loss of the normal relationships between growth hormone, growth hormone-binding protein and...
TRANSCRIPT

Clinical Endocrinology (1994) 41, 517-524
Loss of the normal relationships between growth hormone, growth hormone-binding protein and insulin-like growth factor-I in adolescents with insulin-dependent diabetes mellitus
Kharen L. Clayton*, Jeff M. P. Hollyt, Lena M. S. Carlsson*, Jenny Jones§, Tim D. Cheetham*, Alistair M. Taylor* and David B. Dunger* 'Department of Paediatrics, University of Oxford, UK; $Research Centre for Endocrinology and Metabolism, University of Goteborg, Sweden; §Institute of Child Health, London, UK; and TDepartment of Medicine, University of Bristol, UK
(Received 76 March 1994; returned for revision 27 April 1994; finally revised 26 May 7994; accepted 14 June 7994)
Summary
OBJECTIVE It has been proposed that the dissociation between growth hormone secretion and insulin-like growth factor-I (IGF-I) concentrations in insulin-dependent dia- betes mellitus arises because of partial resistance at the GH receptor. In order to explore this hypothesis further we have examined the relations between IGF-I, GH-binding protein (GHBP), and GH secretion in normal subjects and patients with diabetes during puberty.
tion of IGF-I and GHBP levels were obtained from 104 patients with diabetes and 89 puberty matched controls. Thirty-four of the controls and 42 of the patients with diabetes also underwent an overnight GH secretory profile with measurements of GH every 15-20 minutes between 2000 and 0800 h. RESULTS In multivariate analysis using sex, puberty stage, and presence or absence of diabetes as depen- dent variables, diabetes was associated with increased GH levels (F = 23-04, P < 0.001), reduced IGF-I (F = 10.89, P < OOOl), and reduced GHBP levels (F = 31.36, P < 0.001). A negative relation between GH and GHBP levels ( r = -0.44, P < 001) was found in normal subjects but this was absent in those with diabetes. Both GHBP and IGF-l levels in the diabetic subjects were correlated with total insulin dose ( r = 04, P < 0.001, and r = 0-46, P < 0.001, respectively). Yet there was no direct correlation between
Correspondence: Dr D. B. Dunger, Department of Paediatrics, John Radcliffe Hospital, Oxford OX3 9DU, UK. Fax: 0865 220479.
DESIGN AND SUBJECTS Blood samples for the estima-
GHBP and IGF-I concentrations. The variation in IGF-I levels was also related to glycosylated haemoglobin levels in the diabetics (r = -0-27, P = 0-01). In a stepwise multiple regression analysis insulin dose contributed 23%, HbA, 4.4% and C-peptide levels 37% to the vari- ation in IGF-I levels. CONCLUSIONS In adolescents with insulin dependent diabetes mellitus, the elevated OH concentrations are associated with low circulating IGF-l and GHBP concen- trations and the normal reciprocal relation between GHBP and GH is no longer evident. Although IGF-I and GHBP are both related to insulin dose, there is no direct correlation between these variables. This may indicate that GHBP reflects GH receptor numbers but not neces- sarily post receptor events, and the weak positive corre- lation between GH and IGF-I indicates that increased growth hormone secretion may compensate for reduced receptor numbers.
Spontaneous growth hormone secretion is increased in adolescents with insulin-dependent diabetes mellitus (IDDM) at all stages of puberty (Edge et al., 1990). Overnight GH secretory profiles are characterized by increases in both pulse amplitude and baseline concentra- tions. These abnormalities have direct effects on insulin sensitivity (Dunger et al., 1991) which may lead to a worsening of metabolic control (Press et al., 1984).
In contrast, circulating concentrations of insulin-like growth factor-I (IGF-I) and IGFBP-3 tend to be low or in the low normal range (Taylor et al., 1988; Batch el al., 1991) and the adolescent growth spurt may be blunted, particu- larly in girls (Salardi et al., 1986). It has been suggested that the partial resistance to the effects of GH occurs a t the level of the hepatic GH receptor and may arise because of inadequate portal delivery of insulin in IDDM. In-vitro studies suggest that insulin enhances IGF-I production (Daughaday et al., 1976) by either direct regulation of the growth hormone receptor (Baxter et al., 1980) or a permissive effect on post growth hormone receptor events (Maes et al., 1986). Some confirmation of the first of these mechanisms has come from recent studies of the GH- binding protein (GHBP). This peptide is probably identical
51 7

518 K . L. Clayton et a / . Clinical Endocrinology (1994) 41
to the extracellular domain of the growth hormone receptor (Leung et al., 1987) and the low levels found in subjects with IDDM has been interpreted as indicating low levels of the growth hormone receptor (Menon et a[., 1992; Massa et al., 1993; Holl e f al., 1993).
