lean daily management: gbmc’s path to building a...
TRANSCRIPT
Lean Daily Management:GBMC’s Path to Building a Problem
Solving Culture
George Bayless IIIVice President of Finance – GBMC
Why We Decided to Use LDM• Started with “basic” Lean processes:
– Kaizen’s: Rapid Cycle Improvement Processes– 5S’s: Organizing workspaces– Value Stream Mapping: Process Flowcharting
• However, we were missing something…– No movement towards real-time problem
solving– Little change in culture– Inconsistent results
1
Why We Decided to Use LDM…
• We wanted more…• We wanted sustainable change… • We wanted culture change…• So… how do you change culture???• You do it every day!• Lean Daily Management
2
What We Do…• Selecting Metrics • Measuring Metrics• Pareto Charts• Problem Solving (5 Whys/5S/Just Do It)• Questioning/Probing:
– What have you learned?– What are you doing to investigate/problem-
solve?– What action are you planning to take?
3
Who We Measure…27 Locations
• Executive Office• Nursing Units• Operating Rooms• PACU• Lab• Pharmacy
• EVS• Emergency Dept.• Hospitalists• Resident Programs• Therapy (PT & OT)• Radiology
4
Gemba Walkers…
• CEO and Executive Leadership • Quality Team• LDM Leader• Nurse Coordinators• Visitors
5
What We Measure:GBMC’s Quadruple Aim
1. The Best Health Outcomes2. The Best Care Experience3. Lowest Cost (Least Waste)4. With the Most Joy for those providing
the care
6
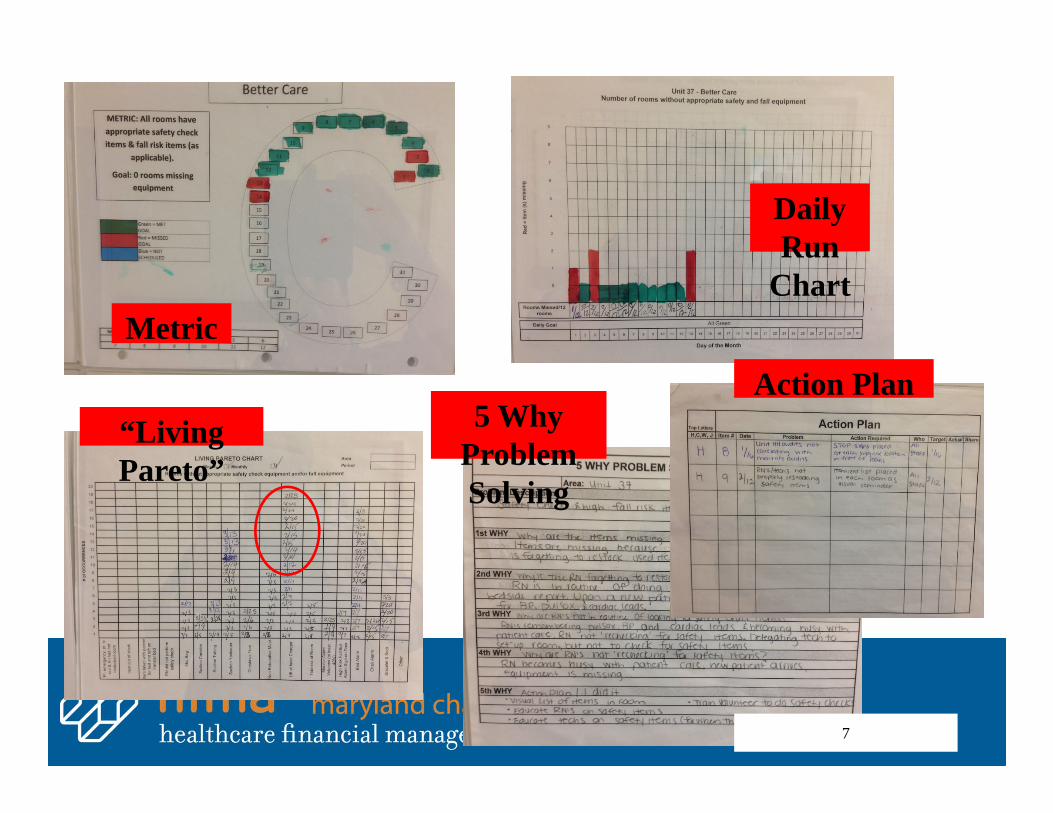
Metric
“Living Pareto”
Daily Run
Chart
5 Why Problem Solving
Action Plan
7
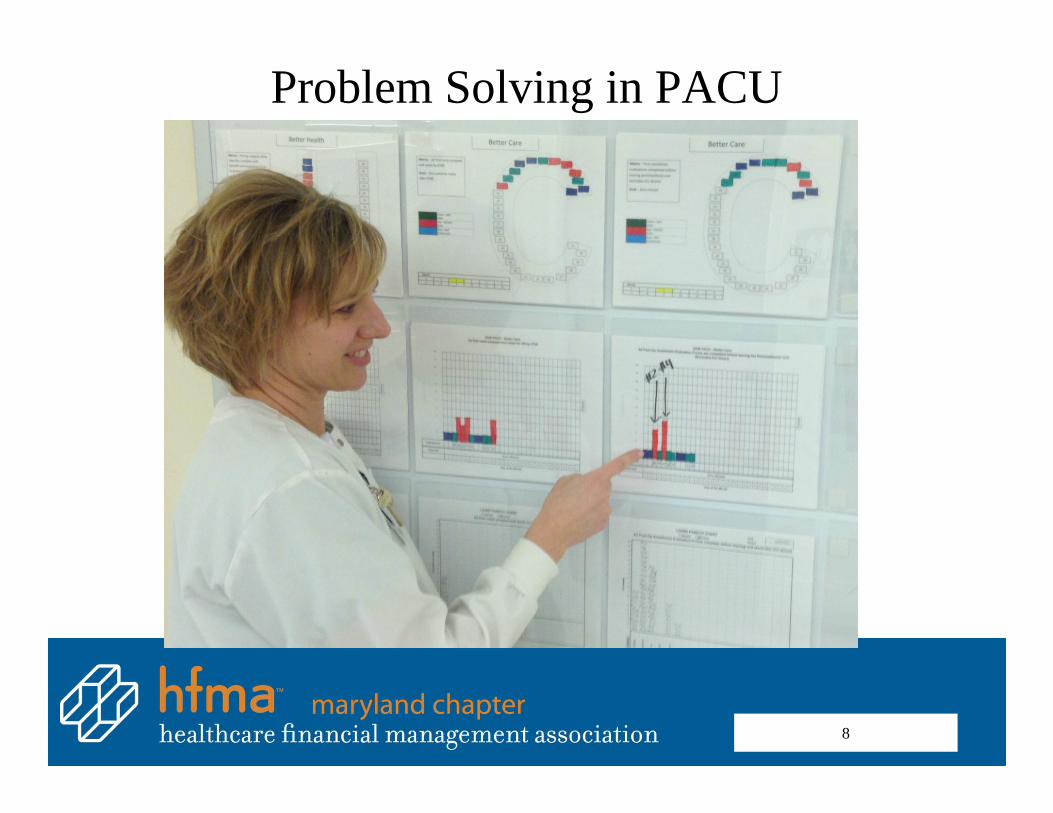
Problem Solving in PACU
8
What We Measure…Better Health
• Incidents of Patient Harm (Tier A MHAC’s)
• Infection Control Quality Indicators
• Patients with INR >4• Hand Hygiene• Patient Falls• Good Catches• Urgent C-Sections w/in 20
