the salient findings of this study can be
summarized in the following points:
(1) L-arginine exerts protective effects against myocardial
ischemic injury through different mechanisms. Evidence
includes reduction in cardiac, coronary, and aortic
histopathological changes, prevention of LDL oxidation,
reduction in myocardial injury, and improvement in
blood-clotting parameters.
Figure 4. Effect of cholesterol-enriched diet either alone (untreatedMI group) or in combination with aspirin or L-arginine on LDL oxidiz-ability (nmole MDA/mL). Data are expressed as mean + SEM. Num-ber of animals were 8, 16, 12, and 12, respectively, for normal,untreated MI, aspirin, and L-arginine groups. a indicates significant dif-ference from normal at P < .05; b, significant difference from untreatedMI group at P < .05; c, significant difference from aspirin group at P <.05; MI, myocardial ischemia; SEM, standard error of mean; LDL,low-density lipoprotein; MDA, malodialdehyde.
Figure 5. Effect of cholesterol-enriched diet either alone (untreatedMI group) or in combination with aspirin or L-arginine on aortic intimalthickness (mm). Data are expressed as mean + SEM. Number of ani-mals were 8, 16, 12, and 12, respectively, for normal, untreated MI,aspirin, and L-arginine groups. a indicates significant difference fromnormal at P < .05; b, significant difference from untreated MI groupat P < .05; C, significant difference from aspirin group at P < .05; MI,myocardial ischemia; SEM, standard error of mean.
6 Journal of Cardiovascular Pharmacology and Therapeutics 000(00)
6
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from

Figure 6. A photomicrograph of a section in heart of a rabbit in the normal, untreated MI, aspirin and L-arginine group. Hx and E,�64. Hx and Eindicates hematoxylin and eosin.
Figure 7. A photomicrograph of a section in coronary blood vessel of a rabbit in the normal, untreated MI, aspirin, and L-arginine group. Hx andE, �40. Hx and E indicates hematoxylin and eosin.
Saleh et al 7
7
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
(2) L-arginine and aspirin have no effect on blood cholesterol.
L-arginine demonstrated better effect in the reduction
of LDL oxidizability, platelet aggregation, and aortic
intimal thickness. Prolongation of PT is the only para-
meter in this study where aspirin was found to be
superior to L-arginine.
(3) Given that L-arginine is a nutritional supplement with a
relatively high safety margin and no tolerance on long-
term use, we recommend considering L-arginine supple-
mentation as a potentially novel nutritional strategy for
preventing and modulating CVD, especially in cases of
aspirin resistance or hypersensitivity.
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the author-
ship and/or publication of this article.
Financial Disclosure/Funding
The authors received no financial support for the research and/or
authorship of this article.
References
1. Gasser R, Schafhalter I, Wolff P, Schwarz T, Furschuss W,
Klein W. Experimental models and definitions of myocardial
ischemia: a review. Int J Angiol. 1994;3:154-156.
2. Grimm D, Elsner D, Schunkert H, et al. Development of heart
failure following isoproterenol administration in the rat: role of
renin-angiotensin system. Cardiovas Res. 1998;37(1):91-100.
3. Shen, H. Illustrated Pharmacology Memory Cards: PharMnemo-
nics. Minireview, 1st edition. United Kingdom; 2009.
4. Wexler BC, Greenberg BP. Protective effects of clofibrate on
isoproterenol-induced myocardial infarction in arteriosclerotic and
non-arteriosclerotic rats. Atherosclerosis. 1978;29(3):373-395.
5. Roy S, Roy G, Mishra SC, Ravi Prakash V. Role of nitric oxide in
central regulation of humoral immune response in rats. Indian
J Pharmacol. 2000;32(5):318-320.
6. Moncada S, Higgs A. The L-arginine-nitric oxide pathway.
N Engl J Med. 1993;329(27):2002-2012.
7. Boger RH, Bode-Boger SM. The clinical pharmacology of
L-arginine. Annu Rev Pharmacol Toxicol. 2001;41:79-99.
8. Wu G, Meininger CJ. Arginine nutrition and cardiovascular
function. J Nutr. 2000;130(11):2626-2629.
Figure 8. A photomicrograph of a section in ascending aorta of normal, untreated MI, aspirin, and L-arginine-treated rabbit. Hx and E,�400. Hxand E indicates hematoxylin and eosin.
8 Journal of Cardiovascular Pharmacology and Therapeutics 000(00)
8
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
9. Dass UN. L-arginine, nitric oxide and collagen vascular diseases:
a potential relationship. Nutrition. 1992;8(5):371.
10. Boger RH, Bode-Boger SM, Mugge A, et al. Supplementation of
hypercholesterolemic rabbits with L-arginine reduces the vascular
release of superoxide anions and restores NO production. Athero-
sclerosis. 1995;117(2):273-284.