The relation between GH levels and those of GHBP and IGF-I has not been previously defined. In order to characterize these complex abnormalities further, we have examined the relation between GH, IGF-I and GHBP in a large cohort of normal subjects and adolescents with IDDM during puberty.
Methods
Control subjects
Random blood samples were obtained from 55 normal adolescents who were participating in a longitudinal study of pubertal growth and development. In addition, samples were obtained from 34 healthy siblings of diabetic children enrolled for metabolic studies. The latter group had normal glycosylated haemoglobin concentrations and all but one were islet cell antibody negative (one subject had an islet cell antibody titre of 40 JDF units, but a glycosylated haemoglobin level of 5.1%). The children enrolled for the metabolic studies also underwent an overnight profile to assess GH levels.
Diabetic subjects
Random blood samples were also obtained from 104 subjects with IDDM attending the children’s diabetes clinic in Oxford. All the subjects were on combinations of soluble and intermediate acting insulin administered as two or four injections daily. Forty-two of these patients with IDDM underwent an overnight GH profile. The median duration of diabetes for the whole cohort was 9.5 years (range 0.65-18.35), HbAl 13.7% (range 7.0-20.3), total insulin dose 1.12 Ujkg (range 0.55-1.68) and C-peptide level 0.44 pmoljl (range 0-0+38).
All the subjects participating in these studies were puberty staged (Tanner, 1962) and for the purpose of analysis, breast stage was used in girls and genital stage in boys. Height SD scores were calculated from the data of Tanner et al. (1966) and body mass index (BMI) from the heights and weights. The characteristics of the various cohorts are summarized in Table 1.
Protocol
The growth hormone profiles in 34 normal subjects and 42
Table 1 Details of puberty stage and sex of total cohort and subjects undergoing overnight GH secretory profiles
Diabetic Normals
Males Females Males Females
All
Puberty stage 1 7 7 10 9 2 14 10 9 8 3 9 7 10 6 4 14 11 10 8 5 6 19 10 9
Total 50 54 49 40
Subjects undergoing overnight GH profiles
Puberty stage 1 2 2 4 4 2 4 1 5 2 3 3 3 3 1 4 4 5 2 3 5 4 14 3 7
Total 17 25 17 17
patients with IDDM were carried out between 2000 and 0800h. Samples were taken every 15 minutes for GH analysis using a heparinized continuous sampling technique. Data from some of these subjects were the subject of an earlier report from our group (Edge et al., 1990).
Assay details
Samples for GH assay were kept at room temperature until the overnight profiles were completed and then spun and separated. Plasma was stored at -20°C. Plasma GH concentrations were measured by an immunoradiometric assay (NETRIA, St Bartholomew’s Hospital, London, UK), using international reference standard 80j505, and all samples from each individual profile were analysed in the same batch. The interassay coefficients of variation at GH concentrations 3.5, 15.2 and 77,4mU/l were 9.4, 7.7 and 10.5% respectively and the intra-assay coefficients of variation at GH concentrations 2.9, 4.8, 17-7 and 69.4mU/1 were 8.0, 9.7, 4.9 and 3.4%.
GHBP concentrations were measured in serum samples using a ligand-mediated immunofunctional assay (Carlsson et al., 1991). This assay system is based on the binding of GHBP to its ligand GH and the specific reactions between both the immobilized monoclonal antibody to the GHBP

Clinical Endocrinology (1994) 41 GH, GHBP, IGF-I relations in IDDM 519
and the enzyme labelled monoclonal antibody to the GH bound to GHBP. The lower limit of detection for the assay was 7.8 pmol/l. The interassay coefficients of variation were 12.9, 11.3 and 9.6% at analyte concentrations of 136, 293 and 674 pmol/l respectively. The intra-assay coefficients of variation ranged between 6.3 and 8.9%.
Samples for IGF-I assay were acid-ethanol extracted and serum IGF-I concentrations were determined by radio- immunoassay using a polyclonal antibody (A/B R557A) raised in rabbits against purified human. IGF-I (Morrell et al., 1989). The interassay coefficients of variation were 9,4.5 and 6.2% at analyte levels of 69, 206 and 672 pg/l respectively and the intra-assay variation was 4% at 206 pg/l.