minutes• Critical Lab values w/in 1
hour
• All rooms clear of potentially harmful items
• Bedside report with Family• Central Line maintenance• Therapy evals within 24
hrs of written order• EKG turnaround
9
What We Measure…Better Care
• Missing Medications/Supplies/ Equipment
• Braden Score Intervention
• Medication Reconciliation
• Patient Triage Time • Customized Care Plans• Call Light Usage
• ED Transfer Time• Patient Med Education• PACU Evaluations• Safety Equipment
Audit• Discharge Summary
Time
10
What We Measure…Least Waste
• Drug Cart Stock Outs
• Supply & Equip Available
• Discharge Barriers• Incidental Overtime • OR Turnover Time
• Transport Time• OR 1st Cases On-
Time
11
What We Measure…More Joy
• Uninterrupted Meal Breaks
• Employee Injuries• Effective Teamwork• Patients Ready for
Tx• Able to Complete
Care
• Reduce OR Trips• Leaving on Time
12
How We Do It…• Going to the Gemba• Senior Team• No Fly Zone• Selecting Units• Timing• Logistics• Closing Huddle
13
How We Do It…• Process versus People• Just Culture• Focus on Process… not Blaming or
throwing People under the Bus
14
Kaizen Value Stream Map
Executive Daily Gemba Walk
15

Then… Now…
16
Real-time Problem SolvingHospitalists and ED
17
Results…
18
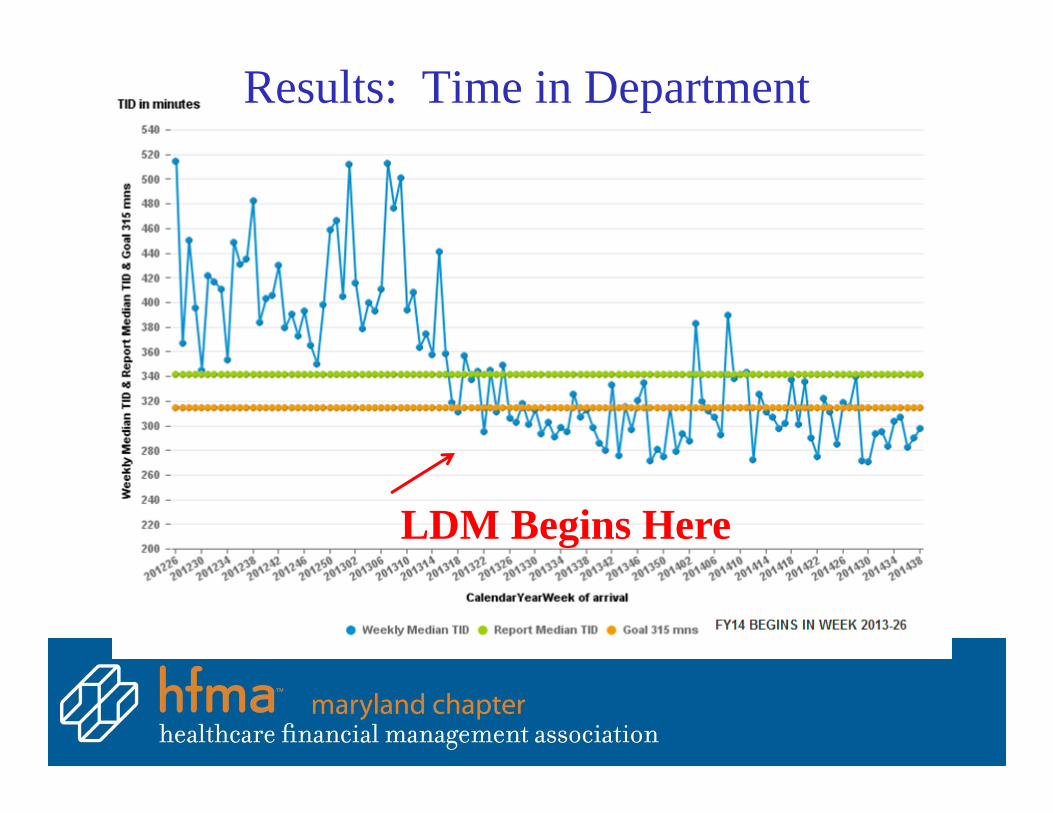
Results: Time in Department
LDM Begins Here
20
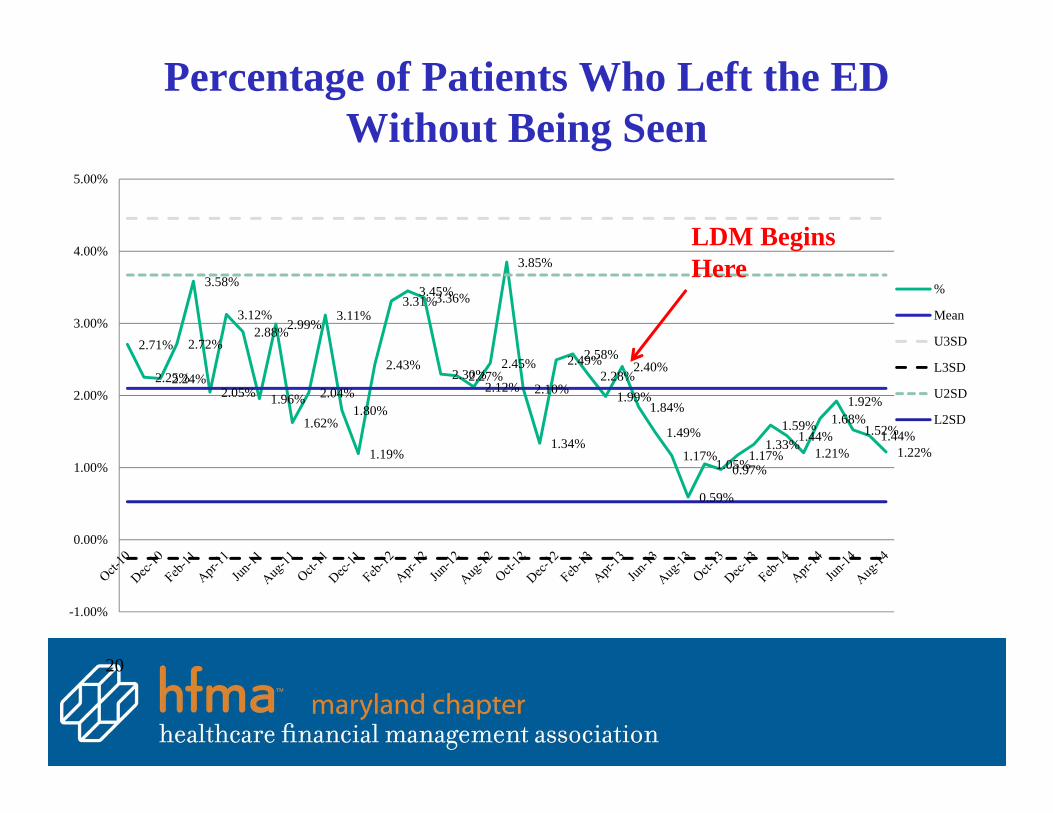
Percentage of Patients Who Left the EDWithout Being Seen
2.71%
2.25%2.24%
2.72%
3.58%
2.05%
3.12%2.88%
1.96%
2.99%
1.62%
2.04%
3.11%
1.80%
1.19%
2.43%
3.31%3.45%3.36%
2.30%2.27%2.12%
2.45%
3.85%
2.10%
1.34%
2.49%2.58%2.28%
1.99%
2.40%
1.84%
1.49%
1.17%
0.59%
1.05%0.97%1.17%
1.33%1.59%
1.44%1.21%
1.68%1.92%
1.52%1.44%1.22%
-1.00%
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