11. Jacobs M, Plane F, Bruckdorfer KR. Native and oxidized low-
density lipoproteins have different inhibitory effects on
endothelium-derived relaxing factor in the rabbit aorta. Br J Phar-
macol. 1990;100(1):21-26.
12. Liao JK, Shin WS, Lee WY, Clark SL. Oxidized low-density lipo-
protein decreases the expression of endothelial nitric oxide
synthase. J Biol Chem. 1995;270(1):319-324.
13. Weyrich AS, Ma XL, Lefer AM. The role of L-arginine in ame-
liorating reperfusion injury after myocardial ischemia in the cat.
Circulation. 1992;86(1):279-288.
14. Govan CD. The effect of salicylate administration on prothrombin
time. J Pediatr. 1946;29:629-636.
15. Piper PJ, Vane JR. The release of prostaglandins during anaphy-
laxis in guinea-pig isolated lungs. In: Mantegazza P, Hor ton EW,
eds. Prostaglandins, Peptides, and Amines. London, UK:
Academic Press; 1969:15-19.
16. Conti CR, Hill JA, Mayfield WR. Unstable angina pectoris:
pathogenesis and management. Curr Probl Cardiol. 1989;
14(10):549-624.
17. Gokkusu C, Oz H. Effect of thymosin fraction 5 (F5) on erythro-
cyte glutathione and lipid peroxide levels in hypercholesterolemic
rabbits. Int Vitam Nutr Res. 1991;61(1):87-90.
18. Cooke JP, Singer AH, Tsao P, Zera P, Rowan RA, Billingham ME.
Antiatherogenic effects of L-arginine in the hypercholesterolemic
rabbit. J Clin Invest. 1992;90(3):1168-1172.
19. Yi G, Qi-zhang W, Bing-shan T, et al. Effects of aspirin on ather-
osclerosis and the cyclooxygenase-2 expression in the athero-
sclerotic rabbits. Chin Med J. 2006;119(21):1808-1814.
20. Kela AK, Reddy LP, Thombre DP. ECG findings in normal rats
after administration of Isoproterenol. Indian J Physiol Pharmacol.
1980;24(2):84-90.
21. Sedgwick CJ. Anesthesia for rabbits. Vet Clin North Am Food
Anim Pract. 1986;2(3):731-736.
22. Tietz NW. Clinical Guide to Laboratory Tests. 3rd ed.
Philadelphia, PA: WB Saunders Co; 1995.
23. Wurzburg U, Hennrich N, Orth HD, Lang H. Quantitative deter-
mination of creatine kinase isoenzyme catalytic concentrations in
serum using immunological methods. J Clin Chem Clin Biochem.
1977;15(3):131-137.
24. Etievent J, Chocron S, Toubin G, et al. The use of cardiac troponin
I as a marker of peri-operative myocardial ischemia. Ann Thorac
Surg. 1995;59(5):1192-1194.
25. Clauss A. Gerinnungsphysiologische Schnellmethode zur
Bestimmung des Fibrinogens. Acta Haematol. 1957;17(4):
237-246.
26. Zhang A, Vertommen J, Van Gaal L, De Leeuw I. A rapid and simple
method for measuring the susceptibility of low-density-lipoprotein
and very-low-density-lipoprotein to copper-catalyzed oxidation.
Clin Chim Acta. 1994;227(1-2):159-173.
27. Born GVR. Aggregation of blood platelets by adenosine
diphosphate and its reversal. Nature. 1962;194(37):927-929.
28. Banchroft JD, Stevens A, Turner DR. Theory and Practice of
Histological Techniques. 4th ed. New York, London,
San Francisco, Tokyo: Churchill Livingstone; 1996.
29. Golino P, Maroko PR, Carew TE. The effect of acute hypercho-
lesterolemia on myocardial infarct size and the NO reflow phe-
nomena during coronary occlusion-reperfusion. Circulation.
1987;75(1):292-298.
30. Sakamoto S, Kashiki M, Imai N, Liang CS, Hood WB Jr. Effects
of short-term, diet-induced hypercholesterolemia on systemic
hemodynamics, myocardial blood flow, and infarct size in awake
dogs with acute myocardial infarction. Circulation. 1991;84(1):
378-386.
31. Hoshida S, Nishida M, Yamashita N, et al. Amelioration of sever-
ity of myocardial injury by a nitric oxide donor in rabbits fed a
cholesterol-rich diet. J Am Coll Cardiol. 1996;27(4):902-909.
32. Bloom S, Davis DL. Calcium as mediator of isoproterenol
induced myocardial necrosis. Am J Pathol. 1972;69(3):459-470.