Glycosylated haemoglobin (HBA,) was measured by agar gel electroendosmosis (Corning method), reference range 5.6-8.2% (Kay et al., 1988). C-peptide levels were measured in the diabetic subjects (stimulated glucose concentration > 7 mmol/l) by radioimmunoassay from Diagnostic Pro- ducts (DPL Division, EUROiDPC Ltd, Glyn Rhonwy, Llanberis, Caernarfon, Gwynedd, Wales LL55 4EL). The assay sensitivity was 19 pmol/l; within assay coefficients of variation were 5-0 and 3.3% at 79 and 248pmol/l respectively and between assay coefficients of variation were 8.8 and 8.0% at 82 and 228 pmol/l.
Statistical analysis
The significance of differences across pubertal stages between the normal and diabetic population and sexes was assessed using a one-way analysis of variance: the Kruskal- Wallis test. The Mann-Whitney U-test was performed to find the significant differences between the normal and diabetic population at each puberty stage. Correlation coefficients were performed in order to assess associations between variables. Multiple and stepwise regression was carried out using Minitab (Minitab Inc., PA., USA). P values < 0.05 were considered significant.
Results
Normal subjects
Mean overnight GH concentrations were elevated in puberty when compared with prepubertal subjects (GI and Bl) and the highest levels were noted in girls at B2/B3 and in boys at G4 and G5 as previously reported (Edge et al., 1990) (Fig. la).
GHBP levels did not show a significant variation with puberty stage in either sex (Fig. 1 b). Levels in females tended to be higher than those in males in prepubertal subjects
T
A 2 200
g 100
E a
a - (3
0
500 Z 400
2 300
T 200
s 100
\ - U
n - 1 2 3 4 5 1 2 3 4 5
Puberty stage
Fig. 1 Changes in a, overnight growth hormone levels; b, growth hormone binding protein levels; and c, IGF-I levels in i, boys and ii, girls according to puberty stage in subjects a, with diabetes and 0, controls. Means and SEM are represented.
(B1 and GI) (204 f 38 and 143 & 29 pmol/l, P < 0.05) and when female subjects B4 were compared with males at G4 (326 & 94 and 120 f 19pmol/l respectively, P < 0.02).
Serum IGF-I concentrations showed a significant increase in relation to puberty stage in both boys (P < 0.002) and girls (P<O.O5) (Fig. Ic), the highest levels being noted in both girls and boys at B4 and G4.
Subjects with IDDM
Mean overnight GH concentrations showed a similar pattern of change in relation to puberty stage as that observed in the normals, but values were greater in the diabetic subjects at all puberty stages except stage B2 as previously reported (Edge et al., 1990) (Fig. la). Compar- ison of the diabetic and control data using multiple regression to allow for the effects of puberty stage and sex revealed that the presence or absence of diabetes was a major determinant of GH levels (F= 23.04, P < 0.001).
GHBP levels did not change in relation to puberty stage in either sex, but levels were significantly lower than controls at

520 K. L. Clayton et al. Clinical Endocrinology (1994) 41
I , , I
0 10 20 30
r ( b )
. *. 0 10 20 30 40
Mean overnight growth hormone (mu/ \ )
fig. 2 The relation between levels of GHBP and mean overnight GH concentrations in a, normal adolescents; and b, adolescents with diabetes.
puberty stage B4 in girls and stages G1, G2 and G3 in boys (Fig. 1 b). Multiple regression confirmed that diabetes was associated with significantly lower levels of GHBP (Fz31.36, P<0.001).
Serum IGF-I concentrations in the diabetic subjects showed no significant changes with pubertal stage in the girls, and levels were significantly lower than control values
Table 2 lniportanl correlations in the diabetic and normal cohorts studied
Normals Diabetics
I n P r n P ~.
Mean overnight GH secretion GHBP -0.46 34 < O . O l IGF-I 0.28 34 0.11 HtSDS -004 34 0.81 BMI -0.37 34 0.03 HbAl Totdl insulin C-peptide
GHBP IGF-I 0.03 89 0.76 HtSDS -0.23 89 0.03 BM I -0.03 85 0.80 HbAi Total insulin C-peptide
IGF-I HtSDS 0.24 89 0.02 BMl 0.27 86 0.009 HbAi Total insulin C-peptide
-0.13 28 0.5 0.34 33 0.051 0.11 31 0.56 0.15 26 0.47 0.07 33 0-71 0.02 31 0.92
-0.07 33 0.72
0.07 82 0.51 -0.11 79 0.32 -0.007 80 0.95 -0.07 82 0.50
0.38 80 <0.001 0.003 82 0.97
0,001 84 0.99 -0.06 80 0.60 -0.27 87 <0.01
0.46 85 <0.001 0.11 87 0.32
at stage B5 (PCO.05) (Fig. lc). In contrast, there was a significant increase with puberty in boys, maximal levels being observed at G5. Levels were lower than control values at all stages but the differences reached statistical signifi- cance only at stage G4 (P<O.Ol). Multiple regression indicated that, independent of the effects of puberty and sex, the presence of diabetes was associated with signifi- cantly lower levels of IGF-I (F= 10.89, P < 0.001).