%
Mean
U3SD
L3SD
U2SD
L2SD
LDM Begins Here
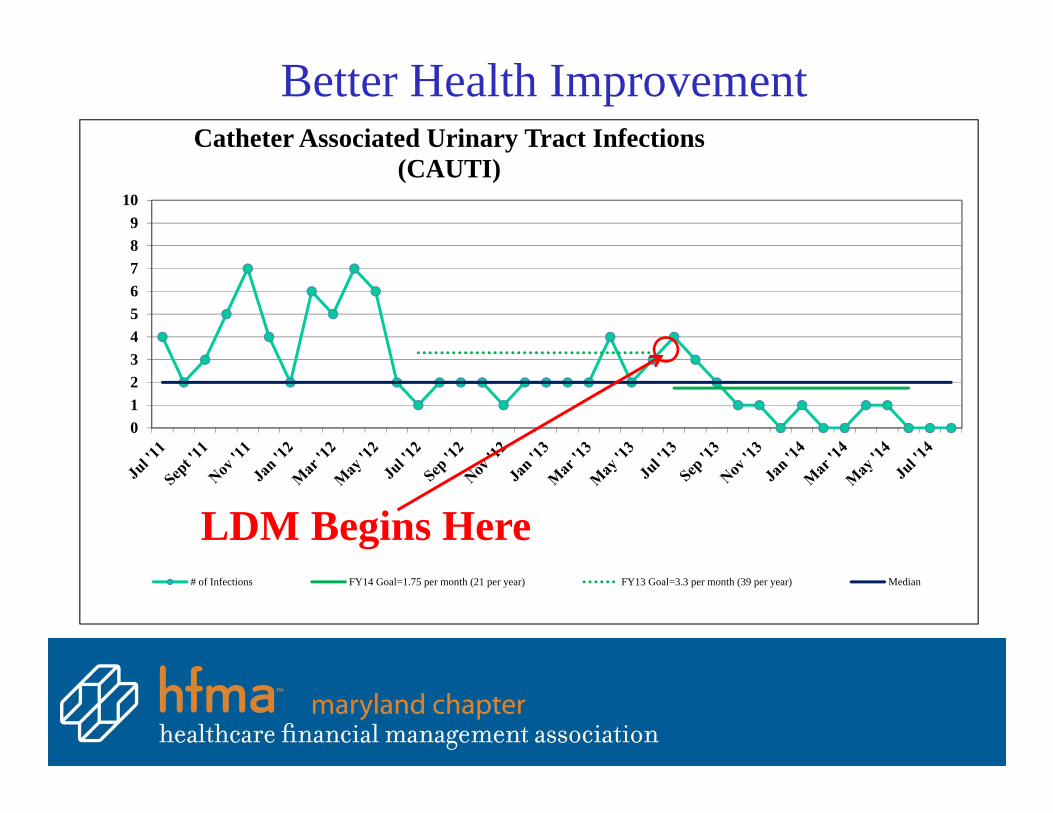
0123456789
10
Catheter Associated Urinary Tract Infections (CAUTI)
# of Infections FY14 Goal=1.75 per month (21 per year) FY13 Goal=3.3 per month (39 per year) Median
Better Health Improvement
LDM Begins Here
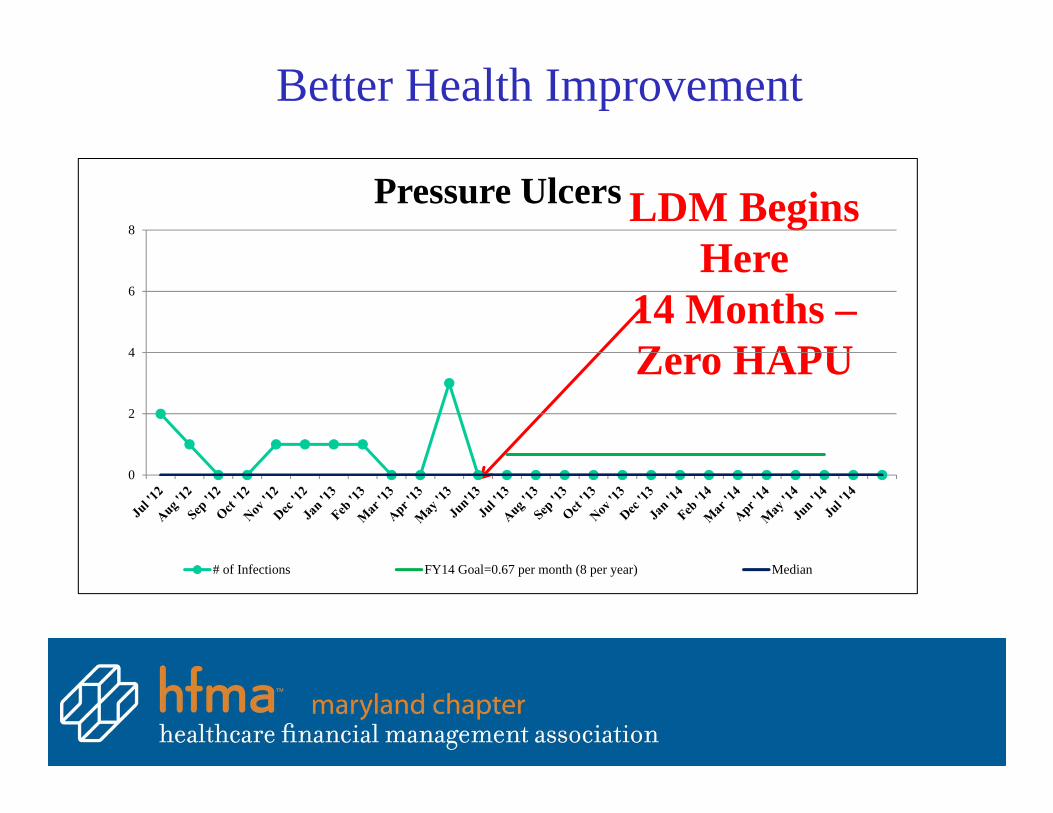
Better Health Improvement
LDM Begins Here
14 Months –Zero HAPU
0
2
4
6
8
Pressure Ulcers
# of Infections FY14 Goal=0.67 per month (8 per year) Median

73%
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
%9's a
nd 10's
Discharge Date
p Chart
Better Care ImprovementHCAHPS ‐ Overall Hospital Rating
The percent of patients scoring 9 or 10 to the question: “Using any number from 0 to 10, where 0 is the worst hospital possible and 10 is the best hospital possible, what number would you use to
rate this hospital during your stay.”