33. Tsao PS, McEvoy LM, Drexler H, Butcher EC, Cooke JP.
Enhanced endothelial adhesiveness in hypercholesterolemia is
attenuated by L-arginine. Circulation. 1994;89(5):2176-2182.
34. El-Maraghy SA, Gad MZ, Fahim AT, Hamdy MA. L-Arginine
supplement, the natural protection from cardiovascular disease:
unraveling the biochemical mechanisms. Arab J Med. 2007;
33(3):333-353.
35. Nematbakhsh M, Haghjooyjavanmard S, Mahmoodi F,
Monajemi AR. The effect of L-arginine on serum lipids and nitrite
levels, and the number of apoptotic cells, iNOS and eNOS expres-
sions of aorta after the formation of fatty streaks in rabbit. J Appl
Biomed. 2008;6(4):203-210.
36. Acikel M, Buyukokuroglu ME, Erdogan F, Akosy H, Bozkurt E,
Senocak H. Protective effect of dantrolene against myocardial
injury induced by isoproterenol in rats: biochemical and histolo-
gical findings. Int J Cardiol. 2005;98(3):389-94.
37. Senthil S, Sridevi M, Pugalendi KV. Cardioprotective effect of
oleanolic acid on isoproterenol-induced myocardial ischemia in
rats. Toxicol Pathol. 2007;35(3):418-423.
38. Otsu N, Yamaguchi I, Komatsu E, Miyazawa K. Changes in crea-
tine kinase M localization in acute ischemic myocardial cells.
Circ Res. 1993;73(5):935-942.
39. Napoli C, Postiglione A, Triggiani M, et al. Oxidative structural
modifications of low density lipoprotein in homozygous familial
hypercholesterolemia. Atherosclerosis. 1995;118(2):259-273.
40. Ignarro LJ, Cirino G, Napoli C. Nitric oxide as a signaling mole-
cule in the vascular system: an overview. J Cardiovasc Pharma-
col. 1999;34(6):876-884.
41. Chatelain P, Gremel M, Brotelle R. Prevention of amiodarone of
phospholipid depletion in isoproterenol-induced ischemia in rats.
Eur J Pharmacol. 1987;144(1):83-90.
42. Sato T, Maegawa H, Kometani M, Fujii T. Collagen-induced cal-
cium influx is enhanced in platelets from hypercholesterolemic
rabbits. Thromb Res. 1985;40(1):59-68.
43. Cook NS, Ubben D. Fibrinogen as major risk factor in cardiovas-
cular disease. Trends Pharmacol Sci. 1990;11(11):444-451.
Saleh et al 9
9
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from
44. Chan P, Tomlinsoin B, Tsai CW, Pan WH, Lee YS. Thrombophi-
lia in patients with hypercholesterolemia. Metabolism. 1996;
45(8):966-969.
45. Gurfinkel E, Bozovich G, Cerda M, Mejaıl I, Oxilia A, Mautner B.
Time significance of acute thrombotic reactant markers in patients
with and without silent myocardial ischemia and overt unstable
angina pectoris. Am J Cardiol. 1995;76(3):121-124.
46. Kraml P, Syrovatka P, Stıpek S, et al. Hyperlipoproteinemia
impairs endothelium-dependent vasodilation. Physiol Res. 2004;
53(5):471-480.
47. Yi G, Qi-zhang W, Bing-shan T, et al. Effects of aspirin on ather-
osclerosis and the cyclooxygenase-2 expression in the athero-
sclerotic rabbits. Chin Med J. 2006;119(21):1808-1814.
48. Yada T, Kaji S, Akasaka T, et al. Changes of asymmetric
dimethylarginine, nitric oxide, tetrahydrobiopterin, and oxida-
tive stress in patients with acute myocardial infarction by med-
ical treatments. Clin Hemorheol Microcirc. 2007;37(3):
269-276.
49. Steer KA, Wallace TM, Bolton CH, Hartog M. Aspirin protects
low density lipoprotein from oxidative modification. Heart.
1997;77(4):333-337.
50. Husain S, Andrews NP, Mulcahy D, Panza JA, Quyyumi AA.
Aspirin improves endothelial dysfunction in atherosclerosis.
Circulation. 1998;97(8):716-720.
51. Roth GJ, Majerus PW. The mechanism of the effect of aspirin on
human platelets. I. Acetylation of a particulate fraction protein.
J Clin Invest. 1975;56(3):624-632.
52. Lopez-Farre A, Caramelo C, Esteban A, et al. Effects of aspirin on
platelet-neutrophil interactions: role of nitric oxide and endothe-
lin-1. Circulation. 1995;91(7):2080-2088.