Relations between GH, GHBP and IGF-I in controls
In the normal subjects there was a negative correlation between mean overnight GH concentrations and GHBP levels ( r = -0.44, P < 0.01, after log transformation r = -0.59, P<O.OOl). The distribution of the data may well be curvilinear (Fig. 2a). There was however no relation with either GH or GHBP levels and IGF-I concentrations.
There was no relation between mean overnight GH concentrations and height SDS. Height SDS did show a weak correlation with GHBP ( r = -0.22, P < 0.03) and IGF-I ( r = 0.24, P < 0.02). BMI was inversely correlated with mean overnight GH ( r = -0.37, P = 0.03) and positively correlated with IGF-I concentrations ( r = 0.27, P= 0.009). There was no correlation between GHBP and BMI (Table 2).
Relations between GH, GHBP and IGF-I in subjects with diabetes
In the subjects with diabetes, these relations were perturbed. There was no correlation between GHBP levels and GH concentrations (Fig. 2b), although it could be argued that the data may define part of the same curvilinear distribution seen in normals.
There was a weak positive correlation between mean overnight GH and IGF-I concentrations ( r = 0.34, P 0.05), but no relation between GHBP and IGF-I concentrations.
Height SDS was not related to either GHBP or IGF-I concentrations in the diabetic subjects.
BMI was significantly greater in diabetic than in normal subjects (20.2 i 0.26 vs 18.95 f 0.3, P < 0.001) of both sexes. However, there were no correlations with IGF-I, GH or GHBP in these subjects.
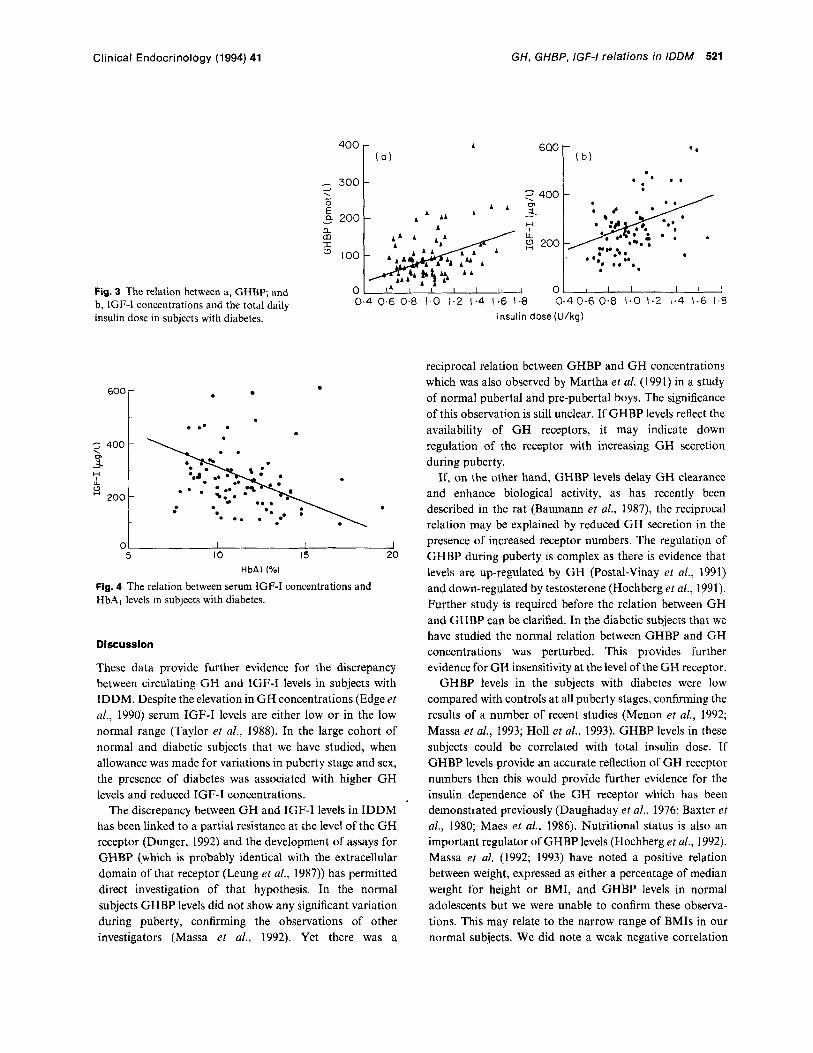
In the diabetic subjects both GHBP levels and IGF-I concentrations were related to their total insulin dose ( r = 0.4, P < 0,001 and r = 0.46, P < 0,001 respectively) (Fig. 3a and b). IGF-I concentrations were also related to HbA, ( r = -0.27, P=O.Ol) (Fig. 4). In a stepwise multiple regression analysis total insulin dose contributed 23%, HbAl 4.4% and C- peptide 3.7% to the variation in IGF-I levels.