LDM Begins
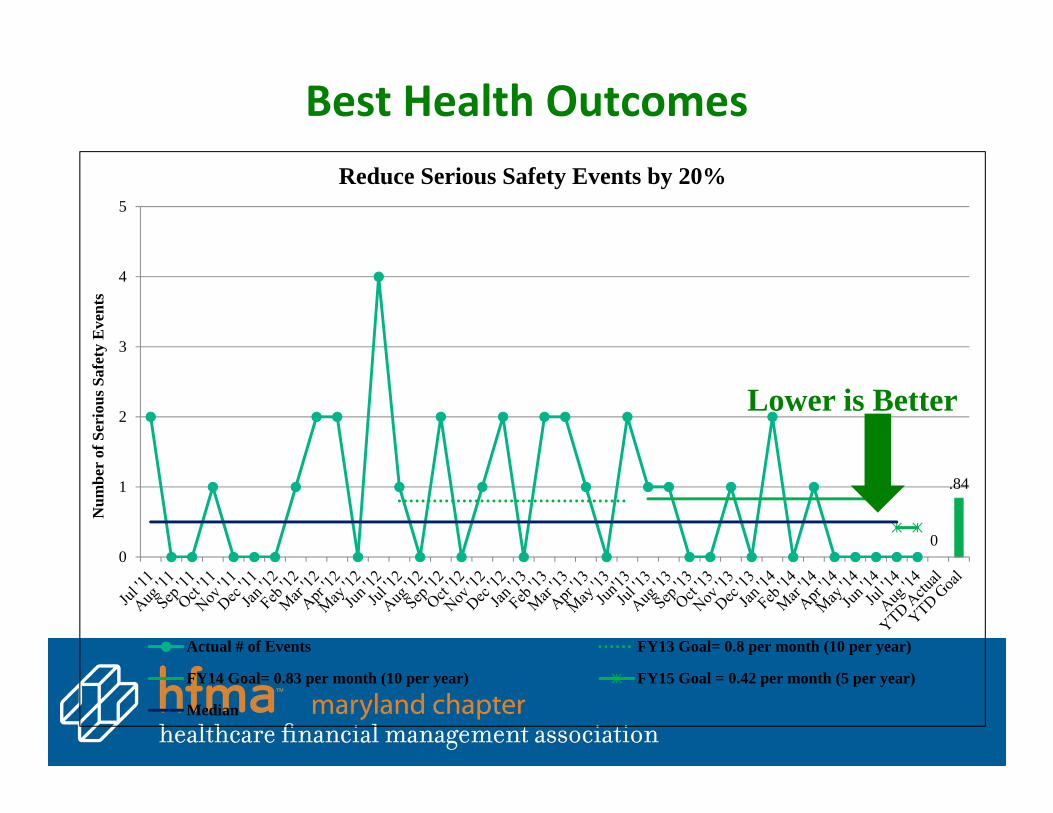
.84
00
1
2
3
4
5
Num
ber
of S
erio
us S
afet
y E
vent
s
Reduce Serious Safety Events by 20%
Actual # of Events FY13 Goal= 0.8 per month (10 per year)
FY14 Goal= 0.83 per month (10 per year) FY15 Goal = 0.42 per month (5 per year)
Median
Best Health Outcomes
Lower is Better

Best Health OutcomesReduce Incidents of Harm by 8% as Defined by
Tier A Maryland Hospital Acquired Conditions (MHAC)Lower is Better
*Dotted lines mean preliminary number
3158.813
0
10
20
30
40
50
60
70
Mon
thly
MH
AC
s
Monthly MHACs FY15 Goal = 29.4 per month (353 per year) Median
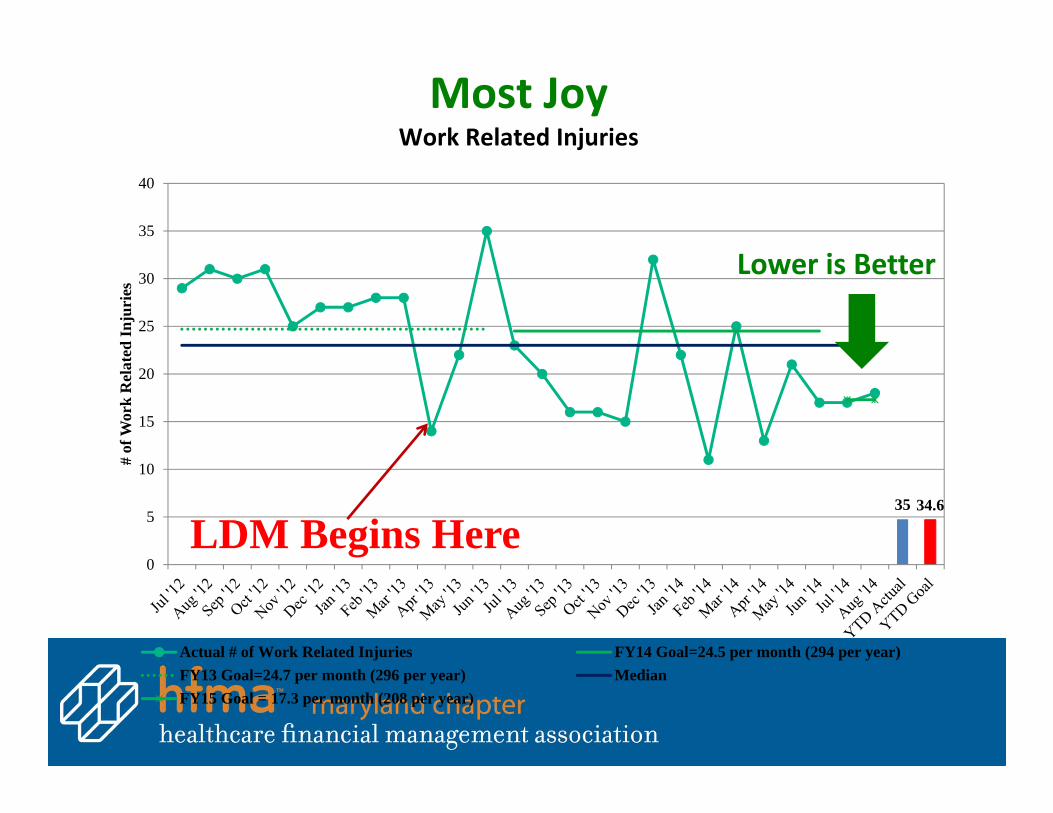
35 34.6
0
5
10
15
20
25
30
35
40
# of
Wor
k R
elat
ed In
juri
es
Actual # of Work Related Injuries FY14 Goal=24.5 per month (294 per year)FY13 Goal=24.7 per month (296 per year) MedianFY15 Goal = 17.3 per month (208 per year)
LDM Begins Here
Most JoyWork Related Injuries
Lower is Better
Lessons Learned
• Selecting Metrics…• Enrolling Staff/Physicians/Board….• Identify Goals…• Leadership Training…• Executive Sponsorship…• No Fly Zones…• How often…
27
Speaker Biography• George E.S. Bayless, III, CPA, Vice President – Finance
• George Bayless joined GBMC HealthCare in August 2006 as vice president of finance and serves as a member of the GBMC Executive Team. A veteran of more than 25 years of corporate financial experience in the public accounting and healthcare industries, Mr. Bayless is responsible for the development, implementation and maintenance of accounting systems for GBMC HealthCare. He is also responsible for system-wide financial planning and the annual operating and capital budget process.
• Prior to joining GBMC, Mr. Bayless served the University of Maryland Medical System (UMMS) for over 14 years. During that time Mr. Bayless served as the chief financial officer of two UMMS hospitals for 10 years and as the senior director of corporate internal audit and chief audit executive for 4 years. Prior to his service at UMMS, Mr. Bayless was with KPMG-Peat Marwick for 7 years, most recently as an audit senior manager.
• Mr. Bayless earned a Bachelor of Science in accounting from the University of Baltimore and is a licensed certified public accountant in the state of Maryland. Mr. Bayless holds memberships in the American Institute of Certified Public Accountants, the Maryland Association of Certified Public Accountants.
• Mr. Bayless has been a member of HFMA since 1989 and has served in many chapter leadership roles. During his membership, he has served as a board director and each of the officer positions including President. Mr. Bayless has also served on many chapter committees and has been the chair of the Sponsorship, Program, Strategic Planning, and Newsletter committees. Recently, Mr. Bayless served as the Regional Executive for HFMA Region 4, which includes the Maryland, Virginia/DC, North Carolina, West Virginia, and Kentucky chapters.
28