53. Bjornsson TD, Schneider DE, Berger H. Aspirin acetylates fibri-
nogen and enhances fibrinolysis. Fibrinolytic effect is indepen-
dent of changes in plasminogen activator levels. J Pharmacol
Exp Ther. 1989;250(1):154-161.
54. Ajjan RA, Standeven KF, Khanbhai M, et al. Effects of aspirin on
clot structure and fibrinolysis using a novel in vitro cellular sys-
tem. Arterioscler Thromb Vasc Biol. 2009;29(5):712-717.
55. Szczeklik A, Krzanowski M, Gora P, Radwan J. Antiplatelet
drugs and generation of thrombin in clotting blood. Blood.
1992;80(8):2006-2011.
56. Jacek M, Anetta U, Robert U, Jan B, Andrzej S. Treatment with
simvastatin and low-dose aspirin depresses thrombin generation
in patients with coronary heart disease and borderline-high cho-
lesterol levels. Thromb Haemost. 2001;85(2):221-225.
57. Guo Y, Jiang X, Chen S, Zhao HW, Gu KY. Changes of C-
reactive protein level and prognosis of ischemic stroke. Chin J
Clin Rehabil. 2004;8:753-755.
58. Thrombosis Prevention Trial: randomised trial of low-intensity
oral anticoagulation with warfarin and low-dose aspirin in the pri-
mary prevention of ischaemic heart disease in men at increased
risk. The Medical Research Council’s General Practice Research
Framework. Lancet. 1998;351(9098):233-241.
59. Wang BY, Singer AH, Tsao PS, Drexler H, Kosek J, Cooke JP.
Dietary arginine prevents atherogenesis in the coronary artery of
hypercholesterolemic rabbits. J Am Coll Cardiol. 1994;23(2):
452-458.
60. Boger RH, Bode-Boger SM, Brandes RP. Dietary L-arginine
reduces the progression of atherosclerosis in cholesterol-fed
rabbits: comparison with lovastatin. Circulation. 1997;96(4):
1282-1290.
61. Carrier M, Pellerin M, Perrault LP, et al. Cardioplegic arrest
with L-arginine improves myocardial protection: results of a
prospective randomized clinical trial. Ann Thorac Surg.
2002;73(3):837-842.
62. Kumar P, Agarwal JL, Kumar A. Effect of long term oral admin-
istration of L-arginine on experimentally produced myocardial
ischemia in rabbits. Indian J Physiol Pharmacol. 2007;51(2):
147-152.
63. Jablecka A, Checinski P, Krauss H, Micker M, Ast J. The influ-
ence of two different doses of L-arginine oral supplementation
on nitric oxide (NO) concentration and total antioxidant status
(TAS) in atherosclerotic patients. Med Sci Monit. 2004;10(1):
CR29-CR32.
64. Wascher TC, Posch K, Wallner C, Hermetter A, Kostner GM,
Graier WF. Vascular effects of L-arginine: anything beyond a
substrate for the NO synthase? Biochem Biophys Res Commun.
1997;234(1):35-38.
65. Wolf A, Zalpour C, Theilmeier G, et al. Dietary L-arginine
supplementation normalizes platelet aggregation in hypercho-
lesterolemic humans. J Am Coll Cardiol. 1997;29(3):479-485.
66. Diodati JG, Dakak N, Gilligan DM, Quyyumi AA. Effect of
atherosclerosis on endothelium-dependent inhibition of platelet
activation in humans. Circulation. 1998;98(1):17-24.
67. Udvardy M, Posan E, Palatka K, Altorjay I, Harsfalvi J. Effect of
L-arginine on in vitro plasmin generation and fibrinogenolysis.
Thromb Res. 1997;87(1):75-82.
68. Cylwik D, Mogielnicki A, Kramkowski K, Stokowski J,
Buczko W. Antithrombotic effect of L-arginine in hypertensive
rats. J phys Pharmacol. 2004;55(3):563-574.
69. McNamara DB, Bedi B, Aurora H, et al. L-arginine inhibits bal-
loon catheter-induced intimal hyperplasia. Biochem Biophys Res
Commun. 1993;193(1):291-296.
70. Drexler H, Zeiher AM, Meinzer K, Just H. Correction of
endothelial dysfunction in coronary microcirculation of hyperch-
olesterolaemic patients by L-arginine. Lancet. 1991;
338(8782-8783):1546-1550.
71. Hayashi T, Juliet PAR, Matsui-Hirai H, et al. L-citrulline and
L-arginine supplementation retards the progression of high-
cholesterol-diet-induced atherosclerosis in rabbits. Proc Natl
Acad Sci U S A. 2005;102(38):3681-13686.
10 Journal of Cardiovascular Pharmacology and Therapeutics 000(00)
10
by Alaaeldin Saleh on October 12, 2010cpt.sagepub.comDownloaded from