Clinical Endocrinology (1994) 41
600
3 400 . 0, - i L H
2 0 0 -
GH, GHBP, IGF-I relations in IDDM 521
-
-
Fig. 3 The relation between a, GHBP; and b, IGF-I concentrations and the total daily insulin dose in subjects with diabetes.
400
- 300 1 --I
E" - a 200 a m I
100
0
. . .* . .
A 600 ( a ) . * ' I . .
I I I I I I j
0.4 06 0.8 1.0 1.2 1.4 1.6 1-8 0.40.6 0.8 I.0 1.2 1.4 1-6 1.8 insulin dose (U/kg)
- - .
5 10 15 20 HbAl (%)
Fig. 4 The relation between serum IGF-I concentrations and HbA, levels in subjects with diabetes.
Discussion
These data provide further evidence for the discrepancy between circulating GH and IGF-I levels in subjects with IDDM. Despite the elevation in GH concentrations (Edge et al., 1990) serum IGF-I levels are either low or in the low normal range (Taylor et al., 1988). In the large cohort of normal and diabetic subjects that we have studied, when allowance was made for variations in puberty stage and sex, the presence of diabetes was associated with higher GH levels and reduced IGF-I concentrations.
The discrepancy between GH and IGF-I levels in IDDM has been linked to a partial resistance at the level of the GH receptor (Dunger, 1992) and the development of assays for GHBP (which is probably identical with the extracellular domain of that receptor (Leung et al., 1987)) has permitted direct investigation of that hypothesis. In the normal subjects GHBP levels did not show any significant variation during puberty, confirming the observations of other investigators (Massa et al., 1992). Yet there was a
reciprocal relation between GHBP and GH concentrations which was also observed by Martha et al. (1991) in a study of normal pubertal and pre-pubertal boys. The significance of this observation is still unclear. If GHBP levels reflect the availability of GH receptors, it may indicate down regulation of the receptor with increasing GH secretion during puberty.
If, on the other hand, GHBP levels delay GH clearance and enhance biological activity, as has recently been described in the rat (Baumann et al., 1987), the reciprocal relation may be explained by reduced GH secretion in the presence of increased receptor numbers. The regulation of GHBP during puberty is complex as there is evidence that levels are up-regulated by GH (Postal-Vinay et al., 1991) and down-regulated by testosterone (Hochberg et al., 1991). Further study is required before the relation between GH and GHBP can be clarified. In the diabetic subjects that we have studied the normal relation between GHBP and GH concentrations was perturbed. This provides further evidence for GH insensitivity at the level of the GH receptor.
GHBP levels in the subjects with diabetes were low compared with controls at all puberty stages, confirming the results of a number of recent studies (Menon et al., 1992; Massa et al., 1993; Holl et al., 1993). GHBP levels in these subjects could be correlated with total insulin dose. If GHBP levels provide an accurate reflection of GH receptor numbers then this would provide further evidence for the insulin dependence of the GH receptor which has been demonstrated previously (Daughaday et al., 1976; Baxter et a/., 1980; Maes et al., 1986). Nutritional status is also an important regulator of GHBP levels (Hochberg et al., 1992). Massa et al. (1992; 1993) have noted a positive relation between weight, expressed as either a percentage of median weight for height or BMI, and GHBP levels in normal adolescents but we were unable to confirm these observa- tions. This may relate to the narrow range of BMIs in our normal subjects. We did note a weak negative correlation

522 K. L. Clayton et a/. Clinical Endocrinology (1994) 41
between GH and BMI together with a positive correlation between IGF-I and BMI which is compatible with previous observations of the nutritional regulation of the GH-IGF-I axis (Counts et al., 1992). In the diabetic subjects these correlations were no longer evident. If the nutritional relation between these variables is mediated by insulin then this observation is not unexpected as insulin doses in our diabetic subjects are not necessarily adjusted to BMI but determined by a number of other variables.
We were able to detect weak negative correlations between height SDS and GHBP but no relation with GH concentrations in the normal subjects. Hqight velocity data were not available in the majority of these subjects and the interpretation of these observations is difficult. Height SDS also correlated with IGF-I concentrations in the normal subjects, but not in patients with IDDM. In this respect it was of interest to note that girls with IDDM showed no rise in IGF-I concentrations with puberty, whereas the boys did show a modest increase. Girls with IDDM often show blunting of the pubertal growth spurt, which is more severe than that noted in boys (Salardi et a/., 1986; Brown et al., 1994). Recent studies in normal subjects indicate that the relation between GH concentrations and growth velocity is more clearly evident in girls than in boys (Edge et al., 1989; Merimee et al., 1991). The more deranged GH-IGF-I axis in the girls with IDDM may explain their impaired growth.
Serum IGF-I levels in our diabetic subjects were related to total insulin dose, C-peptide status and overall glycaemic control as judged by HbAl concentrations. These findings are similar to those reported by other investigators (Salardi et al., 1986; Rogers et al., 1991; Massa et al., 1993). Thus, both IGF-I and GHBP levels were related to insulin dose, yet there was no direct correlation between GHBP and IGF-I concentrations. Massa et a[. (1993) made similar observations and concluded that decreased hepatic GH receptor levels play only a minor role in the regulation of circulating IGF-I concentrations. There may be alternative explanations for these findings. Insulin may be exerting differential effects at the level of the GH receptor (Daughaday et al., 1976; Baxter et af., 1980), and at the post receptor translational level (Maes et al., 1986). Circulating GHBP levels may reflect receptor numbers, but not post receptor translational events. The C-peptide status of our subjects was also shown to be an independent determinant of IGF-I concentrations, and the appropriate portal delivery of insulin may be as important a determinant of IGF-I levels as total insulin dose (Dunger et al., 1993). The other determinant of circulating IGF-I levels in IDDM would appear to be the GH concentration as we were able to show a weak positive correlation between GH and IGF-I.
It has been argued that low levels of IGF-I and reduced
IGF bioactivity are the principal determinants of GH hypersecretion in IDDM (Dunger, 1992). Some confirma- tion of this hypothesis has come from recent studies where restoration of normal concentrations of IGF-I using rhIGF-I have led to consistent reductions in GH secretion (Cheetham et al., 1993). We might therefore expect a negative correlation between mean overnight GH and IGF-I concentrations, similar to that reported by Rieu and Binoux (1985) in subjects with IDDM during acute metabolic decompensation; in fact, we observed a weak positive correlation between IGF-I and GH, similar to that reported by Batch et al. (1991). This positive correlation could be explained by an altered set point for trophic stimulation whereby an increase in GH secretion might lead to improved IGF-I generation. However, a simple relation between GH and IGF-I in subjects with IDDM is unlikely. Intensification of insulin therapy, which leads to an increase in portal delivery of insulin sufficient for normal IGF-I production, may, paradoxically, through the production of peripheral hyperinsulinaemia, result in further stimulation of G H production (Press et a/., 1992). Thus IGF-I levels may reflect increasing GH levels in under-insulinized subjects, whereas those who are over-insulinized may show rises in both GH and IGF-I.
We can conclude that in adolescents with IDDM the elevated GH concentrations are associated with low circulating levels of IGF-I and GHBP and the normal reciprocal relation between GHBP and GH is no longer evident. In these subjects, total insulin dose is an important determinant of both IGF-I and GHBP concentrations. The lack of any relation between IGF-I and GHBP may indicate that although GHBP levels may reflect GH receptor numbers they do not necessarily correlate directly with post receptor events.
The positive correlation between GH and IGF-I may indicate that increased GH secretion may overcome the effect of reduced receptor numbers in insulin deficient subjects.
Acknowledgements
We would like to thank Dr Julie Edge and Jan Gilbert for their help in collecting samples from normal and diabetic subjects, Professor M. A. Preece and Dr L. Cox for providing samples from the Chard study of normal pubertal growth, and Marita Dover for her secretarial help.
Tim Cheetham was supported by Kabi Pharmacia.
References
Batch, J.A., Baxter, R.C. & Werther, G. (1991) Abnormal regulation of insulin-like growth factor binding proteins in

Clinical Endocrinology (1994) 41 GH, GHBP, IGF-I relations in IDDM 523
adolescents with insulin-dependent diabetes. Journal of Clinical Endocrinology and Metabolism, 73, 964-968.
Baumann, G., Amburn, K.D. & Buchanan, T.A. (1987) The effect of circulating growth hormone-binding protein on metabolic clearance, distribution and degradation of human growth hormone. Journal of Clinical Endocrinology and Metabolism, 64, 657-660.
Baxter, R.C., Bryon, J.M. & Turtle, J.R. (1980) Somatogenic receptors of rat liver: regulation by insulin. Endocrinology, lW,
Brown, M., Ahmed, M.L., Clayton, K.L. & Dunger, D.B. (1994) Growth during childhood and final height in Type 1 diabetes. Diabetic Medicine, 11, 182-187.
Carlsson, L.M.S., Rowland, A.M., Clark, R.G., Gesundheit, N. & Wong, W.L.T. (1991) Ligand-mediated immunofunctional assay for quantitation of growth hormone-binding protein in human blood. Journal of Clinical Endocrinology and Metabolism, 13, 121 6- 1223.
Cheetham, T.D., Jones, I., Taylor, A.M., Holly, J.M.P., Matthews, D.R. & Dunger, D.B. (1993) The effects of recombinant insulin- like growth factor-I administration on growth hormone levels and insulin requirements in adolescents with Type I (insulin- dependent) diabetes mellitus. Diabetologia, 36, 678-681.
Counts, D.R., Gwirtsman, H., Carlsson, L.M.S., Lesem, M. & Cutler Jr, G.B. (1992) The effect of anorexia nervosa and refeeding on growth hormone-binding protein, the insulin-like growth factors (IGFs), and the IGF-binding proteins. Journal of Clinical Endocrinology and Metabolism, 15,762-761.
Daughaday, W.H., Phillips, L.S. & Mueller, M.S. (1976) The effects of insulin and growth hormone on the release of somatomedin by the isolated rat liver. Endocrinology, 98, 1214-1219.
Dunger, D.B., Edge, J.A., Pal, R., Taylor, A.M., Holly, J.M.P. & Matthews, D.R. (1991) Impact of increased growth hormone secretion on carbohydrate metabolism in adolescents with diabetes. Acta Paediatrica Scandinavica Supplement, 311, 69-77.
Dunger, D.B. (1992) Diabetes in puberty. Archives of Disease in Childhood, 61, 569- 573.
Dunger, D.B., Cheetham, T.D., Holly, J.M.P. & Matthews, D.R. (1993) Does recombinant insulin-like growth factor I have a role in the treatment on insulin-dependent diabetes mellitus. Acta Paediatrica Supplemenr, 388,49-52.
Edge, J.A., Dunger, D.B., Matthews, D.R., Gilbert, J.P. & Smith, C.P. (1990) Increased overnight growth hormone concentrations in diabetics compared with normal adolescents. Journal of Clinical Endocrinology and Metabolism, 71, 1356-1362.
Edge, J.A., Hourd, P., Edwards, R. & Dunger, D.B. (1989) Urinary growth hormone during puberty in normal and diabetic children. Clinical Endocrinology, 30, 41 3-420.
Hochberg, Z., Barkey, R.J., Even, L., Peleg, I., Youdim, M.B.H. & Amit, T. (1991) The effect of human growth hormone therapy on GH binding protein in GH-deficient children. Acta Endocrinolo- gica (Copenh), 121, 603-608.
Hochberg, Z., Hertz, P., Colin, V., Ish-Shalon, S., Youdim, M.B.H. & Amit, T. (1992) The distal axis of growth hormone in nutritional disorders: GH binding protein, insulin like growth factor-I (IGF-I) and IGF-I receptors in obesity and anorexia nervosa. Metabolism, 41, 106-1 12.
Holl, R.W., Seigler, B , Scherbaum, W.A. & Heinze, E. (1993) The serum growth hormone-binding protein is reduced in young patients with insulin-dependent diabetes mellitus. Journal of Clinical Endocrinology and Metabolism, 76, 165-167.
1176-1 181.
Kay, J.D.S., Standing, S., Strang, S. & Dunger, D.B. (1988) Glycated haemoglobin in specimens collected by fingerprick from children: performance data, comparison with venous blood specimens and reference values. Annals of Clinical Biochemistry,
Leung, D.W., Spencer, S.A., Cachianes, G., Hammonds, R.G., Collins, C., Henzel, W.J., Barnard, R., Waters, M.J. & Wood, W.I. (1987) Growth hormone receptor and serum binding protein: purification, cloning and expression. Nature, 330, 537- 43.
Maes, M., Underwood, L.E. & Ketelslegers, J.-M. (1986) Low serum somatomedin-C in insulin-dependent diabetes: evidence for a post receptor mechanism. Endocrinology, 118, 377-382.
Martha, P.M., Reiter, E.O., Davila, N., Shaw, M.A., Holcombe, J.H. & Baumann, G. (1991) Growth hormone-binding protein activity is inversely related to 24-hr growth hormone release in normal boys. Journal of Clinical Endocrinology and Metabolism,
Martha Jr, P.M., Rogol, A.D., Carlsson, L.M.S., Gesundheit, N. & Blizzard, R.M. (1993) A longitudinal assessment of hormonal and physical alterations during normal puberty in boys. I Serum growth hormone-binding protein. Journal of Clinical Endocrinol- ogy and Metabolism, 11,452-457.
Massa, G., Bouillon, R. & Vanderschueren-Lodeweyckx, M. (1992) Serum levels of growth hormone-binding protein and insulin-like growth factor-I during puberty. Clinical Endocrinology, 31, 175- 180.
Massa, G., Dooms, L., Bouillon, R. & Vanderschueren-Lode- weyckx, M. (1993) Serum levels of growth hormone-binding protein and insulin-like growth factor-I in children and adolescents with type 1 (insulin-dependent) diabetes mellitus. Diabetologia, 36, 239-243.
Menon, R.K., Arslanian, S., May, B., Cutfield, W.S. & Sperling, M.A. (1992) Diminished growth hormone-binding protein in children with insulin-dependent diabetes mellitus. Journal of Clinical Endocrinology and Metabolism, 74, 934-938.
Merimee, T.J., Russell, B., Quinn, S. & Riley, W. (1991) Hormone and receptor studies: relationship to linear growth in childhood and puberty. Journal of Clinical Endocrinology and Metabolism,
Morrell, D.J., Dadi, H., More, J., Taylor, A.M., Dabestani, A,, Buchanan, C.R., Holder, A.T. & Preece, M.A. (1989) A monoclonal antibody to human insulin-like growth factor-I: Characterisation, use in radioimmunoassay and effect on the biological activities of growth factor. Journal of Molecular Endocrinology, 2, 201-206.
Postal-Vinay, M.-C., Tar, A,, Hocquette, J.F., Clot, J.P., Fontoura, M., Brauner, R. & Rappaport, R. (1991) Human plasma growth hormone-binding proteins are regulated by growth hormone and testosterone. Journal of Clinical Endocrinology and Metabolism,
Press, M., Tamborlane, W.V. & Sherwin, R.S. (1984) Importance of raised growth hormone levels in mediating the metabolic derangements of diabetes. New England Journal of Medicine,
Press, M., Caprio, S., Tamborlane, W.V., Bhushan, R., Thorner, M., Vale, W., Rivier, J. & Sherwin, R.S. (1992) Pituitary response to growth hormone-releasing hormone in IDDM. Abnormal responses to insulin and hyperglycaemia. Diabetes, 41, 17-21.
Rieu, M. & Binoux, M. (1985) Serum levels of insulin-like growth factor (IGF) and IGF binding proteins in insulin dependent
25,95-96.
73, 175-181.
73, 1031-1037.
13, 197-202.
310,810-815.

524 K. L. Clayton et a / .
diabetics during an episode of severe metabolic decompensation and during the recovery phase. Journal of Clinical Endocrinology and Metabolism, 60, 781-785.
Rogers, D.G., Sherman, L.D. & Gabbay, K.H. (1991) Effect of puberty on insulin like growth factor I and HbAl in Type 1 diabetes. Diabetes Care, 14, 1031-1035.
Salardi, S., Cacciari, E., Ballardini, D., Righetti, F., Capelli, M., Cicognani, A., Zucchini, S., Natali, G. & Tassinari, D. (1986) Relationship between growth factors (Somatomedin-C and growth hormone) and body development, metabolic control and retinal changes in children and adolescents with IDDM. Diabetes, 35, 832-836.
Clinical Endocrinology (1994) 41
Tanner, J.M. (1962) Growth at Adolescence. Blackwell Scientific Publications, Oxford.
Tanner, J.M., Whitehouse, R.H. & Takaishi M. (1966) Standards from birth to maturity for height, weight, height velocity and weight velocity: British Children 1965. Parts 1 and 2. Archives of Disease in Childhood, 41, 454-471; 613-635.
Taylor, A.M., Dunger, D.B., Grant, D.B. & Preece, M.A. (1988) Somatomedin-C/IGF-I measured by radioimmunoassay and somatomedin bioactivity in adolescents with insulin dependent diabetes mellitus compared with puberty matched controls. Diabetes Research, 9, 177-181.